Back to Journals » Drug Design, Development and Therapy » Volume 20
Liposomal Bupivacaine versus Ropivacaine with Dexamethasone in Rectus Sheath Block for Laparoscopic Gastrectomy: A Randomized Controlled Trial
Authors Yi K ![]() , Zhan Y, Wei A, Chen S, Zhang Y
, Zhan Y, Wei A, Chen S, Zhang Y ![]()
Received 16 October 2025
Accepted for publication 14 February 2026
Published 25 February 2026 Volume 2026:20 574724
DOI https://doi.org/10.2147/DDDT.S574724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Kun Yi,* Yanping Zhan,* Aiping Wei,* Shibiao Chen, Yang Zhang
Department of Anesthesiology, First Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shibiao Chen; Yang Zhang, Email [email protected]; [email protected]
Background: The optimal analgesia regimen for patients undergoing laparoscopic gastrectomy is still unclear. This study evaluated the efficacy of ultrasound-guided rectus sheath block (RSB) with liposomal bupivacaine in providing sustained and effective analgesia to enhance recovery after laparoscopic gastrectomy.
Methods: The study population comprised 102 individuals who underwent randomization to receive a rectus sheath block with one of the following: Ropivacaine-Dexamethasone (RD group), Liposomal Bupivacaine (LB group), or Liposomal Bupivacaine-Dexamethasone (LBD group). The primary efficacy measure was defined as total opioid consumption (within 72 hour postoperative), converted to morphine milligram equivalents (MME). Secondary outcomes included pain scores at rest and during movement (within 72 hours postoperatively), QoR-15-based recovery quality, perioperative satisfaction, inflammatory biomarker levels (preoperative, 24h and 72h postoperatively), PACU/hospital stay duration, and adverse events.
Results: The RD group had significantly higher total opioid consumption compared with the LB group and the LBD group. The LB group and the LBD group had significantly lower pain scores at rest and on movement at 12 h, 24 h, and 48 h after surgery, when compared with the RD group. The LB group and the LBD group had lower concentrations of Interleukin-1β (IL-1β) and interleukin-6 (IL-6) at 24 h compared with the RD group. In addition to reporting significantly better QoR-15 scores in the initial 48 hours, patients receiving liposomal bupivacaine (with or without dexamethasone) also experienced lower rates of PONV compared to the ropivacaine-dexamethasone cohort. Furthermore, there were no statistically significant differences between the three groups regarding length of post-anesthesia care unit stay, perioperative satisfaction, and length of hospital stay. There were no statistical differences between the LB group and the LBD group in all data. And the addition of dexamethasone to LBD provided no additional benefit over liposomal bupivacaine alone LB.
Conclusion: In conclusion, ultrasound-guided rectus sheath block with liposomal bupivacaine provided superior analgesia and reduced opioid consumption for up to 48 hours compared with a ropivacaine-dexamethasone regimen in patients undergoing laparoscopic gastrectomy. However, the addition of perineural dexamethasone to liposomal bupivacaine did not confer further analgesic benefit.
Trial Registration: www.chictr.org.cn: Identifier: ChiCTR2500098338.
Keywords: ropivacaine, liposomal bupivacaine, rectus sheath block, laparoscopic gastrectomy, acute postoperative pain, regional anesthesia
Introduction
The ultrasound-guided rectus sheath block is a cornerstone of multimodal analgesic regimens for midline incisions following abdominal surgery.1 Evidence confirms that RSB significantly reduces total opioid consumption and the incidence of key complications such as nausea, ileus, and sedation. By preserving motor function, it facilitates early ambulation and shorter urinary catheterization, directly contributing to Enhanced Recovery After Surgery (ERAS) protocols. Owing to its technical feasibility and favorable safety profile, ultrasound-guided RSB is well-established in ERAS pathways for gastrectomy and holds a Grade A recommendation (Evidence Level Ib) from the 2016 American Society of Regional Anesthesia and Pain Medicine (ASRA) guidelines.2–4
Despite its benefits, postoperative analgesia remains suboptimal. A multicenter survey of 26,193 surgical patients in China highlighted a critical need for improvement, revealing a 61.99% incidence of moderate-to-severe pain after gastrectomy.5 Inadequate acute pain management is a recognized risk factor for chronic postsurgical pain, which develops in approximately 12.6% of cases and can severely impede long-term recovery.6
The clinical utility of RSB in major abdominal surgery is often limited by the finite duration of conventional local anesthetics.7–10 This has driven the search for longer-acting options. Ropivacaine, with its differential sensory-motor blockade and superior cardiovascular safety, is a mainstay for RSB. However, its relatively low lipid solubility results in a moderate duration of action, typically 8–12 hours, which falls short of the sustained analgesic requirements for procedures like gastrectomy.11,12
To bridge this gap, research has focused on strategies to extend the analgesic window, primarily through perineural adjuvants and sustained-release formulations. Dexamethasone has emerged as a widely utilized adjuvant.13 When administered perineurally with local anesthetics, it prolongs analgesia by approximately 6–8 hours through multifactorial mechanisms, including the suppression of inflammatory mediators and modulation of neuronal excitability.12,14 Substantial evidence supports its efficacy and safety as an adjunct for nerve blocks in abdominal surgery, including gastrectomy.13,15–17
An alternative strategy is liposomal bupivacaine, an extended-release local anesthetic designed for single-dose administration to provide opioid-sparing analgesia. Approved by the US FDA in 2011 for surgical site infiltration and specific nerve blocks, it theoretically provides up to 72 hours of analgesia.18 While clinical studies demonstrate its superiority over placebo and standard bupivacaine in reducing pain and opioid consumption,19,20 recent evidence from various surgical models indicates that liposomal bupivacaine provides comparable analgesia to the combination of standard bupivacaine with dexamethasone, without demonstrating sustained superiority in pain reduction or opioid-sparing effects within the first 72 hours.11,21,22
Given the significant clinical demand for effective, prolonged analgesia after laparoscopic gastrectomy and the current lack of high-quality evidence directly comparing different local anesthetic regimens for rectus sheath block, we conducted this randomized trial to evaluate the analgesic efficacy of a liposomal bupivacaine–based rectus sheath block compared with an enhanced standard-of-care regimen (ropivacaine plus dexamethasone) in patients undergoing laparoscopic gastrectomy.
Materials and Methods
Ethics Statement
This prospective, single-center, double-masked, randomized controlled trial was conducted at the First Affiliated Hospital of Nanchang University (Nanchang, Jiangxi, na) between April and July 2025. The study protocol was approved by the Institutional Ethics Committee and registered at the Chinese Clinical Trial Registry (ChiCTR2500098338) on March 6, 2025. The study findings will be reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Patients
The study recruited consecutive candidates scheduled for elective laparoscopic radical gastrectomy at our institution. Inclusion criteria comprised an age range of 18–75 years, a body mass index (BMI) of 19.0–26.0 kg m−2, and an American Society of Anesthesiologists (ASA) physical status of I to III. Exclusion criteria was as follows: refusal of rectus sheath block, history of atopic disease or known allergy to experimental medication, abdominal wall skin lesions or infection, coagulopathy (INR>1.5 or beyond institutional laboratory reference ranges), chronic neuropathic pain, concurrent participation in other trials. Withdrawal criteria included: life-threatening local anesthetic systemic toxicity (LAST), drug-related serious adverse events, emergency intervention, or voluntary withdrawal.
Randomization and Blinding
Following written informed consent, 102 patients were randomly allocated in a 1:1:1 ratio to one of three groups: RD group, the LB group, and the LBD group via computer-generated randomization sequences (SAS 9.4 PROC PLAN), with allocation concealment maintained by an independent statistician. The study pharmacist prepared interventions in a dedicated medication room, with a total volume of 40 mL for each group. All solutions were loaded into identical black-light protective syringes (Becton Dickinson, USA) and sealed in sequentially numbered opaque envelopes. Upon patient arrival in the operating room, the anesthesiologist opened envelopes sequentially to perform blocks. A research assistant blinded to group assignment recorded data, ensuring double blinding (patients and operators).
Anesthetic Procedure
Anesthesia was induced with intravenous midazolam (0.05 mg kg−1), sufentanil (0.4 μg kg−1), 1.5–2 mg kg−1 propofol, and cisatracurium (0.3 mg kg−1). Following preoxygenation, perform endotracheal intubation under visualization. General anesthesia was maintained with target-controlled infusion of propofol and remifentanil, with bispectral index (BIS) values maintained between 40–60 through continuous titration of remifentanil.
All surgical procedures were performed by a single attending surgeon. Upon completion, patients were transferred to the post-anesthesia care unit (PACU) according to protocol. Postoperative analgesia was maintained via a sufentanil-based patient-controlled intravenous analgesia regimen (background infusion 0.1 mL h−1, bolus dose 2 μg, lockout interval 10 min, 4-hour maximum limit 0.6 μg kg−1). Supplemental analgesia with intravenous nefopam (20 mg) was administered at 6-hour intervals for breakthrough pain (Numerical Rating Scale score ≥4).
Interventions
Rectus Sheath Block Procedure
Following transfer to the anesthetic preparation room, all patients received standard monitoring (five-lead ECG, heart rate, non-invasive blood pressure, and pulse oximetry). Ultrasound-guided rectus sheath block (RSB) was performed by attending anesthesiologists or supervised residents using a high-frequency linear transducer. A 22-gauge, 80-mm needle was used to deposit the study solution between the posterior rectus sheath and the rectus muscle at the planned surgical incision site. (Figure 1)
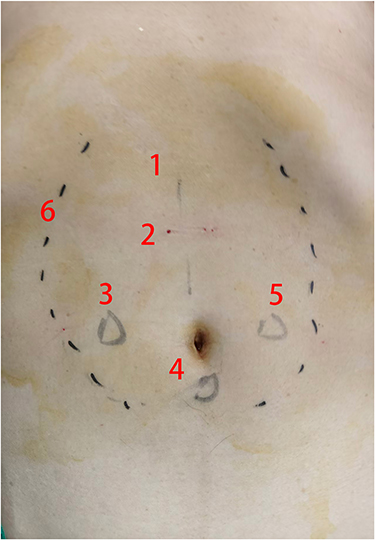 |
Figure 1 Block area of rectus sheath block. 1. Surgical Incision; 2. Needle Insertion Point; 3, 4, 5: Trocar Sites; 6. Area of Analgesia. |
Intervention Groups and Study Solutions
Patients were randomized to one of three intervention groups. All solutions were prepared aseptically immediately prior to administration. For groups containing liposomal bupivacaine, the solution was allowed to stand for 20 minutes per manufacturer’s instructions before use. RD Group (Ropivacaine–Dexamethasone): 20 mL of 0.75% ropivacaine (AstraZeneca, Sweden) mixed with 2 mg (2 mL) preservative-free dexamethasone (Fresenius Kabi, Germany) and 18 mL of 0.9% saline.
LB Group (Liposomal Bupivacaine): 20 mL (266 mg) of liposomal bupivacaine (13.3 mg/mL; Hengrui Pharmaceuticals, China) mixed with 20 mL of 0.9% saline. The final concentration was 0.665% (266 mg/40 mL). LBD Group (Liposomal Bupivacaine–Dexamethasone): 20 mL (266 mg) of liposomal bupivacaine mixed with 2 mg (2 mL) dexamethasone and 18 mL of 0.9% saline. The final concentration was 0.665% (266 mg/40 mL).
Administration Protocol
The total volume for all groups was 40 mL. A volume of 20 mL (10 mL per hemi-abdomen) was administered for the bilateral RSB. The remaining 20 mL was equally distributed (3 mL per site) for local infiltration at the five trocar puncture sites during wound closure. The injection rate was strictly limited to ≤0.5 mL/s. Block efficacy was assessed 30 minutes post-procedure via cold sensation testing with an ice cube.
Ultrasound-Guided RSB Procedure
Using a high-frequency linear-array ultrasound probe (Huasheng, Shenzhen, China), the ultrasound-guided RSB was performed with the patient in horizontal position. Following standard skin antisepsis, an experienced anesthesiologist positioned the linear probe along the anterior abdominal midline to identify the target hypoechoic plane between the posterior rectus sheath and the rectus abdominis epimysium, within the region extending from the xiphoid process to the umbilicus.
At the level of distance between the xiphoid process and the umbilicus, a puncture needle (Henan Tuoren, China) was inserted into the fascial plane between the rectus abdominis muscle and its posterior sheath. Following hydrodissection with 3 mL of normal saline to confirm needle position (Figure 2), patients in the RD, LB, and LBD groups respectively received a bilateral injection of 40 mL of 0.375% ropivacaine with 2 mg dexamethasone, 40 mL of 0.665% liposomal bupivacaine, or 40 mL of 0.665% liposomal bupivacaine with 2 mg dexamethasone.
 |
Figure 2 Ultrasound image of rectus sheath block. 1. Subcutaneous Tissue; 2. Needle; 3. Anterior Rectus Sheath; 4. Rectus Abdominis Muscle; 5. Local Anesthetic Solution / Drug Solution; 6. Posterior Rectus Sheath; 7. Peritoneum. |
Plasma Bupivacaine Concentration Assay
To assess the systemic absorption and safety profile of the studied regimens, venous blood samples (3 mL) were drawn from a separate peripheral line at 30min after intervention, 24h after surgery, 72h after surgery. Plasma was separated by centrifugation and stored at −80°C until analysis. Total bupivacaine (free + liposomal encapsulated) concentrations were quantified using high-performance liquid chromatography with tandem mass spectrometry (HPLC-MS/MS), with a lower limit of quantification of 0.01 μg/mL. The established safety threshold for potential systemic toxicity was set at 2.0 μg/mL. Ethics committee approval and patient informed consent were obtained for this section.
Outcomes
The primary outcome was total opioid consumption (including intraoperative remifentanil) converted to MME, calculated using CDC-specified conversion factors. Total opioid consumption was defined as the sum of all opioids administered from induction of anesthesia until 72 hours postoperatively, converted to morphine milligram equivalents (MME). This includes intraoperative remifentanil, as its total dose may reflect intraoperative nociceptive burden and has been used as a comprehensive metric of perioperative opioid exposure in similar regional anesthesia studies.23–25 The secondary outcomes included postoperative pain intensity (measured on a 0–10 NRS) assessed at predefined intervals over 72 hours both at rest and with movement (coughing); QoR-15-based recovery quality, incidence of PONV, total hospitalization Cost (CNY), time to tracheal extubation, incidence of nerve block-related adverse events, and incidence of local anesthetic systemic toxicity, anesthesia satisfaction (100 mm visual analog scale), PACU length of stay, discharge readiness (Post-Anesthesia Discharge Score), adverse events (graded per CTCAE v5.0), rescue analgesic consumption, and serum inflammatory factors (IL-6, TNF-α, IL-1β) at baseline and 24/72h postoperatively.
Statistical Analysis
Sample Size Determination
This was a superiority trial. The sample size was calculated for the primary outcome, total 72-hour postoperative opioid consumption in morphine milligram equivalents (MME). The calculation was based on pilot data from our institution, which indicated a standard deviation (SD) of approximately 12 MME. The minimum clinically important difference (MCID) was set at 15 MME. This value was derived as follows: Published evidence specific to abdominal surgery identifies an MCID of 10 MME over the first 24 postoperative hours as clinically meaningful.26–28 As our primary outcome extends over a 72-hour period, we reasoned that a clinically important effect should reflect a proportionally greater total opioid sparing. Therefore, we conservatively targeted a total reduction of 15 MME over 72 hours. This target aligns with the concept that a meaningful reduction in cumulative opioid exposure over a longer period requires a larger absolute saving, while remaining within a plausible and conservative range relative to the 24-hour benchmark. Using PASS software (NCSS LLC) for a one-way analysis of variance (ANOVA) F-test, with an effect size (f) of 0.417 (derived from SD=12 and mean difference=15), a two-sided alpha of 0.05, and 90% power, the analysis indicated a requirement of 27 participants per group. To account for a potential 20% attrition rate, we aimed to recruit 34 participants per group, resulting in a total target sample size of 102 participants.
Ultimately, 99 participants completed the trial and were included in the final analysis (34, 33, and 32 in LB, RD, and LBD groups, respectively), with only 3 participants lost to follow-up (actual attrition rate ~3%). This actual attrition was substantially lower than the anticipated 20%. Consequently, the final analyzed sample size (N=99) very closely approximates the target (N=102), which increases the effective power of the study beyond the initially planned 90%. Given that the primary outcome (total opioid consumption) exhibited a non-normal distribution and is appropriately presented as median (IQR) [RD: 95.66 (74.09–112.84); LB: 76.20 (69.45–81.51); LBD: 80.80 (66.28–88.77)], a conventional post-hoc power calculation based on means and standard deviations is not methodologically appropriate. However, the key determinants of power—sample size and data variability—favor our study: the achieved sample size is virtually identical to the powered target, and the observed IQRs indicate that the data variability is contained within a range comparable to our pre-trial estimate. Therefore, we are confident that the study maintained at least the planned 90% power to detect the pre-specified clinically important difference.
Outcome Measures
As detailed in the Outcomes section, the primary outcome was total opioid consumption (MME) from induction to 72 hours postoperatively. Key secondary outcomes included pain scores (NRS), QoR-15-based recovery quality, adverse events and incidence of PONV.
Statistical Methods
Continuous variables were presented as mean with standard deviation (SD) for normally distributed data or median with interquartile range (IQR) for non-normally distributed data. Normality was assessed using the Shapiro–Wilk test, supplemented by visual inspection of Q-Q plots. Homogeneity of variances was verified using Levene’s test. For the primary outcome (total opioid consumption), which exhibited a non-normal distribution, intergroup comparisons were performed using the Kruskal–Wallis test. When a significant difference was detected, Dunn’s test with Bonferroni correction was applied for post hoc pairwise comparisons. For secondary outcomes, if data satisfied parametric assumptions, one-way ANOVA followed by Tukey’s test was used. For data violating parametric assumptions, the Kruskal–Wallis test followed by Dunn’s test with Bonferroni correction was employed. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate. All hypothesis tests were two-sided with a significance level of α=0.05. Statistical analyses were performed using R language (version 4.3.0) and SPSS 27.0 (IBM Corp., Armonk, NY, USA).
Results
After the eligibility assessment of 184 patients, 102 were enrolled. Reasons for exclusion were failure to meet inclusion criteria (n=24) and declined participation (n=58).Overall, 102 patients were randomly assigned to three groups: RD group, LB group, and LBD group, and 2 patients in LBD and 1 in LB were excluded from final analysis due to protocol deviations (failure to complete >50% of scheduled follow-ups).Ultimately, 99 patients (34 in RD, 33 in LB, 32 in LBD) were included in statistical analysis and patient flow diagram was shown in Figure 3. There were no significant differences in baseline demographics between the groups (Table 1).
 |
Table 1 Patient Characteristics and Procedure Duration |
 |
Figure 3 Liposomal bupivacaine consolidated Standards of reporting Trials flow. |
Total Opioid Consumption (Primary Outcome)
Total opioid consumption outcomes are summarized in Figure 4a and Table 2 (stratified by postoperative day (POD) and overall). Overall median MME (IQR): 95.66 (74.09–112.84) for RD group, 76.20 (69.45–81.51) for LB group, and 80.80 (66.28–88.77) for LBD group. Kruskal–Wallis test revealed significant intergroup differences (P < 0.0001); post hoc Dunn test with Bonferroni adjustment confirmed higher consumption in RD versus LB (P < 0.0002) and LBD (P < 0.0017). Stratified by POD (Figure 4b): On POD1, significant differences existed (P=0.002) with higher MME in RD versus LB (P=0.002) and LBD (P=0.045); on POD2–3, differences remained significant (P=0.043 and P=0.045), but RD only showed lower consumption versus LB (P=0.043 and P=0.041). No differences were observed intraoperatively or in PACU (P=0.247 and P=0.430; Table 2). Notably, pairwise comparisons revealed no statistically significant differences in any measured outcomes—including total opioid consumption and pain scores at all time point—between the LB group and the LBD group (all P > 0.05 with Bonferroni correction). This indicates that the addition of dexamethasone to liposomal bupivacaine did not confer any detectable incremental analgesic benefit in this setting.
 |
Table 2 Opioid Consumption |
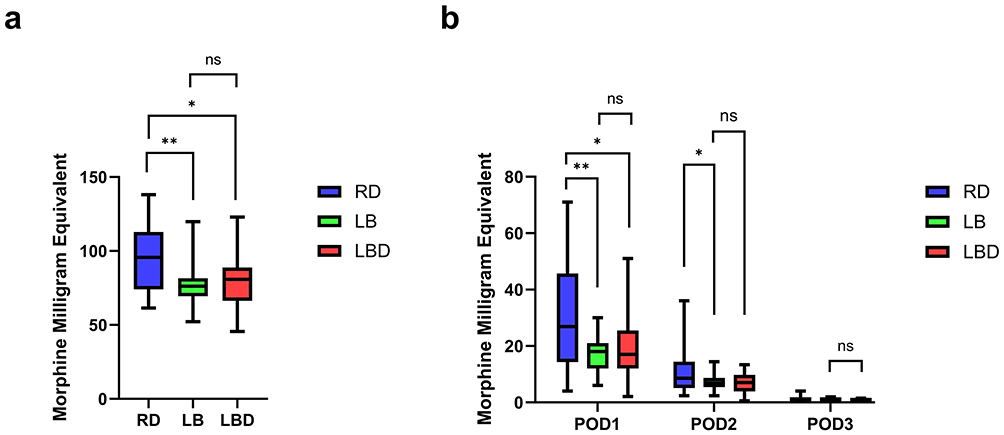 |
Figure 4 (a): Morphine Milligram Equivalents in Perioperative; (b) Morphine Milligram Equivalents in Postoperative 72h. * indicates P < 0.05, ** indicates P < 0.01, ns indicates not significant among two groups. |
Average Numerical Rating Scale Pain Score Over 3 Days
Postoperative pain assessment results (Table 3 and Figure 5) demonstrated that both the LB and LBD groups showed significantly lower NRS scores at rest at 12 h, 24 h, and 48 h postoperatively compared to the RD group (p < 0.0001, p = 0.022, and p = 0.031, respectively, Figure 5a). Similarly, during movement, the LB and LBD groups also exhibited significantly lower NRS scores at 12 h, 24 h, and 48 h compared to the RD group (p = 0.011, p = 0.037, and p = 0.043, respectively, Figure 5b).
 |
Table 3 Pain Interference Scores |
 |
Figure 5 (a) Resting Numerical Rating Scale Score Postoperative in Postoperative 72h; (b) Movement Numerical Rating Scale Score in Postoperative 72h. * indicates P < 0.05, **** indicates P < 0.0001. |
Plasma Bupivacaine Concentration
Plasma concentrations of bupivacaine remained well below the safety threshold of 2.0 μg/mL at all measured time points in both the LB and LBD groups. The median (IQR) concentrations were as follows: at 30 minutes post-block, 0.18 μg/mL (0.10–0.30) in the LB group versus 0.20 μg/mL (0.12–0.32) in the LBD group (p=0.65); then increase to 0.24 μg/mL (0.16–0.34) and 0.25μg/mL (0.15–0.32) at 24 hours (p=0.81); and were near the limit of quantification at 72 hours, with medians of 0.05 μg/mL (0.02–0.10) in both groups (p=0.93). No patient in any group exhibited signs or symptoms suggestive of local anesthetic systemic toxicity (LAST).
Postoperative Recovery Indicators and Adverse Events
As shown in Table 4 and Figure 6, QoR-15 scores demonstrated significant intergroup differences within 48 hours (p < 0.0001), but no significant difference was observed at 72 hours (p = 0.062). Specifically, on POD1, the RD group had significantly lower scores than the LB (85.2 vs 91.8, p = 0.00018) and LBD (85.2 vs91.6, p = 0.00024) groups, with significant overall difference (p < 0.0001). On POD2, the RD group still showed significantly lower scores than the LB (98.4 vs 105.2, p < 0.0001) and LBD (98.4 vs 103.5, p < 0.0001) groups, with significant overall difference (p < 0.0001). For recovery quality, no significant differences were observed among groups in time to tracheal extubation, PACU stay duration, total hospital costs, other postoperative adverse effects (fever, dizziness), perioperative satisfaction, or ERAS-related indicators (length of hospital stay, time to first flatus/defecation, time to first ambulation) (all p > 0.05,Table 4). Furthermore, no nerve block-related adverse events (eg, hematoma, local infection, neurological injury) were recorded in any patient and no clinical signs or symptoms suggestive of LAST occurred in any participant throughout the study period.
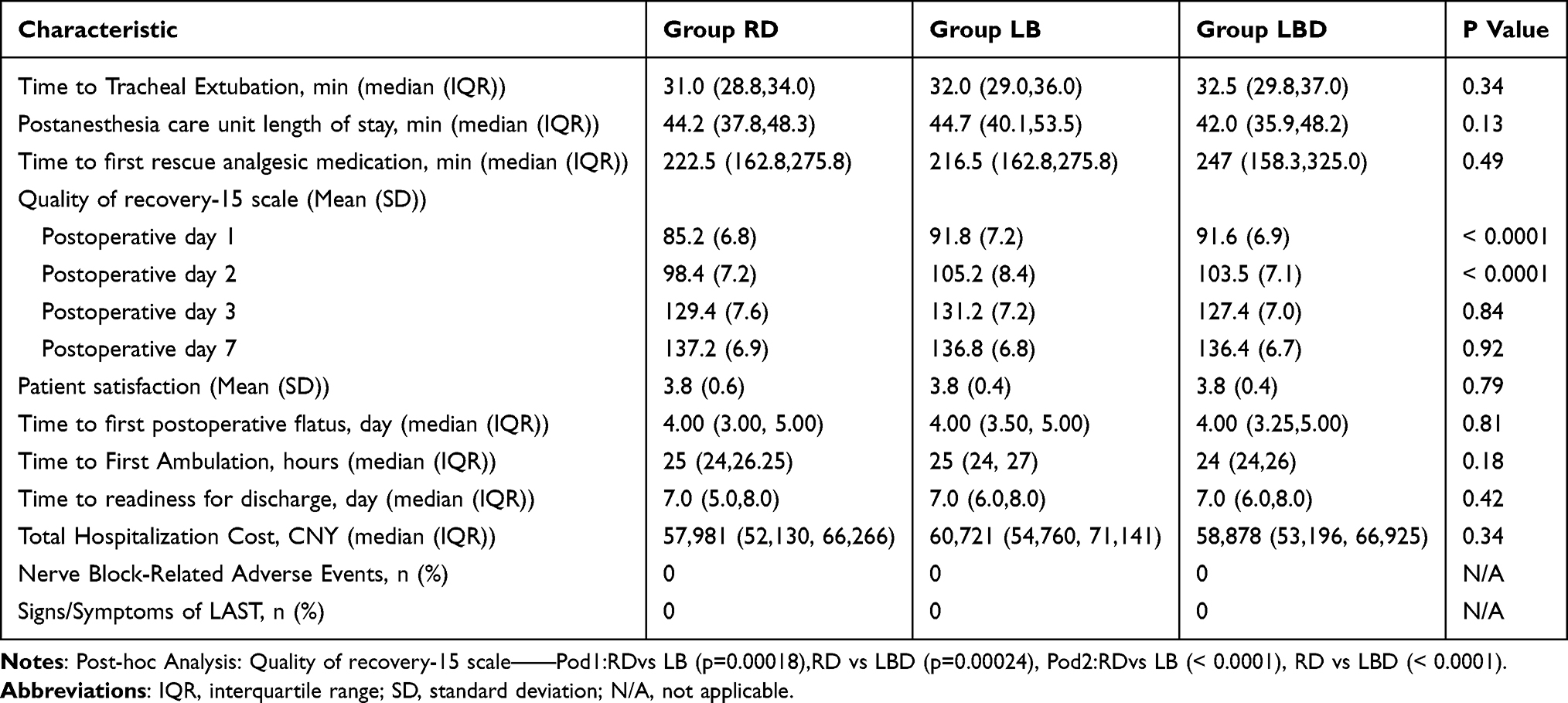 |
Table 4 Postoperative Recovery Indicators |
 |
Figure 6 Quality of recovery-15 score in Perioperative. **** indicates P < 0.0001. |
For the incidence of PONV, significant intergroup differences were observed within 48 hours (p < 0.05, Table 5), but these differences disappeared at 72 hours (p = 0.77). On postoperative day 1 (POD1), the RD group showed a significantly higher PONV incidence than both the LB (21% vs 9%, p = 0.042) and LBD (21% vs 6%, p = 0.038) groups, with significant overall intergroup difference (p = 0.043). This trend persisted on POD2, with the RD group exhibiting higher incidence than the LB (15% vs 6%, p = 0.047) and LBD (15% vs3%, p = 0.041) groups, showing significant overall difference (p = 0.049).
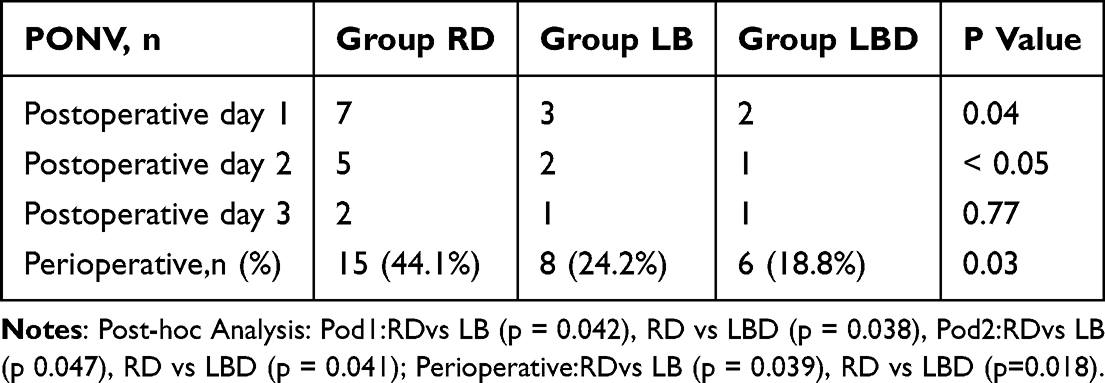 |
Table 5 Postoperative Nausea and Vomiting |
Inflammatory markers: IL-1β, IL-6 and TNF-α
Analysis of inflammatory markers (Table 6 and Figure 7) revealed significant intergroup differences in interleukin-1β (IL-1β) concentrations at 24 hours postoperatively (p = 0.0096, Figure 7a), with the RD group showing significantly higher levels versus LB group (p = 0.013) and LBD group (p = 0.008). Concurrently, interleukin-6 (IL-6) concentrations at 24 hours also differed significantly (p = 0.0093, Figure 7b and 7c), with RD exhibiting higher concentrations than LB (p = 0.012) and LBD (p = 0.007). No baseline differences were observed pre-intervention: IL-1β (p = 0.078, Figure 7a), IL-6 (p = 0.324, Figure 7c), and tumor necrosis factor-α (TNF-α) (p = 0.189, Figure 7d). At 24 hours postoperatively, TNF-α levels showed no significant differences (p = 0.792), and at 72 hours all inflammatory markers remained comparable across groups (IL-1β: p = 0.324; IL-6: p = 0.853; TNF-α: p = 0.838).
 |
Table 6 Concentrations of IL-1β, IL-6, TNF-α |
 |
Figure 7 (a) Concentration of IL-1β in Pre-intervention, Postoperative day 1 and Postoperative day 3; (b) Concentration of IL-6 in Postoperative day 1; (c) Concentration of IL-6 in Pre-intervention and Postoperative day 3; (d) Concentration of TNF-α in Pre-intervention, Postoperative day 1 and Postoperative day 3. * indicates P < 0.05, ** indicates P < 0.01; ns indicates not significant among three groups. |
Adjuvant Analgesics
Nefopam hydrochloride injection served as the foundational analgesic in this study, with dosage dynamically adjusted based on pain scores >4 (20mg incremental doses). As summarized in Table 7, the RD group demonstrated significantly higher daily nefopam consumption than both LB (median:45 mg vs 30 mg, IQR:40–52 vs 25–35, p<0.0001) and LBD (42.5 mg, IQR:38–48, p<0.0001) groups on postoperative day 1 (POD1), with significant overall intergroup difference (p<0.0001). On POD2, intergroup difference persisted (p=0.003) but RD only exceeded LBD (30 mg vs 22.5 mg, IQR:25–35 vs 20–25, p<0.005). Total 72-hour consumption analysis revealed RD (105mg, IQR:92–120) consumed significantly more than LB (75 mg, IQR:68–85, p<0.0001) and LBD (80 mg, IQR:72–90, p<0.0001). No intergroup differences were observed on POD3 (p=0.134).
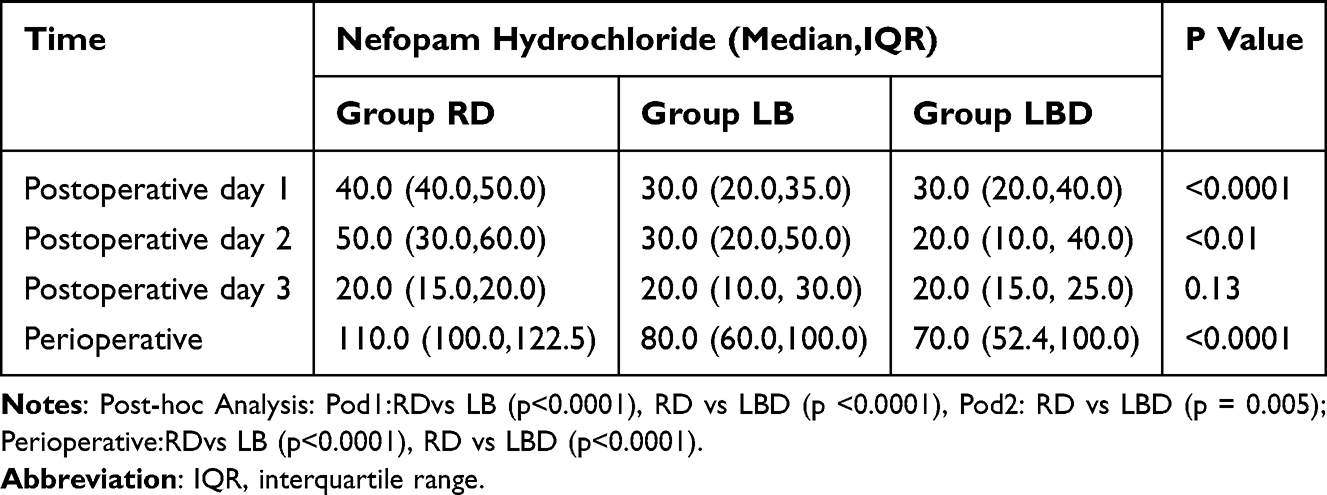 |
Table 7 Adjuvant Analgesia |
Discussion
Within the Enhanced Recovery After Surgery pathway for radical gastrectomy, multimodal analgesia strategies are employed to achieve effective postoperative pain control while minimizing opioid-related adverse effects. These approaches integrate regional anesthesia techniques—such as various nerve blocks—with non-opioid analgesics (eg, NSAIDs and nefopam hydrochloride injection) and local anesthetic adjuvants like dexmedetomidine. By doing so, they not only alleviate surgical pain but also help reduce complications such as nausea, vomiting, and ileus, thereby facilitating the recovery of gastrointestinal function and enhancing overall postoperative rehabilitation.2,3 Current evidence indicates that optimized multimodal analgesic protocols continue to evolve with the incorporation of advanced nerve blocks and adjuvant technologies. These developments have improved analgesic efficacy and decreased reliance on opioids. However, further research remains necessary to standardize technical details and adjuvant use, ensuring both safety and effectiveness across diverse patient populations.3
The analgesic benefits of conventional local anesthetics, even with adjuvants, are often limited to ≤24 hours. Liposomal bupivacaine addresses this limitation through a sustained-release mechanism, offering a novel strategy to extend analgesia beyond 24 hours.29,30 Building on this evidence, our study pioneers the combined perineural administration of liposomal bupivacaine and dexamethasone in RSB for patients undergoing gastrectomy. While some studies have compared liposomal bupivacaine to ropivacaine/dexamethasone mixtures in abdominal surgery, robust evidence specific to gastrectomy remains scarce. This randomized controlled trial therefore aims to compare perineural liposomal bupivacaine with ropivacaine-dexamethasone RSB, with the goal of informing clinical decision-making on optimized multimodal analgesia for gastric cancer surgery. The combination is supported by a favorable pharmacological profile. Existing evidence indicates no clinically significant pharmacokinetic interactions between liposomal bupivacaine and various co-administered medications, including corticosteroids, with no observed adverse synergistic effects.31 Pretrial pharmacokinetic data from our study confirmed that all measured plasma concentrations fell within established safety margins. Based on this safety profile, we included a liposomal bupivacaine-dexamethasone combination group to investigate potential therapeutic enhancement without compromising safety.
This randomized controlled trial systematically compared the analgesic efficacy and safety profiles of three regimens for ultrasound-guided rectus sheath block in patients undergoing laparoscopic gastrectomy: RD, LB alone, LBD. The primary finding was that the RD group required significantly higher total opioid consumption both overall and within the first 72 hours postoperatively compared to the LB and LBD groups. A stratified time-interval analysis further delineated this difference, revealing statistically significant reductions in opioid requirement for the liposomal bupivacaine groups at 24 and 48 hours, but not at 72 hours, confirming the sustained analgesic duration of liposomal bupivacaine formulations for up to 48 hours. Consistent with the opioid consumption data, both resting and activity-related NRS scores were significantly lower in the LB and LBD groups at 12, 24, and 48 hours postoperatively compared to the RD group, with no significant differences observed at other time points.
Regarding opioid sparing, a reduction of 10–15 MME is a proposed MCID in laparoscopic surgery.26–28 The median difference in total opioid consumption between the RD group and the LB group (approximately 19.5 MME) reached this clinically important threshold. Conversely, the difference between the LB and LBD groups was minimal and far below any plausible MCID. For postoperative pain measured on a 0–10 NRS, a reduction of 1.0 points is considered clinically meaningful.27,28 The differences in pain scores between the RD group and the liposomal bupivacaine groups at key time points met or exceeded this range, confirming that the analgesic superiority was not only statistical but also patient-relevant.
It is noteworthy that the consumption of the rescue analgesic nefopam also demonstrated significant intergroup differences during these same intervals, reinforcing the synergistic effect of a well-structured multimodal analgesia approach in clinical practice. Regarding safety, plasma concentrations of bupivacaine in both the LB and LBD groups remained consistently within the established safe threshold (below 2 μg mL⁻1) throughout the monitoring period, with no incidents of local anesthetic systemic toxicity recorded.
A pivotal and consistent finding of our study is the lack of significant difference between the LB and LBD groups across all efficacy endpoints. This null result carries substantial clinical relevance. Dexamethasone, while inexpensive, is used off-label as a perineural adjuvant and is not without potential concerns, such as transient hyperglycemia,32,33 especially in vulnerable populations. Our data suggest that when liposomal bupivacaine is employed for RSB, the routine addition of dexamethasone may not provide additional analgesic advantage within the first 72 postoperative hours. This challenges the assumption of a universal additive effect. Consequently, omitting dexamethasone from such regimens could simplify clinical practice by avoiding off-label use considerations, mitigate even minimal risks (eg, glycemic disturbances), and reduce unnecessary complexity and cost at a systemic level, all without compromising analgesic efficacy. The novelty of our work lies not only in demonstrating the efficacy of liposomal bupivacaine but also in providing evidence that questions the necessity of a common adjuvant in its context, thereby guiding more refined and cost-effective application.
The absence of an enhanced effect when dexamethasone was added to liposomal bupivacaine (LBD vs LB) warrants consideration. Dexamethasone is known to prolong analgesia primarily by inhibiting inflammatory mediators and reducing local edema, effects that are most potent in the early to intermediate phases of postoperative pain.12,34 In contrast, liposomal bupivacaine is designed to provide sustained analgesia over 72 hours or more through its unique depot release mechanism. It is plausible that the robust and prolonged analgesic “ceiling effect” provided by liposomal bupivacaine itself may have overshadowed any incremental benefit from dexamethasone within our 72-hour observation window. Furthermore, the primary mechanism of dexamethasone—delaying the onset of inflammatory pain—might have less measurable impact when the baseline blockade is already profoundly effective at suppressing nociceptive transmission across the entire critical postoperative period.
It is important to note that recent systematic reviews and meta-analyses have concluded that although liposomal bupivacaine demonstrates statistically superior performance in certain analgesic endpoints relative to traditional local anesthetics, these advantages do not consistently translate into clinically meaningful improvements; consequently, its overall clinical value remains a subject of debate.29,35–37 Current evidence suggests that liposomal bupivacaine provides enhanced analgesia over conventional agents within the first 24–48 hours after surgery. Nevertheless, the observed effect size—often corresponding to a mean reduction of less than 1 point on the NRS—generally falls below the established threshold for the minimal clinically important difference (MCID). Moreover, its influence on long-term recovery outcomes, such as hospital length of stay and functional recovery, appears limited. This ongoing controversy may be attributable to considerable heterogeneity among published studies, including differences in surgical procedures, nerve block techniques, and outcome assessment methods. In addition, the pharmacoeconomic implications—specifically, the balance between its substantially higher drug cost and its modest clinical benefits—represent a critical consideration that warrants further investigation.29,35–37
Notably, several recent studies have presented divergent perspectives on the analgesic efficacy of LB in TAP blocks. For instance, A retrospective study on lower abdominal surgeries found that using a mixture of LB and conventional bupivacaine (CB) for TAP blocks was not associated with reduced opioid consumption or improved pain control within 72 hours after elective abdominopelvic surgery.21 Similarly, a prospective randomized controlled trial in patients undergoing open hysterectomy detected no significant differences in total opioid usage or pain levels among LB, CB, and LB-CB mixture groups.38 Furthermore, a study comparing LB and CB for TAP blocks in bariatric surgeries (including laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy) demonstrated that LB did not significantly decrease total opioid consumption or pain scores.39 The discrepancy between these reports and the findings of the present study may be attributed to heterogeneity in surgical procedures, patient populations, outcome assessment methods, or technical aspects of the block itself. This inconsistency underscores the necessity for more precise patient selection criteria and standardized technical protocols to better define the specific clinical scenarios in which liposomal bupivacaine provides a clear and optimal analgesic benefit. In contrast to the conflicting reports, several studies have demonstrated favorable outcomes with liposomal bupivacaine. A recent systematic analysis of 22 clinical studies on laparotomy indicated that patients receiving LB-based TAP blocks during cesarean delivery under neuraxial anesthesia with intrathecal morphine exhibited significant opioid-sparing effects with comparable pain control. Notably, in such settings, LB abdominal wall blocks may represent a viable alternative when epidural analgesia is contraindicated.40 However, evidence for other laparotomy procedures remains inconclusive. Regarding RSB—the technique directly relevant to the present study—a case report described improved pain scores and earlier ambulation following conversion from laparoscopic appendectomy to open right hemicolectomy using LB RSB.41 Additionally, a case series involving three patients undergoing elective midline laparotomy documented sustained effective analgesia, both immediately after surgery and for up to two weeks, with ultrasound-guided LB RSB.42
Further supporting its potential, recent comparative studies have reported positive findings. A randomized trial in cesarean section patients found that TAP blocks performed with LB or an LB–plain bupivacaine mixture led to significantly better 24-hour postoperative recovery quality scores (assessed by the QoR-15 scale) than plain bupivacaine alone.43 Similarly, for patients undergoing robot-assisted hysterectomy, the LB group demonstrated significantly reduced 72-hour opioid consumption and lower maximum pain intensity at all time points compared to the CB group.44 Consistent results were observed in laparoscopic hand-assisted nephrectomy, where LB TAP blocks reduced opioid use between 48–72 hours and decreased maximum pain scores at the 24–48 h and 48–72h intervals.45 Collectively, the existing literature presents contradictory conclusions regarding the analgesic efficacy of liposomal bupivacaine. Given the evidence generated by our trial, further rigorous investigation in larger, more diverse patient populations is warranted to definitively evaluate the clinical utility and optimal application of liposomal bupivacaine.
Acknowledging the economic dimension, any formal cost-effectiveness analysis was beyond the scope of this study. However, a qualitative discussion is warranted. The primary cost driver is the high acquisition price of liposomal bupivacaine. Against this, our observed benefits—a median reduction of ~19.5 MME in opioid consumption and correspondingly lower pain scores—must be weighed. These benefits may translate into downstream cost offsets by potentially reducing opioid-related adverse effects (eg, nausea, sedation, ileus), simplifying nursing care, and facilitating earlier mobilization. Furthermore, our pivotal finding that adding dexamethasone (LBD) conferred no incremental benefit over LB alone suggests that a single-agent LB regimen could optimize value by avoiding unnecessary adjuvant cost and complexity. Ultimately, whether the magnitude of benefit justifies the cost in our setting likely depends on institutional pricing, patient-specific risk factors for severe pain or opioid-related complications, and the priority placed on opioid-sparing strategies. Future studies incorporating formal economic evaluations are needed to definitively answer this question.
Several limitations should be considered. First, while total opioid consumption is an objective endpoint, its inclusion of intraoperative remifentanil (with its ultra-short half-life) may dilute differences in strictly postoperative analgesic requirements. Second, the assessment of block success was performed under general anesthesia, which may limit the reliability of sensory testing. Third, this single-center study had a sample size powered for efficacy, which may limit generalizability and be underpowered for rare adverse events. Fourth, we did not perform a formal cost-effectiveness analysis, which is crucial given the high acquisition cost of liposomal bupivacaine. Fifth, the optimal dose of liposomal bupivacaine for this block remains undefined, and the perineural use of dexamethasone constitutes an off-label application, both of which present challenges for clinical adoption.
Conclusion
In conclusion, ultrasound-guided rectus sheath block with liposomal bupivacaine provided superior analgesia and reduced opioid consumption for up to 48 hours compared with a ropivacaine-dexamethasone regimen in patients undergoing laparoscopic gastrectomy. However, the addition of perineural dexamethasone to liposomal bupivacaine did not confer further analgesic benefit.
Abbreviations
RSB, Rectus Sheath Block; RD, Ropivacaine-Dexamethasone; LB, Liposomal Bupivacaine; LBD, Liposomal Bupivacaine-Dexamethasone; MME, morphine milligram equivalents; PONV, postoperative nausea and vomiting; ERAS, Enhanced Recovery After Surgery; PACU, post-anesthesia care unit; NRS, Numerical Rating Scale; CDC, Centers for Disease Control and Prevention; PCIA, patient-controlled intravenous analgesia; POD, postoperative day; TAP, transversus abdominis plane; CB, conventional bupivacaine.
Data Sharing Statement
For reasonable data requests, contact the corresponding authors (Dr Shibiao Chen and Yang Zhang) by Email ([email protected] and [email protected]).
Ethics Approval and Consent to Participate
Our study complies with the Declaration of Helsinki. This study was approved by the First Affiliated Hospital of Nanchang University registered in the Chinese Clinical Trial Registry. Written informed consent was obtained from each patient.
Acknowledgments
The authors acknowledge financial supports from National Natural Science Foundation of China (No. 82360385).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Finnerty O, Carney J, McDonnell JG. Trunk blocks for abdominal surgery. Anaesthesia. 2010;65(s1):76–17. doi:10.1111/j.1365-2044.2009.06203.x
2. Mortensen K, Nilsson M, Slim K, et al. Consensus guidelines for enhanced recovery after gastrectomy. Br J Surg. 2014;101(10):1209–1229. doi:10.1002/bjs.9582
3. Hu Y, Hsu AW, Strong VE. Enhanced Recovery After Major Gastrectomy for Cancer. Ann Surg Oncol. 2021;28(12):6947–6954. doi:10.1245/s10434-021-09906-y
4. Abrahams M, Derby R, Horn JL. Update on Ultrasound for Truncal Blocks: a Review of the Evidence. Reg Anesth Pain Med. 2016;41(2):275–288. doi:10.1097/AAP.0000000000000372
5. Liu Y, Xiao S, Yang H, et al. Postoperative pain-related outcomes and perioperative pain management in China: a population-based study. Lancet Reg Health West Pac. 2023;39:100822. doi:10.1016/j.lanwpc.2023.100822
6. Ding X, Ma Y, Ma Y, et al. Efficacy of nonopioid analgesics and regional techniques for perioperative pain management in laparoscopic gynecological surgery: a systematic review and network meta-analysis. Int J Surg Lond Engl. 2023;109(11):3527–3540. doi:10.1097/JS9.0000000000000630
7. Winnie L, Kao YH, Liao CC, Tamura T, Chang ML, Hsieh KY. Comparative Analgesic Efficacies of Ropivacaine and Bupivacaine for Postoperative Rectus Sheath Block in Paediatric Abdominal Surgery: a Meta-Analysis of Randomized Controlled Trial and Retrospective Cohort Studies. Pain Res Manag. 2021;2021:5535730. doi:10.1155/2021/5535730
8. Sinnott CJ, Strichartz GR. Levobupivacaine versus ropivacaine for sciatic nerve block in the rat. Reg Anesth Pain Med. 2003;28(4):294–303. doi:10.1016/s1098-7339(03)00188-3
9. Knudsen K, Beckman Suurküla M, Blomberg S, Sjövall J, Edvardsson N. Central nervous and cardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth. 1997;78(5):507–514. doi:10.1093/bja/78.5.507
10. McClure JH. Ropivacaine. Br J Anaesth. 1996;76(2):300–307. doi:10.1093/bja/76.2.300
11. Kim DH, Liu J, Beathe JC, et al. Interscalene Brachial Plexus Block with Liposomal Bupivacaine versus Standard Bupivacaine with Perineural Dexamethasone: a Noninferiority Trial. Anesthesiology. 2022;136(3):434–447. doi:10.1097/ALN.0000000000004111
12. Kalagac Fabris L. PRO AND CONTRA ON ADJUVANTS TO NEUROAXIAL ANESTHESIA AND PERIPHERAL NERVE BLOCKS. Acta Clin Croat. 2022;61(Suppl 2):57–66. doi:10.20471/acc.2022.61.s2.07
13. Pehora C, Pearson AM, Kaushal A, Crawford MW, Johnston B. Dexamethasone as an adjuvant to peripheral nerve block. Cochrane Database Syst Rev. 2017;2017(11):CD011770. doi:10.1002/14651858.CD011770.pub2
14. Kirkham KR, Jacot-Guillarmod A, Albrecht E. Optimal Dose of Perineural Dexamethasone to Prolong Analgesia After Brachial Plexus Blockade: a Systematic Review and Meta-analysis. Anesth Analg. 2018;126(1):270–279. doi:10.1213/ANE.0000000000002488
15. Zhang D, Zhou C, Wei D, Ge L, Li Q. Dexamethasone added to local anesthetics in ultrasound-guided transversus abdominis plain (TAP) block for analgesia after abdominal surgery: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2019;14(1):e0209646. doi:10.1371/journal.pone.0209646
16. Alsharari AF, Abuadas FH, Alnassrallah YS, Salihu D. Transversus Abdominis Plane Block as a Strategy for Effective Pain Management in Patients with Pain during Laparoscopic Cholecystectomy: a Systematic Review. J Clin Med. 2022;11(23):6896. doi:10.3390/jcm11236896
17. Zeng H, Yin F, Fan L, et al. Combination of dexamethasone and dexmedetomidine as adjuvants of transversus abdominis plane block for postoperative analgesia in gastric cancer patients: a double-blinded randomized controlled trial. J Clin Anesth. 2024;97:111543. doi:10.1016/j.jclinane.2024.111543
18. FDA. Drugs@FDA: FDA-Approved Drugs. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=BasicSearch.process.
19. Patel MA, Gadsden JC, Nedeljkovic SS, et al. Brachial Plexus Block with Liposomal Bupivacaine for Shoulder Surgery Improves Analgesia and Reduces Opioid Consumption: results from a Multicenter, Randomized, Double-Blind, Controlled Trial. Pain Med. 2019; pnz103. doi:10.1093/pm/pnz103.
20. Vandepitte C, Kuroda M, Witvrouw R, et al. Addition of Liposome Bupivacaine to Bupivacaine HCl Versus Bupivacaine HCl Alone for Interscalene Brachial Plexus Block in Patients Having Major Shoulder Surgery. Reg Anesth Pain Med. 2017;42(3):334–341. doi:10.1097/AAP.0000000000000560
21. Osuchukwu O, Gagnon J, Richard J, Craig W, Quaye A. Liposomal bupivacaine in transversus abdominis plane blocks for lower abdominal surgery. Pain Pract off J World Inst Pain. 2024;24(5):717–723. doi:10.1111/papr.13347
22. Ganguly K, Van Helmond N, Friedman A, et al. Liposomal Bupivacaine Versus Bupivacaine and Dexamethasone Intercostal Nerve Blocks for Robotic Thoracic Surgery: a Randomized Clinical Trial. Cureus. 2024;16(6):e62085. doi:10.7759/cureus.62085
23. La SCM, Liu R, Bharadwaj KM, et al. Association of Intraoperative Opioid Administration With Postoperative Pain and Opioid Use. JAMA Surg. 2023;158(8):854. doi:10.1001/jamasurg.2023.2009
24. Aguerreche C, Cadier G, Beurton A, et al. Feasibility and postoperative opioid sparing effect of an opioid-free anaesthesia in adult cardiac surgery: a retrospective study. BMC Anesthesiol. 2021;21(1):166. doi:10.1186/s12871-021-01362-1
25. Wu JX, Assel M, Vickers A, et al. Impact of intraoperative remifentanil on postoperative pain and opioid use in thyroid surgery. J Surg Oncol. 2019;120(8):1456–1461. doi:10.1002/jso.25746
26. Hong B, Jo Y, Baek S, Chung W, Oh C, Park S. Analgesic effects of transversus abdominis plane and quadratus lumborum blocks are not clinically meaningful for laparoscopic nephrectomy: systematic review and network meta-analysis. Korean J Pain. 2025;38(4):412–426. doi:10.3344/kjp.25147
27. Howle R, Ng SC, Wong HY, Onwochei D, Desai N. Comparison of analgesic modalities for patients undergoing midline laparotomy: a systematic review and network meta-analysis. Can J AnaesthesiaJournal Can Anesth. 2022;69(1):140–176. doi:10.1007/s12630-021-02128-6
28. Olsen MF, Bjerre E, Hansen MD, Hilden J, A E. Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017. doi:10.1186/s12916-016-0775-3
29. Ilfeld BM, Eisenach JC, Gabriel RA. Clinical Effectiveness of Liposomal Bupivacaine Administered by Infiltration or Peripheral Nerve Block to Treat Postoperative Pain. Anesthesiology. 2021;134(2):283–344. doi:10.1097/ALN.0000000000003630
30. Fallon F, Moorthy A, Skerritt C, Crowe GG, Buggy DJ. Latest Advances in Regional Anaesthesia. Medicina. 2024;60(5):735. doi:10.3390/medicina60050735
31. Kharitonov V. A Review of the Compatibility of Liposome Bupivacaine with Other Drug Products and Commonly Used Implant Materials. Postgrad Med. 2014;126(1):129–138. doi:10.3810/pgm.2014.01.2733
32. Dhatariya II K. Does dexamethasone-induced hyperglycaemia contribute to postoperative morbidity and mortality? Br J Anaesth. 2013;110(5):674–675. doi:10.1093/bja/aet010
33. Herbst RA, Telford OT, Hunting J, et al. The Effects of Perioperative Dexamethasone on Glycemic Control and Postoperative Outcomes. Endocr Pract. 2020;26(2):218–225. doi:10.4158/EP-2019-0252
34. Shishido H, Kikuchi S, Heckman H, Myers RR. Dexamethasone decreases blood flow in normal nerves and dorsal root ganglia. Spine. 2002;27(6):581–586. doi:10.1097/00007632-200203150-00005
35. Ilfeld BM, Sessler DI. Liposomal Bupivacaine in Peripheral Nerve Blocks: duration and Meaningful Differences. Anesthesiology. 2024;141(4):638–642. doi:10.1097/ALN.0000000000005133
36. Hussain N, Brull R, Sheehy B, et al. Perineural Liposomal Bupivacaine Is Not Superior to Nonliposomal Bupivacaine for Peripheral Nerve Block Analgesia: a Systematic Review and Meta-analysis. Anesthesiology. 2021;134(2):147–164. doi:10.1097/ALN.0000000000003651
37. Dinges HC, Wiesmann T, Otremba B, Wulf H, Eberhart LH, Schubert AK. The analgesic efficacy of liposomal bupivacaine compared with bupivacaine hydrochloride for the prevention of postoperative pain: a systematic review and meta-analysis with trial sequential analysis. Reg Anesth Pain Med. 2021;46(6):490–498. doi:10.1136/rapm-2020-102427
38. Fidkowski CW, Choksi N, Alsaden MR. A randomized-controlled trial comparing liposomal bupivacaine, plain bupivacaine, and the mixture of liposomal bupivacaine and plain bupivacaine in transversus abdominus plane block for postoperative analgesia for open abdominal hysterectomies. Can J Anaesth J Can Anesth. 2021;68(6):773–781. doi:10.1007/s12630-020-01911-1
39. Wong KA, Cabrera AG, Argiroff AL, et al. Transversus abdominis plane block with liposomal bupivacaine and its effect on opiate use after weight loss surgery: a randomized controlled trial. Surg Obes Relat Dis off J Am Soc Bariatr Surg. 2020;16(7):886–893. doi:10.1016/j.soard.2020.03.031
40. Vereen MS, Bidault VJ, Krabbendam E, Hoeks SE, Stolker RJ, Dirckx M. The effectiveness of liposomal bupivacaine in ultrasound‐guided abdominal wall blocks after open abdominal surgery: a systematic review. Pain Pract. 2025;25(3):e70016. doi:10.1111/papr.70016
41. Patzkowski MS, Stevens G. Multimodal analgesia in abdominal sepsis: a case report of liposome bupivacaine in ultrasound-guided rectus sheath blocks after unexpected open hemi-colectomy. Mil Med. 2015;180(6):e728–731. doi:10.7205/MILMED-D-14-00512
42. Vereen MS, Harms F, Stolker RJ, Dirckx M. Liposomal bupivacaine for ultrasound-guided rectus sheath blocks after midline laparotomy. Anaesth Rep. 2024;12(1):e12284. doi:10.1002/anr3.12284
43. Liu HH, Qiu D, Xu DR, Yang JJ, Teng PL. Recovery quality of transversus abdominis plane block with liposomal bupivacaine after cesarean delivery: a randomized trial. J Clin Anesth. 2024;99:111608. doi:10.1016/j.jclinane.2024.111608
44. Hutchins J, Delaney D, Vogel RI, et al. Ultrasound guided subcostal transversus abdominis plane (TAP) infiltration with liposomal bupivacaine for patients undergoing robotic assisted hysterectomy: a prospective randomized controlled study. Gynecol Oncol. 2015;138(3):609–613. doi:10.1016/j.ygyno.2015.06.008
45. Hutchins JL, Kesha R, Blanco F, Dunn T, Hochhalter R. Ultrasound-guided subcostal transversus abdominis plane blocks with liposomal bupivacaine vs. non-liposomal bupivacaine for postoperative pain control after laparoscopic hand-assisted donor nephrectomy: a prospective randomised observer-blinded study. Anaesthesia. 2016;71(8):930–937. doi:10.1111/anae.13502
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing Liposomal Bupivacaine and Ropivacaine in Serratus Anterior Plane Block for Thoracoscopic Lobectomy: A Randomized Controlled Trial
Zhang Y, Li W, Wei A, Chen S, Wang X
Drug Design, Development and Therapy 2025, 19:4717-4726
Published Date: 4 June 2025
The Emerging Role of Liposomal Bupivacaine in Erector Spinae Plane Blocks for Post-Operative Pain Management in Spine Surgeries: A Narrative Review
Delaney JB, Landry LP, Coggins NC, Ahmadzadeh S, Patil SS, Dorius B, Shekoohi S, Kaye AD
Clinical Pharmacology: Advances and Applications 2025, 17:339-346
Published Date: 22 December 2025
Effect of Liposomal Bupivacaine for Intercostal Nerve Block on Chronic Postoperative Pain Following Video-Assisted Thoracoscopic Lung Resection: A Retrospective Cohort Study
Yan J, Zhang Y, Tang HL, Li XY, Liu HY, Peng K, Liu H, Wang YQ, Ji FH, Shan XS
Drug Design, Development and Therapy 2026, 20:576594
Published Date: 25 March 2026