Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Lipoprotein(a) as a Risk Factor for Recurrent Ischemic Stroke in Type 2 Diabetes
Authors Chen R, Zhang K, Liu H, Liu L, Li H, Yan Y, Zhou Z, Meng C, Wang X, Wu H, Miao R, Wang R, Liu X ![]()
Received 23 October 2024
Accepted for publication 9 May 2025
Published 17 May 2025 Volume 2025:18 Pages 1631—1641
DOI https://doi.org/10.2147/DMSO.S502459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Ruomeng Chen,1,2 Kun Zhang,1,2 Hui Liu,1,2 Lijuan Liu,1,2 Hui Li,3 Yan Yan,1,2 Zhou Zhou,1,2 Chaoyue Meng,1,2 Xuelin Wang,4 Haoran Wu,4 Ruihan Miao,4 Rui Wang,1,2 Xiaoyun Liu1,2,4,5
1Department of Neurology, The First Hospital of Hebei Medical University, Shijiazhuang City, Hebei Province, People’s Republic of China; 2Department of Neurology, Hebei Hospital of Xuanwu Hospital Capital Medical University, Shijiazhuang City, Hebei Province, People’s Republic of China; 3Department of Neurology, Hengshui People’s Hospital, Hengshui City, Hebei Province, People’s Republic of China; 4Department of Neurology, The Second Hospital of Hebei Medical University, Shijiazhuang City, Hebei Province, People’s Republic of China; 5Neuroscience Research Center, Medicine and Health Institute, Hebei Medical University, Shijiazhuang City, Hebei Province, People’s Republic of China
Correspondence: Xiaoyun Liu, Department of Neurology, The First Hospital of Hebei Medical University, Shijiazhuang City, Hebei Province, People’s Republic of China, Email [email protected]
Objective: This study aimed to investigate the effect of LP(a) on recurrent ischemic stroke among persons with and without diabetes, providing a basis for the precise management of patients with recurrent ischemic stroke with diabetes in clinical practice.
Methods: This study was conducted on consecutive patients with cerebral infarction diagnosed between January 2019 and March 2023 in the Second Hospital of Hebei Medical University. Stratified analyses were performed according to LP(a) level (≤/> 90th percentile) and logistic regression modeling was performed to investigate the relationship between LP(a) and recurrent ischemic stroke with or without T2DM.
Results: In the final enrollment of 2029 patients, the number of recurrent ischemic stroke according to LP(a) > 90th percentile combined with T2DM was 59.15%, which was significantly higher than in LP(a) ≤ 90th percentile combined with T2DM (46.17%, P=0.039). After multivariate adjustment, LP(a) > 90th percentile emerged as an independent risk factor for patients with T2DM (OR=2.062, 95% CI 1.218– 3.489, P=0.007). In patients with large artery atherosclerotic ischemic stroke, LP(a) was an independent risk factor for recurrent ischemic stroke in diabetic patients (OR=2.553, 95%CI 1.385– 4.707, P = 0.003), while this was not in non-diabetic patients (P = 0.228).
Conclusion: LP(a) is an independent risk factor for recurrent ischemic stroke in the diabetic population but not in nondiabetic individuals. Simple categorization based on the presence or absence of comorbid T2DM significantly influences the association between LP(a) and recurrent ischemic stroke. Therefore, in clinical practice, for ischemic stroke patients with comorbid diabetes, the LP(a) level should be more strictly controlled.
Keywords: type 2 diabetes mellitus, lipoprotein(a), recurrent ischemic stroke
Introduction
Ischemic stroke is associated with high rates of recurrence, disability, and mortality. Despite significant advancements in the prevention and early treatment of ischemic stroke, its recurrence rates remain concerningly elevated.
Lipoprotein a (LP(a)) is a low-density lipoprotein variant produced in the liver and containing apolipoprotein(a), which is well-established risk factors for ischemic stroke,1 is also a major contributor to residual cardiovascular risk.2,3 Elevated LP(a) levels are associated with an increased risk of atherosclerotic plaque formation, thrombosis, and inflammation in the cerebrovascular system.4–6 Recent multiple studies have demonstrated that LP(a) can directly or indirectly contribute to the occurrence, development of ischemic stroke,7–9 which is a risk factor for stroke recurrence.10 LP(a) can affect the risk of stroke through various pathways. In terms of promoting inflammation, it is prone to oxidative modification, producing pro-inflammatory and pro-atherosclerotic substances, which sustain local inflammation.11 It can also promote the differentiation of pro-inflammatory M1 macrophages, leading to the production of various cytokines and chemokines that inhibit angiogenesis and affect vascular function.5 In terms of promoting thrombosis, LP(a) can influence platelet aggregation to facilitate thrombus formation.12–15 Moreover, it promotes the expression of pro-inflammatory cytokines, induces endothelial activation, affects the homeostasis of endothelial cells, leading to endothelial cell dysfunction, and increases the probability of stroke.11 Type 2 diabetes mellitus (T2DM) is independent risk factor for ischemic stroke.16 The chronic hyperglycemia and metabolic derangements characteristic of T2DM lead to endothelial dysfunction, abnormal lipid metabolism, and enhanced platelet aggregation, all of which promote the occurrence of ischemic stroke.17–19 Stroke patients with T2DM have a significantly higher risk of mortality and recurrent ischemic strokes compared to patients without diabetes.20 The effects of LP(a) on cardiovascular disease and its prognosis appears to vary across different diabetic states, and current studies remain controversial. As for cerebrovascular disease, elevated LP(a) are significantly associated with carotid atherosclerotic plaques in both patients with impaired fasting glucose or T2DM.21,22 Moreover, Previous studies have demonstrated that LP(a) is an independent predictor of recurrent cardiovascular events (CVE), which include cardiovascular death, non-fatal MI and stroke, in patients with T2DM who have a history of CVE.23 In terms of treatment, the search for more precise treatment regimens for diabetes and hyperlipidemia is still ongoing.24,25 In the field of biological research, nanomaterials have emerged prominently in drug delivery and may play a significant role in related treatments in the future. However, the impact of LP(a) on the recurrence of ischemic stroke in T2DM patients has not been fully investigated. This study aims to fill this knowledge gap by exploring the relationship between LP(a) and recurrent ischemic stroke in patients with T2DM, as well as whether the co-existence of LP(a) and T2DM increases the risk of recurrent ischemic stroke.
Materials and Methods
Study Population
This is a cross-sectional study, which was conducted at the Second Hospital of Hebei Medical University in northern China from January 1, 2019 to March 1, 2023. Ischemic stroke was defined as acute focal neurological deficit with radiological evidence of cerebral infarction.26 Our inclusion criteria are: Patients who met the diagnostic criteria for acute ischemic stroke according to the Chinese Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke 2018.27 Presence of acute focal neurological deficit symptoms, imaging evidence of cerebral infarction shown on diffusion weighted imaging (DWI) of cranial magnetic resonance imaging (MRI) or computed tomography (CT). According the Trial of Org 101072 in Acute Stroke Treatment (TOAST) classification,28 the etiologies of ischemic stroke patients were classified. The Patients who were hospitalized multiple times for cerebral infarction were defined as any infarctive event occurring 21 days after the initial ischemic stroke, lasting for more than 24 hours.29,30 Data from the last hospitalization was selected for analysis.
The study was approved by the Ethical Review Committee of the Second Hospital of Hebei Medical University, which waived the requirement for informed consent and patient consent to review medical records. The Institutional Review Committee waived informed consent as the analysis exclusively utilized anonymized data that posed minimal risks to patient privacy. Conducted in accordance with the principles of the Declaration of Helsinki, all patient related data were de-identified and handled confidentially. Only aggregated and anonymized data were used for analysis, ensuring patient identities remained unidentifiable. This approach meets ethical and legal requirements for protecting patient privacy while facilitating valuable research.
All patients diagnosed with cerebral infarction were screened for inclusion in the cohort. Exclusion criteria included (1) patients who did not meet the diagnostic criteria for cerebral infarction (2) patients lacking data on LP(a), and (3) patients with insufficient information: ①Neuroimaging Data, patients were excluded if they did not undergo brain MRI or intracranial vascular assessments (eg, MRA, CTA, or DSA).② Laboratory Data, patients were excluded if they lacked complete biochemical profiles, including: Routine blood tests, liver function tests, renal function tests, lipid profiles. For patients with multiple test data results, the first test result after hospitalization was selected. T2DM was defined as a previous history of diabetes or current use of hypoglycemic medication.
During the research process, we strictly adhered to the standard procedures. The data were all sourced from the electronic medical record system of the Second Hospital of Hebei Medical University. All the personnel involved in data collection underwent unified training and were familiar with the standards and processes of data collection. During the collection process, we used standardized data collection forms to clearly record information such as the collection time and collectors of each item of data. We collected information about the patients at the time of admission, including demographics, medical history, physical examination findings, laboratory results, and imaging data. Peripheral blood was collected from the antecubital vein for glucose, lipid, and LP(a) testing after 12 hours of fasting. Blood tests were routinely performed in the central laboratory of the hospital. Our center uses an automatic biochemical and immunological analyzer (LABOSPECT 008, HITACHI, Tokyo, Japan) to measure the concentration of LP(a) by immunoturbidimetry. The detection reagents are provided by Hitachi. Glycated hemoglobin was measured by immunagglutination method using the DCA2000 + HbA1c analyzer and kits from Siemens Corporation in the United States.
Statistical Analysis
Based on previous studies, among 2284 patients with diabetes, 55 patients experienced recurrent stroke.23 With α = 0.05 (two-sided) and 1 - β = 0.8 set, the calculated sample size is 528 cases, and we finally included 645 patients with diabetes. Continuous variables were described by mean ± standard deviation or interquartile range (IQR), while categorical variables were presented as counts and percentages. Differences between groups were analyzed using appropriate methods according to the characteristics and grouping of the variables. The chi-square test was applied for count data. Variables that did not meet the normality assumption were expressed as medians (quartiles), and nonparametric tests were employed for analysis of variance. In assessing the association between LP(a) level and recurrent ischemic stroke, we performed stratified analyses according to LP(a) level (≤90/>90th percentile). LP(a) percentile groupings have been previously used in studies published by other investigators,31–33 and it is appropriate to pool cohort-specific percentile groupings to minimize potential bias resulting from differences in absolute LP(a) levels observed among our different cohorts or assays examined in the current study. We screened for confounding variables through univariate analysis and only included the variables with P< 0.05 in the univariate analysis in the multivariate analysis. Binary logistic regression was used to analyze the relationship between LP(a) and recurrent ischemic stroke. Multivariate models were adjusted as follows: model 1: age, sex, hypertension; model 2: age, sex, hypertension, total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and apolipoprotein B (Apo(B)). Finally, the relationship between LP(a) and recurrent ischemic stroke in patients with LAA ischemic stroke with or without T2DM. Data were analyzed using SPSS software (version 26.0) and the R statistical package. Statistically significant was set at P<0.05.
Results
From January 1, 2019 to March 1, 2023, a total of 3010 patients diagnosed with ischemic stroke. Among them, 981 patients were excluded because they did not meet the inclusion and exclusion criteria. The results revealed that 645 patients were in the diabetic group and 1384 patients were in the non-diabetic group (Table 1). The proportion of males was significantly lower in the diabetic group than in the non-diabetic group (64.96% vs 70.52%, P=0.012). The proportion of recurrent ischemic stroke was significantly higher in the diabetic group compared to the non-diabetic group (47.6% vs 39.60%, P=0.001). Additionally, the prevalence of hypertension was significantly higher in the diabetic group (73.33% vs 67.77%, P=0.011). TC levels were lower in the diabetic group than in the non-diabetic group (3.98 mmol/L vs 4.06 mmol/L, P=0.015), while triglyceride(TG) levels were higher in the diabetic group (1.42 mmol/L vs 1.27 mmol/L, P<0.001). HDL levels were lower in the diabetic group (1.0 mmol/L vs 1.07 mmol/L, P<0.001), and LDL levels were also lower in the diabetic group (2.40 mmol/L vs 2.52 mmol/L, P=0.008). Furthermore, HbA1c levels were significantly higher in the diabetic group (6.8% vs 6.0%, P<0.001), and Apo(B) levels were higher in the diabetic group (0.90 g/L vs 0.87 g/L, P=0.022), LP(a) levels were lower in the diabetic group; however, the difference between the two groups was not statistically significant (13.33 mg/dl vs 14.62mg/dl, P=0.114), the distribution of LP(a) levels between the two groups is shown in Figure 1.
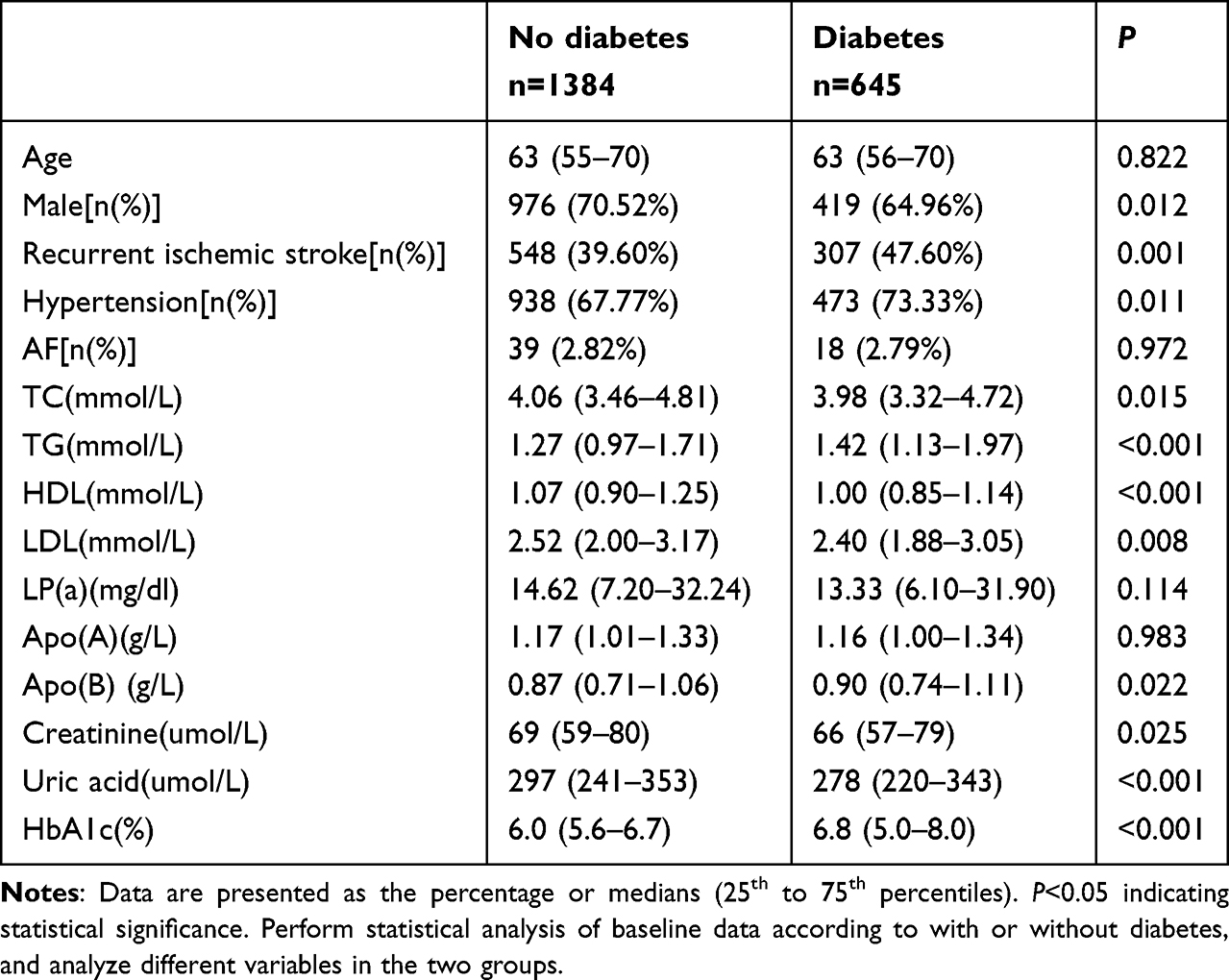 |
Table 1 Baseline Information of Patients in the Diabetic and Non-Diabetic Groups |
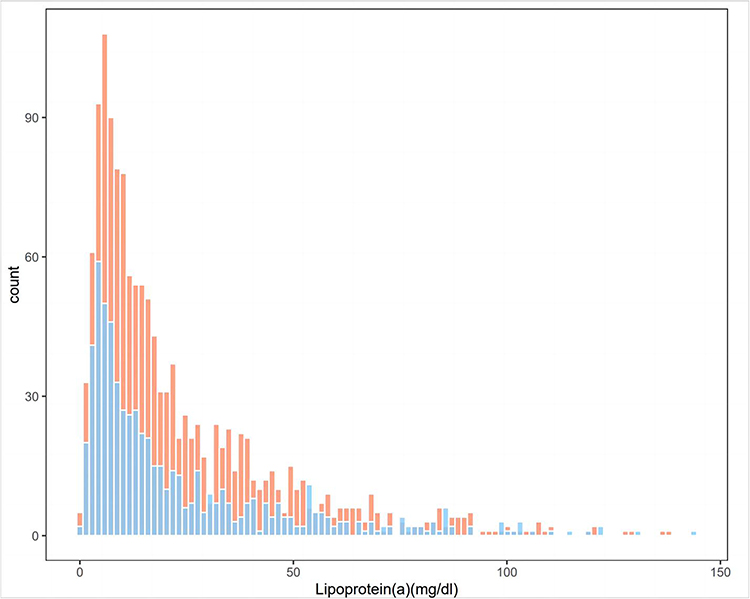 |
Figure 1 Distribution of LP(a) between the two groups. Notes: Distribution of LP(a) between the two groups with and without diabetes and LP(a) is lower in the diabetes group. Orange represents the non-diabetic group and blue represents the diabetic group. |
Grouped according to LP(a) (>/≤90th percentile, 55.46 mg/dl), statistical analysis of baseline data was performed (Table S1), and TC, HDL, LDL, and Apo(B) levels were significantly higher in the >90th percentile group than in the ≤90th percentile group. There was no statistically significant difference in the incidence of recurrent ischemic stroke, gender, hypertension, age, atrial fibrillation, creatinine, TG, Apo(A), and HbA1c between the two groups.
When analyzing the relationship between recurrent ischemic stroke and LP(a) levels in patients with and without diabetes, the groups were categorized according to the 90th percentile of LP(a) levels, as shown in Figure 2. In the non-diabetic group, the difference in recurrent ischemic strokes was not statistically significant in the groups with LP(a)≤90th percentile and LP(a)>90th percentile. However, in the diabetic group, the rate of recurrent ischemic stroke in the group with LP(a)>90th percentile was significantly higher than that in the LP(a)≤90th percentile group (P=0.039).
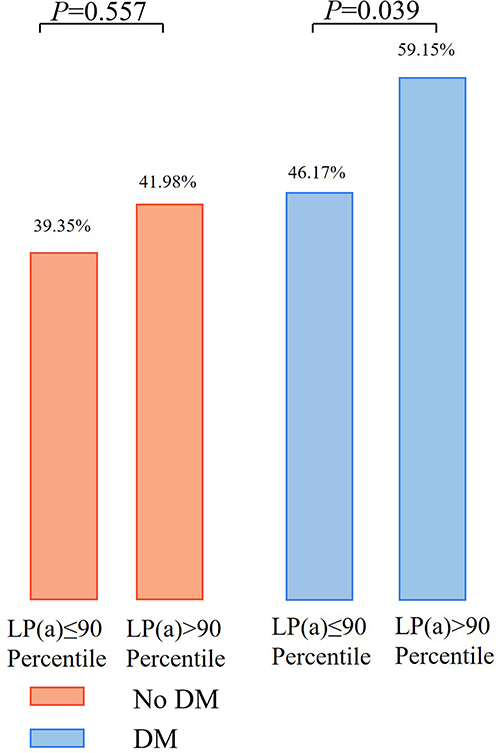 |
Figure 2 Incidence of recurrent ischemic stroke in LP(a) levels ≤90th percentile and >90th percentile in patients with and without diabetes. Notes: The incidence of recurrent ischemic stroke is the highest in the group of patients with diabetes and LP(a) levels >90th percentile. Orange represents the non-diabetic group and blue represents the diabetic group. |
To analyze the factors associated with recurrent ischemic stroke, we conducted a univariate analysis (Table 2). The results showed that in the non-diabetic group, there were significant differences in age, hypertension, TC, TG, LDL, Apo(B), and glycosylated hemoglobin between the two groups, while there was no statistically significant difference in LP(a). In the diabetic group, there were significant differences in age, atrial fibrillation, TC, TG, LDL, LP(a), Apo(B), and glycosylated hemoglobin between the two groups (Table 2).
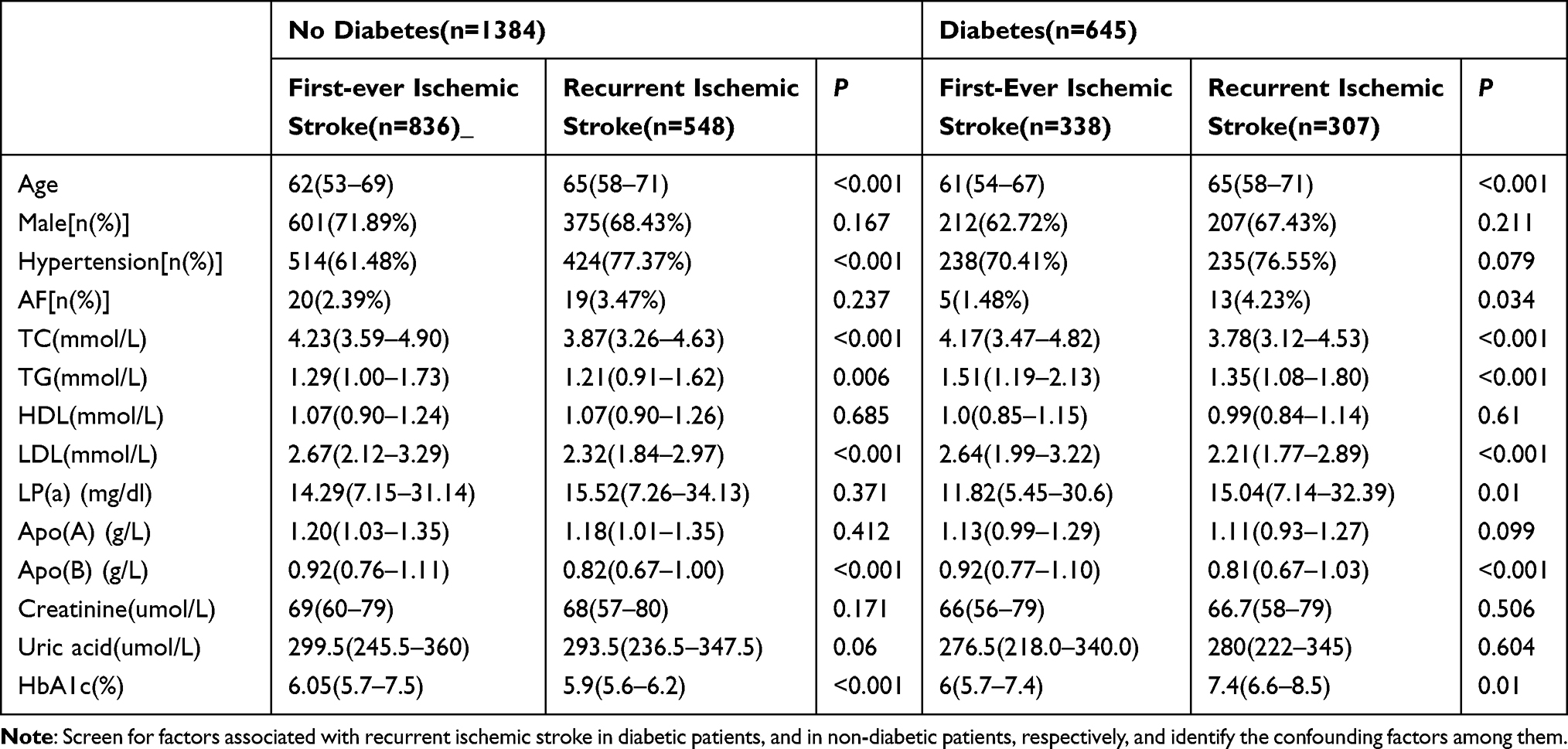 |
Table 2 Univariate Analysis Associated with Recurrent Ischemic Stroke in the Diabetic Group and Non-Diabetic Group |
Based on the results of the univariate analysis, to analyze the effect of LP(a) on ischemic stroke recurrence in patients with and without diabetes, binary logistic regression analysis was performed by grouping LP(a) levels (>/≤ 90th percentile), with the ≤ 90th percentile group serving as the control group (Table 3). The results showed that LP(a) level was a risk factor for recurrent ischemic stroke in patients with a history of diabetes (P=0.04, OR=1.689,95%CI 1.023–2.787). Age, gender, and hypertension were included as confounders in the analysis, and it was found that LP(a) level was an independent risk factor for recurrent ischemic stroke in patients with T2DM (OR=2.062,95%CI 1.218–3.489, P=0.07).
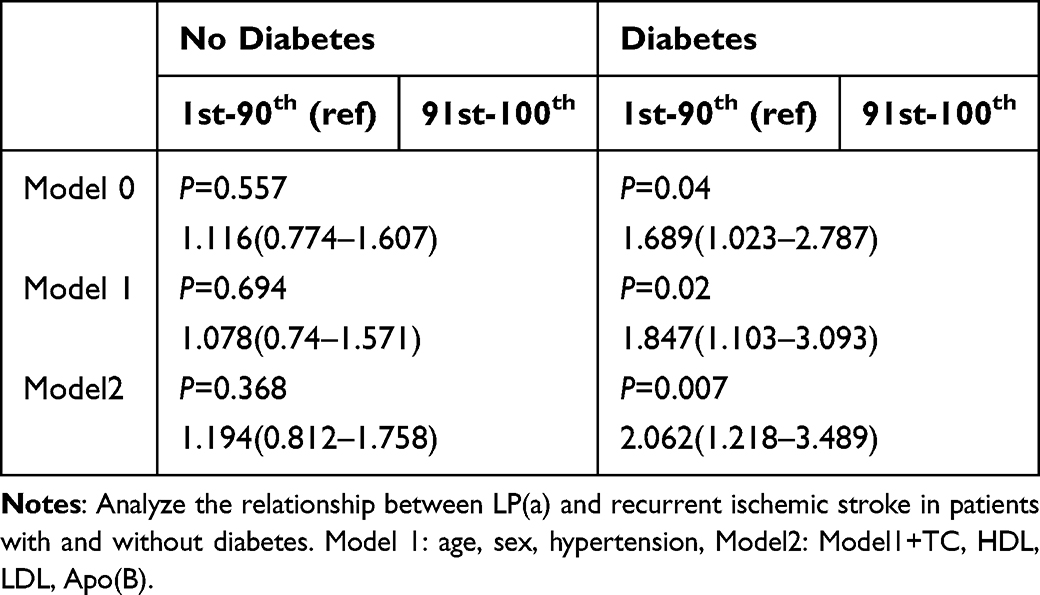 |
Table 3 Association of LP(a) with Recurrent Ischemic Stroke in Patients with and Without Diabetes |
To analyze the impact of LP(a) on recurrent ischemic stroke in diabetic patients with large artery atherosclerotic(LAA) ischemic stroke, we conducted a subgroup analysis. There were a total of 1463 cases of LAA ischemic stroke. The baseline data grouped according to LP(a) levels (> / ≤ 90th percentile, 55.46 mg/dl) are shown in Table 4. There were significant differences in recurrent stroke, TC, HDL, LDL, and Apo(B) between the two groups. A binary Logistic regression analysis was performed. The results showed that in patients with LAA ischemic stroke, LP(a) was an independent risk factor for recurrent ischemic stroke in diabetic patients (OR=2.553, 95%CI 1.385–4.707, P = 0.003), while this was not in non-diabetic patients (P = 0.228) (Table 5).
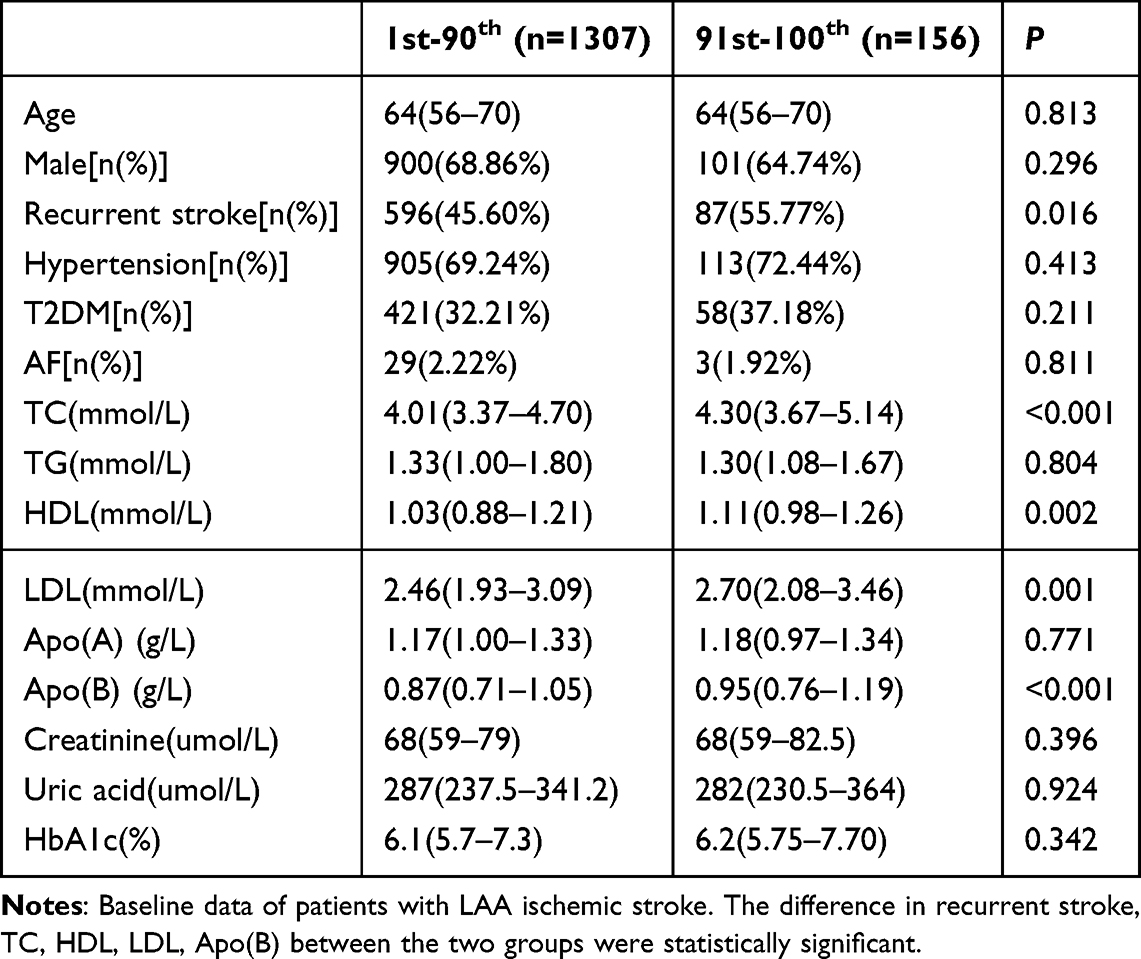 |
Table 4 Baseline of LAA Ischemic Stroke Grouped According to LP(a) Levels |
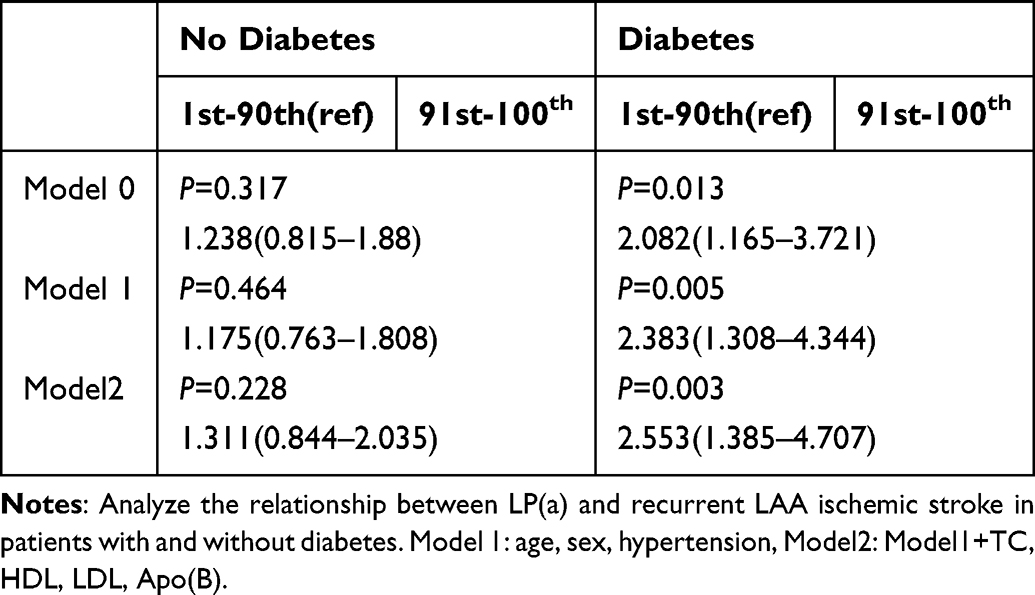 |
Table 5 Association of LP(a) with Recurrent LAA Ischemic Stroke in Patients with and Without Diabetes |
Discussion
This study assessed the effect of LP(a) on recurrent ischemic stroke in patients with and without diabetes. The main findings were as follows: the incidence of recurrent ischemic stroke was significantly higher in the diabetic group than in the nondiabetic group, and the highest incidence of recurrent ischemic stroke was observed in the presence of both T2DM and an elevated level of LP(a) (>90th percentile). LP(a) was an independent risk factor for recurrent ischemic stroke in patients with T2DM, but not in patients without T2DM. The same applies to patients with LAA ischemic stroke.
In our study, it was found that among the diabetic group, in the subgroup of patients with LP(a) > 90% percentile, the proportion of recurrent cerebral infarction was 59.15%, which was significantly higher than that in the patients with LP(a) ≤ 90% percentile (46.17%), in other words, when the LP(a) > 90% percentile and is accompanied by T2DM, patients have the highest recurrence rate in our study. Many recurrent stroke patients in our study were on statin therapy, primarily atorvastatin, which is known to slightly elevate LP(a) levels, possibly affecting the results. Atorvastatin can also reduce the level of LDL, which can explain why the level of LDL in the recurrent ischemic stroke group is lower. The reason why these patients still experience recurrence may be that although the average level of LDL is low, the proportion of patients who meet the secondary prevention criteria for cerebrovascular diseases may still be small. In addition, in the diabetes group, the HbA1c of patients with recurrent ischemic stroke increased significantly (7.4% vs 6.0%, P = 0.01), which means that the blood glucose levels of these patients are poorly controlled. Poor long- term management of blood glucose and lipid levels may be associated with the recurrence of ischemic stroke in patients.
In this study, it was found that the LP(a) level in the diabetic group was lower than that in the non-diabetic group (13.33mg/dl vs 14.62mg/dl), but the difference was not statistically significant. Previous studies have consistently found that the plasma LP(a) level in patients with T2DM is lower than that in the control group, which is consistent with the results of this study.34 This is known as the LP(a) paradox in T2DM.35 LP(a) is a large lipoprotein molecule formed by the covalent bonding of one Apo(a) molecule to one LDL molecule,2 and there is a complex relationship between LP(a) and T2DM. On one hand, low LP(a) levels have been associated with an increased risk of T2DM,36–38 especially in male patients over 60 years of age, where LP(a) levels greater than 28.72 mg/dl are considered low risk for T2DM.39 The 2022 consensus of the European Atherosclerosis Society clearly states that very low LP(a)levels are associated with an increased risk of incident T2DM.40 In an initial study, the risk of T2DM increased by 28% in the lowest quintile compared with the highest quintile of LP(a) levels.34 On the other hand, high LP(a) levels have been linked to an increased risk of diabetic vascular complications.41 Recent research has found that the level of LP(a) is a major risk factor for the formation of carotid artery plaques in patients with T2DM.41 Moreover, an elevated LP(a) level can increase the incidence and recurrence rate of CVEs in patients with T2DM.23,42 Currently, more evidence is needed to demonstrate the improvement of cardiovascular outcomes by reducing LP (a). There are few recommendations regarding the reduction of LP(a), and further clinical research is still required. In addition, whether reducing the level of LP(a) will increase the risk of developing diabetes needs further investigation.
In this study, elevated LP(a) was independently associated with recurrent ischemic stroke in diabetic patients but not in non-diabetes patients. The same result in the subgroup analysis of patients with LAA ischemic stroke. For one thing, existing research indicates that LP(a) is closely associated with an increased risk of microvascular and macrovascular complications in diabetic patients. There is a synergistic effect between elevated LP(a) levels and elevated blood glucose levels. This effect exacerbates the damage to the vascular endothelium, making diabetic patients more prone to vascular complications.43–45 In contrast, non-diabetic patients have fewer comprehensive cardiovascular risk factors compared to diabetic patients. This may endow their bodies with stronger tolerance to some weaker risk factors. Therefore, the recurrence of ischemic stroke in non-diabetic patients is less likely to be affected by weaker risk factors. These differences may explain why, in this study, the impact of LP(a) on recurrent ischemic stroke varies between diabetic and non-diabetic patients. Shiyovich et al pointed out that LP(a) is an independent risk factor for coronary atherosclerotic heart disease (CAD) in both diabetes and non - diabetic patients.46 A prospective study found that LP(a) ≥ 50 mg/dl predicts poor prognosis of ST-segment elevation myocardial infarction (STEMI) in patients with diabetes, but this is not the case in non-diabetic patients.47 Compared with other glucose metabolism states, patients with DM and high LP(a) have the highest risk of CVEs.48 However, a real-world study found that an elevated LP(a) level is associated with recurrent myocardial infarction or mortality in non-diabetic patients, but not in diabetic patients.49 Previous studies have also established a significant correlation between elevated LP(a) and carotid atherosclerosis in T2DM patients.21 In patients with CAD complicated by pre-diabetes or diabetes, elevated LP(a) levels are associated with an increased risk of recurrent CVEs. The recurrence aspect is consistent with the results of this study.42 In patients with T2DM who have a history of CVEs, LP(a) is an independent predictor of the recurrence of CVEs.23 The findings are consistent with those of this study, indicating that LP(a) is a risk factor for stroke recurrence in diabetes patients. Most of the research results suggest that when high-level LP(a) is combined with diabetes, it increases the risk of the occurrence and recurrence of cardiovascular diseases. Differences in study outcomes may be attributable to variations in study populations, LP(a) subgroup levels, and clinical endpoints.
In clinical practice, the management of patients with elevated LP(a) should be prioritized, especially in patients with comorbid T2DM. Incorporating LP(a) into risk assessment requires strict control of LP(a) levels. 90% of LP(a) levels are determined by the number of copy variants in the structural domains of the kringle IV4 type and by genetic factors related to the single-nucleotide polymorphisms of the LPA gene.50 While statin therapy may modestly elevate LP(a) levels,51 other therapies such as proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, Pelacarsen, Lepodisaran, Olpasiran lower LP(a) levels.52,53 Clinical trials have demonstrated that PCSK9 inhibitors reduce the incidence of cardiovascular events, and LP(a) monoclonal harvesting lowers LP(a) levels and reduces adverse cardiovascular events.54 However, it remains unclear whether lowering LP(a) increases the risk of developing T2DM, and further research is necessary to determine the long-term effects of LP(a)-lowering interventions on both cardiovascular and diabetic outcomes.
This study has several limitations. First, the study population was recruited from a single medical center in North China, which may introduce selection bias. Additionally, as a cross-sectional study, it cannot establish causal conclusions. The generalizability of the findings is limited by regional and population differences, and further investigation is required to extend the results to other populations. Moreover, the cross-sectional nature of the study precludes longitudinal follow-up, limiting the assessment of LP(a)’s long-term prognostic impact on stroke recurrence. The inclusion of patients on statin therapy prior to admission may have influenced the observed LP(a) levels and, consequently, the study results. Lastly, since the patients in our center did not routinely undergo long-term ambulatory electrocardiogram and electrocardiogram monitoring, it may have led to the missed diagnosis of some patients with AF, resulting in a low incidence of AF.
Conclusion
Elevated LP(a) levels were independently associated with the risk of recurrent ischemic stroke in diabetic patients but not in nondiabetic patients. This finding underscores the potential influence of diabetic status on the relationship between LP(a) and stroke recurrence. Given the strong association between LP(a) and ischemic stroke in diabetic individuals, measuring LP(a) and considering it in the comprehensive risk assessment of stroke recurrence is essential, particularly in those with T2DM who need to strictly control their LP(a) levels. Our results confirm that when the LP(a) levels is above the 90th percentile, it will increase the risk of stroke recurrence in T2DM patients. However, prospective clinical trials are needed in the future to clarify whether reducing LP(a) can decrease the risk of recurrent ischemic stroke in T2DM.
Abbreviations
T2DM, type 2 diabetes mellitus; LP(a), Lipoprotein a; CVE, cardiovascular events; MRI, Magnetic resonance imaging; DWI, diffusion weighted imaging; CT, computed tomography; AF, atrial fibrillation; TC, total cholesterol; TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein; Apo(B), apolipoprotein (B); Apo(A), apolipoprotein (A); PCSK9, proprotein convertase subtilisin/kexin type 9.
Data Sharing Statement
The datasets analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Committee of the second hospital of Hebei Medical University (Approval letter No:2023-R082). Informed consent was waived by the Institutional Review Board because the data had been anonymized.
Consent for Publication
All authors agree to publication.
Acknowledgments
We thank all the authors and team members who have helped us. Thanks to the corresponding author who guided us.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, giving insight/feedback and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The project was supported by the S&T Program of Hebei No.22377712D, The Hebei Provincial Department of Finance and the Health Commission ZF2024142, Hebei Provincial Health Commission Medical Science Research Project 20252051.
Disclosure
The authors declare that they have no competing interests.
References
1. Xu J, Hao X, Zhan R, et al. Effect of lipoprotein(a) on stroke recurrence attenuates at Low LDL-C (low-density lipoprotein) and inflammation levels. Stroke. 2022;53(8):2504–2511. doi:10.1161/STROKEAHA.121.034924
2. Tsimikas S. A test in context: lipoprotein(a): diagnosis, prognosis, controversies, and emerging therapies. J Ame College Cardiol. 2017;69(6):692–711. doi:10.1016/j.jacc.2016.11.042
3. Shah NP, Pajidipati NJ, McGarrah RW, et al. Lipoprotein (a): an update on a marker of residual risk and associated clinical manifestations. Am J Cardiol. 2020;126:94–102. doi:10.1016/j.amjcard.2020.03.043
4. Ugovšek S, Šebeštjen M. Lipoprotein(a)-the crossroads of atherosclerosis, atherothrombosis and inflammation. Biomolecules. 2021;12(1):26. doi:10.3390/biom12010026
5. Orsó E, Schmitz G. Lipoprotein(a) and its role in inflammation, atherosclerosis and malignancies. Clin Res Cardiol Supplements. 2017;12(Suppl 1):31–37. doi:10.1007/s11789-017-0084-1
6. Ferretti G, Bacchetti T, Johnston TP, Banach M, Pirro M, Sahebkar A. Lipoprotein(a): a missing culprit in the management of athero-thrombosis? J Cell Physiol. 2018;233(4):2966–2981. doi:10.1002/jcp.26050
7. Farina JM, Pereyra M, Mahmoud AK, et al. Current management and future perspectives in the treatment of Lp(a) with a focus on the prevention of cardiovascular diseases. Pharmaceuticals. 2023;16(7):919. doi:10.3390/ph16070919
8. Kosmas CE, Bousvarou MD, Papakonstantinou EJ, Zoumi EA, Rallidis LS. Lipoprotein (a) and cerebrovascular disease. J Int Med Res. 2024;52(7):3000605241264182. doi:10.1177/03000605241264182
9. Lange KS, Nave AH, Liman TG, Grittner U, Endres M, Ebinger M. Lipoprotein (a) levels and recurrent vascular events after first ischemic stroke. Stroke. 2017;48(1):36–42. doi:10.1161/STROKEAHA.116.014436
10. Feng Y, Zhang S, Li H, et al. Association of lipoprotein-associated phospholipase A2 and lipoprotein(a) with the risk of recurrence stroke in patients with acute ischemic stroke. J Clin Lab Anal. 2024;38(24):e25120. doi:10.1002/jcla.25120
11. Pirro M, Bianconi V, Paciullo F, Mannarino MR, Bagaglia F, Sahebkar A. Lipoprotein(a) and inflammation: a dangerous duet leading to endothelial loss of integrity. Pharmacol Res. 2017;119:178–187. doi:10.1016/j.phrs.2017.02.001
12. Desai K, Bruckdorfer KR, Hutton RA, Owen JS. Binding of apoE-rich high density lipoprotein particles by saturable sites on human blood platelets inhibits agonist-induced platelet aggregation. J Lipid Res. 1989;30(6):831–840. doi:10.1016/S0022-2275(20)38312-7
13. Ezratty A, Simon DI, Loscalzo J. Lipoprotein(a) binds to human platelets and attenuates plasminogen binding and activation. Biochemistry. 1993;32(17):4628–4633. doi:10.1021/bi00068a021
14. Rand ML, Sangrar W, Hancock MA, et al. Apolipoprotein(a) enhances platelet responses to the thrombin receptor-activating peptide SFLLRN. Arteriosclerosis Thrombosis Vasc Biol. 1998;18(9):1393–1399. doi:10.1161/01.ATV.18.9.1393
15. Boffa MB, Koschinsky ML. Lipoprotein (a): truly a direct prothrombotic factor in cardiovascular disease? J Lipid Res. 2016;57(5):745–757. doi:10.1194/jlr.R060582
16. Iwase M, Komorita Y, Ohkuma T, et al. Incidence of stroke and its association with glycemic control and lifestyle in Japanese patients with type 2 diabetes mellitus: the Fukuoka diabetes registry. Diabetes Res Clin Pract. 2021;172:108518. doi:10.1016/j.diabres.2020.108518
17. Kaur R, Kaur M, Singh J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: molecular insights and therapeutic strategies. Cardiovasc Diabetol. 2018;17(1):121. doi:10.1186/s12933-018-0763-3
18. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287(19):2570–2581. doi:10.1001/jama.287.19.2570
19. Nesto RW. Correlation between cardiovascular disease and diabetes mellitus: current concepts. Am J Med. 2004;116 Suppl 5 A:11s–22s. doi:10.1016/j.amjmed.2003.10.016
20. Kristensen FPB, Svane HML, Laugesen K, et al. Risk of mortality and recurrence after first-time stroke among patients with type 2 diabetes: a Danish nationwide cohort study. Eur Stroke J. 2024;2024:23969873241260956.
21. Jun JE, Kang H, Hwang YC, Ahn KJ, Chung HY, Jeong IK. The association between lipoprotein (a) and carotid atherosclerosis in patients with type 2 diabetes without pre-existing cardiovascular disease: a cross-sectional study. Diabetes Res Clin Pract. 2021;171:108622. doi:10.1016/j.diabres.2020.108622
22. Wang J, Sun H, Wang Y, An Y, Liu J, Wang G. Glucose metabolism status modifies the relationship between lipoprotein(a) and carotid plaques in individuals with fatty liver disease. Front Endocrinol. 2022;13:947914. doi:10.3389/fendo.2022.947914
23. Zhang Y, Jin JL, Cao YX, et al. Lipoprotein (a) predicts recurrent worse outcomes in type 2 diabetes mellitus patients with prior cardiovascular events: a prospective, observational cohort study. Cardiovasc Diabetol. 2020;19(1):111. doi:10.1186/s12933-020-01083-8
24. Pattnaik S, Thalluri C, Swain K. Rise of gold nanoparticles as carriers of therapeutic agents. Acta Chimica Slovenica. 2023;70(4):467–478. doi:10.17344/acsi.2023.8216
25. Garcia DA, Pierre AF, Quirino L, et al. Lipid nanoparticle delivery of TALEN mRNA targeting LPA causes gene disruption and plasma lipoprotein(a) reduction in transgenic mice. Mol Ther. 2025;33(1):90–103. doi:10.1016/j.ymthe.2024.11.020
26. Stacey A, Toolis C, Ganesan V. Rates and risk factors for arterial ischemic stroke recurrence in children. Stroke. 2018;49(4):842–847. doi:10.1161/STROKEAHA.117.020159
27. Chinese Society of Neurology CSS. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin J Neurol. 2018;51(9):666–682.
28. Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
29. Chen Y, Wright N, Guo Y, et al. Mortality and recurrent vascular events after first incident stroke: a 9-year community-based study of 0·5 million Chinese adults. Lancet Glob Health. 2020;8(4):e580–e590. doi:10.1016/S2214-109X(20)30069-3
30. Hankey GJ, Jamrozik K, Broadhurst RJ, et al. Long-term risk of first recurrent stroke in the Perth community stroke study. Stroke. 1998;29(12):2491–2500. doi:10.1161/01.STR.29.12.2491
31. Shiyovich A, Berman AN, Besser SA, et al. Association of lipoprotein (a) and standard modifiable cardiovascular risk factors with incident myocardial infarction: the mass general Brigham Lp(a) registry. J Ame Heart Assoc. 2024;13(10):e034493. doi:10.1161/JAHA.123.034493
32. Li S, Liu HH, Zhang Y, et al. Prognostic role of lipoprotein(a) in atherosclerotic cardiovascular disease risk from a perspective on current risk stratification. MedComm. 2024;5(11):e773. doi:10.1002/mco2.773
33. Wong ND, Fan W, Hu X, et al. Lipoprotein(a) and long-term cardiovascular risk in a multi-ethnic pooled prospective cohort. J Ame College Cardiol. 2024;83(16):1511–1525. doi:10.1016/j.jacc.2024.02.031
34. Mora S, Kamstrup PR, Rifai N, Nordestgaard BG, Buring JE, Ridker PM. Lipoprotein(a) and risk of type 2 diabetes. Clin Chem. 2010;56(8):1252–1260. doi:10.1373/clinchem.2010.146779
35. Kostner KM, Kostner GM. Lp(a) and the risk for cardiovascular disease: focus on the Lp(a) paradox in diabetes mellitus. Int J Mol Sci. 2022;23(7):3584. doi:10.3390/ijms23073584
36. Tsamoulis D, Kosmas CE, Rallidis LS. Is inverse association between lipoprotein(a) and diabetes mellitus another paradox in cardiometabolic medicine? Expert Rev Endocrinol Metab. 2024;19(1):63–70. doi:10.1080/17446651.2023.2293108
37. Liu W, Zhang G, Nie Z, et al. Low concentration of lipoprotein(a) is an independent predictor of incident type 2 diabetes. Hormone Metab Res. 2024;56(7):504–508. doi:10.1055/a-2316-9124
38. Pablo C, Matías A, Lavalle Cobo A, Sergio G, Federico RN. Exploring the interplay between diabetes and Lp(a): implications for cardiovascular risk. Current Diabetes Rep. 2024;24(7):167–172. doi:10.1007/s11892-024-01543-5
39. Fu Q, Hu L, Xu Y, Yi Y, Jiang L. High lipoprotein(a) concentrations are associated with lower type 2 diabetes risk in the Chinese Han population: a large retrospective cohort study. Lipids Health Dis. 2021;20(1):76. doi:10.1186/s12944-021-01504-x
40. Kronenberg F, Mora S, Stroes ESG, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022;43(39):3925–3946.
41. Chen J, Li W, Cao J, Lu Y, Wang C, Lu J. Risk factors for carotid plaque formation in type 2 diabetes mellitus. J Transl Med. 2024;22(1):18. doi:10.1186/s12967-023-04836-7
42. He J, Yang M, Song C, et al. Lipoprotein(a) is associated with recurrent cardiovascular events in patients with coronary artery disease and prediabetes or diabetes. J Endocrinol Invest. 2024;47(4):883–894. doi:10.1007/s40618-023-02203-3
43. Lamina C, Ward NC. Lipoprotein (a) and diabetes mellitus. Atherosclerosis. 2022;349:63–71. doi:10.1016/j.atherosclerosis.2022.04.016
44. Ren X, Zhang Z, Yan Z. Association between lipoprotein (A) and diabetic nephropathy in patients with type 2 diabetes mellitus: a meta-analysis. Front Endocrinol. 2021;12:633529. doi:10.3389/fendo.2021.633529
45. Moosaie F, Firouzabadi FD, Abouhamzeh K, et al. Lp(a) and Apo-lipoproteins as predictors for micro- and macrovascular complications of diabetes: a case-cohort study. Nutr Metab Cardiovasc Dis. 2020;30(10):1723–1731. doi:10.1016/j.numecd.2020.05.011
46. Shiyovich A, Berman AN, Besser SA, et al. Lipoprotein(a) as a cardiovascular risk factor among patients with and without diabetes mellitus: the mass general Brigham Lp(a) registry. Cardiovasc Diabetol. 2024;23(1):257. doi:10.1186/s12933-024-02348-2
47. Li N, Zhou J, Chen R, et al. Prognostic impacts of diabetes status and lipoprotein(a) levels in patients with ST-segment elevation myocardial infarction: a prospective cohort study. Cardiovasc Diabetol. 2023;22(1):151. doi:10.1186/s12933-023-01881-w
48. Jin JL, Cao YX, Zhang HW, et al. Lipoprotein(a) and cardiovascular outcomes in patients with coronary artery disease and prediabetes or diabetes. Diabetes Care. 2019;42(7):1312–1318. doi:10.2337/dc19-0274
49. Silverio A, Cancro FP, Di Maio M, et al. Lipoprotein(a) levels and risk of adverse events after myocardial infarction in patients with and without diabetes. J Thrombosis Thrombolysis. 2022;54(3):382–392. doi:10.1007/s11239-022-02701-w
50. Wilson DP, Jacobson TA, Jones PH, et al. Use of lipoprotein(a) in clinical practice: a biomarker whose time has come. A scientific statement from the national lipid association. J Clin Lipidol. 2019;13(3):374–392. doi:10.1016/j.jacl.2019.04.010
51. Tsimikas S, Gordts P, Nora C, Yeang C, Witztum JL. Statin therapy increases lipoprotein(a) levels. Eur Heart J. 2020;41(24):2275–2284. doi:10.1093/eurheartj/ehz310
52. Bittner VA, Szarek M, Aylward PE, et al. Effect of alirocumab on lipoprotein(a) and cardiovascular risk after acute coronary syndrome. J Ame College Cardiol. 2020;75(2):133–144. doi:10.1016/j.jacc.2019.10.057
53. Fichtner I, Macchi C, Rizzuto AS, Carugo S, Corsini A, Ruscica M. Lipoprotein(a) and the atherosclerotic burden - Should we wait for clinical trial evidence before taking action? Atherosclerosis Plus. 2024;58:16–23. doi:10.1016/j.athplu.2024.09.004
54. Schumann F, Kassner U, Spira D, et al. Long-term lipoprotein apheresis reduces cardiovascular events in high-risk patients with isolated lipoprotein(a) elevation. J Clin Lipidol. 2024;18(5):e738–e745. doi:10.1016/j.jacl.2024.04.134
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.