Back to Journals » Infection and Drug Resistance » Volume 15
Linezolid-Induced Pancytopenia in Patients Using Dapagliflozin: A Case Series
Authors Li MM, Shen WC, Li YJ, Teng J ![]()
Received 21 May 2022
Accepted for publication 3 September 2022
Published 19 September 2022 Volume 2022:15 Pages 5509—5517
DOI https://doi.org/10.2147/IDR.S375694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Meng Mei Li,1 Wen Cheng Shen,2 Yu Jin Li,1 Jun Teng1
1Qingdao Central Hospital, The Second Affiliated Hospital of Medical College of Qingdao University, Qingdao, People’s Republic of China; 2Department of Emergency, Qingdao Municipal Hospital (Group), Qingdao, People’s Republic of China
Correspondence: Jun Teng, Email [email protected]
Background: Linezolid is classed as oxazolidinone antibiotics which can be used to treat severe infections caused by vancomycin-resistant Enterococcus faecium, hospital-acquired pneumonia caused by Staphylococcus aureus, complicated skin, and uncomplicated skin structure infections (SSSIs) caused by methicillin-susceptible S. aureus or Streptococcus pyogenes, and community-acquired pneumonia caused by Streptococcus pneumoniae. However, many studies have suggested it can also cause thrombocytopenia and pancytopenia.
Patients and Methods: We report on three patients with linezolid-pancytopenia. Patients in cases 1 and 2 were diagnosed with heart failure with preserved ejection fraction (HFpEF) and were both administered with dapagliflozin, one of the sodium-dependent glucose transporters 2 inhibitors (SHLT-2i).
Results: Two patients were diagnosed with type 2 diabetes, pneumonia, and hyponatremia. Severe myelosuppression occurred in both patients, with a severe decrease in leukocytes and platelets and a moderate decrease in hemoglobin, who eventually passed away despite the discontinuation of linezolid and adopting appropriate treatment measures. The patient in case 3 was diagnosed with pneumonia, type 2 diabetes, and sequelae of cerebral thrombosis. After twelve days of treatment, the patient developed moderate thrombocytopenia and anemia. She recovered without any additional treatment after the discontinuation of linezolid.
Conclusion: In this case series, two patients with irreversible myelosuppression were treated with both linezolid and SGLT-2i, and one diabetic patient with single linezolid use presented with reversible pancytopenia, suggesting that SGLT-2i may exacerbate myelosuppression of linezolid. Linezolid should be used with caution in infectious patients with a history of SGLT-2i. We will conduct relevant animal experiments to clarify the interaction between the two drugs.
Keywords: linezolid, pancytopenia, SGLT-2 inhibitor, HFpEF
Introduction
Vancomycin is the first choice for methicillin-resistant Staphylococcus aureus (MRSA), methicillin-resistant Staphylococcus epidermidis (MRSE), Enterococcus faecalis, and Enterococcus faecium. However, recent studies demonstrated that vancomycin AUC/MIC of ≥400 mg·h/L and vancomycin trough levels of >20 mg/L are associated with a very high nephrotoxicity rate.1,2 Due to more drug resistance to vancomycin and adverse events, linezolid is prescribed to patients as an alternative treatment. Linezolid is a synthetic antibiotic that blocks bacterial protein synthesis by binding to rRNA on both the 30S and 50S subunits of the ribosome,1 preventing formation of the initiation complex required for protein systhesis. This can reduce the length of the developing peptide chain and decreasing the rate of translation reactions.3 Linezolid may also prevent the expression of toxins, such as those produced by Gram-positive pathogens.4 Linezolid has been approved to treat gram-positive infections, including bloodstream infections, and is used in hospital-acquired pneumonia, community-acquired pneumonia, skin and soft-tissue infections, and Methicillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococcus (VRE) infections from any source.1 However, the increased use of linezolid has resulted in adverse effects being widely reported. One of the most prevalent (15–50%) side effect being observed in patients is thrombocytopenia, which is considered the major adverse event induced by linezolid.5–10 Risk factors include prolonged dosing beyond two weeks,5–7 higher doses per body weight,9,10 renal insufficiency,3–7 and hypoalbuminemia.9 Neutropenia is a rare adverse effect of linezolid that has been reported once,11 and pancytopenia is a rare adverse effect of linezolid, which usually manifests as a sudden decrease in leukocytes and hemoglobin and is reversible. Most reports regarding pancytopenia are seen in pediatrics and long-term use. There are few reports about it in adults. The previous studies about linezolid-induced pancytopenia are further clarified in Table 1.
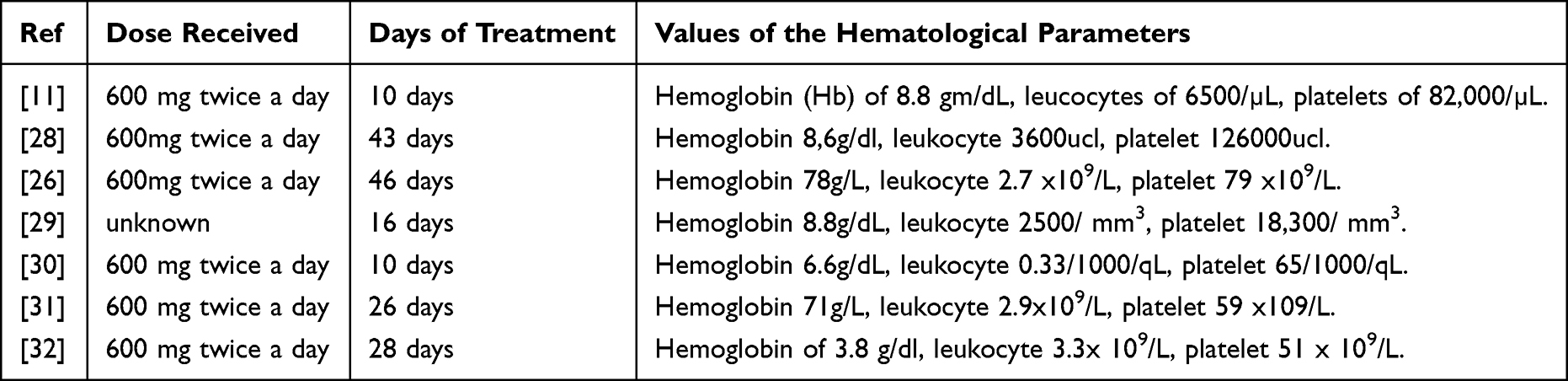 |
Table 1 Details of Linezolid Use in Previously Reported Cases |
Dapagliflozin is a highly potent, reversible, and selective sodium-glucose cotransporter-2 inhibitor (SGLT-2i) indicated worldwide for the treatment of type 2 diabetes (T2D).12 Recent studies have recommended it be prescribed to patients with heart failure with preserved ejection fraction (HFpEF).13 Currently, there are no reports of drug interactions between dapagliflozin and linezolid. The aim of this study is to report a case series of linezolid-induced pancytopenia exacerbated by dapagliflozin.
Cases and Methods
We enrolled patients diagnosed with linezolid-induced pancytopenia in Qingdao Central Hospital and Qingdao Municipal hospital from June 2021 to June 2022. Three patients were enrolled. Clinical characteristics and drug using history were collected.
Case 1
A 61-year-old female was admitted to the emergency department (ED) due to dyspnea, fever, and frequent urination. The patient was previously diagnosed with HfpEF and type 2 diabetes, for which she was administered dapagliflozin. She also had a history of hypertension, for which valsartan was administered. Physical examination showed that the patient was febrile, with a temperature of 38.5°C, blood pressure 145/96mmHg, and no abnormal findings on abdominal examination. A cardiac examination revealed a pulse deficit. Cardiac auscultation showed the variable intensity of the first heart sound and irregular pulse consistent with atrial fibrillation. On auscultation of the lungs, bilateral rales were heard. After admission, we initially diagnosed the patient with HFpEF, atrial fibrillation, type2 diabetes, hypertension, and a urinary tract infection.
Case 2
A 71-year-old female was admitted to the emergency department due to lethargy, dyspnea, and fever. The patient was previously diagnosed with HfpEF and type 2 diabetes, for which she was administered dapagliflozin. She had a history of refractory respiratory failure. Physical examination showed that the patient was febrile, with a temperature of 38.8°C, blood pressure 100/66mmHg, and no abnormal findings on abdominal examination. A cardiac examination revealed enlarged cardiac dullness. On auscultation of the lungs, bilateral rales were heard. After admission, respiratory failure was considered. The results of a blood gas analysis showed PH 7.28, PaO2 50mmHg, PaCO2 59mmHg, BE 1.0 mmol/L, which is consistent with type 2 respiratory failure. The patient was placed on a bipap Ventilator with the following mode: S/T mode, IPAP 18cm H2O, EPAP 5cm H2O, RR 14, I:E 1.2s, and FiO2: 55%. We initially diagnosed the patient with severe pneumonia, type 2 respiratory failure, and type 2 diabetes.
Case 3
A 76-year-old female was admitted to the ED because of cough and dyspnea for three days. The patient had previously been diagnosed with type 2 diabetes and sequelae of cerebral thrombosis (with which she had been bed-ridden for five years). Physical examination showed that the patient was febrile, with a temperature of 38.2°C, blood pressure of 134/78mmHg, and no abnormal findings on abdominal and cardiac examination. On auscultation of the lungs, bilateral rales were heard. A chest CT scan showed pneumonia in the bilateral lobes of the lung. We initially diagnosed the patient with pneumonia, type2 diabetes, and sequelae of cerebral thrombosis.
Results
Treatment Process
Case 1
We administered valsartan 80mg per day, and metoprolol (47.5mg per day), torasemide (20 mg per day) intravenously, and milrinone. Ceftizoxime was administered empirically, due to impaired renal function, to treat urinary tract infection. Despite the administration of antibiotics, the patient’s body temperature remained elevated, within the range 38–39°C. On the third day after admission, the urine culture and drug sensitivity result returned, showing a resistant strain of Enterococcus faecium which was only sensitive to linezolid and telicoplanin, but intermediate to ciprofloxacin. Therefore, we ceased prescribing ceftizoxime and began administering linezolid (600 mg twice per day). The patient’s symptoms alleviated, and her body temperature retuned to a normal range after three days of receiving linezolid. However, on the tenth day of treatment with linezolid, the patient suddenly began suffering from nosebleeds. Based on the result of blood count analysis, we diagnosed the patient with myelosuppression. We ceased administering linezolid immediately and replaced it with ciprofloxacin (0.2g twice a day through iv). A hematologist was consulted, who suggested administering recombinant human granulocyte factor and recombinant human thrombopoietin to increase the patient’s leukocyte count and platelet count. A platelet and red blood cells transfusion was also carried out. Despite this intervention, the patient’s leukocyte and platelet count did not normalize, and the patient passed away five days after linezolid administration was discontinued.
Case 2
Levofloxacin (0.5g per day) and dihydroxypropyl theophylline (0.5g per day) were administered through iv to treat the pneumonia, while aspartic insulin, dapagliflozin, and insulin degludec were administered to treat the diabetes. Budesonide was administered (1 mg twice per day) through aerosol inhalation. The patient’s dyspnea was alleviated after three days of treatment, and the PaO2 was within 80–90 mmHg. However, the patient still suffered from a fever. At that point, we received the results of the sputum bacterial culture which indicated MRSA and which was also resistant to levofloxacin, but sensitive to vancomycin and linezolid. Therefore, levofloxacin was replaced with vancomycin which induced a severe allergic reaction in the patient. Vancomycin was therefore stopped immediately and replaced with linezolid. Over the period of five days post admission, the patient’s symptoms gradually alleviated, until she was afebrile. The settings of the Bipap ventilator were changed to the following: S/T mode, IPAP 12cm H2O, EPAP 4cm H2O. Blood gas analysis showed: PH 7.42, PaO2 75mmHg, PaCO2 50mmHg, BE7.9 mmol/L, and potassium 3.4mmol/L. Oral potassium tablets were administered. On the seventh day, the settings were further altered to: S/T mode, IPAP 10cm H2O, EPAP 4cm H2O. However, on the 11th day after admission, the patient suddenly developed black stools and vaginal bleeding. We advised the patient to stop eating and drinking. Hemocoagulase and pantoprazole were administered. Based on the blood count analysis (Table 2), we diagnosed the patient with myelosuppression. Linezolid was immediately replaced with tigecycline (50 mg twice a day through iv). A consulting hematologist suggested administering recombinant human granulocyte factor and recombinant human thrombopoietin to increase leukocyte count and platelet count. The patient also received a platelet transfusion. Despite appropriate treatment, the patient’s leukocyte and platelet count did not improve, and the patient passed away six days after treatment with linezolid ceased.
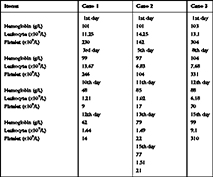 |
Table 2 Blood Count Analysis |
Case 3
Levofloxacin (0.5g per day) and dihydroxypropyl theophylline (0.5g per day) were administered through iv to treat pneumonia, and metformin 0.5g twice per day was administered to treat her diabetes. Budesonide (1 mg twice per day) was administered via aerosol inhalation. However, after three days of treatment, the patient was still febrile (body temperature between 38–39°C), and was producing copious amounts of yellow-to-greenish sputum. The results of sputum culture showed MRSA, which was also resistant to levofloxacin and vancomycin, but sensitive to linezolid and tigecycline. Therefore, levofloxacin was substituted to linezolid (600 mg twice per day). After two days of this treatment, the patient’s symptoms, including a raised temperature, alleviated. Linezolid was continually administered for 12 days before being discontinued. A rechecked blood count analysis showed moderate anemia and thrombocytopenia (Table 2). Since linezolid was stopped and hemoglobin and platelet transfusion were not needed, we did not take any treatment measures. The patient had no symptoms. Blood count analysis was normal three days later. A second chest CT scan showed that pneumonia was mostly absorbed in the bilateral lobes. The patient was discharged from the hospital.
The clinical characteristics of the three patients are further shown in Table 3, and the blood count analysis of three patients is shown in Table 2.
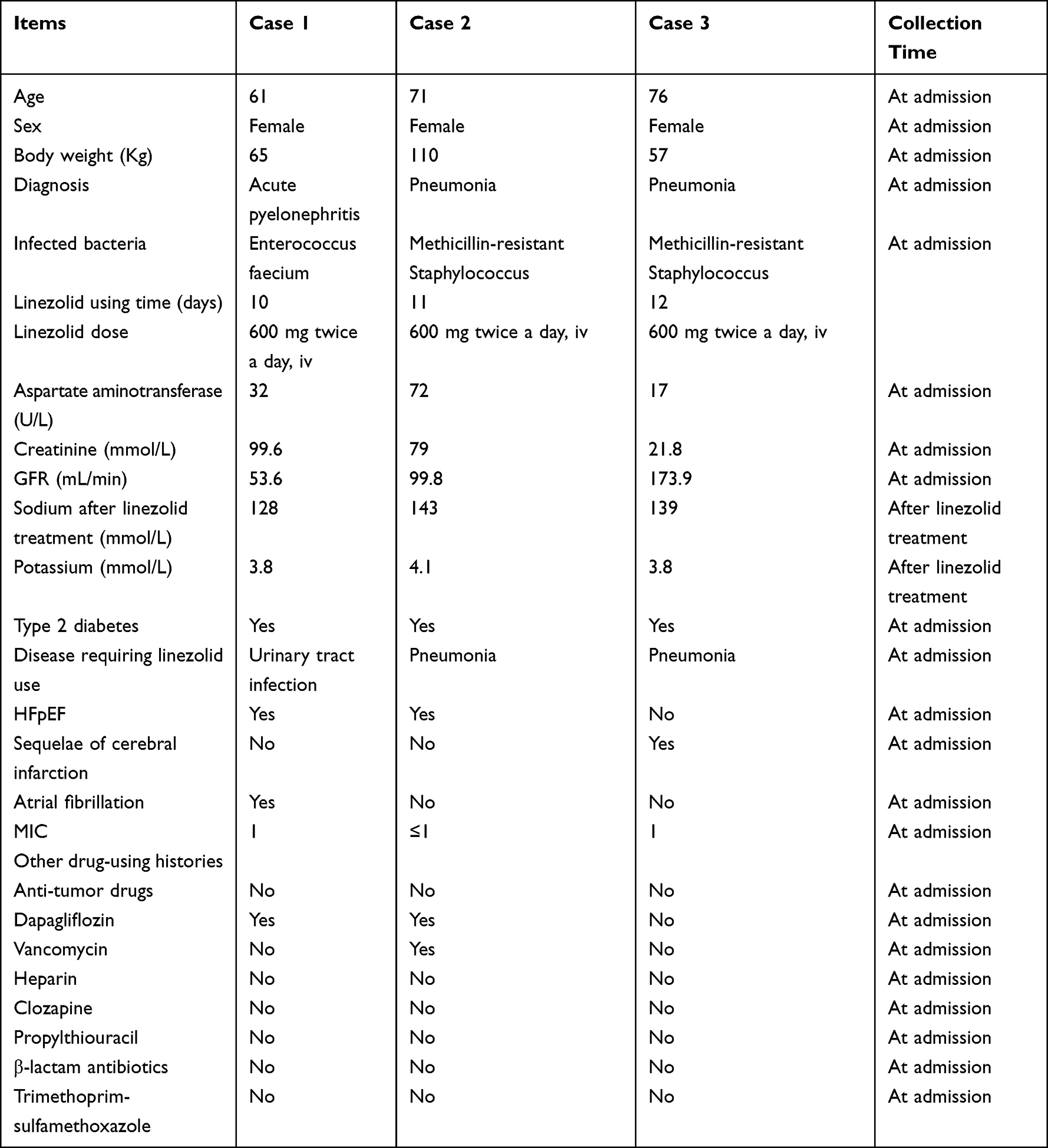 |
Table 3 Clinical Characteristics of Three Patients |
Discussion
Linezolid is now widely used in treating hospital and community-acquired pneumonia, especially sensitive to MRSA.3 The three patients in this case series were diagnosed with Enterococcus faecium and Methicillin-resistant Staphylococcus aureus. Linezolid was determined to be the best option for these patients. However, studies have demonstrated that linezolid can cause many adverse drug reactions, including thrombocytopenia, anemia, lactic acidosis, peripheral neuropathy, optic neuropathy, and serotonin syndrome.14 Myelosuppression is a rarely reported adverse drug reaction from linezolid. In this study, three patients with linezolid-induced cytopenia were observed. The common characteristics of the patients in cases 1 and 2 included that they were both diagnosed with HFpEF, type 2 diabetes, pneumonia, and hyponatremia. The patient in case 3 also had type 2 diabetes and pneumonia, and was not diagnosed with HFpEF. Francesca Conradie et al15 prescribed linezolid to patients with drug-resistant forms of tuberculosis, and myelosuppression was shown in the patients. The myelosuppression was found to be reversible during the six months of treatment. However, many patients require prolonged use of linezolid, which can cause more severe adverse drug reactions to occur. The patients in this study were given linezolid for a relatively short period, and irreversible pancytopenia was induced, which makes this case series more unique. There have also been reports of myelosuppression in pediatric patients using linezolid. There have been few reports of pancytopenia induced by combinations of linezolid with other drugs. Only one study reported thrombocytopenia due to the interaction of linezolid and digoxin. A comparison of this study with other studies is shown in Table 4.
 |
Table 4 Comparison with Other Studies |
Myelosuppression can manifest as one or more types of peripheral blood cytopenia, including anemia, leukopenia, and thrombocytopenia. Drugs often cause peripheral cytopenia by shortening peripheral blood cell survival rather than by suppressing marrow cell production, eg, autoimmune hemolytic anemia and immune thrombocytopenia.16 The patients in this study had a decreased leukocyte, hemoglobin, and platelet count, consistent with a diagnosis of myelosuppression. The patients in cases 1 and 2 were treated with linezolid. The other drugs used on these two patients, including dapagliflozin and dihyprophylline, did not cause myelosuppression. The patient in case 3 used metformin, which did not cause cytopenia. Therefore, we diagnosed linezolid-induced pancytopenia in these patients. This side effect is common in pediatric patients and patients with tuberculosis who require long-term use of linezolid. It is reversible by initiating appropriate treatment and stopping the use of the drug. The next step was to establish whether this is due to a reduction in the output of cells from the bone marrow (myelosuppression) or to a shortened survival period of the affected cell type(s) in the peripheral blood. According to related studies, a reduction in the output of cells from the bone marrow was the cause of myelosuppression in the patients. The treatment of drug-induced cytopenia begins with stopping the use of the drug. Then empirical and prophylactic antimicrobial therapy should be initiated. The two patients in cases 1 and 2 were switched to other antibiotics, according to the treatment principles. Colony-Stimulating Factors were initiated. The colony-stimulating factors G-CSF and GM- CSF can reduce the severity and duration of neutropenia after cytotoxic therapy. Hemorrhage Prophylactic platelet concentrate transfusion should be considered if the platelet count is <10 × 109/L due to myelosuppression. In an actively bleeding patient, transfusion to maintain the count >50 × 109/L is justified. The patient in case 1 had a lower platelet count and needed a platelet transfusion. Although the patient in case 2 had a relatively higher platelet count, she had a active bleeding for which platelet transfusion was needed. Therefore, recombinant human granulocyte factor and recombinant human thrombopoietin were administered to both patients. The patient in case 3 did not need further treatment according to the treatment guidelines. Despite the correct and timely treatment of the patients in cases 1 and 2, the pancytopenia was not reversed. Eventually, the two patients died. Further investigation is needed to determine what caused the pancytopenia to be irreversible.
The reason why linezolid causes myelosuppression is still not clear. One study demonstrated that cytotoxicity of linezolid is relieved by the knockdown of superoxide dismutase-1 in U937 cells. However, no autophagy has been observed in cells treated with linezolid. This indicates that mitochondrial damages would be linked to the induction of apoptosis in U937 cells treated with linezolid and that its mechanism does not involve autophagy.17 Current evidence supports the hypothesis that the inhibition of mitochondrial protein synthesis, due to the interaction of oxazolidinones with mitochondrial ribosomes, is the underlying cause of pancytopenia.18 Bacterial ribosomes and mitochondrial ribosomes are both of prokaryotic origin and have some similarities, which provides a theoretical basis to explain why linezolid binds to these mitochondrial ribosomes and thus causes loss of mitochondrial function in hemopoietic cells,18,19 which in turn causes a reduction in the output of cells from the bone marrow. The MIC of each pathogen was low in all three patients (Table 3), which indicates that all three pathogens were extremely sensitive. Therefore, mitochondrial function in hemopoietic cells was more inhibited, and a reduction in the output of cells from the bone marrow occurred earlier, resulting in early pancytopenia. In contrast to the patient in case 3, patients in cases 1 and 2 showed severe and irreversible pancytopenia, which may be due to the interaction of linezolid with dapagliflozin. One study has demonstrated that SGLT-2 activates AMPK by inhibiting mitochondrial function,20 which indicates that dapagliflozin and linezolid may co-inhibit the mitochondrial function in hemopoietic cells and cause early pancytopenia in patients. The patients in cases 1 and 2 showed pancytopenia on the 10th day and 11th day, respectively. Patient in case 3 did not have a history of dapagliflozin use, and showed moderate pancytopenia on the 12th day. The pancytopenia occurred earlier in all three patients than in most previous studies. We think this early pancytopenia is due to high sensitivity and low MIC of linezolid in all three patients.
Studies have demonstrated that risk factors that exacerbate linezolid-induced pancytopenia include prolonged treatment,5,15,21 chronic liver and kidney disease, underlying malignancy, and prior vancomycin treatment.22,23 Another study concluded that impaired renal function increases thrombocytopenia by a pharmacokinetic mechanism.24 The factor of prolonged treatment can be excluded in all three patients. The GFR of the patient in case 1 decreased, and the patient was diagnosed with moderate renal dysfunction, one of the risk factors that contributed to linezolid-induced pancytopenia. Among such risk factors, prolonged treatment and renal insufficiency are the most prevalent.5,25 One study has also demonstrated that linezolid administered to patients with renal dysfunction may reach a high blood level and subsequently increase the AUC (0–24), which may then induce severe thrombocytopenia and anemia.33 Another study showed that patients with chronic liver disease are at high risk of developing linezolid-related thrombocytopenia.22 Underlying malignancy and prior vancomycin treatment are relatively rare risk factors.26 Other studies have also suggested that hepatitis C and renal dysfunction may contribute to thrombocytopenia.24,27 The patient in case 1 had moderate renal insufficiency. The patient’s GFR was 53.6mL/min. However, the patient in case 2 had normal renal function. Both patients had irreversible pancytopenia. Thus, the role of renal insufficiency in this adverse reaction is still not clear. The patient in case 3 only had mild thrombocytopenia and anemia, which was reversible. There was no underlying malignancy in any of the three patients. The patient in case 2 had previously undergone vancomycin treatment. However, vancomycin was only administered one time and was ceased because of allergy, and the concentration of vancomycin was not high enough to interact with linezolid. None of the three patients were diagnosed with neutropenia, leukemia, or any hematological diseases, which excluded the possibility of underlying hematological abnormalities in patients. As shown in Table 3, no history of concomitant drug use was demonstrated, which excludes the possibility of concomitant drug use.
The two patients in cases 1 and 2 had the following common characteristics: 1. They were both diagnosed with hyponatremia after the initiation of linezolid. Hyponatremia is an adverse effect of linezolid. 2. They were both diagnosed with HFpEF and type 2 diabetes, for which they both had used dapagliflozin. 3. They were both elderly females. As shown in Table 4, most relevant cases of linezolid-induced cytopenia were seen in pediatric patients or in patients with long-term use, and most cases are reversible. However, in this study, both patients had short-term linezolid use and irreversible pancytopenia. This may be due to the interaction of dapagliflozin and linezolid. There are currently no studies on the interaction of linezolid and dapagliflozin. One study has demonstrated that SGLT-2 activates AMPK by inhibiting mitochondrial function.20 As we have discussed above, linezolid binds to human mitochondrial ribosomes and thus causes loss of mitochondrial function in hemopoietic cells.18,19 There are currently no studies about the hematological toxicity of dapagliflozin. We hypothesized that dapagliflozin and linezolid may co-inhibit the mitochondrial function in hemopoietic cells and cause sudden and irreversible pancytopenia in patients. However, further animal experiments should be conducted to prove this hypothesis.
Various authors have suggested that the administration of a continuous infusion of linezolid could be an alternative option to avoid the toxicity problems that can occur when increasing the dose. We do not agree with this idea. According to the instructions in the drug’s manual, the dose of linezolid is 600 mg every 12 hours for MRSA and Enterococcus faecium. According to the pharmacodynamics of linezolid, it is a time-dependent antibiotic, and should be administered every 12 hours. 600 mg is the minimum dose of linezolid for MRSA and Enterococcus faecium. The concentrations of linezolid remain at their peak for 12 hours. Continuous administration of linezolid will increase the dosage. However, the concentration of linezolid is constant, and the efficacy of linezolid depends on its concentration. If we do not increase its dose, the efficacy of linezolid will not improve, and the pathogen can not be eliminated. In a word, we can only increase the efficacy of linezolid by increasing the dose. Therefore, the toxicity of linezolid is unavoidable. The administration of a continuous infusion of linezolid is not an alternative option to avoid toxicity problems that can occur when increasing the dose.
Physicians, pharmacists, and healthcare professionals should monitor the blood count when treating patients with risk factors for linezolid-induced pancytopenia and avoid using SGLT-2 inhibitors together with linezolid.
Ethics and Dissemination
Informed written consent was obtained from three patients’ children for the publication of this report. Patient in case 3 was diagnosed with sequelae of cerebral thrombosis, for which she had trouble communicating. Therefore, a informed consent was obtained from the patient’s child. The case series was approved to publish by Qingdao Central Hospital.
Acknowledgment
We also thank Dr Meili Zhou and Dr Ling Song for their contribution to case 3 in this case series.
Author Contributions
Mengmei Li, Yujin Li, and Jun Teng were the patients’ attending physicians, reviewed the literature, and contributed to manuscript drafting; Wencheng Shen designed the case seies and critically reviewed the manuscript. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
None of the authors has a conflict of interest to declare in this article.
References
1. Katip W, Oberdorfer P, Monocentric Retrospective A. Study of AUC/MIC ratio of vancomycin associated with clinical outcomes and nephrotoxicity in patients withEnterococcal infections. Pharmaceutics. 2021;13(9):1378. doi:10.3390/pharmaceutics13091378
2. Katip W, Okonogi S, Oberdorfer P. The thirty-day mortality rate and nephrotoxicity associated with trough serum vancomycin concentrations during treatment of enterococcal infections: a propensity score matching analysis. Front Pharmacol. 2022;12:773994. doi:10.3389/fphar.2021.773994
3. Batts DH. Linezolid-A new option for treating Gram-positive infections. Oncology. 2000;14(8):23–29.
4. Zurenko GE, Gibson JK, Shinabarger DL, Aristoff PA, Ford CW, Tarpley WG. Oxazolidinones: a new class of antibacterials. Curr Opin Pharmacol. 2001;1(5):470–476. doi:10.1016/S1471-4892(01)00082-0
5. Hirano R, Sakamoto Y, Tachibana N, et al. Retrospective analysis of the risk factors for the linezolid-induced thrombocytopenia in adult Japanese patients. Int J Clin Pharm. 2014;36:795–799. doi:10.1007/s11096-014-9961-6
6. Attassi K, Hershberger E, Alam R, et al. Thrombocytopenia associated with linezolid therapy. Clin Infect Dis. 2002;34(5):695–698. doi:10.1086/338403
7. Chen C, Guo DH, Cao X, et al. Risk factors for thrombocytopenia in adult Chinese patients receiving linezolid therapy. Curr Ther Res Clin Exp. 2012;73(6):195–206. doi:10.1016/j.curtheres.2012.07.002
8. Niwa T, Suzuki A, Sakakibara S, et al. Retrospective cohort chart review study of factors associated with the development of thrombocytopenia in adult Japanese patients who received intravenous linezolid therapy. Clin Ther. 2009;31(10):2126–2133. doi:10.1016/j.clinthera.2009.10.017
9. Wu VC, Wang YT, Wang CY, et al. High frequency of linezolid-associated thrombocytopenia and anemia among patients with end-stage renal disease. Clin Infect Dis. 2006;42(1):66–72. doi:10.1086/498509
10. Sasaki T, Takane H, Ogawa K, et al. Population pharmacokinetic and pharmacodynamic analysis of linezolid and a hematologic side effect, thrombocytopenia, in Japanese patients. Antimicrob Agents Chemother. 2011;55(5):1867–1873. doi:10.1128/AAC.01185-10
11. Singhania SVK, Shenoy S, Kapoor D. Linezolid-induced rare triad of hypoglycaemia, bone marrow suppression and hyponatraemia in elderly. J Clin Pharm Ther. 2020;45(2):376–378. doi:10.1111/jcpt.13069
12. Sohita D. Dapagliflozin: a review in type 2 diabetes. Drugs. 2019;79(10):1135–1146. doi:10.1007/s40265-019-01148-3
13. Zannad F, Ferreira JP, Pocock SJ, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet. 2020;396(10254):819–829. doi:10.1016/S0140-6736(20)31824-9
14. Kishor K, Dhasmana N, Kamble SS, et al. Linezolid induced adverse drug reactions - an update. Curr Drug Metab. 2015;16(7):553–559. doi:10.2174/1389200216666151001121004
15. Conradie F, Diacon AH, Ngubane N, et al. Treatment of highly drug-resistant pulmonary tuberculosis. N Engl J Med. 2020;382(10):893–902. doi:10.1056/NEJMoa1901814
16. Carey PJ. Drug-induced myelosuppression: diagnosis and management. Drug Saf. 2003;26(10):691–706. doi:10.2165/00002018-200326100-00003
17. Fujii S, Muraoka S, Miyamoto A, et al. Linezolid-induced apoptosis through mitochondrial damage and role of superoxide dismutase-1 in human monocytic cell line U937. Yakugaku Zasshi. 2018;138(1):73–81. doi:10.1248/yakushi.17-00133
18. Leach KL, Swaney SM, Colca JR, et al. The site of action of oxazolidinone antibiotics in living bacteria and in human mitochondria. Mol Cell. 2007;26(3):393–402. doi:10.1016/j.molcel.2007.04.005
19. Nagiec EE, Wu L, Swaney SM, et al. Oxazolidinones inhibit cellular proliferation via inhibition of mitochondrial protein synthesis. Antimicrob Agents Chemother. 2005;49(9):3896–3902. doi:10.1128/AAC.49.9.3896-3902.2005
20. Tsai KL, Hsieh PL, Chou WC, Cheng HC, Huang YT, Chan SH. Dapagliflozin attenuates hypoxia/reoxygenation-caused cardiac dysfunction and oxidative damage through modulation of AMPK. Cell Biosci. 2021;11(1):44. doi:10.1186/s13578-021-00547-y
21. Hanai Y, Matsuo K, Ogawa M, et al. A retrospective study of the risk factors for linezolid-induced thrombocytopenia and anemia. J Infect Chemother. 2016;22(8):536–542. doi:10.1016/j.jiac.2016.05.003
22. Ikuta S, Tanimura K, Yasui C, et al. Chronic liver disease increases the risk of linezolid-related thrombocytopenia in methicillin-resistant Staphylococcus aureus-infected patients after digestive surgery. J Infect Chemother. 2011;17:388–391. doi:10.1007/s10156-010-0188-8
23. Smith PF, Birmingham MC, Noskin GA, et al. Safety, efficacy and pharmacokinetics of linezolid for treatment of resistant Gram-positive infections in cancer patients with neutropenia. Ann Oncol. 2003;14:795–801. doi:10.1093/annonc/mdg211
24. Tsuji Y, Holford NHG, Kasai H, et al. Population pharmacokinetics and pharmacodynamics of linezolid-induced thrombocytopenia in hospitalized patients. Clin Pharmacol. 2017;83(8):1758–1772.
25. Tsuji Y, Hiraki Y, Matsumoto K, et al. Thrombocytopenia and anemia caused by a persistent high linezolid concentration in patients with renal dysfunction. J Infect Chemother. 2011;17:70–75. doi:10.1007/s10156-010-0080-6
26. Leader R, Hackett J, Allan A, Carter P. Linezolid-induced pancytopenia. BMJ Case Rep. 2018;2018:225480.
27. Lee EY, Caffrey AR. Thrombocytopenia with tedizolid and linezolid. Antimicrob Agents Chemother. 2017;62(1):e01453–e01517. doi:10.1128/AAC.01453-17
28. Ballesteros MDM, Milián MEO, Velázquez ED, et al. Myelosupression induced by linezolid: a pediatric case. Arch Argent Pediatr. 2017;115(6):e420–e423. doi:10.5546/aap.2017.e420
29. Parlak E, Tan H. Pancytopenia due to linezolid treatment. Turk Pediatri Ars. 2015;50(3):185–188. doi:10.5152/TurkPediatriArs.2015.1133
30. Varkal G, Paydas S, Gural MC, et al. Pancytopenia associated with linezolid therapy in a hemodialysis patient. Turk Nephrol Dial Transplant J. 2017;26(1):121–123. doi:10.5262/tndt.2017.1001.21
31. N Lakhani, W Thompson. Probable linezolid-induced pancytopenia. Can J Infect Dis Med Microbiol. 2005;16(5):286–288. doi:10.1155/2005/961613
32. Sharma S, Syal A, Gupta M, et al. Reversible myelosuppresion with prolonged usage of linezolid in treatment of methicillin-resistant staphylococcus aureus. Cureus. 2020;12(10):e10890. doi:10.7759/cureus.10890
33. Kraleti S, Soultanova I. Pancytopenia and lactic acidosis associated with linezolid use in a patient with empyema. J Ark Med Soc. 2013;110(4):62–63.
34. Yulin Z, Lingti K, Shan G, Yong Z. A possible interaction between linezolid and digoxin: a case report of therapeutic drug monitoring. Saudi Pharm J. 2020;28(11):1408–1410. doi:10.1016/j.jsps.2020.09.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.