Back to Journals » International Journal of Women's Health » Volume 18
Limited Survival Benefit of Preoperative Conization Before Radical Surgery in Stage IB Cervical Cancer: An IPTW-Adjusted Retrospective Cohort Study
Authors Gao S ![]() , Wang K, Su X, Wu Y, Li B
, Wang K, Su X, Wu Y, Li B
Received 26 March 2026
Accepted for publication 11 June 2026
Published 14 July 2026 Volume 2026:18 612277
DOI https://doi.org/10.2147/IJWH.S612277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Songkun Gao,1,* Kunyu Wang,1,* Xiaomeng Su,2 You Wu,1 Bin Li1
1Department of Gynecological Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Obstetrics and Gynecology Department, Beijing Huairou Maternal and child health care Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: You Wu, Department of Gynecological Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China, Email [email protected] Bin Li, Department of Gynecological Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China, Email [email protected]
Background: Cervical cancer remains a major global health burden. Preoperative conization has been proposed to reduce tumor burden and potential intraoperative tumor dissemination, but its survival benefit in patients with stage IB cervical cancer remains uncertain. This study aimed to evaluate the association between preoperative conization and survival outcomes after radical surgery in patients with FIGO 2018 stage IB cervical cancer.
Methods: This retrospective study included 1,614 patients with FIGO 2018 stage IB1–IB3 cervical cancer who underwent radical surgery between 2007 and 2016 at a single center. Patients were classified into four groups based on surgical approach and conization status. Progression-free survival (PFS) and overall survival (OS) were analyzed. Inverse probability of treatment weighting (IPTW) based on propensity scores was used to balance baseline characteristics. Survival outcomes were compared using weighted Kaplan–Meier analysis.
Results: After IPTW adjustment, baseline covariate balance was substantially improved, although residual imbalances remained for FIGO stage, depth of stromal invasion, neoadjuvant chemotherapy, and tumor differentiation. Weighted survival analysis showed no consistent survival advantage associated with preoperative conization. In pairwise OS comparisons, the laparotomy with conization group appeared to have superior OS compared with the other groups; however, this finding should be interpreted cautiously because no death events occurred in this group, resulting in non-estimable hazard ratios for comparisons involving this group. For PFS, no significant differences were observed between groups, including laparotomy with versus without conization (HR = 2.61, 95% CI: 0.62– 11.02, P = 0.54), laparoscopic surgery without conization versus laparotomy without conization (HR = 1.97, 95% CI: 0.98– 3.94, P = 0.21), laparoscopic surgery with conization versus laparotomy without conization (HR = 0.84, 95% CI: 0.21– 3.49, P = 1.00), laparoscopic surgery without conization versus laparotomy with conization (HR = 0.75, 95% CI: 0.18– 3.08, P = 0.98), laparoscopic surgery with conization versus laparotomy with conization (HR = 0.32, 95% CI: 0.05– 2.02, P = 0.60), and laparoscopic surgery with versus without conization (HR = 0.43, 95% CI: 0.12– 1.59, P = 0.56).
Conclusion: Preoperative conization was not associated with improved OS or PFS in patients with FIGO 2018 stage IB cervical cancer undergoing radical surgery. The apparent OS advantage observed in the laparotomy with conization group was based on zero death events and non-estimable hazard ratios, and therefore should not be interpreted as definitive evidence of a survival benefit. Further prospective multicenter studies with larger conization cohorts and longer follow-up are warranted.
Keywords: cervical cancer, FIGO stage IB, conization, radical hysterectomy, survival outcomes
Introduction
Cervical cancer remains one of the most prevalent malignancies among women worldwide, particularly in developing countries, where it continues to impose a substantial burden of morbidity and mortality.1 Although screening programs and human papillomavirus (HPV) vaccination have contributed to reducing the overall disease burden, a considerable proportion of patients still present with invasive disease at initial diagnosis, necessitating radical treatment.2 For patients with stage IB cervical cancer classified by the 2018 FIGO staging system, radical hysterectomy combined with pelvic lymphadenectomy remains one of the established standard therapeutic modalities.3
In recent years, the impact of surgical approaches and perioperative management on oncological outcomes in cervical cancer has garnered increasing attention. Particularly in the context of emerging safety concerns regarding minimally invasive surgery, optimizing preoperative and intraoperative strategies to minimize tumor dissemination risk and improve survival outcomes has become a critical direction in clinical research.4,5 Conization, serving as both a diagnostic and therapeutic procedure, holds distinct clinical value in the management of early-stage cervical cancer. Several studies have suggested that preoperative conization may enhance the oncological safety of subsequent radical surgery by reducing tumor burden and minimizing tumor exposure with potential dissemination risk. In an observational study, cervical conization prior to radical hysterectomy significantly decreased the risk of recurrence and mortality among patients with stage IB1 disease.6 In addition, conization can provide more accurate pathological information regarding tumor size, depth of invasion, and margin status, which may improve preoperative risk stratification and treatment planning.
Given the reported differences in oncological outcomes between open and minimally invasive radical hysterectomy, surgical approach represents an important factor when evaluating the prognostic role of preoperative conization. Therefore, both laparotomy and laparoscopic surgery were included in the present study to determine whether the potential effect of conization differed according to surgical approach.
However, the prognostic value of preoperative conization in patients with stage IB cervical cancer undergoing radical surgery remains controversial. Previous studies have suggested that conization may reduce recurrence risk and improve survival, particularly in selected patients with smaller tumors or those undergoing minimally invasive radical hysterectomy. In contrast, other studies have failed to demonstrate an independent survival benefit after adjusting for clinicopathological factors. These inconsistent findings may partly stem from variations in study design, FIGO staging systems, tumor size, surgical approaches, pathological risk factors, and statistical adjustment methods. Consequently, the clinical value of preoperative conization in the broader stage IB population remains unclear.Moreover, heterogeneity in surgical approaches (laparotomy versus laparoscopy), tumor stage, and pathological characteristics across previous studies has precluded direct comparison of their findings.7,8 In particular, because minimally invasive surgery and open surgery may differ in terms of tumor manipulation, tumor exposure, and potential dissemination risk, the effect of preoperative conization should be evaluated separately according to surgical approach.
Although FIGO 2018 sub-stages IB1, IB2, and IB3 differ in tumor size and prognostic characteristics, they are all classified as stage IB and amenable to radical surgery in appropriately selected patients. In clinical practice, treatment decisions for stage IB cervical cancer are influenced not only by tumor size but also by surgical approach, pathological features, and institutional strategies. Therefore, we included patients with FIGO 2018 IB1–IB3 disease in a unified analytical framework to evaluate the role of preoperative conization in the broader stage IB surgical population.
Therefore, this study was conducted using a large-scale, single-center retrospective cohort of patients with stage IB1–IB3 cervical cancer according to the 2018 FIGO classification. Inverse probability of treatment weighting (IPTW) was employed to balance baseline characteristics between treatment groups. We systematically evaluated the impact of preoperative conization on progression-free survival (PFS) and overall survival (OS) across different surgical modalities, aiming to provide robust evidence-based guidance for perioperative management in patients with stage IB cervical cancer.
Methods
We retrospectively reviewed medical records of patients who underwent radical hysterectomy for cervical cancer at Cancer Hospital, Chinese Academy of Medical Sciences, between 2007 and 2016. Eligibility criteria included: (1) histopathologically confirmed cervical cancer by biopsy; (2) restaging according to the 2018 FIGO classification with definitive stage IB1, IB2, or IB3 disease; and (3) complete clinical and pathological documentation. Patients were excluded if follow-up was discontinued for personal reasons, resulting in unavailable data on overall survival or progression-free survival.
Patients were stratified into four groups based on preoperative conization status and surgical approach: Group A (laparotomy without preoperative conization), Group B (laparotomy with preoperative conization), Group C (laparoscopic surgery without preoperative conization), and Group D (laparoscopic surgery with preoperative conization).
The following clinicopathological variables were extracted from medical records: age at surgery, body mass index, FIGO stage, depth of stromal invasion, parametrial involvement, lymphovascular space invasion, neoadjuvant chemotherapy status, histologic differentiation grade, postoperative lymph node metastasis, adjuvant radiotherapy, and adjuvant chemotherapy. Postoperative surveillance was conducted to document disease recurrence and survival status. Progression-free survival and overall survival were calculated from the date of surgery to the date of first recurrence or death, and to the date of death from any cause, respectively.
Patients with unavailable survival outcomes were excluded from the analysis. For clinicopathological variables with missing or uncertain information, the missing values were retained as separate “Unknown” or “Not reported” categories when applicable, rather than being imputed, to preserve the original data structure and avoid introducing additional assumptions.
Neoadjuvant chemotherapy regimens and cycles were administered at the discretion of treating physicians based on multidisciplinary team assessment. Postoperative adjuvant therapy was determined according to institutional protocols and pathological risk factors.
To address baseline confounding across the four treatment groups, we employed inverse probability of treatment weighting based on propensity scores estimated via generalized boosted modeling. All baseline covariates were incorporated into the propensity score model. Stabilized weights were derived to minimize variance inflation, with truncation at the 1st and 99th percentiles to attenuate the influence of extreme weights. Final weights were normalized to a mean of 1. Covariate balance was evaluated using standardized mean differences before and after weighting, with values less than 0.1 indicating adequate balance. Balance diagnostics were visualized using Love plots. The validity of the IPTW approach was considered based on the assumptions of exchangeability, positivity, and correct specification of the propensity score model. To assess these assumptions, we examined covariate balance before and after weighting using absolute standardized mean differences and Love plots. In addition, the distribution of stabilized weights was inspected to identify extreme weights, and weights were truncated at the 1st and 99th percentiles to reduce the influence of highly influential observations. Effective sample sizes after weighting were also calculated to evaluate the stability of the weighted pseudo-population.
Statistical analyses were performed using SigmaStat 3.5, SPSS 26.0, and R version 4.5.2. The R packages WeightIt, cobalt, survey, and tableone were utilized for propensity score analysis, balance assessment, weighted estimation, and descriptive statistics, respectively.
Results
A total of 1,614 patients were included in this analysis (Table 1). The mean follow-up time was 76.84 months, with a median of 74 months (IQR, 55–96 months).Significant baseline imbalances were observed across the four groups with respect to FIGO stage (P < 0.001), depth of stromal invasion (P < 0.001), lymphovascular space invasion (P = 0.031), neoadjuvant chemotherapy status (P < 0.001), tumor differentiation grade (P < 0.001), lymph node metastasis (P = 0.002), and postoperative radiotherapy (P < 0.001). Intergroup comparisons revealed that patients undergoing laparoscopic surgery had significantly more favorable tumor characteristics than those undergoing laparotomy, including earlier stage, less stromal invasion, lower rates of lymphovascular space invasion, better differentiation grade, and reduced lymph node involvement (Supplementary Table 1).
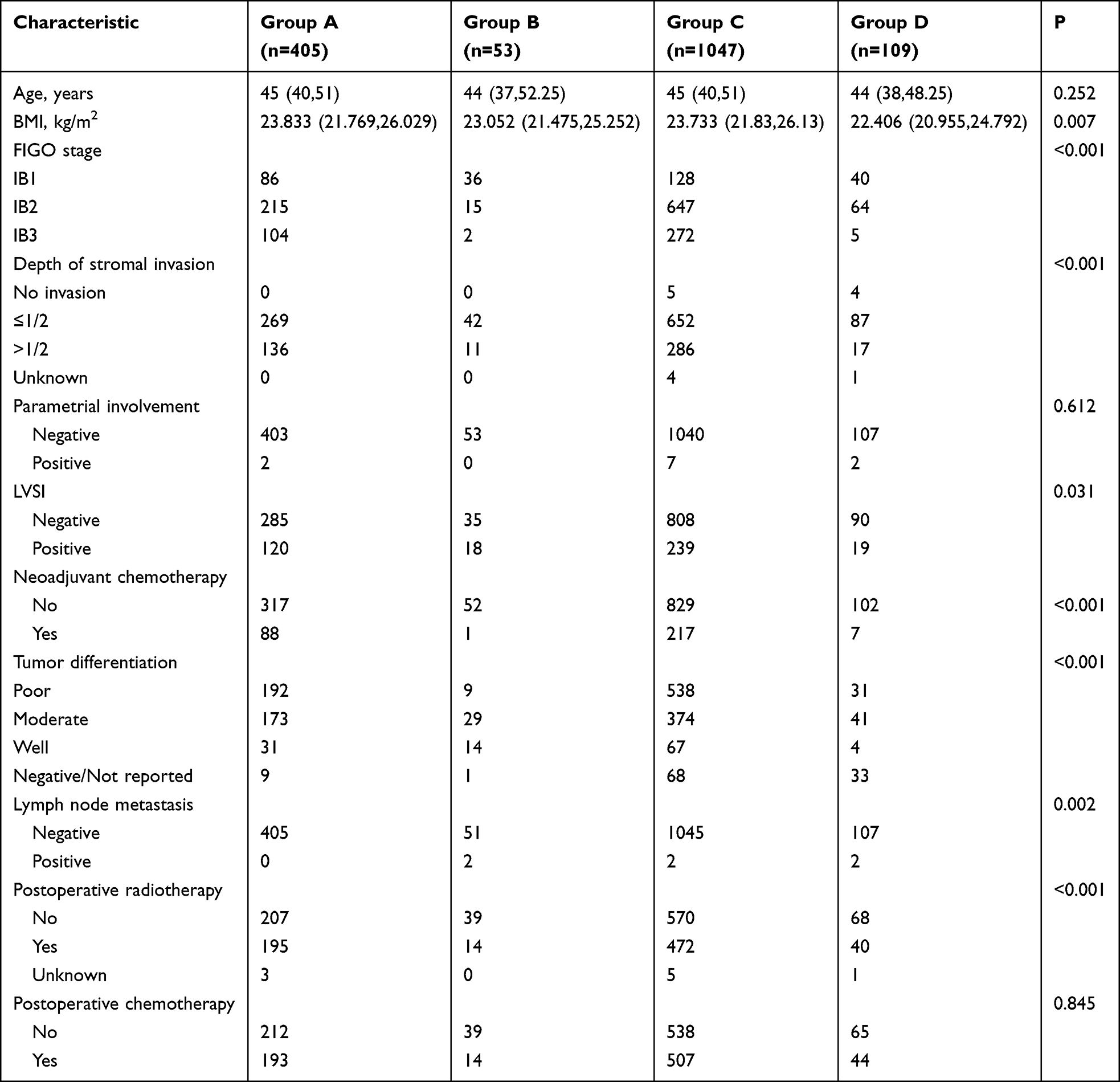 |
Table 1 Baseline Clinicopathological Characteristics of Patients in the Four Groups |
Following IPTW adjustment, baseline covariate balance was substantially improved across treatment groups. Standardized mean differences after weighting were 0.088 for age, 0.029 for body mass index, and 0.057 for lymphovascular space invasion, all indicating adequate balance (SMD < 0.1). Residual imbalances persisted for certain variables, including FIGO stage (SMD = 0.239), depth of stromal invasion (SMD = 0.143), neoadjuvant chemotherapy (SMD = 0.207), and tumor differentiation grade (SMD = 0.313) (Supplementary Figure 1). However, these imbalances were markedly attenuated compared with the unweighted population. The effective sample sizes after weighting were 497.35 for Group A, 290.96 for Group B, 507.12 for Group C, and 318.57 for Group D, indicating a more balanced distribution across groups.
Weighted Kaplan-Meier analysis revealed no statistically significant differences in overall survival or progression-free survival among the four treatment groups (Figure 1). Pairwise comparisons demonstrated that Group B exhibited significantly superior overall survival compared with the other three groups (P < 0.05; Table 2), whereas no significant differences were observed among the remaining comparisons. For progression-free survival, no significant differences were detected between any groups (P > 0.05 for all comparisons; Table 3).
 |
Table 2 Comparison of Overall Survival Among Groups After IPTW Adjustment |
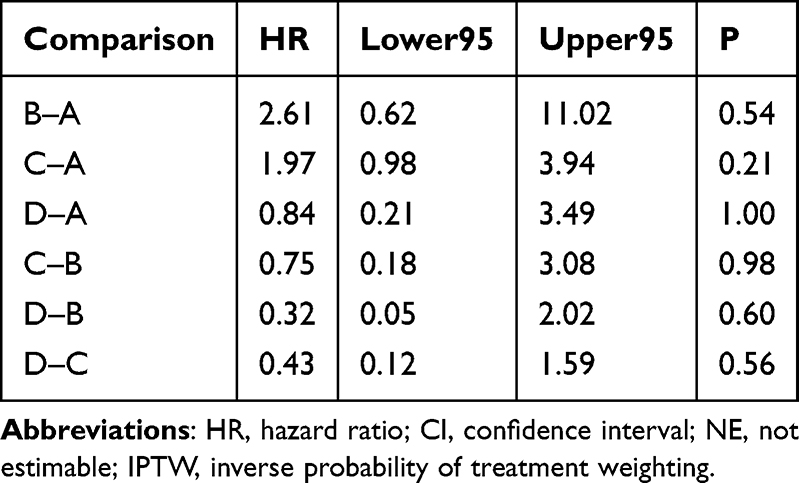 |
Table 3 Comparison of Progression-Free Survival Among Groups After IPTW Adjustment |
 |
Figure 1 Weighted Kaplan–Meier curves of overall survival and progression-free survival among the four groups after IPTW adjustment. (A) Overall survival. (B) Progression-free survival. |
To evaluate the independent effect of preoperative conization on oncological outcomes, we pooled Group A with Group C (no conization) and Group B with Group D (conization). Weighted survival analyses stratified by surgical approach showed no significant differences in overall survival or progression-free survival between patients who did and did not undergo preoperative conization, regardless of whether laparotomy or laparoscopic surgery was performed (Figure 2).
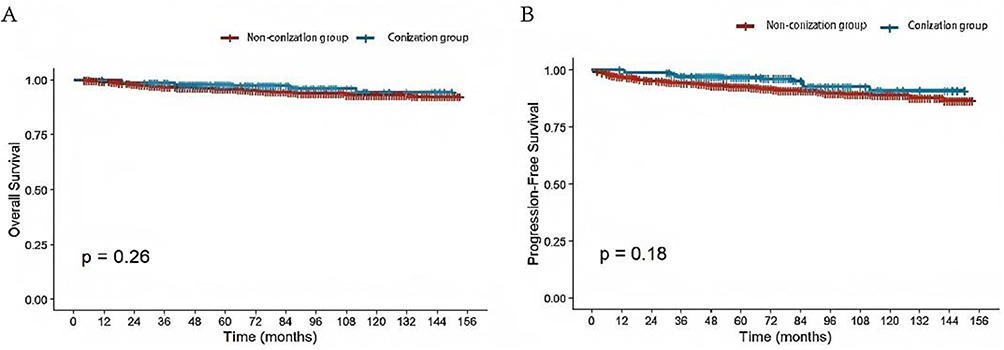 |
Figure 2 Weighted Kaplan–Meier survival curves comparing patients with and without conization after IPTW adjustment. (A) Overall survival. (B) Progression-free survival. |
Discussion
This retrospective analysis of 1,614 patients with stage IB cervical cancer treated between 2007 and 2016 systematically evaluated the impact of preoperative conization on survival outcomes across different surgical approaches. After adjusting for baseline imbalances using inverse probability of treatment weighting, three principal findings emerged: first, no significant differences in overall survival or progression-free survival were observed among the four treatment groups in the overall cohort; second, pairwise comparisons revealed a statistically significant overall survival advantage for the laparotomy with conization group, but this finding was not consistently supported by progression-free survival analysis or confirmed in pooled analyses; third, after merging groups to evaluate the independent effect of conization, preoperative conization did not significantly improve overall survival or progression-free survival in either the laparotomy or laparoscopic surgery cohorts.9
Minimally invasive surgery has been associated with increased risks of tumor dissemination due to tumor manipulation and the pneumoperitoneum environment, which may contribute to inferior oncological outcomes in cervical cancer, particularly among patients with locally advanced disease.10,11 Strategies to mitigate intraoperative tumor spread and achieve equivalence with open surgery have been extensively investigated. Conization has been hypothesized to confer a protective effect by reducing tumor volume, minimizing intraoperative tumor exposure, and lowering potential dissemination risk during subsequent radical surgery. Therefore, whether preoperative conization can compensate for this potential deficiency has remained a subject of considerable research interest. However, our findings indicate that preoperative conization did not significantly improve survival outcomes in patients undergoing laparoscopic radical hysterectomy after IPTW adjustment. This suggests that conization itself may not be a critical determinant of long-term prognosis in patients with stage IB cervical cancer undergoing definitive surgical treatment.Compared with previous studies, our findings offer a more cautious interpretation of the prognostic role of preoperative conization. The SUCCOR cone study primarily included patients with FIGO 2009 stage IB1 cervical cancer and reported that conization before radical hysterectomy was associated with reduced recurrence and mortality risk.6 Klapdor et al also suggested that absence of preoperative conization might be associated with increased recurrence risk after radical hysterectomy, and that patients with smaller tumors who underwent conization may have better outcomes.7 Additionally, Zhu et al’s systematic review and network meta-analysis indicated that preoperative conization might reduce postoperative recurrence risk in early-stage cervical cancer.8 However, these studies largely focused on selected early-stage or low tumor burden patients, with recurrence as the primary outcome. In contrast, our study included patients with FIGO 2018 stage IB1–IB3 cervical cancer, representing a broader, more heterogeneous population with greater tumor burden. We applied IPTW to adjust for baseline differences and performed four-group stratified analysis by surgical approach and conization status to systematically evaluate OS and PFS. Our results showed no consistent survival benefit from preoperative conization. Although Group B (laparotomy with preoperative conization) demonstrated an OS advantage, this finding was based on zero death events and an inestimable HR, and was not supported by PFS analysis or combined group analysis. Therefore, our results should be regarded as complementary to, rather than a direct refutation of, previous studies. The potential protective effect of preoperative conization may be more applicable to carefully selected low-risk patients with smaller tumors, but may not be generalizable to the broader FIGO 2018 stage IB1–IB3 cervical cancer population.
Notably, patients in the laparoscopic surgery groups exhibited more favorable pathological characteristics prior to weighting, including earlier stage, less stromal invasion, and lower rates of lymph node metastasis, indicating substantial selection bias in surgical approach decisions in clinical practice. This pattern is consistent with findings from previous studies demonstrating comparable outcomes between minimally invasive and open surgery in early-stage cervical cancer even without special intraoperative precautions.12,13 Inverse probability of treatment weighting is a robust methodological approach for estimating treatment effects in observational studies, particularly those with large sample sizes.14,15 By applying IPTW, we mitigated this selection bias to a considerable extent, enhancing comparability across treatment strategies. Given the inherent prognostic differences between laparoscopic and open surgery, we did not directly compare outcomes across surgical approaches. The observed overall survival advantage for the laparotomy with conization group in pairwise comparisons was not replicated in progression-free survival analysis or pooled analyses. This discrepancy between overall survival and progression-free survival findings may reflect sample size imbalance, limited event numbers, or residual confounding rather than a genuine survival benefit of conization. Specifically, the absence of death events in Group B during the observed follow-up period resulted in quasi-complete separation, yielding non-estimable hazard ratios for comparisons involving this group. Consequently, the overall survival advantage observed for Group B should be interpreted with caution, as it may be driven by favorable baseline characteristics or selection effects rather than a true protective effect of conization. Furthermore, residual imbalances persisted after weighting for certain variables, including FIGO stage, depth of stromal invasion, and tumor differentiation grade, which may have influenced the results. Complete elimination of baseline differences is challenging given the inherent correlations between treatment pathways and tumor characteristics. Nevertheless, IPTW substantially improved intergroup comparability and provided a more reliable statistical foundation for outcome analysis, though our findings require further validation.
From a clinical perspective, our results suggest that the decision to routinely perform preoperative conization in patients with stage IB1–IB3 cervical cancer should not be based solely on its potential survival benefits. While the diagnostic, staging, and local control values of conization remain undisputed, its impact on long-term oncological outcomes appears limited. Clinical decision-making should instead integrate tumor stage, pathological features, surgical approach, and individual patient factors.
This study has several limitations. First, as a single-center retrospective analysis, it remains susceptible to selection bias and unmeasured confounding despite IPTW adjustment. Although IPTW substantially improved covariate balance across groups, residual imbalance could not be completely eliminated because treatment allocation in clinical practice was closely related to tumor characteristics and surgical decision-making. Second, patients with stage I cervical cancer generally have relatively low recurrence and mortality rates, resulting in a limited number of survival events during follow-up. In particular, no death events were observed in the laparotomy with conization group during the study period, which led to quasi-complete separation and non-estimable hazard ratios for OS comparisons involving this group. Therefore, the apparent OS advantage observed in this subgroup should be interpreted cautiously and should not be regarded as definitive evidence of a survival benefit from preoperative conization. Third, the relatively small number of patients undergoing preoperative conization, especially within specific surgical approach subgroups, may have limited the statistical power and stability of subgroup comparisons. Finally, prospective multicenter studies with larger conization cohorts, standardized surgical procedures, and longer follow-up are warranted to further clarify whether preoperative conization provides any oncological benefit in patients with stage IB cervical cancer.
In conclusion, this large-scale retrospective cohort study employing propensity score weighting found no evidence that preoperative conization significantly improves overall survival or progression-free survival following radical hysterectomy via either laparotomy or laparoscopic approach in patients with stage IB cervical cancer. Our findings provide new evidence-based reference for the clinical application of preoperative conization in this population and suggest that its survival benefit may be limited.
Ethical Approval
The study was carried out in accordance with the ethical standards laid down in the Declaration of Helsinki, and was approved by the ethics committees of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences (NCC2025C-842).The ethics committee felt that this study could exempt patients from informed consent.Potential participants’eligibility was established by reviewing their medical records. As this was a retrospective study and all patient treatments and outcomes had already been determined, the ethics committee waived the requirement for informed consent.All patients’ privacy is ensured by assigning anonymous codes instead of personal identifiers.
Acknowledgments
This manuscript was edited for language and style by Kimi, an AI language model developed by Moonshot AI. Kimi assisted in refining the text to ensure clarity, coherence, and adherence to scientific writing standards. The authors are responsible for the content and any errors that remain.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Special Research Fund for Central Universities, Peking Union Medical College (3332025186).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang Y, Lin W, Chen X, Zheng X, Yi H, Zhang L. Analyzing and forecasting global cervical cancer burden based on WHO’s elimination strategy: insights and projections from a 1990-2021 global burden of disease (GBD) study covering 204 countries and territories. J Adv Res. 2025;S2090-1232(25):742. doi:10.1016/j.jare.2025.09.038.
2. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2025 update. Int J Gynaecol Obstet. 2025;71(Suppl 1):87–9. doi:10.1002/ijgo.70277.
3. Wipperman J, Neil T, Williams T.Cervical cancer: evaluation and management. Am Fam Physician. 2018;97(7):449–454.
4. Gitas G, Pados G, Laganà AS, Guenther V, Ackermann J, Alkatout I. Role of laparoscopic hysterectomy in cervical and endometrial cancer: a narrative review. Minim Invasive Ther Allied Technol. 2023;32(1):1–11. doi:10.1080/13645706.2022.2154166.
5. Fusegi A, Kanao H, Tsumura S, et al. Minimally invasive radical hysterectomy and the importance of avoiding cancer cell spillage for early-stage cervical cancer: a narrative review. J Gynecol Oncol. 2023;34(1):e5. doi:10.3802/jgo.2023.34.e5.
6. Chacon E, Manzour N, Zanagnolo V, et al; SUCCOR study group; SUCCOR study Group. SUCCOR cone study: conization before radical hysterectomy. Int J Gynecol Cancer. 2022;32(2):117–124. doi:10.1136/ijgc-2021-002544
7. Klapdor R, Hertel H, Delebinski L, Hillemanns P. Association of preoperative cone biopsy with recurrences after radical hysterectomy. Arch Gynecol Obstet. 2022;305(1):215–222. doi:10.1007/s00404-021-06145-0.
8. Zhu X, Ye L, Fu Y, You B, Lu W. Radical hysterectomy with preoperative conization in early-stage cervical cancer: a systematic review and pairwise and network meta-analysis. J Minim Invasive Gynecol. 2024;31(3):193–199. doi:10.1016/j.jmig.2023.11.019.
9. Quan C, Liang S, Feng Z, Zhu J, Zhang M, Huang Y. Surgical and oncologic outcomes between laparoscopic and radical abdominal hysterectomy for IB1-IIA2 cervical cancer. Asian J Surg. 2023;46(1):105–110. doi:10.1016/j.asjsur.2022.01.033.
10. Yang X, Chen S, Li Y, et al. Laparoscopic radical hysterectomy with Karez technique for stage IB3 and IIA2 cervical cancer: a multicenter retrospective cohort study. Int J Surg. 2025;111(7):4516–4527. doi:10.1097/JS9.0000000000002522.
11. Li RZ, Sun LF, Li R, Wang HJ. Survival after minimally invasive radical hysterectomy without using uterine manipulator for early-stage cervical cancer: a systematic review and meta-analysis. BJOG. 2023;130(2):176–183. doi:10.1111/1471-0528.17339.
12. Plante M, Mahner S, Sebastianelli A, et al. Minimally invasive compared to open surgery in patients with low-risk cervical cancer following simple hysterectomy: an exploratory analysis from the gynegologic cancer intergroup/canadian cancer trials group CX.5/SHAPE trial. Int J Gynecol Cancer. 2025;35(1):100001. doi:10.1016/j.ijgc.2024.100001.
13. Kim SI, Yoo JG, Lee SJ, Park DC, Yoon JH. Robot-assisted versus conventional laparoscopic radical hysterectomy in cervical cancer stage IB1. Int J Med Sci. 2023;20(3):287–291. doi:10.7150/ijms.79830.
14. Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34(28):3661–3679. doi:10.1002/sim.6607.
15. Chesnaye NC, Stel VS, Tripepi G, et al. An introduction to inverse probability of treatment weighting in observational research. Clin Kidney J. 2021;15(1):14–20. doi:10.1093/ckj/sfab158.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.