")
Back to Journals » Clinical Ophthalmology » Volume 17
Limited Clinical Value of Anti-Retinal Antibody Titers and Numbers in Autoimmune Retinopathy
Authors Rujkorakarn P , Margolis MJ, Morvey D, Zhou Y , Foster CS
Received 14 January 2023
Accepted for publication 1 March 2023
Published 7 March 2023 Volume 2023:17 Pages 749—755
DOI https://doi.org/10.2147/OPTH.S404826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ploysai Rujkorakarn,1– 3 Michael J Margolis,1,2 Diana Morvey,1,2 Yujia Zhou,1,2 C Stephen Foster1,2,4
1Massachusetts Eye Research and Surgery Institution, Waltham, MA, USA; 2The Ocular Immunology and Uveitis Foundation, Waltham, MA, USA; 3Suddhavej Hospital Department of Ophthalmology, Mahasarakham University, Maha Sarakham, Thailand; 4Department of Ophthalmology, Harvard Medical School, Cambridge, MA, USA
Correspondence: C Stephen Foster, Massachusetts Eye Research and Surgery Institution, 1440 Main St. #201, Waltham, MA, 02451, USA, Tel +1 781 891-6377, Fax +1 781 647-1430, Email [email protected]
Purpose: To assess the possible correlation of anti-retinal antibody titers and number of anti-retinal antibodies with outcome measurements including visual acuity, subjective vision loss, visual field, and electroretinography in patients with autoimmune retinopathy.
Design: Single-center, retrospective cross-sectional study.
Patients and Methods: Patients with autoimmune retinopathy who underwent anti-retinal antibody testing at least twice during their follow-up were enrolled. Anti-retinal antibody titers and numbers were grouped as improved, stable, or worsened. Outcomes included Snellen visual acuity, patient-reported vision loss, Humphrey visual field mean deviations, and electroretinography parameters.
Results: Thirty-one eyes among 16 patients with autoimmune retinopathy were included. Between-group analyses of visual acuity, subjective vision loss, visual field, and electroretinography outcomes did not reveal any significant differences by anti-retinal antibody titer or number group at a 95% confidence interval.
Conclusion: Changes in anti-retinal antibody titers or numbers were not associated with any vision outcome. Repeated anti-retinal antibody testing may be unnecessary after diagnosis of autoimmune retinopathy and detection of an anti-retinal antibody.
Keywords: autoimmune retinopathy, anti-retinal antibody, visual field, electroretinography, outcome measurements
Introduction
Autoimmune retinopathy (AIR) is a rare group of autoimmune diseases driven by auto-antibodies against the retina and typically results in progressive vision loss. Most instances primarily affect the peripheral retina and are characterized as either paraneoplastic (pAIR) or non-paraneoplastic (npAIR). Differences in disease course also exist between the two groups. The paraneoplastic group, including cancer-associated retinopathy (CAR) and melanoma-associated retinopathy (MAR), usually involves the pigment epithelial membrane while the non-paraneoplastic group does not.1
Early stages of the disease often present with a normal fundus examination. However, pigment epithelium damage and vascular attenuation may be seen in later stages. Patients may report unilateral, bilateral, or asymmetric scotomas, photopsias, visual field defects, and rapid progressive visual loss. Objective central visual acuity may be decreased if the macula is affected. Perimetry may also reveal visual field deficits and scotomas, often correlating with retinal damage and inflammation seen on optical coherence tomography (OCT), fundus autofluorescence (FAF) and fluorescein angiography (FA). In addition, electrophysical activity of retinal rod and cone cells may be assessed by electroretinography (ERG) and the integrity of the retinal pigment epithelium may be measured with electro-oculograms (EOGs).1,2 Treatment involves the use of corticosteroids, immunomodulatory therapies (IMTs), and intravenous immunoglobulin (IVIG) with regular follow-up.
The rarity of the disease complicates efforts to draft a diagnostic criterion aside from the presence of serum antiretinal antibodies (ARAs), which are essential for diagnosis. Antiretinal antibodies may be classified by serum titers and number of binding targets. However, associations between serum ARAs and clinical outcomes have been questionable. The aim of this study is to examine correlations between ARA titers and numbers, and outcome measurements including visual acuity, subjective vision loss, visual fields, and ERG findings.
Materials and Methods
Patients
This was a single-center, retrospective study of patients with AIR who presented to the Massachusetts Eye Research and Surgery Institution (MERSI) between August 2011 and August 2021. Approval for this study was obtained through the New England Independent Review Board which issued a waiver of informed consent based on standard procedures for retrospective chart reviews. Study practices were performed in accordance with the Declaration of Helsinki and were compliant with the Health Insurance Portability and Accountability Act.
Diagnosis criteria for AIR included the presence of serum ARAs with at least one of the following findings not better explained by another etiology: 1. vision symptoms including vision loss, scotomas, visual field deficits, photopsias, nyctalopia, or photosensitivity; 2. abnormal ERG; 3. abnormal fundus examination with vascular attenuation, retinal pigment epithelial changes, retinal atrophy, or optic disc pallor. All patients were diagnosed with AIR by one of the three experienced uveitis specialists (Peter Y. Chang, MD, Stephen D. Anesi, MD or C. Stephen Foster, MD).
The electronic medical records of all AIR patients with ARA testing at least twice during follow-up were included. Data on age, sex, race, subjective visual loss, Snellen best-corrected visual acuity (BCVA) within one week of ARA testing, ocular comorbidities, systemic diseases, family history of cancers and autoimmune diseases, current medications, related laboratory examinations, and ocular findings on slit-lamp microscopy were analyzed. Both eyes were included except for monocular patients. Each eye was considered independent in statistical analysis. Data were recorded within 3 months of serum collection for ARA testing.
Ophthalmic Testing
Two ERG machines were used according to the standard protocol recommended by the International Society for Clinical Electrophysiology of Vision.3,4 Full-field ERG (ffERG) with SG-2002 Ganzfeld system (LKC Technologies, Gaithersburg, MD) parameters consisted of 30-Hz flicker implicit time.5 Diopsys® Fixed Luminance Flicker (FL-flicker) and Multi-Luminance Flicker (ML-flicker) ERG parameters included FL-flicker magnitude and phase, ML magnitude and phase area under the curve (AUC),6 but were later excluded due to small sample size (4 patients).
Visual field mean deviations (MDs) were obtained with the Humphrey Visual Field Analyzer (Carl Zeiss Meditec Inc., Dublin, California, USA) using the Swedish Interactive Threshold Algorithm (SITA) fast 24–2 test protocol. Short-wavelength automated perimetry (SITA-SWAP) was performed in some patients with previous suspicion for birdshot chorioretinopathy as it has been shown to be more sensitive.7,8
ARA testing was performed at the Casey Eye Institute Ocular Immunology Laboratory, Oregon Health & Science University, currently the only Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory in the United States for ARA testing. Western blot (WB) was used to detect specific retinal proteins based on molecular weight in kilodaltons (kDa), and repeated titers were reported by the laboratory as increasing, decreasing, or no change according to standard protocols.9 ARA changes were considered improved if there was a decrease in ARA titers or number of WB bands, stable if there was no change in ARA titers and number of WB bands, and worsened if there was an increase in ARA titers or appearance of new WB bands.
Statistical Analysis
Data collection and management was performed on Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA). Appropriate parametric tests were performed, and assumptions assessed on IBM SPSS 28 (International Business Machines Corp., Armonk, NY, USA). A 95% confidence interval was used for statistical significance unless otherwise stated. Snellen visual acuities were converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis. All vision outcomes were averaged between both eyes at each time point.
Results
Sixteen patients with AIR had at least two serum tests for ARAs. Patient demographics are reported in Table 1. The mean age of patients was 52.5 years (SD 13.18) and most were female (81.25%). Fourteen of 16 patients were diagnosed with npAIR. The other two patients were diagnosed with MAR and CAR. One patient had a history of cutaneous malignant melanoma, and one patient had a history of squamous cell carcinoma of the mandible and basal cell carcinoma of the medial canthus. One patient had a history of monoclonal gammopathy. Seven patients had a family history of malignancy. One-third of patients had another autoimmune disease such as spondyloarthropathy, systemic lupus erythematosus, ocular cicatricial pemphigoid, or psoriasis. The most common presenting symptoms were decreased vision (93.75%), followed by visual field deficits (37.5%) and nyctalopia (31.25%). Ocular examination findings by slit-lamp microscopy and indirect fundoscopy are described in Table 2. The most common ARA targets (Table 3) in our patients were α-enolase (46 kDa), followed by carbonic anhydrase II (30 kDa).
 |
Table 1 Autoimmune Retinopathy Patient Characteristics |
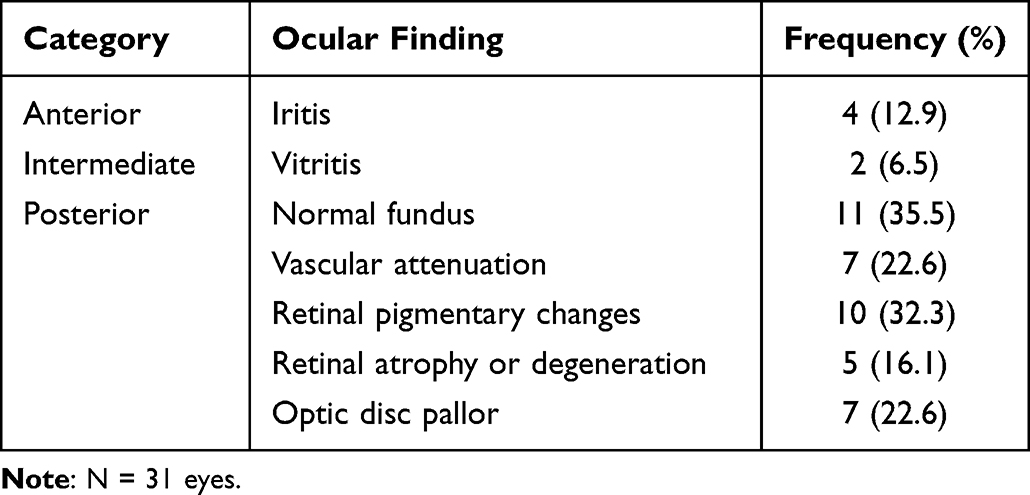 |
Table 2 Ocular Findings of Autoimmune Retinopathy on Initial Examination |
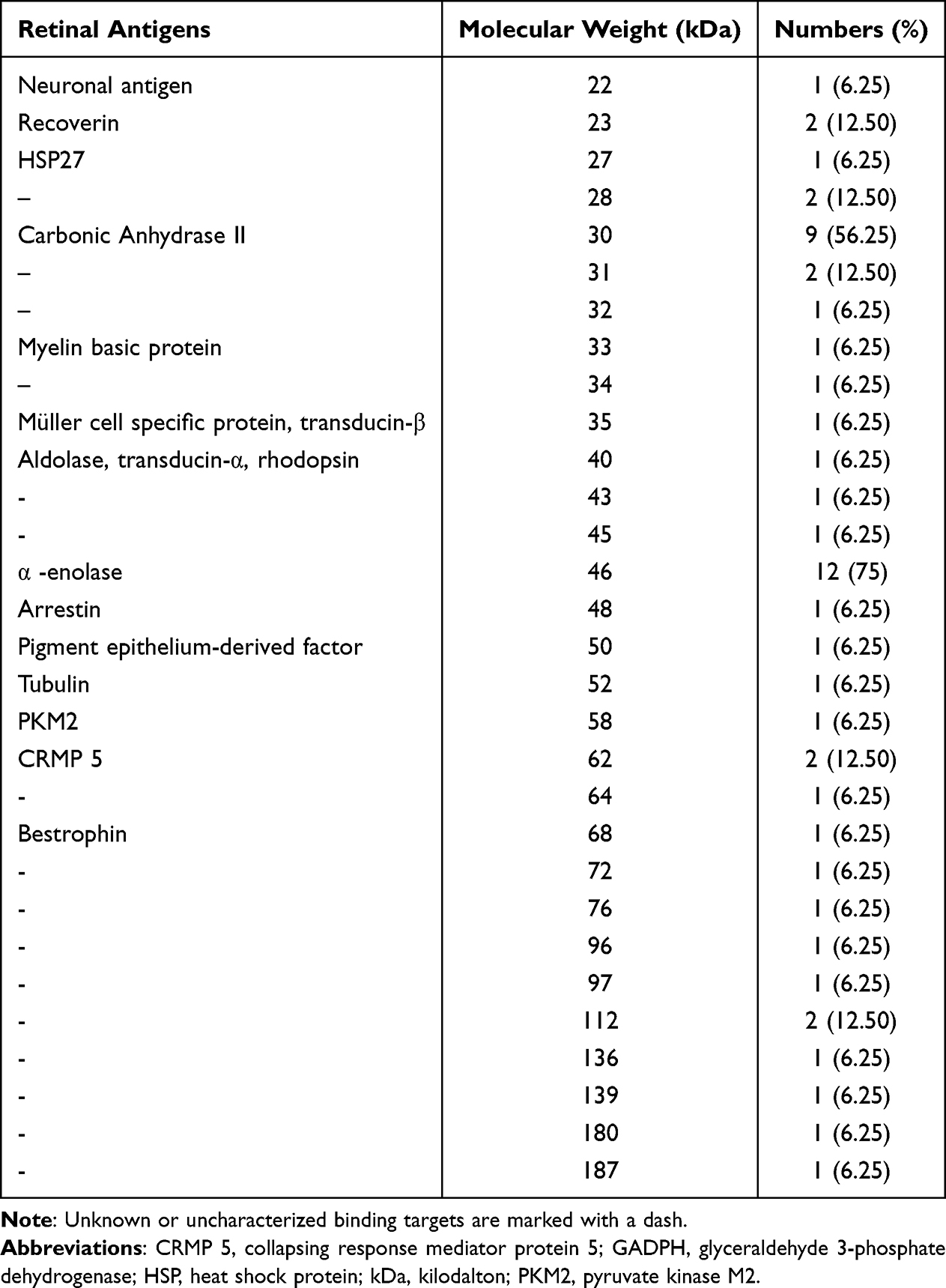 |
Table 3 Anti-Retinal Antibodies at Diagnosis by Western Blot |
Between-group analyses of change in visual field mean deviations (ANOVA, p = 0.189), 30-Hz flicker implicit times (ANOVA, p = 0.679), or logMAR visual acuities (ANOVA, p = 0.820) did not reveal any significant differences by ARA status (Figure 1). Only four patients had repeated Diopsys measurements, and statistical power was insufficient to draw any reliable conclusion. Kruskal–Wallis H-test also did not reveal any association between ARA status and patient-reported vision symptom change (H = 0.751, p = 0.687).
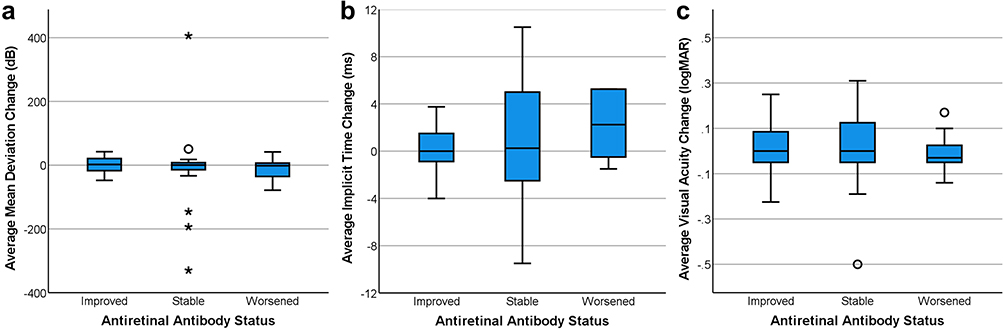 |
Figure 1 Boxplots of vision change compared by antibody status. Circles indicate outliers and asterisks indicate far outliers. (a) Average change in visual field mean deviations for both eyes in decibels, (b) average change in ERG implicit time for both eyes in milliseconds, and (c) average change in visual acuity for both eyes in logMAR. |
Discussion
Diagnosis and management of AIR is complicated by its low incidence, lack of standard diagnostic criteria, lack of management guidelines, and limited availability of clinical biomarkers. Therefore, multimodal assessment is necessary for diagnosis and follow-up of treatment response. This practice pattern, however, may result in delayed diagnosis and treatment due to multiple tests and serologies needed to rule out more common and likely diagnoses. Within this delay, AIR may cause rapidly progressive vision loss.
The presence of ARAs is currently the most definitive modality for diagnosis. Some antibodies are specific for the retina, such as recoverin (23 kDa) and rhodopsin (40 kDa),10 while others such as α-enolase (46 kDa) are not.11 Numerous antibodies have been reported to be associated with AIR such as carbonic anhydrase (30kDa), arrestin (48 kDa), Muller-cell-specific antigen (35 kDa), and transducing (35 or 40 kDa). The most commonly detected and relevant antibodies include recoverin, α-enolase (46 kDa), and transient receptor potential cation channel subfamily M member 1 (TRPM1), while recoverin and α-enolase are the most widely studied.2,11 ARAs can be found in other ocular diseases such as retinitis pigmentosa, Vogt-Koyanagi-Harada, sympathetic ophthalmia, toxoplasma retinochoroiditis, diabetic retinopathy, exudative age-related macular degeneration, and cystoid macular edema as well as in systemic diseases such as systemic lupus erythematous, multiple sclerosis, Behcet’s disease, and inflammatory bowel disease.12 ARAs may also be absent in diagnosed patients and present in healthy patients2,13,14 or patients with AIR quiescence for years.15
Three laboratory techniques have been described for serum ARA detection, including immunohistochemistry (IHC), WB, and enzyme-linked immunosorbent assay (ELIZA), among which IHC and WB are more commonly used. However, none of them are definitive. Each technique has advantages and disadvantages.11 For example, WB identifies antibodies based on the size of the protein and is both technically difficult and lacking in specificity. Therefore, two techniques should be performed concurrently to maximize sensitivity and specificity.16
The knowledge on correlation of ARAs with clinical presentation and treatment outcomes is limited. Saito et al reported a patient complained night blindness and central visual loss, but WB analysis did not detect antibodies. One year after presentation, an ARA was detected but systemic workup did not reveal malignancy. Two years after presentation, BCVA continued to decrease. On repeat examination for malignancy, the patient was diagnosed with colonic adenoma. ARA seropositivity may therefore be indicative of malignancy and demonstrates the value of repeat ARA testing in ARA seronegative patients with a strong clinical suspicion for AIR.17 We similarly report that one patient who presented with worsening vision was diagnosed with presumptive AIR and treated with IMTs. ERG testing disclosed further deterioration in the electrophysiologic parameters while on IMTs. Two repeated ARA tests were initially negative, but repeated testing 3 months later demonstrated ARAs. Ten Berge et al demonstrated that antibody staining between the inner nuclear layer and the outer plexiform layer and/or between the outer nuclear layer and the photoreceptors on indirect immunofluorescence was more common in patients with a visual acuity of <0.1.2 Sudden onset of vision loss was more often related to anti-recoverin, anti-P62, and anti-arrestin in CAR.18
Presentation of visual loss and severe deterioration have been found more often in ARA seropositive women with breast cancer, compared to seronegative women.19 Another case report showed decrease or absence of antibody titer corresponding to improvement in VA in CAR after a variety of treatments including plasmapheresis, chemotherapy, and prednisone.20–22 Conversely, antibody titers increased while BCVA worsened.20 Therefore, some ophthalmologists hypothesized that ARA titers can be used as a biomarker of disease activity. However, there was a case where BCVA did not improve after treatment despite the appearance of antibody.23 Another study by Stanwyck et al and Moussa et al did not show a correlation between ARA band decrease and VA, ERG parameters, or central retinal thickness on optical coherence tomography. They also concluded that ARAs were not a biomarker for response to treatment.24,25 In review, Fox et al developed consensus among uveitis specialists in the American Uveitis Society, concluding that there is not enough evidence to determine whether the number of positive ARAs or any specific subtypes are clinically relevant.16
Our study did not show significant correlation between ARA titers or numbers and VA, subjective vision, or investigations including ff-ERG parameter and MD in HVF. In summary, we found that ARA status is not associated with vision outcomes, with a few study limitations. AIR diagnosis in our cohort was limited to ARA testing by WB in a single laboratory and included both retina-specific and retina-nonspecific ARAs. The limited number of patients due to disease rarity also limits the statistical power of our methodology.
Conclusion
ARA testing is essential for diagnosis of AIR and should be repeated in seronegative patients if clinical suspicion is high, as seroconversion is sometimes observed. However, ARA titers and numbers are not significantly associated with vision outcomes or symptomatology. Therefore, after diagnosis of AIR with ARA seropositivity, repeat testing should not be used to monitor therapeutic response or indicate treatment modality. Also, the presence or absence of antibody should not be the primary driver for treatment decisions. Instead, multimodal investigation and clinical response should drive clinical decisions.
Disclosure
Dr C Stephen Foster reports personal fees from Bausch & Lomb, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Braithwaite T, Vugler A, Tufail A. Autoimmune retinopathy. Ophthalmologica. 2012;228(3):131–142. doi:10.1159/000338240
2. Ten Berge JC, Schreurs MW, Vermeer J, Meester-Smoor MA, Rothova A. Prevalence and clinical impact of antiretinal antibodies in uveitis. Acta Ophthalmol. 2016;94(3):282–288. doi:10.1111/aos.12939
3. Marmor MF, Fulton AB, Holder GE, et al. ISCEV Standard for full-field clinical electroretinography (2008 update). Doc Ophthalmol. 2009;118(1):69–77. doi:10.1007/s10633-008-9155-4
4. McCulloch DL, Marmor MF, Brigell MG, et al. ISCEV Standard for full-field clinical electroretinography (2015 update). Doc Ophthalmol. 2015;130(1):1–12. doi:10.1007/s10633-014-9473-7
5. Zacks DN, Samson CM, Loewenstein J, Foster CS. Electroretinograms as an indicator of disease activity in birdshot retinochoroidopathy. Graefes Arch Clin Exp Ophthalmol. 2002;240(8):601–607. doi:10.1007/s00417-002-0506-7
6. Maleki A, Ueberroth JA, Manhapra A, et al. Fixed-luminance and multi-luminance flicker electroretinography parameters in patients with early active birdshot chorioretinopathy. Ocul Immunol Inflamm. 2022;30(1):129–135. doi:10.1080/09273948.2020.1797113
7. Silpa-Archa S, Lee JJ, Boonsopon S, et al. Poor prognostic factors in patients with birdshot retinochoroidopathy. Retina. 2016;36(11):2220–2226. doi:10.1097/IAE.0000000000001051
8. Maleki A, Swan RT, Silpa-Archa S, Preble JM, He Y, Foster CS. Short-wavelength automated perimetry parameters at baseline and following remission in patients with birdshot retinochoroidopathy. Am J Ophthalmol. 2016;163(83–92.e6). doi:10.1016/j.ajo.2015.11.024
9. Forooghian F, Macdonald IM, Heckenlively JR, et al. The need for standardization of antiretinal antibody detection and measurement. Am J Ophthalmol. 2008;146(4):489–495. doi:10.1016/j.ajo.2008.05.046
10. Fox AR, Sen HN, Nussenblatt RB. Chapter 80. Autoimmune Retinopathies. In: Schachat AP, Wilkinson CP, Hinton DR, Sadda SR, Wiedemann P, editors. Ryan: Retina.
11. Grange L, Dalal M, Nussenblatt RB, Sen HN. Autoimmune retinopathy. Am J Ophthalmol. 2014;157(2):266–272.e1. doi:10.1016/j.ajo.2013.09.019
12. Bagheri S, Sobrin L. Autoimmune retinopathy: challenges in diagnosis and management. Adv Ophthalmol Optom. 2018;3(1):375–387. doi:10.1016/j.yaoo.2018.04.018
13. Chen JJ, McKeon A, Greenwood TM, et al. Clinical utility of antiretinal antibody testing. JAMA Ophthalmol. 2021;139(6):658–662. doi:10.1001/jamaophthalmol.2021.0651
14. Comlekoglu DU, Thompson IA, Sen HN. Autoimmune retinopathy. Curr Opin Ophthalmol. 2013;24(6):598–605. doi:10.1097/ICU.0b013e3283654e1e
15. Heckenlively JR, Lundy SK. Autoimmune retinopathy: an immunologic cellular-driven disorder. Adv Exp Med Biol. 2018;1074:193–201. doi:10.1007/978-3-319-75402-4_24
16. Fox AR, Gordon LK, Heckenlively JR, et al. Consensus on the diagnosis and management of nonparaneoplastic autoimmune retinopathy using a modified delphi approach. Am J Ophthalmol. 2016;168:183–190. doi:10.1016/j.ajo.2016.05.013
17. Saito W, Kase S, Ohguro H, Ishida S. Autoimmune retinopathy associated with colonic adenoma. Graefes Arch Clin Exp Ophthalmol. 2013;251(5):1447–1449. doi:10.1007/s00417-012-2131-4
18. Adamus G, Champaigne R, Yang S. Occurrence of major anti-retinal autoantibodies associated with paraneoplastic autoimmune retinopathy. Clin Immunol. 2020;210:108317. PMID: 31770612; PMCID: PMC6989367. doi:10.1016/j.clim.2019.108317
19. Adamus G. Latest updates on antiretinal autoantibodies associated with vision loss and breast cancer. Invest Ophthalmol Vis Sci. 2015;56(3):1680–1688. doi:10.1167/iovs.14-15739
20. Keltner JL, Thirkill CE, Tyler NK, Roth AM. Management and monitoring of cancer-associated retinopathy. Arch Ophthalmol. 1992;110(1):48–53. doi:10.1001/archopht.1992.01080130050025
21. Eltabbakh GH, Hoogerland DL, Kay MC. Paraneoplastic retinopathy associated with uterine sarcoma. Gynecol Oncol. 1995;58(1):120–123. doi:10.1006/gyno.1995.1194
22. Murphy MA, Thirkill CE, Hart WM
23. Guy J, Aptsiauri N. Treatment of paraneoplastic visual loss with intravenous immunoglobulin: report of 3 cases. Arch Ophthalmol. 1999;117(4):471–477. doi:10.1001/archopht.117.4.471
24. Stanwyck LK, Moussa K, Chan W, Aitken PA, Sobrin L. Lack of correlation between number of antiretinal antibodies and clinical outcome measures in autoimmune retinopathy patients. Ophthalmol Retina. 2019;3(11):1007–1009. doi:10.1016/j.oret.2019.06.007
25. Moussa K, Stanwyck LK, Sobrin L. Correlation of anti-retinal antibodies with clinical outcome measures before and after immunosuppressive treatment in autoimmune retinopathy patients. Invest Ophthalmol Vis Sci. 2018;59(9):4209.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.