Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Lifetime Prevalence and Determinants of Suicidal Ideation and Attempt Among All Patients Living with HIV/AIDS in Hiwot Fana Specialized Hospital, Harar, Ethiopia, 2020
Authors Gebreegziabhier Kindaya G, Kassaw Demoze C ![]()
Received 9 April 2020
Accepted for publication 31 July 2020
Published 6 August 2020 Volume 2020:12 Pages 331—339
DOI https://doi.org/10.2147/HIV.S257502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Gebreslassie Gebreegziabhier Kindaya,1 Chalachew Kassaw Demoze2
1Department of Psychiatry, College of Health Science, Aksum University, Aksum, Ethiopia; 2Department of Psychiatry, College of Medicine and Health Science, Dilla University, Dilla, Ethiopia
Correspondence: Chalachew Kassaw Demoze Email [email protected]
Background: Suicide is a psychiatric emergency and the second leading cause of death among youths. Suicide risk is 7 to 36 times greater among PLWHA as compared to the general population. This study was aimed at determining the prevalence of suicide and its associated factors among PLWHA and attendings at Hiwot Fana Specialized University Hospital, Ethiopia, 2020.
Patients and Methods: We conducted a cross-sectional study on 412 randomly selected respondent PLWHA and attendingz at Hiwot Fana Specialized University Hospital from February 1–March 1, 2020. The interviewers administered a structured questionnaire consisting of the World Health Organization Composite International Diagnostic Interview (CIDI) tool to measure suicidality. We used the clinical records to collect clinical variables of the respondents. We used simple logistic regression ≤ 0.25 at p-value ≤ 0.25 and multiple logistic regression at p-value ≤ 0.05 to identify the predictor variables of the outcome.
Results: A total of 412 participants have completed the questionnaire, with a response rate of 97.4%. The majority, 252 (61.2) of the participants were female, while 112 (27.2%) of the respondents were in the age group of 28– 37. The prevalence of suicidal ideation and attempt among PLWHA was 24.3% (CI; 20.4, 28.4) and 12.6% (9.5– 15.8), respectively. Predictors for suicidal ideation were being in extreme poverty, living alone, widowed, CD4 level less than 250, and current alcohol use, and for suicidal attempt were an urban residence, stage IV HIV, family history of suicide, and depression.
Conclusion: Nearly one-fourth of the respondents reported suicidal ideation. So, early screening and working on those identified predictors of suicidality is vital to prevent the mortality of it in PLWHA.
Keywords: suicide, HIV/AIDS, Harar, Ethiopia
Introduction
Suicide is an intentional, deliberate, self-inflicted act. Suicidal behavior is a leading cause of injury and death worldwide. Suicidal ideation is the initial phase of the suicidal process, preceding attempted suicide; which is the risk factor for completed suicide, and is also a potentially fatal event.1,2
Suicide is a global public health concern, which is the 10th Leading cause of death worldwide, the second leading cause of death among those aged 15–29 years.3 Globally every year, almost one million people die from suicide; this is about 1.5% of all deaths.4 In 2030, the number of inflicted death will increase by 30%, and suicidal compilation will also estimate to increase up to 1.53 million per year. In other words, there will be one death every 20 seconds and one attempt every 1–2 seconds.5
The suicide rate remains high among HIV-positive persons than in the general population. Comorbid psychiatric conditions among HIV-positive persons may partially explain the higher suicide rate, particularly in the ART era.6
Worldwide, it was estimated to be that 36 million people were living with HIV. There were 2.3 million new HIV infections globally, showing a 33% decline in the number of new infections from 3.4 million in 2001. And the majority of them around 25.5 million peoples with HIV are living in sub-Saharan-Africa, in Ethiopia, it was 0.6% among men and 1.2% women in the age (15–49).7,8
The Suicide risk among PLWHA was 7 to 36 times greater as compared to the general population. The most common psychiatric conditions seen in PLWHA were depression, emotional disorder, bipolar disorder, and psychotic illness and contribute to drug non-adherence.9
Predictive factors for suicidal ideation and attempts among PLWHA were low income, single marital status, substance abuse, depression, multiple physical symptoms, loneliness, lack of support, and being younger age.10
The magnitude of suicidal ideation among PLWHA in Kenya was 10.5%,11 China 31%,12 and Nigeria 34.7%.13 While the magnitude of suicidal attempt in Uganda was 3.9%14 and France 23%.15 The prevalence of suicidal ideation and attempt in Addis Ababa was 22.5% and 13.9%, respectively.16
Although few studies conducted the suicidality among PLWHA in Sub Saharan–Africa countries, the problem is still increasing. In Ethiopia, there are limited data on the magnitude of suicidal ideation and attempt among PLWHA. Therefore, the current study aimed to determine the prevalence of suicidal ideation and attempt and its associated factors.
Methods and Materials
Study Design, Period, Area and Participants
This study was a hospital-based cross-sectional study design conducted from February 1 to March 1, 2020, at Hiwot Fana Specialized university hospital, Harar. It is in Harar town, kebele 14, and the ART service was started in 1997 by 180 clients but, now the hospital gives this service for 915 patients monthly. All PLWHA and attending at ART clinic outpatient service were the source of the population for the study, and those who came during the study period were study populations. All respondents age 18+ were the inclusion criteria of the study, and those with serious illness who were not able to communicate were the exclusion criteria for the study.
Sample Size Determination and Sampling Technique
The sample size, we used a single population proportion formula incorporating the following assumptions: the proportion of patients with an unknown population of suicidal ideation and attempt as 50%, with 95% certainty and 5% of maximum discrepancy between the upper and lower sample size. By adding a 10% non-response rate, the total calculated sample size was 423 participants. The sampling technique of the study was a simple random sampling technique and computer generating method used to select the required number of samples for the study.
Data Collection Tools
The data were collected using a structured interview questionnaire. We used chart review to gather data regarding stages of HIV, CD4 count, and history of tuberculosis and mental illness.
We used the World Bank international poverty line (1.90 $ per day), which had three classifications, under the poverty line (< $1.90), on the poverty line ($1.90) and above the poverty line (> $ 1.90) to classify respondents current poverty status.17
To assess the current Suicidal ideation and attempt, we used the World Mental Health (WMH) survey initiative version 3.0 of the World Health Organization (WHO) composite international diagnostic interview (CIDI) (validated in Ethiopia). If the patient answers “yes” for the question: have you ever seriously thought about committing suicide?; He/she had suicidal ideation and also if the patient report “yes” for the item question: have you ever attempt suicide?; He/she had a Suicide attempt.18
We used the Patient health questioner (PHQ-9) assessment tool to measure depression with a cut point of ≥10.19
We used the Oslo social support scale (Oslo-3), which had three classifications based on their score of 14. (Poor support: 3–8, Moderate support: 9–11 and Strong support: 12–14) to measure their social Support level.20
The final standard tool was Alcohol, Smoking, and Substance Involvement Screening Test version 2.0 (ASSIST), used for measuring the lifetime (at least once in a lifetime), and current use (less three than) history of substance (alcohol, khat, tobacco, others).21
Data Collection Procedure
Data were collected using face to face interviews, and card review at ART outpatient service. Four professional nurses for data collector and two mental health nurses for supervisor were recruited from Hiwot Fana specialized university hospital. The training was given for data collectors and supervisors by the principal investigator on the aims and procedures of data collection.
Data Quality Control
We translated a standardized questionnaire into local languages, Amharic, and back to English for consistency. We used the Amharic version of the questioner to collect the data. We did the pretest on 5% of the total sample at Jegula hospital for clarity of questionnaires. During data collection, the questioner was checked for its completeness daily by data collectors, supervisors, and then by the investigator. If there was a problem encounter during data collection, there was a discussion with supervisors and data collectors accordingly.
Data Processing and Analysis
The data were cleaned, coded, and entered into the computer using Epi-data version 3.1 then exported to SPSS (Statistical Package for the Social Sciences) version 20. We used the rule of thumb (p<0.25) in binary logistic regression to determine candidate variables for multiple logistic regression analysis. The multiple logistic regression analysis at p ≤ 0.05 used to identify variables independently predicts the outcome variable at a 95% confidence interval.
Ethical Consideration
Ethical approval was obtained from Haramaya University College of Medical and Health Science, and our study was conducted in accordance with the Declaration of Helsinki.
We discussed with the study participants about the objective of the study, voluntarism, and confidentiality. We obtained the written Informed consent from all respondents who were participating in the study.
Result
Sociodemographic Characteristics of the Respondent
A total of 412 participants were complete the questioner with a response rate of 97.4%. Majority 252 (61.2) of the participants were female, while 112 (27.2%) of the respondents were in the age group of 28–37. The mean age of respondents was 40.45 years old (SD=±12. 6). Among the study participants, 200 (48.5%) was an orthodox Christian, and 360 (87.4%) were living at Urban. Majority 260 (63.1%) were married, 120 responders could not read and write, and 240 (60.2%) were employed. Nearly half of 181 (43%) of the individuals who involved in this study were living under extreme poverty (<1.90$ per day income), and 176 (42.7%) participants were living with their partner (Table 1).
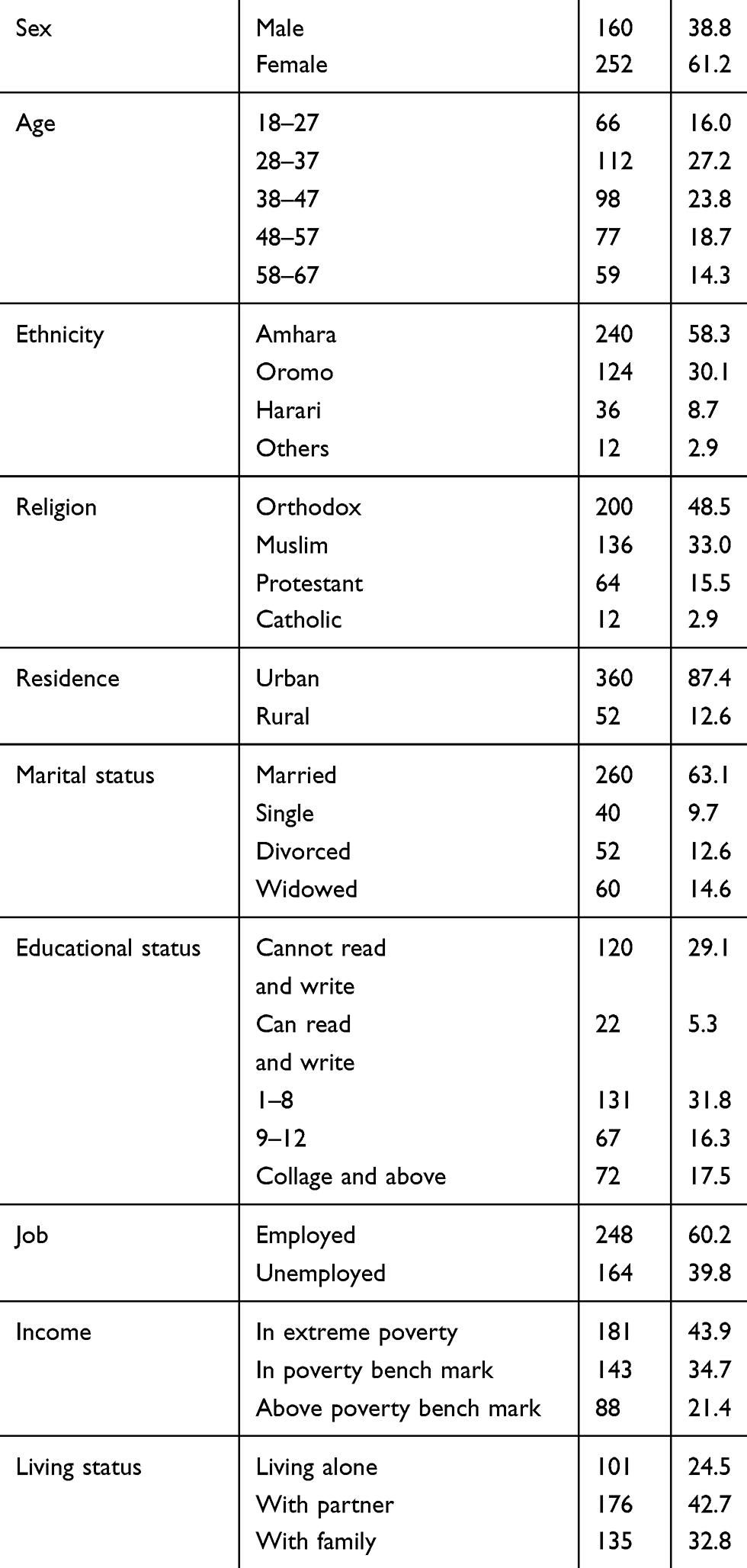 |
Table 1 Sociodemographic Characteristics of PLWHA Attending ART Clinic at HFSUH, Harar, Ethiopia, 2020 (N=412) |
Clinical Characteristics of Study Participants
From this study, 159 (38.6%) had stage I HIV status, 124 (30.1%) were 2–5 years since they know their HIV status, 228 (55.3%) had comorbid tuberculosis, 128 (31.1%) had comorbid mental illness, 137 (33.3) had a family history of suicide, and 213 (51.7%) had depression (Table 2) .
Social Support Level
Among the study participants, Majority 275 (66.7%) had poor social support, 23.5% had moderate social support, and 9.7% had strong social support.
Substance Use Conditions of Study Participants
Among the respondents ever users of alcohol were reported by 48.5%, while 20.6% were current users (Figure 1).
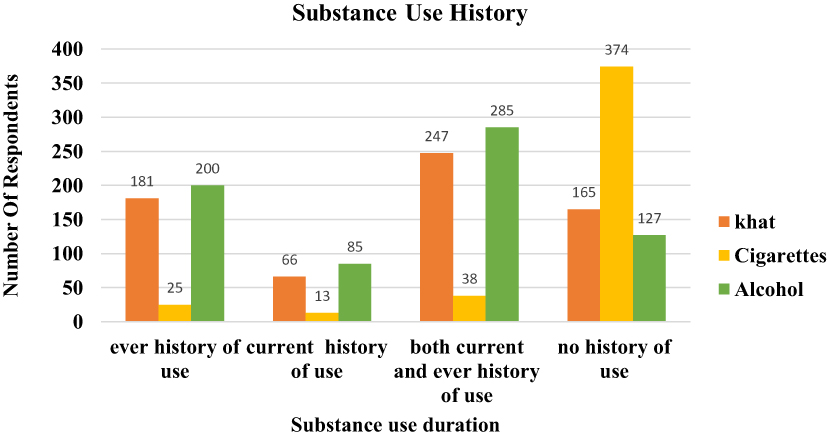 |
Figure 1 The frequency percentage of ever and current substance users of PLWHA attending ART clinic at HFSUH, Harar, Ethiopia, 2020, (N=412). |
Prevalence and Determinants of Suicidal Ideation and Attempt
The prevalence of suicidal ideation and attempt among PLWHA was found 24.3% (CI; 20.4, 28.4) and 12.6% (9.50−15.8) respectively. Multiple logistic regression analysis showed that there was a statistically significant association between suicidal ideation and being widowed (AOR= 1.73, 95%: 1.01,2.96), under extreme poverty (AOR=2.40, 95% CI: 1.05,5.47), living alone (AOR=8.50 95% CI: 3.60,20.03), a CD4 level less than 250 (AOR= 3.97; 95% CI: 1.90, 8.27), and Current alcohol use (AOR=6.73; 95% CI: 3.26, 13.88).
The odds of having suicidal ideation 1.73 times higher among widowed than the married one. The odds of having suicidal ideation were 2.40 times more among those living in under extreme poverty than living above the poverty line. The odds of having suicidal ideation were 8.50 times higher in those who are living alone than those living with family. The odds of having suicidal ideation were 3.92 times more among respondents CD 4 levels than the referent group (>1000). The odds of suicidal ideation were 6.73more in current alcohol users than not (Table 3).
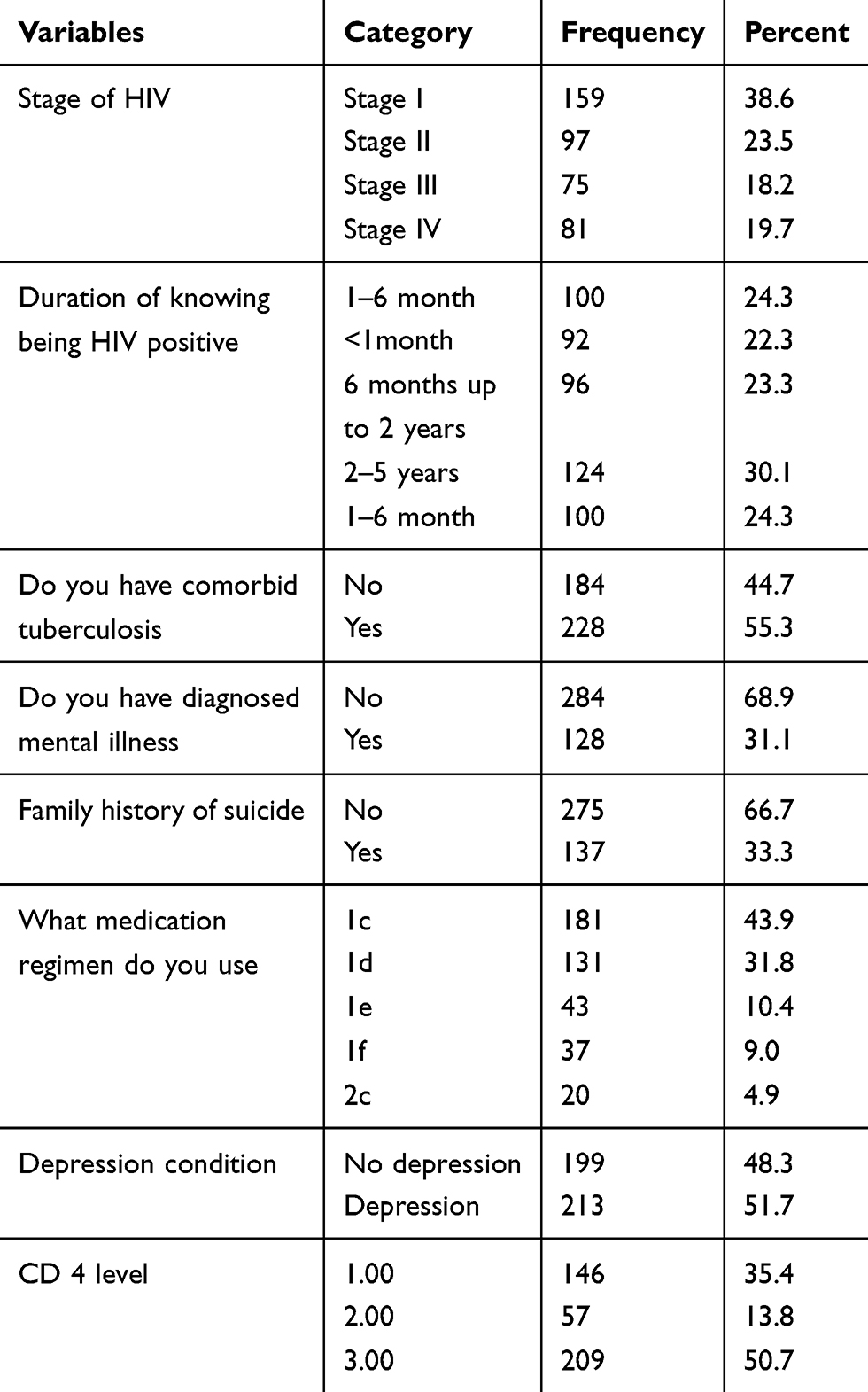 |
Table 2 Clinical Status of PLWHA Attending ART Clinic at HFSUH, Harar, Ethiopia, 2016 (n=412) |
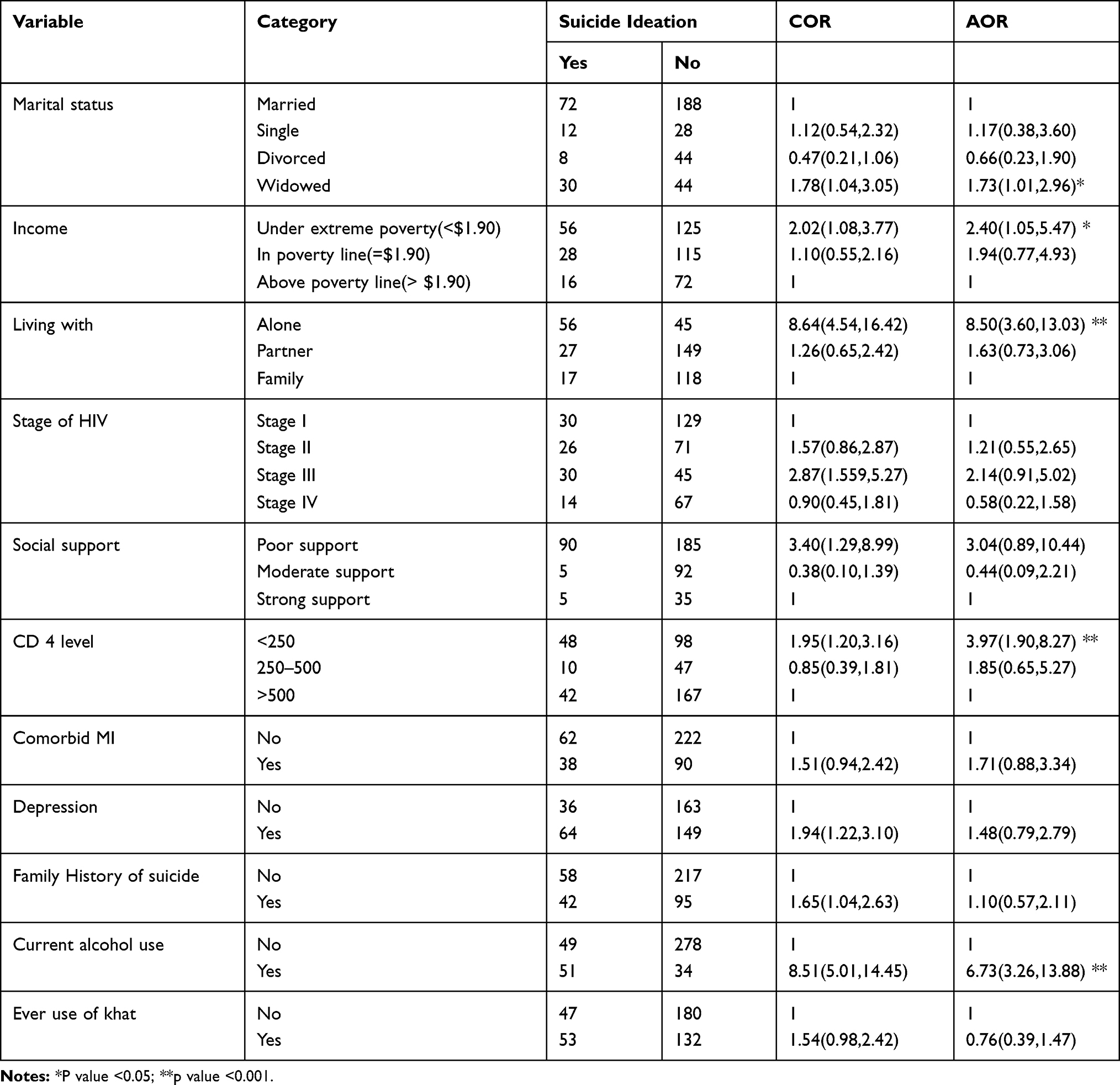 |
Table 3 Factors Associated with Suicidal Ideation Among PLWHA Attending ART Clinic at HFSUH, Harar, Ethiopia, 2016 (n=412) |
Multivariate analysis showed there was a statistically significant association between suicidal attempt and Urban residence (AOR=4.16; 95% CI: 1.62, 10.72), stage IV HIV stage (AOR=5.65; 95% CI: 2.14, 14.93), Family history of suicide (AOR=2.13, 95% CI: 1.13, 4.30) and depression (AOR=4.10; 95% CI: 1.92, 8.79). The respondents were living in urban were 4.16 times more likely to have suicidal attempts than those who were living in rural. The odds of having suicidal attempts among those who were in stage IV were 5.65 times more than those in stage I. Those who had a family history of suicide were 0.24 times more likely to have suicidal attempts than not having a family history of suicide. The odds of suicidal attempts in those having depression were 4.10 times higher than those without depression (Table 4).
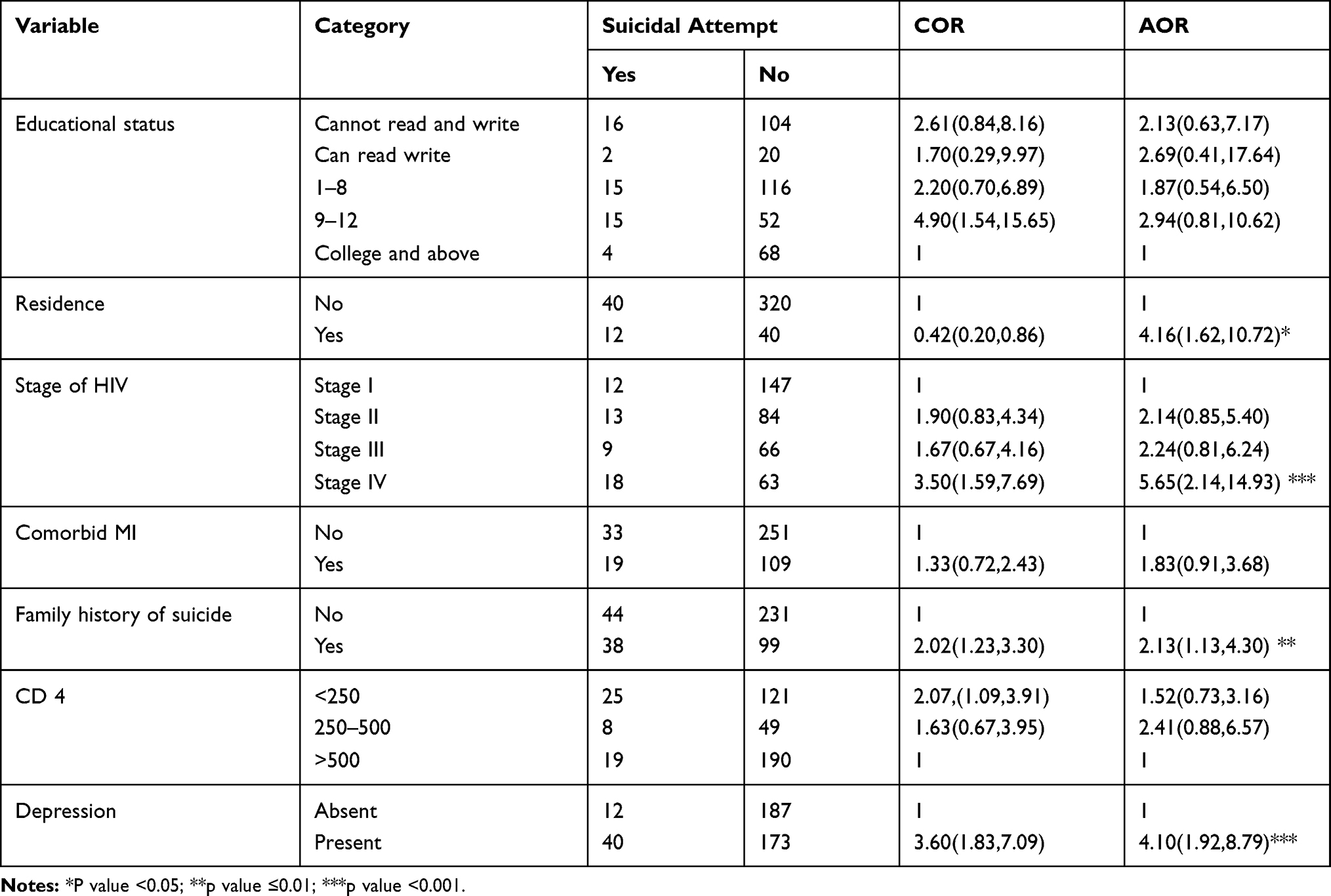 |
Table 4 Factors Associated with Suicidal Attempt Among PLWHA Attending ART Clinic at HFSUH, Harar, Ethiopia, 2016 (n=412) |
Discussion
Among the total 412 respondents, the prevalence of suicide ideation was 24.3% (CI: 20.4%–28.4%). This study was inconsistent with the studies done in the USA, 27%.9
It was higher than the study conducted in the general adult population and PLWHA in Addis Ababa, Ethiopia, in 1994.16,22 This difference may be due to the variation in the study group and the increasing prevalence of mental illness. It was also higher than the study reported in South Africa, 17.1%,23 Uganda 7.8%.14 The possible reason for this variation may be due to the difference in study design, sample size, and the socio-cultural difference between these countries. This study report was lower than the study from the United States in which suicidal ideation rate of diagnosis was 30.6%,24 and United Kingdom 31%.25 This difference may be due to the socioeconomic status and the student design difference, which was a retrospective cohort design used in the UK. It is also lower than the study conducted in Nigeria, which was 34.7%.13 This may occur due to the difference in study design and tool difference.
From all respondents, 52 (12.6%), (95% CI: 9.5–15.8%) reported suicidal attempt. This study in line with the study conducted in the United States at 13%.26 Whereas, the magnitude report of this study was lower than the studies conducted in the United States, 50%.27 It is also higher than the studies conducted in New York at 26%,28 Puerto Rican 22%,29 and France 23%.15 The possible reason for this variation may be due to the difference in socioeconomic status, culture (willingness for open discussion on sensitive issues is uncommon in developing countries), sample size, study design, study period, and tool.
This study was reported higher than the studies conducted in Nigeria at 9.3%13 and Uganda 3.9%.14 It might be due to the variation in sample size, time of the investigation, and study design.
Being widowed was significantly associated with suicidal ideation. Those who were widowed were 1.73 times more likely to have suicidal ideation than a married one (AOR= 1.73; 95% CI (1.01, 2.96). It was supported by the study done in Uganda.30 The psychological impact of widowed such as loneliness, low self-esteem, and difficulty coping with loss leads to suicidal ideation and attempt.
Those who were living under extreme poverty were 2.4 times more to attempt suicide than who were living above the poverty line (AOR=2.4; 95% CI: 1.05, 5.47). This finding was supported by the study done in India.31 The low monthly income has an impact on life dissatisfaction, in addition to their stress( having HIV), may prone them to a suicidal attempt. Additionally, those who are under extreme poverty may lack to fulfil their basic needs, which leads to hopelessness and suicidal thoughts.
The odds of having suicidal ideation were 8.5 times higher among those who live alone than living with their family (AOR=8.5; 95% CI: 3.6, 20.03). Supported by studies conducted in Ethiopia and Uganda.22,32 It might be because of lacking physical and psychological support.
Those who had CD 4 level less than 250 were 3.97 times more likely to have suicidal than those who had CD 4 levels more than 1000 (AOR=3.97; 95% CI: 1.90, 8.27). This finding was consistent with the study done in Addis Ababa.16 The low baseline of CD 4 counts is associated with high-level complications and chronic deterioration, which leads to hopelessness difficulty of coping with their many physical symptoms and suicidal ideation.
Another factor that had significant association with suicidal ideation was substance use condition. Current alcohol users were 6.73 times more to have suicidal ideation than non-users (AOR=6.73; 95% CI: 3.26, 13.88). This finding was supported by the study done in Addis Ababa.16 It might be due to the toxic effect of the alcohol, and the interaction with ART, which may affect the treatment adherence negatively and result in complications of illness, worthlessness, and suicidal thoughts.
Those who were living in urban were 4.16 times more to attempt suicide than those living in rural (AOR=4.16; 95% CI: 1.62, 10.72). This finding was inconsistent with the study done on mettu university students.33 Living in a rural residence might contribute to strong cultural and social in-acceptability of attempting suicide.
Those who were WHO stage of HIV stage IV were 5.65 times more likely to attempt suicide than those in stage I (AOR=5.65; 95% CI: 2.14, 14.93). This study was in line with the study done in Addis Ababa.16 The WHO stage IV is associated with an opportunistic infection, chronic deteriorating complicated nature of the illness, and immune compromising reaction, which all affect the psychological coping of the respondent’s illness and contribute to low self-esteem and thought of self-harm.
Participants with a family history of suicide were 2.13 times more likely to attempt suicide than without a family history of suicide (AOR= 2.13, 95% CI: 1.13, 4.30). It was supported by the study done in Addis Ababa.16 The possible reason might be the fact that genetics has a high impact on suicidality.
The odds of suicidal attempt were 4.10 times higher among depression than those with no depression (AOR=4.10 1.90, 8.79). It was supported by a similar study from Puerto pecan.29 This might be associated with the severity of depression and Neuro-amine neurotransmitter deficiency.
Limitation of the Study
The cross-sectional nature of the study makes it difficult to determine the direction of causality; therefore, further analytical findings would be needed to understand the direct causal relationships of variables.
Conclusion
This study found a high prevalence of suicidal ideation and attempt among PLWHA. The predictors of suicidal ideation were, being widowed, under the extreme poverty line, living alone, CD4 < 250, and current alcohol use, while living in urban, stage IV HIV stage, family history of suicide and depression were predictors of suicidal attempt. Therefore, early screening of suicidality among PLWHA is necessary for preventing the morbidity and mortality of mental illness on those groups of populations. There should be regular screening on those identified groups of respondents. Moreover, ART and Mental health services should be integrated and sustainable.
Abbreviations
AIDS, acquired immune deficiency syndrome; AOR, adjusted odds ratio; ART, anti-retroviral therapy; CD4, cluster of differentiation 4; CI, confidence interval; COR, crude odds ratio; HFSUH, Hiwot Fana Specialized University Hospital; HIV, human immune deficiency virus; PLWHA, patents living with human immune virus and acquired immune deficiency syndrome; WHO, World Health Organization.
Acknowledgment
We express great gratitude for the study participants, health care providers working on ART services, and Haramaya University College medical and health science for their invaluable support and cooperation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Lee JI, Lee MB, Liao SC, et al. Prevalence of suicidal ideation and associated risk factors in the general population. J Formos Med Assoc. 2010;109(2):138–147. doi:10.1016/S0929-6646(10)60034-4
2. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Lippincott Williams & Wilkins; 2011. doi:10.1371/journal.pmed1000097
3. Borges G, Nock MK, Abad JMH, et al. Attempts in the WHO World Mental Health Surveys. J Clin Psychiatry. 2011;71(12):1617–1628. doi:10.4088/JCP.08m04967blu.Twelve
4. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet Psychiatry. 2013;382(9904):1575–1586. doi:10.1016/S0140-6736(13)61611-6
5. Steiner G. Circulation of cerebrospinal fluid. Br Med J. 1964;1(5384):697. doi:10.1136/bmj.1.5384.697-a
6. Schlebusch L, Govender RD. Elevated risk of suicidal ideation in HIV-positive persons. Depress Res Treat. 2015;2015:1–7. doi:10.1155/2015/609172
7. Piot P, Bartos M, Ghys PD, Walker N, Schwartländer B. The global impact of HIV/AIDS. Nature. 2001;410:968–973. doi:10.1038/35073639
8. Daba S. HIV Prevention in Ethiopia National Road Map. November 2018:2–3.
9. Kalichman SC, Heckman T, Kochman A, Sikkema K, Bergholte J. Depression and thoughts of suicide among middle-aged and older persons living with HIV-AIDS. Psychiatr Serv. 2000;51(7):903–907. doi:10.1176/appi.ps.51.7.903
10. Komiti A, Judd F, Grech P, et al. Suicidal behaviour in people with HIV/AIDS: a review. Aust N Z J Psychiatry. 2001;35(6):747–757. doi:10.1046/j.1440-1614.2001.00943.x
11. Ndetei DM, Khasakhala LI, Mutiso V, Mbwayo AW. Suicidality and depression among adult patients admitted in general medical facilities in Kenya. Ann Gen Psychiatry. 2010;9:1–6. doi:10.1186/1744-859X-9-7
12. Wu YL, Yang HY, Wang J, et al. Prevalence of suicidal ideation and associated factors among HIV-positive MSM in Anhui, China. Int J STD AIDS. 2015;26(7):496–503. doi:10.1177/0956462414544722
13. Chikezie UE, Otakpor AN, Kuteyi OB, James BO. Suicidality among individuals with HIV/AIDS in Benin City, Nigeria: a case-control study. AIDS Care. 2012;24(7):843–845. doi:10.1080/09540121.2011.645008
14. Kinyanda E, Hoskins S, Nakku J, Nawaz S, Patel V. The prevalence and characteristics suicidality in HIV/AIDS as seen in an African population in Entebbe district, Uganda. BMC Psychiatry. 2012;12(1):63. doi:10.1186/1471-244X-12-63
15. Preau M, Bouhnik AD, Peretti-Watel P, et al. Suicide attempts among people living with HIV in France. AIDS Care. 2008;20(8):917–924. doi:10.1080/09540120701777249
16. Gebremariam EH, Reta MM, Nasir Z, Amdie FZ. Prevalence and associated factors of suicidal ideation and attempt among people living with HIV/AIDS at Zewditu memorial hospital, Addis Ababa, Ethiopia: a cross-sectional study. Psychiatry J. 2017;2017. doi:10.1155/2017/2301524
17. Jolliffe D, Prydz EB. Estimating international poverty lines from comparable national thresholds. J Econ Inequal. 2016;14(2):185–198. doi:10.1007/s10888-016-9327-5
18. Ambrosini PJ, Kaufman J, Birmaher B, et al. Historical development and present status of the schedule for affective disorders and schizophrenia for school-age children (K-SADS). J Am Acad Child Adolesc Psychiatry. 2000;39(1):49–58. doi:10.1097/00004583-200001000-00016
19. Gelaye B, Williams MA, Lemma S, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210(2):653–661. doi:10.1016/j.psychres.2013.07.015
20. Dalgard OS, Dowrick C, Lehtinen V, et al. Negative life events, social support and gender difference in depression. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–451. doi:10.1007/s00127-006-0051-5
21. Henry-Edwards S, Humeniuk R, Ali R, Poznyak V, Monteiro M, Poznyak Brief V. ASSIST Guidelines for Use in Primary Care. Geneva: World Heal Organ; 2003.
22. Kebede D, Alem A. Suicide attempts and ideation among adults in Addis Ababa, Ethiopia. Acta Psychiatr Scand. 1999;100:35–39. doi:10.1111/j.1600-0447.1999.tb10692.x
23. Schlebusch L. Suicidal Ideation in Seropositive Patients Seen at a South African HIV Voluntary Counselling and Testing Clinic. 2012:94–98.
24. Perry S, Jacobsberg L, Fishman B. Suicidal ideation and HIV. JAMA. 1990;263:679–682. doi:10.1001/jama.1990.03440050073036
25. Sherr L, Lampe F, Fisher M, et al. Suicidal ideation in UK HIV clinic attenders. AIDS. 2008;22:1651–1658. doi:10.1097/QAD.0b013e32830c4804
26. Badiee J, Moore DJ, Atkinson JH, et al. Lifetime suicidal ideation and attempt are common among HIV+ individuals. J Affect Disord. 2012;136(3):993–999. doi:10.1016/j.jad.2011.06.044
27. Shelton AJ, Atkinson J, Risser JMH, McCurdy SA, Useche B, Padgett PM. The prevalence of suicidal behaviours in a group of HIV-positive men. AIDS Care. 2006;18(6):574–576. doi:10.1080/09540120500274992
28. Cooperman NA, Simoni JM. Suicidal ideation and attempted suicide among women living with HIV/AIDS. J Behav Med. 2005;28(2):149–156. doi:10.1007/s10865-005-3664-3
29. Quintana-Ortiz RA, Gomez MA, Báez Feliciano DV, Hunter-Mellado RF. Suicide attempts among Puerto Rican men and women with HIV/AIDS: a study of prevalence and risk factors. Ethn Dis. 2008;18(2 Suppl 2):S2–224.
30. Mugisha J, Muyinda H, Kagee A, et al. Prevalence of suicidal ideation and attempt: associations with psychiatric disorders and HIV/AIDS in post-conflict northern Uganda. Afr Health Sci. 2016;16(4):1027–1035. doi:10.4314/ahs.v16i4.20
31. Jhansi D, Rai P, Malhotra AK. Section: community medicine suicide ideation in depressed people living with HIV/AIDS in section: community medicine. Int J Contemp Med Res. 2019;6(2):6–9.
32. Alice O’Dowd M, Biderman DJ, Patrick McKegney F. Incidence of suicidality in AIDS and HIV-positive patients attending a psychiatry outpatient program. Psychosomatics. 1993;34(1):33–40. doi:10.1016/S0033-3182(93)71925-8
33. Abdu Z, Hajure M, Desalegn D. Suicidal behavior and associated factors among students in mettu university, south west ethiopia, 2019: an institutional based cross-sectional study. Psychol Res Behav Manag. 2020;13:233–243. doi:10.2147/PRBM.S240827
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.