Back to Journals » Clinical Interventions in Aging » Volume 21
Lifetime Endurance Physical Activity Is Related to Better Cardiometabolic Profile but May Be Insufficient to Preserve Muscle Strength and Power in Middle Aged and Older Men
Authors Pigłowska M, Kwaśniewska M, Kostka J ![]() , Jegier A
, Jegier A ![]() , Drygas W, Dzięcioł KA
, Drygas W, Dzięcioł KA ![]() , Szmigielska K, Kostka T
, Szmigielska K, Kostka T ![]()
Received 17 December 2025
Accepted for publication 1 April 2026
Published 2 June 2026 Volume 2026:21 584734
DOI https://doi.org/10.2147/CIA.S584734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Małgorzata Pigłowska,1 Magdalena Kwaśniewska,2 Joanna Kostka,3 Anna Jegier,4 Wojciech Drygas,2 Karolina Agnieszka Dzięcioł,1 Katarzyna Szmigielska,4 Tomasz Kostka1
1Department of Geriatrics, Medical University of Lodz, Lodz, Poland; 2Department of Preventive Medicine, Medical University of Lodz, Lodz, Poland; 3Department of Physioprophylaxis, Medical University of Lodz, Lodz, Poland; 4Department of Sports Medicine, Medical University of Lodz, Lodz, Poland
Correspondence: Małgorzata Pigłowska, Department of Geriatrics, Medical University of Lodz, Pomorska Street 251, Lodz, 92-213, Poland, Email [email protected]
Purpose: The aim of this study was to compare the effects of lifetime endurance physical activity (PA) on cardiometabolic profile and muscle function in middle aged and older men.
Patients and Methods: The study was conducted in 59 men aged 66.7± 8.8 years, engaged in endurance training and followed for over 30 years. Biochemical and anthropometric measurements were taken. The Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was assessed. The submaximum exercise test was performed to verify physical fitness. The strength of multiple muscle groups was measured with dynamometers (Saehan, Microfet 2) and Keiser pneumatic resistance training equipment. Muscle power was examined with Keiser equipment and a friction-loaded cycle ergometer. Historical PA data were checked based on PA examinations performed in the past. Participants’ PA levels in the last 10 years were categorized and 3 groups with an equal number of participants were created: low, medium and high.
Results: The low PA group was characterized by inferior aerobic fitness parameters and higher waist circumference, insulin level and HOMA-IR in comparison with the medium and high PA groups, as well as a higher body mass index (BMI) compared with the medium PA group. None of the strength and power parameters differed between the PA groups. Many significant relationships between PA in different life periods and cardiometabolic profile (negative with body mass, BMI, waist circumference, insulin, HOMA-IR, triglycerides and positive with HDL-cholesterol, Augmentation Index and aerobic fitness data) were found but not with strength and power measures.
Conclusion: Higher lifetime endurance PA is related to a better cardiometabolic profile in older physically active males but does not affect muscle strength and power. These findings emphasize that despite cardiometabolic benefits, endurance PA alone may not be sufficient to be prescribed for muscle strength and power preservation in aging.
Keywords: cardiovascular, exercise, muscle, metabolism
Introduction
In the 1970s, endurance physical activity (PA) was considered as a synonym of health training. Some even believed that very intensive workouts, such as marathon running, guaranteed protection against atherosclerosis, coronary heart disease and myocardial infarction.1 Although this was not confirmed in later observations,2,3 endurance training remains the primary mode of exercise for health even today.
With further development of exercise science, other training modes have been included in exercise recommendations, especially for different groups of patients and for older individuals.4 Currently, endurance, strength, stretching, balance and coordination exercises have been included in recent recommendations.4,5 In rapidly growing older populations, there is evidence indicating an association between muscle strength and mortality.6,7 Furthermore, research shows that muscle power has been connected with better preservation of function as compared to muscle strength.8–10 Therefore, power training has been proposed to optimally improve neuromuscular function in advanced age.11
Nevertheless, the popularity of long-distance running, including different competitions, and common trust in the benefits of running makes many subjects restrict their exercise habits to running. With aging societies, there is a question about whether this mode of exercise confer protection against the dangers of declining functionality with advancing age. Available literature provides inconsistent results. Growing evidence indicates that resistance training is effective in maintaining muscle function with aging, whereas endurance PA is not, as it does not specifically address the preservation of muscle strength, contraction velocity and power.12–14 However, a variety of mechanisms, such as improved mitochondrial function, enhanced motor unit function, and reduced fat infiltration into muscle, explain the role of endurance training in the preservation of skeletal muscle mass and function with age.15–18 Some existing studies reveal that aerobic physical activity is related to physical function, muscle strength, flexibility and physical fitness in older adults.16,19
Our center provides a unique possibility of monitoring exercising subjects for several decades. Therefore, the aim of this study was to compare the effects of lifetime endurance physical activity (PA) on cardiometabolic profile and muscle function in middle aged and older men.
Materials and Methods
Study Group
The study was conducted in male volunteers, who were the patients of the Healthy Men Clinic and the Department of Preventive Medicine, Medical University of Lodz (Poland), mostly for over 30 years. The initial group of 577 male volunteers participated in baseline structured health check-up in 1985–1990. Next, the respondents were invited to take part in regular control examinations. Subjects reporting endurance PA at minimum once a week for most study periods were selected for this study. The complete recruitment procedure and other methods were described previously in our papers.20,21 Subjects included in this study participated in the full panel of diagnostic procedures during at least five examinations between baseline 1985–90 and the final examination in 2018. The observation period was 28–33 years. The participants from the previous examinations were invited to take part in the final study. The inclusion criteria comprised: regular attendance in the control examinations, a signed informed consent form, participation in endurance physical activity at least once a week, and no contraindications to undergo the full panel of tests. Selected men were involved in purely endurance activities, those involved in resistance training were excluded from this study. Of the 75 male participants who provided informed consent, 59 met the inclusion criteria. As the PA level may vary within individuals across time, we analyzed PA levels throughout the whole observation. Most subjects were characterized by performing non-competitive endurance sports activities like jogging, cycling or swimming, which rely on aerobic energy production. Therefore, the final study group was composed of 59 older and middle-aged men aged from 44 to 87 years (mean age 66.7 ± 8.8 years). Three participants were under the age of 50.
All subjects participated in anthropometric and biochemical measurements, PA questionnaires, the graded submaximal exercise test and muscle strength and power examinations.
The study was approved by the Bioethics Committee of the Medical University of Łódź (RNN/174/18/KE) and complies with the Helsinki Declaration and Good Clinical Practice Guidelines.
Anthropometric, Biochemical and Arterial Stiffness Measurements
Body weight was measured to the nearest 0.1 kg in light indoor clothes and without shoes on a calibrated scale (Radwag, model C315.100/200.OW-3). Height was measured to the nearest 0.5 cm. Waist circumference was measured to the nearest 0.5 cm in the standing position with a tape measure at the midpoint of the distance between the lowest rib and the iliac crest. Body mass index (BMI) was calculated as weight (kilograms) divided by the square of height (meters).
Fasting blood samples were drawn from the antecubital vein. To determine serum total cholesterol, triglycerides (TG), and glucose, enzymatic methods were used (COBAS INTEGRA 400 Plus, Roche). High-density lipoprotein cholesterol (HDL-C) was measured by the precipitation method while low-density lipoprotein cholesterol (LDL-C) was estimated using the Friedewald formula. Glucose was given in mmol/l. Insulin was measured by the electrochemiluminescence method and given in mU/l.
The Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was used to assess participants’ insulin resistance. The HOMA-IR index was calculated using fasting glucose and fasting insulin levels using the following formula: HOMA-IR = (fasting glucose (mmol/l))*(fasting insulin (mU/l))/22.5.22
Augmentation Index (AI) was provided by the Endopat device and it was given in percentages (%). AI measures the arterial stiffness, reporting the difference between first (P1) and second (P2) peaks of the arterial waveform according to the equation: (AI (%)=(P2-P1)/P1).23
Physical Activity Level
Historical PA data were verified based on PA levels reported during past examinations. It was assessed for each subject according to Kriska et al24 This is a validated tool designed to retrospectively evaluate PA levels throughout different periods of life. The questionnaire is divided into three main components: the Leisure Physical Activity section, the Occupational Activity section, and the Inactivity and Sedentary Behavior section. The participants were asked to recall the type of physical activities in the following life periods: 12–34, 35–49, over 50 years old period, the last 5 years, the last 10 years and the whole period from 12th year of life to the day of examination. These activities were summed up according to their duration, frequency, and intensity. All results were summed up according to hours per year, weeks of activity during the month, months of activity during the year, and years of activity during the examined period. The number of hours obtained during the examined period was divided by the number of years. Finally, the results of historical PA are expressed as hours per year and the weighted MET-hours per year (MET·hour·year −1). For comparing cardiometabolic parameters in different PA groups, PA level in last 10 years was categorized and 3 groups the best matched with the number of participants were created: low (PA level <1600 MET·hour·year−1), medium (1600 MET·hour·year−1 ≤ PA level >2250 MET·hour·year−1) and high (PA level >2250 MET·hour·year−1).
Physical Fitness
Resting electrocardiographic examination was performed using a FARUM E60 model. The graded submaximal exercise test was performed on a Monark type 818E (Stockholm, Sweden) with continuous VO2 uptake and 12-lead electrocardiographic monitoring using Cardiovit CS-200 Ergo Spiro system (Schiller, Switzerland). The exercise test protocol included an initial workload of 60 Wat (W) and an increase of the workload by 30 W every 3 minutes to achieve at least 85% of maximal age-predicted heart rate (220-age). After completing the exercise phase, participants were monitored for five minutes or longer if necessary. A cooldown phase consisted of two minutes of unloaded pedaling and then three to five minutes of rest. Blood pressure was measured at rest, within the last 30 seconds of each stage of the exercise test, and every two minutes during the recovery phase. The two aerobic fitness measures were calculated: peak oxygen uptake (VO2peak) and physical working capacity at 85% of the maximal heart rate (PWC85%HRmax). VO2peak was defined as the highest value of VO2 achieved during the exercise test. VO2peak was expressed in absolute values (VO2peak) and relative to body mass (VO2peak∙kg−1)]. Heart rate (continuous ECG tracing) was regressed against the three last workloads. The resultant linear regression equation was used to calculate the second aerobic capacity index, ie, PWC85%HRmax PWC85%HRmax was calculated by interpolating the workload-heart rate regression line at the point of 85% of the maximal age-predicted heart rate.25 This methodology, even with a lower (PWC75%HRmax) exercise test intensity level, has been proposed as a valuable measure of aerobic power for epidemiological studies. PWC85%HRmax was expressed in absolute values [PWC (W)] and relative to body mass [PWC∙kg−1 (W∙kg−1)]. This procedure ensures the use of the same units (W) for aerobic and anaerobic power assessment.
Muscle Strength
Three different methods were used to assess muscle strength of the participants
1. A handgrip test using a hydraulic hand dynamometer (Saehan, Korea) was used to assess the muscle strength of the upper extremities.26 Participants, standing upright with their arms at their sides without touching the body, were instructed to squeeze the dynamometer with maximal force. The test was performed in three trials for each hand, with a 20–30-second pause between trials to avoid muscle fatigue. The highest value was used for analysis. Results were recorded to the nearest kilogram.
2. Muscle strength of lower extremities was determined using Keiser pneumatic resistance training equipment fitted with A300 electronics (Keiser Sports Health Equipment, Fresno, CA), as previously described.27 One-repetition maximum (1RM) for bilateral leg press and leg extension was assessed, with each leg evaluated separately. For the leg press assessment, the seat position was adjusted to achieve a 90° angle between the thigh and the lower leg at the knee joint. Participants were instructed to fully extend both legs while keeping their arms crossed over the chest. For the leg extension assessment, participants were seated upright with their arms crossed over the chest and instructed to extend the knee (right and left legs tested separately) as forcefully as possible. The 1RM was determined by progressively increasing the resistance to the maximum load that allowed completion of the full range of motion.
3. The maximal voluntary force of 11 muscle groups of both extremities was measured with a handheld dynamometer (Microfet 2, Hogan Health Industries, USA): wrist, elbow extension, elbow flexion, shoulder extension, shoulder flexion, shoulder abduction, hip flexion, hip abduction, ankle dorsiflexion, knee extension, and knee flexion.28 All tests were performed according to the instruction manual of the manufacturer. Each movement was tested twice, and the average scores were included in the analysis. Mean strength of particular muscle groups was the result of measurements and was given in kilograms.
Muscle Power
Two methods were used to assess the muscle power of the participants.
1. Keiser pneumatic resistance training equipment fitted with A300 electronics (Keiser Sports Health Equipment, Fresno, CA). Leg press and leg extension power were assessed at 40% and 70% of 1RM.27 In the leg press trial, the highest power of both legs was recorded, while for the leg extension, the highest power of each leg, separately, was taken for further analyses.
2. Friction-loaded cycle ergometer (Monark type 818E Stockholm, Sweden) equipped with a strain gauge (KMM20 type, 200N, WObit, Poznan, Poland) and an incremental encoder (Rotapuls141-H-200ZCU46L2 type, 200 pts/turn, Lika Electronic, Carre, Italy) for measurement of the friction force applied by the tension of the belt that surrounded the flywheel and the flywheel displacement, respectively.
Maximal short-term power (Pmax) and corresponding optimal movement velocity (υopt) which is defined as velocity at which the power reaches its maximum value were calculated from a third-order polynomial function. Pmax was expressed as absolute values [Pmax (W)] and relative to body mass [Pmax/kg (W∙kg−1)]. υopt was expressed in the number of rotations per minute (rpm).29
Statistical Analysis
All analyses were performed with Statistica version 13 CSS software (StatSoft, Krakow, Poland). Data were verified for normality of distribution and equality of variance. Numeric variables were presented as mean ± standard deviation (SD) for data with normal distribution or median (quartile) for data without normal distribution. Correlations between quantitative variables were tested with the Spearman rank correlation test or Pearson correlation. To compare cardiometabolic indices in three historical PA groups, the One-way Analysis of Variance (ANOVA) with LSD post-hoc test or Kruskal–Wallis analysis of variance by ranks and Dunn post-hoc test were used in variables with and without normal distribution, respectively. To examine whether the strength of the association between physical activity and aerobic power differed from that between physical activity and anaerobic power, Steiger’s test for comparing dependent correlations was conducted. Effect sizes based on Cohen’s d were reported. An effect size of 0.2 to < 0.5 and ≥ 0.5 to < 0.8 has been suggested to represent a small and medium effect, respectively, while an effect size ≥ 0.8 represents a large effect. The limit of significance was assumed as a p-value of 0.05 or less for all analyses.
Results
The age and historical PA data are presented in Table 1. The age of the three compared groups was not statistically different. PA differed between the groups by design.
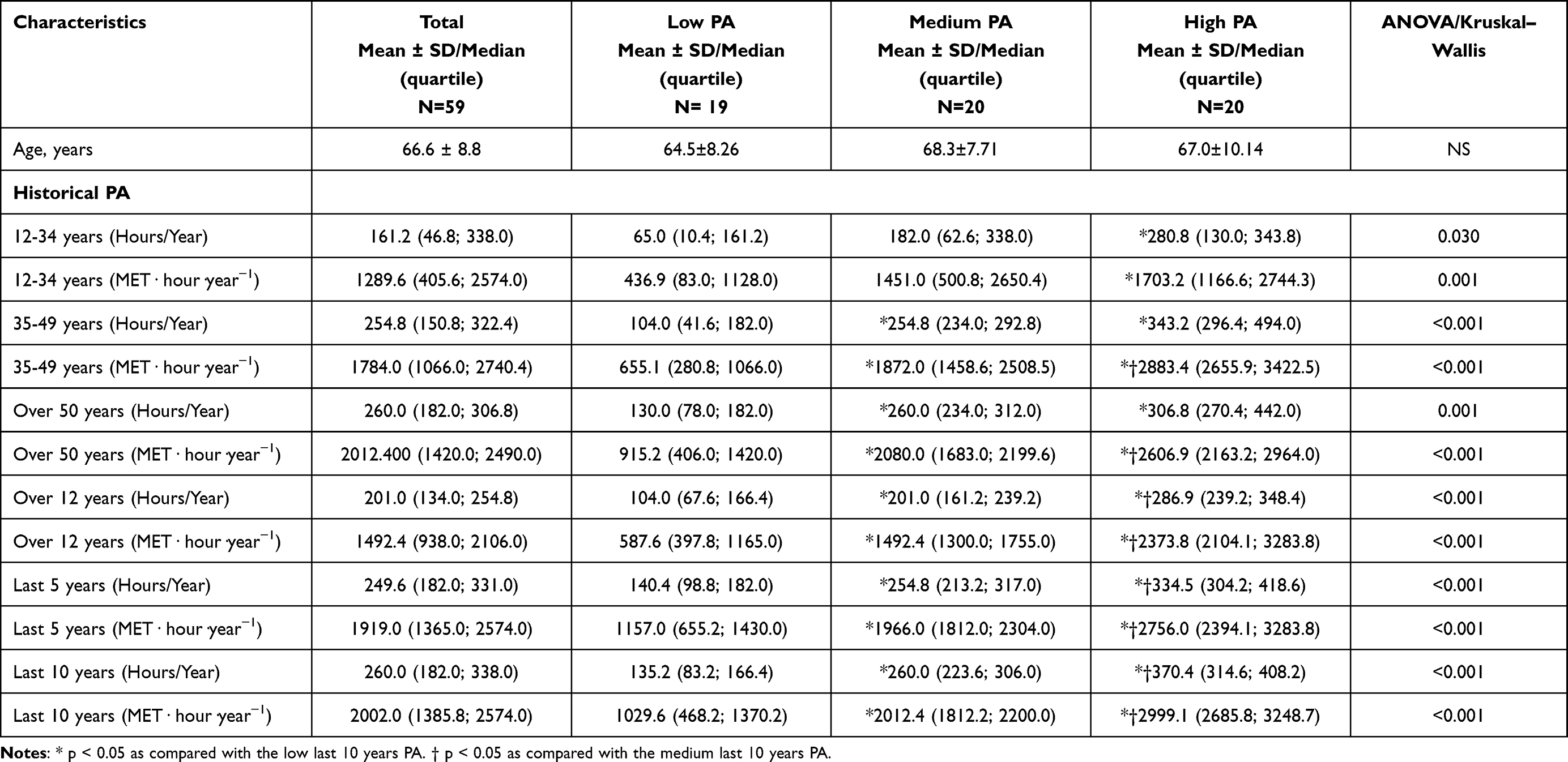 |
Table 1 Age and Historical PA Data of the Whole Group and Divided Into Low, Medium and High Last 10 years PA |
Table 2 shows anthropometric indices, cardiometabolic profile and exercise test results. Participants in the low PA level group presented significantly higher insulin level, HOMA-IR, and waist circumference in comparison with the medium and high PA level groups. BMI was significantly higher in the low PA group compared to the medium PA level group.
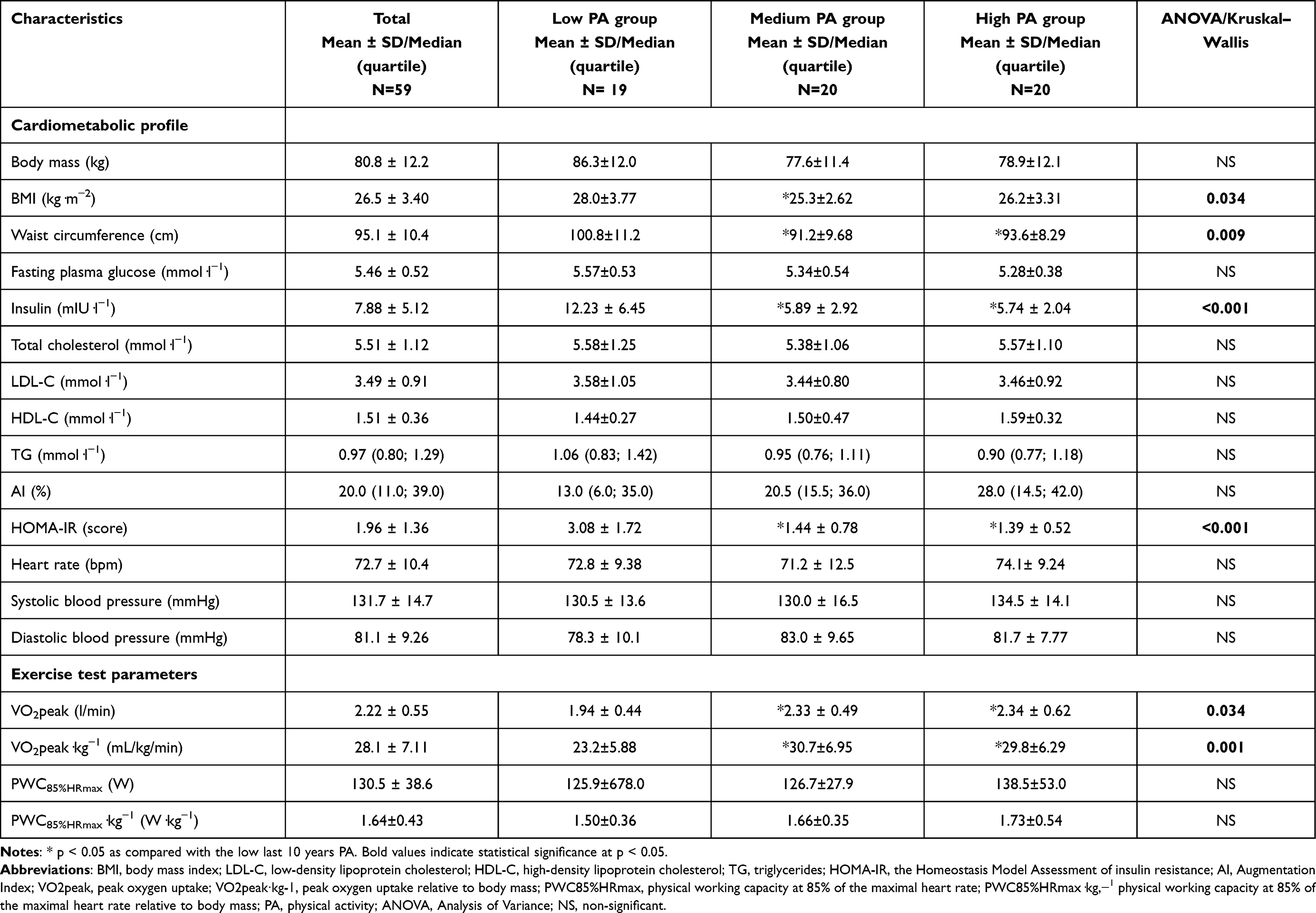 |
Table 2 Cardiometabolic Parameters of the Whole Group and Divided Into Low, Medium and High Last 10 years PA |
The VO2peak of the low PA level group was significantly lower in comparison with that of the medium and high PA level groups. PWC and PWC∙kg−1 showed a tendency to increase with higher PA levels.
Supplementary Figure 1 presents BMI, HOMA-IR, insulin, and aerobic power in participants characterized with low, medium and high historical PA in the last 10 years.
None of strength and power parameters differed between the groups with low, medium and high PA levels (Supplementary Table 1).
Table 3 shows the relationships between anthropometric indices, cardiometabolic profile, aerobic exercise test data, and historical PA in the whole studied group. Many significant relationships were found with PA in different life periods. Anthropometric indices (body mass, BMI, and waist circumference) were negatively related to three of the historical PA periods. Insulin levels as well as HOMA-IR were negatively correlated with the level of PA in all studied periods. HDL levels were positively related to most PA periods (except for the 12–34-year period). Similar relationships were observed for AI. Negative correlation was significant for TG level and one PA period (over 12 years). Aerobic exercise test data were also generally positively related to most historical PA periods.
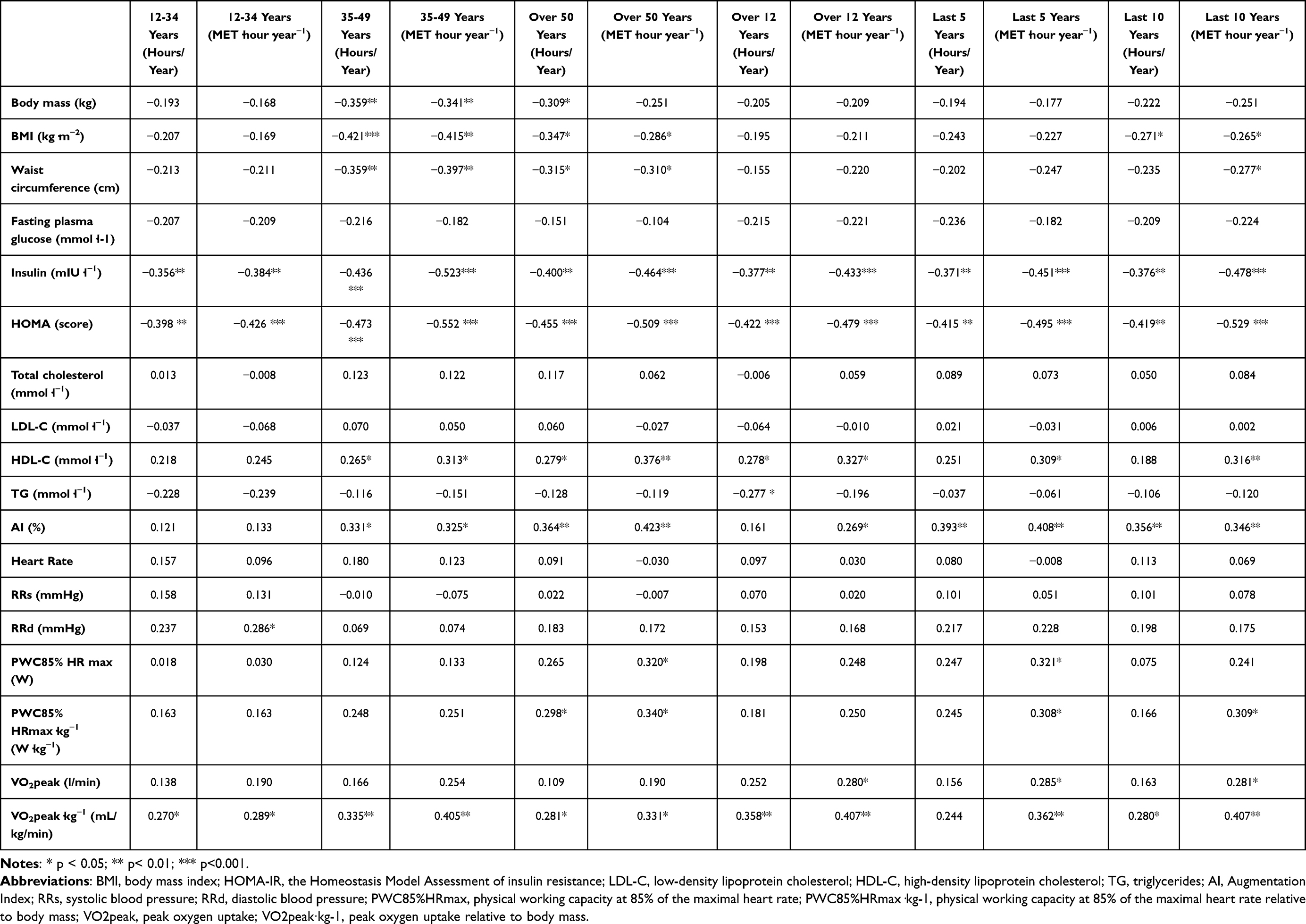 |
Table 3 Relationships Between Anthropometric, Cardiometabolic, Aerobic Exercise Test Data and Historical PA in the Whole Group |
In contrast to cardiometabolic profile data, muscle strength and power parameters were not related to historical PA. Moreover, from a few significant relationships, those with negative signs were observed. Relationships between muscle strength and power parameters and historical PA in the whole studied group are presented in Supplementary Table 2. Despite statistically significant relationships being found, all reported correlation coefficients were relatively low (all were characterized by r < 0.5) which may be related to the small final sample size of the study. Effect sizes were small.
The relationships between aerobic (PWC85%HRmax) and anaerobic (Pmax) power expressed relative to body mass with the last 10 years of PA level are presented in Supplementary Figure 2. A positive correlation between aerobic power and PA was found, while anaerobic power was not related to PA.
Steiger’s test for comparing two dependent correlations indicated the correlation between physical activity and aerobic power (r = 0.309) was significantly stronger than the correlation between physical activity and anaerobic power (r = 0.03); t(56) = −2.07, p = 0.043.
Discussion
Among dozens of results of PA, benefits for cardiovascular risk factors and cardiometabolic profile are among the most important. The effects of PA for physical performance should also include maintaining physical fitness, muscle strength and power, which becomes crucial while getting older. Our study results showed that a higher lifetime endurance PA level in adult men was connected with better cardiometabolic profile in old age; however we did not find long-term benefits for muscle strength and power.
In our study, BMI and waist circumference were negatively correlated with historical PA in the age group 35–49 years old, during the over 50 years old period and the last 10 years period. These results indicate the protective role of longitudinal PA in avoiding becoming overweight/obese. Literature confirms the negative directions of the relationships between longitudinal PA and weight gain, waist circumference and prevalence of obesity30,31 Available literature shows that PA has a positive impact on insulin sensitivity.32 PA may significantly lower insulin levels, and high-intensity physical activity still has additional potential benefits for insulin levels.33 In our study, insulin level and HOMA-IR were negatively correlated with PA level in all studied periods while glucose level was not. It shows that even in a physically active group a higher level of PA is related to better insulin sensitivity. Further reduction of glucose level is obviously not desirable in subjects with proper glycemia. However, our results may also emphasize the importance of measuring insulin rather than relying solely on glucose measurements in routine blood analyses. Previous studies showed that aerobic exercises significantly reduce TC, triglycerides, and LDL cholesterol, while increase HDL cholesterol in the older population.34 Our study did not reveal differences in the complete lipid profile between the three PA groups, but the level of HDL cholesterol was significantly related to PA in most of the analyzed periods. Triglycerides were inversely related to the PA period over 12 years of age. Nevertheless, the observed correlations were generally low.
The mechanisms of the relationships between PA and cardiovascular diseases (CVD) may be explained with the beneficial effects of PA on exercise capacity, endothelial function, and influence on biomarkers of atherosclerosis, including inflammatory markers and adipokines.35 The results of the British Regional Heart Study showed that a higher PA level from midlife to old age was associated with a lower risk of all-cause mortality, cardiovascular mortality, coronary heart disease, and all cardiovascular events.36 A dose–response relationship was found. In the population-based cohort study, older participants who maintained moderate PA levels in a ten-year follow-up were at a lower risk of all-cause mortality compared with those who presented low PA levels throughout the whole follow-up period.37 The results of the present study show positive relationships between aerobic exercise capacity and historical PA in a homogenous group of persistently active men. Significant differences were observed between low and medium as well as between low and high PA levels. These results underline the role of a higher level of lifetime PA in maintaining exercise capacity and aerobic power in older age.
As the relationship between long-life PA for cardiometabolic health in older age was found in our study, and the effect of PA for cardiometabolic profile and mortality was observed in some prospective studies, the interesting question is whether all analyzed periods of PA play a similar role. According to the British results, the most important factor for the protection against mortality was the most recent PA. Participants characterized with increasing PA over the 20-year follow-up (inactive at baseline and active at the final examination) exhibited a reduced mortality risk, similar to that of persistently active individuals.36 Other study participants who presented a decline in PA level were characterized with similar mortality to those who maintained a low PA level.37 In our study, the number of significant correlations between cardiovascular parameters and specific historical PA periods was lowest for the 12–34 years period (4 variables) and highest for participants over 50 years old (10 variables) and for the last 10 years (9 variables). However, it is worth emphasizing, as confirmed by other authors, that being active in earlier life periods is crucial for the continuation of PA in subsequent years.36
In contrast to the cardiometabolic profile, our results did not reveal relationships between lifetime endurance PA and muscle strength and power in later life. As numerous studies show that muscle strength wasting may be decelerated by regular PA, the role of strength training is indisputable and well documented.12–14 The available evidence on endurance training is inconclusive. While most studies report no significant improvements in muscle strength and power, some suggest a potential beneficial effect. According to the study on the skeletal muscle phenotype, aerobic PA partially protects from the effects of ageing on muscle phenotype, mitochondrial content, and lipid accumulation.18 Distefano et al16 showed that older subjects performing regular aerobic exercise presented similar mitochondrial function to young, physically active individuals. Additionally, the time required to complete the physical tests was significantly longer in sedentary subjects. Another study revealed that higher level of lifelong aerobic PA was correlated with more favourable fitness outcomes (higher lower and upper limb strength, lower body flexibility and aerobic capacity) in older women.19
Although potential positive effects of endurance training on muscle strength have been reported,15 many studies have demonstrated a lack of effect compared with resistance training, as endurance training does not specifically target improvements in muscle mass, muscle strength, or agility. In a Norwegian study, endurance-trained master athletes were characterized by a lower proportion of type II fibers in comparison with strength-trained older master athletes, similarly to recreationally active older adults. Compared to non-active as well endurance-trained groups, strength-trained athletes were characterized with less prevalent myofiber grouping and lower fiber atrophy, exhibiting a signs of myocellular denervation.12 In another study, endurance master athletes were characterized with longer contraction time (in comparison with power master athletes and nonathletes) suggesting that regular endurance sport activity exacerbates skeletal muscle slowing in ageing.13 Endurance athletes presented higher VO2peak, as well as the peak rate of fat oxidation during steady-state cycling in comparison with power athletes, while the anaerobic power was higher in power than endurance athletes.38 In summary, while showing the benefits of regular PA, these studies also point to the specificity of different training modes on muscle morphology and functioning.
Some authors emphasized that aerobic training combined with resistance exercises is an effective way to improve endurance and muscle strength.39,40 Positive long-term effects of this type of training on muscle strength and power were observed after 12 weeks in healthy middle-aged and older participants aged between 50 and 73 years.40 Better long-term effects for muscle strength have been obtained while strength exercises were performed before aerobic training.39 Moderate-to-high intensity aerobic exercise in young and middle-aged trained male individuals affected muscle strength decline, while aerobic training with low intensity did not. Moreover, aerobic training that lasts over 30 minutes resulted in a large acute decline in muscle strength, and ≤ 30 min of aerobic training was connected with a moderate decline. These results indicate the key issues that are connected with the intensity and length of aerobic training before strength exercises.41
There is evidence indicating an association of muscle strength and mortality, as a recent cohort study of older women showed that higher skeletal muscle strength was associated with significantly lower all-cause mortality.6 Other studies show that muscle power is a superior predictor of functional performance and mortality than muscle strength.8,9 In a large prospective study, relative muscle power was found as a stronger predictor of mortality than relative muscle strength in middle-aged and older men and women.10 Therefore, power training has been proposed to optimally improve neuromuscular function in advanced age.11,42,43
Previous studies showed that age-associated decline in anaerobic power is steeper than that of aerobic power and habitual PA alleviates an aerobic but not anaerobic power decline in older adults.44–46 Our results extend the findings of previous studies. Out of many different methods used and a great number of analyzed parameters of muscle strength and power, the results of the present study did not show relationships between lifetime habitual endurance PA level and muscle strength and power in older age.
Some limitations of this study should be acknowledged. Firstly, the relatively small sample size may limit the strength and generalizability of the findings. Secondly, the lack of a control group makes it impossible to compare active participants with their inactive peers. Thirdly, PA data were collected using a retrospective questionnaire rather than direct measurement methods, what may introduce a risk of recall bias, particularly for early life periods. Some engagement in other types of physical activity, such as resistance workouts, cannot be undoubtedly excluded. Moreover, due to the exclusion of participants with severe conditions at various stages of the study, we were unable to assess the prevalence of cardiovascular incidents, chronic conditions and functional outcomes in more and less active groups. The participants were all male and the majority had been physically active for most of their lives, making the group relatively homogeneous. However, this homogeneity enhances the value of our study – participants were carefully selected for each examination stage, and the analysis focused on physically active individuals. The long follow-up period and the comprehensive assessment of PA and physiological outcomes allowed us to investigate whether lifetime endurance PA provides benefits for cardiometabolic health, muscle strength, and muscle power.
Conclusions
In summary, our study confirms that lifelong endurance training is important for maintaining a healthy cardiometabolic profile in older age. Moreover, physical activity provide additional long-term benefits. However, despite cardiometabolic benefits, lifelong endurance activity does not significantly impact muscle strength and power. These findings may be valuable for practitioners when prescribing endurance training to improve overall health, particularly cardiometabolic health. At the same time, they highlight that endurance training alone is not sufficient to preserve muscle strength and power in older adults. Further longitudinal studies are needed to determine the amount of strength and power training that should be incorporated into endurance exercise programs to support muscle strength and power in later life.
Abbreviations
1RM R, one repetition maximum, right leg; 1RM L, one repetition maximum, left leg; AI, Augmentation Index; ANOVA, Analysis of Variance; BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, Homeostasis Model Assessment of Insulin Resistance; LDL-C, low-density lipoprotein cholesterol; MET, Metabolic Equivalent of Task; NS, non-significant; p, statistical significance; P40% LE R, muscle power of low force/high velocity (40%), leg extension, right leg; P70% LE R, muscle power of high force/low velocity (70%), leg extension, right leg; P40% LE L, muscle power of low force/high velocity (40%), leg extension, left leg; P70% LE L, muscle power of high force/low velocity (70%), leg extension, left leg; P40% LP, muscle power of low force/high velocity (40%), leg press; P70% LP, muscle power of high force/low velocity (70%), leg press; PA, physical activity; Pmax, maximal short-term power; Pmax·kg-1, maximal short-term power relative to body mass; PWC85%HRmax, physical working capacity at 85% of the maximal heart rate; PWC85%HRmax·kg-1, physical working capacity at 85% of the maximal heart rate relative to body mass; rpm, number of rotations per minute; RRs, systolic blood pressure; RRd, diastolic blood pressure; SD, standard deviation; TG, triglycerides; W, watt; VO2peak, peak oxygen uptake; VO2peak∙kg−1, peak oxygen uptake relative to body mass; υopt, optimal movement velocity corresponding to Pmax.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Bioethics Committee of the Medical University of Łódź (RNN/174/18/KE) and complies with the Helsinki Declaration and Good Clinical Practice Guidelines.
Acknowledgments
We appreciate the valuable assistance of Mrs Ewa Rębowska in laboratory measurements.
Funding
The study was supported by the National Science Centre (the scientific grant: NN 404 258940) and by grant 503/6-077-01/503-61-001 from the Medical University of Lodz.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bassler TJ. Marathon running and immunity to heart disease. Phys Sportsmed. 1975;3(4):77–13. doi:10.1080/00913847.1975.11948178
2. Noakes TD, Opie LH, Rose AG. Marathon running and immunity to coronary heart disease: fact versus fiction. Clin Sports Med. 1984;3(2):527–543. doi:10.1016/S0278-5919(20)31342-9
3. Noakes TD. Heart disease in marathon runners: a review. Med Sci Sports Exerc. 1987;19(3):187–194. doi:10.1249/00005768-198706000-00001
4. World Health Organization. WHO guidelines on physical activity and sedentary behaviour: at a glance. World Health Organization; 2020.
5. Izquierdo M, Merchant RA, Morley JE, et al. International exercise recommendations in older adults (ICFSR): expert consensus guidelines. J Nutr Health Aging. 2021;25(7):824–853. doi:10.1007/s12603-021-1665-8
6. LaMonte MJ, Hyde ET, Nguyen S, et al. Muscular strength and mortality in women aged 63 to 99 years. JAMA Network Open. 2026;9(2):e2559367–e2559367. doi:10.1001/jamanetworkopen.2025.59367
7. Andersen LL, López-Bueno R, Núñez-Cortés R, Cadore EL, Polo-López A, Calatayud J. Association of muscle strength with all-cause mortality in the oldest old: prospective cohort study from 28 countries. J Cachexia, Sarcopenia Muscle. 2024;15(6):2756–2764. doi:10.1002/jcsm.13619
8. Reid KF, Fielding RA. Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc Sport Sci Rev. 2012;40(1):4–12. doi:10.1097/JES.0b013e31823b5f13
9. Byrne C, Faure C, Keene DJ, Lamb SE. Ageing, muscle power and physical function: a systematic review and implications for pragmatic training interventions. Sports Med. 2016;46(9):1311–1332. doi:10.1007/s40279-016-0489-x
10. Araújo CGS, Kunutsor SK, Eijsvogels TMH, et al. Muscle power versus strength as a predictor of mortality in middle-aged and older men and women. Mayo Clin Proc. 2025;28(25):S0025–6196.
11. Radaelli R, Trajano GS, Freitas SR, Izquierdo M, Cadore EL, Pinto RS. Power training prescription in older individuals: is it safe and effective to promote neuromuscular functional improvements? Sports Med. 2022;53(3):569–576. doi:10.1007/s40279-022-01758-0
12. Tøien T, Nielsen JL, Berg OK, et al. The impact of life-long strength versus endurance training on muscle fiber morphology and phenotype composition in older men. J Appl Physiol. 2023;135(6):1360–1371. doi:10.1152/japplphysiol.00208.2023
13. Šimunic B, Pišot R, Rittweger J, Degens H. Age-related slowing of contractile properties differs between power, endurance, and nonathletes: a tensiomyographic assessment. J Gerontol a Biol Sci Med Sci. 2018;73(12):1602–1608. doi:10.1093/gerona/gly069
14. Mastalerz A, Hooshmand-Moghadam B, Moazamigoudarzi S, et al. Changes in muscle quality and biomarkers of neuromuscular junctions and muscle protein turnover following 12 weeks of resistance training in older men. Biol Sport. 2024;41(4):285–292. doi:10.5114/biolsport.2024.141064
15. Laurin JL, Reid JJ, Lawrence MM, Miller BF. Long-term aerobic exercise preserves muscle mass and function with age. Curr Opin Physiol. 2019;10:70–74. doi:10.1016/j.cophys.2019.04.019
16. Distefano G, Standley RA, Zhang X, et al. Physical activity unveils the relationship between mitochondrial energetics, muscle quality, and physical function in older adults. J Cachexia, Sarcopenia Muscle. 2018;9(2):279–294. doi:10.1002/jcsm.12272
17. Dimmick HL, Miller JD, Sterczala AJ, Trevino MA, Herda TJ. Vastus lateralis muscle tissue composition and motor unit properties in chronically endurance-trained versus sedentary women. Eur J Appl Physiol Occup Physiol. 2018;118(9):1789–1800. doi:10.1007/s00421-018-3909-9
18. St-Jean Pelletier F, Pion CH, Leduc-Gaudet J-P, et al. The impact of ageing, physical activity, and pre-frailty on skeletal muscle phenotype, mitochondrial content, and intramyocellular lipids in men. J Cachexia, Sarcopenia Muscle. 2017;8(2):213–228. doi:10.1002/jcsm.12139
19. Kaczorowska A, Kołodziej M, Sebastjan A, Ignasiak Z. Association between lifelong physical activity, physical fitness, and quality of life in older adults in Poland. Sci Rep. 2026;16(1):5934. doi:10.1038/s41598-026-36742-5
20. Kwaśniewska M, Jegier A, Kostka T, et al. Long-term effect of different physical activity levels on subclinical atherosclerosis in middle-aged men: a 25-year prospective study. PLoS One. 2014;9(1):e85209. doi:10.1371/journal.pone.0085209
21. Drygas W, Kostka T, Jegier A, Kunski H. Long-term effects of different physical activity levels on coronary heart disease risk factors in middle-aged men. Int J Sports Med. 2000;21(4):235–241. doi:10.1055/s-2000-309
22. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. doi:10.1007/BF00280883
23. Munir S, Guilcher A, Kamalesh T, et al. Peripheral augmentation index defines the relationship between central and peripheral pulse pressure. Hypertension. 2008;51(1):112–118. doi:10.1161/HYPERTENSIONAHA.107.096016
24. Kriska AM, Caspersen CJ. Historical leisure activity questionnaire: a collection of physical activity questionnaires for health-related research. Med Sci Sports Exerc. 1997;29(Supplement):S43–S45. doi:10.1097/00005768-199706001-00011
25. Gorem CJ, Booth ML, Bauman A, Owen N. Utility of pwc75% as an estimate of aerobic power in epidemiological and population-based studies. Med Sci Sports Exerc. 1999;31(2):348–351. doi:10.1097/00005768-199902000-00020
26. Rantanen T, Guralnik JM, Foley D, et al. Midlife hand grip strength as a predictor of old age disability. JAMA. 1999;281(6):558–560. doi:10.1001/jama.281.6.558
27. Fife E, Kostka J, Kroc Ł, et al. Relationship of muscle function to circulating myostatin, follistatin and GDF11 in older women and men. BMC Geriatr. 2018;18(1):200. doi:10.1186/s12877-018-0888-y
28. Nowicka M, Górska M, Edyko K, et al. Association of physical performance, muscle strength and body composition with self-assessed quality of life in hemodialyzed patients: a cross-sectional study. J Clin Med. 2022;11(9):2283. doi:10.3390/jcm11092283
29. Kostka T, Kostka J. Feasibility and reliability of quadriceps muscle power and optimal movement velocity measurements in different populations of subjects. Biology. 2024;13(3):140. doi:10.3390/biology13030140
30. Fuentes GC, Bawaked RA, Martínez González MA, et al. Association of physical activity with body mass index, waist circumference and incidence of obesity in older adults. Eur J Public Health. 2018;28(5):944–950. doi:10.1093/eurpub/cky030
31. Waller K, Kaprio J, Kujala UM. Associations between long-term physical activity, waist circumference and weight gain: a 30-year longitudinal twin study. Int J Obes Lond. 2008;32(2):353–361. doi:10.1038/sj.ijo.0803692
32. Małkowska P. Positive effects of physical activity on insulin signaling. Curr Issues Mol Biol. 2024;46(6):5467–5487. doi:10.3390/cimb46060327
33. Lin Y, Fan R, Hao Z, et al. The association between physical activity and insulin level under different levels of lipid indices and serum uric acid. Front Physiol. 2022;13:809669. doi:10.3389/fphys.2022.809669
34. Yun H, Su W, Zhao H, et al. Effects of different exercise modalities on lipid profile in the elderly population: a meta-analysis. Medicine. 2023;102(29):e33854. doi:10.1097/MD.0000000000033854
35. Palmefors H, DuttaRoy S, Rundqvist B, Borjesson M. The effect of physical activity or exercise on key biomarkers in atherosclerosis–a systematic review. Atherosclerosis. 2014;235(1):150–161. doi:10.1016/j.atherosclerosis.2014.04.026
36. Aggio D, Papachristou E, Papacosta O, et al. Trajectories of physical activity from midlife to old age and associations with subsequent cardiovascular disease and all-cause mortality. J Epidemiol Community Health. 2020;74(2):130–136. doi:10.1136/jech-2019-212706
37. Hassan L, Huhndorf P, Mikolajczyk R, Kluttig A. Physical activity trajectories at older age and all-cause mortality: a cohort study. PLoS One. 2023;18(1):e0280878. doi:10.1371/journal.pone.0280878
38. Bagley L, McPhee JS, Ganse B, et al. Similar relative decline in aerobic and anaerobic power with age in endurance and power master athletes of both sexes. Scand J Med Sci Sports. 2019;29(6):791–799. doi:10.1111/sms.13404
39. Murlasits Z, Kneffel Z, Thalib L. The physiological effects of concurrent strength and endurance training sequence: a systematic review and meta-analysis. J Sports Sci. 2018;36(11):1212–1219. doi:10.1080/02640414.2017.1364405
40. Markov A, Hauser L, Chaabene H. Effects of concurrent strength and endurance training on measures of physical fitness in healthy middle-aged and older adults: a systematic review with meta-analysis. Sports Med. 2023;53(2):437–455. doi:10.1007/s40279-022-01764-2
41. Markov A, Chaabene H, Hauser L, et al. Acute effects of aerobic exercise on muscle strength and power in trained male individuals: a systematic review with meta-analysis. Sports Med. 2022;52(6):1385–1398. doi:10.1007/s40279-021-01615-6
42. El Hadouchi M, Kiers H, de Vries R, Veenhof C, van Dieën J. Effectiveness of power training compared to strength training in older adults: a systematic review and meta-analysis. Eur Rev Aging Phys Act. 2022;19(1):18. doi:10.1186/s11556-022-00297-x
43. El Hadouchi M, Kiers H, Veenhof C, van Dieën J. The impact of power training on muscle power, physical performance, and physical functioning in older adults: a descriptive case series. Clin Interv Aging. 2025;20:849–857. doi:10.2147/CIA.S511954
44. Kostka T, Drygas W, Jegier A, Zaniewicz D. Aerobic and anaerobic power in relation to age and physical activity in 354 men aged 20 – 88 years. Int J Sports Med. 2009;30(03):225–230. doi:10.1055/s-0028-1104591
45. Gent DN, Norton K. Aging has greater impact on anaerobic versus aerobic power in trained masters athletes. J Sports Sci. 2013;31(1):97–103. doi:10.1080/02640414.2012.721561
46. Luneau E, Rozand V, Millet GY. Are maximal power and maximal aerobic capacity in older and very old adults dependent on their level of physical activity? J Gerontol a Biol Sci Med Sci. 2025;80(7):glaf048. doi:10.1093/gerona/glaf048
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Microbial Champions: The Influence of Gut Microbiota on Athletic Performance via the Gut-Brain Axis

Xia W, Li X, Han R, Liu X
Open Access Journal of Sports Medicine 2024, 15:209-228
Published Date: 13 December 2024
Impact of Propranolol and Psychologically Informed Intervention on Pain Sensitivity: Secondary Analysis from the Biopsychosocial Influence on Shoulder Pain Preclinical Randomized Trial
Bishop MD, Simon CB, Huo Y, Wallace MR, Borsa PA, Fillingim RB, Staud R, Wu SS, George SZ
Journal of Pain Research 2025, 18:1837-1850
Published Date: 5 April 2025