Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Lifespan and Associated Factors of Peripheral Intravenous Cannula Among Hospitalized Children in Public Hospitals of the Gurage Zone, Ethiopia, 2021
Authors Mewahegn AA ![]() , Tadesse B, GebreEyesus FA
, Tadesse B, GebreEyesus FA ![]() , Tarekegn TT, Amlak BT, Emeria MS
, Tarekegn TT, Amlak BT, Emeria MS ![]() , Temere BC
, Temere BC ![]() , Terefe TF
, Terefe TF ![]() , Zewudie BT
, Zewudie BT ![]() , Geletie HA
, Geletie HA ![]() , Mengist ST
, Mengist ST ![]()
Received 29 November 2021
Accepted for publication 1 February 2022
Published 25 March 2022 Volume 2022:13 Pages 81—93
DOI https://doi.org/10.2147/PHMT.S351759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Agerie Aynalem Mewahegn, Betelhem Tadesse, Fisha Alebel GebreEyesus, Tadesse Tsehay Tarekegn, Baye Tsegaye Amlak, Mamo Solomon Emeria, Bogale Chekole Temere, Tamene Fetene Terefe, Bitew Tefera Zewudie, Haymanot Abebe Geletie, Shegaw Tesfe Mengist
Department of Nursing, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
Correspondence: Agerie Aynalem Mewahegn, Department of Nursing Ethiopia, College of Medicine and Health Sciences, Wolkite University, PO Box 07, Wolkite, Ethiopia, Tel +251 915715727, Email [email protected]
Background: Peripheral intravenous cannulas are routinely used in hospital-admitted children requiring intravenous therapy. The majority of peripheral IVC lines are removed before completion of therapy due to cannula complications in children. Peripheral intravenous cannula securing is a painful procedure for children, so recognizing the variables associated with the peripheral intravenous cannula lifespan would help decrease the complications and increase the duration of cannula patency.
Objective: The main aim of this study was to determine the lifespan and associated factors of peripheral intravenous cannula among hospitalized children in Gurage zone public hospitals, Ethiopia, 2021.
Methods: We conducted an institution-based cross-sectional study design among 422 admitted children in public hospitals of the Gurage zone using a systematic random sampling technique. We collected data from interviews of parents using structured questionnaires and direct observations using checklists. The data was coded and entered into EPI-DATA version 3.1 and exported to SPSS version 25 for analysis. Bivariable and multivariable analysis was used by using a binary logistic regression model. Finally, the variables with a p-value of < 0.05 with a 95% confidence interval (CI) from the multivariable analysis were considered statistically significant.
Results: One hundred and sixty-six children (41.4%) had a short cannula lifespan (below 30 h). Multivariable logistic regression analysis showed that neonatal intensive care unit (NICU) [AOR = 4.975; 95% CI (2.811– 8.805)], reason for removal (complication) [AOR = 3.277; 95% CI (1.924– 5.583)], fluid [AOR = 2.285; 95% CI (1.274– 4.100)], and blood transfusion [AOR = 2.407; 95% CI (1.005– 5.572)] were the statistically significant variables associated with the lifespan of a peripheral intravenous cannula.
Conclusion and Recommendation: The proportion of the short lifespan of the peripheral intravenous cannula was higher in hospitalized children and health care providers better to use low concentration electrolytes, low osmotic pressure, and weak alkalinity fluid. The cannula access might be the responsibility of the health-trained staff, and conserving immediate removal upon the presence of a signal that indicates a complication.
Keywords: lifespan, peripheral intravenous cannula, associated factors, hospitalized children
Introduction
Intravenous therapy (IVT) is the administration of therapeutic solutions directly into a vein.1 IV therapy is the fastest and most reliable way for the administration of fluid and electrolyte, chemotherapy administration, infused medications, transfused blood or blood components and provided some nutritional provisions such as total parenteral nutrition.2,3 Peripheral intravenous cannula (PIVC) is one of the most commonly performed procedures in any hospital. It is a common and universal medical practice to provide therapeutic IV medication4 with up to 70–80% of hospitalized patients requiring medication delivered through a vein cannula.5
In particular, preterm or critically ill infants and children are slow to tolerate the introduction of enteral feeding because of the immaturity of the gastrointestinal tract, delayed gastric emptying, and intestinal peristalsis.6 The intravenous route is the main access for medication administration in hospitalized children and is vital to their survival. A study conducted in Rio de Janeiro, among five neonatal units reported that 99.6% of newborns below 1.5 kg received intravenous drugs, these indicate great usage rates for peripheral vascular devices.7
Critically ill children frequently require intravenous therapy for more than seven days, comprising different drugs that irritate the vascular endothelium, which hinders peripheral vascular cannula maintenance for the time needed and enhances the risk of complications. Health care professionals consider drugs features, therapy duration, suitability, and assessment of the child’s venous before starting Intravenous therapy. Intravenous therapy quality is achieved when professionals manage to reduce related complications, the number of punctures, costs to optimize work and enhance patient safety.8
The need for vascular access in the child patient is frequent, but it is difficult, time-consuming, and frustrating to obtain reliable and confident vascular access in the pediatric patient, especially newborns. In addition to this, the veins in neonates and children are very tiny and easily ruptured, so the frequency of cannula change is high. Also, due to the diminishment of the intravenous devices, it is difficult to gain the vein of newborns. However, it requires considerable experience and skill to achieve this and good care of the child. Veins in the child are small and fragile, which implies low tolerance to pH and osmolality. Because of these factors, the extravasation rates are more than 40%, and about 91% of peripheral IV lines are removed before therapy is complete due to cannula complications in children9.
An intravenous cannula was removed if the intravenous cannula site became painful or erythematous, the cannula failed to function, fell out, or was removed as it was no longer required.10,11
The lifespan of PIVC is a significant issue, and its survival depends on many variables previous researchers had shown that child sex, cannula size, site of insertion, methods of administration of medications and fluids, blood transfusion, clinical experience of PIVC inserted nurse, and complications such as clotting, occlusion, leakage, infiltration, extravasation, phlebitis, and infection significantly affect the Lifespan of PIVC.12–14
The average lifespan of PIVC in neonates and children reported in different kinds of literature is 10 to 50 hours and 15 to 276 hours (hr), respectively.15,16 PIVC can be safely maintained with adequate monitoring for up to 144 hours in critically ill children.17
The consequence of cannula failure for patients and healthcare organizations is extensive and includes treatment delay, pain, distress, increased morbidity from complications, increased workloads on health care providers, and increased health care costs.18
The parent’s socio-demographic characteristic was not included in the previous study, but the current study was addressed.
In one study conducted in Mekelle, Ethiopia, this study only includes infants, but the lifespan of PIVC is a big issue in admitting children, and this study includes all admitted children in the hospital.
Identifying the factors that affect the lifespan of PIVC would help to increase cannula duration, reduce complications and identify areas of caregivers in need of change, and decide which interventions to implement for further supporting patients. It is essential to understand the factors that affect the lifespan of PIVC to find possible solutions for improving health care for hospitalized children. Therefore, this study aimed to assess the lifespan of PIVC among hospitalized children in public hospitals of the Gurage zone.
Materials and Methods
Study Design and Setting
We used an institution-based cross-sectional study design from June/1 to August/30/2021. The study was conducted in public hospitals of the Gurage zone, Southern Nation, Nationality People Region (SNNPR) South-West Ethiopia. Wolkite town is the capital of the Gurage zone, which is located 158 Km southwest of Addis Ababa and 260 Km from Hawassa. The Gurage Zone has a total area of 5932 square kilometers. It has 20 woredas and two municipalities with a total of 443 kebele of which 411 are rural and 32 urban. According to 2012 population projection by CSA, the total population is 1,767,518 among these under-five children comprising 15.6% (275,910).19
There are seven hospitals (five public and two non-governmental). Five of the hospitals are primary hospitals, one general hospital, and the other one is a specialized comprehensive hospital, 79 health centers (7 are NGO HC), and 444 Functional health posts serving the total population in the zone. All public hospitals in a Gurage zone that provide pediatric inpatient care were involved in the study.
Study Population
The study population involved selected neonates and children admitted to pediatric wards and units with an intravenous cannula in public hospitals of the Gurage zone during the data collection period.
Inclusion Criteria
Neonates and children admitted to the pediatric ward/unit with a PIVC for the administration of intravenous therapy were included.
Exclusion Criteria
Neonate and children secure PIVC and immediately discontinue after a procedure, the child’s death with a PIVC, and Children referred from another hospital with a PIVC were excluded.
Sampling Methods and Sampling Procedure
The sample size was determined using the single population proportion formula assumption that the proportion of short lifespan peripheral intravenous cannula was 52.8%16 from previous literature with 5% marginal error and 95% confidence interval (CI).
(1)
where n = Initial sample size, α = Precision level or level of significance, P = population Proportion of the lifespan of PIVC, w = Marginal error, Za/2 = the value under the standard normal table is 1.96. By adding a non-response rate of 10%, the final sample size was 422.
To select 422 admitted neonates and children in the pediatric ward/unit for all public hospitals in the Gurage zone, the last six months’ admission Neonate and children of each hospital were used to pediatrics in the patient flow rate of the respective hospitals. The sample size was proportionally allocated to each hospital in the Gurage zone based on the expected paediatric inpatient flow rate. A stratified random sampling technique was used to select admitted children in the hospital and ward/unit, and a systematic random sampling technique was used to select the study unit.
According to pre-assessment, the total sample size was met by a systematic random sampling technique (ie K=N/n =460/422 = 1.1 = 2) every two-interval admission included in the sample until the total sample size for this study had been obtained in all public hospitals. Based on the registration book, which is used as a sampling frame, a starting sample is determined by using simple random sampling by lottery method. The procedure continued throughout the data collection period until the required sample size was achieved.
Variables
Dependent variables
The lifespan of a peripheral intravenous cannula
Independent variables
Socio-demographic characteristics
Children clinical characteristics
Cannula characteristics
Healthcare-related characteristics
Operational Definition
- Hospitalized children: Children admitted in pediatric ward or unit in less than 15 years.
- Neonate: birth for up to 28 days.
- The Lifespan of PIVC: Calculated from the time of insertion to the time of removal.
- The Short Lifespan of PIVC is the duration of the PIVC is less than or equal to 30 hours.16
- The long Lifespan of PIVC is the duration of PIVC greater than 30 hours.
Data Collection Tool and Procedure
We developed the questionnaire from an extensive literature search by adapted from previously conducted studies14,16,20 with some changes based on the local context and consisted of five main themes: 1) parent socio-demographics, which surveyed parents’ socio-demographic characteristics, including gender, age, educational status, marital status, occupation, residence, religion, and relationship to the child 2) children socio-demographic age, gender.
3) Children clinical characteristics, including admission hospital, admission ward/unit, disease condition, length of ward stay, health status, weight and height/length 4) cannula characteristics, including cannula size or gauge, site of insertion, venous condition, use of glove, attached material and reason for removal and 5) healthcare-related factors including clinical experience, educational level, attempt to insert, medication type, fluid type, infusion type, and blood transfusion.
We determined the peripheral intravenous cannula lifespan, the times of insertion and removal noted, and then we calculated the lifespan from the time of insertion to the time of removal.
Categorizing into a short-life span of PIVC, the duration of PIVC is less than or equal to 30 hours and long lifespan of PIVC is the duration of PIVC greater than 30 hours.
Then, the designed questionnaires were changed from English to local language and back to English to check the consistency of the questionnaire. We used eight nurses for data collection and two nurses for supervision. The collected questionnaire was checked for completeness of the data by the principal investigator daily.
Data were collected through face-to-face interviews of the parents using structured questionnaires, chart review for children’s clinical related characteristics, and observational methods for cannula characteristics.
Data Quality Assurance
The quality of data was ensured through training of data Collectors and pretesting of the questionnaire. We tested the instrument by taking 5% of the sample size. Based on the pretest, the time needed to complete an interview and the total number of days needed for data collection were estimated.
The principal investigator and data collectors made frequent checks on the data collection process to ensure the completeness and consistency of the gathered data.
Data Processing and Analysis
We used EPI-DATA version 3.1 for data entry and SPSS version 25 for analysis. We presented the findings of the study using tables, graphs, pie charts, and narration.
Bivariate analysis and crude odds ratio with 95% confidence interval (CI) were used by using a binary logistic regression model. Adjusted odds ratio along with 95% CI was used to identify the factors associated with the lifespan of PIVC. Finally, the variables with a p-value ≤0.05 from the multivariable analysis were considered statistically significant.
Ethical Consideration
Wolkite University's Ethical Review Committee has approved this study and the verbal consent process. Upon this clearance, the managers of each public hospital in the Gurage zone took written permission. The responsible person in pediatric inpatient care talked about the purpose of the study, and the verbal consent to confirm willingness was taken from the participants. They notified that to have the right to refuse or terminate at any point of the interview and also the extracted information would not be used other than study purpose. We conducted the study per the declaration of Helsinki.
Result
Parent Socio-Demographic Characteristics of the Respondents
There were 401 study participants involved in this study with a response rate of 95%. The highest proportion of respondents (65.3%) was within the age group of 21–30 years with a mean age of 28.88 with SD 6.039. (76.8%) were the mothers of the children. Regarding marital status, majorities (93.5%) of the participants were married, and half of the participants (56.9%) lived in a rural area. Regarding the educational status of the respondents, one-third 35.4% were completed primary education, and (56.4%) were housewives. Half of the participants (52.1%) were Muslim followers (Table 1).
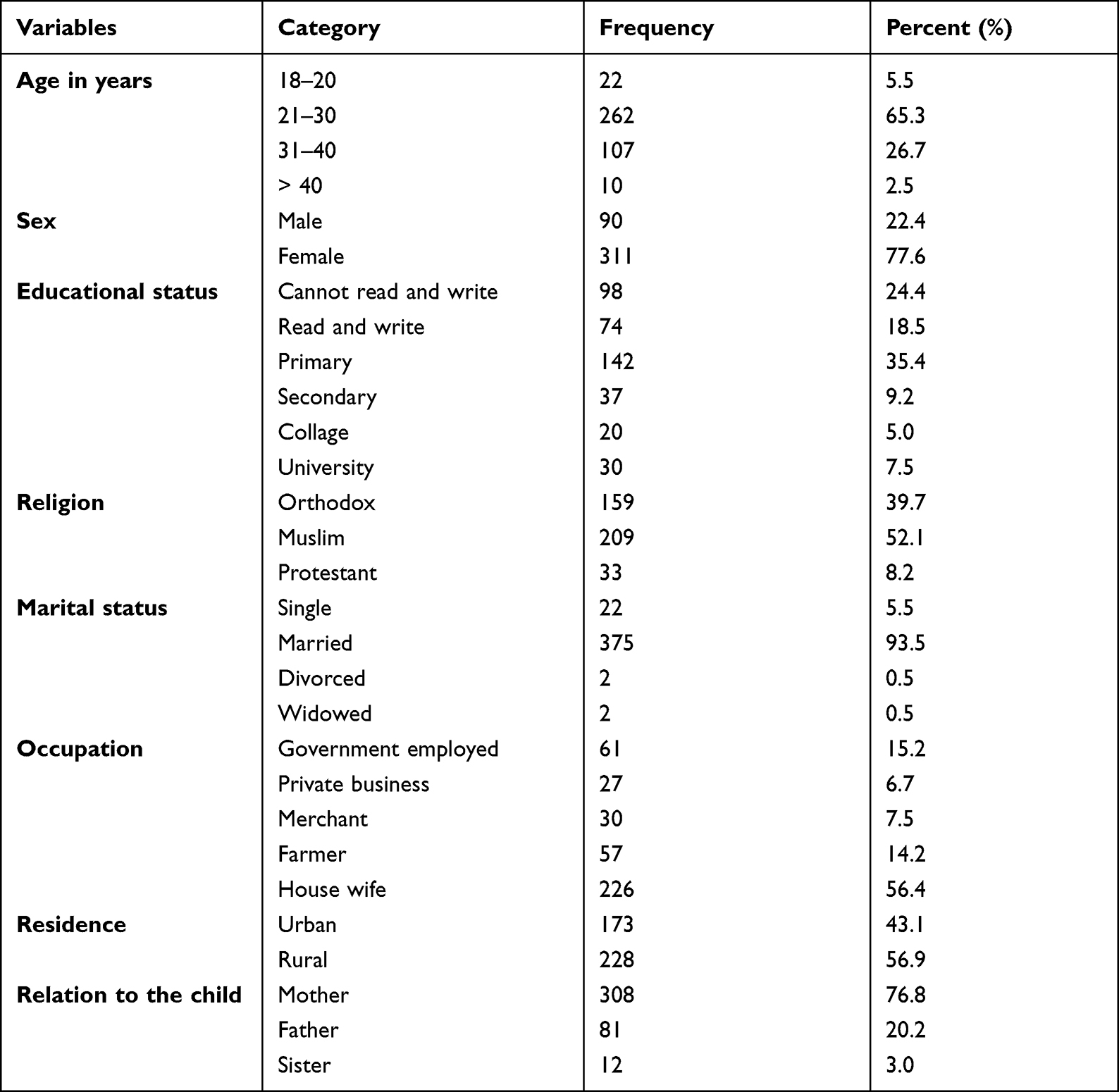 |
Table 1 Socio-Demographic Information About Parents in Gurage Zone Public Hospitals, Ethiopia, 2021 (n = 401) |
Children Socio-Demographic Characteristics
Among a total of 401 children who participated in the study, the highest proportion of children age (70.6%) was within the age group of 0–1 years with the median age of the children was 0.41 years with Inter-Quartile Range (IQR), 0.03–1.5 years. Regarding the sex of the children, the majority of the respondents (77.6%) were females (Table 2).
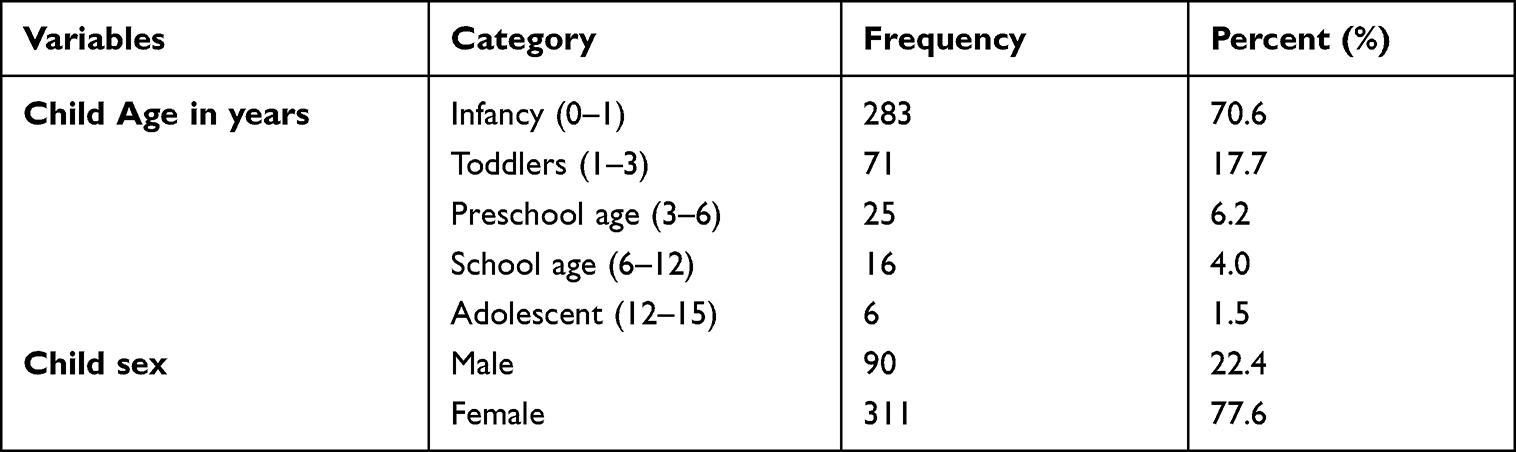 |
Table 2 Socio-Demographic Information About Children in Gurage Zone Public Hospitals, Ethiopia, 2021 (n = 401) |
Children Clinical Characteristics
Of the 401 children who participated in the study, half of the children were admitted to the general hospital. Regarding the admission of children in pediatric units (56.6%) children were admitted to the pediatric ward. The mean weight of the child was 7.38 with SD 5.74, and the mean height or length of the child 65.90 was with SD 20.61, regarding the length of stay in the ward or unit majorities (87.3%) children stay in the ward were less than or equal to 7 days. Majorities (94.5%) of children were acutely sick, and 189 (47.1%) were sub-critical health conditions. Regarding the diagnosis of the child, the highest disease cause for admissions was Severe community-acquired pneumonia (22.9%), followed by late-onset neonatal sepsis (14.0%) (Table 3).
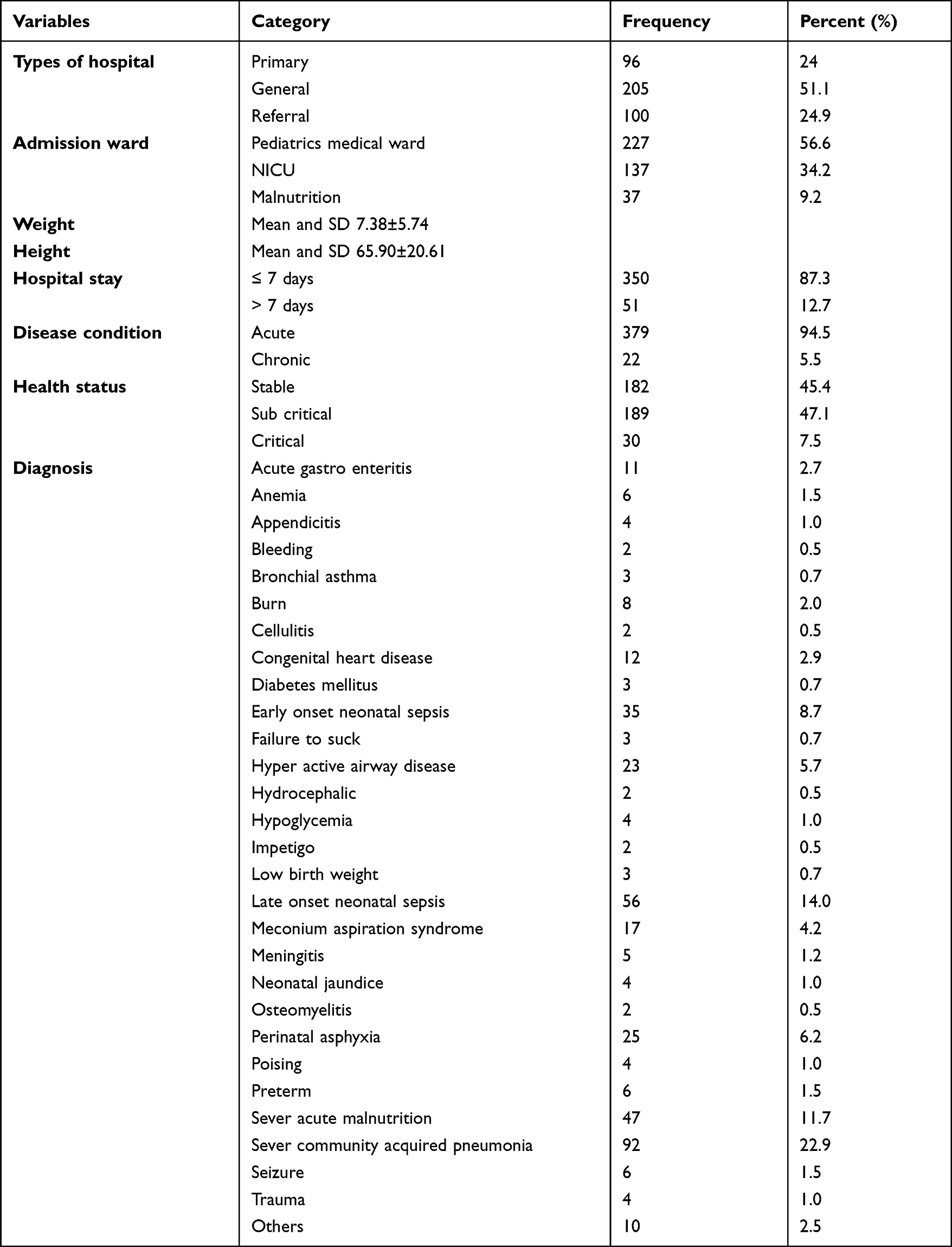 |
Table 3 Children Clinical Characteristics in Gurage Zone Public Hospitals, Ethiopia, 2021 (n = 401) |
Cannula Related Characteristics
Regarding the cannula size, a total of 401 peripheral intravenous cannula insertions were considered. Insertion was accomplished for 376 children (93.8%) by 24 gauge cannulas. When looking at inserted place 281 (70.1%), cannulas were inserted into veins of the hand. About 99% of the peripheral intravenous cannulas were attached to the insertion site by plaster. Regarding the type of glove used during insertion of peripheral intravenous cannula 337 (89.0%) were used sterile glove and majorities of 359 (89.5%) number of cannula inserted until the data collection time was one up to three cannulas. More than half of 215 (53.6%) cannulas were inserted in veins that were visible but not palpable. Half of the peripheral intravenous cannulas 202 (50.4%) were discontinued due to complications (Table 4).
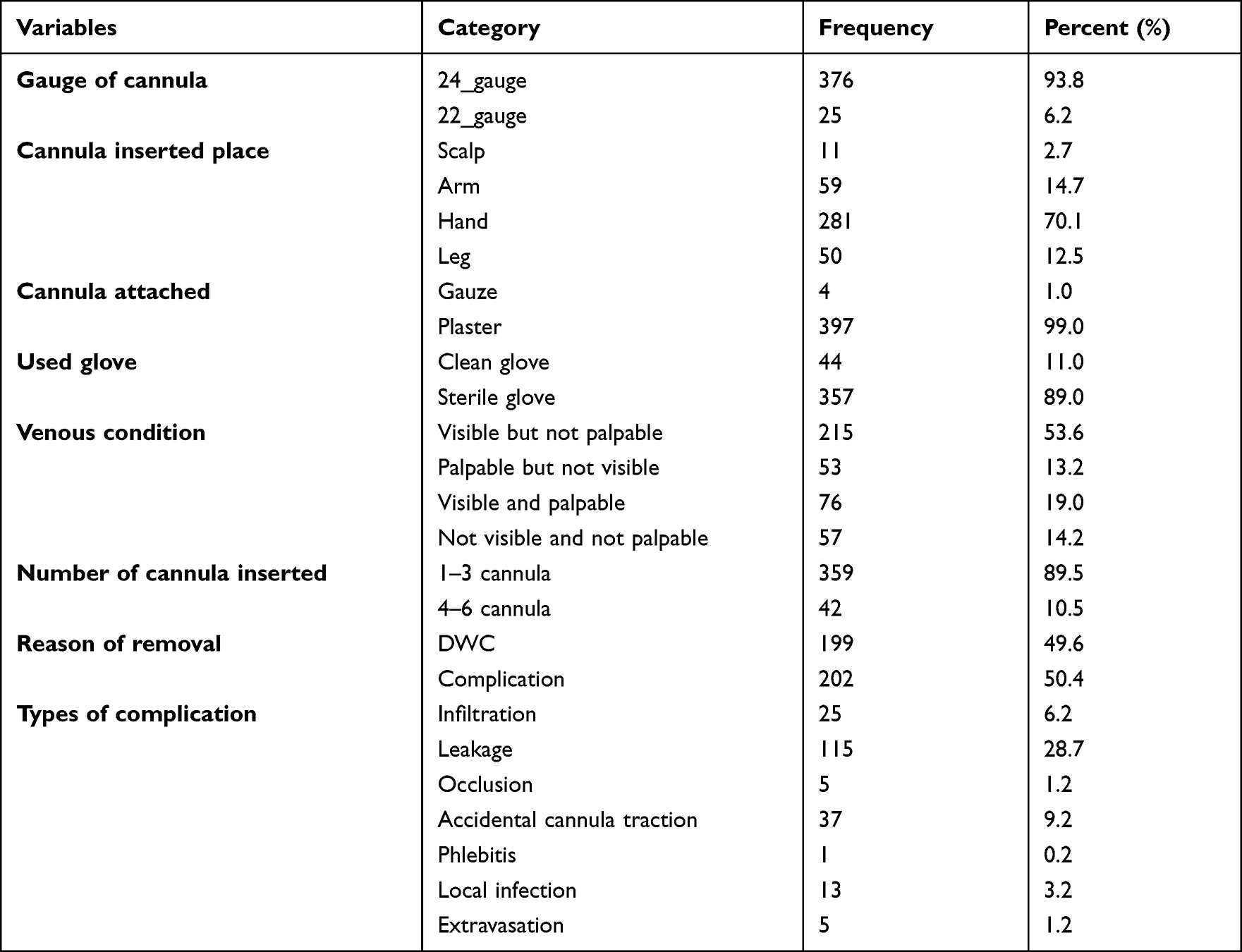 |
Table 4 Cannula-Related Characteristics of Children in Gurage Zone Public Hospitals, Ethiopia, 2021 (n = 401) |
Healthcare-Related Characteristics
Based on the data received, of the total sampled children with a peripheral intravenous cannula, in 192 cases 47.9% insertion was accomplished in 2–3 attempts, about 179 (44.6%) nurses who insert the cannula had 2–3 years of clinical experience, and 363 (90.5%) held degrees. About 377 (94.0%) of the peripheral intravenous cannulas were placed for administration of medication with or without fluid and blood transfusion. Around 290 (72.3%) of the peripheral intravenous cannula were used 1–2 times per day for medication administration and 360 (89.8%) were 1–2 drugs, antibiotics were among the most commonly administered medications accounting for 348 (86.8%) of peripheral intravenous cannulas. About 125 (31.2%) peripheral intravenous cannulas were placed for fluid administration, 95 (23.7%) children were resuscitated with maintenance fluid, and 67 (16.7%) were infused continuously.
Around 38 (9.5%) peripheral intravenous cannula was placed for blood transfusion. Twenty (5%) children were transfused whole blood (Table 5).
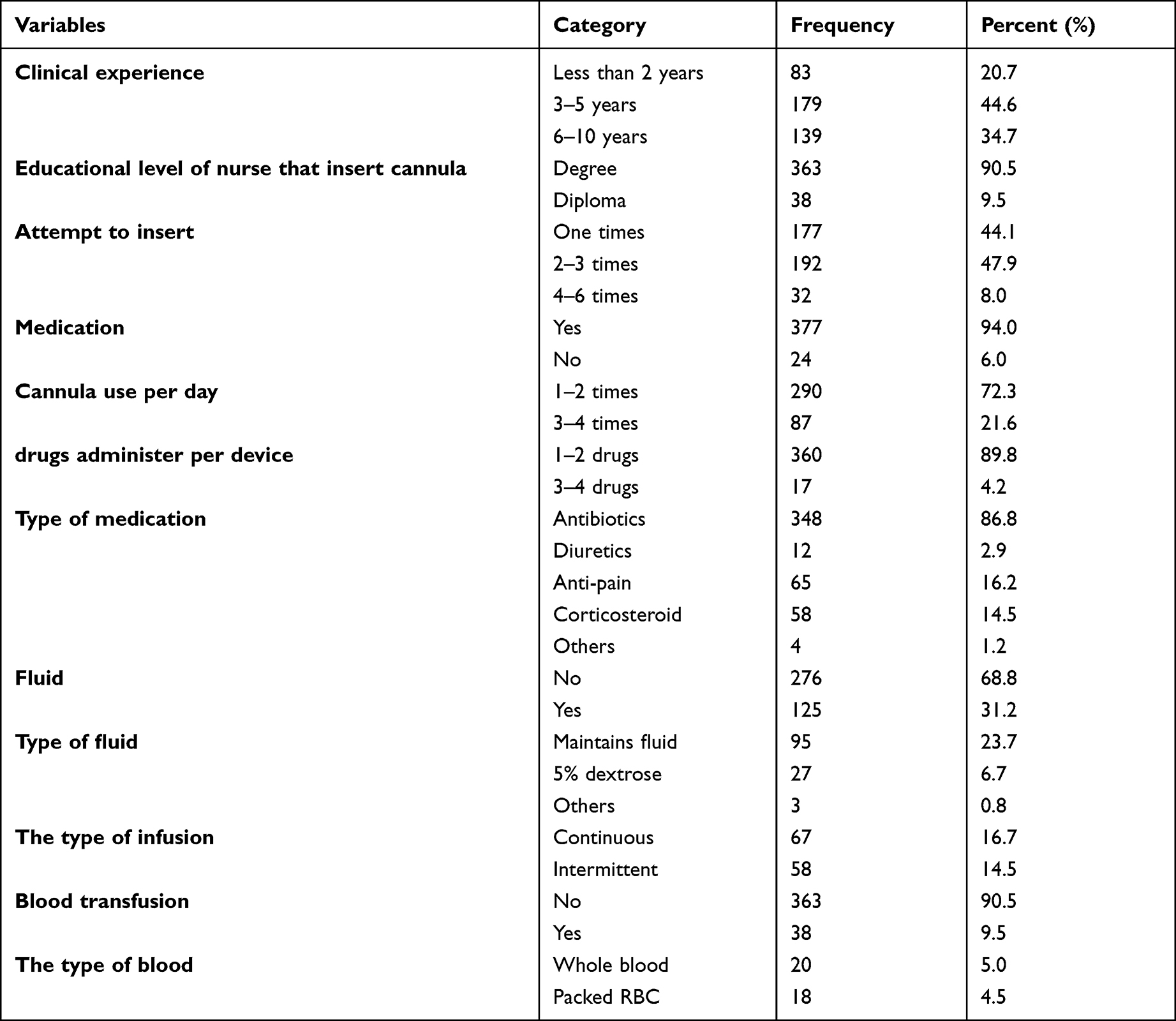 |
Table 5 Health Care Characteristics of Children in Gurage Zone Public Hospitals, Ethiopia, 2021 (n = 401) |
The Lifespan of a Peripheral Intravenous Cannula
The duration of peripheral intravenous cannulas in hospitalized children (n = 401) ranges from 10 to 183 hours for a median of 48 hours with an interquartile range of 24–72 hours. This study revealed that the proportion of the short lifespan of a peripheral intravenous cannula in hospitalized children was 166 (41.4%) with a 95% confidence interval (36.9–45.6%) (Figure 1).
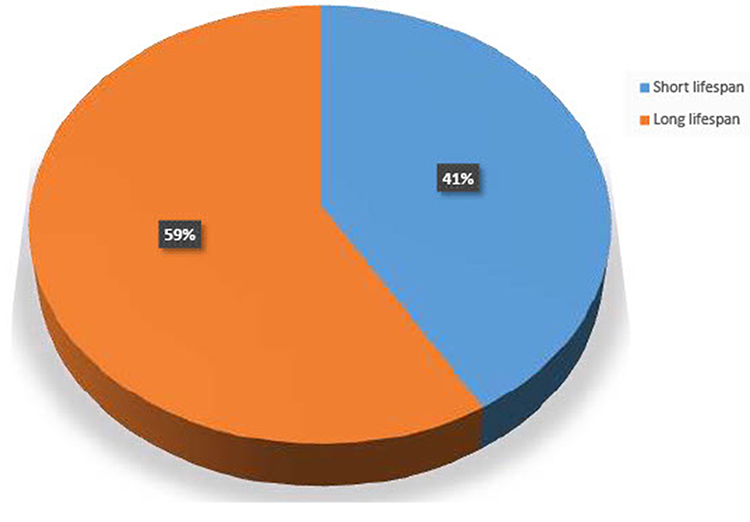 |
Figure 1 The peripheral intravenous cannula lifespan of children in Gurage zone public hospitals, Ethiopia, 2021 (n = 401). |
Factors Associated with the Peripheral Intravenous Cannula
Lifespan
From the bivariate analysis, types of hospital, admission ward, health status, inserted place, number of PIVC inserted, reason of removal, attempt to insert, medication, fluid, and blood transfusion were variables taken into consideration for multivariable analysis.
In multivariable logistic regression analysis, factors such as admission ward in a neonatal intensive care unit (NICU) [AOR = 4.975; 95% CI (2.811–8.805)], the reason for removal due to complication [AOR = 3.277; 95% CI (1.924–5.583)], fluid administration [AOR = 2.285; 95% CI (1.274–4.100)], and blood transfusion [AOR = 2.407; 95% CI (1.005–5.572)] were the statistically significant variables associated with the peripheral intravenous cannula lifespan among hospitalized children (Table 6).
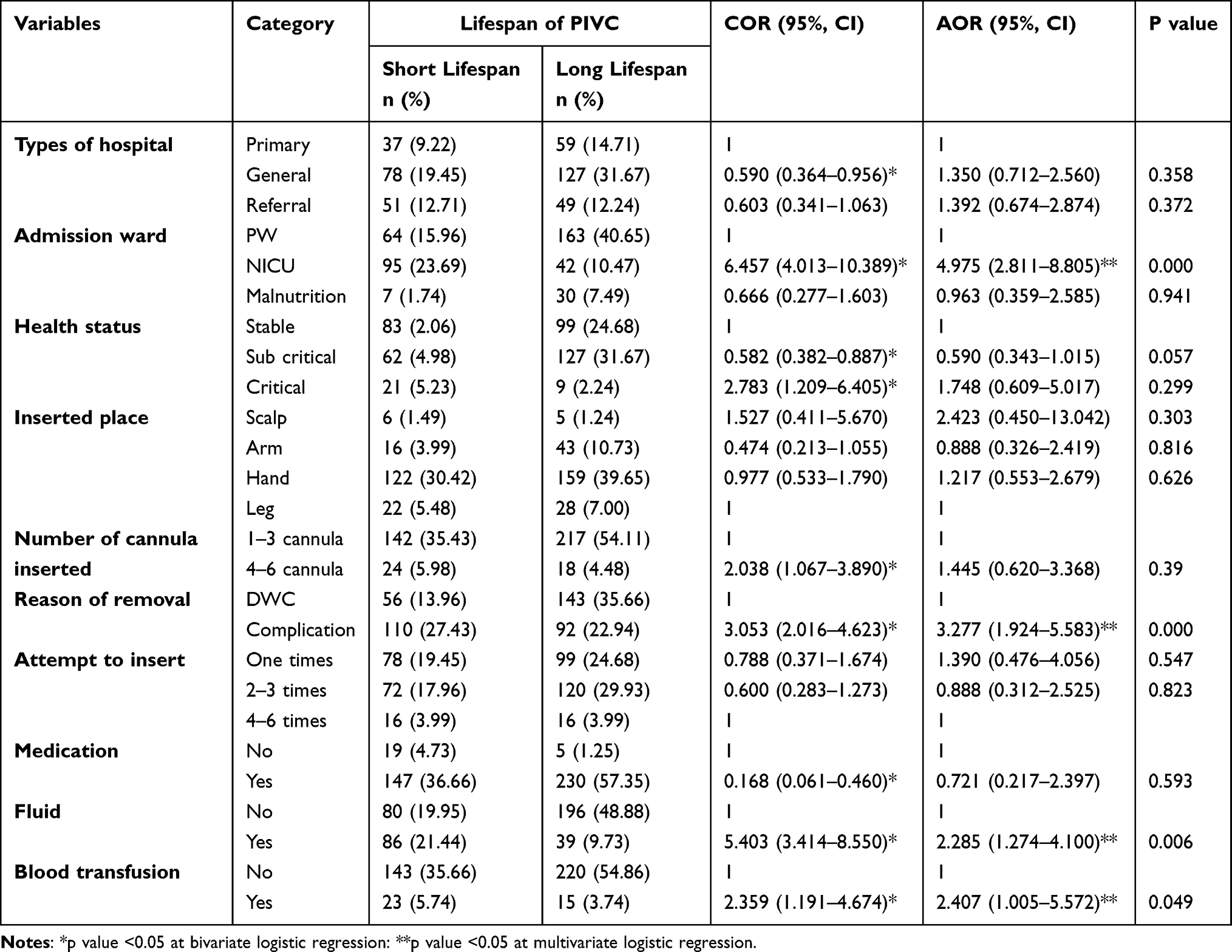 |
Table 6 Bivariate and Multivariable Logistic Regression Analysis Result of Lifespan and Associated Factors of Peripheral Intravenous Cannula Among Hospitalized Children in Gurage Zone Public Hospitals, SNNPR, South-West, Ethiopia, 2021 |
Discussion
In this study, one hundred sixty-six (41.4%) with a 95% confidence interval (36.9–45.6%) of the children had a short cannula lifespan (<30 hours). This study is lower than the study finding of Tigray, Ethiopia (52.8%) 16. It may be related to different study populations, different study setups, and different backgrounds could be the attributes for the difference.
In this study, the median lifespan of the cannula was 48 hours lower than the studies conducted previously in Colombia, among 223 hospitalized children reported that the median lifespan of the peripheral intravenous cannula was 129 h.21
However, in this study, the median lifespan of the cannula was 48 hours higher than the studies conducted previously reported from Australia (29 hr),22 India (40 hr),20 and the United States (33 hr).23 Maybe related to characteristics of the study population, socio-cultural difference, the type of health facilities, health service quality, contributions of the emerging advanced technology, different analysis methods and techniques used to compute the overall lifespan of the peripheral intravenous cannula according to the main objectives could be the attributes for the difference.
In the multivariable analysis, the admission ward showed a significant association with the peripheral intravenous cannula lifespan. PIVC lifespan was short in neonates admitted to a neonatal intensive care unit compared to those admitted to the pediatric ward. Similar findings were also observed in an earlier study conducted in the southwestern United States and Tigray, Ethiopia.15,16 It might be due to the reason that neonates admitted to neonates’ intensive care units were critically ill and were more likely to concurrently require more medications, and the neonates’ veins are very small and easily ruptured.
According to this study, complications affect the lifespan of PIVC. Similar findings were observed in an earlier study conducted in Tigray, Ethiopia.16 Maybe due to the cannula being foreign material inserted into the human body, the presence of a foreign body in the vein stimulates an inflammatory response, which disposes of the development of thrombus and complication.
Our finding also showed that the lifespan of a peripheral intravenous cannula with fluid administration was shorter than those who had not fluid administration. Similar findings were also observed in an earlier study conducted in Tunisia.24 This may be due to children who have taken high-concentration electrolytes, high osmotic pressure, and strong alkalinity that can damage the vein. And also, hyperosmolar agents such as 10% dextrose or total parenteral nutrition solutions can cause skin necrosis and serious issue damage.25 Children who had significant local tissue necrosis by peripheral extravasation of intravenous solutions containing high concentration electrolytes and/or 10% dextrose cause short peripheral intravenous cannula lifespan.
Our study also revealed that the peripheral intravenous cannula lifespan with the transfusion of blood was shorter than that of those who did not have to be blood transfused. Similar findings were also observed in an earlier study conducted in the southwestern United States and Tigray, Ethiopia.15,16 This might be due to the reason that it was hypothesized that alkalinity solutions infused in the peripheral intravenous cannula may be affecting the peripheral intravenous cannula lifespan.
Limitation of the Study
Since the data collection method used an observational checklist, the study might have been subjected to the Hawthorne effect, though this effect was tried to minimize by concealing the observation from the study participants. The lack of repeated observation of cannula-related characteristics may compromise the ascertainment of the peripheral intravenous cannula lifespan.
Strength of the Study
The strength of this study was the sample size and use of different variables, especially parent socio-demographic part and children clinical-related factors in hospitalized children. Careful selection of patients should have reduced the potential misrepresentation and bias estimates. Another strength is the insertions, and the removal date of the peripheral intravenous cannula was recorded by clinical staff and reduced the potential outcome misclassification.
Conclusion and Recommendation
Based on our findings, the proportion of the short peripheral intravenous cannula lifespan in hospitalized children was higher in public hospitals of the Gurage zone, Ethiopia.
The finding revealed that the Admission ward (neonatal intensive care unit), the reason for the removal (complication), fluid administration, and blood transfusion were the statistically significant variables associated with the peripheral intravenous cannula lifespan.
Health care providers better use low concentration electrolytes, low osmotic pressure, and weak alkalinity fluid. Health care providers better pay attention to neonates admitted to the neonatal intensive care unit the PIVC, access that might be the responsibility of the health-trained staff, and conserving immediate removal upon the presence of a signal that indicates a complication.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; CMHC, College of Medicine and Health Sciences; COR, crude odds ratio; CSA, Central Statistical Agency; HR, hours; IV, intravenous; IVC, intravenous cannula; IVT, intravenous therapy; NICU, neonatal intensive care unit; PICU, pediatric intensive care unit; PIVC, peripheral intravenous cannula; PW, pediatrics ward; SNNP, south nation, nationality and people; SPSS, Statistical Product and Service Solution; WKUCSTH, Wolkite University Comprehensive Specialized Teaching Hospital.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author under the permission of Wolkite University on reasonable request.
Ethic’s Approval and Consent to Participate
Wolkite University's Ethical Review Committee has approved this study and the verbal consent process. Upon this clearance, the managers of each public hospital in the Gurage zone took written permission. The responsible person in pediatric inpatient care talked about the purpose of the study, and the verbal consent to confirm willingness was taken from the participants. They notified that to have the right to refuse or terminate at any point of the interview and also the extracted information would not be used other than study purpose. This study was conducted per the declaration of Helsinki.
Consent for Publication
The study did not include images or videos relating to an individual, but rather obtaining consent from each participant and information to publish the findings addressed, and participants agreed on that.
Acknowledgments
We would like to express our deepest gratitude to Wolkite University for its holistic support. Secondly, we would like to express our profound gratitude to the Gurage zone public hospital health office administration and health care providers for their valuable support while collecting the data. Our thanks also go to all data collectors for carrying out their responsibilities effectively during the data collection and all study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work and that they have no financial or non-financial competing interests.
References
1. Ingram P, Livery I. Peripheral intravenous therapy: key risks and implications for practice. Nurs Stand. 2005;19:46.
2. Pettit J. Fostering a new era of vascular access device selection in neonates. Newborn Infant Nurs Rev. 2006;6(4):186–192. doi:10.1053/j.nainr.2006.09.004
3. The Royal Children's Hospital Melbourne. Peripheral intravenous (IV) device management; 2018. Accessed March 15, 2022.
4. Dougherty L. Back to basics in IV therapy: an unfortunate necessity MA Healthcare London. Br J Nurs. 2008;17:S3.
5. Alexandro E, Raman L, Murphy J, Hunt L, Bentihavas V, Frost SA. Training of undergraduate clinicians in vascular access an integrative review. J Assoc Vasc Access. 2012;17(3):146–158. doi:10.1016/j.java.2012.07.001
6. Ainsworth S, McGuire W. Percutaneous central venous catheters versus peripheral cannula for delivery of parenteral nutrition in neonates. Cochrane Database Syst Rev. 2015;(10). doi:10.1002/14651858.CD004219.pub4
7. Zing W, Pitted D. Peripheral venous catheters: an under-evaluated problem. Int J Antimicrob Agents. 2009;34:S38–S42. doi:10.1016/S0924-8579(09)70565-5
8. Larsen P, Eldridge D, Brinkley J, et al. Pediatric peripheral intravenous access does Nursing experience and competence make a difference. J Infus Nurs. 2010;33(4):226–235. doi:10.1097/NAN.0b013e3181e3a0a8
9. Spas SK, Singh SK. Venous access in neonates’. Int J Contemp Pediatr. 2018;5(4):1571. doi:10.18203/2349-3291.ijcp20182567
10. Acar Mdad Güner ÜÇ, Yilmaz G. Evaluation of the duration of peripheral venous catheter in vein in hospitalized children. J Contemp Med. 2022;11(5):1–7.
11. Thigpen J. Peripheral intravenous extravasation: nursing procedure for initial treatment. Neonatal Netw. 2007;26(6):379–384. doi:10.1891/0730-0832.26.6.379
12. De la Vieja-soriano M, Blanco-Daza M, Macip-Belmonte S, Dominguez-Muñoz M, López-Sánchez E, Pérez-Pérez E. Vía venosa difícil en una unidad de cuidados intensivos pediátricos. Enferm Intensiva. 2021. doi:10.1016/j.enfi.2021.03.007
13. Wallis MC, McGrail M, Webster J, et al. Risk factors for peripheral intravenous catheter failure: a multivariate analysis of data from a randomized controlled trial. Infect Control Hosp Epidemiol. 2014;35(1):63–68. doi:10.1086/674398
14. Shenoy S, Karunakar B. Factors influencing the peripheral venous catheter survival in critically ill children in a pediatric intensive care unit the Indian. J Pediatr. 2014;81(12):1293–1296.
15. Smith AB, Wilkinson-Faulk D. W-FD factors affecting the life span of peripheral intravenous lines in hospitalized infants. Pediatr Nurs. 1994;20(6):543–547.
16. Birhane E, Kidanu K, Kassa M, et al. Lifespan and associated factors of peripheral intravenous Cannula among infants admitted in public hospitals of Mekelle City, Tigray, Ethiopia, 2016. BMC Nurs. 2017;16(1):1–8. doi:10.1186/s12912-017-0227-1
17. Owen VS, Rosgen BK, Cherak SJ, et al. Adverse events associated with administration of vasopressor medications through a peripheral intravenous catheter: a systematic review and meta-analysis. Crit Care. 2021;25(1):1–12. doi:10.1186/s13054-021-03553-1
18. Helm RE, Klausner JD, Klemperer JD, Flint LM, Huang E. Accepted but unacceptable: peripheral IV catheter failure. J Infus Nurs. 2015;38(3):189–203. doi:10.1097/NAN.0000000000000100
19. Central Statistical Agency. Population and household census of Ethiopia; 2007.
20. Gupta P, Ray R, Base S, Farida M. Life span of a peripheral intravenous cannula in a neonatal intensive care unit of a developing country. J Pediatr Nurs. 2003;18(4):287–292. doi:10.1016/S0882-5963(03)00052-6
21. Elizabeth Gómez-Neva M, Alonso Rendon Sepulveda M, Buitrago-Lopez A. Lifespan of peripheral intravenous short catheters in hospitalized children: a prospective study. J Vasc Access. 2021;11297298211005299. doi:10.1177/11297298211005299
22. Mallon L, Ullman AJ, Phillips N, et al. Peripheral intravenous catheter duration and failure in pediatric acute care: a prospective cohort study. Emerg Med Australas. 2014;26(6):602–608. doi:10.1111/1742-6723.12305
23. Johnson RV, Donn SM. The life span of intravenous cannulas in a neonatal intensive care unit. Am J Dis Child. 1988;142(9):968–971. doi:10.1001/archpedi.1988.02150090066024
24. Abdelaziz RB, Hafsi H, Hajji H, et al. Full title: peripheral venous catheter complications in children: predisposing factors in a multicenter prospective cohort study. BMC Pediatr. 2017;17(1):1–11. doi:10.1186/s12887-016-0759-7
25. Doellman D, Hadaway L, Bowe-Geddes LA, et al. Infiltration and extravasation: update on prevention and management. J Infus Nurs. 2009;32(4):203–211. doi:10.1097/NAN.0b013e3181aac042
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.