Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Life’s Crucial 9 Score as a Novel Role for Chronic Obstructive Pulmonary Disease Screening
Authors Li W ![]() , Wen Y, Fan Y, Hu Z, Deng Z
, Wen Y, Fan Y, Hu Z, Deng Z ![]() , Huang Q
, Huang Q ![]()
Received 2 February 2025
Accepted for publication 5 June 2025
Published 2 July 2025 Volume 2025:20 Pages 2161—2171
DOI https://doi.org/10.2147/COPD.S515649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Wenqiang Li,1,* Youli Wen,1,* Yuting Fan,2 Zefu Hu,3 Zhiping Deng,1 Qian Huang3
1Department of Respiratory and Critical Care Medicine, Zigong First People’s Hospital, Zigong, Sichuan Province, 643000, People’s Republic of China; 2Department of Clinical Medicine, North Sichuan Medical College, Nanchong, Sichuan Province, 637000, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, Dazhou Dachuan District People’s Hospital (Dazhou Third People’s Hospital), Dazhou, Sichuan Province, 635000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Huang, Department of Respiratory and Critical Care Medicine, Dazhou Dachuan District People’s Hospital (Dazhou Third People’s Hospital), Dazhou, 635000, Sichuan Province, People’s Republic of China, Tel +8615196767955, Email [email protected] Zhiping Deng, Department of Respiratory and Critical Care Medicine, Zigong First People’s Hospital, Zigong, 643000, Sichuan Province, People’s Republic of China, Tel +8613608158051, Email [email protected]
Purpose: This study aims to investigate the association between the Life’s Crucial 9 (LC9) score and chronic obstructive pulmonary disease (COPD) in middle-aged and older adults.
Patients and Methods: We screened the NHANES database for data from 2007– 2018. Logistic regression analysis and subgroup analysis were used to explore the association between LC9 score and COPD in middle-aged and older adults. Additionally, restricted cubic spline (RCS) was plotted to visually depict the dose-response relationship between the two.
Results: A total of 12,030 participants were included, of whom 815 had COPD. After multivariate adjustment, the LC9 score was found to be inversely associated with COPD diagnosis. The RCS visually demonstrated a linear decreasing relationship between the two. Furthermore, subgroup analysis revealed no significant interaction across different subgroups, except for education level.
Conclusion: The LC9 score is linearly and inversely associated with COPD diagnosis. Higher LC9 scores are associated with a lower COPD diagnosis in individuals aged 40 and above.
Keywords: COPD, middle-aged and older adults, life’s crucial 9, diagnosis, cardiovascular health
Introduction
The concept of “Life’s Essential Metrics” was introduced by the American Heart Association (AHA) in 2010 as a critical framework for defining cardiovascular health.1 Initially launched as Life’s Simple 7 (LS7), the metrics included: blood glucose, blood pressure, cholesterol levels, smoking, alcohol consumption, body mass index (BMI), and physical activity.1 In 2022, sleep health was added the framework, updating the metric to Life’s Essential 8 (LE8).1,2 By 2024, Circulation published research highlighting mental health as a vital component of cardiovascular well-being, expanding the framework to Life’s Essential 9 to incorporate this dimension.3 Nowadays, the LC9 score is an ideal indicator to quantify CVH. Moreover, several studies have shown that life element also serve as predictors of other diseases.Tang et al showed that LE8 scores were positively correlated with bone mineral density and negatively correlated with osteoporosis, regardless of age or gender.4 Chen et al found that higher LE8 scores are associated with a reduced risk of periodontitis.5
Chronic Obstructive Pulmonary Disease (COPD) is a common respiratory disorder characterized by symptoms such as cough, sputum production, and wheezing. It often leads to complications like heart disease and respiratory failure, resulting in adverse outcomes.6 According to statistics, COPD is now the third leading cause of death worldwide, with 33 million deaths in 2019 alone.7 Additionally, COPD imposes a substantial and unevenly distributed economic burden globally, with 90% of COPD-related deaths occurring in low- and middle-income countries. Notably, China and the United States face the most severe economic burdens due to high prevalence rates, healthcare costs, and productivity losses linked to COPD.7 Research estimates that COPD will result in losses of $43.26 trillion between 2020 and 2050, equivalent to 0.11% of global GDP annually in taxes.7 Therefore, COPD diagnosis and early intervention are very important.
Mental health is currently a major public issue, especially depressive symptoms. According to World Health Organization (WHO) statistics, more than 350 million people worldwide suffer from depression, and approximately 1 million people commit suicide each year.8 In particular, the global prevalence of major depressive disorder in older persons is 13.3%, which is increasing year after year.9 It is expected to contribute significantly to the global disease burden by 2030.10 Furthermore, there is an interplay between depressive symptoms and COPD. Depressive symptoms may be an underlying etiology of COPD, and COPD is more likely to be comorbid with depressive symptoms.11,12 Compared to LE8 and LS7, the LC9 score integrates mental health components. Utilizing the LC9 score to investigate COPD allows for a more comprehensive reflection of the true association between these factors.
COPD is a systemic disease closely related to multiple other diseases.13 Life element have been proven to be closely related to CVH.1–3,14 Currently, the LC9 score is recognized as the latest ideal indicator for quantifying CVH.3 However, the relationship between the LC9 score and COPD diagnosis has not been studied yet. Therefore, our study aims to explore the association between LC9 scores and COPD diagnosis based on the contents of the National Health and Nutrition Examination Survey (NHANES) database. This study provides references for clinical practice and personal lifestyle choices, with the goal of improving the quality of life and overall health of individuals.
Research Design and Methods
Study Population
The NHANES database (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx) is a public database that is rich in content, authentic and reliable, with a nationally representative sample obtained through a stratified multi-stage probability sampling design (a combination of multistage stratified sampling, oversampling, and weight adjustment). The database follows a two-year cycle, conducting annual surveys of approximately 5000 individuals nationwide each year. And all participants signed an informed consent form provided by the NHANES Ethics Review Board.
We selected participants from the NHANES database from 2007 to 2018 (N=75,402). The following exclusion criteria were applied: 1) missing LC9 data (N=2738); 2) age <40 years (N=44,873); 3) pregnancy (N=11); 4) tumors (N=2836); 5) other missing data (N=12,964). Ultimately, a total of 12,030 participants were included for analysis, of which 815 had COPD (Figure 1).
 |
Figure 1 Participant screening flowchart. |
Definition of COPD
COPD was primarily identified based on pulmonary function tests, COPD questionnaire reports (MCQ160G, MCQ160P), and medication use. Additionally, these criteria have been widely applied in NHANES-related studies.15–18 Therefore, meeting one of the following three criteria is sufficient to classify a participant as having COPD. The criteria are as follows:
- FEV1/FVC < 0.7 after inhalation of a bronchodilator.
- The patient has a prior diagnosis of emphysema/COPD made by a physician.
- Aged over 40 years, with a history of smoking or chronic bronchitis, and use of medications for COPD (including leukotriene modifiers, inhaled corticosteroids, selective phosphodiesterase-4 inhibitors, and mast cell stabilizers).
Description of LC9 Scores
Gaffey et al clearly defined LC9, which more accurately quantifies cardiovascular health than LS7 and LE8.3 The LC9 includes four health behavioral factors (physical activity, tobacco, diet, and sleep) and five health factors (weight, cholesterol, blood glucose, blood pressure, and psychological health). According to the characteristics of the NHANES database and previous related studies, the LC9 score in this study was calculated as follows: LC9 score = the mean of the sum of the LE8 score and the depressive symptom score.2,19–21 Depressive symptom scores were determined from the Patient Health Questionnaire 9 (PHQ-9) scores. Depression scores were categorized as 100, 75, 50, 25, and 0, corresponding to 0–4, 5–9, 10–14, 15–19, and 20–27 on the PHQ-9 scale, respectively.19 The LC9 score is categorized as high (80–100), moderate (50–79), or low (0–49).3 The higher the score, the better the state of cardiovascular health.2,20 Detailed scoring criteria for each factor can be found in the Supplementary File 2.
Research Variables
Based on previous literature, we included variables that may affect the association between LC9 score and COPD. Demographic variables include age (40–64 years or ≥65 years), sex (male or female), race (White or Other), and marriage (Married/Living with Partner, Widowed/Divorced/Separated, or Never married). Socioeconomic variables include education (Less than high school, High school diploma, or More than high school), poverty income ratio (PIR) (<1.3, 1.3–3.5, or >3.5), and household insurance (Yes or No). The PIR ranges from 0 (no family income) to 5 (family income is at least five times the federal annual poverty level).
Statistical Analysis
This study included data from six cycles of the NHANES database. Appropriate weights (wtdrd1) were selected based on the study factors and outcomes, and all subsequent statistical analyses were conducted on weighted data. All statistical analyses were performed using R software version 4.3.2, with a two-sided P < 0.05 considered statistically significant. All study variables were converted into categorical variables and presented as percentages. The chi-square test was used for between-group comparisons. Logistic regression analysis was employed to evaluate the odds ratios (OR) of COPD diagnosis associated with the LC9 score, and 95% confidence intervals (CI) were calculated.
We constructed three models for analysis. The crude model did not adjust for any factors. Model 1 adjusted for age, sex, race, marriage, and education. Model 2 adjusted for PIR and household insurance based on Model 1. And subgroup analyses by age, sex, race, marriage, household insurance, and education level assessed whether the above relationships were affected by underlying factors. Additionally, we explored whether the dose-response relationship between the two was affected by nonlinearity using a restricted cubic spline (RCS) function. The interpretation criteria for the results were as follows:
- P overall < 0.05 and P for nonlinearity < 0.05, indicating that the indicator is associated with the outcome and the relationship is nonlinear.
- P overall < 0.05 and P for nonlinearity > 0.05, indicating that the indicator is associated with the outcome, but nonlinearity cannot be proven, suggesting a linear relationship to some extent.22–25
- P overall > 0.05 and P for nonlinearity < 0.05, this situation does not exist in reality.
- P overall > 0.05 and P for nonlinearity > 0.05, indicating that the indicator is not correlated with the outcome and there is no nonlinearity.
Results
Baseline Characteristics
We included a total of 12,030 participants, among which 815 had COPD. As shown in Table 1, COPD is commonly found in individuals aged 40–64, whites, those who are married or living with a partner, have higher education levels, and have household insurance. The distribution across different PIR levels is similar. The higher incidence in whites may be due to the fact that the NHANES database data comes from the US population, which is predominantly white. The LC9 score is currently the most comprehensive and ideal international indicator for assessing CVH. As shown in Table 1, the proportion of COPD patients is highest when the LC9 score is at the moderate level (50–79) and lowest at the high level (80–100).
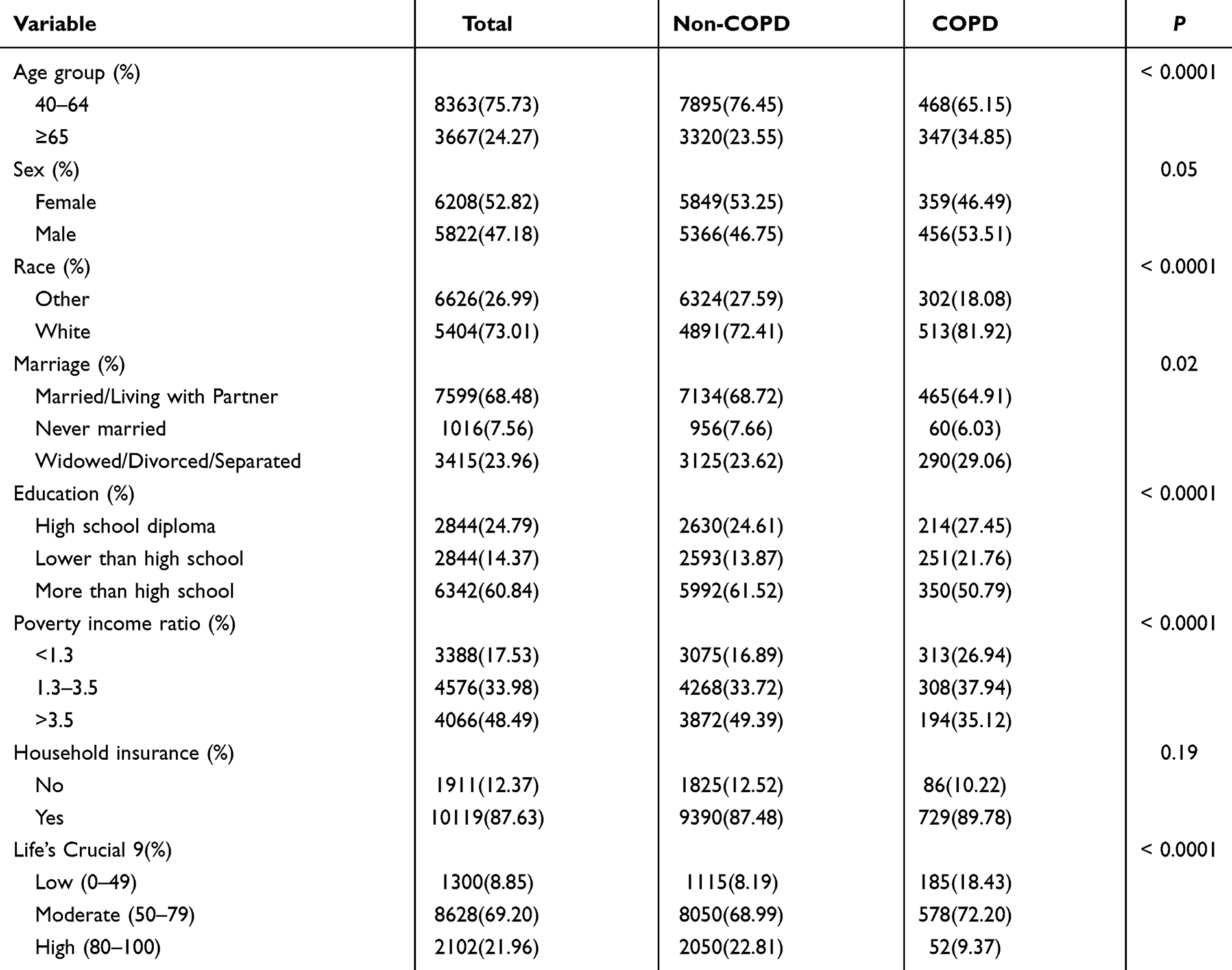 |
Table 1 Baseline Characteristics of the Study Population |
Association Between the LC9 Score and COPD
We categorized the LC9 score into low (0–49), moderate (50–79), and high (80–100) levels and explored the potential dose-response relationship between the LC9 score and COPD diagnosis from a class variable perspective in multiple models. We found a linear decreasing relationship between the LC9 score and COPD diagnosis, regardless of age, sex, or socioeconomic status (P for trend < 0.0001). In the fully adjusted model, compared to individuals with low LC9 scores, those with moderate LC9 scores showed an approximately 49% reduction in COPD diagnosis risk (OR 0.51, 95% CI (0.41, 0.65)), while high LC9 scores were associated with a 76% reduction (OR 0.24, 95% CI (0.14, 0.39)). The additional 27% risk reduction observed in the high vs moderate LC9 score groups was statistically significant (P < 0.0001), with a pronounced linear trend (P for trend < 0.0001) (Table 2). Meanwhile, we plotted the RCS to visualize the dose-response relationship between the two from a continuous variable perspective. As shown in Figure 2, the OR for COPD diagnosis equals 1 at an LC9 score of 67.2, indicating no increased or decreased risk at this threshold. Overall, the relationship between LC9 scores and COPD risk follows a monotonically decreasing curve. As the LC9 score increases, the risk of COPD diagnosis progressively declines, demonstrating a significant linear inverse association (P overall<0.0001, P for nonlinear=0.289).
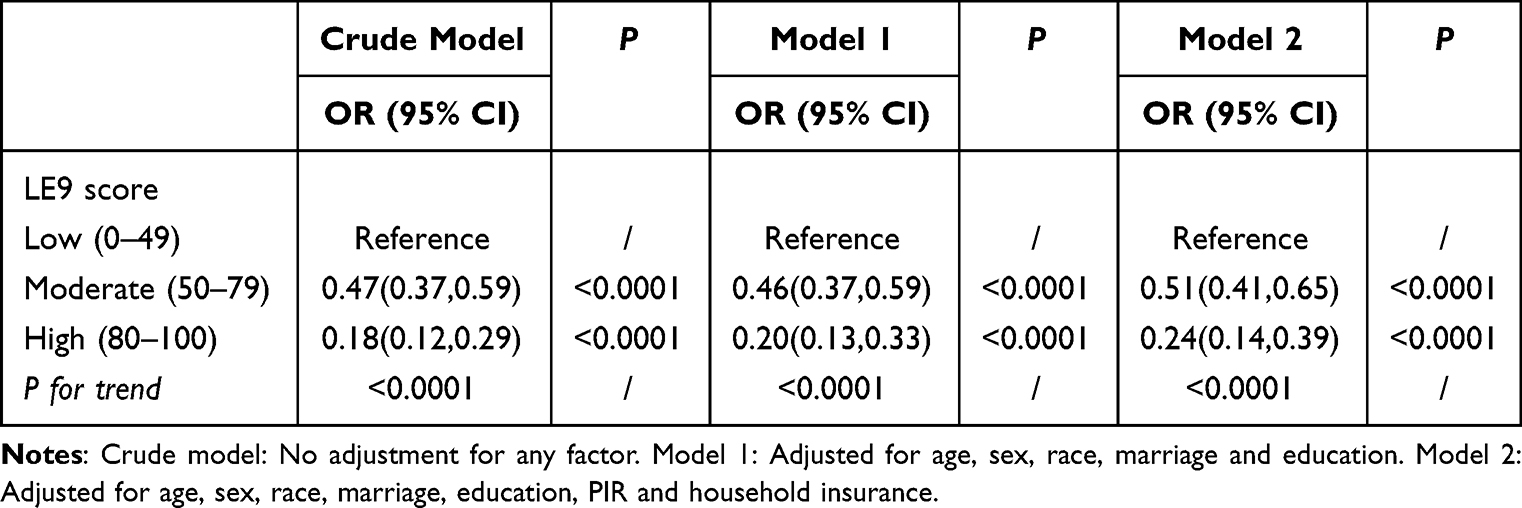 |
Table 2 Association Between the Life’s Crucial 9 (LC9) Score and Chronic Obstructive Pulmonary Disease (COPD) Diagnosis |
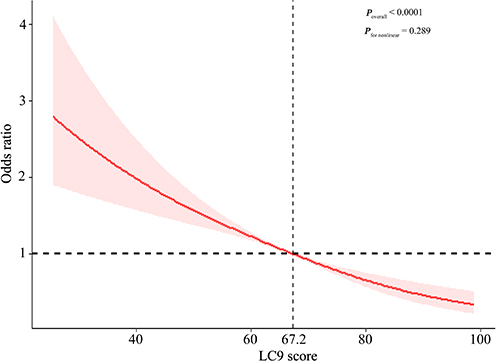 |
Figure 2 The linear relationship between LC9 score and COPD diagnosis. |
Subgroup Analysis
We further explored whether there was an interaction effect between the relationship between LC9 score and COPD diagnosis across subgroups. The results showed that there was no interaction effect between the subgroups of sex, age, race, PIR, and household insurance, except for education level (P for interaction>0.05, Table 3). However, in the education level grouping, we found that there was no decreasing relationship between the LC9 score and COPD diagnosis in individuals with a high school education level (P for trend = 0.46, in Table 3). Similarly, the household insurance grouping revealed that this relationship was also absent in individuals without insurance (P for trend = 0.10, in Table 3).
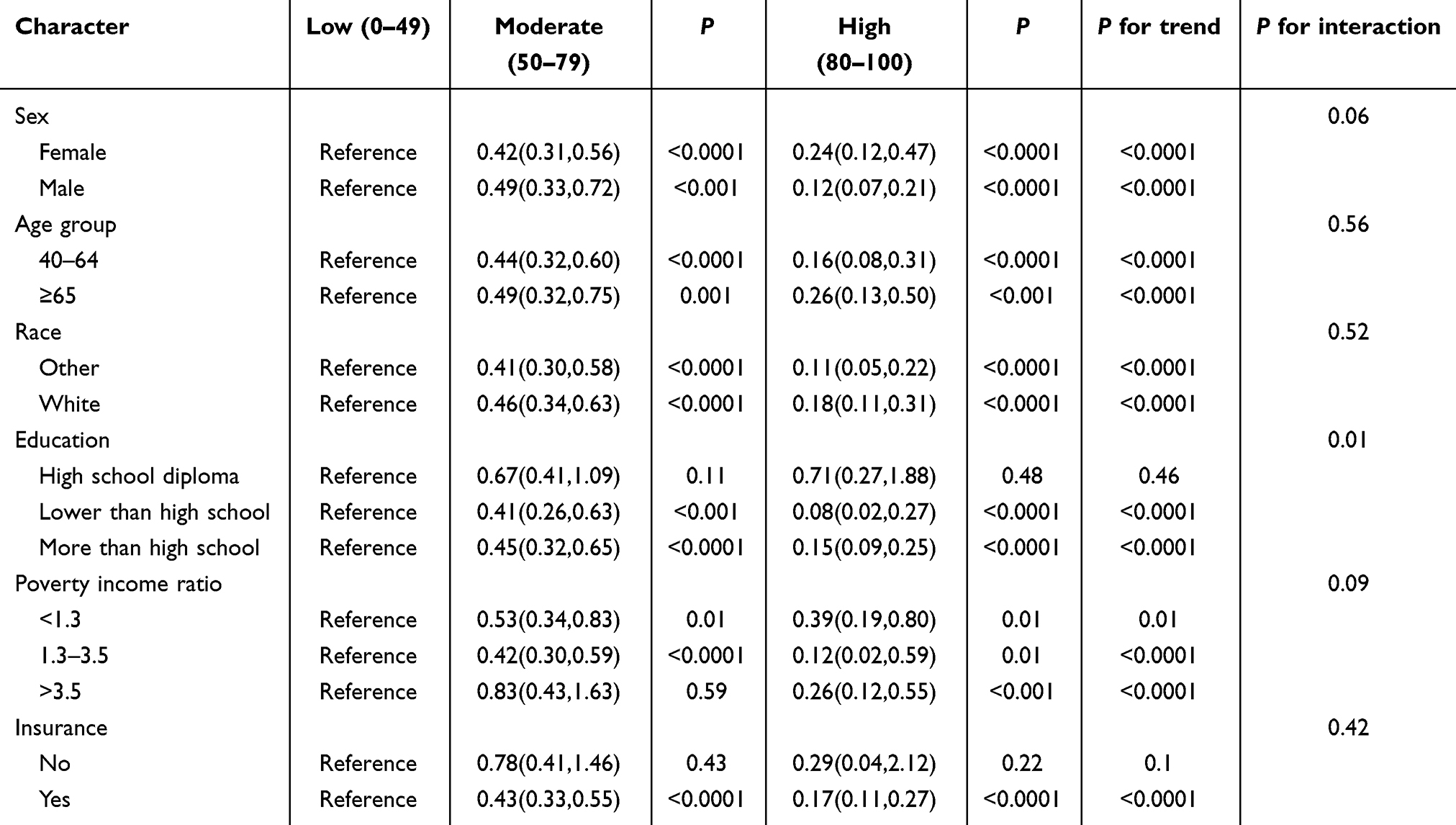 |
Table 3 Subgroup Analysis of the Association Between the LC9 Score and COPD Diagnosis |
Discussion
We conducted the first exploration of the relationship between LC9 scores and COPD diagnosis in middle-aged and elderly individuals using cross-sectional survey data from the NHANES database from 2007 to 2018. The results showed a nonlinear decreasing relationship between LC9 score and the risk of developing COPD in middle-aged and older adults. As LC9 scores increased, COPD diagnosis risk in middle-aged and elderly individuals decreased. However, this relationship was not confirmed in populations with a high school education level or those without insurance coverage. Subgroup analysis indicated that education level may be a confounding factor in this relationship (P for interaction = 0.01, Table 3).
LC9 has recently been updated to describe the most ideal indicators of CVH, which are closely related to the occurrence of cardiovascular diseases (CVD).3 Moreover, CVD and COPD often influence each other, with pathological and physiological connections between them, and share similar pathogenic mechanisms and risk factors.3,26,27 CVD is associated with reduced exercise capacity and excessive lung inflation caused by pulmonary edema, which may lead to decreased lung function and may be linked to the development of COPD.28,29 Additionally, CVD can reduce the lung tissue available for gas exchange, leading to ventilation-perfusion mismatch, which is an important cause of acute exacerbation of COPD, hospitalizations, and even death.30 In addition, COPD is an independent risk factor for CVD, possibly related to the fact that COPD can cause microvascular inflammation.31 A prospective study of patients undergoing microvascular evaluation showed a significant association with lung disease and smoking.32 Therefore, there may also be a connection between LC9 score and COPD. Our study has confirmed the close correlation between them and has described a linear decreasing relationship between LC9 scores and COPD diagnosis risk.
LC9 scores are derived from a comprehensive assessment of four health behavior factors (physical activity, tobacco, diet, and sleep) and five health factors (weight, cholesterol, blood glucose, blood pressure, and psychological health). These nine factors are closely related to the onset of COPD, thereby establishing the relationship between LC9 scores and COPD. It is well known that COPD is caused by exposure to harmful particles, especially tobacco smoke. Tobacco smoke causes airway inflammation, oxidative stress damage, and excessive activation of tissue remodeling, leading to the development of COPD.33,34 The relationship between dietary patterns and chronic diseases is a hot topic of research today, and several studies have shown that dietary patterns are strongly associated with COPD.35–37 Diet significantly affects an individual’s level of lung function and risk of COPD by influencing the oxidative and antioxidant balance and inflammatory state in the body.38 Physical activity and COPD mutually influence each other. Regular physical activity can improve symptoms of breathlessness, health status, and exercise tolerance in COPD patients.39 The level of physical activity can also predict the risk of hospitalization for acute exacerbation of COPD and all-cause mortality.40,41 However, COPD patients experience symptoms such as breathlessness and fatigue, leading to a decrease in physical activity levels early in the disease, which becomes more pronounced over time.42,43 Sleep has a significant impact on respiration and gas exchange. Sleep disorders may lead to changes in functional residual capacity as well as ventilation/perfusion disturbances.44,45 Underweight individuals have reduced muscle mass and an increased risk of respiratory infections, which are risk factors for the development of COPD.46,47 Hyperlipidemia induces inflammation in immune cells, while hyperglycemia causes mitochondrial damage leading to excessive production of reactive oxygen species (ROS) due to oxidative stress.48,49 Both conditions are characterized by insulin resistance and hyperinsulinemia, which can influence parasympathetic signaling to induce bronchial hyper-responsiveness and promote tissue fibrosis.50,51 Additionally, patients with hypertension have elevated levels of C-reactive protein (CRP), and the severity of COPD is associated with CRP levels in the body.52,53 Furthermore, psychological health is a focal point of concern in today’s society. Depression is associated with chronic stress, and patients with depression often have persistent activation of the sympathetic nervous system and increased systemic inflammatory responses, which may lead to the development of COPD.53 Moreover, patients with depression may experience increased frequency of COPD exacerbation due to cognitive impairment and poor treatment adherence.54
LC9 has the same factors as LS7 and LE8 but is richer, involving cardiopulmonary, endocrine metabolic, neurological, and psychological aspects to comprehensively assess the risk of developing COPD. Prior research has demonstrated a non-linear negative correlation between LE8 scores and COPD, where individuals with higher LE8 scores exhibited a significantly lower COPD diagnosis risk (OR 0.169, 95% CI (0.115, 0.249).55 Similarly, LS7 scores showed a positive correlation with lung function and a negative association with the odds of COPD.56 Mental health is closely linked to COPD risk and may serve as a potential etiological factor in COPD development.11 However, both the LE8 and LS7 scores lack assessment of mental health. The LC9 score addresses this gap by incorporating a depression symptom metric. Our study demonstrated a linearly decreasing association between LC9 scores and COPD. Compared to individuals with low LC9 scores, those with high LC9 scores exhibited an approximately 76% reduction in COPD diagnosis risk (OR 0.24, 95% CI (0.14, 0.39)). Our findings demonstrate distinct differences compared to previous studies.55,56 Notably, subgroup analyses revealed a significant interaction effect of educational attainment on the relationship between LC9 and COPD diagnosis. Specifically, among individuals with high school education, no inverse dose-response relationship was observed between LC9 scores and COPD diagnosis risk (P for trend = 0.46), suggesting that mental health metrics integrated into LC9 may differentially impact COPD screening efficacy in this population. Previous studies have shown that there is an interaction between education, mental health, and COPD.11,12,57–59 the prevalence of both COPD and depressive symptoms is lower in those with higher levels of education than in those with lower levels of education.57,59 And there is also an impact of mental health on COPD. Studies have shown that depressive symptoms may be a cause of COPD, and COPD is also prone to comorbid depressive symptoms.11,58 Therefore, the LC9 score provides a more comprehensive assessment of the relationship between CVH status and COPD. Our study found that good CVH status reduces COPD diagnosis risk.
Our study is the first to explore the relationship between LC9 scores and COPD diagnosis based on the NHANES database, which is nationally representative. Inevitably, this study also has some limitations. First, the calculation of the LC9 score includes items based on self-reported data, which may introduce recall bias and self-reporting bias. Second, our study is a cross-sectional survey, and therefore it cannot establish a causal relationship or temporal sequence between the two variables. Third, the participants in our study were over 40 years of age and the results cannot be extrapolated to those under 40 years of age. Excluding younger individuals may overlook the long-term effects of earlier exposures (eg, chronic smoking, air pollution, and occupational exposures) on lung function and COPD development, making it possible that the results may not fully reflect the role of risk factors at younger ages. Although exclusion of persons younger than 40 years of age may improve the focus and statistical power of the study, it may also limit the applicability and generalizability of the results to younger populations. Future studies may need to balance these issues in their design to ensure that the results more fully serve the public health needs of different age groups. Fourth, the determination of COPD is not exactly the gold standard in the GOLD guidelines, which may lead to biased results. However, pulmonary function tests for COPD screening can have false negatives, and some participants may be unable to complete the tests due to severe pulmonary function impairment.60 To identify COPD as accurately as possible and avoid its associated harms, we adopted the criteria used in this study. These criteria are widely used in many NHANES-related studies, making their adoption reasonable.15–17 Additionally, not all three components of these criteria are assessed every year in the NHANES program, so we cannot provide the frequency of cross-verification for all three components.
Conclusion
There was a linear decreasing relationship between the LC9 score and COPD diagnosis risk in middle-aged and older adults. The LC9 score is simple and easy to obtain, providing a more comprehensive assessment of the participants compared to the LS7 and LE8 scores. This makes it more accurate in reflecting the association.
Abbreviations
LS7, Life’s Simple 7; AHA, American Heart Association; CVH, cardiovascular health; LE8, Life’s Essential 8; LC9, Life’s Crucial 9; COPD, Chronic Obstructive Pulmonary Disease; NHANES, National Health and Nutrition Examination Survey; PIR, poverty income ratio; OR, odds ratios; CI, confidence intervals; CVD, cardiovascular diseases; ROS, reactive oxygen species; CRP, C-reactive protein.
Data Sharing Statement
The dataset for this study can be found on the NHANES website NHANES - National Health and Nutrition Examination Survey Homepage (cdc.gov). And we have provided that portion of the data in the Supplementary File 1.
Ethics Approval
This study was based on the NHANES database, a publicly available anonymized database, and therefore was not required to comply with ethical norms. All participants in this database have signed informed consent forms provided by the NHANES Ethics Review Board. Meanwhile, we also obtained a waiver from Zigong First People’s Hospital for the study (Ethics no. M2025-031).
Consent for Publication
Not applicable.
Acknowledgments
The authors would like to thank all the staff of the NHANES for their contributions to the Human Health and Nutrition Status Research Program.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article. All authors approved the manuscript. All authors have agreed to submit this manuscript to the International Journal of Chronic Obstructive Pulmonary Disease and take full responsibility for all aspects of the work.
Funding
This study was supported by the Zigong Science and Technology Bureau (grant no. 2023YLWS21 and 2023YKY07).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. All authors approved the present submitted version and their institutions have no objections to the manuscript’s contents.
References
1. Lloyd-Jones DM, Hong Y, Labarthe D. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American heart association’s strategic impact goal through 2020 and beyond. Circulation. 2010;121(4):586–613. doi:10.1161/circulationaha.109.192703
2. Lloyd-Jones DM, Allen NB, Anderson CAM. Life’s essential 8: updating and enhancing the American heart association’s construct of cardiovascular health: a presidential advisory from the American heart association. Circulation. 2022;146(5):e18–e43. doi:10.1161/cir.0000000000001078
3. Gaffey AE, Rollman BL, Burg MM. Strengthening the pillars of cardiovascular health: psychological health is a crucial component. Circulation. 2024;149(9):641–643. doi:10.1161/circulationaha.123.066132
4. Tang Y, Dong W, Shen J, et al. Life’s essential 8 and osteoporosis in adults aged 50 years or older: data from the national health and nutrition examination survey. Arch Osteoporos. 2024;19(1):13. doi:10.1007/s11657-024-01368-5
5. Chen X, Sun J, Zeng C, et al. Association between life’s essential 8 and periodontitis: a population-based study. BMC Oral Health. 2024;24(1):19. doi:10.1186/s12903-023-03816-z
6. Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis Management and Prevention of Chronic Obstructive Pulmonary Disease. (2025 report)[EBOL]. 1.2025 GOLD Report - Global Initiative for Chronic Obstructive Lung Disease - GOLD. 2025
7. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e93. doi:10.1016/s2214-109x(23)00217-6
8. Kessler RC, Sampson NA, Berglund P. Anxious and non-anxious major depressive disorder in the world health organization world mental health surveys. Epidemiol Psychiatr Sci. 2015;24(3):210–226. doi:10.1017/s2045796015000189
9. Abdoli N, Salari N, Darvishi N, et al. The global prevalence of major depressive disorder (Mdd) among the elderly: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2022;132:1067–1073. doi:10.1016/j.neubiorev.2021.10.041
10. O’Leary K. Global increase in depression and anxiety. Nat Med. 2021. doi:10.1038/d41591-021-00064-y
11. Ran B, Zhang Y, Wu Y, Wen F. Association between depression and COPD: results from the nhanes 2013-2018 and a bidirectional Mendelian randomization analysis. Expert Rev Respir Med. 2023;17(11):1061–1068. doi:10.1080/17476348.2023.2282022
12. Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345–349. doi:10.1183/09059180.00007813
13. Agusti A, Soriano JB. COPD as a systemic disease. COPD. 2008;5(2):133–138. doi:10.1080/15412550801941349
14. Li C, Li Y, Zhao M, Zhang C, Bovet P, Xi B. Using the new “life’s essential 8” metrics to evaluate trends in cardiovascular health among Us adults from 2005 to 2018: analysis of serial cross-sectional studies. JMIR Public Health Surveill. 2023;9:e45521. doi:10.2196/45521
15. Fei Q, Weng X, Liu K, et al. The relationship between metal exposure and chronic obstructive pulmonary disease in the general Us population: nhanes 2015-2016. Int J Environ Res Public Health. 2022;19(4). doi:10.3390/ijerph19042085
16. Han L, Wang Q. Associations of brominated flame retardants exposure with chronic obstructive pulmonary disease: a Us population-based cross-sectional analysis. Front Public Health. 2023;11:1138811. doi:10.3389/fpubh.2023.1138811
17. Zheng D, Liu X, Zeng W, Zhou W, Zhou C. Association of hepatic steatosis and liver fibrosis with chronic obstructive pulmonary disease among adults. Sci Rep. 2024;14(1):10822. doi:10.1038/s41598-024-61696-x
18. Yan Z, Xu Y, Li K, Liu L. Heavy metal levels and flavonoid intakes are associated with chronic obstructive pulmonary disease: an NHANES analysis (2007-2010 to 2017-2018). BMC Public Health. 2023;23(1):2335. doi:10.1186/s12889-023-17250-x
19. Zhang Z, Jackson SL, Gillespie C, Merritt R, Yang Q. Depressive symptoms and mortality among US adults. JAMA Network Open. 2023;6(10):e2337011. doi:10.1001/jamanetworkopen.2023.37011
20. Ge J, Peng W, Lu J. Predictive value of life’s crucial 9 for cardiovascular and all-cause mortality: a prospective cohort study from the NHANES 2007 to 2018. J Am Heart Assoc. 2024;13(20):e036669. doi:10.1161/jaha.124.036669
21. Li XR, Liu HL, Wang L, et al. Association between life’s crucial 9 and kidney stones: a population-based study. Front Med. 2025;12:1558628. doi:10.3389/fmed.2025.1558628
22. Wang X, Yan X, Zhang J, et al. Associations of healthy eating patterns with biological aging: national health and nutrition examination survey 1999-2018. Nutr J. 2024;23(1):112. doi:10.1186/s12937-024-01017-0
23. Zhang F, Hou X. Association between the triglyceride glucose index and heart failure: NHANES 2007-2018. Front Endocrinol. 2023;14:1322445. doi:10.3389/fendo.2023.1322445
24. Liu S, Ben X, Liang H. Association of acrylamide hemoglobin biomarkers with chronic obstructive pulmonary disease in the general population in the US: NHANES 2013-2016. Food Funct. 2021;12(24):12765–12773. doi:10.1039/d1fo02612g
25. Wu M, Si J, Liu Y, Kang L, Xu B. Association between composite dietary antioxidant index and hypertension: insights from NHANES. Clin Exp Hypertens. 2023;45(1):2233712. doi:10.1080/10641963.2023.2233712
26. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):180057. doi:10.1183/16000617.0057-2018
27. Linden F, Domschke G, Erbel C, Akhavanpoor M, Katus HA, Gleissner CA. Inflammatory therapeutic targets in coronary atherosclerosis-from molecular biology to clinical application. Front Physiol. 2014;5:455. doi:10.3389/fphys.2014.00455
28. Poole DC, Richardson RS, Haykowsky MJ, Hirai DM, Musch TI. Exercise limitations in heart failure with reduced and preserved ejection fraction. J Appl Physiol. 2018;124(1):208–224. doi:10.1152/japplphysiol.00747.2017
29. Ponikowski P, Voors AA, Anker SD. Esc guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (Esc)developed with the special contribution of the heart failure association (Hfa) of the Esc. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
30. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. doi:10.1183/09031936.00012408
31. Zagaceta J, Bastarrika G, Zulueta JJ. Prospective comparison of non-invasive risk markers of major cardiovascular events in COPD patients. Respir Res. 2017;18(1):175. doi:10.1186/s12931-017-0658-y
32. Freund O, Shetrit A, Bar-Shai A. Smoking and respiratory diseases in patients with coronary microvascular dysfunction. Am J Med. 2024;137(6):538–44.e1. doi:10.1016/j.amjmed.2024.02.034
33. Upadhyay P, Wu CW, Pham A, et al. Animal models and mechanisms of tobacco smoke-induced chronic obstructive pulmonary disease (COPD). J Toxicol Environ Health B Crit Rev. 2023;26(5):275–305. doi:10.1080/10937404.2023.2208886
34. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
35. Wen J, Gu S, Wang X, Qi X. Associations of adherence to the dash diet and the Mediterranean diet with chronic obstructive pulmonary disease among US adults. Front Nutr. 2023;10:1031071. doi:10.3389/fnut.2023.1031071
36. Møgelberg N, Tobberup R, Møller G, Godtfredsen NS, Nørgaard A, Andersen JR. High-protein diet during pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Dan Med J. 2022;69(11):1.
37. Ghosn B, Onvani S, Ardestani ME, Feizi A, Azadbakht L, Esmaillzadeh A. The association between diet quality and chronic obstructive pulmonary disease: a case-control study. BMC Public Health. 2023;23(1):2071. doi:10.1186/s12889-023-16586-8
38. Scoditti E, Massaro M, Garbarino S, Toraldo DM. Role of diet in chronic obstructive pulmonary disease prevention and treatment. Nutrients. 2019;11(6):1357. doi:10.3390/nu11061357
39. Demeyer H, Donaire-gonzalez D, Gimeno-santos E. Physical activity is associated with attenuated disease progression in chronic obstructive pulmonary disease. Med Sci Sports Exerc. 2019;51(5):833–840. doi:10.1249/mss.0000000000001859
40. Esteban C, Arostegui I, Aburto M, et al. Influence of changes in physical activity on frequency of hospitalization in chronic obstructive pulmonary disease. Respirology. 2014;19(3):330–338. doi:10.1111/resp.12239
41. Vaes AW, Garcia-Aymerich J, Marott JL. Changes in physical activity and all-cause mortality in COPD. Eur Respir J. 2014;44(5):1199–1209. doi:10.1183/09031936.00023214
42. Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005–1011. doi:10.1016/j.rmed.2010.01.012
43. Sievi NA, Brack T, Brutsche MH, et al. Physical activity declines in COPD while exercise capacity remains stable: a longitudinal study over 5 years. Respir Med. 2018;141:1–6. doi:10.1016/j.rmed.2018.06.013
44. newton K, Malik V, Lee-Chiong T. Sleep and breathing. Clin Chest Med. 2014;35(3):451–456. doi:10.1016/j.ccm.2014.06.001
45. Hudgel DW, Devadatta P. Decrease in functional residual capacity during sleep in normal humans. J Appl Physiol Respir Environ Exerc Physiol. 1984;57(5):1319–1322. doi:10.1152/jappl.1984.57.5.1319
46. Benz E, Trajanoska K, Lahousse L, et al. Sarcopenia in COPD: a systematic review and meta-analysis. Eur Respir Rev. 2019;28(154). doi:10.1183/16000617.0049-2019
47. Li J, Zhu L, Wei Y, et al. Association between adiposity measures and COPD risk in Chinese adults. Eur Respir J. 2020;55(4). doi:10.1183/13993003.01899-2019
48. Baffi CW, Wood L, Winnica D, et al. Metabolic Syndrome and the Lung. Chest. 2016;149(6):1525–1534. doi:10.1016/j.chest.2015.12.034
49. González P, Lozano P, Ros G, Solano F. Hyperglycemia and oxidative stress: an integral, updated and critical overview of their metabolic interconnections. Int J Mol Sci. 2023;24(11):9352. doi:10.3390/ijms24119352
50. Nie Z, Jacoby DB, Fryer AD. Hyperinsulinemia potentiates airway responsiveness to parasympathetic nerve stimulation in obese rats. Am J Respir Cell Mol Biol. 2014;51(2):251–261. doi:10.1165/rcmb.2013-0452OC
51. Lee H, Kim SR, Oh Y, Cho SH, Schleimer RP, Lee YC. Targeting insulin-like growth factor-i and insulin-like growth factor-binding protein-3 signaling pathways. A novel therapeutic approach for asthma. Am J Respir Cell Mol Biol. 2014;50(4):667–677. doi:10.1165/rcmb.2013-0397TR
52. Dodson PM, Shine B. Retinal vein occlusion: c-reactive protein and arterial hypertension. Acta Ophthalmol. 1984;62(1):123–130. doi:10.1111/j.1755-3768.1984.tb06765.x
53. Pinto-Plata VM, Müllerova H, Toso JF, et al. C-reactive protein in patients with COPD, control smokers and non-smokers. Thorax. 2006;61(1):23–28. doi:10.1136/thx.2005.042200
54. Martínez-Gestoso S, García-Sanz M-T, Carreira J-M. Impact of anxiety and depression on the prognosis of COPD exacerbations. BMC Pulm Med. 2022;22(1):169. doi:10.1186/s12890-022-01934-y
55. Liu Y, Li W, Tang J, Gao S. Association of life’s essential 8 with chronic obstructive pulmonary disease: a population-based analysis of NHANES 2007-2018. BMC Public Health. 2024;24(1):3144. doi:10.1186/s12889-024-20534-5
56. Fan W, Lee H, Lee A, Kieu C, Wong ND. Association of Lung function and chronic obstructive pulmonary disease with American heart association’s life’s simple 7 cardiovascular health metrics. Respir Med. 2017;131:85–93. doi:10.1016/j.rmed.2017.08.001
57. Li L, Sun W, Luo J, Huang H. Associations between education levels and prevalence of depressive symptoms: NHANES (2005-2018). J Affect Disord. 2022;301:360–367. doi:10.1016/j.jad.2022.01.010
58. Hetlevik Ø, Melbye H, Gjesdal S. Gp utilisation by education level among adults with COPD or asthma: a cross-sectional register-based study. NPJ Prim Care Respir Med. 2016;26:16027. doi:10.1038/npjpcrm.2016.27
59. Lutter JI, Jörres RA, Welte T. Impact of education on COPD severity and all-cause mortality in lifetime never-smokers and longtime ex-smokers: results of the cosyconet cohort. Int J Chron Obstruct Pulmon Dis. 2020;15:2787–2798. doi:10.2147/COPD.S273839
60. Maldonado-Franco A, Giraldo-Cadavid LF, Tuta-Quintero E, Bastidas Goyes AR, Botero-Rosas DA. The challenges of spirometric diagnosis of COPD. Can Respir J. 2023;2023:6991493. doi:10.1155/2023/6991493
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.