Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Levetiracetam is associated with decrease in subclinical epileptiform discharges and improved cognitive functions in pediatric patients with autism spectrum disorder
Authors Wang MJ, Jiang L, Tang XJ
Received 14 June 2017
Accepted for publication 4 August 2017
Published 31 August 2017 Volume 2017:13 Pages 2321—2326
DOI https://doi.org/10.2147/NDT.S143966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Minjian Wang,1–4 Li Jiang,2–5 Xiaoju Tang5
1Department of Psychology, 2Ministry of Education Key Laboratory of Child Development and Disorders, 3Key Laboratory of Pediatrics in Chongqing, 4Chongqing International Science and Technology Cooperation Center for Child Development and Disorders, 5Department of Neurology, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Objective: Subclinical epileptiform discharges (SEDs) are common in pediatric patients with autism spectrum disorder (ASD), but the effect of antiepileptic drugs on SEDs in ASD remains inconclusive. This physician-blinded, prospective, randomized controlled trial investigated an association between the anticonvulsant drug levetiracetam and SEDs in children with ASD.
Methods: A total of 70 children with ASD (4–6 years) and SEDs identified by electroencephalogram were randomly divided into two equal groups to receive either levetiracetam and educational training (treatment group) or educational training only (control). At baseline and after 6 months treatment, the following scales were used to assess each individual’s behavioral and cognitive functions: the Chinese version of the Psychoeducational Profile – third edition (PEP-3), Childhood Autism Rating Scale (CARS), and Autism Behavior Checklist (ABC). A 24-hour electroencephalogram was recorded on admission (baseline) and at follow-up. The degree of satisfaction of each patient was also evaluated.
Results: Relative to baseline, at the 6-month follow-up, the PEP-3, CARS, and ABC scores were significantly improved in both the treatment and control groups. At the 6-month follow-up, the PEP-3 scores of the treatment group were significantly higher than those of the control, whereas the CARS and ABC scores were significantly lower, and the rate of electroencephalographic normalization was significantly higher in the treatment group.
Conclusion: Levetiracetam appears to be effective for controlling SEDs in pediatric patients with ASD and was also associated with improved behavioral and cognitive functions.
Keywords: autism spectrum disorder, subclinical epileptiform discharges, levetiracetam, behavioral function, cognitive function, randomized controlled trial
Introduction
Autism spectrum disorder (ASD) is a common neurodevelopmental disability that is characterized by impaired social communication and interaction, restricted interests, repetitive and stereotyped behaviors, and abnormal sensory response.1–3 Early onset of ASD is detectable in children aged 12 to 18 months. As awareness of this disease has improved, the rates of early recognition and diagnosis have significantly increased.4,5
ASD is also associated with epilepsy and epileptiform discharges on electroencephalogram (EEG). Approximately one-third of children with ASD develop epilepsy, although the definitive prevalence is inconclusive because the data have varied considerably.6 Subclinical epileptiform discharges (SEDs) are commonly detected on EEG in 4%–61% of patients without clinical seizures, depending on the method of sampling.6 Clinical evidence indicates that in children with ASD, SEDs may be associated with impaired cognitive and behavioral functions,7,8 and suppressing SEDs in these patients may lessen the symptoms of ASD and improve social functions.9,10 Recently, antiepileptic drugs have been investigated for managing SEDs in children with ASD, but the efficacy of such treatment remains controversial.11
Levetiracetam is an anticonvulsant agent used to treat epilepsy. It may selectively prevent hypersynchronization of epileptiform burst firing and propagation of seizure activity by binding to synaptic vesicle glycoprotein 2A (SV2A) protein. Levetiracetam is considered to regulate the release of neurotransmitters and impulse conduction across synapses.12,13 Previous clinical studies have suggested that levetiracetam modulates EEG background frequency and improves cognitive functions in patients with epilepsy.14 Nevertheless, there are also studies that have associated levetiracetam with negative results for managing ASD patients.15–17
This study investigated the efficacy of levetiracetam for controlling SEDs in children with ASD and an association between levetiracetam treatment and changes in cognitive and behavioral functions.
Methods
The institutional review board and ethics committee of Children’s Hospital of Chongqing Medical University approved this physician-blinded prospective randomized controlled trial. All guardians of the children provided written informed consent.
Patients
The study population consisted of 70 consecutive pediatric inpatients of Children’s Hospital of Chongqing Medical University between January 2014 and May 2016. Pediatric psychiatrists conducted all the diagnoses of ASD using the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).1 Patients with any of the following were excluded from the study: disorders of mental development, comprehensive developmental delays, cerebral palsy, or previous history of epileptic seizures. Epileptiform discharges were identified on a 24-hour EEG, and the results were reassessed by two pediatric neurologists independently.
Grouping and treatment
The 70 patients were randomly and equally apportioned to either a treatment or control group using a random number table. The treatment group (n=35) received levetiracetam and educational training. The control group (n=35) received educational training only. The physician-investigators were blinded to the study group assignment.
Patients in the treatment group were given levetiracetam at a dosage of 60 mg/kg/day; plasma concentrations of levetiracetam were measured at 1 and 6 months after the beginning of treatment. The educational training included the Treatment and Education of Autistic and Communication Handicapped Children program, verbal behavior training, the Relationship Development Intervention program, and the Developmental, Individual-Differences, Relationship-Based (DIR/Floortime) model. Follow-up data were obtained by telephone interviews. No other antipsychotic medications were used during the study period.
Psychological assessment
Before treatment (baseline) and at the 6-month follow-up, individual behavioral and cognitive functions were assessed using the following: Psychoeducational Profile – third edition (PEP-3; Chinese version), Childhood Autism Rating Scale (CARS), and Autism Behavior Checklist (ABC). The PEP-3 scale that was used to assess children’s language levels in this study was the revised Chinese version adopted in Hong Kong.18 The sections that are closely related to the development of cognitive function were used, including the cognitive verbal/preverbal (CVP) function, expressive language, and receptive language. The communication composite score combined the CVP, expressive language, and receptive language raw scores. The physical and behavioral sections of the PEP-3 scale were not included in this study. The PEP-3 tests were performed by a staff who was trained and qualified for special education assessment.
The CARS is a reliable scoring system for diagnosing ASD and evaluating its severity; a score ≥30 points supports a diagnosis of ASD.19,20 CARS scores were evaluated by pediatric psychiatrists.
The ABC scale21 was recorded by caregivers. The 57 items regarding behavioral functions were organized into five groups: social and self-help, language, body and object use, sensory, and relating. A score ≥67 points supports a diagnosis of ASD. ABC examinations were finished by individual parents under the guidance of pediatric psychiatrists.
EEG and satisfaction investigation
A 24-hour EEG was recorded on admission and during the follow-up, and the results were reassessed independently by two neurologists blinded to the study group. The guardians’ satisfaction was investigated using a 10-point questionnaire (poor, 1–4; fair, 5–7; good, 8–10).
Statistical analysis
All statistical analyses were performed using SPSS software (version 23.0; IBM Corporation, Armonk, NY, USA). Data are expressed as mean ± standard deviation. The variables in the two groups were compared using the chi-squared test or Student’s t-test. A P-value <0.05 was considered as statistically significant.
Results
Demographic characteristics
In the treatment group, three children were withdrawn from the study since they did not take levetiracetam as required, and thus, a total of 32 patients were included (Table 1). There were no significant differences in the male-to-female ratios or the average ages of the treatment and control groups (P>0.05).
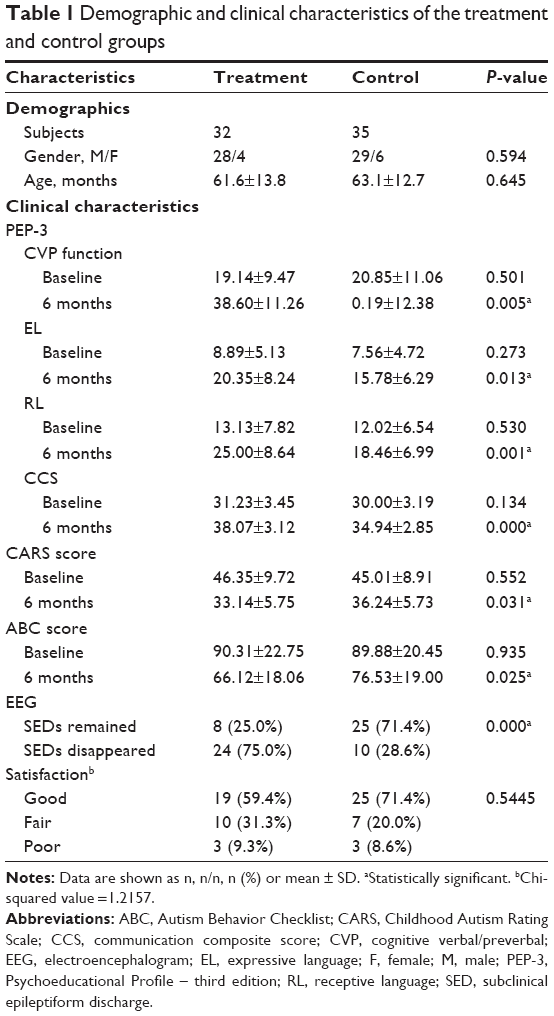 | Table 1 Demographic and clinical characteristics of the treatment and control groups |
Levetiracetam treatment and adverse effects
The average plasma levetiracetam concentrations at 1 and 6 months after treatment were 30.9 and 34.4 μg/mL, respectively. During the treatment, one child developed fatigue and somnolence during titration and one child exhibited irritability. These symptoms were relieved after the dosage of levetiracetam was reduced. One child experienced anorexia, which resolved spontaneously. Laboratory examinations (including complete blood count, urinalysis, electrocardiogram, and hepatorenal functions) showed no significant abnormality before or after the treatment.
PEP-3 evaluation
The baseline PEP-3 scores of the treatment and control groups were statistically comparable (P>0.05; Table 1). In each group, the following scores at the 6-month follow-up were significantly higher compared with the corresponding baseline scores: CVP, expressive language, receptive language, and communication composite score (P<0.05). However, these 6-month follow-up scores were all significantly higher in the treatment group compared with the control (P<0.05).
CARS assessment
Prior to the start of treatment, the baseline CARS scores of the treatment and control groups were statistically similar (P>0.05; Table 1). In each group, the CARS scores at the 6-month follow-up were significantly lower than the corresponding baseline scores (P<0.05), but the 6-month CARS scores of the treatment group were significantly lower than those of the control group (P<0.05).
ABC evaluation
Before the treatment, the baseline ABC scores of the treatment and control groups were not significantly different (P>0.05; Table 1). In each group, the ABC scores at the 6-month follow-up were significantly lower than the corresponding baseline levels (P<0.05). The 6-month ABC scores of the treatment group were significantly lower than those of the control group (P<0.05).
EEG examination and individual satisfaction
Before the treatment, SEDs were identified in each patient (Table 1). At the 6-month follow-up, SEDs were absent in 24 of the 32 patients (75.0%) in the treatment group and 5 of the 35 patients (14.3%) in the control group. The chi-squared test showed a significant difference in the electroencephalographic normalization rate of the two groups (P<0.05). There was no significant difference in individual satisfaction between the two groups (P>0.05).
Discussion
Autism was originally described by Kanner in 1943,22 and the umbrella term “autism spectrum disorder (ASD)” was introduced in the DSM-5 to define a continuum of autistic symptoms. In recent years, extensive studies have documented the clinical manifestation, etiology, and treatment of ASD.21,23,24 The core symptoms of ASD include deficits in social communication and interaction and restricted or repetitive patterns of behavior, interests, or activities; in addition, pediatric patients with ASD may also have concurrent intellectual and/or language deficiencies and/or comorbid diseases (such as epilepsy).25 Although there has been no specific treatment for ASD, a diverse range of psychosocial, behavioral, and educational interventions have been attempted to alleviate various core symptoms of ASD.26,27 Seida et al27 performed an umbrella systematic review of psychosocial interventions for ASD and proposed that some forms of psychosocial interventions were associated with positive outcomes. This indicated that these treatments may be favorable compared with no treatment. Nevertheless, they also emphasized that there was little evidence for the relative effectiveness of these psychosocial interventions.27 Subsequently, some scholars conducted systematic reviews of psychosocial interventions for patients with ASD and found that the effects of psychosocial treatment in adult ASD were largely positive.26,28,29 However, the quantity and quality of these studies have been limited. Further high-quality randomized controlled trials are warranted to evaluate the definitive effectiveness of psychosocial treatment for ASD. Moreover, the current psychosocial intervention approaches all target the core symptoms and behavioral disorders of ASD but provide no benefit for comorbid diseases such as epilepsy.
Epilepsy and epileptiform EEGs are closely associated with ASD. As previously reported, ASD patients had a high rate of developing epilepsy with an estimated prevalence ranging from 5% to 46%. The rate of ASD is also high in epilepsy populations, with as much as 32% meeting the diagnostic criteria.6 Extensive studies have noted that SEDs are commonly detected in patients with ASD.6,30 Some scholars assumed that SEDs in childhood can cause behavioral or cognitive deterioration by disturbing the formation of synapses.7 As early as 1993, Binnie10 noted that the presence of SEDs was associated with impaired behavioral and cognitive functions in children. Kanemura et al31 after long-term observation found that ASD children with SEDs can develop epileptic seizures. Hollander et al9 performed an open trial and found that divalproex sodium can suppress EEG abnormalities, alleviate ASD symptoms, and improve individual social functions.
However, it is not known whether levetiracetam may control SEDs or improve the behavioral and cognitive functions of patients with ASD. In the current study, we demonstrated that levetiracetam, combined with educational intervention, can effectively control SEDs and improve the behavioral and cognitive functions of children with ASD. After a 6-month treatment period, both the treatment and control groups showed significant improvements in their behavioral and cognitive functions, confirmed by the cognitive evaluation scales PEP-3, CARS, and ABC. Moreover, functional improvement in the treatment group was much more remarkable than in the control, which suggests that levetiracetam can facilitate cognitive rehabilitation. In previous studies, Rugino and Samsock32 also noted consistent results that indicated the nootropic bioactivity of levetiracetam.
According to the EEG examination results, after 6 months of treatment, SEDs were significantly better controlled in the treatment group compared with the control, evidenced by a remarkably higher electroencephalographic normalization rate. This suggests that levetiracetam may be an effective agent for controlling SEDs in patients with ASD. A previous study has reported safe and effective dosages of levetiracetam ranging from 70 to 275 mg/kg/day (mean 146 mg/kg/day).33 Because of individual differences in response to antiepileptic drugs, underlying developmental defects, and electroencephalographic patterns, individualized levetiracetam regimens are recommended.15 In the present study, the association between electroencephalographic normalization rate and improvements in behavioral and cognitive functions warrants much longer follow-up studies involving a larger sample size.
Based on the present findings, we speculate that early use of antiepileptic drugs can help suppress SEDs and further improve behavioral, cognitive, and language skills in children with ASD. According to previous studies, antiepileptic drugs such as sodium valproate, levetiracetam, lamotrigine, and others ameliorate significantly the clinical symptoms of SEDs that accompany ASD and also help control irritability, impulsiveness, and other emotional symptoms. Chez et al23 found that the prevalence of SEDs in patients with ASD was ~60.7%. Among 176 ASD patients with SEDs, 80 experienced electroencephalographic normalization after administration of sodium valproate and 30 showed significant clinical improvement. In a meta-analysis of seven relevant studies, Hirota et al34 found that SEDs were frequently detected in children with ASD. However, antiepileptic drugs seemed to be ineffective for improving the clinical symptoms of ASD. These results require further verification due to the limited sample size.
The efficacy of antiepileptic drugs for improving behavioral symptoms of ASD (eg, irritability and compulsivity) is also controversial. Hollander et al24,35 found that sodium valproate can effectively ameliorate impulsive and irritable behaviors. However, Hellings et al36 reported that the effect of sodium valproate was similar to a placebo for controlling aggressive behaviors. In the current study, we found that levetiracetam treatment was associated with an improvement in behavioral defects in children with ASD.
Levetiracetam is not generally considered to be a mood stabilizer. Studies regarding the administration of levetiracetam and evaluation of behavioral and cognitive functions in pediatric patients with ASD are sparse. Rugino and Samsock32 followed 10 ASD patients (aged 4–10 years) and reported that a 4-week treatment with levetiracetam effectively reduced symptoms of hyperactivity, impulsivity, emotional instability, and regression, but there were no significant nootropic effects.
In addition, some scholars have observed negative results when managing ASD patients with antiepileptic drugs. Wasserman et al17 administered levetiracetam for 10 weeks to 20 ASD children (aged 5–17 years), and no improvement in behavioral abnormalities was noted. Rajapakse and Pringsheim16 found that levetiracetam was ineffective for controlling stereotyped movements in patients with ASD. Moreover, Camacho et al15 even reported a 6-year-old girl who developed stereotypies and severely deteriorated social and communicative dysfunction after administration of levetiracetam, suggesting that levetiracetam may provoke unusual behavioral adverse effects. In the current study, we did not note significant levetiracetam-related complications or cognitive deterioration. However, a conclusion regarding the definitive safety of long-term use of levetiracetam still requires much longer observation.
Conclusion
In this physician-blinded, prospective, randomized controlled trial, we found that levetiracetam is a safe and effective agent for controlling SEDs in pediatric patients with ASD and may improve behavioral and cognitive functions. We recommend a dosage of 60 mg/kg/day and a therapeutic course of 6 months.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association, DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association; 2013. | ||
Harstad EB, Fogler J, Sideridis G, Weas S, Mauras C, Barbaresi WJ. Comparing diagnostic outcomes of autism spectrum disorder using DSM-IV-TR and DSM-5 criteria. J Autism Dev Disord. 2015;45(5):1437–1450. | ||
Levy F. Child and adolescent changes to DSM-5. Asian J Psychiatr. 2014;11:87–92. | ||
Monteiro SA, Dempsey J, Broton S, Berry L, Goin-Kochel RP, Voigt RG. Early intervention before autism diagnosis in children referred to a regional autism clinic. J Dev Behav Pediatr. 2016;37(1):15–19. | ||
Fernell E, Eriksson MA, Gillberg C. Early diagnosis of autism and impact on prognosis: a narrative review. Clin Epidemiol. 2013;5:33–43. | ||
Spence SJ, Schneider MT. The role of epilepsy and epileptiform EEGs in autism spectrum disorders. Pediatr Res. 2009;65(6):599–606. | ||
Nicolai J, Aldenkamp AP, Arends J, Weber JW, Vles JS. Cognitive and behavioral effects of nocturnal epileptiform discharges in children with benign childhood epilepsy with centrotemporal spikes. Epilepsy Behav. 2006;8(1):56–70. | ||
Kavros PM, Clarke T, Strug LJ, Halperin JM, Dorta NJ, Pal DK. Attention impairment in rolandic epilepsy: systematic review. Epilepsia. 2008;49(9):1570–1580. | ||
Hollander E, Dolgoff-Kaspar R, Cartwright C, Rawitt R, Novotny S. An open trial of divalproex sodium in autism spectrum disorders. J Clin Psychiatry. 2001;62(7):530–534. | ||
Binnie CD. Significance and management of transitory cognitive impairment due to subclinical EEG discharges in children. Brain Dev. 1993;15(1):23–30. | ||
Hartley-McAndrew M, Weinstock A. Autism spectrum disorder: correlation between aberrant behaviors, EEG abnormalities and seizures. Neurol Int. 2010;2(1):e10. | ||
Lynch BA, Lambeng N, Nocka K, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci U S A. 2004;101(26):9861–9866. | ||
Kaminski RM, Matagne A, Leclercq K, et al. SV2A protein is a broad-spectrum anticonvulsant target: functional correlation between protein binding and seizure protection in models of both partial and generalized epilepsy. Neuropharmacology. 2008;54(4):715–720. | ||
Cho JR, Koo DL, Joo EY, et al. Effect of levetiracetam monotherapy on background EEG activity and cognition in drug-naive epilepsy patients. Clin Neurophysiol. 2012;123(5):883–891. | ||
Camacho A, Espin JC, Nunez N, Simon R. Levetiracetam-induced reversible autistic regression. Pediatr Neurol. 2012;47(1):65–67. | ||
Rajapakse T, Pringsheim T. Pharmacotherapeutics of Tourette syndrome and stereotypies in autism. Semin Pediatr Neurol. 2010;17(4): 254–260. | ||
Wasserman S, Iyengar R, Chaplin WF, et al. Levetiracetam versus placebo in childhood and adolescent autism: a double-blind placebo-controlled study. Int Clin Psychopharmacol. 2006;21(6):363–367. | ||
Chen KL, Chiang FM, Tseng MH, Fu CP, Hsieh CL. Responsiveness of the psychoeducational profile-third edition for children with autism spectrum disorders. J Autism Dev Disord. 2011;41(12):1658–1664. | ||
Nah YH, Young RL, Brewer N. Using the autism detection in early childhood (ADEC) and Childhood Autism Rating Scales (CARS) to predict long term outcomes in children with autism spectrum disorders. J Autism Dev Disord. 2014;44(9):2301–2310. | ||
Kurita H, Miyake Y, Katsuno K. Reliability and validity of the Childhood Autism Rating Scale – Tokyo version (CARS-TV). J Autism Dev Disord. 1989;19(3):389–396. | ||
Eaves RC, Milner B. The criterion-related validity of the Childhood Autism Rating Scale and the autism behavior checklist. J Abnorm Child Psychol. 1993;21(5):481–491. | ||
Kanner L. Autistic disturbance of affective contact. Acta Paedopsychiatr. 1968;35(4):100–136. | ||
Chez MG, Chang M, Krasne V, Coughlan C, Kominsky M, Schwartz A. Frequency of epileptiform EEG abnormalities in a sequential screening of autistic patients with no known clinical epilepsy from 1996 to 2005. Epilepsy Behav. 2006;8(1):267–271. | ||
Hollander E, Soorya L, Wasserman S, Esposito K, Chaplin W, Anagnostou E. Divalproex sodium vs. placebo in the treatment of repetitive behaviours in autism spectrum disorder. Int J Neuropsychopharmacol. 2006;9(2):209–213. | ||
Christon LM, Arnold CC, Myers BJ. Professionals’ reported provision and recommendation of psychosocial interventions for youth with autism spectrum disorder. Behav Ther. 2015;46(1):68–82. | ||
Bishop-Fitzpatrick L, Minshew NJ, Eack SM. A systematic review of psychosocial interventions for adults with autism spectrum disorders. J Autism Dev Disord. 2013;43(3):687. | ||
Seida JK, Ospina MB, Karkhaneh M, Hartling L, Smith V, Clark B. Systematic reviews of psychosocial interventions for autism: an umbrella review. Dev Med Child Neurol. 2009;51(2):95. | ||
Kreslins A, Robertson AE, Melville C. The effectiveness of psychosocial interventions for anxiety in children and adolescents with autism spectrum disorder: a systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health. 2015;9(1):22. | ||
Parsons L, Cordier R, Munro N, Joosten A, Speyer R. A systematic review of pragmatic language interventions for children with autism spectrum disorder. PLoS One. 2017;12(4):e0172242. | ||
Baird G, Robinson RO, Boyd S, Charman T. Sleep electroencephalograms in young children with autism with and without regression. Dev Med Child Neurol. 2006;48(7):604–608. | ||
Kanemura H, Sano F, Tando T, Sugita K, Aihara M. Can EEG characteristics predict development of epilepsy in autistic children? Eur J Paediatr Neurol. 2013;17(3):232–237. | ||
Rugino TA, Samsock TC. Levetiracetam in autistic children: an open-label study. J Dev Behav Pediatr. 2002;23(4):225–230. | ||
Obeid M, Pong AW. Efficacy and tolerability of high oral doses of levetiracetam in children with epilepsy. Epilepsy Res. 2010;91(1):101–105. | ||
Hirota T, Veenstra-Vanderweele J, Hollander E, Kishi T. Antiepileptic medications in autism spectrum disorder: a systematic review and meta-analysis. J Autism Dev Disord. 2014;44(4):948–957. | ||
Hollander E, Chaplin W, Soorya L, et al. Divalproex sodium vs placebo for the treatment of irritability in children and adolescents with autism spectrum disorders. Neuropsychopharmacology. 2010;35(4):990–998. | ||
Hellings JA, Weckbaugh M, Nickel EJ, et al. A double-blind, placebo-controlled study of valproate for aggression in youth with pervasive developmental disorders. J Child Adolesc Psychopharmacol. 2005;15(4):682–692. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.