Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Levels of serum immunomodulators and alterations with electroconvulsive therapy in treatment-resistant major depression
Authors Zincir S, Öztürk PK, Bilgen AE, Izci F, Yükselir C
Received 18 February 2016
Accepted for publication 11 April 2016
Published 15 June 2016 Volume 2016:12 Pages 1389—1396
DOI https://doi.org/10.2147/NDT.S106652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Serkan Zincir,1 Pelin Öztürk,2 Ali Emrah Bilgen,3 Filiz İzci,4 Cihad Yükselir5
1Department of Psychiatry, Gölcük Military Hospital, Kocaeli, 2Psychiatry Clinic, Erenkoy Training and Research Hospital for Psychiatric and Neurological Diseases, Istanbul, 3Department of Psychiatry, Etimesgut Military Hospital, Ankara, 4Department of Psychiatry, Istanbul Bilim University, Istanbul, 5Department of Psychiatry, Gulhane Military Medical Faculty, Ankara, Turkey
Abstract: Studies in recent years have indicated that neuroimmunological events and immune activation may have a place in the etiology of depression. It has been suggested from data that there is a causal relationship between activation of the immune system and excessive release of proinflammatory cytokines, such as interleukin 1 (IL-1), IL-6, and tumor necrosis factor-alpha (TNF-alpha), and the etiology of depression. Although the mechanism of action of electroconvulsive therapy (ECT) is unclear, there is evidence that it can reduce cytokines and immune system changes. In our study, we aimed to determine how levels of serum immunomodulators were affected by ECT in major depression patients. This study was conducted on 50 patients with treatment-resistant major depression. The data of the patients were compared with 30 healthy individuals with similar demographic characteristics. A clinical response occurred in the patients and at the end of therapy, IL-1, IL-6, TNF-alpha, IL-10, IL-4, and interferon-gamma levels were measured. The disease severity was assessed with the 17-item Hamilton Depression Rating Scale. Data analysis was performed using SPSS Version 15. Significant differences were determined between the patients with major depression and control group with respect to basal serum IL-1, IL-6, TNF-alpha, IL-10, IL-4, and interferon-gamma levels. ECT treatment was shown to reduce these differences. ECT may cause significant changes in the activity of the immune system. The consideration of the relationship between the immune endocrine neurotransmitter systems could contribute to new theories regarding the mechanism of antidepressant treatment and biology of depression.
Keywords: the pathophysiology of depression, the immune system, cytokines
Introduction
Major depression is a chronic mood disorder, which may be seen frequently and repetitively, disrupting the quality of life and social cohesion of patients, and may even have serious consequences, such as suicide. It is estimated that by 2020, major depression will be accepted as the second most important cause of disability worldwide.1 Nevertheless, the etiology of major depression is still not clear.
The interactions and relationships of hormones, neurotransmitters, and peptides included in the immune system and the central nervous system have been examined in many studies.2–4 There is consensus that stress and depression have adverse effects on the immune system.5–7 The changes caused by stress on the immune system have been reported to vary depending on whether the stress is acute or chronic.8,9 Immune mediators appear to contribute to the pathophysiology of diseases, such as schizophrenia, depression, and dementia.10 Increased serum concentrations of the proinflammatory cytokines, interleukin 1 (IL-1) and IL-6, C-reactive protein (CRP), haptoglobin, and alpha-1 acid glycoprotein as acid phase reactants have been found in major depressive patients.11 Clinical trials have demonstrated that cytokines are associated with the development of depression. Interferon (IFN)-alpha therapy is used at high rates in cases of major depression.10,11 The source of immune activation in depression is unknown, although stress and cortisol-releasing hormone have been shown in previous studies to induce cytokines in the absence of a general immune response.
Astrocytes, microglia, and the triggering of peripheral immune cells result in the release of certain transmitters in these cells. They include cytokines, such as IL, IFN, and tumor necrosis factor (TNF). Other transmitters, such as nitric oxide, prostaglandins, and excitatory amino acids, are involved in this process.
Stress and inflammation (autoimmune diseases, allergic reactions, post-ischemic brain injury) are known to cause cytokine production.12–14 Depressive symptoms can be seen in illnesses with increased cytokines and because of psychiatric symptoms in immunosuppressed diseases, such as syphilis and systemic lupus erythematosus, it is thought that the immune system may play a role in the pathophysiology of depression. Psychiatric changes observed in hepatitis and cancer patients receiving immunotherapy support this view. IFN use in “sickness behavior” has been associated with emotional and behavioral changes.15 In studies involving depressed patients, proinflammatory cytokines (IL-1, IL-6, and TNF-alpha) and acute phase reactants have been reported to be increased.16,17 Electroconvulsive therapy (ECT) is a very effective method of treatment for treatment-resistant major depression, although the mechanism of action has not yet been fully understood. It has been suggested that it may be due to a complex network of neurotransmitters, neurohormones, and a neurotrophic system.18–22 Studies have shown that the adrenal (hypothalamic–pituitary–adrenal [HPA]) axis hormones, such as prolactin, adrenocorticotropin, arginine vasopressin, growth hormone, and neuropeptide Y, are changed by ECT.20–23 The effect of ECT on HPA axis has been widely studied. Although the findings of these studies have not always been consistent, after successful ECT treatment, it has been shown that the HPA axis has a role in supporting the mediation of the therapeutic effects of ECT. There is evidence showing that the immune system is involved in the pathogenesis of depression. In addition, antidepressants have immunomodulating properties and, vice versa, interventions that restore normal immune functioning can have antidepressant effects. It may be considered that immune pathways play a role in the mechanism of action of ECT.23,24
The aim of this study was to examine the effects on immune factors (IL-1, IL-4, IL-6, IL-10, TNF-alpha, and IFN-gamma) of ECT in treatment-resistant major depression patients. Comparisons were made with a control group prior to ECT, when a clinical response occurred, and at the end of the ECT treatment. Changes in immune factors and the relationship with the severity of depression were also investigated. The study was performed in order to examine the hypothesis that in depression, rising serum levels of proinflammatory cytokines would return to normal levels by ECT.
Participants and methods
Participants
ECT was applied to treatment-resistant major depression patients at Gulhane Military Medical Academy Psychiatry Department and a comparison was made with a healthy control group. The study included 50 patients diagnosed with treatment-resistant major depression (18 males, 32 females) and 30 healthy volunteers with no psychiatric or medical disorders (ten males, 20 females). The study was carried out with the approval of the Gulhane Military Medical Academy review boards.
The diagnosis was made with the Structured Clinical Interview for DSM-Axis 1 Disorders diagnostic criteria according to Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR). Disease severity and control group were evaluated with the 17-item Hamilton Depression Rating Scale (HAM-D). Control group that had a HAM-D score <7 was included. A form was completed before the study with the sociodemographic data of both the patients and the control group (age, education level, marital status, alcohol and substance use history, familial history of psychiatric illness in the family, physical or psychiatric illness, suicide attempts, antidepressants and psychotropic medication history, number of episodes, and duration of recent disease).
Resistance to therapy was considered as a lack of response to the appropriate dose and duration of antidepressant treatment of two different groups.25 To determine the effect of ECT only, no antidepressant or antipsychotic drugs were used during treatment. Written informed consent was obtained from all the study participants.
Exclusion criteria were those with comorbid axis I diagnoses (including bipolar depression), no history of organic illness, psychoactive substance use in the previous month, mental retardation, acute or chronic infections in the previous month, nonsteroidal anti-inflammatory drugs or psychotropic drug use in the previous 6 weeks, autoimmune, allergic, neoplastic, or endocrine disease which would constitute a risk for ECT, failure to respond to 12 sessions of ECT, and familial history of suicide or major depression (for the control group).
Application and sample collection
The necessary biochemical tests were applied and patients were evaluated in terms of risk of ECT. The HAM-D scale was applied at three different times: the day before starting ECT treatment (T0), the time of ECT clinical response (T1) (defined as ≥50% in HAM-D scale compared to the initial value), and the day after the end of ECT treatment (T2). Blood was taken for measurement of IFN-gamma, IL-1, IL-6, TNF-alpha, IL-10, and IL-4. Blood was collected only once from the control group for the IFN-gamma, IL-1, IL-6, TNF-alpha, IL-10, and IL-4 measurements.
ECT application
ECT was applied in the ECT room by a team of psychiatric nurses, anesthesia technicians, anesthesia specialist, and psychiatrist. All patients were administered propofol (0.75–1 mg/kg) and succinylcholine (1 mg/kg) intravenously for induction of anesthesia by an anesthesiologist. A bilateral–bitemporal method, Spectrum Mecta 5000 Q brand ECT device (MECTA Corporation, Tualatin, OR, USA) was used. Brief pulse, square wave type 550–800 mA (stimulus width 1–2 ms frequency of 40–90 Hz, duration 0.5–4 seconds, maximum charge 1,172 mC) was targeted to occur by giving seizures for at least 25 seconds. The total number of ECT sessions was between five and 12, applied at three times a week. The ECT could be reduced or increased depending on the patient’s clinical response.
IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma measurement
After 8–12 hours of fasting between 8 and 10 am, 5 mL blood samples were withdrawn from the antecubital vein of the patients and the control group. Blood was transferred to plain tubes without anticoagulants for the measurement of IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma. After storage at 4.0°C for 4 hours, the blood samples were centrifuged at 3,000 rpm for 15 minutes. Until the time of analysis, blood was stored at -80°C in Eppendorf tubes. Measurement of cytokines was performed by enzyme-linked immunosorbent assay method with Cyteelisa kits (RayBiotech Inc., Norcross, GA, USA).
Statistical methods
For data analysis, SPSS Version 15 (SPSS Inc., Chicago, IL, USA) was used. Continuous variables were expressed as mean ± standard deviation and discrete variables were expressed as number and percentage. Conformity to normal distribution of the continuous variables was examined with the Kolmogorov–Smirnov test. Differences between the groups in discrete variables were evaluated using Pearson’s chi-square test. The Kruskal–Wallis test was performed to compare multiple groups. When continuous variables did not show normal distribution, the Bonferroni corrected Mann–Whitney U-test was used for post hoc comparisons. The Student’s t-test was used for continuous variables with parametric conditions, and the Mann–Whitney U-test was used with nonparametric conditions. The paired-sample t-test was used for comparison of dependent groups and for evaluation of the correlation between variables, the Pearson’s correlation test was used. A value of P<0.05 was considered statistically significant.
Results
Sociodemographic characteristics
The study was conducted on 50 patients with treatment-resistant major depression. The data of the patient group were compared with the control group data. No statistically significant difference was determined between the groups with respect to age, sex, marital status, and education level.
The sociodemographic characteristics of the patient and control groups are presented in Table 1.
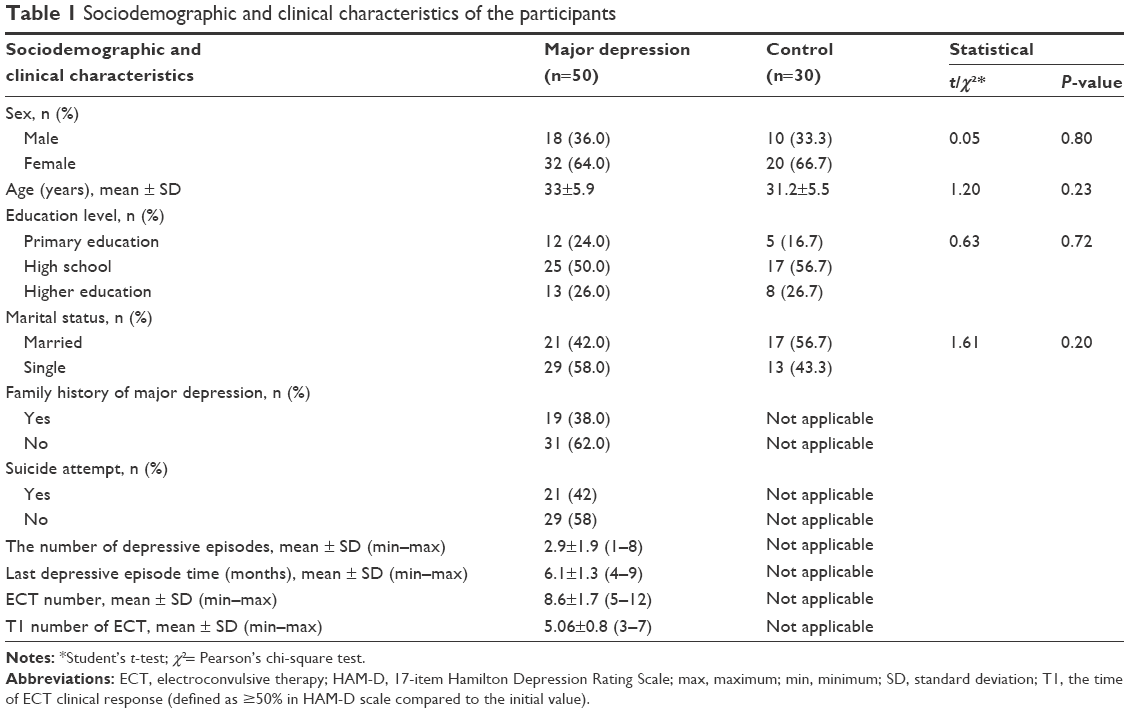 | Table 1 Sociodemographic and clinical characteristics of the participants |
Clinical treatment and change scale
The mean HAM-D scores of the patients were determined as 30.66±4.11 at T0, 15.73±3.36 at T1, and 12.93±4.98 at T2. The reduction in HAM-D scores was found to be statistically significant in the periods T0–T1, T1–T2, and T0–T2 with ECT treatment (T0–T1: t=38.65, P<0.05; T0–T2: t=21.64, P<0.05; T1–T2: t=4.14, P<0.05; t: dependent samples t-test).
IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma measurement
In the 50 cases of treatment-resistant major depression, the mean values of IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma before treatment were found to be 45.40±33.46, 34.98±36.89, 86.49±17.06, 16.88±24.84, 22.60±14.12, and 21.56±20.67 pQ/mL, respectively. The pretreatment levels of IL-1, IL-4, IL-6, IL-10, TNF-alpha, and IFN-gamma of the patient group were compared with the control group, and statistically significant differences were determined. The levels of IL-1, TNF-alpha, and IL-10 were lower in the patient group than in the control group, and IL-4 and IFN-gamma were significantly higher than in the control group (IL-1: t=3.81, P<0.05, TNF-alpha: t=3.05, P<0.05, IL-10: t=2.29, P<0.05, IL-4: t=3.43, P<0.05, IFN-gamma: t=2.88, P<0.05) (Table 2).
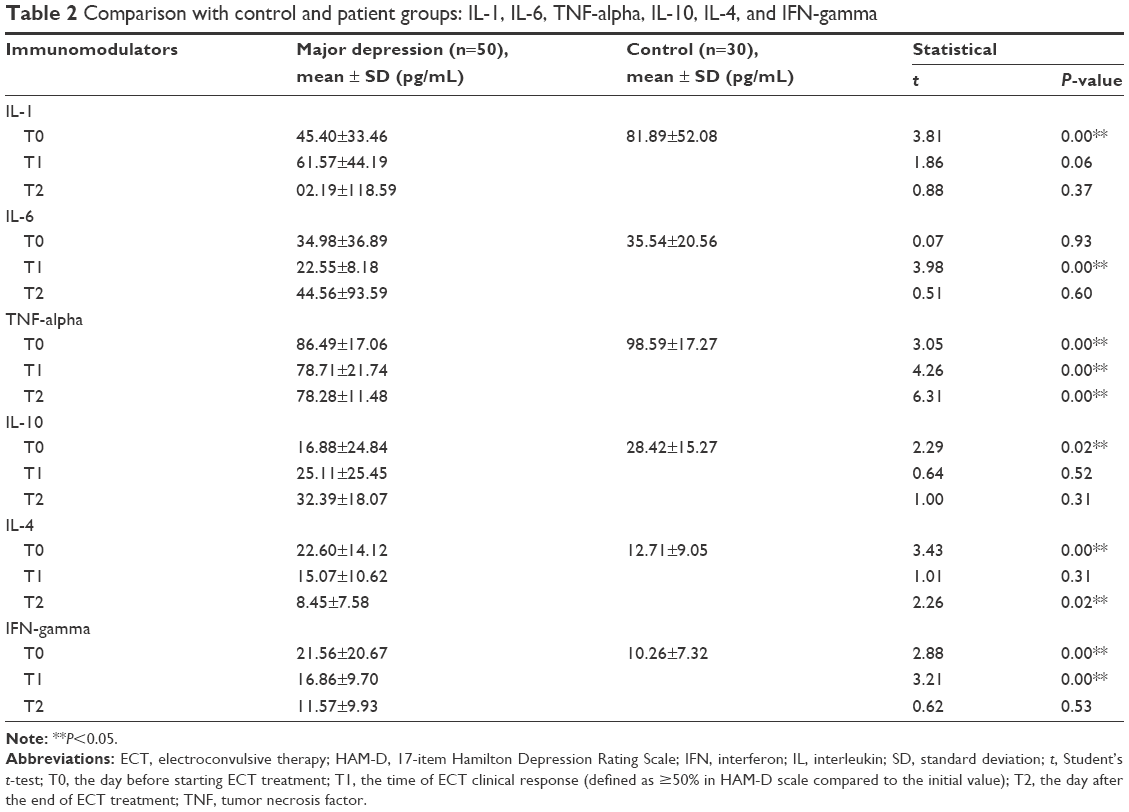 | Table 2 Comparison with control and patient groups: IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma |
No statistically significant correlation was determined between the HAM-D scores and pretreatment levels of IL-1, IL-6, TNF-alpha, IL-10, IL-4, IFN-gamma, and demographic data (age, sex, family history, marital status, suicide tendencies) of the patient group.
The mean values of IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma of the patients treated with ECT at T0, T1, and T2 are given in Figure 1.
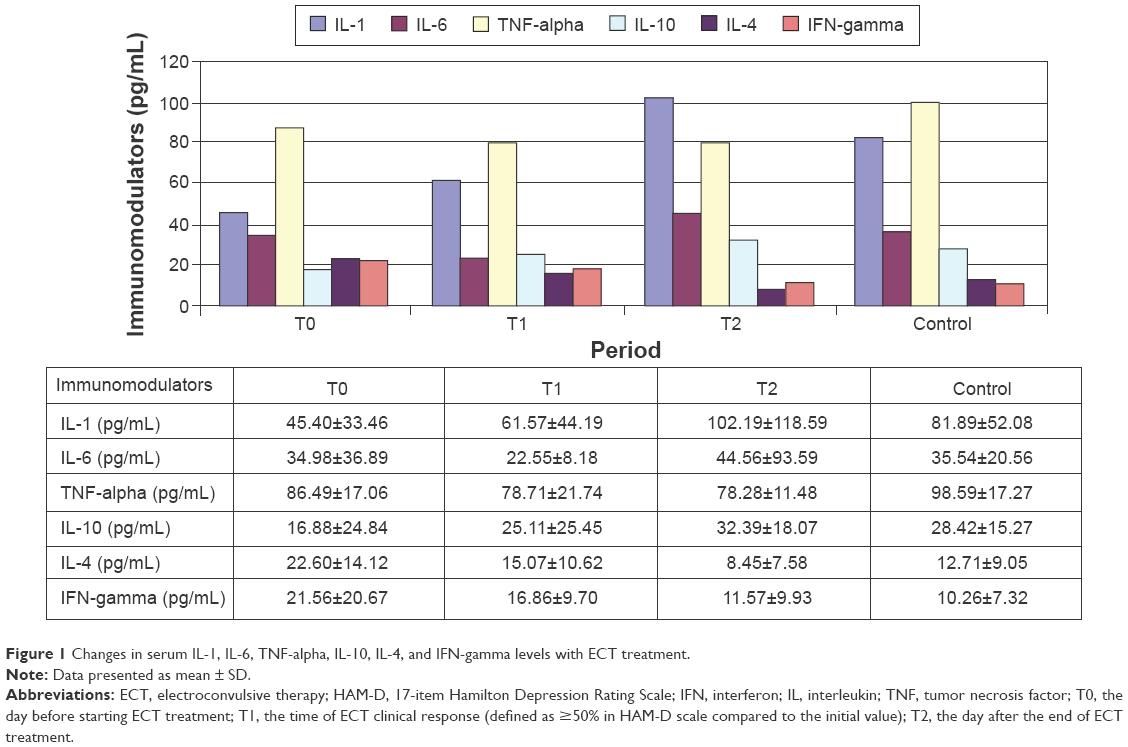 | Figure 1 Changes in serum IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma levels with ECT treatment. |
The mean levels of IL-1 and IL-10 increased in all periods (T0–T1, T1–T2, T0–T2) in the patient group treated with ECT. Mean IL-4, TNF-alpha, and IFN-gamma levels decreased in all periods (T0–T1, T1–T2, T0–T2). The decrease in IL-4 levels and the increase in IL-1 and IL-10 levels were statistically significant at all periods. The increase in IFN-gamma levels at T1–T2 and T0–T2 was statistically significant and not significant at T0–T1 (Table 3).
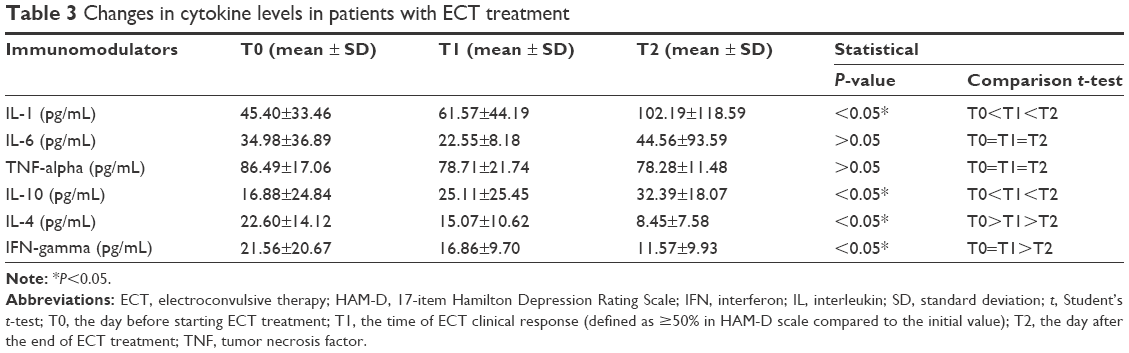 | Table 3 Changes in cytokine levels in patients with ECT treatment |
Relationship between HAM-D scores with IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma measurement
No statistically significant correlation was determined between the HAM-D scores (T1, T2) and the mean levels of IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma (T1, T2) in the patients after ECT (r=0.121, P=0.61). There was no statistically significant correlation between the reduction in HAM-D scores and the changes in the IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma levels (T0–T2: IL-1 [r=0.52, P=0.78], IL-6 [r=0.00, P=0.96], TNF-alpha [r=0.00, P=0.75], IL-10 [r=0.12, P=0.49], IL-4 [r=0.16, P=0.37], and IFN-gamma [r=0.07, P=0.69]).
Discussion
This prospective, nonrandomized, controlled study investigated the levels of serum IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma and their alterations due to ECT therapy in patients with treatment-resistant major depression. The levels of IL-1, TNF-alpha, and IL-10 were found to be higher before treatment in the patients with treatment-resistant major depression than in the control group. There was no significant difference in the levels of IL-6 before and after the treatment when compared to the control group. It was seen that the increase in the levels of IL-1 and IL-10 and the decrease in the levels of IL-4 and IFN-gamma were statistically significant with the treatment. In addition, it was considered that the severity of major depression decreased with ECT. Nevertheless, no significant relationship was determined between the decrease in the severity of major depression (decrease in HAM-D scores) and the alteration in the levels of IL-1, IL-6, TNF-alpha, IL-10, IL-4, and IFN-gamma after the ECT.
In a meta-analysis study investigating cytokine levels in depressive disorder, a significant positive correlation was detected between depression and the levels of IL-1, IL-6, and CRP.10 In another meta-analysis, it was determined that TNF-alpha and IL-6 levels were higher in the depression group than the control group but IL-1β, IL-4, IL-8, IL-10, and IFN-gamma levels were not different between the patient and control groups. As a result, it was concluded that the levels of TNF-alpha and IL-6 increase in major depression and these findings prove that there is an activation of the immune system in depression.11 In a community study with a large sample size (2,861 individuals), a positive correlation was determined between depressive symptoms and the levels of IL-6, TNF-alpha, and CRP. It was reported that there is a relationship between the somatic symptoms of both depression and anxiety and the levels of IL-6, TNF-alpha, and CRP. It was claimed that depression and somatic symptoms of anxiety may have a relationship with inflammation.12 Furthermore, it was proposed that the levels of proinflammatory cytokines decrease with antidepressant treatment.26–28 When the studies investigating the effect of ECT on the levels of serum cytokines were reviewed, it was seen in one study that the levels of IL-1 beta and IL-6 increased after the third and sixth hours of ECT treatment. In the same study, a correlation was also determined between IL-6 levels and the stimulus applied and it was stated that this may be a mechanism that indicates neuronal depolarization.29 In another study, the TNF-alpha levels of 15 patients with depression were compared with healthy individuals before, during, and after ECT treatment and the TNF-alpha levels were seen to significantly decrease with ECT treatment.30 Furthermore, the hypothesis of dysregulated cytokine levels is strengthened by the report of the successful use of ECT in a patient who developed major depression while receiving IFN-alpha-2b for hepatitis C.31 These results demonstrate that ECT is associated with cytokine levels in the circulation. However, the present study differs in some respects from these studies. It is known that IL-1, IL-2, IL-6, TNF-alpha, and IFN-gamma are proinflammatory and IL-4, IL-10, IL-12, and IL-13 are anti-inflammatory cytokines. Some cytokines, such as IL-8, have both proinflammatory and anti-inflammatory effects. The common opinion in psychoneuroimmunological studies is that just as there is an increase in proinflammatory cytokine levels as a response to encountering a pathogen or to tissue damage, psychosocial stressors also cause an increase in the cytokine levels and mediate the communication between the immune system and the brain. In the current study, in parallel with previous studies, the levels of IFN-gamma, which is a proinflammatory cytokine, were found to be higher in the patients with depression than in the control group and levels of IL-10, which is an anti-inflammatory cytokine, were lower than in the control group. Serum IFN-gamma levels significantly decreased, while serum IL-10 levels increased with ECT treatment. Similar levels were observed after the treatment when compared with healthy controls. In addition, IL-10 levels responded faster to the treatment than IFN-gamma levels and displayed a profile similar to the healthy control subjects in the T1 period (Table 2). In contrast to previous studies, in the current study, IL-1 and TNF-alpha levels, which are proinflammatory cytokines, were found to be lower in the patients with depression than in the healthy control group, whereas no significant alteration in IL-6 levels was detected. Contrary to previous research, levels of IL-4, which is an anti-inflammatory cytokine, were observed to be higher in patients with depression. This finding may be due to significant methodological factors that may have affected the results. These discrepancies in the results may be explained by the following elements: the inclusion of patients with bipolar depression, patients receiving different antidepressant treatment, or patients with no previous treatment and that the study was conducted at different stages of the disease. The type of application of ECT, anesthetic drugs used, and time of convulsion may also affect results, as there are data suggesting that ECT treatment increases the proinflammatory cytokines independently of the clinical process of the patients. Lehtimaki et al29 reported that IL-1A and IL-6 levels increase after the third and sixth hours of ECT treatment. The current study also supports the hypothesis that ECT treatment causes an increase in IL-1 levels.
However, there are also studies reporting that there is no association between depression and cytokines.32,33 In a study by Hocaoğlu et al33 comparing patients with major depression and healthy controls, no difference was determined between 30 depressed patients and a healthy control group with respect to the levels of IL-1β, IL-6, IL-8, IL-10, TNF-alpha, and IFN-gamma. Although there is evidence suggesting the opposite, the findings of previous studies and those of the current study indicate that neuroinflammation has a role in the etiopathogenesis and clinical process of depressive disorder.
Limitations
One of the main limitations of the current study is the low sample count, although in comparison with similar studies, it can be said to be higher or similar. To determine the change in cytokine levels in ECT, broad participation studies are needed to evaluate the significance of the relationship between a reduction in depression severity and cytokine level change.
Apart from age and sex, other factors, such as smoking, alcohol use, exercise, and menstrual cycle can affect cytokine levels. In the current study, the menstrual characteristics of female patients and smoking habits were not evaluated. Other limitations include the use of muff instead of electroencephalography to evaluate seizure duration and effect, and the seizure durations were not similar for each patient. It is still unclear what length of time is required for the realization of significant changes with treatment (antidepressants or ECT). Future studies with longer-term follow-up after treatment could provide more meaningful results.
Conclusion and recommendations
The results of this study indicate that serum cytokine levels in depressed patients are affected, however the changes did not correlate with the severity of depressive symptoms. The study also demonstrated that ECT treatment causes changes in cytokine levels. There is a current debate regarding immune mediators as biological markers for diagnosis and the response to treatment of major depression. Immune mediators in patients with major depression have been shown to be different from those of healthy control subjects and the decrease in this difference with treatment suggests that immune mediators might be useful markers. As there are a variety of cytokines in immune modulation, it would be valuable to achieve clarity of the biology of cytokines for diagnosis and the follow-up process of psychiatric disorders. From the data of previous studies, it is difficult to say that immune mediators are a specific marker for major depression. There is a need for further studies of combined assessment to provide a better understanding of the neuroimmunological and genetic processes and psychobiological features of mental disorders.
Acknowledgment
The authors sincerely thank the participant psychiatrists for kindly collecting the data for analysis in this study.
Author contributions
This was a collaborative work, and the authors worked closely with each other. All authors participated in the design of the original study, or in the interpretation and analysis of data, contributed to drafting the manuscript, and approved the final version of manuscript. All authors were responsible for literature review and extraction of references, and also for making the decision to submit the paper for publication.
Disclosure
All of the authors report no conflicts of interests in this work. No payments or honoraria were received as a consequence of authorship for this manuscript.
References
Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020. Global burden of disease study. Lancet. 1997;349(9064):1498–1504. | ||
Hansen-Grant SM, Pariante CM, Kalin NH. Neuroendocrine and immune system pathology in psychiatric disease. In: Schatsberg AF, Nemeroff CB, editors. Textbook of Psychopharmacology. 2nd ed. Washington, DC: American Psychiatric Press, 1998:171–194. | ||
Seidel A, Arolt V, Hunstiger M, Rink L, Behnisch A, Kirchner H. Cytokine production and serum proteins in depression. Scand J Immunol. 1995;41(6):534–538. | ||
Stein M, Miller AH, Trestman RL. Depression, the immune system, and healthy and illness. Arch Gen Psychiatry. 1991;48(2):171–177. | ||
Glaser R, Kiecolt-Glaser JK, Bonneau RH. Stress-induced modulation of the immune response to recombinant hepatitis B vaccine. Psychosom Med. 1992;54(1):22–29. | ||
Lanquillon S, Krieg JC, Bening-Abu-Shach U, Veddar H. Cytokine production and treatment response in major depressive disorder. Neuropsychopharmacology. 2000;22(4):370–379. | ||
Seidel A, Arolt V, Hunstiger M, Rink L, Behnisch A, Kirchner H. Major depressive disorder is associated with elevated monocyte counts. Scand J Immunol. 1996;94(3):198–204. | ||
Miller AH, Spancer RL, McEwen BS. Depression adrenal steroids, and the immune system. Ann Med. 1993;25(5):481–487. | ||
Miller AH. Neuroendocrine and immune system interaction in stress and depression. Psychiatr Clin North Am. 1998;21(2):443–463. | ||
Ressler KJ, Nemeroff CB. Role of serotonergic and noradrenergic systems in the pathophysiology of depression and anxiety disorders. Depress Anxiety. 2000;12(1):2–19. | ||
Demir S, Atli A, Bulut M, et al. Neutrophil-lymphocyte ratio in patients with major depressive disorder undergoing no pharmacological therapy. Neuropsychiatr Dis Treat. 2015;27(11):2253–2258. | ||
LeMay GL, Wander AJ, Kluger MJ. The effects of psychological stress on plasma interleukin-6 activity in rats. Physiol Behav. 1990;47(5):957–961. | ||
Zhou D, Kusnecov AW, Shurin MR. Exposure to physical and psychological stressors elevates plasma interleukin 6: relationship to the activation of the hypothalamic-pituitary-adrenal axis. Endocrinology. 1993;133(6):2523–2530. | ||
Zincir S, Zincir SB, Doruk A, et al. Asymmetric dimethylarginine (ADMA) and treatment response relationship in male patients with first-episode schizophrenia: a controlled study. Psychiatry Res. 2014;220(1–2):76–80. | ||
Kent S, Bluthe RM, Kelley KW. Sickness behaviour as a new target for drug development. Trends Pharmacol Sci. 1992;13(1):24–28. | ||
Maes A. A review on the acute phase response in major depression. Rev Neurosci. 1993;4(4):407–416. | ||
Sluzewska A, Rybakovsky J, Bosmans E. Indicators of immune activation in major depression. Psychiatry Res. 1996;64(3):161–167. | ||
McCall WV, Andrade C, Sienaert P. Searching for the mechanism(s) of ECT’s therapeutic effect. J ECT. 2014;30(2):87–89. | ||
Lanzenberger R. Neurotransmitters and ECT. J ECT. 2014;30(2):116–121. | ||
Haskett RF. Electroconvulsive therapy’s mechanism of action: neuroendocrine hypotheses. J ECT. 2014;30(2):107–110. | ||
Farzan F, Boutros NN, Blumberger DM, Daskalakis ZJ. What does the electroencephalogram tell us about the mechanisms of action of ECT in major depressive disorders? J ECT. 2014;30(2):98–106. | ||
Bolwig TG. Imaging the brain during/after ECT: a look inside the mechanism of action. J ECT. 2014;30(2):143–152. | ||
Bolwig TG. How does electroconvulsive therapy work? Theories on its mechanism. Can J Psychiatry. 2011;56(1):13–18. | ||
Fink M. Should the dexamethasone suppression test be resurrected? Acta Psychiatr Scand. 2005;112(4):245–249. | ||
Nierenberg AA, Amsterdam JD. Treatment-resistant depression: definition and treatment approaches. J Clin Psychiatry. 1990;51(Suppl. 39–47):48–50. | ||
Janssen DG, Caniato RN, Verster JC, Baune BT. A psychoneuroimmunological review on cytokines involved in antidepressant treatment response. Hum Psychopharmacol. 2010;25(3):201–215. | ||
Krishnadas R, Cavanagh J. Depression: an inflammatory illness? J Neurol Neurosurg Psychiatry. 2012;83(5):495–502. | ||
Hannestad J, DellaGioia N, Bloch M. The effect of antidepressant medication treatment on serum levels of inflammatory cytokines: a meta-analysis. Neuropsychopharmacology. 2011;36(12):2452–2459. | ||
Lehtimaki K, Keranen T, Huuhka M, et al. Increase in plasma proinflammatory cytokines after electroconvulsive therapy in patients with depressive disorder. J ECT. 2008;24(1):88–91. | ||
Hestad KA, Tønseth S, Støen CD, Ueland T, Aukrust P. Raised plasma levels of tumor necrosis factor alpha in patients with depression: normalization during electroconvulsive therapy. J ECT. 2003;19(4):183–188. | ||
Zincke MT, Kurani A, Istafanous R, Kellner C. The successful use of electroconvulsive therapy in a patient with interferon-induced psychotic depression. J ECT. 2007;23(4):291–292. | ||
Kocabaşoğlu N, Konuk N, Öztürk S, Bayar R. A controlled trial on the associations between depression and acute phase reactants, immunity. Yeni Symposium. 2000;38(3):83–87. | ||
Hocaoğlu Ç, Kural B, Aliyazicioglu R, Deger O, Cengiz S. IL-1 β, IL-6, IL-8, IL-10, IFN-γ, TNF-α and its relationship with lipid parameters in patients with major depression. Metab Brain Dis. 2012;27(4):425–430. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.