Back to Journals » Research and Reports in Tropical Medicine » Volume 11
Level of Perceived Attitude and Practice and Associated Factors Towards the Prevention of the COVID-19 Epidemic Among Residents of Dessie and Kombolcha Town Administrations: A Population-Based Survey
Authors Muluneh Kassa A ![]() , Gebre Bogale G
, Gebre Bogale G ![]() , Mekonen AM
, Mekonen AM ![]()
Received 21 September 2020
Accepted for publication 29 October 2020
Published 19 November 2020 Volume 2020:11 Pages 129—139
DOI https://doi.org/10.2147/RRTM.S283043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario Rodríguez-Pérez
Ayesheshim Muluneh Kassa,1 Getahun Gebre Bogale,2 Asnakew Molla Mekonen3
1Department of Nursing, Dessie Health Science College, Dessie, Ethiopia; 2Department of Health Informatics, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 3Department of Health System Management, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Ayesheshim Muluneh Kassa
Department of Nursing, Dessie Health Science College, Dessie 1212, Ethiopia
Tel +251– 9-11-19-96-45
Email [email protected]
Purpose: COVID-19 has been declared a pandemic by the World Health Organization. The unprecedented global health crisis we are facing is affecting all parts of society and changing lives and livelihoods. International efforts have been applied to prevent the spread of the virus through personal hygiene, masks and social distancing as prevention measures. The aim of this study is to assess the level of perceived attitude and practice and associated factors among Dessie and Kombolcha Town administrations, north-east Ethiopia.
Patients and Methods: A cross-sectional population-based survey was conducted using a structured interview-administered questionnaire from June 7 to 14, 2020, among Dessie and Kombolcha town residents. The data were entered to Epi Info-7.1 and exported to SPSS-23. Bivariable logistic regression was done, and variables with p < 0.25 were entered a multivariable logistic regression analysis model. Statistically significant level was declared at 95% CI and a p-value < 0.05.
Results: A total of 828 participants were involved with a response rate of 98%. Of the total participants, 29.35% (95% CI: 26.3, 32.5) had poor attitude and 41.79% (95% CI: 38.5, 45.3) had poor practice towards COVID-19 prevention. Multivariable regression results showed a significant association with being male, unable to read and write, and mass media with attitude and rural residence, being widowed, a merchant, family size 4– 6, spring water source and information heard from social media with practice.
Conclusion: Our findings revealed that there are inappropriate practices and poor attitudes towards COVID-19 prevention among Dessie and Kombolcha residents.
Keywords: attitude, practice, COVID-19, Dessie, Kombolcha, Ethiopia
Introduction
COVID-19 (Corona Virus Disease 19) is a disease caused by the family of the Corona viruses that were first described in 1966 which cultivated the viruses from patients with common cold.1 Corona viruses are classified most commonly based on their morphology are termed corona viruses (Latin: corona = crown). There are four Corona virus subfamilies, these are alpha, beta, gamma and delta corona viruses, where beta corona viruses may cause severe disease and fatalities and alpha corona viruses cause asymptomatic or mildly symptomatic infections.2 They are transmitted from animals to humans. While alpha and beta corona viruses apparently originate from mammals, in particular from bats, gamma and delta viruses originate from pigs and birds.1,2
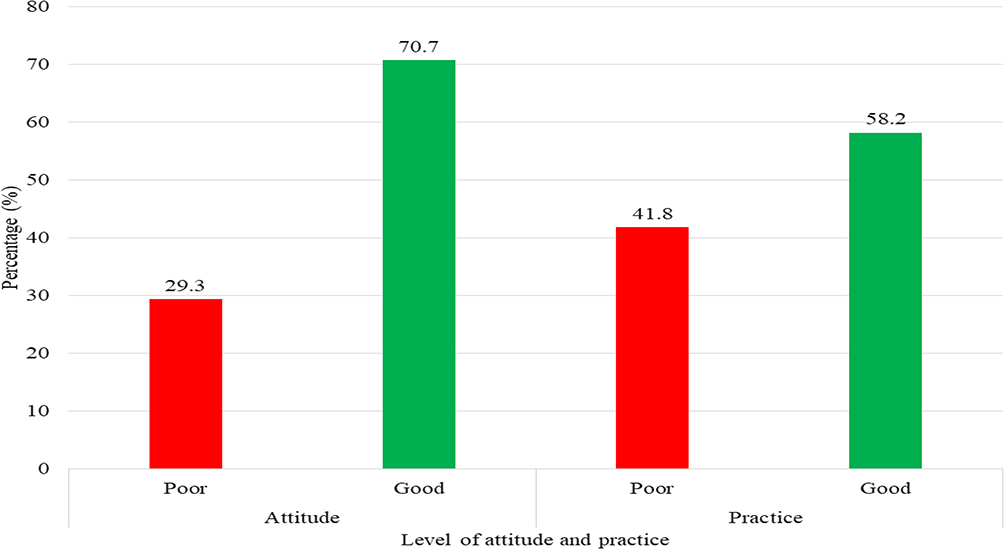 |
Figure 1 Level of attitude and practice towards prevention of COVID-19 among Dessie and Kombolcha residents, north-east Ethiopia, 2020. |
COVID-19 was first detected in Wuhan, China, in December 2019, and on January 30, 2020 WHO declared that the current outbreak constituted a public health emergency of international concern based on growing case notification rates at Chinese and international locations when the virus causes a large burden of morbidity and mortality.2 COVID-19 is highly transmitted and spread from a single town to the entire country in just 30 days.15 Within that time the epidemic may double in the number of affected people every seven days and each patient spreads infection to 2.2 other individuals.15 The outbreak estimates a mean range from 2.2 to 3.58.16,17 The reason for this transmission across the world might be both geographical expansion and the sudden increase in numbers of cases which surprised and quickly overwhelmed health and public health services.12 COVID-19 has threatened the world with a public health crisis. Globally more than 10 million people are infected and nearly 500,000 fatalities have been reported after being declared a pandemic by the World Health Organization (WHO) (June 26, 2020, 11:40 GMT). International borders have been locked down, travel restricted, economies slashed and billions of people are isolated at their own homes as a measure to contain the outbreak.18
Studies done in Italy among undergraduate students and mass media have a significant influence both on the knowledge and attitudes of people as well as on their risk perception.26 The attitude towards COVID-19 is significantly lower among male respondents, lower education and those living among more crowded households.3,4 Additionally, increasing the response rate of public awareness of the media reports can both significantly bring forward the peak time and reduce the peak size of the infection, which is a result of creating a positive attitude among people.5–7 Social and mass media could influence the risk perception because the information might refer to heuristics.29 Studies showed a significant correlation between female gender, higher age, and higher education with practice.1–4
Ethiopia is one of the countries threatened by COVID-19; 5175 COVID-19 cases have been reported, among whom 81 died and 1544 recovered (June 26, 2020, 11:40 GMT). The country has not taken a nation-wide lockdown, but the country has declared a state of emergency. In Ethiopia, many organizations including the government sector have to implement different measurement plans to prevent the virus. In the community there is still a gap in using a prevention mechanism despite many media and organizations mobilizing the community and advocacy of a strategy to curb the pandemic. Most of the reason is perception of less susceptibility and lack of practice of prevention techniques.20,23
Preventive measures such as masks, hand hygiene practices, avoidance of public contact, case detection, contact tracing, and quarantines have been discussed as ways to reduce transmission.25 In several Asian countries, mask adoption seems to correlate with slowing down the pace of COVID-19 transmission. China, South Korea and Vietnam are all good examples.28 This also includes social distancing for all ages and helps protect vulnerable older adults.27 To date, no specific antiviral treatment has proven effective; hence, infected people primarily rely on symptomatic treatment and supportive care.24,26
There is a huge gap in preventing viruses because it is a new emerging phenomenon. Little is known about the perception of these diseases by the general public and everyday practices of adhesion to these rules by different social groups, psychological patterns of coping with restrictive measurements in different countries make a challenge in preventing the virus. Cultural determinants play an important role in controlling infection behavior.27
This all shows the need for research in every aspect, but in the end, prevention is the only effective way to cut the virus, so to do this the community must know and implement the prevention mechanism. For intervention, you need to have evidence that shows the level of the intervention and to continue it. So, the aim of this study was to determine the level of attitude and practice and associated factors towards COVID-19 prevention in Dessie and Kombolcha town administrations. In our research, sex, educational status and information heard from mass media are the main determinants associated with poor attitude. Furthermore, marital status, residence, main occupation, family size, type of water and information heard from social media are associated with poor practice. This is a broader research compared to another study conducted in a single institution, and this view point provides potential reasons for these findings, which might be for programmers, policy makers and implementers in the region, Dessie and Kombolcha town administration, Health Department office and Water Supply and Sewerage Service offices for their evidence-based decisions in interventions towards COVID-19 prevention.
Materials and Methods
A population-based cross-sectional survey was conducted from June 7 to 14, 2020, in Dessie and Kombolcha town administrations, Amhara National Regional State, north-east Ethiopia. Dessie is 401 km and Kombolcha is 376 km from Addis Ababa, the capital of Ethiopia, respectively. Dessie town has 26 kebeles, 18 urban and 8 rural, and Kombolcha has 11 kebeles, 5 urban and 6 rural, a total of 37 kebeles in the two town administrations. Dessie and Kombolcha vital statistics office report showed that the total population of Dessie is 385,850 and Kombolcha 143,214. The two town administrations have 529,064 inhabitants, of whom 262,157 are male and 266,907 are female.
The study population was residents found in the selected kebeles in Dessie and Kombolcha Town administrations who had the chance to be included in the sample. Participants critically and mentally ill during the study period were excluded from the study. The sample size for this study was calculated using a single population proportion formula, the estimation of the sample size was done by assuming a prevalence of 50%, 95% confidence level and 5% margin of error. The calculated sample size of this study was 768 participants with a design effect of two. By adding a tolerable non-response rate (10%), the total sample size was 845 participants.
A two-stage sampling technique was employed to select the study participants. A total of 845 participants from their respective households were included in the study. A simple random sampling technique was applied to select kebeles to eliminate selection bias. In the first stage, nine kebeles were selected out of 37 kebeles using a lottery method by assuming the residents of the two towns are homogeneous. In the second stage, data were collected from households using a systematic sampling technique, where participants have the chance to be selected. Then, based on their population size, the sample size was proportionally allocated to each of the sampled kebeles and samples were drawn, and it was representative of the population characteristics for policy implications.
The outcome variables were attitude and perceived practice. The determinant factors were; socio-demographic variables (sex, age, marital status, residence, religion, level of education, occupation, family size and income), availability of household materials/related variables (water source, amount of water, functional TV/radio, functional cell phone) and source of information related variables (mass media, health care workers, family members, social media, religious leaders).
Operational Definition of Attitude and Practice
About 32 attitudes of COVID-19-related questions were provided to respondents, and those who answered below 50% were assigned as having a poor attitude, whereas those who answered 50% and above were assigned as having a good attitude on COVID-19 prevention. About 14 practices of COVID-19 related questions were provided to respondents, and the respondents who answered below 50% were assigned as having a poor practice, whereas those who answered 50% and above were assigned as having a good practice on COVID-19 prevention.
The questionnaire for this study was a structured interview-administered questionnaire which was adopted from the WHO COVID-19 guideline5 and scientific studies,6 prepared in English and translated to the Amharic local language then re-translated back to English used for conceptual equivalence by language experts. To check the validity of the tool, the adopted questionnaire was sent to a group of experts, chosen according to their experience and expertise in related fields (health promotion, environmental health and medical internist). The experts appraised the questions in terms of consistency, intelligibility and generalizability. Internal consistency of attitude measures was tested using a reliability test where the Cronbach alpha coefficient aided in determining the reliability of the variables. The results showed that the Cronbach alpha for attitude was 0.7. The result added credibility. According to Griethuijsen, a range of Cronbach alpha from 0.6 to 0.7 is considered adequate and reliable.7
Pre-test was conducted on 5% of the total sample size in Kalu district, and the amendment was done according to the finding. The questionnaires used in the pre-test were not included in the analysis as part of the main study. Training on the objectives of the study was given to data collectors and supervisors before the day of the data collection. Regular supervision, control as well as support of data collectors by the supervisors were made daily, and each completed questionnaire was checked and the necessary feedback was offered to interviewers. The collected data were properly handled, reviewed and checked for completeness and consistency by the supervisor and before the analysis began each day. The data were collected by 10 public health officers and eight nurses, and the data collection process was supervised by five masters of public health professionals. A day training was given to both the data collectors and the supervisors prior to the data collection process. It was used to check the goodness of the fit of the model.
The collected data were coded, edited, entered into Epi Info version 7 and analyzed using the Statistical Package for the Social Sciences (SPSS) version 23. Descriptive summary statistics such as mean ± SD, median ± IQR, frequencies and proportions were presented as appropriate. The Chi-square test was checked for count frequencies per cell in two by two data presentation. Binary logistic regression analysis was done and all independent variables at p-value <0.20 were taken to a multivariable logistic regression analysis to identify associated factors with outcome variables. Statistical significance of variables in the final model was declared at p-value <0.05 and 95% confidence level for the adjusted odds ratio. The Hosmer and Lemeshow statistics and the deviance coefficient were used to check the goodness of the fit of the model.
Ethical Considerations
Ethical review (with ref. no.: CMHS/311/036/20) was obtained from institutional review board (IRB) of the College of Medicine and Health Sciences, Wollo University. Verbal informed consent was approved by the IRB. Permission was obtained from Dessie Health Science College. Informed consent was obtained from each study participants prior to data collection. Strict confidentiality of responses was maintained during the study and the data given by the participants were used only for research purposes. This study was conducted in accordance with the Declaration of Helsinki.
Results
Figure 1 showed that the level of attitude and practice towards the prevention of the COVID-19 epidemic among residents of Dessie and Kombolcha town administrations. Among the study participants, 243 (29.35%) had a poor attitude and, 585 (70.7%) had a good attitude towards COVID-19 prevention in both towns. The practice of the study participants were, 346(41.8%) had poor practice, 482(58.2%) had good practice in the prevention of the COVID-19 epidemic.
Factors Associated with Attitude of Participants Towards COVID-19 Epidemic
Variables associated with poor attitude towards COVID-19 prevention were sex, educational level and information from mass media.
Those male participants were 1.02 times more likely to have a poor attitude towards COVID-19 prevention as compared to their counterparts (AOR=1.02; 95% CI: 1.02, 2.10). Regarding educational level, those who were unable to read and write were 76% times more likely to have a poor attitude as compared to those who had attended a higher level of education towards COVID-19 prevention (AOR = 1.76; 95% CI: 1.06, 2.92). Participants who were not receiving information about COVID-19 from the mass media were 99% times more likely to have a poor attitude compared to those who received information from the mass media (AOR = 1.99; 95% CI: 1.30, 3.05) (Table 1).
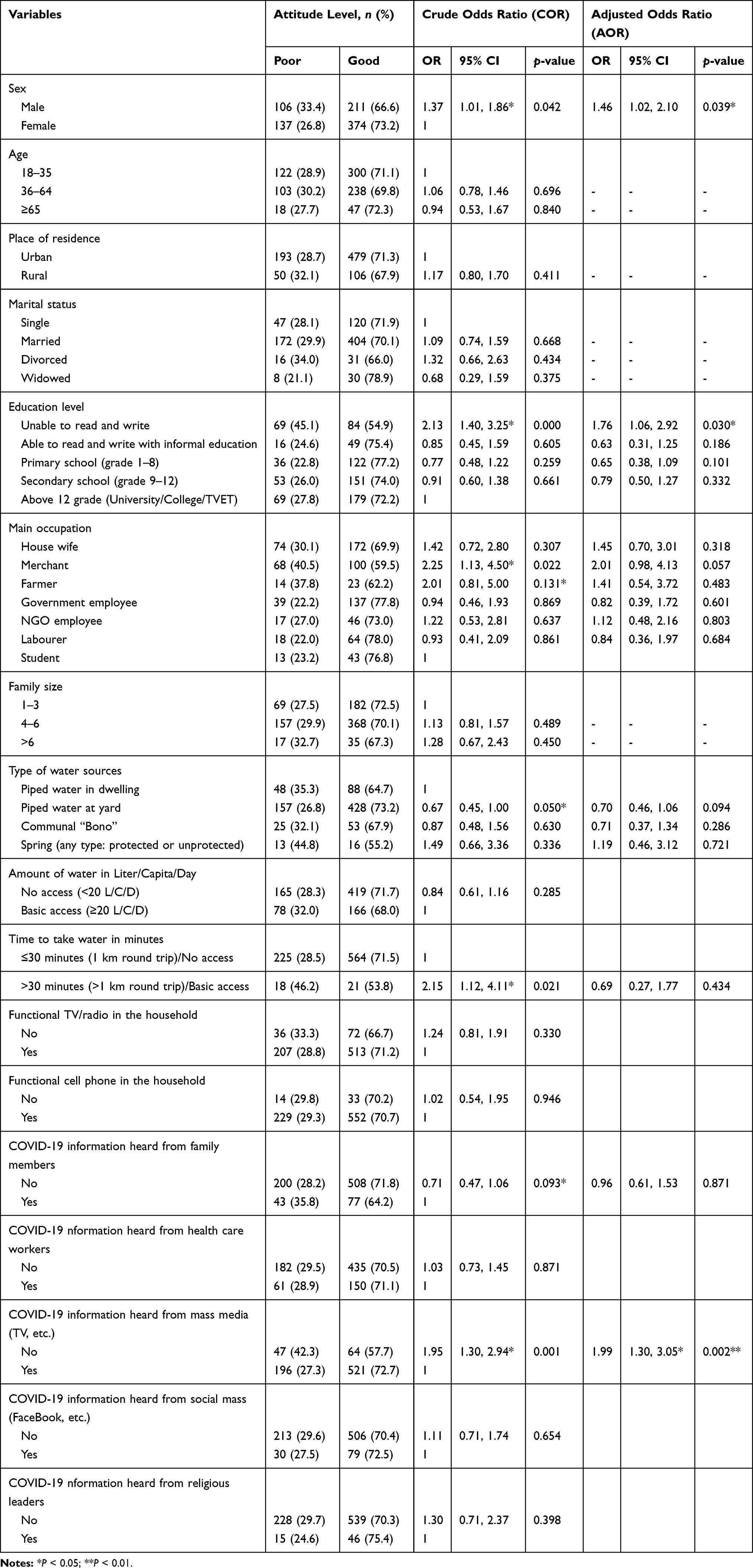 |
Table 1 Bivariable and Multivariable Logistic Regression of Attitude Towards COVID-19 Epidemic Among Residents of Dessie and Kombolcha Town Administration, north-east Ethiopia, June, 2020 (n = 828) |
Factors Associated with Practice of Participants Towards COVID-19 Epidemic
Variables associated with poor practice towards COVID-19 prevention were residence, marital status, main occupation, family size, type of water sources, and COVID-19 information heard from social media.
Participants who were rural residents were 2.58 times more likely to have poor practice than urban residents (AOR = 2.58; 95% CI: 1.65, 4.03). Participants who were widowed were 68% less likely to have poor practice than single (AOR = 0.32; 95% CI: 0.14, 0.76). Participants who were merchants were 57% less likely to have poor practice than housewives (AOR = 0.43; 95% CI: 0.27, 0.66). Participants who were government employees were 36% less likely to have poor practice than housewives (AOR = 0.64; 95% CI: 0.42, 0.97). Participants who had family sizes of 4–6 members were 30% less likely to have poor practice towards COVID-19 prevention than those who had family sizes of 1–3 members (AOR = 0.70; 95%: 0.49,0.98). Participants who had piped water at their yard water source were 1.59 times more likely to have poor practice compared to those who had water at indwelling towards the prevention of COVID-19 (AOR = 1.59; 95% CI: 1.03, 2.44). Participants who had a spring water source (protected and unprotected) were 4.37 times more likely to have poor practice towards the prevention of COVID-19 than piped water sources in a dwelling (AOR = 4.37; 95% CI: 1.36, 14.04). Participants who did not get COVID-19 information from social media were 1.73 times more likely to have poor practice than their counter parts (AOR = 1.73: 95% CI: 1.08, 2.79) (Table 2).
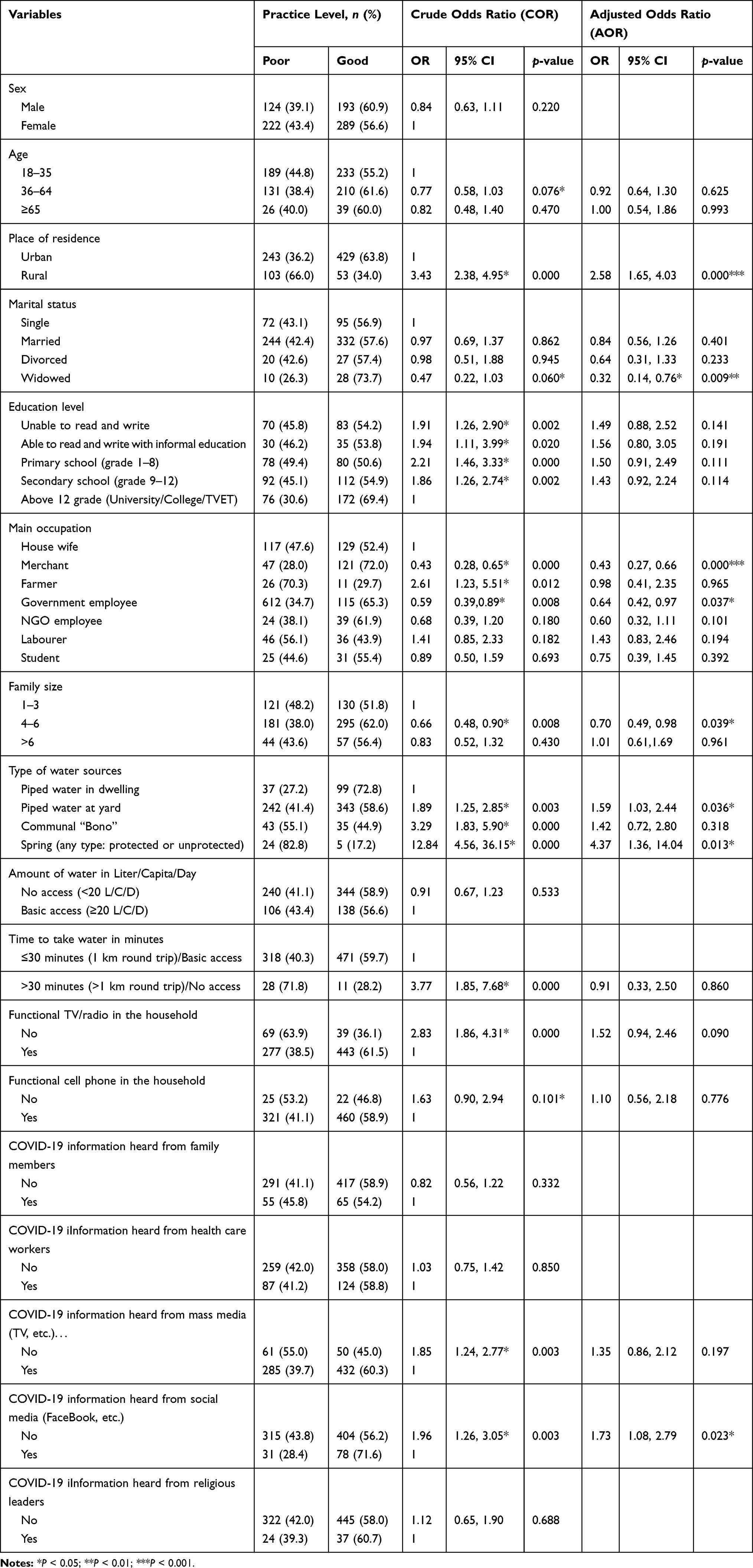 |
Table 2 Bivariable and Multivariable Logistic Regression of Practice Towards COVID-19 Epidemic Among Residents of Dessie and Kombolcha Town Administration, north-east Ethiopia, June, 2020 (n = 828) |
Discussion
The prevalence of poor attitude among participants was 29.35% (95% CI: 26.3, 32.5), which is consistent with a study in Bangladesh, Thailand and India,8–10 but it shows a disparity with studies done in China, Nepal and USA, which had comparably high attitude toward prevention of COVID-19.11–13 The possible explanation could be due to differences in the study participants, socio-economic status and the study area.
Male participants were 1.2 more likely to have a poor attitude toward COVID-19 prevention. This finding is supported by studies in Egypt, Iran and China.11,14,15 The possible explanations may be that males have less perceived susceptibility to disease. Female gender has been linked to more worry and engagement in preventive and treatment-seeking behaviors. A few other studies also reported that women were superior to men in terms of the positive attitude related to infectious diseases.11,16
Participants who were unable to read and write were 1.76 more likely to have a poor attitude toward COVID-19 prevention. This finding was supported by studies in Thailand, Iran, Bangladesh and China.8,9,11,14 The reasons may be that uneducated participants who lack retrieving basic information from a different source were related to awareness and perception of prevention mechanisms.9
Those participants who did not have access to mass media were 1.99 times more likely to have a poor attitude towards COVID-19 prevention. The finding was supported by a study done in Iran, Vietnam and Tanzania.14,17,29 The reasons might be that mass media had a wide range of coverage and the perceived trustworthiness of its source.18,19
The study showed that 41.79% (95% CI: 38.5, 45.3) had poor practice towards COVID-19. The proportion of participants with poor practice in this study was much higher than findings from similar studies conducted in Malaysia (25.87%), Nepal (2.9%), Iran (11%) and Paraguay (18.67%).1,7,20,21 This difference may be due to socio-economic and access to media differences in the study populations and the way the outcome variables were measured. However, the poor practice in our study was lower than in similar studies conducted in Jimma (73.11%) and Pakistan (63.5%).22,23 Possible reasons might be due to variation in the sampling techniques, data collection tool and/or the sample sizes.
Participants who were residents of the rural areas were 2.58 times more likely to have poor practice than urban residents. This may be due to lack of awareness on COVID-19 prevention, lack of water and soap among rural residents. Participants who were widowed were 68% less likely to have poor practice than those who were single. This study is supported by a previous study that single women behaved in poor practice.1,21 This may mean that widowed women had previous experience of personal hygiene and family values than single women. In contrast to this study, a study done in Paraguay showed that married women have good practice.21 This may be due to socio-demographic, sample size, and study participant differences among studies.
Participants who were merchants were 57% less likely to have poor practice than the housewives. Participants who were government employees were 36% less likely to have poor practice than the housewives. Findings from Jimma supported this study that private business and government officers had less poor practice.22 This could be due to them having high educational levels and practice COVID-19 prevention methods that are got from different information sources.
Participants who had 4–6 member family sizes were 30% less likely to have poor practice of COVID-19 prevention than those who had 1–3 member family sizes. The possible explanation may be that participants who have a large family may fear the spread of the disease and the cost of the expense related to the infection. However, a finding from another study in Iran shows that the number of household members is not associated with poor practice.1 This may be due to cultural, economic, and sample size differences between the two studies.
Participants who had piped water sources at their yard were 1.59 times more likely to have poor practice in COVID-19 prevention than those who had piped water sources at the dwelling. The reason might be those who have water sources at their yard are far away from the dwelling and not easily accessible at any time. Participants who had a spring water sources were 4.37 times more likely to have poor practice on COVID-19 prevention than piped water sources in the dwelling. This could be because spring water sources are distant from the household and provide an inadequate amount of water, so they have poor practice in hand washing as recommended by the guidelines.
Participants who had not received the COVID-19 information from social media were 1.73 times more likely to have poor practice than their counterparts. Evidence from Saudi Arabia showed that social media was the main source of information about Coronavirus prevention.24 The possible explanation might be more cell phone usage by the participants. However, evidence from different studies showed that gender, age, knowledge, educational level, and health -related occupations1,6,20,21,25 are associated with poor practice in contrast to this study.
Conclusion
In this study, nearly one third of participants had a poor attitude and 42% of them had poor practice towards COVID-19 prevention among residents of Dessie and Kombolcha town administrations, north-east Ethiopia. Findings from this study showed that sex, educational level and information heard from mass media were associated with poor attitude of participants. Furthermore, residence, marital status, main occupation, family size, type of water sources and information heard from social media were associated with poor practice towards the prevention of COVID-19.
These findings may have implications on the prevention campaign/program of the new corona virus epidemic, particularly in the study settings. As described above, the empowerment of female to formal education and employment shall be strengthened to increase their awareness and exposure to the latest information. Mass media have a tremendous role to provide information to the community, so focus should be on their rural residents to access and have appropriate information towards COVID-19 prevention. Mass media should have a program in analyzing information provided by social media and broadcasting appropriate evidences to the community and prepare attitude-booster programs for the male community in the prevention of COVID-19. In the meantime, the adequacy and accessibility of water for households should be provided to be effective in the prevention measures at this time. There is no previous research done on COVID-19 in Dessie and Kombolcha; therefore, this research would be a baseline for feature researchers for community-level studies.
Acknowledgments
The authors wish to thank Dessie Health Science College for their financial and administrative support for data collectors. Moreover, we recognize Mr. Getachew G/Mariam, Mr. Andargie Simegne, Mr. Sentayehu Mohammed and all the participants who supported the research.
Disclosure
The authors declared no conflicts of interest.
References
1. Kakemam E, Ghoddoosi-Nejad D, Chegini Z, et al. Knowledge, attitudes, and practices among the general population during COVID-19 outbreak in Iran: A national cross-sectional survey. medRxiv. 2020.
2. Haque T, Hossain KM, Bhuiyan MMR, et al. Knowledge, attitude and practices (KAP) towards COVID-19 and assessment of risks of infection by SARS-CoV-2 among the Bangladeshi population: an online cross sectional survey. 2020.
3. Kumar J, Katto MS, Siddiqui AA, et al. Knowledge, attitude, and practices of healthcare workers regarding the use of face mask to limit the spread of the new coronavirus disease (COVID-19). Cureus. 2020;12(4):e7737–e.
4. Silva O, Palomino S, Robles A, Ríos J, Mayta-Tovalino F. Knowledge, attitudes, and practices on infection control measures in stomatology students in lima, Peru. J Environ Public Health. 2018;2018:8027130. doi:10.1155/2018/8027130
5. World Health O. Critical preparedness, readiness and response actions for COVID-19: interim guidance. Geneva: World Health Organization; 2020 2020. Contract No.: WHO/COVID-19/Community_Actions/2020.1.
6. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752.
7. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E, Tu W-J. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668–e. doi:10.1371/journal.pone.0233668
8. Srichan PAT, Tamornpark R, Yeemard F, et al. Knowledge, attitude and preparedness to respond to the 2019 novel coronavirus (covid-19) among the bordered population of northern thailand in the early period of the outbreak: a cross-sectional study. SSRN Electronic J. 2020. doi:10.2139/ssrn.3546046
9. Haque THK, Bhuiyan M, Ananna S, et al. Knowledge, attitude and practices (KAP) towards COVID-19 and assessment of risks of infection by SARS-CoV-2 among the Bangladeshi population: An online cross sectional survey. 2020.
10. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
11. Zhong B-L LW, Li H-M, Zhang -Q-Q, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752.
12. A GT U, Singh BM, Ram R, Tripti RP. Knowledge, attitudes, and practices towards COVID-19 among Nepalese Residents: A quick online cross-sectional survey. Asian J Medical Sciences. 2020;11(3):6–11.
13. Everett JA, Colombatto C, Chituc V, Brady WJ, Crockett M. The effectiveness of moral messages on public health behavioral intentions during the COVID-19 pandemic. 2020. Available from: https://psyarxiv.com/9yqs8/. doi:10.31234/osf.io/9yqs8
14. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A & Moghadami M. Knowledge, Attitude and Practice toward the Novel Coronavirus (COVID-19) Outbreak: A Population-Based Survey in Iran. [Preprint]. Bull World Health Organ. E-pub: 30 March 2020. doi:10.2471/BLT.20.256651
15. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;1–10.
16. Lee M, You M. Psychological and behavioral responses in South Korea during the early stages of coronavirus disease 2019 (COVID-19). Int J Environ Res Public Health. 2020;17(9):2977. doi:10.3390/ijerph17092977
17. Byanaku AIM. Knowledge, attitudes, and practices (KAP) towards COVID-19: A quick online cross-sectional survey among Tanzanian residents. medRxiv. 2020.
18. Wang CHP, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
19. Van Bavel JJ, Baicker K, Boggio PS, et al. Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour. 2020;1–12.
20. Hussain A, Garima T, Singh BM, Ram R, Tripti RP. Knowledge, attitudes, and practices towards COVID-19 among Nepalese Residents: A quick online cross-sectional survey. Asian J Medical Sciences. 2020;11(3):6–11. doi:10.3126/ajms.v11i3.28485
21. Rios-González CM. Knowledge, attitudes and practices towards COVID-19 in Paraguayans during outbreaks: a quick online survey. 2020. doi:10.1590/SciELOPreprints
22. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744–e. doi:10.1371/journal.pone.0233744
23. Salman M, Mustafa ZU, Asif N, et al. Knowledge, attitude and preventive practices related to COVID-19: a cross-sectional study in two Pakistani university populations. Drugs Ther Perspect. 2020;1–7.
24. White MS, Omer M, Mohammad GN. Knowledge, attitude and practice on prevention of airborne and droplet infections during the outbreak of corona virus among the College Students in University of Bisha, Saudi Arabia. Int J Contemporary Research Review. 2020;11(04):6–20773.
25. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward covid-19 among the public in the kingdom of saudi arabia: a cross-sectional study. Front Public Health. 2020;8:217. doi:10.3389/fpubh.2020.00217
26. Gallè F, Sabella EA, Da Molin G, De Giglio O, Caggiano G, Di Onofrio V, et al. Understanding Knowledge and Behaviors Related to CoViD-19 Epidemic in Italian Undergraduate Students: The EPICO Study. Int J Environ Res Public Health. 2020;17(10):3481.
27. Huynh TLD. Does culture matter social distancing under the COVID-19 pandemic? Saf Sci. 2020;130(p):104872. doi:10.1016/j.ssci.2020.104872
28. Huynh TLD. The COVID-19 containment in Vietnam: what are we doing? J Glob Health. 2020;10(1):
29. Huynh TLD. Data for understanding the risk perception of COVID-19 from Vietnamese sample. Data in Brief. 2020;30:
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.