Back to Journals » Infection and Drug Resistance » Volume 15
Lessons Learned from the Ebola Virus Disease and COVID-19 Preparedness to Respond to the Human Monkeypox Virus Outbreak in Low- and Middle-Income Countries
Authors Tusabe F ![]() , Tahir IM
, Tahir IM ![]() , Akpa CI, Mtaki V, Baryamujura J, Kamau B, Lidoroh S, Kobugabe PL, Maaga NO
, Akpa CI, Mtaki V, Baryamujura J, Kamau B, Lidoroh S, Kobugabe PL, Maaga NO ![]() , Bongomin F
, Bongomin F ![]()
Received 30 July 2022
Accepted for publication 8 October 2022
Published 28 October 2022 Volume 2022:15 Pages 6279—6286
DOI https://doi.org/10.2147/IDR.S384348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Fred Tusabe,1 Imtiaz Mahmood Tahir,2 Chijioke Igwe Akpa,3 Victor Mtaki,4 Jovan Baryamujura,5 Beatrice Kamau,6 Sharon Lidoroh,7 Penlope Lillian Kobugabe,8 Nathan Okemwa Maaga,9 Felix Bongomin10
1Global Health Security Department, Infectious Diseases Institute, Makerere University, Kampala, Uganda; 2College of Allied Health Professionals, Faculty of Medical Sciences, Government College University, Faisalabad, Pakistan; 3Surveillance and Epidemiology Department, Nigeria Centre for Disease Control (NCDC), Abuja, Nigeria; 4Medical Laboratory Department, Baylor College of Medicine Children’s Foundation, Mwanza, Tanzania; 5Global Health Security Department, Baylor College of Medicine Children’s Foundation, Kampala, Uganda; 6Health Services Department, Nairobi County, Nairobi, Kenya; 7Public Health Department, Africa Centers for Disease Control and Prevention (Africa CDC), Addis Ababa, Kenya; 8Counselling Department, Makerere University-John Hopkins Research Collaboration, Kampala, Uganda; 9Department of Diagnostics, Ministry of Health, Kisii County Government, Nairobi, Kenya; 10Department of Medical Microbiology & Immunology, Gulu University, Gulu, Uganda
Correspondence: Fred Tusabe, Tel +256 777317065, Email [email protected]
Abstract: Recently, the World Health Organization (WHO) declared the human monkeypox virus disease an international health emergency. In the past decades, infectious disease epidemics have significantly impacted low- and middle-income countries (LMICs), with coronavirus disease-2019 (COVID-19) being the most recent. LMICs, particularly in Africa and Asia, responded reasonably well by strengthening health systems, including infection prevention and control strategies, laboratory systems, risk communication, and training of essential healthcare workers for surge capacity in preparation for and response to COVID-19. With the possibility of other epidemics, such as the current epidemic of human Monkeypox, a consolidated global response is required. This article discusses lessons learned from previous Ebola and COVID-19 outbreaks and also provides recommendations on how these lessons can be useful to strengthen monkeypox disease outbreak preparedness and response in LMIC.
Keywords: COVID-19, Ebola virus disease, low-middle income countries, health system, preparedness, monkeypox, epidemic
Introduction
Some epidemics such as Ebola virus disease (EVD) which was first identified in 1976 have occurred 29 times with case fatality rates ranging from 25% to 90%1 with the current outbreak being of the Sudan ebolavirus in Mubende district central part of Uganda.2 Ebola virus disease is primarily transmitted through direct patient contact and contact with infectious body fluids3 comparable to the transmission of the species, severe acute respiratory syndrome-related coronavirus (SARS-CoV2) that has been associated with three primary modes known as “contact” “droplet” and “airborne” transmission.4
Epidemics and pandemics of infectious diseases have been documented for many centuries.5 The most recent pandemic is the ongoing coronavirus disease – 2019 (COVID-19), which has infected over 500 million people and killed nearly 6.5 million worldwide.6 COVID-19 infections are currently experiencing a global decline in prevalence.7
However, other emerging and re-emerging infectious diseases, 60% of which originate from animals (zoonotic), such as monkeypox disease, are on the rise worldwide.8
Monkeypox is a zoonosis, thus an animal-to-human disease transmitted primarily by monkeys and Rodentia.9 Since 1958, the human monkeypox virus (MPV) has been identified and has predominantly occurred in West and Central Africa.9 In 1970, a nine-year-old boy in Zaire (now the Democratic Republic of the Congo) was the first person to be diagnosed with human Monkeypox.9 It became endemic in the tropical rainforests of central and western Africa, where eleven nations have reported cases.9 In June 2003, the virus was detected for the first time outside of Africa in the United States of America (USA). The Centers for Disease Control and Prevention (CDC) reported 87 cases with no fatalities at the time.10
According to the World Health Organization (WHO), there was a significant outbreak of Monkeypox disease in Nigeria in 2017, with more than 200 confirmed cases and a mortality rate of approximately 3%.11 Since 2017, sporadic cases have been reported worldwide among travellers arriving from Nigeria, particularly in the United Kingdom, Israel, Singapore, and the United States. May 2022 witnessed a deluge of cases identified in non-African nations among individuals without travel ties to the region.9
Transmission of Human Monkeypox Virus
The MPV spreads in ways comparable to Ebola virus and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) responsible for EVD and COVID-19 disease respectively.3 Direct contact with the infectious rash, scabs, or body fluids, including respiratory secretions, as well as touching items (such as clothing or linens) that have previously come into contact with the infectious rash or body fluids, are all means of transmission of MPV.12 Pregnant mothers can transmit the MPV through the placenta to their unborn children. Additionally, it is possible for humans to contract the monkeypox virus from infected animals, either by being scratched or bitten, consuming infected animals, or using animal products. From the onset of symptoms until the rash has completely healed and a new layer of skin has formed, Monkeypox can spread. The illness typically lasts between 14 and 28 days. Those without symptoms of Monkeypox cannot transmit the virus to others. At this time, additional research is being conducted to rule out the spread of Monkeypox through sperm or vaginal fluids.13 Most cases have been reported in Europe (Spain and Germany), the United Kingdom, and the United States of America (USA)14 as shown in Figure 1.
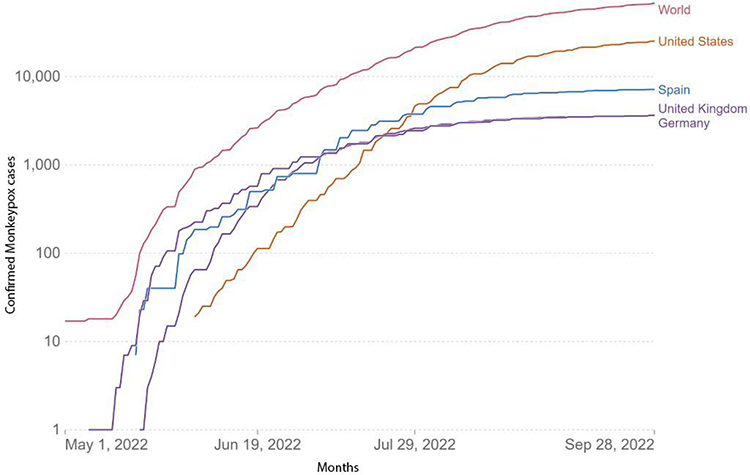 |
Figure 1 Countries with the highest number of Monkeypox Infections. As of 30th Sept 2022, 7188 cases have been confirmed for Spain, 3625 for Germany, 3635 for the United Kingdom and 5434 for the USA. Adapted from: Mathieu E, Spooner F, Dattani S, Ritchie H, Roser M. Monkeypox. Our World in Data [Internet]; 2022. Available from: https://ourworldindata.org/monkeypox.14 |
Clinical Features of Human Monkeypox Virus Infection
The incubation period for Monkeypox is typically between 6 and 13 days but can range between 5 and 21 days. The immediate symptoms of an infection with Monkeypox are headache, fever, muscle pain, lymph node enlargement, and back pain.15 Skin fluorescence refers to observable skin changes in certain instances. Depending on the disease’s progression, these skin changes resemble chickenpox or syphilis. There may be nodules, blisters, or pustules. Typically, they begin on the face and then spread to other body parts, such as the legs and arms (Figure 2). Some of the cases reported in May 2022 also involved genitourinary skin lesions.16
 |
Figure 2 A visual example of Monkeypox rash. The rash is in form of lesions that are the commonest sign of Monkeypox disease. These evolve in four stages; Macular (a flat lesion), Papular (an elevated lesion), Vesicular (a fluid-filled lesion) and Pustular (an inflamed, pus-filled lesion) after that, they scab and flake. Photo Credit: NHS England High consequence Infectious Diseases Network. Adapted from Centers for Disease Control and Prevention. Monkeypox in the US [Internet]; 2022. Available from: https://www.cdc.gov/poxvirus/monkeypox/transmission.html.12 |
Then again, even when the virus is not highly contagious or infectious, it can cause severe health complications in some people. These complications worsen in people with an immunosuppressed system or undergoing chemotherapy, increasing the hospitalization rate. These include chest infections, neurological complications such as encephalitis, sepsis, and even eye infections and blindness.15
Treatment of Human Monkeypox Virus
There are currently no approved treatments for monkeypox virus infections. Given that monkeypox and smallpox viruses are genetically identical, antiviral drugs and vaccines developed to protect against smallpox can be used to prevent and treat infections caused by the monkeypox virus. Antivirals such as tecovirimat (TPOXX) are recommended for immunocompromised patients and others who are more susceptible to severe illness.17
Global Distribution of Monkey Pox Infections
On 23 July 2022, the World Health Organization (WHO) declared the ongoing global outbreak of Monkeypox to be an international emergency (PHEIC)18 that has grown to nearly 70,000 cases and 27 deaths across 106 countries as of October 01, 2022. About 68,430 people in 106 countries have been diagnosed with Monkeypox and out of these cases, 67,741 come from non-endemic countries (n=99) and 689 cases from endemic countries (n=7) (Figure 3).19
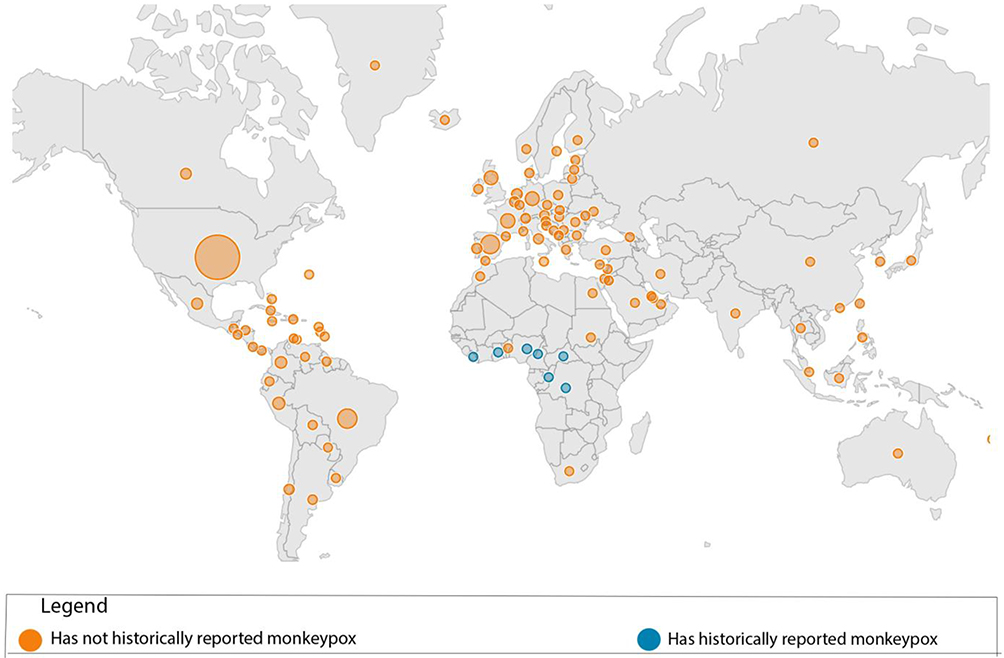 |
Figure 3 Countries with and without having reported Monkeypox infections. These data have been reported since January 1, 2022, and provide for situational awareness and are subject to change. Confirmed cases include those laboratory-confirmed as monkeypox virus (MPX) and may include cases only confirmed as orthopoxvirus. Among locations (including countries, territories, and areas) that have not historically reported MPX, several have reported sporadic cases linked to travel or imported animals before 2022. Additionally, Ghana has not historically reported MPX cases, however, the country was identified as the source of a shipment of wild mammals that subsequently led to the 2003 outbreak in the US. Adapted from Centers for Disease Control and Prevention. Monkeypox in the U.S; 2022. Available from: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html.19 |
Lessons Learned from the Ebola and COVID-19 Epidemics
We discuss the lessons learned from the Ebola epidemics and COVID-19 in LMIC and highlight relevant strategies to strengthen public health and responses to the ongoing monkeypox outbreak. To prevent the Monkeypox outbreak from escalating into a pandemic, six core interventions must be implemented, just as they were during the EVD and COVID-19 preparedness and response: Infection prevention and control strategies, laboratory systems, Rapid data sharing and risk communication, and training of critical healthcare workers for surge capacity, effective systems for identifying emerging and re-emerging infectious diseases and advancing drug and vaccine manufacturing capacity.
The identification of emerging and re-emerging infectious diseases requires an efficient system. During the Ebola outbreak in the Democratic Republic of the Congo and west Africa, surveillance and contact tracing were enforced with the participation of national, private, and partner stakeholders. This determined the contact rate between infected and susceptible individuals within distinct populations. Additionally, the WHO recommends effective contact tracing to prevent human-to-human transmission of monkeypox infections.20 Some LMICS have mathematical disease modeling and diagnostic systems (local/regional) to aid in early detection, including zoonotic spillovers.21 During the 2014 Ebola outbreak in West Africa, post-outbreak zoonotic niche models demonstrated that the risk of Ebola transmission in West Africa was comparable to that of central Africa, where all previous Ebola outbreaks had occurred.21 This data suggested that the region’s susceptibility to the Ebola outbreak was predictable before identifying the index cases.
Some LMICs have expanded their laboratory capacities to manage testing for COVID-19 on a large scale using nucleic acid amplification technology (NAAT). Other significant players, such as private and academic laboratories, have supported government initiatives. Likewise, a case from Uganda facilitated the transition to COVID-19 testing by leveraging existing laboratory capabilities developed during Ebola preparedness.22
The same laboratory capacity could be utilized for diagnosing Monkeypox. For instance, Nigeria could leverage investments in surge capacity during the immediate wake of the COVID-19 pandemic to expand its functional public health laboratory network from 12 laboratories to 77 fully equipped and functional laboratories capable of testing at varying capacities. On November 24, 2021, a new SARS Cov2 variant B.1.1.529, 20K (Omicron) was identified for the first time in South Africa, demonstrating the capabilities of gene sequencing.23
Responders must practice proper Infection Prevention and Control and have a comprehensive case management plan that includes isolation and treatment. Infection, prevention, and control (IPC) guidelines must be developed in collaboration with the ministries of health, animal and water, and the environment, employing the “One Health” approach, which has been a buzzword but never put into practice. In response to the Ebola virus, countries initiated the IPC cascade, standardizing training curricula and enforcing modifications for resilient health security at entry points, hospitals, and community sites which cabbed the further spread of infections.24 Notably, there have been sustainable global investments geared towards improving hand hygiene practices,25 and various non-pharmaceutical measures, such as social distancing, have been tested with positive results in reducing the rate of infection transmission26 that could be leveraged to stop the escalation of Monkeypox Infections.
In addition to preventing and diagnosing infections, drug manufacturing must be improved in LMICs. Before the COVID-19 Pandemic, most LMICs had little or no ability to make medical tools, diagnostics, or reagents in-country, so they had to import many of them. The closed borders made it hard for the country to get the medical countermeasures and diagnostics it needed to fight COVID-19.27,28 For political economies and transnationalism, governments have made efforts to build capacity for drug development and improve research capacities to comprehend the social pathways of transmission of emerging and re-emerging infectious diseases, as well as the challenges and opportunities for international collaboration to combat the disease.29 Twelve vaccine production facilities in six countries (Algeria, Senegal, Egypt, Morocco, Rwanda, and South Africa) are anticipated to produce a vast array of COVID-19 vaccines. Through the implementation of the Partnership for African Vaccine Manufacturer (PAVM) framework for Action 2022, technology transfer on mRNA vaccines has been established. South Africa and Kenya Biovax Institute have already signed a memorandum of understanding. These facilities should be utilized to create antivirals and vaccines for endemic diseases like monkeypox. Jynneos, the only vaccine approved to prevent monkeypox, could be manufactured in LMICs for equitable access.30 The CDC vaccination campaign relies on the two-dose Jynneos, which the FDA approved in 2019 for adults 18 and older at high risk of monkeypox or smallpox infection.
Even if the aforementioned measures are in place, misinformation and infodemics within communities could impede intervention efforts in the absence of effective risk communication.31 Most LMICs were able to activate their risk communication and community engagement plans during the peak of the COVID-19 pandemic. The majority of Ugandans were able to obtain information on the symptoms, transmission, and nature of COVID-19, according to a UNICEF assessment.32
Following reputable information sources such as Non -Govermental Organizations (NGOs) in the health sector, the Ministry of Health, and United Nations agencies, healthcare professionals and village health teams were the most recommended. However, the most preferred communication channels were radio, virtual platforms, television, and loudspeakers.32 Due to a history of trust, influential community leaders such as traditional rulers and faith leaders should be employed to disseminate monkeypox information to locals in most LMICs. Similarly, this strategy proved to be highly effective for the pandemic response and can therefore be explored further for monkeypox outbreaks.31
In Nigeria, where numerous indigenous languages exist, information, education, and communication (IEC) materials have been translated into these languages to facilitate optimal comprehension among the country’s diverse tribes. In addition, community health care workers and volunteers need training in Infection Prevention and Control (IPC) and hand washing techniques, which they should promote and advocate for within their respective communities.
It is nearly impossible for a single sector to lead the preparedness and response to a zoonotic outbreak, so this fight should be a multisectoral collaboration. Some countries have mobilized financial resources from different sectors; the National Treasury, multilateral organizations such as the World Bank Group, and bilateral organizations to support the COVID-19 emergency response. Nigeria successfully established arevolving outbreak investigation Fund on the timeliness of outbreak responses in 2019; the fund has supported responses to 14 outbreaks, including Monkeypox. Further, Regional nodes, including emergency operations centers, should be established for stockpiling and prepositioning supplies using a multisectoral approach to ensure timely access to supplies during crises.
Therefore, there must be a close collaboration between human and veterinary public health authorities to manage exposed pets and prevent transmission to wildlife
states the Rapid Risk Assessment.8 In addition, there is a global campaign to equip field epidemiologists to serve as national/regional responders during disease outbreaks. This should be carried out in a multisectoral plan by all One Health Ministries, including the Ministry of Health (MoH), Ministry of water and environment (MWE), Ministry of Agriculture, Animal Industry and Fisheries (MAAIF), and Ministry of Tourism, Wildlife and Antiquities (MTWA).33
Gaps and Recommendations
This plan is informed by the lessons learned from the Ebola virus disease and COVID-19 outbreaks and acknowledges International Health Regulations (IHR). Despite the favourable response, there were implementation challenges and gaps that may include;
- In countries such as Kenya, Uganda, and the Democratic Republic of the Congo, the militarization of the public health response to epidemics eroded community trust significantly. Monkeypox is endemic in Africa, but no disease modeling studies have been conducted to prepare the rest of the world, nor have any therapeutics been developed based on its content. This response should not be militarized; instead, budgets should be allocated for research and innovation to foster natives’ trust.
- Policymaking procedure, obstacles to transnational cooperation, and power dynamics; Inadequate political leadership combined with info-demic, sometimes with deliberate misinformation in some countries, denied the evidence, with severe global repercussions as an illustration. For example in point, Tanzania denied the existence of COVID-19 during the presidency of the late Magufuli.34 During the response to outbreaks of monkeypox, there is a need to bolster the role of global public health institutions in each nation.
- Emerging and re-emerging pathogens, such as SARS, COV-2, and EBV, are highly transmissible via respiratory routes and have the potential to cause severe and fatal diseases. These presented a steep learning curve and were difficult to manipulate. Severe respiratory diseases necessitate intensive care, for which LMICs have limited capacity. This necessitates that each nation has a revised monkeypox response plan, which may not be as fatal as EVD. According to the UK Public Health Rapid Support Team, reliance on societal level interventions such as “lockdowns” could have severe economic, mental, and other health consequences.
- Africa has reported 4667 cases of Monkeypox infections in 13 countries as of September 22, including 559 laboratory-confirmed cases in nine countries.35 Despite the laboratory capabilities in some countries, generally in Africa, diagnostic methods are limited out of the six used globally. Budgetary allocations for enhancing diagnostics, training of human resources, and international accreditation should motivate and encourage initiatives of this nature.
- Elimination of monkeypox disease-related stigma and discrimination is also important to discuss as with Ebola and COVID-19. This can be enhanced through effective communication via social media and other platforms with the ability to fight conspiracists and increase disease surveillance.
Conclusion
Monkeypox disease is a painful reminder that endemic infectious diseases may pose a significant global threat.
Lessons from the Ebola outbreak and COVID −19 pandemic should be put into action to enable countries to respond swiftly to the monkeypox outbreak. Those at high risk of contracting the monkeypox virus must be vaccinated, but there has been no vaccination call for the mass Population at risk such as immunocompromised and Healthcare workers. During the COVID-19 vaccine rollout in developed countries, LMICs watched from the sidelines as other countries vaccinated their populations despite limited supplies; such a situation should not be allowed to erupt.
Although LMICs have improved their ability to handle outbreaks and emergencies, this improvement is not huge hence the need for more improvement. LMIC should strengthen their coordination of response to epidemics so that healthcare facilities are not overwhelmed and also create more support systems for research, data sharing through social media, magazines, and sample delivery/transfer.
Further, community systems need to be strengthened to support quick and efficient responses during Epidemics with emphasis on health promotion. Despite healthcare system capabilities in LMIC, additional support is required to expand the manufacturing of vaccines antivirals, disinfectants and antiseptics with competitive pricing and non-wasteful systems, as well as the need for a balance between control measures and access to life-sustaining supplies, including food security.
Lastly, the current Field Epidemiologist training program must establish national early warning systems for disease threats and national and international teams responsible for preparing nations and coordinating responses to regional outbreaks before they become pandemics.
Acknowledgments
The authors thank all lecturers of the Pandemics course at the London School of Hygiene and Tropical Medicine.
Funding
No funding associated with this work.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Coltart CEM, Lindsey B, Ghinai I, Johnson AM, Heymann DL. The Ebola outbreak, 2013–2016: old lessons for new epidemics. Philos Trans R Soc Lond B Biol Sci. 2017;372(1721):20160297. doi:10.1098/rstb.2016.0297
2. Uganda declares Ebola virus disease outbreak [Internet]. WHO | Regional Office for Africa; [cited September 30, 2022]. Available from: https://www.afro.who.int/countries/uganda/news/uganda-declares-ebola-virus-disease-outbreak.
3. Osterholm MT, Moore KA, Kelley NS, et al. Transmission of Ebola viruses: what we know and what we do not know. MBio. 2015;6(2):e00137–15.
4. Choudhary OP, Singh I, Patra G. Aerosol transmission of SARS-CoV-2: the unresolved paradox. Travel Med Infect Dis. 2020;37:101869.
5. VM Anantha Eashwar. Epidemics and pandemics in India throughout history: a review article. Indian J Public Health Res Dev. 2019;10(8).
6. Weekly epidemiological update on COVID-19—20 April 2022. (n.d.). Available from https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---20-april-2022.
7. Weekly epidemiological update on COVID-19 - 14 September 2022 [Internet]; [cited September 30, 2022]. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---14-september-2022.
8. Baker RE, Mahmud AS, Miller IF, et al. Infectious disease in an era of global change. Nat Rev Microbiol. 2022;20(4):193–205. doi:10.1038/s41579-021-00639-z
9. Monkeypox timeline: from beginnings in Africa to global spread [Internet]. The Star; [cited July 25, 2022]. Available from: https://www.thestar.com.my/lifestyle/health/2022/07/25/monkeypox-timeline-from-beginnings-in-africa-to-global-spread.
10. Monkeypox [Internet]; [cited July 25, 2022]. Available from: https://www.who.int/news-room/fact-sheets/detail/monkeypox.
11. Monkeypox – Nigeria [Internet]; [cited July 25, 2022]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/05-october-2018-monkeypox-nigeria-en.
12. CDC. Monkeypox in the U.S. [Internet]. Centers for Disease Control and Prevention; 2022 [cited July 25, 2022]. Available from: https://www.cdc.gov/poxvirus/monkeypox/transmission.html.
13. Monkeypox [Internet]. [cited October 2, 2022]. Available from: https://www.who.int/news-room/questions-and-answers/item/monkeypox.
14. Mathieu E, Spooner F, Dattani S, Ritchie H, Roser M. Monkeypox. Our World in Data [Internet]; 2022 May 24 [cited October 2, 2022]. Available from.: https://ourworldindata.org/monkeypox.
15. CDC. Monkeypox in the U.S. [Internet]. Centers for Disease Control and Prevention; 2022 [cited September 30, 2022]. Available from: https://www.cdc.gov/poxvirus/monkeypox/resources/graphics.html.
16. Shafaati M, Zandi M. Monkeypox virus neurological manifestations in comparison to other orthopoxviruses. Travel Med Infect Dis. 2022;49:102414. doi:10.1016/j.tmaid.2022.102414
17. CDC. Monkeypox in the U.S. [Internet]. Centers for Disease Control and Prevention. 2022 [cited October 2, 2022]. Available from.: https://www.cdc.gov/poxvirus/monkeypox/clinicians/treatment.html.
18. The second meeting of the International Health Regulations (2005) (IHR) emergency committee regarding the multi-country outbreak of Monkeypox [Internet]; [cited July 25, 2022]. Available from: https://www.who.int/news/item/23-07-2022-second-meeting-of-The-international-health-regulations-(2005)-(ihr)-emergency-committee-regarding-The-multi-country-outbreak-of-monkeypox.
19. CDC. Monkeypox in the U.S. [Internet]. Centers for Disease Control and Prevention; 2022 [cited October 2, 2022]. Available from: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html.
20. Surveillance, case investigation and contact tracing for Monkeypox: interim guidance [Internet]. [cited July 25, 2022]. Available from: https://www.who.int/publications-detail-redirect/WHO-MPX-Surveillance-2022.2.
21. Pigott DM, Golding N, Mylne A, et al. Mapping the zoonotic niche of Ebola virus disease in Africa. eLife. 2014;3:e04395. doi:10.7554/eLife.04395
22. Naluyima P, Kayondo W, Ritchie C, et al. The Joint Mobile Emerging Disease Clinical Capability (JMEDICC) laboratory approach: capabilities for high-consequence pathogen clinical research. PLoS Negl Trop Dis. 2019;13(12):e0007787.
23. Oladipo EK, Ajayi AF, Odeyemi AN, et al. Laboratory diagnosis of COVID-19 in Africa: availability, challenges and implications. Drug Discov Ther. 2020;14(4):153–160.
24. Aceng JR, Ario AR, Muruta AN, et al. Uganda’s experience in Ebola virus disease outbreak preparedness, 2018–2019. Global Health. 2020;16(1):1–12.
25. Berendes D, Martinsen A, Lozier M, et al. Improving water, sanitation, and hygiene (WASH), with a focus on hand hygiene, globally for community mitigation of COVID-19. PLOS Water. 2022;1(6):e0000027.
26. Zheng Q, Jones FK, Leavitt SV, et al. HIT-COVID, a global database tracking public health intervention to COVID-19. Sci Data. 2020;7(1):1–8.
27. Simpson S, Kaufmann MC, Glozman V, Chakrabarti A. Disease X: accelerating the development of medical countermeasures for the next pandemic. Lancet Infect Dis. 2020;20(5):e108–15.
28. World Health Organization. SARS-CoV-2 antigen-detecting rapid diagnostic tests: an implementation guide; 2020.
29. Lee VJ, Aguilera X, Heymann D, et al. Preparedness for emerging epidemic threats: a Lancet infectious diseases commission. Lancet Infect Dis. 2020;20(1):17–19.
30. Jynneos. FDA [Internet]; 2021 Jun 21 [cited July 25, 2022]; Available from: https://www.fda.gov/vaccines-blood-biologics/jynneos.
31. Matta G. Science communication as a preventative tool in the COVID19 pandemic. Humanit Soc Sci Commun. 2020;7(1):1–14.
32. UNICEF Uganda COVID-19 situation report 1–15 June 2020 | UNICEF Uganda [Internet]. [cited April 28, 2022]. Available from: https://www.unicef.org/uganda/reports/unicef-uganda-covid-19-situation-report-1-15-june-2020.
33. World Health Organization. Taking a multisectoral one health approach: a tripartite guide to addressing zoonotic diseases in countries. Food & Agriculture Org.; 2019.
34. Magufuli J: The cautionary tale of the president who denied coronavirus [Internet]. BBC News. [cited September 30, 2022]. Available from: https://www.bbc.com/news/world-africa-56412912.
35. Monkeypox cases still on the rise: Africa to be watchful [Internet]. Forbes Africa; 2022 [cited July 25, 2022]. Available from.: https://www.forbesafrica.com/health/2022/07/22/monkeypox-cases-still-on-The-rise-africa-to-be-watchful/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.