Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 18
Lenacapavir at the Spatiotemporal Limit: Tissue Pharmacokinetics, Pharmacokinetic Tail Dynamics, and the Emergence of Capsid Resistance in Long-Acting HIV Prevention
Authors Chris-Uchendu HC ![]() , Olwit G
, Olwit G ![]() , Atuhaire A, Matovu I, Kirumira HN, Sasiita PK, Odongo L
, Atuhaire A, Matovu I, Kirumira HN, Sasiita PK, Odongo L ![]() , Mutekanga A, Nkwanga J
, Mutekanga A, Nkwanga J
Received 7 May 2026
Accepted for publication 17 June 2026
Published 19 June 2026 Volume 2026:18 622588
DOI https://doi.org/10.2147/CPAA.S622588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Arthur E. Frankel
Hans Chinomso Chris-Uchendu,1 Gerald Olwit,2 Arnold Atuhaire,3 Isaac Matovu,2 Hope Nakakande Kirumira,4 Patrick Kambale Sasiita,2 Leo Odongo,3,5 Andrew Mutekanga,2 Jacob Nkwanga2
1Department of Surgery, School of Medicine, Kabale University, Kabale, Uganda; 2Department of Internal Medicine, School of Medicine, Kabale University, Kabale, Uganda; 3Department of Obstetrics and Gynaecology, Kabale University School of Medicine, Kabale, Uganda; 4Department of Nursing Science, School of Medicine, Kabale University, Kabale, Uganda; 5Department of Dermatology, Allergology, and Venereology, Kabale University School of Medicine, Kabale, Uganda
Correspondence: Hans Chinomso Chris-Uchendu, Department of Surgery, School of Medicine, Kabale University, P.O.Box 317, Kabale, Uganda, Tel +256 766607269, Email [email protected] [email protected]
Background: Lenacapavir (LEN), a first-in-class HIV-1 capsid inhibitor administered subcutaneously twice yearly, has demonstrated near-perfect efficacy in Phase 3 trials, generating justified enthusiasm for its potential to reconfigure HIV prevention. However, its revolutionary success obscures critical spatiotemporal vulnerabilities. We critically examined the protective envelope of LEN, specifically focusing on the gap between systemic pharmacokinetics (PK) and mucosal distribution, the dynamics of the prolonged PK tail, and the clinical emergence of capsid resistance.
Methods: A systematic narrative synthesis was conducted through April 2026. We integrated screening and data parameters from the PURPOSE and CAPELLA trials alongside advanced PK-PD modeling and structural biology datasets to comprehensively map the spatiotemporal parameters of lenacapavir-based PrEP.
Findings: We characterize the Limitations of Systemic Surrogacy, highlighting that no published empirical data exist characterizing LEN concentrations in human mucosal sanctuary sites; the sole registered tissue distribution trial (Pro00043856) remains unpublished four years post-registration. While modeling baseline assumptions establish a wild-type 95% preventive plasma concentration (EC95) of 5.8 ng/mL, the terminal absorption-limited elimination phase creates a definitive 106– 235 day Mutant Selection Window (MSW) following drug discontinuation. Based on the 58 studies included in the full synthesis, falling sub-therapeutic drug concentrations during this tail phase exert selective pressure that favors high-fitness capsid substitutions (eg, Q67H), lowering the genetic barrier for complex, high-level resistance mutations (eg, N74D). Clinical breakthrough infections observed across the CAPELLA trial (19%) and rare PURPOSE infections (0.07 per 100 person-years) validate this corridor of vulnerability, highlighted by a recorded seroconversion occurring 16 months post-injection.
Conclusion: Optimizing the public health impact of lenacapavir requires transitioning from simple serum-based monitoring toward tissue-informed clinical stewardship. Unlike conventional oral PrEP, twice-yearly lenacapavir involves an extended pharmacological commitment of nearly 12 months, requiring pre-planned clinical protocols for bridging therapy during drug discontinuation. Implementation requires the evaluation of high-sensitivity viral surveillance tools (LOD ≤ 10 copies/mL) and global access reconfigurations to resolve the economic and licensing barriers separating low-cost generic synthesis from international list prices, protecting the long-term viability of the capsid inhibitor class across all implementation sectors. A flowchart detailing three phases: active prophylaxis, discontinuation and clinical stewardship.
Keywords: lenacapavir, HIV pre-exposure prophylaxis, pharmacokinetics, drug resistance, viral, global health equity, capsid inhibitor, area under curve
Introduction
The Promise of Long-Acting HIV Prevention
Globally, 1.3 million new HIV infections occurred in 2023, with 39.9 million people living with HIV and 630,000 HIV‑related deaths.1,2 Daily oral tenofovir‑based pre‑exposure prophylaxis (PrEP) reduces HIV acquisition risk by approximately 99% when taken as prescribed, yet global uptake remains far below UNAIDS targets: by 2023, only 3.5 million people had used PrEP at least once, against a 2025 target of 21.2 million individuals at substantial risk.3,4 Adherence, the Achilles’ heel of oral PrEP, is particularly challenging for young women in sub‑Saharan Africa and other key populations facing structural barriers to daily pill‑taking.3,5 This regional context underscores the critical biological and structural vulnerabilities of adolescent girls and young women in high-incidence settings, emphasizing the need for discrete, female-controlled biomedical prevention options.5 Long‑acting injectable formulations offer a paradigm shift, uncoupling prevention from daily behavior and potentially closing the adherence gap.3 The success of cabotegravir long‑acting PrEP in the HPTN 083 and 084 trials established proof‑of‑concept for bimonthly injectable prevention.3 Lenacapavir, the first‑in‑class HIV‑1 capsid inhibitor administered subcutaneously every six months, represents the next frontier in this evolution.6
Lenacapavir: A First-in-Class Capsid Inhibitor
Lenacapavir (GS-6207) received its first regulatory approval in the European Union on August 22, 2022, followed by U.S. Food and Drug Administration (FDA) approval on December 22, 2022, for the treatment of heavily treatment-experienced adults with multidrug-resistant HIV-1 in combination with other antiretrovirals.7–9 Subsequently, on the basis of the PURPOSE 1 and PURPOSE 2 trials, the FDA approved lenacapavir (brand name Yeztugo) for HIV pre‑exposure prophylaxis (PrEP), making it the first and only FDA-approved HIV prevention option offering six months of protection per subcutaneous injection.10,11
The drug binds at a highly conserved interface between subunits of capsid hexamers, a site critical for both the orderly assembly of new virions and the interaction with host cell factors that mediate nuclear import of the viral genome.6 This conserved binding site renders the capsid an attractive target with minimal pre‑existing drug resistance in treatment‑naïve populations.6,12 Lenacapavir exhibits sub‑nanomolar potency in target cells, with an EC50 of 23 pM in a full‑cycle assay and EC50 values ranging from 21 to 115 pM across diverse HIV‑1 subtypes (A1, AE, AG, B, C, D, F1, G, H), confirming its pan‑genotypic activity.13,14
Beyond its antiviral potency, lenacapavir possesses a unique pharmacologic profile ideally suited for long‑acting formulation. The drug shows exceptionally low systemic clearance following intravenous administration in nonclinical species and humans.13 Formulated as an aqueous suspension for subcutaneous injection, lenacapavir exhibits two‑phase absorption kinetics, an initial fast‑release phase followed by a slow‑release phase, resulting in “flip‑flop” pharmacokinetics where the input rate from the injection depot is substantially slower than the systemic elimination rate.13,15 This property prolongs the apparent terminal half‑life to approximately 10–12 weeks in humans, enabling dosing intervals of up to 26 weeks.15 The combination of high potency, exceptional stability, and optimal release rate from the injection depot makes lenacapavir well suited for a parenteral long‑acting formulation that can be administered once every six months for the prevention and treatment of HIV‑1.13
Importantly, lenacapavir has no known cross‑resistance with other antiretroviral drug classes, including nucleoside reverse transcriptase inhibitors, non‑nucleoside reverse transcriptase inhibitors, protease inhibitors, integrase strand transfer inhibitors, and entry inhibitors.16 This property preserves future treatment options for individuals who acquire lenacapavir‑resistant HIV while receiving PrEP or develop resistance during treatment, a critical consideration for public health implementation.3
The Spatiotemporal Paradox: Why Tissue, Time, and Resistance Matter, and the Failure of Serum Surrogacy
Despite lenacapavir’s remarkable efficacy in clinical trials, demonstrating near-perfect protection with an incidence of 0.07 per 100 person-years in PURPOSE 1 and 99.9% efficacy in PURPOSE 2, the published evidence base reveals a crisis of surrogacy.17,18 Nearly all pharmacokinetic (PK) data derive from serum or plasma measurements, yet the primary sites of HIV acquisition are mucosal tissues (female genital tract, male colorectal mucosa). For decades, traditional HIV prevention has relied on the assumption that plasma concentrations predict protection; however, lenacapavir’s unique compartmental properties render this assumption an area that warrants careful empirical evaluation.
First, the drug’s extraordinary half-life (8–12 weeks) following subcutaneous administration creates a prolonged pharmacokinetic tail during which concentrations decline slowly.13,15 Second, the tail coincides with a “mutant selection window” where sub‑therapeutic levels may select for capsid resistance. An integrated PK-PD model has shown that de novo resistance emergence is possible once lenacapavir concentrations fall below 10 ng/mL after the last injection, with a temporal window of vulnerability lasting up to 235 days depending on the mutation.1 Third, the absence of human mucosal PK data means we are biologically blind to whether protective concentrations ever reach the portal of viral entry. The sole clinical trial designed to evaluate lenacapavir distribution into rectal and female genital tract tissues (Gilead Sciences study GS‑US‑528‑5744, Pro00043856) was registered, but its results remain unpublished.19
This triad of tissue distribution gaps, tail pharmacokinetics, and resistance selection mechanics defines the spatiotemporal boundaries of lenacapavir’s protective envelope. This review posits that traditional plasma‑based monitoring should be augmented with tissue‑informed PK‑PD frameworks and evidence-based discontinuation protocols. Reflecting these risks, regulatory guidance recommends that if lenacapavir is discontinued, a fully suppressive alternative antiretroviral regimen should be initiated no later than 28 weeks after the final injection to minimize the risk of selecting for resistant variants.8
Review Objective and Scope
This narrative review synthesizes published peer-reviewed literature to address three interconnected questions: (1) What is known, and what remains unknown, about lenacapavir distribution into mucosal tissues relevant to HIV acquisition? (2) How does the pharmacokinetic (PK) tail create a window of vulnerability for resistance selection, and what PK-PD models predict about the duration of this window? (3) What is the clinical and epidemiological significance of lenacapavir-associated capsid resistance mutations for PrEP implementation?
Lenacapavir’s exceptional efficacy in clinical trials underscores the importance of characterizing its spatiotemporal boundaries at the mucosal portal of entry, within the prolonged pharmacokinetic tail, and at the threshold of capsid resistance. The convergence of incomplete tissue distribution data, a 106–235 day mutant selection window following drug discontinuation, and rare breakthrough infections demonstrates that the drug’s protective profile requires careful clinical stewardship. Realizing lenacapavir’s full public health potential requires detailed characterization of these parameters and the development of evidence-based discontinuation protocols to ensure trial efficacy translates effectively to real-world deployment.
By examining the evidence at these spatiotemporal boundaries, this review identifies priority areas for future research and informs evidence-based guidelines for lenacapavir PrEP rollout.
Unresolved Controversies Shaping the Field
Despite the remarkable efficacy data from phase 3 trials, the clinical and research communities remain divided on several fundamental questions regarding lenacapavir’s safety profile, mechanistic assumptions, and implementation requirements. These controversies are not merely academic; they directly influence regulatory decisions, clinical guidelines, and the design of future PrEP programs. Table 1 summarizes the three most pressing active debates, each of which will be examined in detail throughout this review.
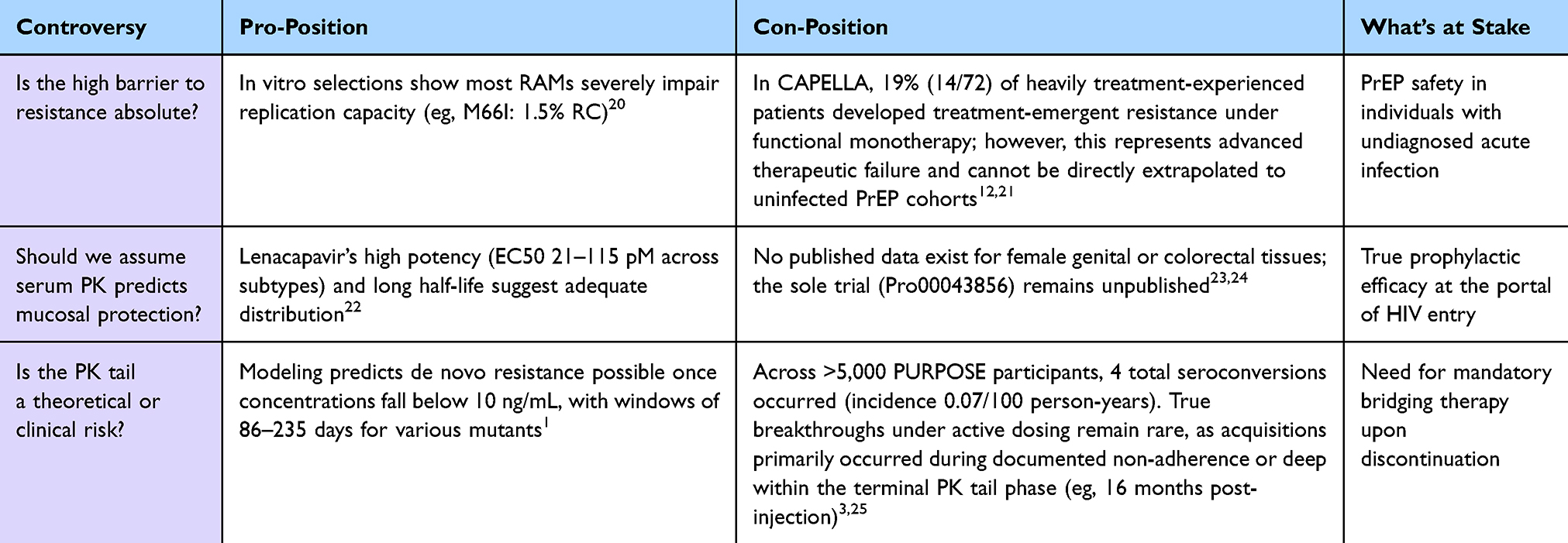 |
Table 1 Matrix of Active Clinical and Pharmacological Controversies |
The following sections critically evaluate the evidence underlying each controversy, with the goal of identifying areas of consensus and, more importantly, the research priorities needed to resolve remaining uncertainties.
Despite this landmark efficacy, a critical spatiotemporal gap remains in our clinical understanding of lenacapavir’s long-term stewardship. The fundamental problem addressed by this review is the “Failure of Systemic Surrogacy”; currently, there are no evidence-based protocols to manage the month-long descent into sub-therapeutic drug levels following treatment discontinuation.26 Integrated PK-PD modeling suggests that a “Mutant Selection Window” (MSW) persists for 106–235 days post-injection, during which sub-therapeutic concentrations exert selective pressure that favors de novo capsid resistance emergence.1,3 By synthesizing the intersection of tissue pharmacokinetics13 and molecular resistance,25 we intend to provide a definitive clinical stewardship framework that identifies the spatiotemporal limits of protection, thereby preventing the emergence of high-level capsid resistance and ensuring the sustained utility of this first-in-class agent.
Methodology
Search Strategy and Information Sources
A systematic search of the peer-reviewed literature was conducted on 20 April 2026 across three databases: PubMed (including MEDLINE), Embase, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL). The study selection process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, as illustrated in the PRISMA Flow Diagram (See Supplementary Figure 1).
The following standardized Boolean search string was applied uniformly across all search engines:
((“lenacapavir”[Mesh] OR “lenacapavir”[tiab] OR “GS-6207”[tiab] OR “Sunlenca”[tiab] OR “Yeztugo”[tiab]) AND (“Pre-Exposure Prophylaxis”[Mesh] OR “PrEP”[tiab] OR “HIV Infections/prevention and control”[Mesh]) AND (“Pharmacokinetics”[Mesh] OR “Tissue Distribution”[Mesh] OR “Mucous Membrane/metabolism”[Mesh] OR “Drug Resistance, Viral”[Mesh] OR “Capsid Proteins/antagonists & inhibitors”[Mesh])) NOT (“editorial”[pt] OR “letter”[pt] OR “comment”[pt])
The comprehensive search query yielded an aggregate total of 485 records, with database-specific yields distributed as follows: PubMed (n = 212), Embase (n = 168), Scopus/Web of Science (n = 92), and the Cochrane Library (n = 13). Following the automated and manual removal of 142 duplicate records, 343 unique titles and abstracts were independently screened by multiple reviewers against pre-defined clinical inclusion parameters, resulting in the exclusion of 248 records.
A total of 95 full-text reports were sought for retrieval, of which 7 were not retrieved. Subsequently, 88 full-text articles were independently assessed for eligibility, with 30 records excluded with reasons (including lack of original PK/PD modeling data (n = 12), absence of resistance or fitness metrics (n = 8), redundant review architectures (n = 6), and incomplete trial cohorts (n = 4)). Ultimately, 58 high-impact studies met all eligibility thresholds and were selected for synthesis.
Inclusion/Exclusion Criteria
Included studies met the following criteria: (1) peer-reviewed original research advanced pharmacometric modeling analyses or systematic review; (2) focused on the capsid inhibitor lenacapavir (GS-6207) for HIV-1 clinical treatment or pre-exposure prophylaxis (PrEP); (3) reported original data on mechanism of action, pharmacokinetics, tissue distribution, efficacy, safety, or resistance; (4) published in English between January 2020 and April 2026. Non-peer-reviewed preprints, isolated conference abstracts missing full-text literature cross-validation, commercial news updates, and opinion pieces were excluded.
The included study topographies encompass in vitro structural biology profiles, nonclinical animal pharmacokinetic parameters, pivotal Phase 2/3 clinical trials (PURPOSE 1, PURPOSE 2, CAPELLA), physiologically based pharmacokinetic (PBPK) and population pharmacokinetic-pharmacodynamic modeling platforms, and rigorous systematic review works.
Synthesis of Evidence
Given the technical heterogeneity of the underlying study matrices (ranging from cellular in vitro evaluations to large-scale randomized human trials), a qualitative, systematic narrative synthesis methodology was deployed. Extracted data points were harmonized and organized thematically across three spatiotemporal axes: mucosal tissue pharmacokinetic penetration, terminal elimination tail dynamics, and molecular resistance emergence pathways. Where divergent outcomes or predictive variations occurred across the 58 evaluated sources, literature strings were compared and contrasted to distinctly demarcate areas of clinical consensus from active implementation controversies.
The Capsid at the Crossroads: Mechanism of Action and the Basis for Spatiotemporal Vulnerability
Lenacapavir’s Multistage Mechanism of Action
Lenacapavir is a picomolar first‑in‑class capsid inhibitor of HIV‑1 with a multistage mechanism of action and no known cross‑resistance to other existing antiretroviral drug classes.13,16 The drug binds to a hydrophobic pocket at the interface between neighboring capsid (CA) proteins within the hexameric lattice, a site critical for both the orderly assembly of new virions and the interaction with host cell factors that mediate nuclear import of the viral genome.27,28
Using two complementary labeling methods, a GFP content marker to measure capsid integrity and GFP‑tagged capsid to track capsid lattice stability, researchers demonstrated that lenacapavir treatment of isolated HIV‑1 cores results in a dose‑dependent loss of core integrity while paradoxically preserving the capsid lattice signal.27 This indicates that lenacapavir disrupts viral core integrity but simultaneously stabilizes the capsid lattice, a unique bifunctional effect not observed with earlier capsid inhibitors.3,27
Viral cores in lenacapavir‑treated cells dock at the nuclear envelope but fail to enter the nucleus, suggesting that lenacapavir‑induced alterations in the capsid lattice impair nuclear import.27 This mechanism is distinct from that of earlier capsid inhibitors such as PF74, which blocks nuclear import by preventing viral core docking with the nuclear envelope.29 Lenacapavir therefore inhibits HIV‑1 at multiple stages of the viral life cycle, including nuclear import, virion assembly, and capsid core maturation, thereby decreasing both virion production and infectivity (Figure 1).13,27 This unique multistage mechanism positions lenacapavir as an effective component of regimens for individuals with multiclass HIV drug resistance, particularly those with limited treatment options.16,21
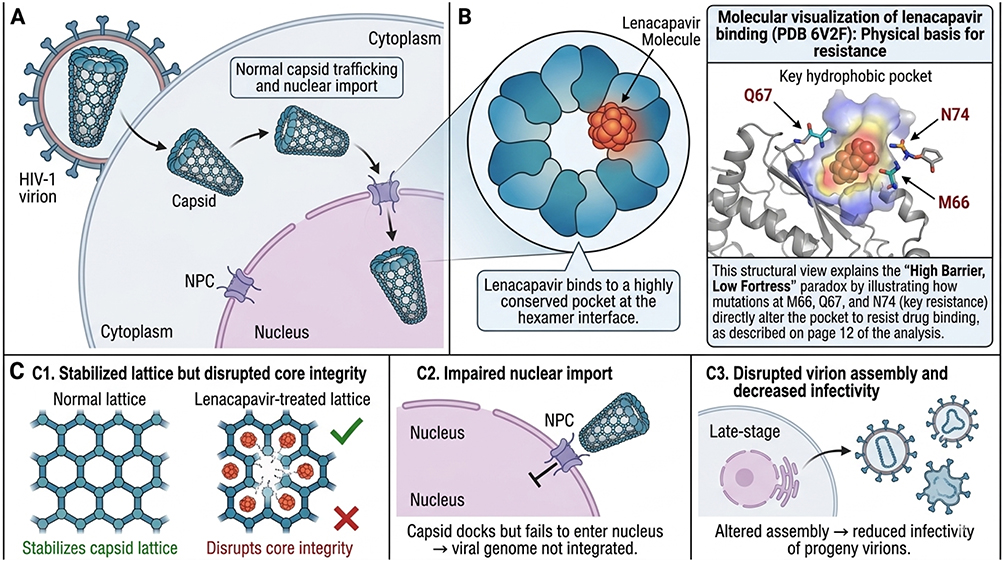 |
Figure 1 Multistage mechanism of lenacapavir. (A) Normal HIV‑1 capsid function: capsid trafficking and nuclear import. (B) Lenacapavir binding at the capsid hexamer interface. (C) Consequences: impaired nuclear import, disrupted virion assembly, and decreased infectivity. Created using BioRender. Data from.13,27 The unique mechanism positions lenacapavir as an effective component of regimens for individuals with multiclass HIV drug resistance.16,21 |
The Capsid as a Dynamic Hub: From Cytoplasm to Nuclear Speckles
Upon viral entry, HIV‑1 capsids are released into the host cell cytoplasm, where they facilitate transport of the viral genome to the nucleus for integration into the host genome.30 Intact capsids can traverse the nuclear pore complex to enter the nucleoplasm, a process that is essential for efficient HIV‑1 replication.31 Lenacapavir’s binding at the hexamer interface disrupts this process at multiple stages, including nuclear import, virion assembly, and capsid core maturation, thereby inhibiting virion production and decreasing virion infectivity.13,27 The capsid’s highly conserved nature explains the minimal pre‑existing drug resistance observed in treatment‑naïve populations, making it an attractive target for antiviral drug development.12
Resistance Mutation Landscape
Primary resistance‑associated substitutions in the HIV‑1 capsid map to seven distinct amino acid positions: L56, M66, Q67, K70, N74, A105, and T107, with specific variants identified in clinical and in vitro settings including L56I, M66I, Q67H/K/N, K70H/N/R/S, N74D/H/K, A105S/T, and T107A/C/N/S.3,12,14 Phenotypic characterization of these mutants in single‑cycle assays shows that most RAMs are associated with severely impaired replication capacity (RC).20 The M66I mutant, for instance, exhibits >2000‑fold reduced lenacapavir susceptibility but only 1.5% RC compared with wild‑type virus.14,20 This severe replication impairment suggests that while these mutations can confer high‑level resistance, their poor viral fitness may limit their transmission and clinical emergence, a finding with important implications for PrEP implementation.20,32
A Unique Pharmacologic Profile: Flip-Flop Kinetics and Atropisomerism
Lenacapavir exhibits exceptionally low systemic clearance following intravenous administration in nonclinical species and humans.13 Formulated as an aqueous suspension or PEG/water solution, the drug shows sustained plasma exposure levels with no unintended rapid drug release following subcutaneous administration.13 The subcutaneous PK profiles display two-phase absorption kinetics in both animals and humans: an initial fast-release absorption phase, followed by a slow-release absorption phase.13 Lenacapavir SC PK shows flip-flop kinetics due to the input rate being substantially slower than the systemic exit rate, with input rates via the slow-release process in humans slower than those in both rats and dogs.13 Overall, the combination of high potency, exceptional stability, and optimal release rate from the injection depot make lenacapavir well suited for a parenteral long-acting formulation that can be administered once up to every 6 months in humans for the prevention and treatment of HIV-1.13
The Tissue Compartment Paradox: Are Serum Levels a Sufficient Surrogate for Mucosal Protection?
The Challenge of HIV Prevention at Mucosal Surfaces
HIV acquisition occurs at mucosal surfaces, the female genital tract and male colorectal mucosa, where the virus encounters target cells (CD4+ T lymphocytes, macrophages, dendritic cells) in the lamina propria.33 For a PrEP agent to be effective, it must achieve concentrations at these mucosal sites that exceed the inhibitory concentration for the infecting viral strain throughout the dosing interval.34 Serum or plasma concentrations are convenient surrogates but may not reflect drug levels in mucosal tissue due to differences in perfusion, protein binding, active transport, and local metabolism.35 This “tissue compartment paradox” has been well documented for other antiretrovirals, where tissue-to-plasma ratios can vary by orders of magnitude.36 The anatomical compartmentalization of drug distribution and the resulting spatiotemporal paradoxes are schematically synthesized in Figure 2.
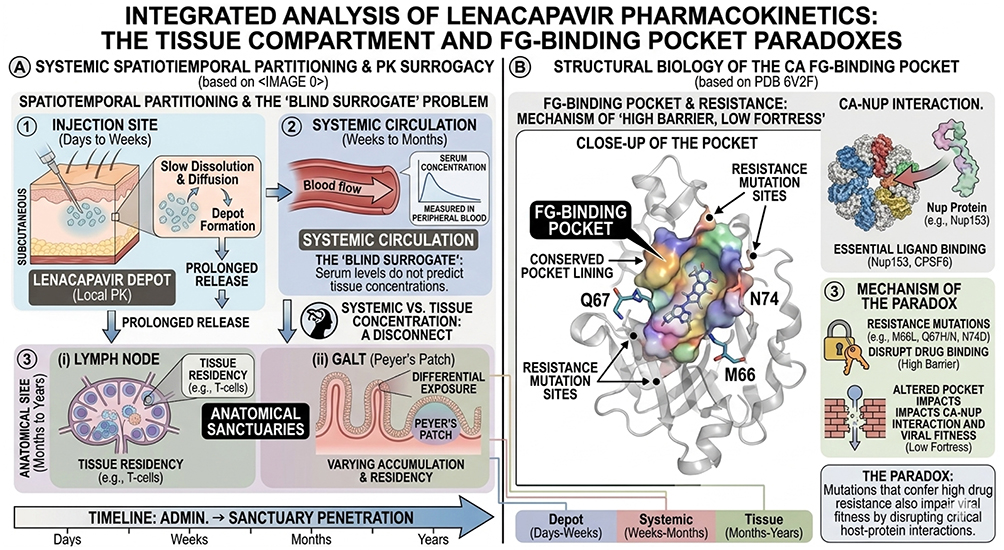 |
Figure 2 Integrated analysis of lenacapavir pharmacokinetics: the tissue compartment and FG-binding pocket paradoxes. (A) Systemic spatiotemporal partitioning and pharmacokinetic surrogacy. Schematic of lenacapavir (LEN) tracking from subcutaneous injection (1) to systemic circulation (2) and final penetration into anatomical tissue sanctuaries (3), including lymph nodes (i) and gut-associated lymphoid tissue (GALT) (ii). Solid black arrows indicate downstream pharmacokinetic transitions; curved circular arrows denote localized cellular residency. (B) Structural biology of the capsid FG-binding pocket. Close-up structural visualization (PDB 6V2F) highlighting primary resistance-associated mutation positions at residues M66, Q67, and N74. (C) Molecular mechanisms of the capsid-host factor interaction and resistance paradox. Structural mapping of competitive lenacapavir binding to block host ligands (Nup153/CPSF6). The padlock icon represents the “high barrier” phenotypic resistance mechanism where specific substitutions physically disrupt drug binding. The stacked brick wall icon represents the “low fortress” biological paradox, where resistance-conferring mutations simultaneously compromise viral replication fitness by disrupting host-protein interactions required for nuclear entry. |
Lessons from Prior Long-Acting PrEP Agents (Cabotegravir, Dapivirine)
The development of cabotegravir long‑acting PrEP and the dapivirine vaginal ring established rigorous standards for mucosal pharmacokinetic (PK) assessment that lenacapavir’s development has not yet matched.37 For cabotegravir, early‑phase studies quantified drug concentrations in cervicovaginal fluid, cervical tissue, and rectal tissue, establishing PK‑PD relationships that directly informed dose selection for the HPTN 083 and 084 phase 3 trials.38,39 For the dapivirine ring, extensive mucosal PK data from the MTN‑020/IPM 027 study and subsequent trials demonstrated that drug concentrations in vaginal fluid and tissue, not plasma, predicted protection against HIV acquisition.40,41 In contrast, lenacapavir’s mucosal PK profile remains largely uncharacterized, with no published data from female genital or male colorectal tissues.42 This evidentiary gap represents a departure from the standards established by its predecessors and undermines confidence that serum concentrations alone can serve as reliable surrogates for mucosal protection.
The Gap in Lenacapavir’s Tissue Pharmacokinetic Data
A systematic review of the published lenacapavir literature reveals a striking absence of mucosal pharmacokinetic (PK) data. While the serum PK profile of lenacapavir is well‑characterized,13,15 no peer‑reviewed study has reported lenacapavir concentrations in female genital tract or male colorectal tissues from healthy volunteers or PrEP users.13 One clinical trial, Gilead Sciences study GS‑US‑528‑5744 (Pro00043856), a Phase 1, open‑label, single‑arm, single‑dose study to evaluate the pharmacokinetics and distribution of lenacapavir into rectal and female genital tract tissues in HIV‑seronegative participants, was registered but its results remain unpublished as of this review.42 The continued absence of these human mucosal results, nearly four years after trial registration, constitutes a significant evidentiary gap that undermines the “Serum Surrogacy” model”. This gap forces clinicians and guideline developers to assume, without evidence, that plasma concentrations, specifically the 95% preventive concentration derived from PK‑PD models, adequately reflect drug levels at the site of viral challenge.43 Until mucosal PK data are available, the true prophylactic efficacy of lenacapavir at the portal of HIV entry, and its vulnerability to local factors that might alter drug exposure (eg, inflammation, microbiome composition, hormonal contraception), remains unknown.43 A comprehensive comparison of the stark discrepancies in mucosal pharmacokinetic data availability between lenacapavir and prior long-acting agents is outlined in Table 2.
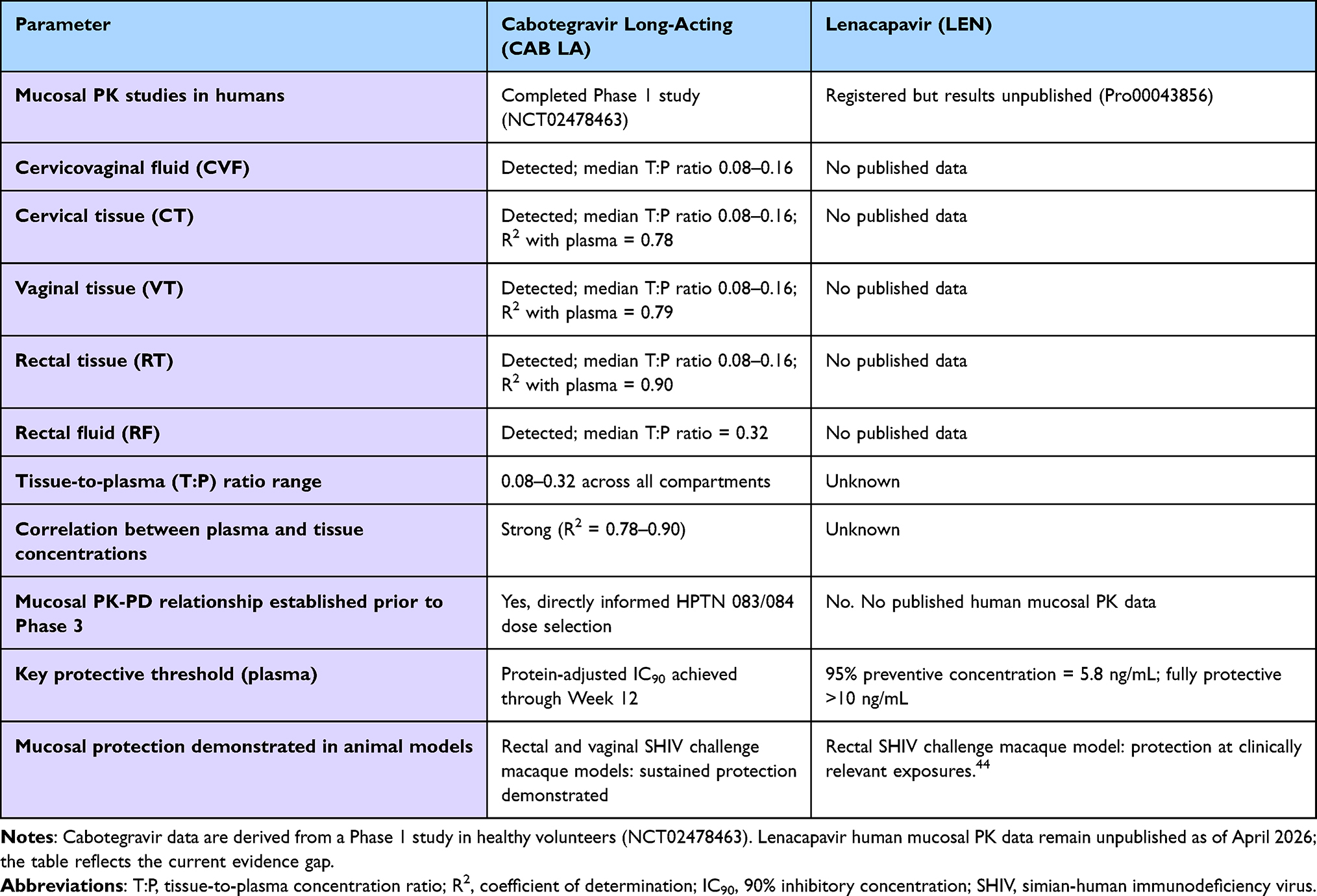 |
Table 2 Comparison of Mucosal Pharmacokinetic Data Availability for Cabotegravir Long‑Acting (CAB LA) and Lenacapavir (LEN) |
Determinants of Tissue Exposure: Transporters, Metabolism, and Protein Binding
The determinants of lenacapavir’s tissue distribution are incompletely characterized. The drug’s high protein binding (estimated >99%) may limit free drug concentrations available for diffusion into mucosal compartments. Active transport mechanisms, including efflux transporters such as P-glycoprotein and breast cancer resistance protein (BCRP), could further restrict mucosal accumulation.45 In the absence of dedicated tissue PK studies, physiologically based pharmacokinetic (PBPK) modeling may offer a provisional approach to predicting tissue concentrations, but such models require validation against empirical data. The field urgently requires a dedicated phase 1 or 2 study of lenacapavir mucosal PK analogous to those conducted for cabotegravir and the dapivirine ring.
The Pharmacokinetic Tail: A Prolonged Period of Vulnerability
Defining the PK Tail: From Therapeutic to Sub-Therapeutic Levels
The extraordinarily long half‑life of lenacapavir, approximately 10–12 weeks following subcutaneous administration, creates an extended period during which drug concentrations gradually decline from fully protective levels to sub‑therapeutic levels.13,15 This “PK tail” is an inherent feature of long‑acting injectable formulations but carries unique risks for pre‑exposure prophylaxis (PrEP). When an individual discontinues lenacapavir (whether intentionally due to side effects, loss to follow‑up, or a decision to stop PrEP) or misses a scheduled injection, they enter a prolonged window of partial protection during which drug concentrations may be too low to reliably prevent infection but sufficiently high to select for resistant viral variants.3
The prolonged PK tail is mechanistically explained by lenacapavir’s unique absorption profile. The subcutaneous pharmacokinetic profile displays two‑phase absorption kinetics in both animals and humans: an initial fast‑release absorption phase, followed by a slow‑release absorption phase.13,46,47 Lenacapavir exhibits “flip‑flop” kinetics because the input rate from the injection depot is substantially slower than the systemic elimination rate, leading to an increased apparent terminal half‑life of approximately 10–12 weeks in humans.15,46 This kinetic property, while enabling twice‑yearly dosing, also ensures that after the last injection, drug levels decline slowly over many months, creating the very window of vulnerability that distinguishes lenacapavir from daily oral PrEP agents.3,43
The mechanistic driver of the prolonged tail is flip‑flop kinetics, where the absorption rate from the subcutaneous depot (ka) is substantially slower than the systemic elimination rate (ke).1,48 In conventional drugs, the terminal half‑life reflects clearance (ke). For lenacapavir, the apparent half‑life is absorption‑limited: the depot continues to release drugs long after plasma levels have peaked.13 Consequently, following discontinuation or loss to follow-up, the tail phase is not simply drug clearing out, it is drug slowly leaking in at sub‑therapeutic levels for up to a year.1,44 This creates a state of functional monotherapy, during which individuals remain exposed to declining but measurable drug concentrations without the benefit of full prophylactic protection, establishing a critical rationale for structured clinical protocol tracking.3,26
PK-PD Modeling of the Protective Threshold
An integrated pharmacokinetic‑pharmacodynamic (PK‑PD) model of lenacapavir, incorporating observed PK variability from Phase III clinical data, has recently been developed to quantify prophylactic efficacy and estimate the probability of drug resistance emergence.43 The model estimated a 95% preventive plasma concentration of 5.8 ng/mL for wild‑type HIV‑1 and a fully preventive concentration of >10 ng/mL.43 The latter (>10 ng/mL) is achieved within 155 hours after the first 927 mg subcutaneous injection in an “average” individual and persists for up to 45 weeks after the last dose.43 However, considering interindividual PK variability, concentrations exceeding either 5.8 ng/mL or 10 ng/mL are not maintained at all times for individuals with lower drug exposure; these thresholds are reliably surpassed only at steady‑state.15,43 For resistant mutants, the concentration required for full protection is substantially higher: 21 ng/mL for the Q67H mutant, 85 ng/mL for N74D, 218 ng/mL for Q67H+T107N, 100 ng/mL for Q67H+N74S, and 3,095 ng/mL for the Q67H+K70R+T107N triple mutant.14,43
The clinical significance of these thresholds becomes stark when comparing the N74D mutation (protective concentration required: 85 ng/mL) to the wild‑type 95% preventive concentration (5.8 ng/mL).1 This represents a 14‑fold increase in the drug concentration required for protection.1,13 In practical terms, once a single resistance‑associated mutation emerges, even a variant with impaired replication capacity, the prophylactic “protective envelope” of lenacapavir is substantially compromised.1 The required concentration (85 ng/mL) is often higher than what steady‑state twice‑yearly dosing provides in many individuals, particularly at the end of the dosing interval.1,13 This suggests that for lenacapavir PrEP, resistance emergence acts as a critical threshold event where the appearance of a primary mutation alters the baseline protective profile.1 These thresholds underscore that even a partial loss of susceptibility can dramatically elevate the drug concentration needed for prevention, a finding that directly informs current PrEP discontinuation protocols and the clinical management of breakthrough infections.1,13
The Tail as a Selection Window for Resistance
The integrated PK‑PD model identified that wild‑type infection with subsequent de novo resistance emergence may occur within a period of approximately 106 to 235 days after stopping lenacapavir injections, depending on the specific resistance mutation pathway (Figure 3).43 Critically, the mutant selection windows for N74D, all double mutants (eg, Q67H+N74D, Q67H+T107N, Q67H+N74S), and the triple mutant Q67H+K70R+T107N overlap with steady‑state lenacapavir concentrations achieved with twice‑yearly dosing.14,43 This means that during the pharmacokinetic tail, drug levels may fall into the “mutant selection window”, the concentration range that suppresses wild‑type virus but permits the outgrowth of resistant mutants.43
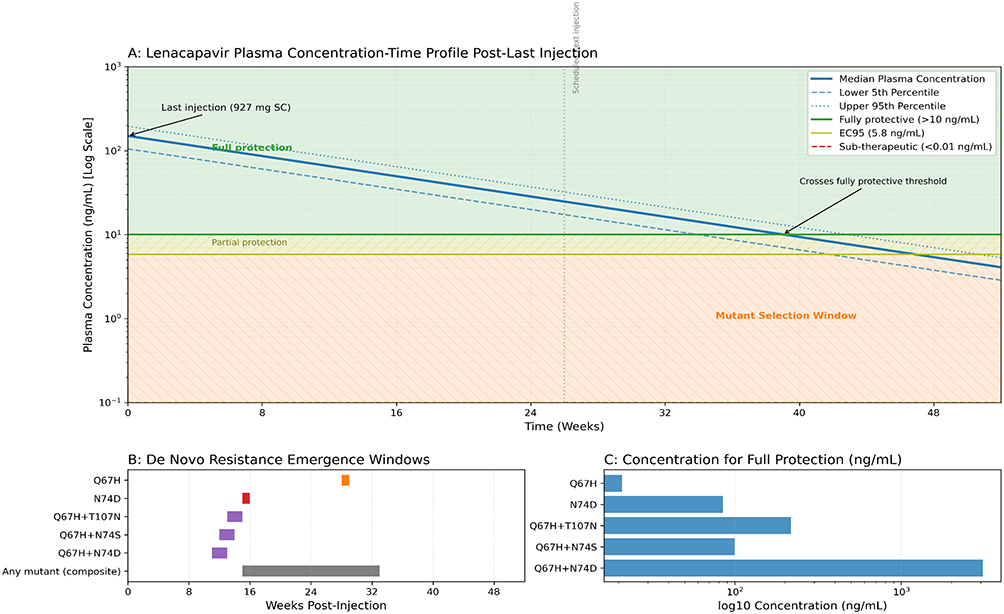 |
Figure 3 The lenacapavir pharmacokinetic tail: Protective threshold, mutant selection window, and resistance emergence. (A) Simulated plasma lenacapavir concentration over 52 weeks after the last 927 mg subcutaneous injection (solid blue line: median; dashed/dotted lines: 5th and 95th percentiles). Horizontal lines indicate the fully protective threshold for wild‑type virus (>10 ng/mL), the 95% preventive concentration (5.8 ng/mL), and the lower bound of the mutant selection window (~0.1 ng/mL). Shaded regions denote full protection (green), partial protection (light green), the mutant selection window (Orange), and sub‑therapeutic levels (red). The orange window (approximately weeks 15–33) is when concentrations fall below the thresholds needed to suppress resistant mutants but remain above 0.1 ng/mL. (B) Horizontal bars indicate the temporal windows for de novo resistance emergence for individual mutants (Q67H, N74D, Q67H+T107N, Q67H+N74S, Q67H+N74D) and the composite window (106–235 days, weeks 15–33). (C) Concentrations required for full protection against key resistant mutants (log scale). Created using Biorender. Data from.1,43 |
Full protection against mutant strains requires substantially higher concentrations than for wild‑type virus: 35 ng/mL for Q67H, 85 ng/mL for N74D, 3,095 ng/mL for Q67H+N74D, 218 ng/mL for Q67H+T107N, and 100 ng/mL for Q67H+N74S.20,43 Because these thresholds are often not maintained during the tail, de novo resistance emergence becomes possible once lenacapavir concentrations fall below 10 ng/mL after the last injection.43 Pharmacokinetic modeling reveals a disproportionate risk for high-fitness mutants; for instance, the selective temporal window for the Q67H substitution persists nearly twice as long as that for N74D (201 vs 105 days), suggesting a tiered risk profile during the terminal elimination phase. Seventy-nine days for Q67H+N74D, 96 days for Q67H+T107N, and 86 days for Q67H+N74S in an “average” individual.1 These findings have profound implications for PrEP discontinuation protocols and call for strategies to manage lenacapavir PrEP discontinuation, including transition to alternative PrEP agents during the tail.3,48
Clinical Correlates: Breakthrough Infections and Adherence Lapses
Across two large clinical trials testing long‑acting lenacapavir for PrEP, encompassing thousands of cisgender women, men who have sex with men, transgender women, transgender men, and gender‑nonbinary individuals, a total of four individuals seroconverted across the trial timelines.25,49 Crucially, these cases must be differentiated by adherence status: true breakthrough infections under active, on-time dosing remain exceedingly rare, as clinical acquisitions occurred primarily during periods of documented injection delays or deep within the sub-therapeutic terminal elimination tail phase rather than under active protective concentrations.
In PURPOSE 1, which enrolled over 5,300 cisgender adolescent and young women in South Africa and Uganda, two seroconversions occurred among 2,134 participants receiving lenacapavir injections every 26 weeks.25 The overall HIV incidence among participants receiving lenacapavir was 0.07 per 100 person‑years, compared to 1.98 per 100 person‑years for the F/TAF arm and 1.94 per 100 person‑years for the F/TDF arm.25 One infected participant had received all injections on schedule and was diagnosed with chlamydia at week 52 before testing positive for HIV at week 65.25 The second participant missed the 26‑week injection, transitioned to open‑label oral PrEP at week 82 while HIV‑negative, but seroconverted at week 95, 16 months after the last lenacapavir injection.3,25
In PURPOSE 2, which enrolled 3,295 cisgender men, transgender women, transgender men, and gender‑nonbinary individuals, two HIV infections occurred in the lenacapavir group.25,49 Overall, 99.9% of participants did not acquire HIV infection across the study timeline.25,49 Data from implementation tracking highlight the clinical communication challenges posed by even rare seroconversions among potential users.50
The contrast between the CAPELLA and PURPOSE study cohorts is highly instructive but requires careful qualification. In the CAPELLA trial, evaluating heavily treatment‑experienced individuals living with multidrug‑resistant HIV‑1, lenacapavir combined with an optimized background regimen (OBR) led to treatment‑emergent capsid resistance in 19% (14/72) of participants.12,21 The key difference is viral load context. In treatment (CAPELLA), lenacapavir confronts billions of virions daily, with a high probability of pre‑existing minority variants.12 In PrEP (PURPOSE), the drug faces only a few hundred virions at the portal of entry, a scenario where resistance selection is statistically rare.25
However, the PK tail introduces a unique selective window. When an individual discontinues lenacapavir and enters the tail, drug levels fall into the mutant selection window.1 If exposure occurs during this period of sub-therapeutic coverage, low-level viral replication could potentially occur at mucosal surfaces, altering the selective pressure profile without replicating the high baseline viral load environment seen in active treatment failure.1
While this modeling-based risk has not been extensively documented in clinical prevention practice, it underscores the rationale for implementing structured, evidence-based discontinuation protocols to preserve future treatment options.1,25 These rare trial seroconversions demonstrate that the spatiotemporal limits of long-acting protection represent real-world clinical implementation factors that warrant systematic stewardship.1,3,21,43
The Resistance Paradox: High Barrier but Low Fortress?
In vitro Resistance Selection: Key Mutations and Pathways
Lenacapavir in vitro resistance selections have identified seven resistance‑associated mutations (RAMs) in HIV‑1 capsid associated with reduced susceptibility: L56I, M66I, Q67H, K70N, N74D, N74S, and T107A/N.14,20 Phenotypic characterization of these mutants in single‑cycle assays indicates that most RAMs are associated with reduced replication capacity (RC). Q67H leads to a 4.6‑fold reduction in susceptibility to lenacapavir and 58% RC compared with wild‑type virus; M66I shows >2000‑fold reduced susceptibility and only 1.5% RC.3,14 In multi‑cycle assays, four of ten mutants lacked measurable infectivity, particularly the M66I and M66I+Q67H mutants, suggesting that the most highly resistant variants are also severely replication‑impaired.3,14,51 The specific fold-resistance shifts and corresponding replication capacities for these key lenacapavir resistance-associated capsid substitutions are detailed in Table 3.14
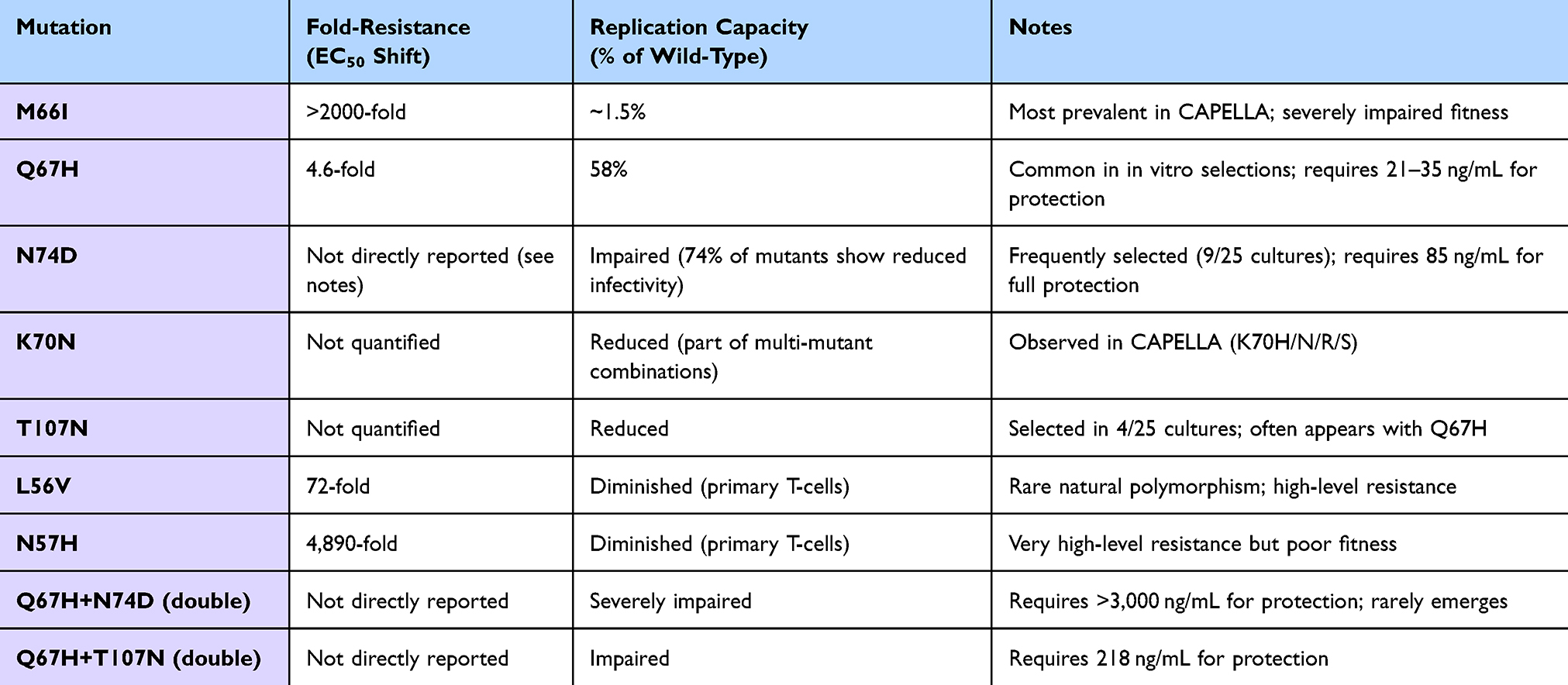 |
Table 3 In vitro Susceptibility and Replication Capacity of Key Lenacapavir Resistance‑associated Capsid Mutations |
Subtype Analysis and Pan‑Genotypic Activity
Resistance selection experiments across HIV‑1 subtypes A1, AE, AG, B, C, D, F1, G, and H demonstrated that wild‑type susceptibility to lenacapavir (EC50 21–115 pM) was observed across all subtypes tested.12,20 Resistance selections in non‑B subtypes led to the emergence of the same mutations with a similar timeframe as in subtype B.20 The most prevalent capsid mutations selected across all subtypes were N74D (9 of 25 cultures), Q67H (4/25), and T107N (4/25), while M66I, K70R/S, and N74H were also observed.12,20 These datasets confirm that lenacapavir functions as a potent pan‑genotypic inhibitor of HIV‑1 capable of maintaining high direct efficacy across globally diverse viral landscapes.3,13
Clinical Resistance Emergence and Cross-Resistance
The M66I variant was the most prevalent capsid substitution identified in patients receiving lenacapavir to treat multidrug‑resistant HIV‑1 infections, and structural studies have elucidated the mechanistic basis for this resistance.20,52 After two years of lenacapavir treatment in the Phase 2/3 CAPELLA study of heavily treatment‑experienced people with multidrug‑resistant HIV‑1, lenacapavir plus an optimized background regimen (OBR) led to HIV‑1 RNA suppression (<50 copies/mL) in 82% of participants.12
Treatment‑emergent capsid resistance occurred in 19% (14/72) of participants, including capsid mutations M66I, Q67H/K/N, K70H/N/R/S, and/or N74D/H/K.12,21 Importantly, these resistance events were all associated with functional lenacapavir monotherapy, meaning participants were effectively receiving lenacapavir without a fully active OBR due to extensive pre-existing baseline resistance.12 Notably, seven participants with lenacapavir-resistance variants reattained HIV‑1 RNA <50 copies/mL upon OBR resumption or change while maintaining lenacapavir therapy.12
Critically, mutants with resistance to lenacapavir were found not cross‑resistant to protease inhibitors, and lenacapavir susceptibility was similar across isolates with diverse HIV‑1 subtypes (A, A1, AE, AG, B, BF, C, D, G, H), with EC50 values ranging from 124 to 357 pM compared to 290 pM for wild‑type control.14,20 All viruses with lenacapavir RAMs remained sensitive to other HIV drug classes, including protease inhibitors, reverse transcriptase inhibitors, and integrase inhibitors.3,14 This absence of cross‑resistance preserves future treatment options for individuals who acquire lenacapavir‑resistant HIV while receiving PrEP or develop resistance during treatment, a critical consideration for public health implementation.3
Prevalence of Pre-Existing Resistance-Associated Mutations in Global Populations
Using a high-resolution co‑crystal structure of lenacapavir in complex with a capsid hexamer, researchers identified 29 binding site residues within five angstroms of lenacapavir and analyzed each for naturally occurring polymorphisms across a multiclade collection of >10,000 unique HIV‑1 gag sequences.3,9,14 Eleven of these capsid (CA) residues, including five (M66, Q67, K70, N74, and A105) previously associated with lenacapavir resistance when mutated, were invariant across these sequences.9,14 The remaining 18 residues showed one or more substitutions with a ≥0.5% prevalence, for a total of 54 CA polymorphisms.3,9,14
When evaluated via site‑directed mutagenesis assays, 74% of these natural polymorphisms caused significantly impaired viral infectivity, and 96% demonstrated negligible changes (less than threefold shifts) in direct susceptibility to lenacapavir.9,14 While CA substitutions L56V and N57H conferred high‑level resistance to lenacapavir (72‑fold and 4,890‑fold, respectively), both variants showed diminished replication capacity in primary T‑cells relative to wild‑type virus.3,9,53 These structural surveillance statistics prove that pre‑existing natural sequence diversity capable of undermining lenacapavir efficacy is exceedingly rare in global populations, ensuring high single-agent efficacy in treatment‑naïve individuals entering prevention networks.9,14,53
Cross-Resistance and the Preservation of Future Treatment Options
A critical feature of lenacapavir’s resistance profile is the absence of cross‑resistance with other antiretroviral drug classes.12,16 The CAPELLA resistance analyses confirmed that lenacapavir‑resistant mutants remained fully susceptible to the protease inhibitors darunavir and atazanavir.12 More broadly, lenacapavir‑associated drug‑resistance mutations do not compromise the effectiveness of WHO‑recommended therapies, as there is no cross‑resistance between lenacapavir and other licensed antiretroviral drugs, including nucleoside reverse transcriptase inhibitors, non‑nucleoside reverse transcriptase inhibitors, integrase strand transfer inhibitors, and entry inhibitors.3,16 This property is essential for preserving future treatment options in the event that an individual acquires lenacapavir‑resistant HIV while receiving PrEP or develops resistance during treatment.12,21
Synthesis and the Unanswered Questions
Integrating the Three Paradoxes: A Unified Framework
The three spatiotemporal vulnerabilities examined in this review, mucosal tissue PK gaps, the PK tail dynamics, and molecular resistance emergence, are not independent but interact in clinically meaningful ways (Figure 4). An individual who discontinues lenacapavir PrEP enters the PK tail, during which mucosal drug concentrations (already poorly characterized) decline below fully protective levels.
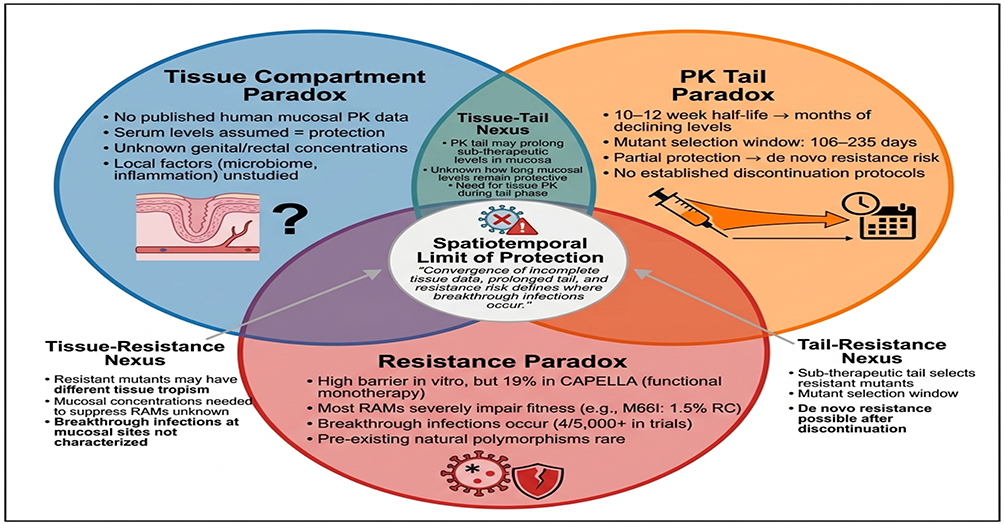 |
Figure 4 The three spatiotemporal paradoxes of lenacapavir PrEP. Three overlapping domains define the limits of lenacapavir’s twice-yearly protective envelope. Blue circle (Tissue Compartment Paradox): absence of human mucosal PK data, unknown genital/rectal concentrations, reliance on serum surrogacy. Orange circle (PK Tail Paradox): 10–12 week half‑life, 106–235 day mutant selection window, risk of de novo resistance after discontinuation. Red circle (Resistance Paradox): 19% treatment‑emergent resistance in CAPELLA (functional monotherapy), severely impaired fitness of most RAMs (eg, M66I: 1.5% replication capacity), rare natural polymorphisms. Pairwise overlaps highlight specific research gaps (tissue‑tail, tail‑resistance, tissue‑resistance). Central triple overlap represents the spatiotemporal limit of protection, where breakthrough infections and de novo resistance may occur. Addressing these converging limits is essential for safe and effective lenacapavir PrEP implementation. Created using Biorender. |
If that individual is subsequently exposed to HIV during this window, the sub-therapeutic drug concentration may theoretically select for resistant variants, particularly if the infecting strain carries pre-existing polymorphisms that reduce susceptibility. While such an event is statistically rare given the low prevalence of natural polymorphisms in the lenacapavir binding site and the severe replication impairment of most resistant variants, the consequences for the affected individual are substantial: acquisition of lenacapavir-resistant HIV that may limit future treatment options using the capsid inhibitor class.
The Implementation Challenges of Long-Acting PrEP
The very properties that make lenacapavir revolutionary, its extraordinary half-life and slow-release kinetics, also introduce unique implementation and monitoring challenges. Unlike daily oral PrEP, which features a rapid drug washout upon cessation, a subcutaneous injection exposes the individual to months of gradually declining drug concentrations after discontinuation. This extended elimination phase introduces a prolonged exposure period that requires active clinical monitoring. Pharmacokinetic-pharmacodynamic modeling estimates indicating a 106–235 day window for potential resistance selection post-discontinuation emphasize that stopping long-acting PrEP is a continuous process rather than a discrete event, requiring structured clinical management.1
The clinical implication of these dynamics is that standard plasma‑based monitoring may provide an incomplete picture of localized tissue protection. This highlights a translational rationale for developing tissue‑informed pharmacokinetic frameworks that account for potential discrepancies between serum and mucosal drug levels. Until empirical tissue distribution parameters are fully characterized, managing individuals who miss doses or discontinue long-acting regimens represents an operational challenge regarding the precise assessment of localized protection.
A Research Agenda for the Spatiotemporal Limits
Based on the gaps identified in this review, a focused research agenda is proposed:
Priority 1: Mucosal PK Studies
A phase 1 or 2 study quantifying lenacapavir concentrations in female genital tract (cervicovaginal fluid, cervical tissue, endometrial tissue) and male colorectal tissue, with comparison to paired plasma samples, is urgently needed. These data should inform PBPK models and establish tissue-specific protective thresholds.
Priority 2: PK Tail Management Protocols
Clinical trials evaluating strategies for managing lenacapavir discontinuation, including bridging with oral PrEP, cabotegravir long-acting, or other agents during the tail, should be prioritized. The optimal duration of bridging and the drug(s) most suitable for this purpose require empirical investigation.
Priority 3: Population-Level Resistance Surveillance
As lenacapavir PrEP scales globally, population-level molecular surveillance for emerging capsid resistance mutations should be implemented, particularly in settings with high HIV incidence and limited genotypic resistance testing capacity.
Priority 4: PBPK Model Validation
Existing PBPK models predicting mucosal lenacapavir concentrations require validation against empirical tissue PK data before they can be used to guide dosing or discontinuation protocols.
Priority 5: Next-Generation Diagnostics for the Tail
We currently utilize short-acting diagnostics (4th-gen Ag/Ab tests) to monitor a long-acting therapeutic. This creates a distinct operational paradox: during the PK tail, standard serology may fail to detect low-level viremia promptly, potentially allowing resistant variants to fixate while the patient remains seronegative. This vulnerability presents a rationale for implementing High-Sensitivity RNA Surveillance (LOD ≤ 10 copies/mL) as an optimized supportive monitoring strategy for individuals entering the terminal elimination phase.
Priority 6: Implementation Equity & Public Health Risks
Implementation research must address the structural dynamics of regional access. Investigating how pricing barriers in middle-income countries influence adherence, informal markets, or fragmented drug use will help identify the operational factors that could generate the sub-therapeutic selective pressure required for the emergence or global dissemination of capsid-resistant strains.
Living Review Framework and Future Directions
Given the rapid pace of lenacapavir research, with at least two major ongoing clinical trials (NCT05009394 for TMR vs. RPNI and the PreventPAP trial) and a once-yearly formulation in Phase 1 development, this narrative review should be considered a “living” document. The field requires: (1) empirical mucosal PK data to resolve tissue distribution uncertainties; (2) prospective clinical registries to track real-world breakthrough events and resistance emergence profiles; (3) implementation science evaluations of optimized discontinuation and bridging protocols; and (4) structured global health tracking to ensure equitable access mechanisms match programmatic rollout demands globally.
Implications for Clinical Practice and Public Health
Guiding PrEP Implementation: Risk Stratification and Monitoring
For clinicians prescribing lenacapavir PrEP, several evidence-based recommendations can be made despite current data gaps. First, HIV testing immediately prior to the first injection is essential to exclude undiagnosed acute infection, as initiating lenacapavir during acute infection could select for resistance. Second, individuals who miss a scheduled injection by more than two weeks should receive oral PrEP bridging until the next injection or until a decision is made to discontinue.49,54
Third, discontinuation should be managed actively: individuals stopping lenacapavir should receive alternative PrEP (oral or cabotegravir long-acting) for at least six months after the last injection to cover the PK tail. Fourth, breakthrough infections during on-time dosing, though rare, warrant thorough resistance testing to inform subsequent treatment and prevention options.
Global Access Dynamics and the Affordability Interface
The pricing of lenacapavir represents one of the most contentious issues in global HIV prevention.7,8,55 While generic production costs are estimated at just $25 per person annually, the U.S. list price for lenacapavir is $28,218–$42,250 per year, a markup of over 1,000‑fold.55,56 Gilead’s voluntary licensing agreements with six generic manufacturers cover 120 low‑income countries, but upper‑middle‑income countries with significant HIV burdens remain excluded, including Argentina, Brazil, Mexico, and Peru, four countries that hosted the pivotal PURPOSE 2 trial.55–57 More than one in four new HIV acquisitions occur in the 26 countries and territories excluded from Gilead’s license agreements, prompting activist organizations to file patent oppositions and demand a $40-per-year universal price.4,57,58
Without broader access commitments, the populations with the highest HIV incidence, young women in sub‑Saharan Africa, transgender individuals, and men who have sex with men in excluded middle‑income countries, will remain unable to benefit from this transformative technology.3,58 From a resistance perspective, lenacapavir pre‑exposure prophylaxis is unlikely to drive population‑level lenacapavir resistance, given the rarity of breakthrough infections and the reduced replication capacity of most lenacapavir‑resistant variants, which likely reduces their transmission potential.3,12,59,60 However, these marked disparities in economic accessibility introduce distinct implementation risks.
Scientific success without global access can result in localized programmatic bottlenecks. The exclusion of middle-income manufacturing hubs presents an operational challenge that can influence regional selective pressures. In settings where the drug is unaffordable, individuals may turn to informal markets, counterfeit formulations, or sub-optimal regimens, creating the sub-therapeutic exposure conditions that facilitate resistance emergence.50,53 Ensuring equitable, structured distribution networks is therefore a critical operational objective to safeguard the long-term clinical utility of the capsid inhibitor class globally.
Limitations of the Review
This synthesis is primarily constrained by its reliance on predictive pharmacokinetic-pharmacodynamic (PK-PD) modeling data and in vitro virological assays, as longitudinal human mucosal tissue cohorts and empirical real-world datasets characterizing lenacapavir tail discontinuation remain sparse through mid-2026. While a structured, systematic search strategy was executed across five major biomedical databases to minimize selection bias and map global yields transparently, narrative syntheses are inherently subject to data interpretation limits, and long-term population-level resistance impacts will require continuous verification as clinical implementation scales globally.
Conclusions
Lenacapavir represents a landmark advance in HIV prevention, offering twice-yearly subcutaneous dosing with near-perfect clinical efficacy. Its unique multistage mechanism, favorable safety profile, and absence of cross-resistance with existing classes position it as a transformative tool for ending the HIV epidemic. However, the success of this molecule is contingent upon our ability to manage the spatiotemporal limits of its protective envelope.
As lenacapavir moves from the controlled environment of clinical trials to real-world implementation, we must move beyond the era of “serum surrogacy” toward a more nuanced, tissue-informed stewardship of the pharmacokinetic tail. The research agenda proposed in this review, emphasizing mucosal PK quantification, ultra-sensitive diagnostic surveillance, and global access equity, is not an obstacle to implementation, but the necessary foundation for a durable and equitable scale-up.
Ultimately, the clinical community must recognize that unlike oral PrEP, which permits rapid drug washout upon cessation, lenacapavir involves a pharmacological commitment of nearly 12 months. This necessitates that the clinical decision to initiate dosing be treated as a definitive clinical contract, including a pre-planned “exit strategy” or bridging protocol to protect both individual outcomes and the long-term utility of the capsid inhibitor class. Only through this rigorous framework can lenacapavir fulfill its promise as a definitive tool in the global HIV prevention strategies.
Acknowledgments
The authors would like to thank the faculty of the School of Medicine at Kabale University for their academic support and institutional guidance. We also express our gratitude to the clinical teams and researchers whose primary data formed the evidentiary basis for this synthesis. Special thanks are extended to the Research4Life partnership for facilitating access to the global scholarly literature essential for this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yeong KH, Liebenberg A, Zhang L, von Kleist M. Pharmacokinetics, pharmacodynamics, efficacy and drug resistance selection of injectable long-acting lenacapavir pre-exposure prophylaxis (PrEP) against HIV. medRxiv. 2025;
2. Koss CA, Parikh UM. Long-acting preexposure prophylaxis: early data on roll-out in the United States. Curr Opin HIV AIDS. 2025;20(1):25. doi:10.1097/COH.0000000000000894
3. van Zyl G, Prochazka M, Ann Schmidt HM, et al. Lenacapavir-associated drug resistance: implications for scaling up long-acting HIV pre-exposure prophylaxis. Lancet HIV. 2025;12(10):e732–19. doi:10.1016/S2352-3018(25)00128-6
4. Activists demand $40-a-year generic price for breakthrough HIV prevention drug be made available to all low- and middle-income countries. Available from: https://www.eatg.org/hiv-news/activists-demand-40-a-year-generic-price-for-breakthrough-hiv-prevention-drug-be-made-available-to-all-lmics/.
5. Musa SS, Othman ZK, Fadele KP, et al. Gender disparities in HIV infections: a narrative review of the persistent vulnerability of adolescent girls in Sub-Saharan Africa. Narra X. 2025;3(2):e211–e211. doi:10.52225/narrax.v3i2.211
6. De Clercq E, Zhang Y, Li G, et al. Lenacapavir: a capsid inhibitor for HIV-1 treatment and prevention. Biochem Pharmacol. 2025;240:117125. doi:10.1016/j.bcp.2025.117125
7. Sunlenca lenacapavir Receives FDA Approval as a First in Class Twice Yearly Treatment Option for People Living With Multi Drug Resistant HIV. https://www.gilead.com/news/news-details/2022/sunlenca-lenacapavir-receives-fda-approval-as-a-first-in-class-twice-yearly-treatment-option-for-people-living-with-multi-drug-resistant-hiv.
8. Sunlenca | European Medicines Agency (EMA). June 22, 2022. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/sunlenca.
9. Hansen D, Hendricks MR, Chang S, et al. Impact of HIV-1 capsid polymorphisms on viral infectivity and susceptibility to lenacapavir. mBio. 2025;16(5):e00187–25. doi:10.1128/mbio.00187-25
10. Editor DT Associate. Gilead’s Yeztugo Demonstrates Strong HIV Prevention Results in Underserved Populations | applied Clinical Trials Online. 2026. Available from: https://www.appliedclinicaltrialsonline.com/view/gilead-s-yeztugo-demonstrates-strong-hiv-prevention-results-underserved-populations?utm_medium=relatedContent&utm_source=www.appliedclinicaltrialsonline.com.
11. Yeztugo® (Lenacapavir). Is Now the First and Only FDA Approved HIV Prevention Option Offering 6 Months of Protection. Available from: https://www.gilead.com/news/news-details/2025/yeztugo-lenacapavir-is-now-the-first-and-only-fda-approved-hiv-prevention-option-offering-6-months-of-protection.
12. Margot NA, Jogiraju V, Pennetzdorfer N, et al. Resistance Analyses in Heavily Treatment-Experienced People With HIV Treated With the Novel HIV Capsid Inhibitor Lenacapavir After 2 Years. J Infect Dis. 2025;231(5):1239–1245. doi:10.1093/infdis/jiaf050
13. Subramanian R, Tang J, Zheng J, et al. Lenacapavir: a Novel, Potent, and Selective First-in-Class Inhibitor of HIV-1 Capsid Function Exhibits Optimal Pharmacokinetic Properties for a Long-Acting Injectable Antiretroviral Agent. Mol Pharm. 2023;20(12):6213–6225. doi:10.1021/acs.molpharmaceut.3c00626
14. Activity and Resistance Characterization of the HIV Capsid Inhibitor Lenacapavir. CROI Conference. Available from: https://www.croiconference.org/abstract/activity-and-resistance-characterization-of-the-hiv-capsid-inhibitor-lenacapavir/.
15. Imperial M, Hughes E, Panchia R, et al. Population Pharmacokinetic Analysis of Lenacapavir in People Who Want or Need Pre-Exposure Prophylaxis for HIV.
16. Diamond TL, Goh SL, Ngo W, et al. No antagonism or cross-resistance and a high barrier to the emergence of resistance in vitro for the combination of islatravir and lenacapavir. Antimicrob Agents Chemother. 2024;68(7):e00334–24. doi:10.1128/aac.00334-24
17. Parkinson J. Gilead Submits FDA New Drug Application for Lenacapavir for HIV Prevention | contagion Live. 2026. Available from: https://www.contagionlive.com/view/gilead-submits-fda-new-drug-application-for-lenacapavir-for-hiv-prevention.
18. Press release: gilead’s twice-yearly lenacapavir for HIV prevention reduced HIV infections by 96% and demonstrated superiority to daily Truvada® in second pivotal Phase 3 trial | EATG. Available from: https://www.eatg.org/hiv-news/press-release-gileads-twice-yearly-lenacapavir-for-hiv-prevention-reduced-hiv-infections-by-96-and-demonstrated-superiority-to-daily-truvada-in-second-pivotal-phase-3-trial/.
19. Vp N. Gilead’s lenacapavir maintains high virologic suppression rates in trial. Clinical Trials Arena.
20. Demirdjian S, Naik V, Margot N, Falkard B, Callebaut C. Phenotypic characterization of replication‐impaired lenacapavir‐resistant HIV clinical isolates. J Med Virol. 2025;97(4):e70340. doi:10.1002/jmv.70340
21. Ogbuagu O, Wiznia A, McGowan JP, et al. Subcutaneous lenacapavir in people with multidrug-resistant HIV-1: 156 week results of the CAPELLA study. Open Forum Infect Dis. 2025;13(1):ofaf763. doi:10.1093/ofid/ofaf763
22. Naik V, Nekkalapudi A, Boopathy AV, Falkard B, Callebaut C, Margot NA. Emergence of in-vitro resistance to lenacapavir is similar across HIV-1 subtypes. AIDS. 2025;39(13):1878. doi:10.1097/QAD.0000000000004334
23. Neverette NC, Dumond JB, McMahon DK, Devanathan AS. Lenacapavir: playing the long game in the new era of antiretrovirals. Clin Pharmacol Ther. 2025;117(2):353–367. doi:10.1002/cpt.3447
24. Pitt+Me ~ Lenacapavir (LEN) for the Prevention of HIV-infection – healthy Volunteers. Available from: https://pittplusme.org/studyarms/publicdetails?guid=70e88f43-6e97-4236-b3da-efc8d897fbf1.
25. Kelley CF, Acevedo-Quiñones M, Agwu AL, et al. Twice-yearly lenacapavir for HIV prevention in men and gender-diverse persons. N Engl J Med. 2025;392(13):1261–1276. doi:10.1056/NEJMoa2411858
26. WHO. Guidelines on lenacapavir for HIV prevention and testing strategies for long-acting injectable pre-exposure prophylaxis. Available from: https://iris.who.int/server/api/core/bitstreams/30ec1404-5338-4459-a6f0-a187c85f3ff1/content.
27. Li C, Burdick RC, Siddiqui R, et al. Lenacapavir disrupts HIV-1 core integrity while stabilizing the capsid lattice. Proc Natl Acad Sci. 2025;122(14):e2420497122. doi:10.1073/pnas.2420497122
28. Bester SM, Adu-Ampratwum D, Annamalai AS, et al. Structural and mechanistic bases of viral resistance to HIV-1 capsid inhibitor lenacapavir. mBio. 2022;13(5):e01804–22. doi:10.1128/mbio.01804-22
29. Bhattacharya A, Alam SL, Fricke T, et al. Structural basis of HIV-1 capsid recognition by PF74 and CPSF6. Proc Natl Acad Sci U S A. 2014;111(52):18625–18630. doi:10.1073/pnas.1419945112
30. Campbell EM, Hope TJ. HIV-1 capsid: the multifaceted key player in HIV-1 infection. Nat Rev Microbiol. 2015;13(8):471–483. doi:10.1038/nrmicro3503
31. Zila V, Müller TG, Müller B, Kräusslich HG. HIV-1 capsid is the key orchestrator of early viral replication. PLoS Pathog. 2021;17(12):e1010109. doi:10.1371/journal.ppat.1010109
32. Weibull Wärnberg A, Ceña‐Diez R, Sönnerborg A, van de Klundert MAA. Natural occurrence of drug resistance mutations to the HIV‐1 capsid inhibitor lenacapavir. HIV Med. 2025;26(11):1881–1886. doi:10.1111/hiv.70092
33. Mestecky J, Moldoveanu Z, Smith PD, Hel Z, Alexander RC. Mucosal immunology of the genital and gastrointestinal tracts and HIV-1 infection. J Reprod Immunol. 2009;83(1):196–200. doi:10.1016/j.jri.2009.07.005
34. Veselinovic M, Yang KH, Sykes C, Remling-Mulder L, Kashuba ADM, Akkina R. Mucosal tissue pharmacokinetics of the integrase inhibitor raltegravir in a humanized mouse model: implications for HIV pre-exposure prophylaxis. Virology. 2016;489:173–178. doi:10.1016/j.virol.2015.12.014
35. Thompson CG, Cohen MS, Kashuba ADM. Antiretroviral pharmacology in mucosal tissues. J Acquir Immune Defic Syndr. 2013;63(0 2):S240–S247. doi:10.1097/QAI.0b013e3182986ff8
36. Heneine W, Kashuba A. HIV prevention by oral preexposure prophylaxis. Cold Spring Harb Perspect Med. 2012;2(3):a007419. doi:10.1101/cshperspect.a007419
37. Improving Pre-Exposure Prophylaxis (PrEp) Delivery for HIV Prevention Among Women of Reproductive Age in Sub-Saharan Africa - ProQuest. Availabe from: https://www.proquest.com/docview/3081986463.
38. Landovitz RJ, Donnell D, Clement ME, et al. Cabotegravir for HIV prevention in cisgender men and transgender women. N Engl J Med. 2021;385(7):595–608. doi:10.1056/NEJMoa2101016
39. Delany-Moretlwe S, Hughes JP, Bock P, et al. Cabotegravir for the prevention of HIV-1 in women: results from HPTN 084, a phase 3, randomised clinical trial. Lancet. 2022;399(10337):1779–1789. doi:10.1016/S0140-6736(22)00538-4
40. Baeten JM, Palanee-Phillips T, Brown ER, et al. Use of a vaginal ring containing dapivirine for HIV-1 prevention in women. N Engl J Med. 2016;375(22):2121–2132. doi:10.1056/NEJMoa1506110
41. Nel A, van Niekerk N, Van Baelen B, et al. Safety, adherence, and HIV-1 seroconversion among women using the dapivirine vaginal ring (DREAM): an open-label, extension study. Lancet HIV. 2021;8(2):e77–e86. doi:10.1016/S2352-3018(20)30300-3
42. Gilead Announces Clinical Hold on Studies Evaluating Injectable Lenacapavir for HIV Treatment and Prevention Due to Vial Quality Concerns. Available from: https://www.gilead.com/news/news-details/2021/gilead-announces-clinical-hold-on-studies-evaluating-injectable-lenacapavir-for-hiv-treatment-and-prevention-due-to-vial-quality-concerns.
43. Choi YH, Zhang C, Liu Z, Tu MJ, Yu AX, Yu AM. A novel integrated pharmacokinetic-pharmacodynamic model to evaluate combination therapy and determine in vivo synergism. J Pharmacol Exp Ther. 2021;377(3):305–315. doi:10.1124/jpet.121.000584
44. Bekerman E, Yant SR, VanderVeen L, et al. Long-acting lenacapavir acts as an effective preexposure prophylaxis in a rectal SHIV challenge macaque model. J Clin Invest. 2023;133(16):e167818. doi:10.1172/JCI167818
45. Han M, Koziolek M. Evaluation of drug absorption from oral dosage forms. In: Developing Solid Oral Dosage Forms. Academic Press; 2026: 369–410. doi:10.1016/B978-0-443-34156-4.00023-6
46. Di Perri G. Pharmacological outlook of Lenacapavir: a novel first-in-class Long-Acting HIV-1 Capsid Inhibitor. Infez Med. 2023;31(4):495–499. doi:10.53854/liim-3104-8
47. Alidori S, Subramanian R, Holm R. Patient-centric long-acting injectable and implantable platforms─an industrial perspective. Mol Pharm. 2024;21(9):4238–4258. doi:10.1021/acs.molpharmaceut.4c00665
48. Rutstein SE, Smith DK, Dalal S, Baggaley RC, Cohen MS. The initiation, discontinuation and re-starting of HIV pre-exposure prophylaxis (PrEP): an ongoing evolution of implementation strategies. Lancet HIV. 2020;7(10):e721–e730. doi:10.1016/S2352-3018(20)30203-4
49. Clinical Results of YEZTUGO (lenacapavir) | YEZTUGO HCP. Available from: https://www.yeztugohcp.com/efficacy.
50. Ma EL. New research: high prevention efficacy and “breakthrough infections” on lenacapavir for PrEP. San Francisco AIDS Foundation. February 24, 2026. Available from: https://www.sfaf.org/collections/beta/new-research-high-prevention-efficacy-and-breakthrough-infections-on-lenacapavir-for-prep/.
51. Pennetzdorfer N, Naik V, Demirdjian S, et al. Lenacapavir treatment–emergent HIV-1 capsid resistance mutations are frequently associated with replication defects. Sci Transl Med. 2026;18(831):eaea0947. doi:10.1126/scitranslmed.aea0947
52. Briganti L, Annamalai AS, Bester SM, et al. Structural and mechanistic bases for resistance of the M66I capsid variant to lenacapavir. mBio. 2025;16(5):e03613–24. doi:10.1128/mbio.03613-24
53. Chen NY, Cheng CY, Lo SH, et al. Prevalence of naturally occurring HIV-1 capsid inhibitor resistance–related mutations in antiretroviral therapy–naïve and –experienced individuals in Taiwan. Open Forum Infect Dis. 2025;12(2):ofaf028. doi:10.1093/ofid/ofaf028
54. Sunlenca Prescribing Information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215973s006,215974s008lbl.pdf.
55. Hill A, Levi J, Fairhead C, et al. Lenacapavir to prevent HIV infection: current prices versus estimated costs of production. J Antimicrob Chemother. 2024;79(11):2906–2915. doi:10.1093/jac/dkae305
56. Adepoju VA, Abdulrahim A. Dollars and dilemmas: lenacapavir’s pricing, patents, and the path to affordability. Int J Equity Health. 2025;24(1):270. doi:10.1186/s12939-025-02610-3
57. Global HIV & AIDS statistics — fact sheet | UNAIDS. Available from: https://www.unaids.org/en/resources/fact-sheet.
58. MSF’s call for direct access to lenacapavir | MSF. Available from: https://www.msf.org.za/news-and-resources/news-and-resources/msf-s-call-direct-access-lenacapavir.
59. Implementation considerations and research gaps: lenacapavir for HIV prevention. In: Guidelines on Lenacapavir for HIV Prevention and Testing Strategies for Long-Acting Injectable Pre-Exposure Prophylaxis [Internet]. World Health Organization; 2025.
60. Marzinke MA, Grinsztejn B, Fogel JM, et al. Characterization of human immunodeficiency virus (HIV) infection in cisgender men and transgender women who have sex with men receiving injectable cabotegravir for HIV prevention: HPTN 083. J Infect Dis. 2021;224(9):1581–1592. doi:10.1093/infdis/jiab152
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lack of Resistance Mutations to the Novel HIV-1 Capsid Inhibitor Lenacapavir Among People Living with HIV in Guangdong, China
Lin Y, Ling X, Li L, Xin R, Hu F, Li J, Li J, Li F, Lan Y
Infection and Drug Resistance 2024, 17:4271-4277
Published Date: 2 October 2024