")
Back to Journals » Open Access Emergency Medicine » Volume 15
Lemierre Syndrome: Incidental Finding of Forgotten Fatal Disease as a Complication of Ludwig’s Angina
Authors Nur Iyow S, Uzel M, Ibrahim IG , Artan Abdi A, Farah Yusuf Mohamud M
Received 10 March 2023
Accepted for publication 19 July 2023
Published 22 July 2023 Volume 2023:15 Pages 259—263
DOI https://doi.org/10.2147/OAEM.S408470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Sowdo Nur Iyow, Muzeyyen Uzel, Ismail Gedi Ibrahim, Abdihakim Artan Abdi, Mohamed Farah Yusuf Mohamud
Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Farah Yusuf Mohamud, Mogadishu Somali-Turkish Education and Research Hospital, 30 Street, Alikamin, Wartanabada District, Mogadishu, Somalia, Tel +252615591689, Email [email protected]
Abstract: Lemierre syndrome (LS) is a rare, life-threatening complication of oropharyngeal infections associated with septicemia and internal jugular thrombosis. Internal jugular vein thrombosis is an uncommon disease associated with central vein catheterization, intravenous drug abuse, hypercoagulability, trauma to the neck, infection, ovarian hyperstimulation syndrome (OHSS), and systemic infections. Here, we highlight a case of a 62-year-old women who presented progressively worsening neck swelling for three weeks, shortness of breath, and fever for four days. Her sepsis due to Ludwig’s angina was accompanied by septic pulmonary embolism and internal jugular vein thrombosis in keeping with a diagnosis of Lemierre syndrome. For this presentation of Lemierre syndrome, the treating physicians recommended surgical excision and drainage, followed by intravenous antibiotics and subcutaneous anticoagulation to treat septic emboli of the lungs and internal jugular veins. Sadly, after being informed about the procedure, the patient refused to consent, and four days later, she passed away. It is essential to remember that early detection and aggressive treatment may significantly impact prognosis and outcome.
Keywords: Lemierre syndrome, internal jugular vein thrombosis, septicemia, Fusobacterium necrophorum, emergency department
Introduction
Lemierre syndrome (LS) is an unusual, potentially life-threatening complication of oropharyngeal infections associated with septicemia and internal jugular thrombosis with septic emboli.1 It was initially described by Courmont and Cade in 1900. Still, in 1936, a French microbiologist named Andre Lemierre initially published a case series of 20 patients having anaerobic septicemia secondary to oropharyngeal infection with cervical extension.1,2 It was initially named post-anginal septicemia, and then a “forgotten disease” by becoming a rare condition after the advent of antibiotics. It has also been named necrobacillosis due to Fusobacterium necrophorum.3,4 The most frequent cause of the disease is thought to be the commensal oral bacteria called Fusobacterium necrophorum. Other bacteria that could be involved include Bacteroides, Enterococcus, Streptococcus groups B and C, Streptococcus oralis, Staphylococcus epidermitis, and Proteus mirabilis.5
Here, we report a 62-year-old women diagnosed with Lemierre syndrome, which resulted from Ludwig’s Angina and complicated with internal jugular veins thrombosis due to septic emboli. For this presentation of Lemierre syndrome, the treating physicians recommended surgical excision and drainage, followed by intravenous antibiotics and subcutaneous anticoagulation to treat septic emboli of the lungs and internal jugular veins. Sadly, after being informed about the procedure, the patient refused to consent, and four days later, she passed away.
Case Report
A 62-year-old women came to the emergency department (ED) complaining of progressively neck swelling for three weeks, shortness of breath and fever for four days. Due to the point of care, she could not eat or drink due to neck swelling and dyspnea. The patient has had a history of esophageal carcinoma for one year. Six months later, after completing chemotherapy, she felt severe pain in the fourth molar, and the infected teeth had been extracted. She took oral klavunat 1000 mg two times per day for 10 days. After one week, she developed bilateral neck and facial swelling that continued up to three weeks, fever and dyspnea. On ER admission, she was confused with signs of respiratory distress. She was febrile (T=39.9°C) with a pulse rate of 131 beats per minute, respiratory rate of 33 breaths per minute, blood pressure of 145/85 mmHg, and oxygen saturation of 88% in room air. On neck examination, diffuse bilateral neck swelling and an infected wound on the right side of the neck, particularly in the submandibular space were detected (Figure 1). Neck extension and rotation were painful and limited. Cervical tender lymph nodes were palpable. The right external jugular vein had become a palpable strand with severe tenderness. Ear examination showed a normal tympanic membrane with no mastoid tenderness bilaterally. There was no evidence of facial nerve palsy or trismus. Her respiratory, cardiovascular, abdomen, and locomotory systems were normal.
 |
Figure 1 CT scan of the neck shows multiple peripheral contrast-enhancing abscesses in both sides of the neck (bilateral neck abscess). |
Results of initial laboratory evaluations was obtained. They revealed a white blood cell (WBC) count of 19.4 (4.1–10×103/uL), elevated C reactive protein level of 35 (0–10mg/dL), and elevated urea level of 77mg/dL. Initial serum electrolytes, blood creatinine levels, and liver function tests were within normal ranges.
Contrast-enhanced computed tomography (CT) of the neck revealed multiple-hypodense lesions, the largest one measuring 4x4cm in size with peripheral contrast enhancement in the bilateral perivertebral, submental, anterior cervical, and right supraclavicular regions (Abscesses) (Figure 1). Also, there is diffuse thickening and edema of the neck skin and subcutaneous area with emphysematous appearances in the subcutaneous area more prominent in the right of the neck and extending up to the right infra-clavicular region (Necrotising fasciitis of the neck) (Figure 2). While contrast-enhanced, CT imaging of the chest revealed multiple small-sized and peripherally located solid nodules and cavotation in the upper lobes of the lungs entering the examination field (Septic emboli) (Figure 3). Bilateral common jugular veins were not visualized and showed a filling defect extending from the jugular foramen to the common jugular confluence, suggestive of high-grade partial occlusion due to septic thrombus formation (Lemierre syndrome) (Figure 4). Also echocardiography was performed, valvular regurgitation and vegetations were not revealed.
 |
Figure 2 Coronal and axial neck CT scan reveals inflamed soft tissue with loculated gas in the right side of the neck and supraclavicular region (necrotising fasciitis of the neck). |
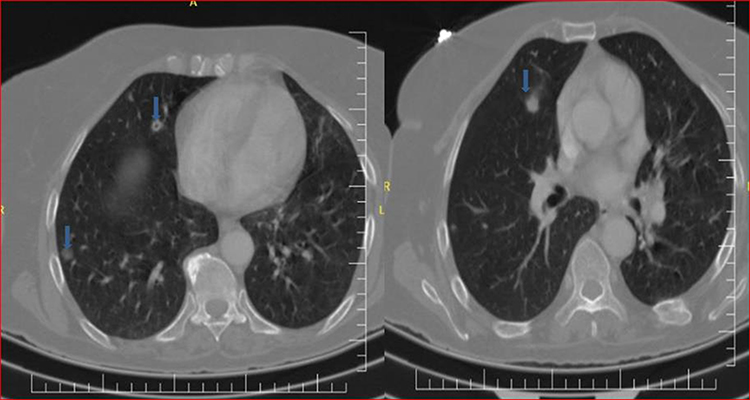 |
Figure 3 Axial chest CT shows several peripheral predominant nodules and some cavitation in both lungs (septic pulmonary embolism). |
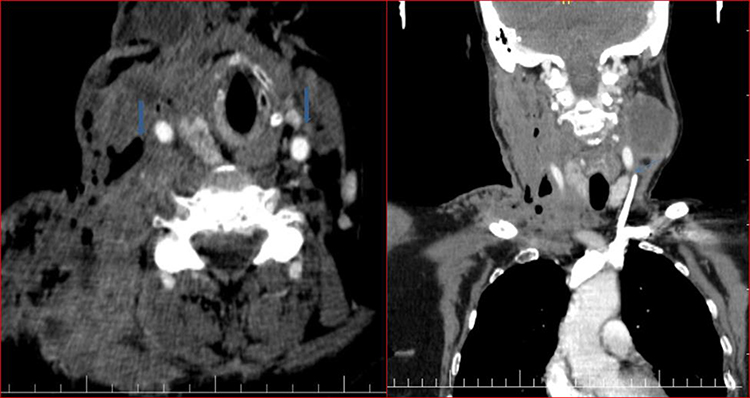 |
Figure 4 A CT scan of the neck reveals no contrast flow and filling defects in both jugular veins, indicating thrombosis. |
In the ED, the patient was kept on intravenous fluid resuscitation with analgesic and non-steroidal anti-inflammatory drugs (tramadol and ketoprofen), metronidazole (500mg 8 hourly via intravenous route), gentamicin (80mg 8 hourly via intravenous route), and ceftriaxone (1 gram 8 hourly via intravenous route). The pus in the right supraclavicular region was aspirated by inserting a 10-mL syringe. The pus was sent for culture and sensitivity. However, no growth was seen. Also, the patient started anticoagulation therapy (enoxaparin 4000 IU subcutaneous injection). For this presentation of Lemierre syndrome, the treating physicians recommended surgical excision and drainage. Also, we planned to take blood culture, unfortunately, the patients family refused for further investigation. Sadly, after being informed about the procedure, the patient refused to consent, and four days later, she passed away.
Discussion
Lemierre syndrome (LS) is a potentially life-threatening complication of oropharyngeal infections combined with suppurative thrombophlebitis of the internal jugular vein, septicemia, and occasionally metastatic septic embolus to various areas of the body, including the lungs.1 The leading cause of Lemierre disease is the pathogen Fusobacterium necrophorum.4 Streptococcus species, Enterococcus species, Bacteroides species, Peptostreptococcus species, Staphylococcus epidermitis species, Proteus mirabilis species, and Eikenella corrodens have all been identified as additional Lemierre disease-causing microbes.5
One particular case of unilateral Lemierre syndrome with cranial epidural abscess complication was reported from Somalia by Ibrahim et al. The patient was a 24-year-old male with a history of sore throat, malaise, fever, and neck and facial edema.6
The prevalence of this condition has substantially decreased since the development of antibiotics. The widespread use of penicillin to treat oropharyngeal infections is thought to be the main factor for the condition’s dramatic decline in prevalence.7
Our patient presented with worsening neck swelling for three weeks, shortness of breath, and fever, similar symptoms noted in previous studies.3,8 Also, neck extension and rotation were painful and limited in our case. The patient developed Lemierre disease despite getting oral antibiotics in this case report. This might be due to her use of chemotherapy which contributed to the propagation of Ludwig’s angina into Lemierre disease. The hallmark of this syndrome is internal jugular vein (IJV) thrombosis or thrombophlebitis. The diagnosis of classical Lemierre syndrome is based mainly on a clinical one fulfilling three criteria: oropharyngeal infection, metastatic infection, and internal jugular vein thrombophlebitis or thrombosis.1,3,4,8 In the current case, contrast-enhanced computed tomography (CT) of the neck and chest revealed multiple hypodense lesions with peripheral contrast enhancement in the bilateral perivertebral, submental, anterior cervical, and right supraclavicular regions (Abscesses), diffuse thickening and edema of the neck skin and subcutaneous area with emphysematous appearances (Necrotising fasciitis of the neck), multiple small-sized and peripherally located solid nodules in the upper lobes of the lungs (Septic emboli), and bilateral internal jugular vein filling defects indicative of high-grade partial occlusion due to septic thrombus formation.
This demonstrates the often different presentation of illness in the elderly and the importance of maintaining a high index of suspicion for necrotizing fasciitis and Lemierre syndrome in the setting of Ludwig’s angina.
Surgery to remove necrotic tissue with abscess drainage, anticoagulation therapy, and empiric broad-spectrum intravenous antibiotics, followed by culture-based antibiotics, are the cornerstones of treatment for necrotising fasciitis of the neck accompanied by Lemierre syndrome.3,4 On ER admission, we started intravenous fluid resuscitation as well as broad-spectrum intravenous antibiotics and anticoagulants. 10 mL of pus syringe was aspirated in the right supraclavicular region. The pus was sent for culture and sensitivity. However, no growth was seen, and this may be whether the previous use of antibiotics or a failure in the collection procedures for anaerobic organisms may have had some influence on the negative bacterial growth outcome. In the current case, she used empiric antibiotics for two weeks. Similarly to our case, Apar et al reported a 70-year-old women who developed LS due to a retropharyngeal space abscess. Around 10mL of pus was aspirated. The pus was sent for culture and sensitivity, and no growth was seen.9
Our case comes with a history of worsening neck swelling for three weeks, shortness of breath, and fever. On radiological examination revealed bilateral neck abscesses, necrotising fasciitis, septic emboli, and bilateral internal jugular vein thrombosis. The patient was managed with fluid resuscitation, analgesics, broad-spectrum antibiotics, and anticoagulants. Although the definitive treatment for this stage of Ludwig’s angina is surgical excision, debridement, and pus drainage. Sadly, after being informed about the procedure, the patient refused to consent, and four days later, she passed away.
Conclusion
Although this is the first case of Lemierre syndrome in Somalia, this condition should not be forgotten because timely and aggressive treatment may improve prognosis and outcome.
Data Sharing Statement
We declared that we had full access to all of the data in this study, and we take complete responsibility for the integrity of the data. All original data are available in the Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia. Data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval
Based on the regulations of the review board of the Mogadishu Somali Turkish Training and Research Hospital, institutional review board approval is not required for case reports.
Consent for Publication
Written informed consent had obtained by the patient and her mother to have the case details and any accompanying images published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We declare that we have not received any financial support.
Disclosure
We declare that we have no conflicts of interest.
References
1. Courmont P. Sur une septico-pyohemie de l’homme simulant la peste et causee par un streptobacille anaerobie. Arch Med Exp Anat Pathol. 1900;12:393–418.
2. Lemierre A. On certain septicaemias due to anaerobic organisms. Lancet. 1936;227(5874):701–703. doi:10.1016/S0140-6736(00)57035-4
3. Gupta T, Parikh K, Puri S, et al. The forgotten disease: bilateral lemierre’s disease with mycotic aneurysm of the vertebral artery. Am J Case Rep. 2014;15:230. doi:10.12659/AJCR.890449
4. Alperstein A, Fertig RM, Feldman M, et al. Septic thrombophlebitis of the internal jugular vein, a case of Lemierre syndrome. Intract Rare Dis Res. 2017;6(2):137–140. doi:10.5582/irdr.2017.01021
5. Vargiami EG, Zafeiriou DI. Eponym: the Lemierre syndrome. Eur J Pediatr. 2010;169:411–414. doi:10.1007/s00431-009-1135-5
6. Ibrahim IG, Osman AA, Elmi AM, et al. Lemierre syndrome with cranial epidural abscess complication: a case report. Ann Med Surg. 2022;81:104478. doi:10.1016/j.amsu.2022.104478
7. Bartlett JG, Gorbach SL. Anaerobic infections of the head and neck. Otolaryngol Clin North Am. 1976;9(3):655–678. doi:10.1016/S0030-6665(20)32670-0
8. Veras RD, Barasuol LL, Lira CP, et al. Síndrome de Lemierre: relato de caso. J Vasc Brasileiro. 2018;17:337–340. doi:10.1590/1677-5449.002418
9. Pokharel A, Basnet P, Sharma B, Thapa K. Lemierre syndrome. A forgotten disease. Case report and review of literature. Int Med Case Rep J. 2019;Volume 12:367–371. doi:10.2147/IMCRJ.S218895
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.