Back to Journals » Infection and Drug Resistance » Volume 15
Lemierre Syndrome Due to Dialister pneumosintes: A Case Report
Authors Hirai J ![]() , Kuruma T
, Kuruma T ![]() , Sakanashi D, Kuge Y, Kishino T, Shibata Y, Asai N, Hagihara M, Mikamo H
, Sakanashi D, Kuge Y, Kishino T, Shibata Y, Asai N, Hagihara M, Mikamo H
Received 21 February 2022
Accepted for publication 20 May 2022
Published 31 May 2022 Volume 2022:15 Pages 2763—2771
DOI https://doi.org/10.2147/IDR.S359074
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Jun Hirai,1,2 Tessei Kuruma,3 Daisuke Sakanashi,2 Yuji Kuge,4 Takaaki Kishino,4 Yuuichi Shibata,5 Nobuhiro Asai,1,2 Mao Hagihara,6 Hiroshige Mikamo1,2
1Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute, Aichi, 480-1195, Japan; 2Department of Infection Control and Prevention, Aichi Medical University Hospital, Nagakute, Aichi, 480-1195, Japan; 3Department of Otolaryngology, Aichi Medical University Hospital, Nagakute, Aichi, 480-1195, Japan; 4Department of Emergency and Critical Care Medicine, Aichi Medical University Hospital, Nagakute, Aichi, 480-1195, Japan; 5Department of Pharmacy, Aichi Medical University Hospital, Nagakute, Aichi, 480-1195, Japan; 6Department of Molecular Epidemiology and Biomedical Sciences, Aichi Medical University, Nagakute, Aichi, 480-1195, Japan
Correspondence: Jun Hirai, Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute, Aichi, 480-1195, Japan, Tel +81-561-62-3311, Fax +81-561-76-2673, Email [email protected]
Abstract: Although Dialister pneumosintes is a commensal microorganism of the oral cavity, it may sometimes cause severe systemic infections. We report a case of Lemierre syndrome (LS), which developed after D. pneumosintes infection, in a 73-year-old Japanese woman who was admitted to the hospital for throat pain, neck swelling, and fever for 3 days. She had a 3-month history of neglected dental caries, gingivitis, and periodontitis. Physical examination revealed right tonsillar erythema and swelling, and computed tomography (CT) showed peritonsillar and retropharyngeal abscesses. Ampicillin/sulbactam was promptly administered after collecting two sets of blood cultures. Surgical drainage for peritonsillar and retropharyngeal abscesses was also conducted on the second hospital day. Although only commensal oral microflora grew in the culture from the drained pus, Gram-negative bacilli were confirmed in the anaerobic blood cultures. Metronidazole was administered intravenously; however, the fever and neck swelling persisted. Repeat CT performed on the fifth hospital day revealed right internal jugular vein thrombosis, a known complication of tonsillitis and pharyngitis once the infection extends beyond the oropharynx. We diagnosed she had coexisting LS, and anticoagulant therapy was added to her treatment regimen. Her condition improved, and she was discharged after completing 3 weeks of antibiotics. Conventional methods failed to identify the isolated bacterium, and 16S rRNA sequencing ultimately identified it as D. pneumosintes. In a literature review of bacteremia due to D. pneumosintes, poor oral hygiene was considered a probable risk factor for invasive D. pneumosintes infection. We consider this to be the case in our patient who presented with dental caries, gingivitis, and periodontitis. In addition, all cases revealed that the 16S rRNA gene sequencing is useful for identifying this species. Although the diagnosis of LS by physical examination is difficult, physicians should always consider it as a potential complication of infections in the pharyngeal area.
Keywords: Dialister pneumosintes, Lemierre syndrome, tonsillar abscess, retropharyngeal abscess, oral hygiene, anticoagulation
Introduction
Dialister pneumosintes, previously called Bacteroides pneumosintes, is a non-fermentative, anaerobic, Gram-negative bacillus. It was first isolated from a patient with influenza virus infection in the early 20th century.1 It is a commensal oral microbe and is mainly associated with oral cavity infections, such as gingivitis,2 periodontitis,3 and periapical abscess;4 however, it sometimes causes severe systemic infections even in previously healthy patients.5
Lemierre syndrome (LS) is a septic thrombophlebitis of the internal jugular vein (IJV) caused by an oropharyngeal infection. In general, the disease begins with an oropharyngeal infection and is often accompanied by inflammation in the venous wall, infected thrombosis in the lumen, inflammation of the surrounding soft tissues, sustained bacteremia, and septic embolism.6
In this report, we describe a case of LS that developed from an oropharyngeal abscess and bacteremia caused by D. pneumosintes in a patient with dental caries. Herein, we provide a checklist and recommendations for describing a case report in medicine.7
Case Report
A 73-year-old Japanese woman visited our hospital with a 3-day history of throat pain, bilateral neck swelling, and fever (day X-3). She had a 3-month history of dental caries on her right upper maxillary teeth, which were also complicated by gingivitis and periodontitis. Despite previous medical advice, these were left untreated. Upon admission (day X), she was noted to be febrile (temperature 40.1oC), trismic, and drooling secondary to odynophagia. On physical examination, right tonsillar erythema and swelling, and left-sided uvular deviation from a bulging soft palate were noted. Blood tests showed an elevated white blood cell count (15,700 cells/μL [normal range: 3300–8600]; neutrophils 93.6%) and C-reactive protein level (33.2 mg/dL [normal range: 0–0.14]). Chest radiography was unremarkable. Contrast-enhanced computed tomography (CT) revealed a right peritonsillar and retropharyngeal abscess (Figure 1). A diagnosis of oropharyngeal abscess was made, and she was started on intravenous ampicillin/sulbactam (ABPC/SBT) 12 g/day immediately after two sets of blood cultures were collected.
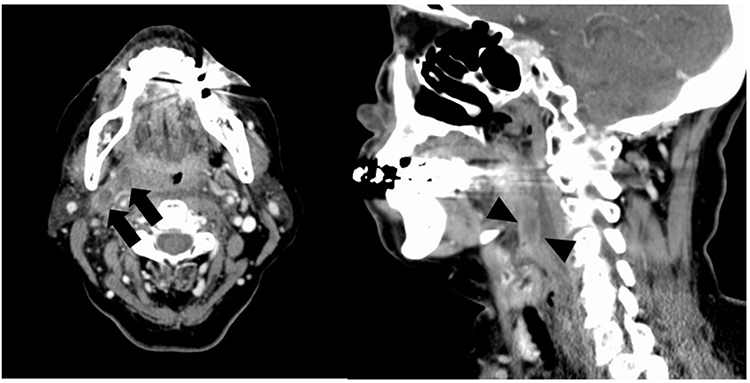 |
Figure 1 Enhanced computed tomography of the neck. Black arrow indicates a right peritonsillar abscess. Black arrowhead shows a retropharyngeal abscess. |
The next day (day X+1), an otolaryngologist performed surgical drainage of peritonsillar and retropharyngeal abscess, and the specimen was sent to the laboratory for culture. Results of the abscess culture later on showed growth of endogenous oral cavity bacteria. On day X+2, however, only anaerobic microorganisms growth was observed in the blood culture collected on admission, and Gram staining confirmed these as Gram-negative rods. Initially, these were thought to be the more commonly isolated Gram-negative anaerobic bacteria such as Fusobacterium spp. or Bacteroides spp., however, these could not be identified by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOFMS). Nonetheless, since the microorganism only grew in anaerobic medium, we treated empirically for an anaerobic infection and metronidazole (MNZ) was added to the ABPC/SBT regimen.
Despite antibiotics and antipyretics, however, the patient had elevation of body temperature, neck pain and swelling, and erythema along the sternocleidomastoid muscle on day X+4. Repeat CT conducted on day X+4 revealed right internal jugular vein thrombosis (IJVT) and a new abscess that was not seen on admission near the right thyroid gland (Figure 2). Since IJVT is the main feature of LS (pulmonary embolism and pulmonary septic emboli were not demonstrated in this case), parenteral heparin (15,000 units/day) was started for IJVT treatment from day X+4, and incision and drainage of the abscess beside the right thyroid gland was performed on day X+4 and X+5, which resulted in gradual recovery. The patient received intravenous antibiotics for 14 days, followed by oral fluoroquinolone for another 7 days. Parenteral heparin was administered for 10 days before switching to oral apixaban (Figure 3). She was discharged on day X+23 and advised proper oral hygiene to prevent recurrence of oropharyngeal infections.
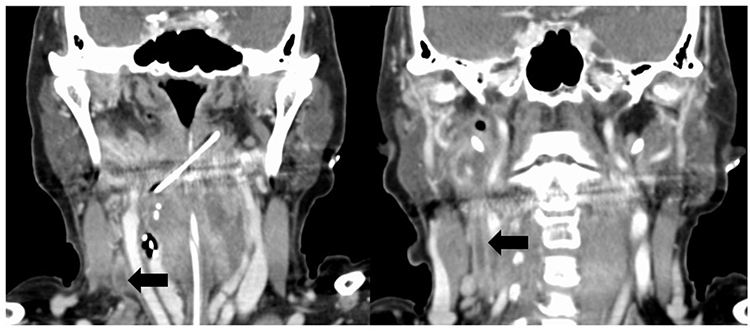 |
Figure 2 Enhanced computed tomography of the neck. Black arrow indicates right internal jugular vein thrombosis. |
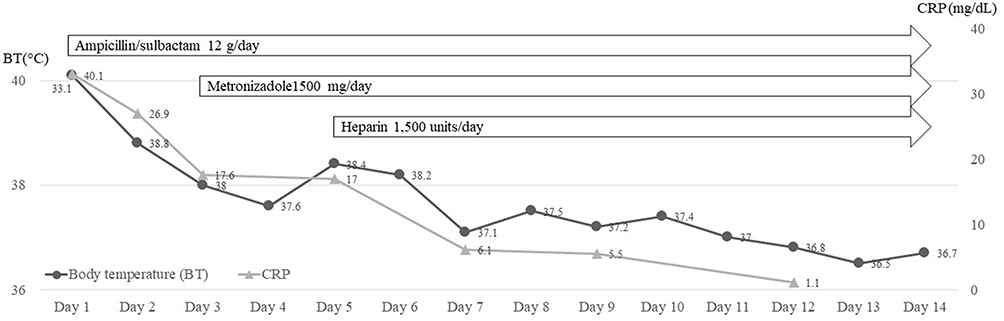 |
Figure 3 Clinical course of the present case. |
Figure 4 shows colony morphology of the isolated strain on Brucella HK agar plate. The colonies were small, circular, transparent, shiny, and smooth. To identify the isolated strain from blood cultures, we conducted PCR using suitable primers (Table 1)8 and amplified the target regions of 16S rRNA. As a result, the isolated pathogen was identified as D. pneumosintes with 99.93% homology. Figure 5 shows 16S rRNA sequences of the isolated strain. Figure 6 shows the hit taxon and name of the isolated strain on the EZ taxon database (http://www.ezbiocloud.net/eztaxon).9 Table 2 shows the antimicrobial susceptibility of the D. pneumosintes detected from blood cultures in the present case.
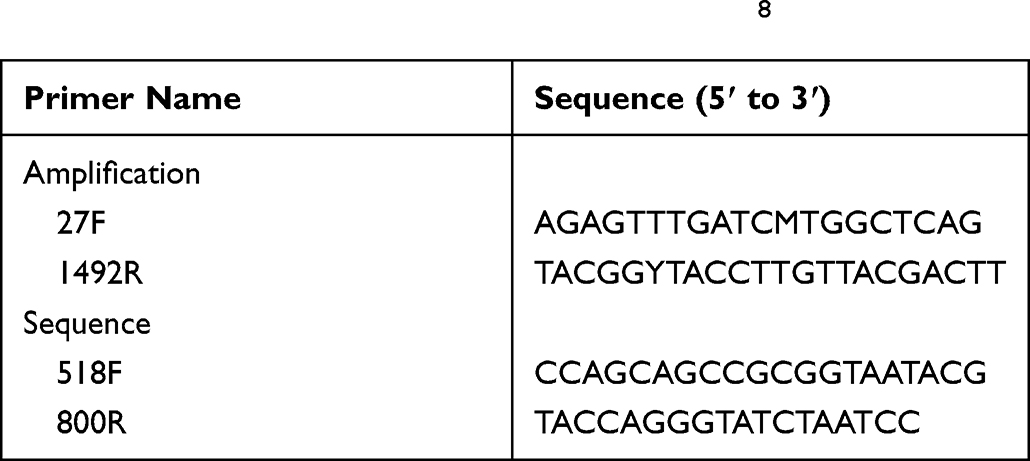 |
Table 1 Primers Used for 16S rRNA Sequencing8 |
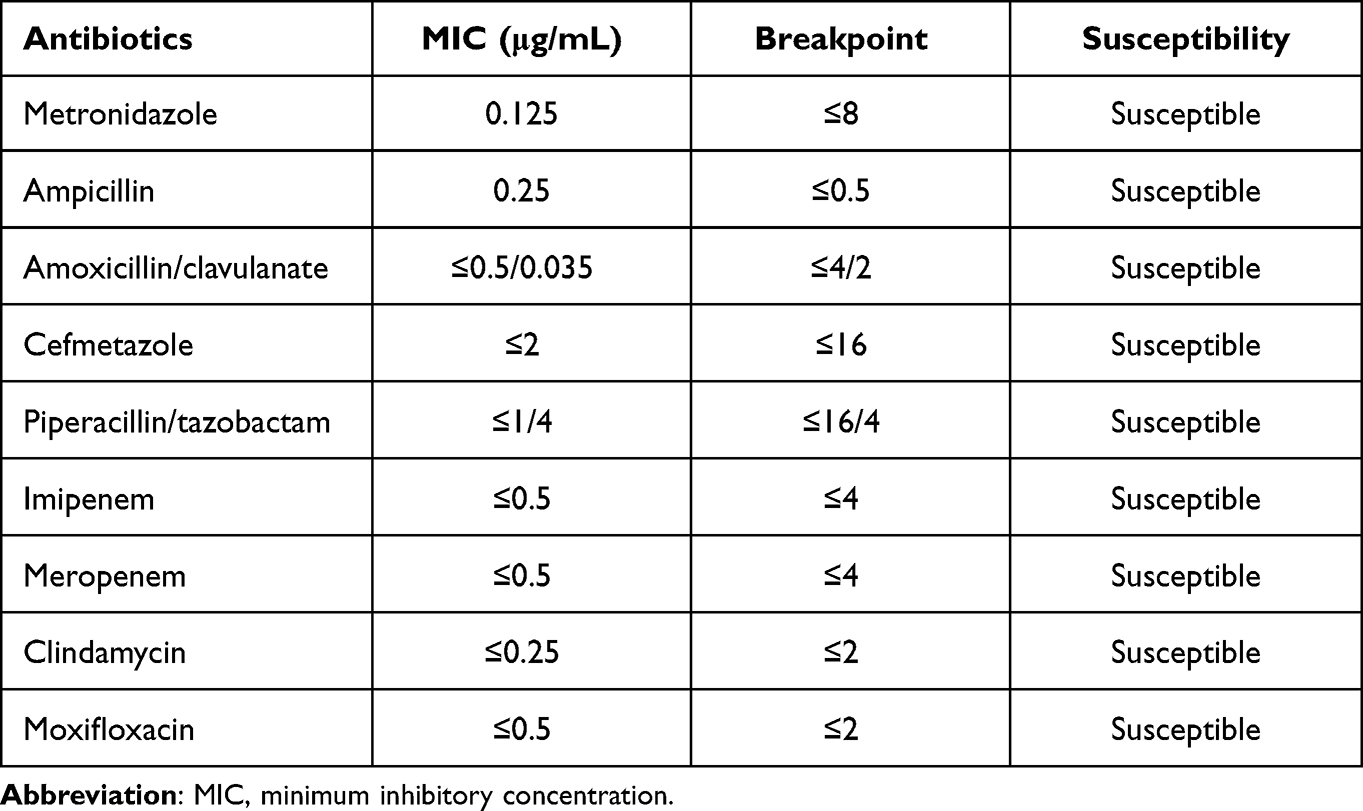 |
Table 2 Antimicrobial Susceptibility of Dialister pneumosintes Isolated in the Present Case. Breakpoint Was Measured Based on Clinical and Laboratory Standards Institute M100-S26 |
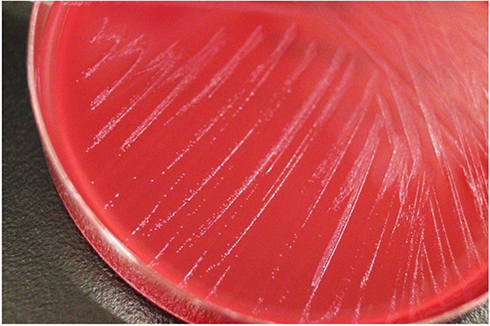 |
Figure 4 Colony morphology of the present strain on Brucella HK agar plate. |
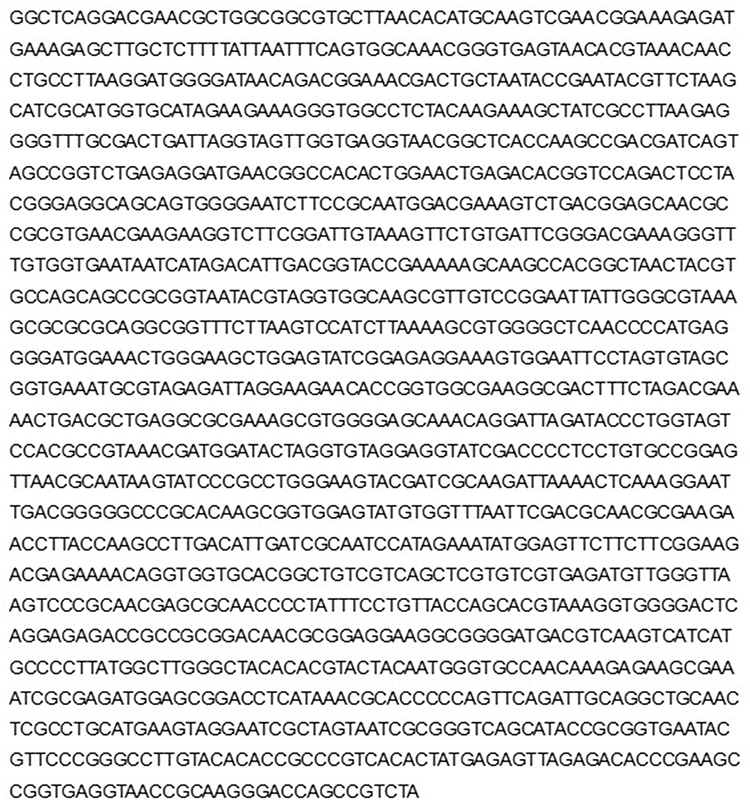 |
Figure 5 16S rRNA sequence of the isolated strain. |
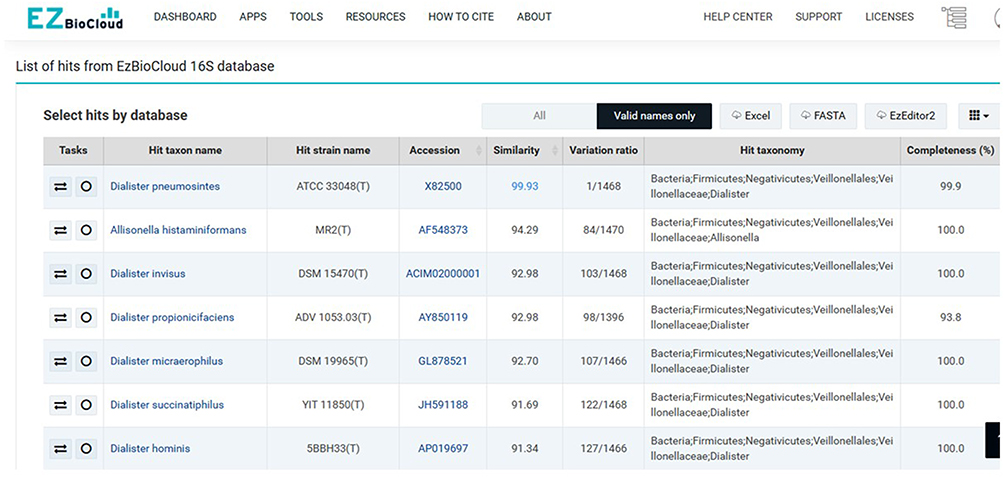 |
Figure 6 Hit taxon and strain name of the isolated strain. |
Discussion
Herein, we describe a case of LS associated with D. pneumosintes bacteremia in a patient with peritonsillar and retropharyngeal abscesses. D. pneumosintes is one of the endogenous bacteria in the oral flora, and previous reports have revealed that this pathogen can cause oral cavity infections, although its mechanism of infection and virulence have not been fully elucidated so far.2,3 A possible reason why our patient developed D. pneumosintes bacteremia was because of her neglected dental caries and poor oral hygiene, which ultimately led to tonsillopharyngitis and neck abscess formation.
LS is frequently preceded by pharyngitis, usually in association with tonsillar or peritonsillar inflammation, which spreads into the lateral pharyngeal spaces, leading to the subsequent formation of septic venous thrombosis of the IJV.6 In general, it is associated with anaerobic septicemia, most commonly caused by the anaerobe Fusobacterium necrophorum that, similar to D. pneumosintes,10 is an endogenous microorganism of the oral cavity and pharynx. Our patient presented with persistent fever with unilateral neck pain and redness, and repeat CT revealed IJVT, which we did not consider at the time of admission. Early diagnosis of LS can be challenging as it is difficult to identify IJVT based on physical examination findings. The neck swelling associated with IJVT can sometimes be mistaken for enlarged cervical lymph nodes instead.11 Strong clinical suspicion and careful examination are necessary for the diagnosis of LS. Although the clinical manifestation of LS may be non-specific, persistent fever and a swollen neck after antibiotic administration can be an important clinical clue for suspecting LS.12 Therefore, physicians should still consider LS when treating patients with oropharyngeal abscesses.
The utility of anticoagulation therapy for LS remains unclear. A recent meta-analysis of 194 patients with LS showed no statistically significant effect of anticoagulation on the LS mortality rate. However, these data were based on case reports.13 We started anticoagulation for vessel recanalization in the present case because there are data to support that anticoagulation may benefit patients whose symptoms do not resolve within 3 days of appropriate antimicrobial agents and drainage of purulent collections.14
As mentioned earlier, D. pneumosintes is typically related to infections of the oral cavity.2–4 However, previous studies also report that this pathogen causes systemic fetal infections such as endocarditis, ventilator-associated pneumonia, and deep-seated brain and liver abscess.15–17 Kaiser et al described a severe case of pneumonia due to D. pneumosintes, which finally induced acute respiratory distress syndrome and the patient required long-term mechanical ventilation. Mannan et al reported a case of neck and mediastinal abscess complicated by pulmonary embolism caused due to D. pneumosintes. Remarkably, these patients were immunocompetent but previously healthy. Therefore, physicians need to follow the clinical course carefully, given that this pathogen causes fetal infection even among healthy individuals. Although data are limited, a PubMed search yielded six other reports of bacteremia due to D. pneumosintes.4,5,18–21 In our available literature review from PubMed search (Table 3), D. pneumosintes caused severe infection in both children and adults, with women more likely to be infected than men. Notably, with our case included, 4 of 7 cases (57%) had oral infections such as cavities, gingivitis, and periodontitis. None of the patients died. One notable feature common to all reports was the use of genomic tests to identify the causative strain.
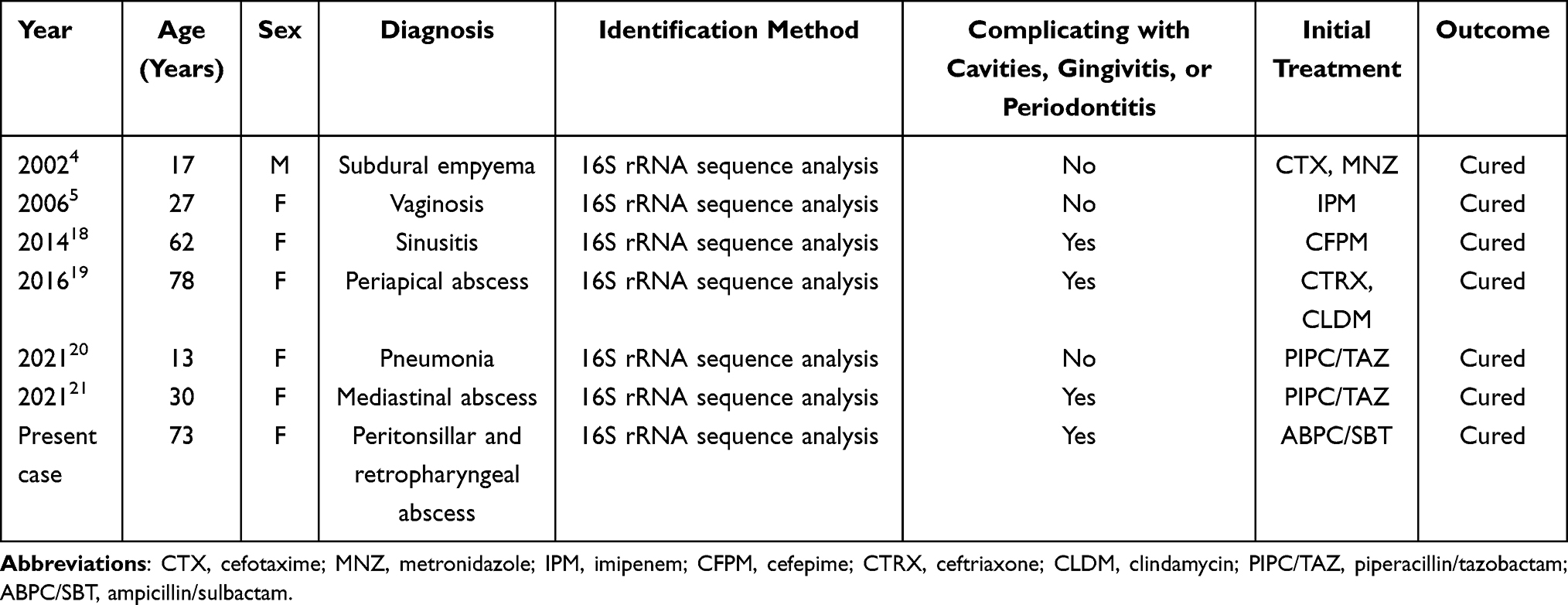 |
Table 3 Reported Cases of Dialister pneumosintes-Associated Bacteremia, Including the Present Case |
As it is difficult to identify D. pneumosintes by conventional biochemical tests, routine culture, MALDI-TOF MS, and genetic tests such as 16S rRNA gene sequencing are useful for the identification of this bacterium.22 The present case also highlights the efficacy of genetic testing in identifying microorganisms that are difficult to culture, such as D. pneumosintes, as is also described in a previous study.17 Although the most common pathogen of LS is an anaerobe,13 at times it is difficult to identify it by conventional methods even in a culture-positive situation as described in the present case report. In this situation, the use of 16S rRNA sequencing is helpful to identify the causative organism, thereby providing specific clues for the infected organ and correct selection of antibacterial agents, along with the determination of the treatment period.
MNZ is a bactericidal agent against anaerobic bacteria including Fusobacterium spp. and Bacteroides spp., which are Gram-negative rod-shaped species like D. pneumosintes, that sometimes cause oropharyngeal infection. Therefore, MNZ is the most commonly prescribed antibiotic when treating anaerobic bacterial infections including those due to Fusobacterium necrophorum, which is the most common cause of anaerobic septicemia. Interestingly, acquired resistance to MNZ among anaerobic bacteria is rare, despite extensive worldwide use.23 It is for these reasons that we administered MNZ for our case after cultures showed anaerobic bacterial growth. However, the patient had a persistent fever even after administration of ABPC/SBT and MNZ; we speculated that inadequate drainage of abscess and the complicated Lemierre syndrome induced such a situation. It is notable that Morio et al reported that D. pneumosintes showed decreased susceptibility to MNZ in 33 isolated strains from various clinical samples.24 They also identified amoxicillin, imipenem (IMP), and moxifloxacin (MFLX) as being very active against D. pneumosintes. Therefore, careful clinical follow-up is needed when treating D. pneumosintes infection with MNZ, and the use of alternative drugs such as IMP or MFLX should be considered when the clinical course worsens.
This case report has several limitations. First, we could not confirm D. pneumosintes from the abscess culture taken from the tonsillar abscess; this may probably have been due to the administration of antibiotics prior to the drainage of pus. We did not analyze the abscess culture taken from the tonsillar abscess for the 16S rRNA sequence, regardless of D. pneumosintes detection. In addition, the tonsillar abscess culture was not preserved at our hospital. Therefore, we cannot conduct 16S rRNA sequence analysis. Second, we did not culture any specimens from the dental cavities to identify D. pneumosintes. However, since this pathogen is mainly found in the oral cavity, we suspected that the dental caries, gingivitis, periodontitis, and bacteremia were due to D. pneumosintes in the present case. Kogure et al and Mannan et al also reported D. pneumosintes bacteremia derived from dental cavities.5,21 Further investigations are needed to clarify the association between D. pneumosintes bacteremia and oral cavity infection.
In summary, we encountered a case of LS with D. pneumosintes-associated bacteremia in a patient with cavities, gingivitis, and periodontitis. The take-home messages are (1) D. pneumosintes can be a cause of LS, (2) poor oral hygiene may be considered a probable risk factor for invasive D. pneumosintes infection, (3) physicians should suspect LS when faced with persistent fever and neck swelling after initiation of appropriate antibiotics in a patient with oropharyngeal infection, and (4) radiographic imaging (such as contrast-enhanced CT) of the neck allows for the evaluation and detection of IJVT.
Abbreviations
LS, Lemierre syndrome; CT, computed tomography; ABPC/SBT, ampicillin/sulbactam; MALDI-TOF MS, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; MNZ, metronidazole; IJVT, internal jugular vein thrombosis; CTX, cefotaxime; IPM, imipenem; CTRX, ceftriaxone; CLDM, clindamycin; PIPC/TAZ, piperacillin/tazobactam.
Data Sharing Statement
The data are available from the corresponding author upon reasonable request.
Ethics and Consent
We obtained written informed consent from the patient to publish the present case. This case report was not required to get the ethics committee approval based on the Japanese ethical guidelines for clinical research to publish the case details.
Acknowledgments
We appreciate Editage for emendation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Olitsky PK, Gates FL. Experimental studies of the nasopharyngeal secretions from influenza patients: i. Transmission experiments with nasopharyngeal washings. J Exp Med. 1921;33(2):125–145. doi:10.1084/jem.33.2.125
2. Sakamoto M, Rôças IN, Siqueira JF
3. Contreras A, Doan N, Chen C, Rusitanonta T, Flynn MJ, Slots J. Importance of Dialister pneumosintes in human periodontitis. Oral Microbiol Immunol. 2000;15(4):269–272. doi:10.1034/j.1399-302x.2000.150410.x
4. Lee MY, Kim YJ, Gu HJ, Lee HJ. A case of bacteremia caused by Dialister pneumosintes and Slackia exigua in a patient with periapical abscess. Anaerobe. 2016;38:36–38. doi:10.1016/j.anaerobe.2015.11.006
5. Mannan S, Ahmad T, Naeem A, Patel V. A case of Dialister pneumosintes bacteremia-associated neck and mediastinal abscess. Am J Case Rep. 2021;22:e930559. doi:10.12659/AJCR.930559
6. Dasari SP, Jha P. A systematic review of Lemierre’s syndrome with a focus on ophthalmologic complications. Cureus. 2020;12(7):e9326. doi:10.7759/cureus.9326
7. Behzadi P, Gajdács M. Writing a strong scientific paper in medicine and the biomedical sciences: a checklist and recommendations for early career researchers. Biol Futur. 2021;72(4):395–407. doi:10.1007/s42977-021-00095-z
8. Lane DJ. 16S/23S rRNA sequencing. In: Stackebrandt E, Goodfellow M, editors. Nucleic Acid Techniques in Bacterial Systematics. New York: John Wiley and Sons; 1991:115–175.
9. Yoon SH, Ha SM, Kwon S, et al. Introducing EzBioCloud: a taxonomically united database of 16S rRNA gene sequences and whole-genome assemblies. Int J Syst Evol Microbiol. 2017;67(5):1613–1617. doi:10.1099/ijsem.0.001755
10. Lee WS, Jean SS, Chen FL, Hsieh SM, Hsueh PR. Lemierre’s syndrome: a forgotten and re-emerging infection. J Microbiol Immunol Infect. 2020;53(4):513–517. doi:10.1016/j.jmii.2020.03.027
11. Allen BW, Anjum F, Bentley TP. Lemierre syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021.
12. Chirinos JA, Lichtstein DM, Garcia J, Tamariz LJ. The evolution of Lemierre syndrome: report of 2 cases and review of the literature. Medicine. 2002;81(6):458–465. doi:10.1097/00005792-200211000-00006
13. Gore MR. Lemierre syndrome: a meta-analysis. Int Arch Otorhinolaryngol. 2020;24(3):e379–e385. doi:10.1055/s-0039-3402433
14. Phua CK, Chadachan VM, Acharya R. Lemierre syndrome-should we anticoagulate? A case report and review of the literature. Int J Angiol. 2013;22(2):137–142. doi:10.1055/s-0033-1336828
15. Park JE, Huh HJ, Ha YE, Kim WS, Ki CS, Lee NY. A case of bacteremia caused by Dialister pneumosintes with Streptococcus anginosus. Ann Clin Microbiol. 2015;18(2):60–63. doi:10.1016/j.anaerobe.2015.11.006
16. Bahrani-Mougeot FK, Paster BJ, Coleman S, et al. Molecular analysis of oral and respiratory bacterial species associated with ventilator-associated pneumonia. J Clin Microbiol. 2007;45(5):1588–1593. doi:10.1128/JCM.01963-06
17. Soeiro C, Quilici IR, Legoff A, et al. Hepatic abscess due to Dialister pneumosintes—a case report. Anaerobe. 2019;59:35–37. doi:10.1016/j.anaerobe.2019.05.006
18. Kaiser M, Weis M, Kehr K, Varnholt V, Schroten H, Tenenbaum T. Severe pneumonia and sepsis caused by Dialister pneumosintes in an adolescent. Pathogens. 2021;10(6):733. doi:10.3390/pathogens10060733
19. Rousée JM, Bermond D, Piémont Y, et al. Dialister pneumosintes associated with human brain abscesses. J Clin Microbiol. 2002;40(10):3871–3873. doi:10.1128/JCM.40.10.3871-3873.2002
20. Pierre Lepargneur J, Dubreuil L, Levy J. Isolation of Dialister pneumosintes isolated from a bacteremia of vaginal origin. Anaerobe. 2006;12(5–6):274–275. doi:10.1016/j.anaerobe.2006.07.004
21. Kogure M, Suzuki H, Ishiguro S, et al. Dialister pneumosintes bacteremia caused by dental caries and sinusitis. Intern Med. 2015;54(6):663–667. doi:10.2169/internalmedicine.54.2904
22. Ferrand J, Bonnet I, Alauzet C, Lozniewski A. Evaluation of the Vitek MS and the MALDI Biotyper systems for the identification of less commonly isolated but clinically relevant anaerobes and facultative anaerobes. Anaerobe. 2018;54:210–216. doi:10.1016/j.anaerobe.2018.05.014
23. Snydman DR, Jacobus NV, McDermott LA, et al. Lessons learned from the anaerobe survey: historical perspective and review of the most recent data (2005–2007). Clin Infect Dis. 2010;50(suppl1):S26–S33. doi:10.1086/647940
24. Morio F, Jean-Pierre H, Dubreuil L, et al. Antimicrobial susceptibilities and clinical sources of Dialister species. Antimicrob Agents Chemother. 2007;51(12):4498–4501. doi:10.1128/AAC.00538-07
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.