Back to Journals » Research Reports in Clinical Cardiology » Volume 14
Left Ventricular Thrombosed Pseudoaneurysm as a Delayed Complication of Myxoma Resection and Mitral Valve Replacement: A Unique Case Report
Authors Omar Hassan M ![]() , Öcal L, Mire Waberi M
, Öcal L, Mire Waberi M ![]() , Abdullahi Ali A
, Abdullahi Ali A ![]() , Mohamud Hilowle N, Abdirahman Ahmed S
, Mohamud Hilowle N, Abdirahman Ahmed S ![]()
Received 25 February 2023
Accepted for publication 1 June 2023
Published 2 June 2023 Volume 2023:14 Pages 49—54
DOI https://doi.org/10.2147/RRCC.S410103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Kones
Mohamed Omar Hassan,1 Lütfi Öcal,1 Mohamud Mire Waberi,1 Abdijalil Abdullahi Ali,2 Nasra Mohamud Hilowle,3 Said Abdirahman Ahmed1
1Department of Cardiology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Cardiovascular Surgery, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 3Department Anesthesia and Reanimation, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Said Abdirahman Ahmed, Tel +252615583381, Email [email protected]
Introduction and Importance: A pseudoaneurysm of the left ventricle (LV) is a partial cardiac rupture surrounded by a pericardium that retains a connection with the LV lumen.
Case Presentation: We present here a 30-year-old patient who came to our clinic for a routine check-up with no symptoms or complaints. After performing echocardiography, the patient’s echocardiography demonstrated a left ventricular pseudo-aneurysm which had collected a massive amount of thrombus. Three years earlier, the patient had a left atrial myxoma excision with mechanical mitral valve replacement following a presentation with shortness of breath.
Clinical discussion: Left ventricular pseudo-aneurysm is a hazardous complication of mostly myocardial infraction and certain cardiac procedures, such as mitral valve replacement, where it may lead to thrombus formation. Due to this condition’s serious risk of lethal rupture and embolization from thrombus formation, as in our case, immediate surgical intervention is essential for its treatment.
Conclusion: Left ventricular pseudo-aneurysm is an abnormal finding post-cardiac surgery, and it should be considered during patient evaluation after the surgery immediately and later in life.
Keywords: myxoma, pseudo-aneurysm, mitral valve, mechanical valve
Introduction
A pseudoaneurysm of the left ventricle (LV) is a partial cardiac rupture surrounded by a pericardium that retains a connection with the LV lumen.1 In a true ventricular aneurysm, the outer layer always contains endocardium and myocardium with intact cardiac muscle.
Many case reports demonstrate that myocardial infarction (MI), cardiac surgery and procedures, infection, or trauma are all factors in its incidence.2,3 Left ventricular pseudo-aneurysm is a serious complication that can lead to heart failure, arrhythmia, distal embolization, and rupture of the left ventricular free wall. Rarely does pseudo-aneurysm of the LV wall lead to thrombus collection, but when it does, the consequences can be devastating.
Spielberg and O’Reilly discovered a pseudo-aneurysm using left ventriculography following mitral valve replacement (MVR), and it was the first case of its sort.4 During mitral valve replacement, the posterior wall can rupture, leading to an acute deterioration of the patient’s condition. Pseudo-aneurysm formation due to incomplete or delayed rupture is a very rare complication.
Case Presentation
This is the case of a 30-year-old man with no chronic diseases who came to our clinic for routine follow-up of his coagulation profile and mitral mechanical valve function and structure. Three years ago, the patient had a bi-leaflet prosthetic mechanical valve replacement of mitral valve due to a myxoma of the left atrium which disrupted the valve function and structural competence. Histopathological findings from the sample from the excisional biopsy showed low-grade myxoma. The tumor extends along stained surgical margins and non-diffusely infiltrates striated muscle cells of the myocardium with no lymphovascular invasion (Figure 1).
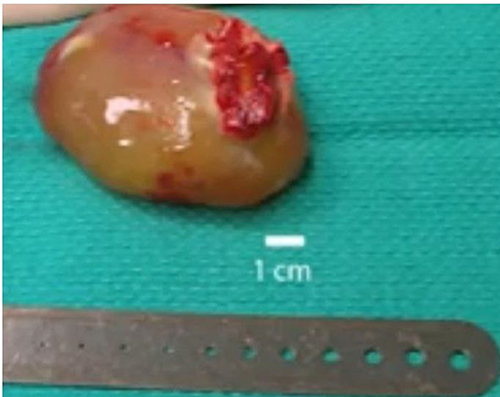 |
Figure 1 Sample from the excisional biopsy showing low-grade myxoma. |
After that, he recovered well and resumed his normal activities. After that, he did not have any symptoms or any complaints, and he was on 5 mg of warfarin with a blood international normalized ratio (INR) mostly above the target value, his latest value being INR 5.63.
At this presentation, the patient’s vital signs were also normal, and during the inspection, a blunted mechanical valve click was noted.
The patient exhibited no prosthetic valve malfunction and no evidence of structural problems during the last regular annual follow-up. However, after obtaining echocardiography for this patient, we discovered that he has multiple problems with his left ventricle and prosthetic valve. The electrocardiography of the patient revealed no abnormalities, including a steady rhythm and rate and no aberrant alterations (Figure 2). Transthoracic echocardiography showed a massive 40x50mm thrombotic mass occupying a pseudo-aneurysm that had developed in the inferior-lateral wall. Furthermore, the pseudo-aneurysm neck was calculated at 12.2mm (Figure 3A). The thrombus extended to the prosthetic valve and left atrium remarkably without causing stenosis of the valve or embolic sequelae (Figure 3B). The echocardiography also showed a large mass protruding longitudinally from the left atrium into the left ventricle, which had a different echogenicity and structure than the thrombus and looked very similar to that of the original myxoma (Figure 3C). The valve function was adequate with a mean gradient of 4 mmHg and no regurgitation was seen (Figure 3D). Due to the presence of a metallic valve, a chest CT scan with contrast was requested with the result of pseudo-aneurysm dilatation and thrombus in both sagittal and axial views (Figure 4A and B).
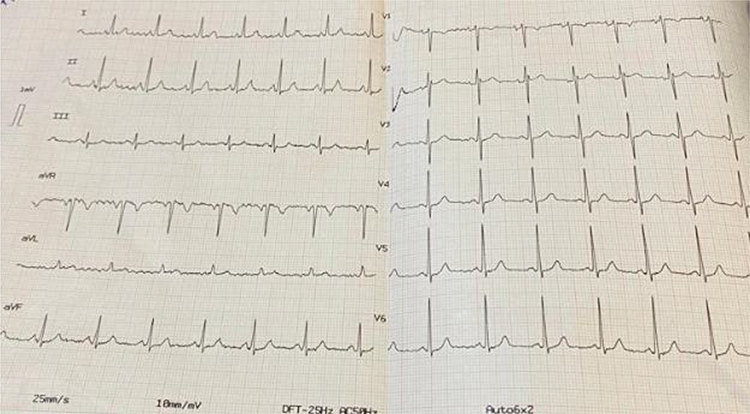 |
Figure 2 Shows normal electrocardiography of the patient. |
 |
Figure 3 (A) shows the narrow neck of the pseudo-aneurysm with diameter of 12mm (red arrow). (B) showing the pseudo-aneurysm as a mass appearing parallel to the left atrium in this view. (C) longitudinal mass protruding from the pseudo-aneurysm towards the left ventricle. (D) Continues wave Doppler assessment of the prosthetic valve. |
 |
Figure 4 Chest CT -Sagittal (A) and Axial (B) both showing left ventricle showing aneurysmic dilatation and thrombus formation (red arrow). |
Discussion
In contrast to a true aneurysm, a ventricular pseudo-aneurysm is surrounded by the pericardium, pericardial adhesions, or a thrombus. Endocardium and myocardium with an intact heart wall are always present in a true ventricular aneurysm’s outer layer.5 After an MI or cardiothoracic surgery, the majority of LV pseudo-aneurysms appear. In a systematic literature analysis of 290 patients, the top 3 associations were MI (55%), surgery (33%), and trauma (7%).6 With a frequency of about 0.23%, LV pseudo-aneurysms are extremely uncommon.7 In our case, the pseudo-aneurysm was a consequence of the surgical resection of myxoma and mitral valve replacement, which had not been reported in the literature as a delayed complication. There may be thrombus inside the LV pseudo-aneurysm, which could lead to a risk of systemic embolism.2 In our case, an organized thrombus had formed inside the pseudo-aneurysm, but luckily it has not embolised. Furthermore, it seems the thrombus had organized to a level at which it started to support the laminar flow of blood in the left ventricle.
In the literature, patients with LV pseudo-aneurysms (LVP) have been successfully diagnosed using non-invasive imaging techniques such as echocardiography, computed tomography angiograms, and cardiac magnetic resonance imaging (CMRI).8 We have successfully diagnosed this patient with noninvasive transthoracic echocardiography and a CT angiogram. The primary imaging technique for detecting LVP, even in asymptomatic individuals, is transthoracic echocardiography (TTE). Numerous publications have noted that TTE is particularly useful for the differential diagnosis of this problem and that it may be more accurate than ventricular angiography, even though occasionally unconventional perspectives are needed to detect tiny wall lesions.9 It can be difficult to distinguish between left ventricular pseudoaneurysms and true aneurysms. Comparing the aneurysm’s orifice/neck diameter to its maximal diameter on an echocardiogram is one approach to evaluating this.10 Similarly, we differentiated both by measuring the neck of the pseudo-aneurysm.
The ideal imaging modalities for separating pseudo-aneurysm from true aneurysm are CT and cardiac MRI because they offer superior spatial resolution and tissue definition to identify the myocardium from scar tissue and the pericardium.11 Due to mechanical valve replacement, we have not done a cardiac MRI, so instead we have requested a CT angiogram to differentiate between an aneurysm and a pseudoaneurysm. Due to its high risk of catastrophic rupture, urgent surgical intervention is crucial in the treatment of this condition.12 A dangerous complication of mitral valve replacement is rupture of the left ventricular posterior wall (MVR). Depending on when it is presented, it is typically divided into three categories: early, delayed, or late. Any time after cardiopulmonary bypass has been stopped, an early rupture incident can happen in the operating room. Delayed rupture is an incident that takes place several days or more after being transferred to the intensive care unit. Late rupture can occur days to years after mitral valve replacement (MVR).7
Risk factors include reoperation, endocarditis, severe annular calcification, poor operating field visibility, a small LV, and oversize prosthetic valves. A rupture of the LV free wall can also be caused by an increase in LV contractility after aortic cross clamping, an increase in LV wall stress from the help of inotropic agents, or other mechanical trauma between the free wall and the papillary muscles, such as when a rubber catheter is pushed into the papillary muscles or a metal pump is used to pull on the papillary muscles during valve replacement.13 Our case had a late LV pseudoeurysm formation due to what we believe is a delayed manifestation of mitral leaflet excision, which caused the LV’s fibrous components to become loose and enlarge overtime. The lack of any myocardial infraction-related findings on the electrocardiogram and echocardiography ruled out the possibility of a limited myocardial infraction, which can happen because of mitral valve replacement surgery. Due to the limited capabilities in our hospital, we recommended the patient go abroad to another hospital with cardiovascular surgery facilities.
Conclusion
LV pseudo-aneurysm is an abnormal finding post-cardiac surgery, and it should be considered during patient evaluation after the surgery immediately and later in life. Although rarely reported, LV pseudoaneurysm post-surgery can have devastating consequences and should be managed accordingly while keeping the patient’s optimal benefit in mind. Further methods should be developed to tackle this issue and treat it in the future.
Consent
Written informed consent had obtained by the patient to have the case details and any accompanying images published.
Acknowledgment
We would like to thank Dr Mohamed Sheikh Hassan (Member of Young Researchers Council) for his assistance and guidance in the manuscript preparation.
Funding
There is no funding to report.
Disclosure
We declare that we have no conflict of interest.
References
1. Jung HS, Chung WB, Yang KS, et al. A case of left ventricular pseudoaneurysm in the left atrioventricular groove after mitral valve replacement. J Cardiovasc Ultrasound. 2010;18(4):157–160. doi:10.4250/jcu.2010.18.4.157
2. Meng X, Yang YK, Yang KQ, et al. Clinical characteristics and outcomes of left ventricular pseudoaneurysm: a retrospective study in a single-center of China. Medicine. 2017;96(18):e6793. doi:10.1097/MD.0000000000006793
3. Spellberg RD, O’Reilly RJ. Pseudoaneurysm of the left ventricle following mitral valve replacement. Chest. 1972;62(1):115–117. doi:10.1378/chest.62.1.115
4. Inayat F, Ghani AR, Riaz I, et al. Left ventricular pseudoaneurysm: an overview of diagnosis and management. J Investig Med High Impact Case Rep. 2018;6:2324709618792025. doi:10.1177/2324709618792025
5. Frances C, Romero A, Grady D. Left ventricular pseudoaneurysm. J Am Coll Cardiol. 1998;32(3):557–561. doi:10.1016/S0735-1097(98)00290-3
6. Prêtre R, Linka A, Jenni R, Turina MI. Surgical treatment of acquired left ventricular pseudoaneurysms. Ann Thorac Surg. 2000;70(2):553–557. doi:10.1016/S0003-4975(00)01412-0
7. Ono M, Wolf RK. Left ventricular pseudoaneurysm late after mitral valve replacement. Ann Thorac Surg. 2002;73(4):1303–1305. doi:10.1016/S0003-4975(01)03268-4
8. Atik FA, Navia JL, Vega PR, et al. Surgical treatment of postinfarction left ventricular pseudoaneurysm. Ann Thorac Surg. 2007;83(2):526–531. doi:10.1016/j.athoracsur.2006.06.080
9. Tuan J, Kaivani F, Fewins H. Left ventricular pseudoaneurysm. Eur J Echocardiogr. 2008;9(1):107–109. doi:10.1016/j.euje.2007.03.043
10. Bisoyi S, Dash A, Nayak D, et al. Left ventricular pseudoaneurysm versus aneurysm a diagnosis dilemma. Ann Card Anaesth. 2016;19(1):169. doi:10.4103/0971-9784.173042
11. Abdelnaby M, Almaghraby A, Saleh Y, et al. A case of left ventricular Pseudoaneurysm [Internet]. J Heart Cardiovascu Res. 2017;1:1.
12. Abbood A, Al Salihi H, Olivier M, Khawaja F, Madruga M, Carlan SJ. Left ventricular pseudoaneurysm and left ventricular thrombus in a patient presenting with an acute ST-elevation myocardial infarction. Am J Case Rep. 2022;23:e934272. doi:10.12659/AJCR.934272
13. Duan QJ, Duan CT, Yang WJ, Dong AQ. Conservative treatment of left ventricular pseudoaneurysm after mitral valve replacement due to early left ventricular rupture: a case report. J Cardiothorac Surg. 2021;16(1):1–4. doi:10.1186/s13019-021-01436-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.