Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Learning Outcomes from Participation in Student-Run Health Clinics: A Systematic Review
Authors Wilson OWA ![]() , Broman P
, Broman P ![]() , Tokolahi E
, Tokolahi E ![]() , Andersen P, Brownie S
, Andersen P, Brownie S
Received 10 August 2022
Accepted for publication 6 December 2022
Published 19 January 2023 Volume 2023:16 Pages 143—157
DOI https://doi.org/10.2147/JMDH.S385709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Oliver WA Wilson,1– 3 Patrick Broman,1 Ema Tokolahi,1,4 Patrea Andersen,1,5,6 Sharon Brownie1,7,8
1Centre for Health and Social Practice, Waikato Institute of Technology Te Pūkenga, Hamilton, New Zealand; 2Department of Kinesiology, Pennsylvania State University, University Park, PA, USA; 3Te Hau Kori, Victoria University of Wellington, Wellington, New Zealand; 4School of Occupational Therapy, Otago Polytechnic Te Pūkenga, Dunedin, New Zealand; 5School of Nursing, Midwifery and Social Science, CQUniversity, Rockhampton, QLD, Australia; 6School of Nursing, Midwifery and Paramedicine, University of the Sunshine Coast, Sippy Downs QLD, Australia; 7School of Health Sciences, Swinburne University, Hawthorne, VIC, Australia; 8School of Medicine & Dentistry, Griffith University, Brisbane QLD, Australia
Correspondence: Sharon Brownie, School of Health Sciences, Swinburne University, Hawthorne, VIC, Australia, Email [email protected]
Abstract: Student-run clinics (SRCs) offer unique opportunities for students to engage in healthcare delivery, but the student learning outcomes of such clinics have not yet been systematically examined in a comprehensive manner. The purpose of this review was to appraise and synthesize existing literature pertaining to student learning outcomes associated with participation in SRCs. A systematic review was undertaken using PubMed, CINAHL, and Web of Science databases. The quality of articles that met inclusion criteria articles was appraised using the Mixed Methods Appraisal Tool (MMAT). Study details, such as learning outcomes, were also extracted. Ninety-two studies met inclusion criteria. Most studies were conducted in North America (n = 73, 79.3%), and related to clinics involving solely medical students (n = 35, 38.0%) or multi-professional clinics (n = 34, 37.0%). Demonstrated learning outcomes of SRC participation include clinical skills, interprofessional skills, empathy/compassion for underserved patients, and leadership. SRC participation had little apparent impact on students’ future career directions. Quality appraisal via the MMAT found mixed levels of research quality amongst reviewed studies. In summary, while SRC participation appears to offer benefits for student learning, improved study design and research outside of North American contexts would further advance knowledge.
Keywords: healthcare, undergraduate education, interprofessional education, multidisciplinary research, health workforce, student-led clinics, student-run, student-assisted
Introduction
A variety of skills and competencies require development as a part of the formal education of health professionals. Experiences outside the traditional classroom and placement settings in student-run clinics (SRCs), also referred to as student-led and/or student-assisted clinics, offer students the opportunity to gain early clinical and leadership experience via direct engagement in healthcare delivery.1 Some argue that such student-led service-learning should be a required component of health professional’s education.2
Understanding the learning outcomes which students achieve from participation is of obvious importance for those involved in SRCs and may have policy and program implications. Previous reviews have focused on students’ experiences and perceptions of participating in student-run clinics (SRCs),3 and the educational or learning outcomes of SRCs have also been the topic of systematic4 and rapid reviews.5 While these reviews offer valuable insight, they are dated and focus solely on entry-level students or interprofessional SRCs, respectively. The literature concerning the learning benefits associated with student involvement in all types of SRCs has not previously been systematically assessed.
Thus, the purpose of this systematic review is to systematically appraise and synthesize the literature concerning the learning outcomes of student involvement in SRCs. It seeks to address the following questions. First, what learning outcomes can students acquire by participating in SRCs? Second, what is the quality of the existing literature on this topic? To answer these questions, we adopt the broadest possible inclusion criteria to encompass SRCs regardless of geographic location, professions, or level of study.
Methods
This systematic review was undertaken in line with the quality guidance of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol.6 A comprehensive search strategy and selection process identified original research relating to student participation in SRCs.
Search Process
A systematic search was conducted in October 2022 using queries developed for several databases, including PubMed (MEDLINE), CINAHL (EBSCOHost), and Web of Science (Clarivate). Search strategies were developed in conjunction with a librarian. Three search term groups were included in search strategies. The first used terms concerning college/university/higher education. The second included the term student, and similar terms, along with “run” or “led” to specify the target population in addition to the context. Finally, the third used terms relating to clinics. The search was restricted to English-language studies only. Full search strategies are provided in Appendix A.
Source Selection
Following the database search, sources were aggregated within reference management software (EndNote X9.3.3, Clarivate, London, UK). Next, duplicates were removed using The Systematic Review Assistant-Deduplication Module (SRA-DM), a program shown to reliably remove duplicate records with excellent sensitivity and specificity.7 Remaining duplicates were removed using the EndNote software de-duplication function,8 as well as manually during abstract and title screening which was managed through the web application Rayyan QCRI.9
Source selection was guided by the inclusion and exclusion criteria detailed in Table 1. Criteria were established to acquire a comprehensive list of sources empirically measuring the learning outcomes of SRCs. Although only research published in English was considered for inclusion, no restrictions were placed on location, discipline, or date of publication.
 |
Table 1 Inclusion/Exclusion Criteria |
Data Extraction and Analyses
Data from each source that met inclusion criteria were extracted into Microsoft Excel (Microsoft Corporation, Redmond WA, version 16.60). Three authors (OW, PB, and ET) extracted source characteristics details (author name, year of publication, study location, study design, sample characteristics), and all authors appraised sources independently, with each source appraised by at least two authors. Discrepancies or uncertainties were then discussed and resolved by OW, PB, and ET. Given the heterogeneity in study approaches, sources were appraised using the Mixed Methods Appraisal Tool (MMAT).10 Educational and learning outcome categories were identified and extracted during the full-text review, and consolidated into broad categories for reporting purposes. Descriptive statistics to accompany a narrative analysis of learning outcomes were computed using Microsoft Excel.
Results
Initial searches retrieved 651 sources after deduplication. Sources were screened at the level of title and abstract followed by a full-text review of 266 sources. An additional 23 sources were identified beyond those identified via the database searches. Ultimately, 92 sources were underwent data extraction and synthesis. Figure 1 details the flow of sources through the review process, according to PRISMA guidelines.6
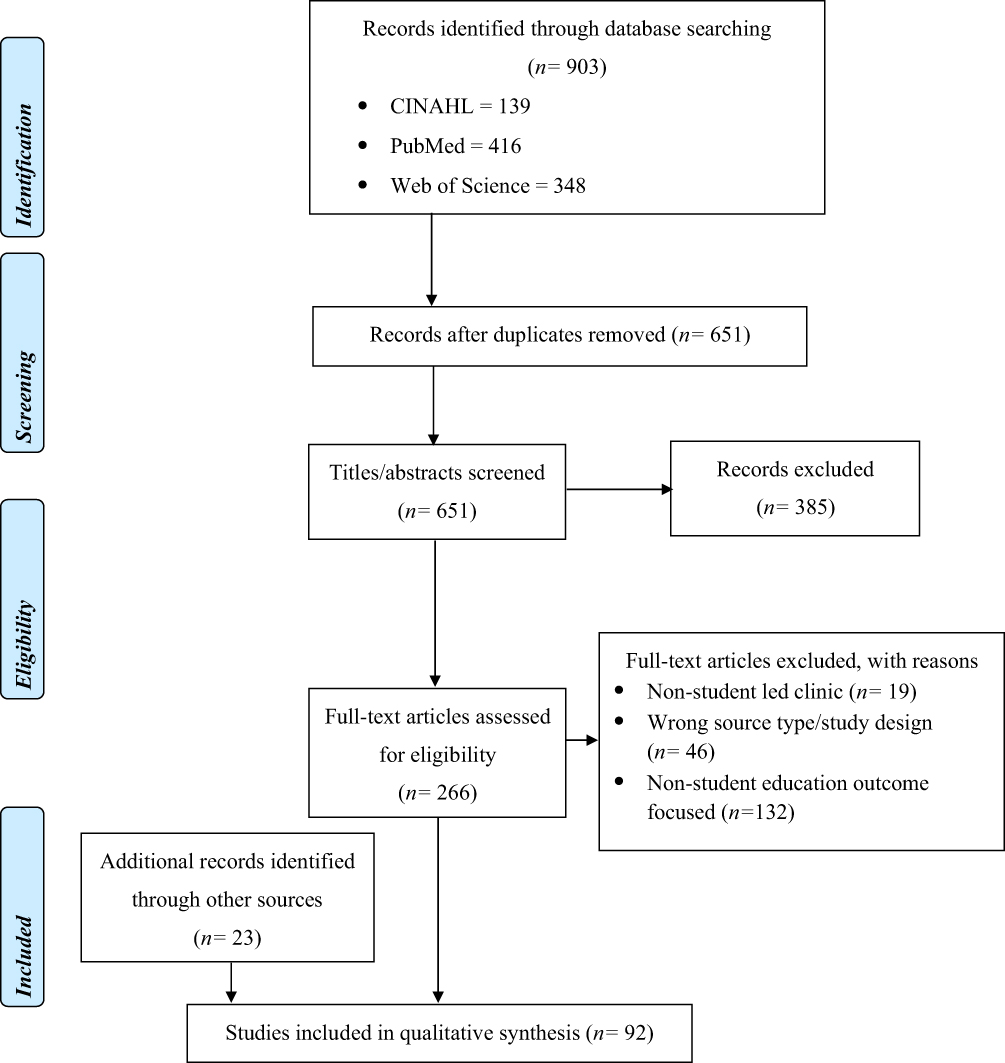 |
Figure 1 Study Flow Diagram. Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097.6 |
Study Characteristics
Study characteristics are displayed in Table 2. Most concerned SRCs in the United States (U.S.) (n = 63, 68.5%), with several in Canada (n = 10, 10.9%), a few in Australia (n = 6, 6.5%), three in The Netherlands (n = 3, 3.2%), two each in Ireland (n = 2, 2.2%), South Africa (n = 2, 2.2%), and Sweden (n = 2, 2.2%) and one each in Brazil, New Zealand, Singapore, and the United Kingdom. The most common type of student sampled was medical (n = 35, 38.0%), followed by an interprofessional group (n = 34, 36.9%), pharmacy (n = 8, 8.7%), physical therapy (n = 7, 7.6%), nursing students (n = 3, 3.3%), with single studies involving dentistry, occupational therapy, osteopathy, physician assistant and midwifery students. The most common design was retrospective (n = 61, 66.3%). Prospective studies, including one intervention (n = 25, 27.2%) were the next most common, with the remaining six cross-sectional (6.5%). Quantitative methods were the most common data collection method (n = 39, 42.4%), while 27 studies (29.3%) used mixed-methods, and 27 (28.3%) employed qualitative techniques such as focus groups, one-on-one interviews, and open-ended/free-text response survey questions.
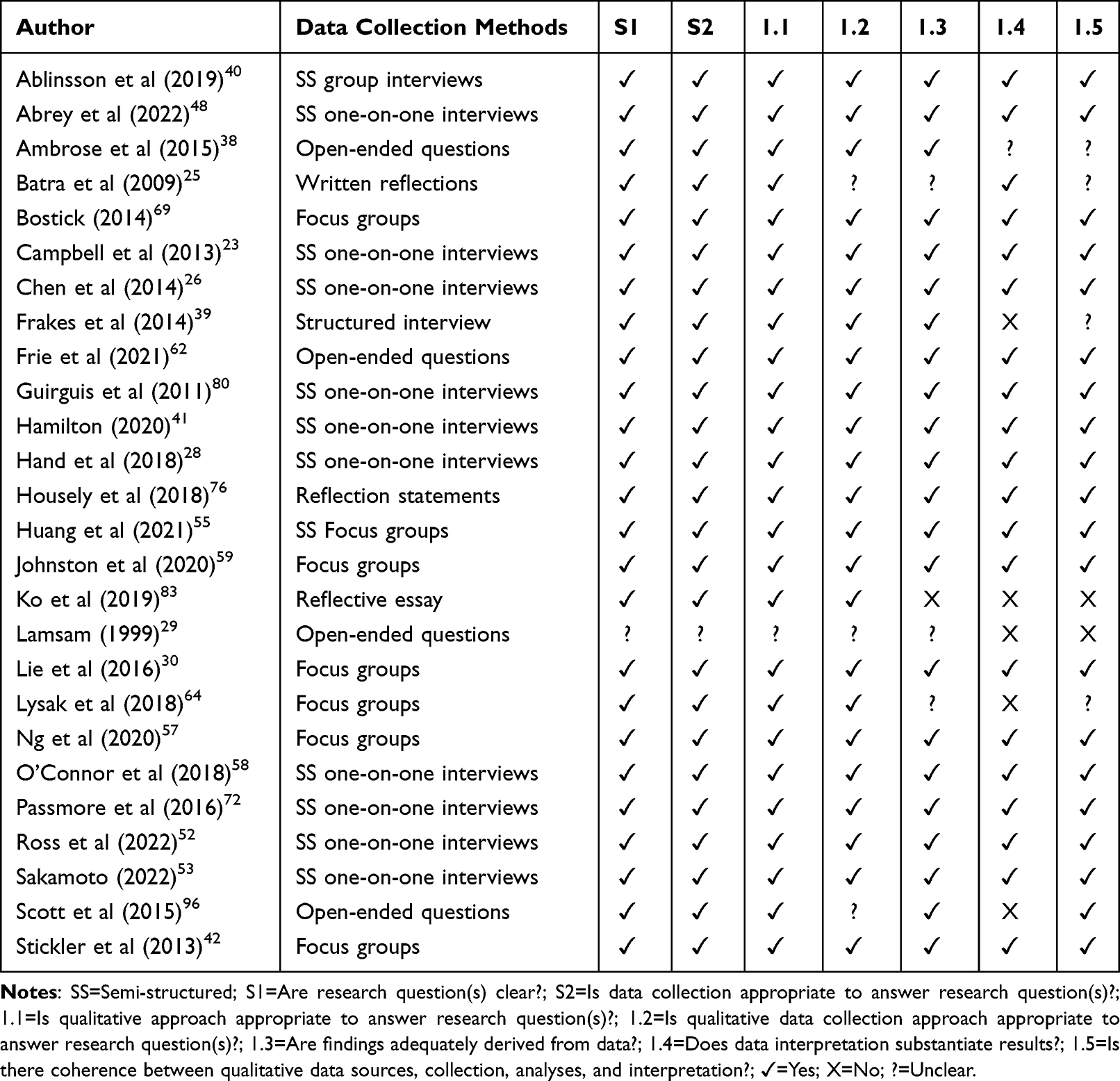 |
Table 2 Qualitative Study Appraisal |
Study Quality
The Mixed Methods Appraisal Tool is a critical appraisal tool/checklist intended to be used to assess the quality of studies included in systematic reviews combining qualitative, quantitative and mixed-methods studies. MMAT assessment showed that all but eight included studies had a clear research question and collected relevant data. The 26 located qualitative studies (Table 2) used a range of methodological approaches and analytical techniques in collecting data (10 involved semi-structured one-on-one interviews, 7 focus groups, 3 reflections, 4 open-ended survey questions and 2 structured interviews). Most qualitative studies (n = 22) adequately derived findings from the qualitative data collected, but six did not adequately substantiate results with data interpretation.
There were 39 quantitative studies, of which almost all collected data via survey (n = 34), less often used quantitative methods included reviewing academic records (n = 5) or analyses of medical files (n = 1). Twenty quantitative studies may be characterised as descriptive, whereby data related to student outcomes was measured only within one group. Most such studies (n = 12) lacked one or more MMAT methodological quality criteria for these types of study (Table 3). A further 19 quantitative studies were non-randomised studies, where outcomes in a student cohort participating in SRCs were compared to a non-participating comparator group. When assessed against criteria outlined in the MMAT, non-randomized studies generally used appropriate measurements (n = 12), had complete outcome data (n = 18), and delivered the intervention as intended (n = 19). However, clarity was lacking and several in particular did not account for confounders (factors that may account for both the learning outcomes observed and the relative likelihood of participating in voluntary SRCs).11–19 It seems apparent that students who participate in such clinics – even within the same program of study – are likely to have somewhat different characteristics from those who do not, and such studies should seek to account for these differences.
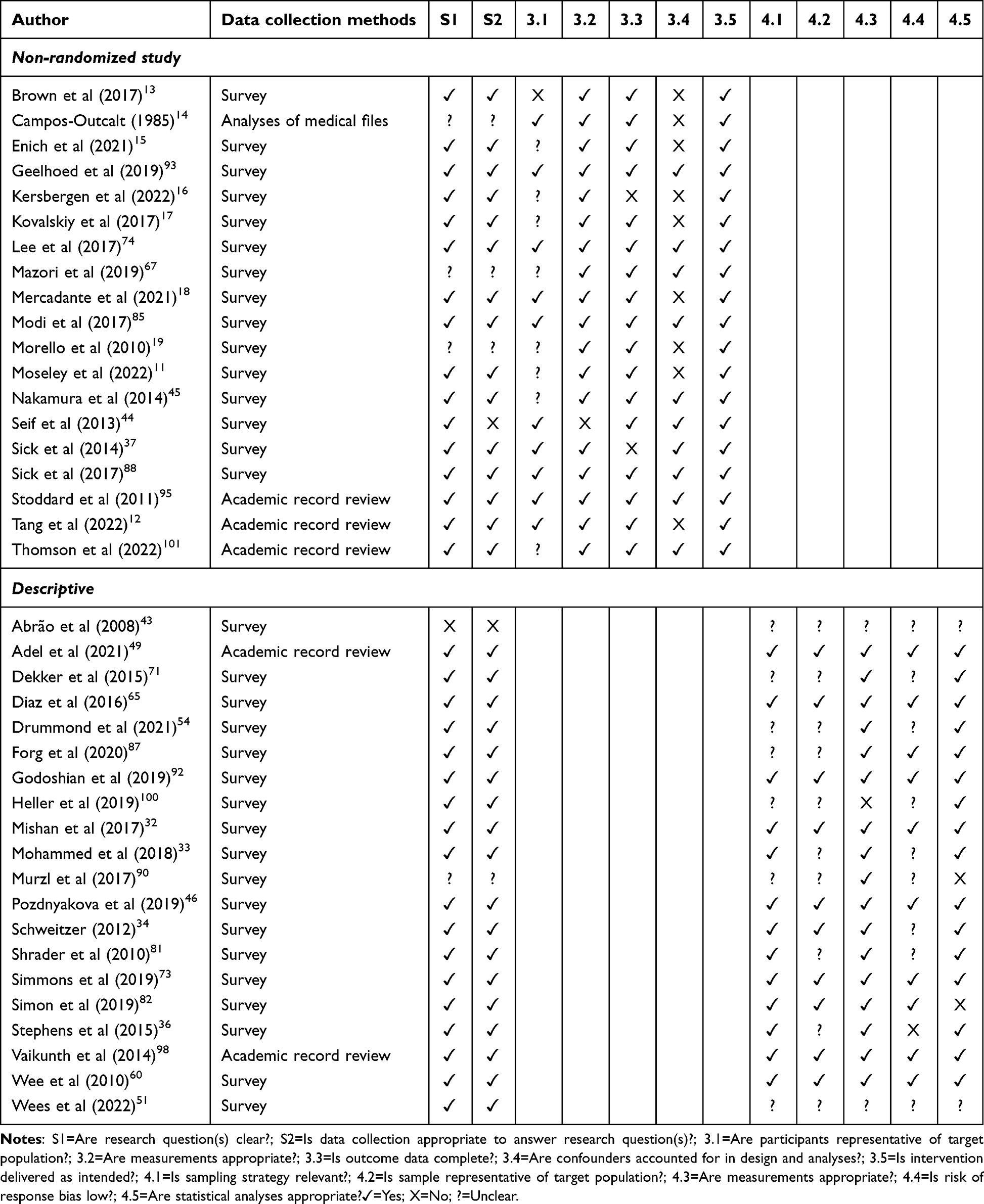 |
Table 3 Quantitative Study Appraisal |
Of the 27 mixed-methods studies (ie, those which adopted both quantitative and qualitative data collection methods) all collected quantitative data via survey, but there was greater variation in qualitative data collection, mostly open-ended survey questions (n = 17) but others via interviews (n = 6), focus groups (n = 3), or student reflections (n = 3). In terms of quality, most mixed-methods studies (n = 26) articulated a clear research question and adopted an appropriate approach to collect data, but just two provided a clear rationale for adopting a mixed-methods approach.20,21 Only one clearly demonstrated all mixed-methods MMAT quality criteria (Table 4).
 |
Table 4 Mixed Methods Study Appraisal |
Student Learning Outcomes
Clinical skills were the most common learning outcome reported to stem from participation in a SRC (n = 52), see Table 5. Participation provided the opportunity to practice, experience, and gain confidence applying clinical skills.11,22–59 Students improve interpersonal skills, including interpersonal communication skills,17,27–29,48,50,60–62 patient interaction relationship skills,19,40,42,43,63,64 team work,60 and experience and comfort managing language barriers (eg, interacting with patients for whom English is not their first language).65–67 Professionalism, including professional skills and competency,29,31,68–70 and autonomy/responsibility (including professional responsibility) are developed too.22,40,42,59,68,71 Other arguably clinically relevant learning outcomes included awareness of personal strengths and weaknesses,42 and the importance of self-advocacy.30
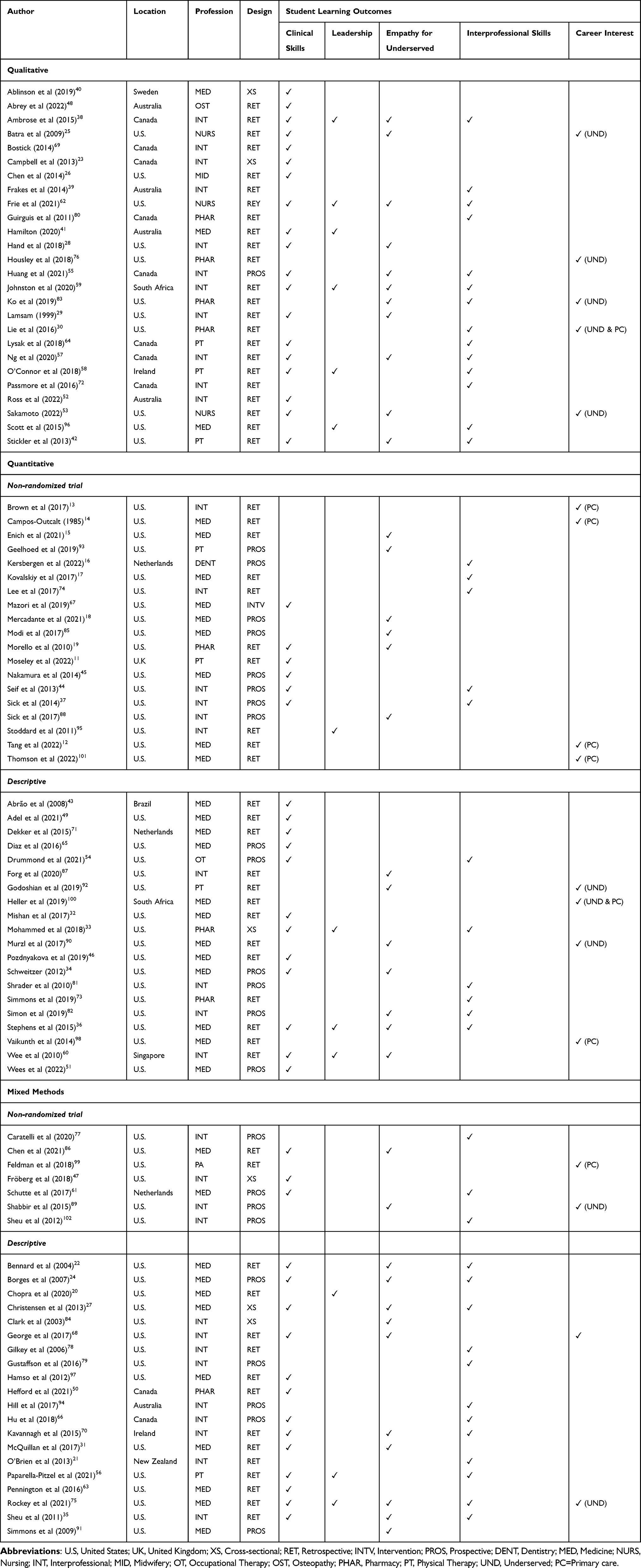 |
Table 5 Study Characteristics and Student Learning Outcomes |
The next most common reported learning outcome pertained to interprofessional skills (n = 40),27,36,37,39,44,56 including experience working in an interprofessional/interdisciplinary environment/team,17,33,35,36,59,64,66,70,72–75 teamwork and interprofessional communication,16,21,41,42,61,76–79 and improved understanding and appreciation of interprofessional roles.21,30,55,79–83 Greater confidence collaborating with community organisations was also reported as a learning outcome in one study.22 Although most relevant studies found SRC participation was associated with improved interprofessional skills, it should be noted that a number17,35,78,82 found more limited or qualified impacts in this area.
The third most frequently reported learning outcome associated with SRC participation revolved around empathy/compassion for underserved individuals (n = 34),15,18,25,27–29,42,53,55,57,59,62,75,83–87 in particular improving attitudes towards,15,18,25,28,34,88 as well as awareness and understanding and of the needs and social reality of, the underserved.19,22,29,31,35,36,55,57,59,60,62,66,68,70,75,76,82,84,86,89–92 Though one study reported no change in overall attitudes towards homeless patients.93 Finally, improved skills working with indigenous populations were noted as a learning outcome in one study.94
Leadership was another commonly reported outcome (n = 15). In particular, SRC participation was consistently found to benefit student’s capacity to lead, including gaining leadership experience and developing leadership skills,30,33,41,58,60,62,75,95,96 as well as experience and confidence teaching other students (ie, peer teaching).20,36,56,59,97
Multiple studies reported on the association between SRC participation and student’s future career interests and choices. Though some studies reported that involvement in an SRC did not influence the setting of students’ future job pursuits (n = 3),13,24,98 others reported SRC participation appeared to be linked with desire to and actual pursuit of a career in primary care (n = 6).12,14,30,99–101 SRC participation was also associated in some studies with increased student desire/commitment/interest to work with underserved communities (n = 12).25,30,50,53,75,83,89,90,92,96,100,102
Discussion
Our review suggests that SRC participation has the potential to facilitate achievement of various student learning outcomes. As detailed in our narrative analysis of the literature, SRC participation was linked with improved clinical skills, interprofessional skills, empathy and compassion for underserved patients, and leadership experience. A strength of our review is the broad focus on the potential learning benefits of SRC participation, regardless of the students’ field of study, and critical evaluation of the study methods which extend preceding reviews that had far narrower scope and less rigorous critical appraisal.3,4 In addition to providing insight into the potential benefits students may obtain from participation, our findings offer insight into the quality of the research to date, as well as practical implications for those seeking to implement and/or evaluate SRCs.
As mentioned, heterogeneity complicated comparisons between studies and further synthesis of the literature. The main takeaways from the appraisal of studies using the MMAT are that there is room for improvement in the design of studies examining student learning outcomes, and that researchers should take care to report in full how they collected, analyzed, and reported any data they collected. With respect to the qualitative literature, an array of methodological approaches and analytical techniques were employed but the major weakness of the qualitative literature was that almost a third of studies did not adequately substantiate results with data interpretation. Quantitative studies were a mixture of descriptive and non-randomised controlled study designs, with nearly all collecting data via surveys. Non-randomised controlled studies were of high quality with few exceptions, whereas clarity regarding one or more MMAT quality criteria was missing for half of descriptive studies. Like qualitative and quantitative studies, mixed-methods studies, for the most part, collected qualitative data using a range of methods and quantitative data using surveys. While most communicated a clear research question, clear rationales for adopting a mixed-methods approach were rare, and most study designs had weaknesses.
Recommendations for future SRC learning outcome evaluation stem from the limitations identified during critical appraisal and synthesis. A lack of detail on the operations of SRCs hampers the ability of readers to determine relevance to their interests, as well as compare studies. Clearly detailing the operation hours, client-base, locale, etc. of SRCs would prove beneficial in future. Similarly, detailed descriptions of interventions (duration, frequency, activity, intensity, etc.) would be of benefit. In some cases, interventions seemed too limited in time and structure to have impacted student outcomes, sometimes as short as a single volunteering shift.93 Moreover, many SRCs serve the needs of underserved communities (uninsured, homeless, elderly, etc.), which may limit their exposure to different standards of care.
Though students will experience natural growth as a part of their wider education, beyond what they may learn in an SRC, future quantitative evaluations should examine the impact of SRCs on learning outcomes prospectively rather than retrospectively, as has been done in most studies to date despite the potential for recall bias. Moreover, prospective (longitudinal) research that accounts for confounders (age, gender, ethnicity, socio-economic status, etc.) and allows for examination of temporal changes in valid outcome variables would provide a more robust understanding of the potential impact of SRC participation on learning outcomes. Especially if changes in outcomes can be compared to peers not involved in an SRC. When it comes to analyses, paired analyses, as opposed to merely reporting descriptive statistics. Also, when data allow, confounders (gender, age, level of study (eg, undergraduate vs postgraduate), profession (in interprofessional contexts) and hours spent involved in clinics) should be accounted for in analyses too, or at the very least measured and reported to characterise the sample.
While not necessarily a recommendation for improving future SRC evaluations per se, examining the impact on non-medical (ie, nursing, midwifery, and allied health, etc.) students would provide insight into the generalizability of student SRC learning benefits. Along similar lines, evaluation of SRCs in countries with public, or state-funded/subsidised, health-care systems would also determine the extent to which existing findings are generalizable to different contexts.
While some of the evidence is mixed, findings suggest that SRCs may benefit learning by providing participating students with experiences not usually available during training. These include opportunities to observe, practice, and develop competency performing various clinical skills, and interaction with other health-care professionals, particularly outside of their own profession, to develop interprofessional skills. Providing students with the chance to care for a diverse range of patients may also help to develop their social consciousness and capacity to understand and empathize with patients. Finally, experience in leadership roles and practicing their health profession in a variety of settings and circumstances can allow students to develop leadership skills and to make informed decisions regarding their future career paths.
Conclusion
SRCs participation can provide students with the opportunity to develop clinical skills, foster leadership, and cultivate empathy. Evidence concerning the impact of SRC participation on student’s interprofessional skills and future career choices is promising, but requires further investigation. There is a need for clear and specific research questions and aims, as well as more purposeful data collection and analyses. Further research across professions and in settings outside of the U.S. is needed given differences in education and health-care systems, and population and disease characteristics.
Acknowledgments
The authors would like to thank Librarian Dr. Christina Wissinger from Pennsylvania State University for assisting with the development of the search strategy, and [names blinded] for their assistance screening titles and abstracts.
Disclosure
Professor Patrea Andersen reports grants from Trust Waikato, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Nagel DA, Naccarato TT, Philip MT., et al. Understanding student-run health initiatives in the context of community-based services: a concept analysis and proposed definitions. Journal of Primary Care & Community Health. 2022;13:215013192211262. doi:10.1177/21501319221126293
2. Nguemeni Tiako MJ, Johnson SF, Nkinsi NT, Landry A. Normalizing service learning in medical education to sustain medical student-led initiatives. Acad Med. 2021;96(12):1634–1637. doi:10.1097/acm.0000000000004432
3. Briggs L, Fronek P. Student experiences and perceptions of participation in student-led health clinics: a systematic review. J Soc Work Educ. 2020;56(2):238–259. doi:10.1080/10437797.2019.1656575
4. Kent F, Keating JL. Interprofessional education in primary health care for entry level students--A systematic literature review. Nurse Educ Today. 2015;35(12):1221–1231. doi:10.1016/j.nedt.2015.05.005
5. Hopkins S, Bacon R, Flynn A. Student outcomes for interprofessional education in student led clinics: a rapid review. J Interprof Care. 2021;1–11. doi:10.1080/13561820.2020.1858767
6. Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
7. Rathbone J, Carter M, Hoffmann T, Glasziou P. Better duplicate detection for systematic reviewers: evaluation of Systematic Review Assistant-Deduplication Module. Syst Rev. 2015;4(1):6. doi:10.1186/2046-4053-4-6
8. Clarivate. EndNote; 2019. Available from: https://www.endnote.com/.
9. Podstawski R, Choszcz D, Klimczak J, Kolankowska E, Żurek P. Habits and attitudes of first-year female students at Warmia and Mazury university: a call for implementing health education programme at universities. Cent Eur J Public Health. 2014;22(4):229–238. doi:10.21101/cejph.a3975
10. Hong QN, Pluye P, Fàbregues S, et al. Mixed Methods Appraisal Tool (MMAT). Canadian Intellectual Property Office, Industry Canada; 2018.
11. Moseley J, Hellawell M, Graham C, Briggs A. Evaluation of a large group supervision model in a university student-led physiotherapy clinic. Br J Health Care Manag. 2022;28(3):61–67. doi:10.12968/bjhc.2021.0098
12. Tang C, Win G, Unangst S, et al. A retrospective study on the influence of participation at a student-run free clinic on medical specialty choice. J Student-Run Clin. 2022;8(1):548.
13. Brown A, Ismail R, Gookin G, Hernandez C, Logan G, Pasarica M. The effect of medical student volunteering in a student-run clinic on specialty choice for residency. Cureus. 2017;9(1):e967. doi:10.7759/cureus.967
14. Campos-Outcalt DE. Specialties chosen by medical students who participated in a student-run, community-based free clinic. Am J Prev Med. 1985;1(4):50–51.
15. Enich M, Hawes M, Lavadera P, Lin KW-R. Impact of student-run free clinic participation on medical student attitudes towards the underserved: a mixed-methods approach. J Student-Run Clin. 2021;7:1.
16. Kersbergen M, Creugers N, Kuijer-Siebelink W, et al. Interprofessional learning in a student-run dental clinic: the effect on attitudes of students in oral healthcare. J Interprof Care. 2022:1–8. doi:10.1080/13561820.2022.2070141
17. Kovalskiy A, Ismail R, Tran K, Desai A, Imran A, Hernandez C. Evaluating student attitudes: perceptions of interprofessional experiences following participation in a student-run free clinic. Cureus. 2017;9(2):e1053. doi:10.7759/cureus.1053
18. Mercadante SF, Goldberg LA, Divakaruni VL, Erwin R, Savoy M, O’Gurek D. Impact of student-run clinics on students’ attitudes toward people experiencing homelessness. PRiMER. 2021;5. doi:10.22454/PRiMER.2021.489756
19. Morello CM, Singh RF, Chen KJ, Best BM. Enhancing an introductory pharmacy practice experience at free medical clinics. Int J Pharm Pract. 2010;18(1):51–57. doi:10.1211/ijpp.18.01.0009
20. Chopra N, Zhou DB, Fallar R, Chadha N. Impact of near-peer education in a student-run free ophthalmology clinic on medical student teaching skills. J Surg Educ. 2020. doi:10.1016/j.jsurg.2020.05.012
21. O’Brien D, McCallin A, Bassett S. Student perceptions of an interprofessional clinical experience at a university clinic. NZ J Physiother. 2013;41(3):54.
22. Bennard B, Wilson JL, Ferguson KP, Sliger C. A student-run outreach clinic for rural communities in Appalachia. Acad Med. 2004;79(7):666–671. doi:10.1097/00001888-200407000-00010
23. Campbell DJ, Gibson K, O’Neill BG, Thurston WE. The role of a student-run clinic in providing primary care for Calgary’s homeless populations: a qualitative study. BMC Health Serv Res. 2013;13:277. doi:10.1186/1472-6963-13-277
24. Borges NJ, Hartung PJ. Service learning in medical education: project description and evaluation. Int J Learn High Educ. 2007;19(1):1.
25. Batra P, Chertok JS, Fisher CE, Manseau MW, Manuelli VN, Spears J. The Columbia-Harlem homeless medical partnership: a new model for learning in the service of those in medical need. J Urban Health. 2009;86(5):781–790. doi:10.1007/s11524-009-9386
26. Chen HC, Sheu L, O’Sullivan P, Ten Cate O, Teherani A. Legitimate workplace roles and activities for early learners. Med Educ. 2014;48(2):136–145. doi:10.1111/medu.12316
27. Christensen D, Belgard A, Craig C, Stephens M. Interest and perceptions of student-run health clinics: a survey at the Uniformed Services University of the Health Sciences. Mil Med. 2013;178(11):1245–1249. doi:10.7205/MILMED-D-13-00203
28. Hand J, Koransky A, Feinman J, et al. Alumni perspectives on the role of medical school service learning experiences in their professional development and practice. J Health Care Poor Underserved. 2018;29(4):1386–1399. doi:10.1353/hpu.2018.0102
29. Lamsam GD. Development of a service-learning program. Am J Pharm Educ. 1999;63(1):41–45.
30. Lie DA, Forest CP, Walsh A, Banzali Y, Lohenry K. What and how do students learn in an interprofessional student-run clinic? An educational framework for team-based care. Med Educ Online. 2016;21:31900. doi:10.3402/meo.v21.31900
31. McQuillan T, Wilcox-Fogel N, Kraus E, Ladd A, Fredericson M. Integrating musculoskeletal education and patient care at medical student-run free clinics. Pm&r. 2017;9(11):1117–1121. doi:10.1016/j.pmrj.2017.03.008
32. Mishan LI, Dragatsi D. Student-run clinics: a novel approach to integrated care, teaching and recruitment. Community Ment Health J. 2017;53(4):460–463. doi:10.1007/s10597-017-0081-3
33. Mohammed D, Turner K, Funk K. Pharmacy student involvement in student-run free clinics in the United States. Curr Pharm Teach Learn. 2018;10(1):41–46. doi:10.1016/j.cptl.2017.09.008
34. Schweitzer PJ, Rice TR. The student-run clinic: a new opportunity for psychiatric education. Acad Psychiatry. 2012;36(3):233–236. doi:10.1176/appi.ap.10110163
35. Sheu LC, Zheng P, Coelho AD, et al. Learning through service: student perceptions on volunteering at interprofessional hepatitis B student-run clinics. J Cancer Educ. 2011;26(2):228–233. doi:10.1007/s13187-010-0142-6
36. Stephens L, Bouvier N, Thomas D, Meah Y. Voluntary participation in a medical student-organized clinic for uninsured patients significantly augments the formal curriculum in teaching underrepresented core competencies. J Student-Run Clin. 2015;1(1):879.
37. Sick B, Sheldon L, Ajer K, Wang Q, Zhang L. The student-run free clinic: an ideal site to teach interprofessional education? J Interprof Care. 2014;28(5):413–418. doi:10.3109/13561820.2014.907779
38. Ambrose E, Baker D, Mahal I, MicFlikier A, Holmqvist M. Interprofessional experiences at a student-run clinic: who participates and what do they learn? J Res Interprof Pract Educ. 2015;5(2). doi:10.22230/jripe.2015v5n2a197
39. Frakes K-A, Brownie S, Davies L, Thomas J, Miller M, Tyack Z. Experiences from an interprofessional student-assisted chronic disease clinic. J Interprof Care. 2014;28(6):573–575. doi:10.3109/13561820.2014.917404
40. Albinsson G, Elmqvist C, Hörberg U. Nursing students’ and lecturers’ experiences of learning at a university-based nursing student–run health clinic. Reflective Pract. 2019;20(4):423–436. doi:10.1080/14623943.2019.1638242
41. Hamilton V, Baird K, Fenwick J. Nurturing autonomy in student midwives within a student led antenatal clinic. Women Birth. 2020;33(5):448–454. doi:10.1016/j.wombi.2019.12.001
42. Stickler L, Grapczynski C, Ritch J. Student perceptions of outcomes from participation in physical therapy pro bono clinics a qualitative study. J Allied Health. 2013;42(1):46–55.
43. Abrão MN, Bensi CG, Gonçalves MS, et al. A medical student-staffed outpatient oncology clinic: a 10-year Brazilian experience. J Cancer Educ. 2008;23(1):63–64. doi:10.1080/08858190701641321
44. Seif G, Coker-Bolt P, Kraft S, Gonsalves W, Simpson K, Johnson E. The development of clinical reasoning and interprofessional behaviors: service-learning at a student-run free clinic. J Interprof Care. 2014;28(6):559–564. doi:10.3109/13561820.2014.921899
45. Nakamura M, Altshuler D, Binienda J. Clinical skills development in student-run free clinic volunteers: a multi-trait, multi-measure study. BMC Med Educ. 2014;14:250. doi:10.1186/s12909-014-0250-9
46. Pozdnyakova A, Andersen M, Cruz S, Wilson H, Pakvasa M, Oyler J. Assessing quality of diabetes care and medical student volunteer knowledge of diabetes care at the University of Chicago Community Health Clinic. Am J Med Qual. 2019;34(6):621. doi:10.1177/1062860619845629
47. Fröberg M, Leanderson C, Fläckman B, et al. Experiences of a student-run clinic in primary care: a mixed-method study with students, patients and supervisors. Scand J Prim Health Care. 2018;36(1):36–46. doi:10.1080/02813432.2018.1426143
48. Abrey C, De Silva N, Godwin J, et al. Does the student-led osteopathy clinical learning environment prepare students for practice? BMC Med Educ. 2022;22(1):603. doi:10.1186/s12909-022-03658-3
49. Adel FW, Berggren RE, Esterl RM, Ratelle JT. Student-run free clinic volunteers: who they are and what we can learn from them. BMC Med Educ. 2021;21(1):356. doi:10.1186/s12909-021-02793-7
50. Hefford H, Kapanen AI, Medgyesi N, Yuen J. Learner perceptions of a video recording activity for patient consultation training in pharmacist-led primary care clinic located in an academic institution. Innov Pharm. 2021;12:3. doi:10.24926/iip.v12i3.3632
51. Wees I, Murtuza MI, Mathisen D, et al. Improving the care of patients with COVID-19 with a medical student-run telemedicine clinic. BMJ Open Qual. 2022;11(1):e001646. doi:10.1136/bmjoq-2021-001646
52. Ross MH, Whitehead A, Jeffery L, Hartley N, Russell T. Supervising students during a global pandemic: clinical educators’ perceptions of a student-led telerehabilitation service during COVID-19. Int J Telerehabilitation. 2022;14:1. doi:10.5195/ijt.2022.6464
53. Sakamoto RR. Influence of “RAP” experiences on nursing students’ career choices in aging: a qualitative exploration. Nurse Educ Today. 2022;109:105218. doi:10.1016/j.nedt.2021.105218
54. Drummond R, Koziol C, Yeats H, Tyminski Q. Occupational therapy student-run free clinic: mutual benefits in expanded homeless and health services and clinical skills development. J Student-Run Clin. 2021;7(1):32.
55. Huang K, Maleki M, Regehr G, McEwen H. Examining the educational value of student-run clinics for health care students. Acad Med. 2021;96(7):1021–1025. doi:10.1097/acm.0000000000003922
56. Paparella-Pitzel S, Anderson EZ, Rothpletz-Puglia P, Parrott JS. Exploring physical therapy students’ experience of peer learning in a student-run clinic. J Educ Health Promot. 2021;10:400. doi:10.4103/jehp.jehp_188_21
57. Ng E, Hu T, McNaughton N, Martimianakis MA. Transformative learning in an interprofessional student-run clinic: a qualitative study. J Interprof Care. 2021;35(5):701–709. doi:10.1080/13561820.2020.1807480
58. O’Connor A, Liston E, O’Donnell M. Student-led community placement in physiotherapy. Clin Teach. 2019;16(6):593–597. doi:10.1111/tct.12988
59. Johnston D, McInerney P, Moch S. Learning experiences of medical and pharmacy students at a student-run clinic in South Africa and the development of a framework for learning. Educ Health. 2020;33(3):87–94. doi:10.4103/efh.EfH_281_18
60. Wee LE, Yeo WX, Tay CM, Lee JJM, Koh GCH. The pedagogical value of a student-run community-based experiential learning project: the Yong Loo Lin School of Medicine Public Health Screening. Ann Acad Med. 2010;39(9):686.
61. Schutte T, Tichelaar J, Dekker RS, et al. Motivation and competence of participants in a learner-centered student-run clinic: an exploratory pilot study. BMC Med Educ. 2017;17(1):1–13. doi:10.1186/s12909-017-0856-9
62. Frie KJ, Timm JR, Koehler AB. Interprofessional student perceptions of planning and implementing a student-led, faculty-guided rural health clinic. Online J Rural Nurs Health Care. 2021;21(2):117–151.
63. Pennington K, Tong IL, Lai CJ, O’Sullivan PS, Sheu L. The value of student-run clinics for premedical students: a multi-institutional study. J Health Care Poor Underserved. 2016;27(3):961–970. doi:10.1353/hpu.2016.0132
64. Lysak K, Berenbaum SL, Landry EJ, et al. Student perceptions of an experiential education clinic within a pharmacy school. Curr Pharm Teach Learn. 2018;10:1636–1640. doi:10.1016/j.cptl.2018.09.001
65. Diaz JE, Ekasumara N, Menon NR, et al. Interpreter training for medical students: pilot implementation and assessment in a student-run clinic. BMC Med Educ. 2016;16(1):256. doi:10.1186/s12909-016-0760-8
66. Hu T, Cox KA, Nyhof-Young J. Investigating student perceptions at an interprofessional student-run free clinic serving marginalised populations. J Interprof Care. 2018;32(1):75–79. doi:10.1080/13561820.2017.1363724
67. Mazori AY, Maron MI, Osterbur MLB, et al. Enhancing medical student-interpreter collaboration in an urban free clinic. Fam Med. 2019;51(7):593–597. doi:10.22454/FamMed.2019.229662
68. George L, Bemenderfer S, Cappel M, et al. A model for providing free patient care and integrating student learning and professional development in an interprofessional student-led clinic. J Phys Ther Educ. 2017;31(2):54–66.
69. Bostick G, Hall M, Miciak M. Novel clinical learning from a student‐led clinic. Clin Teach. 2014;11(7):512–515. doi:10.1111/tct.12214
70. Kavannagh J, Kearns A, McGarry T. The benefits and challenges of student-led clinics within an Irish context. J Pract Teach Learn. 2014;13(2–3):58–72. doi:10.1921/jpts.v13i2-3.858
71. Dekker RS, Schutte T, Tichelaar J, et al. A novel approach to teaching pharmacotherapeutics--feasibility of the learner-centered student-run clinic. Eur J Clin Pharmacol. 2015;71(11):1381–1387. doi:10.1007/s00228-015-1916
72. Passmore A, Persic C, Countryman D, et al. Student and preceptor experiences at an inter-professional student-run clinic: a physical therapy perspective. Physiother Can. 2016;68(4):391–397. doi:10.3138/ptc.2015-87E
73. Simmons K, Klein M, Stevens C, Jacobson T. Implementation of a student pharmacist-run diabetes education and management clinic in a federally qualified health center in Texas. Curr Pharm Teach Learn. 2019;11(8):849–852. doi:10.1016/j.cptl.2019.04.015
74. Lee S, Valtis YK, Jun T, et al. Measuring and improving student engagement in clinical training. Educ Prim Care. 2017;29(1):22–26. doi:10.1080/14739879.2017.1398597
75. Rockey NG, Weiskittel TM, Linder KE, Ridgeway JL, Wieland ML. A mixed methods study to evaluate the impact of a student-run clinic on undergraduate medical education. BMC Med Educ. 2021;21(1):182. doi:10.1186/s12909-021-02621-y
76. Housley CL, Neill KK, White LS, Tedder AT, Castleberry AN. An evaluation of an interprofessional practice-based learning environment using student reflections. J Interprof Care. 2018;32(1):108–110. doi:10.1080/13561820.2017.1356808
77. Caratelli LA, Bostwick JR, Templin T, Fitzgerald M, Filter MS, Ginier E. Development and evaluation of an interprofessional seminar pilot course to enhance collaboration between health professions at a student-run clinic for underserved populations. J Interprof Care. 2020;34(3):422–426. doi:10.1080/13561820.2019.1676208
78. Gilkey MB, Earp JA. Effective interdisciplinary training: lessons from the University of North Carolina’s student health action coalition. Acad Med. 2006;81(8):749–758. doi:10.1097/00001888-200608000-00014
79. Gustafsson L, Hutchinson L, Theodoros D, et al. Healthcare students’ experiences of an interprofessional, student-led neuro-rehabilitation community-based clinic. J Interprof Care. 2016;30(2):259–261. doi:10.3109/13561820.2015.1086730
80. Guirguis L, Sidhu K. An exploration of pharmacist preceptors’ and pharmacy students’ experiences at an interprofessional student-run clinic. Can Pharm J. 2011;144(4):179–185. doi:10.3821/1913-701X-144.4.179
81. Shrader S, Thompson A, Gonsalves W. Assessing student attitudes as a result of participating in an interprofessional healthcare elective associated with a student-run free clinic. J Res Interprof Pract Educ. 2010;1(3):98.
82. Simon L, Beckmann D, Reidy P, Cohen M, Tobey M. Evaluation of an interprofessional student-faculty collaborative clinic in a jail. J Correct Health Care. 2019;25(4):362–372. doi:10.1177/1078345819880901
83. Ko J, Connor S, Jonkman L, Abraham O. Student pharmacists’ perspectives on service-learning experiences in free clinics. Am J Pharm Educ. 2019;83(9). doi:10.5688/ajpe7379
84. Clark DL, Melillo A, Wallace D, Pierrel S, Buck DS. A multidisciplinary, learner-centered, student-run clinic for the homeless. Fam Med. 2003;35(6):394–397.
85. Modi A, Fascelli M, Daitch Z, Hojat M. Evaluating the relationship between participation in student-run free clinics and changes in empathy in medical students. J Prim Care Community Health. 2017;8(3):122–126. doi:10.1177/2150131916685199
86. Chen G, Kazmi M, Chen D, Phillips J. Improving medical student clinical knowledge and skills through influenza education. Med Sci Educ. 2021;31(5):1645–1651. doi:10.1007/s40670-021-01355-2
87. Forg RE, Paun O. Assessing needs of student volunteers related to providing care to a homeless population. J Prof Nurs. 2021;37(1):73–79. doi:10.1016/j.profnurs.2020.10.008
88. Sick B, Zhang L, Weber-Main AM. Changes in health professional students’ attitudes toward the underserved: impact of extended participation in an interprofessional student-run free clinic. J Allied Health. 2017;46(4):213–219.
89. Shabbir SH, Santos MTM. The role of prehealth student volunteers at a student-run free clinic in New York, United States. J Educ Eval Health Prof. 2015;12. doi:10.3352/jeehp.2015.12.49
90. Murzl CA, Durns TA, Mowrey LT, Tubbs AS, Boeve SA. A medical student-run child and adolescent psychiatry clinic: one institution’s experience. Acad Psychiatry. 2017;41(5):582–586. doi:10.1007/s40596-017-0753
91. Simmons BB, DeJoseph D, Diamond J, Weinstein L. Students who participate in a student-run free health clinic need education about access to care issues. J Health Care Poor Underserved. 2009;20(4):964–968. doi:10.1353/hpu.0.0225
92. Godoshian MR, Yorke A. Does participation in physical therapy student-run free clinics relate to altruism, social responsibility, and cultural competency post-graduation? A pilot study. J Student-Run Clin. 2019;5(1):87.
93. Geelhoed MA, Callaway SM, Cruz JM, Subramanian SK. Attitudes of physical therapy students toward the population currently experiencing homelessness: a pilot study. J Allied Health. 2019;48(3):220–225.
94. Hill AE, Nelson A, Copley J, Quinlan T, White R. Development of student clinics in Indigenous contexts: what works? J Clin Pract Speech Lang Path. 2017;19(1):40–45.
95. Stoddard HA, Risma JM. Relationship of participation in an optional student-run clinic to medical school grades. Teach Learn Med. 2011;23(1):42–45. doi:10.1080/10401334.2011.536890
96. Scott EA, Swartz MK. Interprofessional student experiences on the HAVEN free clinic leadership board. J Interprof Care. 2015;29(1):68–70. doi:10.3109/13561820.2014.934339
97. Hamso M, Ramsdell A, Balmer D, Boquin C. Medical students as teachers at CoSMO, Columbia University’s student-run clinic: a pilot study and literature review. Med Teach. 2012;34(3):e189–e197. doi:10.3109/0142159X.2012.642832
98. Vaikunth SS, Cesari WA, Norwood KV, et al. Academic achievement and primary care specialty selection of volunteers at a student-run free clinic. Teach Learn Med. 2014;26(2):129–134. doi:10.1080/10401334.2014.883980
99. Feldman CT, Morici B, Goodrich S. Early exposure to underserved patients and its impact on initial employment decisions regarding physician assistants. J Physician Assist Educ. 2018;29(3):144–149. doi:10.1097/JPA.0000000000000213
100. Heller M, Thomas AM, Peters SM, Düsterwald KM, Klausner JD. An evaluation of patient and student experience at a longstanding student-run free clinic in Cape Town, South Africa. Cureus. 2019;11(12):e6320. doi:10.7759/cureus.6320
101. Thomson KB, Mirpuri P, Chen M. The impact of volunteering with a student-run free clinic on medical student specialty selection. BMC Med Educ. 2022;22(1):714. doi:10.1186/s12909-022-03788-8
102. Sheu L, Lai CJ, Coelho AD, et al. Impact of student-run clinics on preclinical sociocultural and interprofessional attitudes: a prospective cohort analysis. J Health Care Poor Underserved. 2012;23(3):1058–1072. doi:10.1353/hpu.2012.0101
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.