Back to Journals » Patient Preference and Adherence » Volume 16
Learned Helplessness in Renal Dialysis Patients: Concept Analysis with an Evolutionary Approach
Received 2 May 2022
Accepted for publication 17 August 2022
Published 24 August 2022 Volume 2022:16 Pages 2301—2312
DOI https://doi.org/10.2147/PPA.S373134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Chunyan Xie,1,2 Li Li,1– 3 Yamin Li1
1Clinical Nursing Teaching and Research Section, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 2XiangYa Nursing School, Central South University, Changsha, Hunan, 410013, People’s Republic of China; 3The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, 830011, People’s Republic of China
Correspondence: Yamin Li, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China, Email [email protected]
Background: Learned helplessness is an early psychological concept, but in the field of nursing, the concept of learned helplessness in renal dialysis patients and its unique challenges are not well understood.
Objective: This article provides a conceptual analysis of learned helplessness in renal dialysis patients to increase knowledge of this psychological phenomenon in the setting of renal nursing.
Design: Rodgers’ evolutionary concept analysis.
Methods: The literature published in five databases (PubMed, CINAHL, Embase, PsycINFO, CNKI) was searched using specific terms. In the first stage, search terms and strategies were used to narrow the relevant articles. In the second stage, the data were extracted from the included articles. In the third stage, the data were analyzed using thematic analysis, and the results were presented in the form of attributes, antecedents, consequences, surrogate terms, and related terms. We found additional instruments and interventions and presented a model case to emphasize the practicality of the concept. In the fourth phase, experts contributed to the discussion and interpretation of the findings.
Results: A total of 22 articles were included. Four attributes of learned helplessness in renal dialysis patients were identified: low self-concept, perceived loss, negative cognitive set, and abandonment of action. The antecedents were sociodemographic characteristics, disease and treatment, and psychological factors. Consequences were separated into four themes: psychological problems, physiological problems, quality of life, and health-related behavior. Surrogate terms are hopelessness and powerlessness, and the related term is depression.
Conclusion: The process of conceptual analysis in this study provides a means of identifying awareness gaps and practice challenges of learned helplessness in renal dialysis patients and other concepts. The findings can be used to guide the design of tools and interventions to expand the use of learned helplessness theory in nursing.
Keywords: concept analysis, learned helplessness, hemodialysis, hopelessness, powerlessness
Introduction
Healthy People 2010 includes psychological health as one of the ten leading health indicators,1 and learned helplessness is an essential concept in psychological health. Learned helplessness was first introduced in 1967 by Seligman based on his behavioral studies in animals2 and has been widely used in the field of pedagogy. Researchers have different views on the concept of learned helplessness. Huzian O3 considered learned helplessness cognitive and emotional helplessness induced by individuals in resource-poor situations. Bruns B4 considered it an acquired psychological state or behavior pattern of powerlessness or self-abandonment. Furthermore, Günsoy C5 defined learned helplessness as an avoidance pattern of inability to control stress, which is considered as a depression-like coping deficit. However, it is certain that learned helplessness is a negative emotion or action that arises when individuals are exposed to uncontrollable experiences for a long time. In 1990, Smith6 applied it to patients with rheumatoid arthritis and found that it was significantly associated with depression. Learned helplessness has been used in medical research in systemic lupus erythematosus, multiple sclerosis, type 1 diabetes, and Alzheimer’s. Many studies have reported that learned helplessness is a common psychological experience for most people with chronic illness.7,8 Patients who perceive disease as a negative event and feel powerless to change its consequences are more likely to experience learned helplessness.1
Chronic kidney disease (CKD) has high morbidity and mortality rates9,10 and has become a global public health problem because of its long treatment time, high cost, and poor prognosis.11 End-stage kidney disease (ESKD) indicates that a patient’s renal function is in irreversible deterioration. The patient must be kept alive by renal replacement therapy, in which renal dialysis is the main treatment route.12 Renal dialysis imposes many limitations on ESKD patients and results in a high incidence of psychological problems.13 For them, the diagnosis of ESKD and renal dialysis is a stressor. Due to the irreversibility of ESKD, although renal dialysis can replace partial kidney function, it cannot completely stop the deterioration of the disease, and the threat of complications and death always haunts the patients. Patients not only have to go to the hospital several times a week but also have to keep the supine position for four hours at a time. The routine and long-term treatment pattern will greatly affect the patients’ schoolwork, career, and personal development. Besides, the strict restrictions on diet and water make the patients feel out of control of their lives. Therefore, renal dialysis patients are prone to helplessness. Nurses face many challenges in providing care and health education to kidney dialysis patients. Understanding the concept of learned helplessness may enable them to provide better care and help patients cope effectively with their stress. Learned helplessness has been found to be associated with depression, suicidal ideation, and personal behavior in patients, whereby timely identification and intervention of their learned helplessness may be effective in preventing or delaying more serious outcomes.
However, the core concepts should be analyzed before any scientific research to be more sensitive to the use of the specific language of study field,14 thus guiding the development of theory and implementation of practical programs.15 This study is based on the scarcity of studies analyzing the concept of learned helplessness in renal dialysis patients. The approach chosen for the study is Rodgers’s evolutionary concept analysis, which is a strictly inductive approach suitable for the evolving concepts.16 He argued that dynamic concepts in different disciplines have different meanings. Learned helplessness in renal dialysis patients is a multifactorial concept that can change over time with conditions, so Rodgers’ approach is more appropriate for this study. This approach requires a systematic review based on the literature to identify attributes, antecedents, consequences, surrogate terms, and related terms of the concept. Table 1 shows the processes of evolutionary concept analysis.
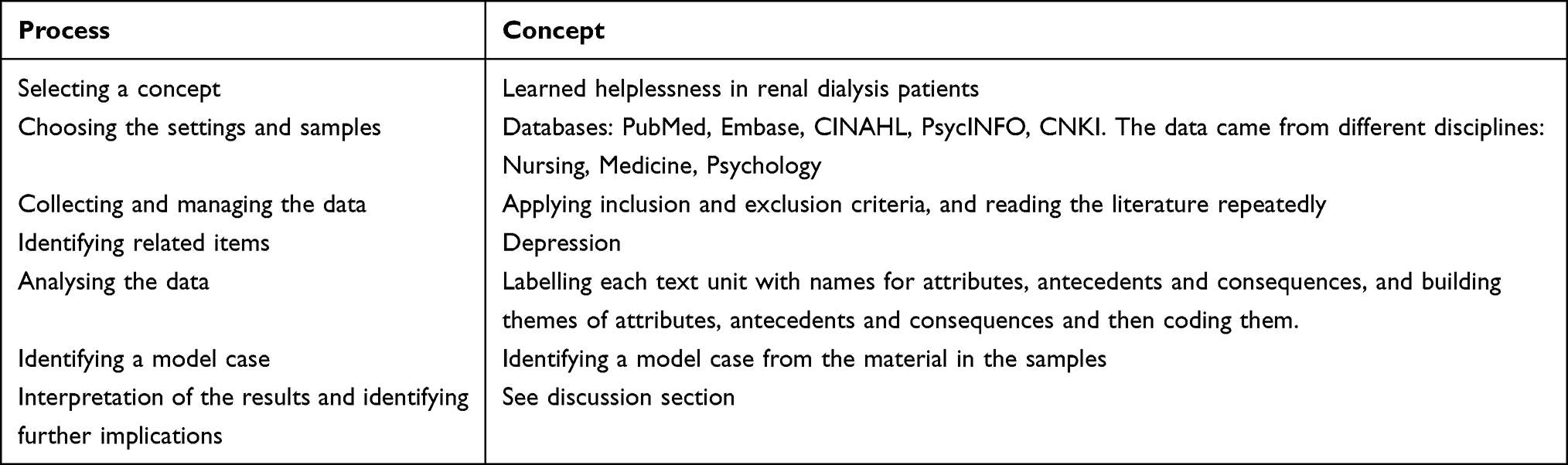 |
Table 1 The Processes of Evolutionary Concept Analysis |
Purpose
To clarify the concept of learned helplessness in renal dialysis patients and to identify its attributes, antecedents, and consequences in the context of the nursing discipline.
Methods
Based on Rodgers’ evolutionary concept analysis, we adapted four phases akin to Tofthagen and Fagerstrom (2010)17 in an iterative manner.
Phase 1: Search Terms, Search Strategy, and Study Selection
After focusing on a core concept, the most critical step is identifying the field and literature. According to Rodgers, concept analysis should begin with a literature search using keywords, titles, or abstracts that mention this concept. In our study, medicine, nursing, and psychology were the settings for data collection. We used a combination of the keywords and entry terms to search English and Chinese databases, including PubMed, Embase, CINAHL, PsycINFO, and CNKI, to retrieve articles published from the database’s inception until February 2022. We restricted the search terms to the title or abstract, and identified the keywords by reviewing the target articles and the author’s knowledge of the field. The keywords were “Helplessness, Learned” and “Renal Dialysis”. The search strategy using PubMed as an example is shown in the Appendix. The inclusion criteria were (i) available full text, (ii) related to the concept’s attributes, antecedents, consequences, surrogate terms, and related terms, and (iii) published in English or Chinese. Grey literature, texts published in nonpeer-reviewed journals, and letters to the editor were excluded.
Phase 2: Data Extraction and Analysis
At the end of data collection, all articles were reviewed, focusing on attributes, antecedents, consequences, surrogate terms, and related terms (see Table 2). Attributes refer to the characteristics of the concept, antecedents are the phenomena associated with the concept, and consequences are the results of the concept.17 Surrogate terms are the words sharing attributes with this concept, and related concepts are the terms having something in common with this concept.17
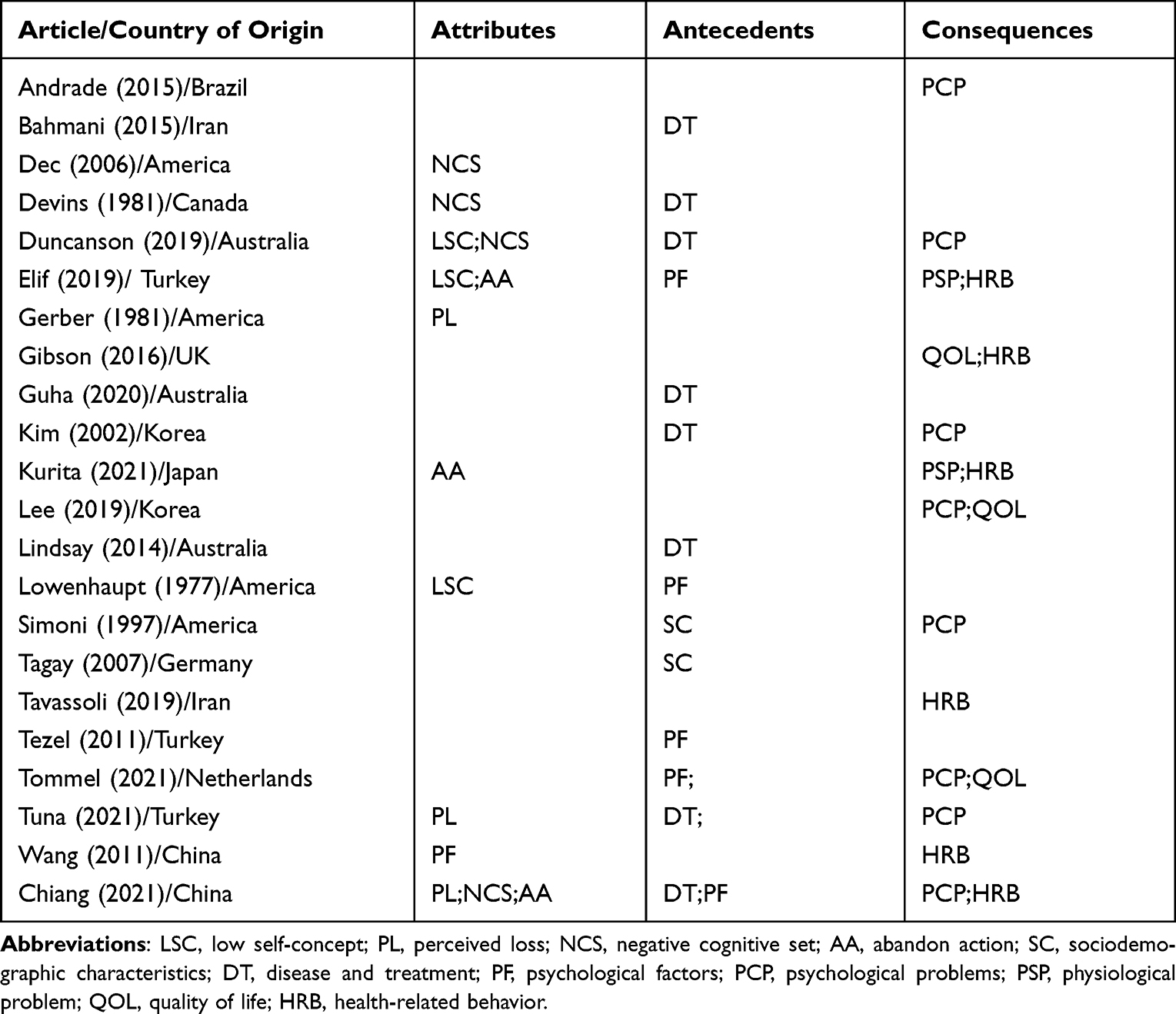 |
Table 2 Summary of Attributes, Antecedents, and Consequences of Learned Helplessness in Renal Dialysis Patients |
Phase 3: Thematic Analysis
Rodgers’ approach relies on thematic analysis, a process of identifying, organizing, describing, and reporting themes in the data.18 We performed multiple readings of selected literature to determine the meaning units in them that are related to the concepts and to assign these to relevant categories.
Phase 4: Experts’ Involvement
The thematic analyses’ results were presented and discussed with experts. We discussed how these themes contribute to our understanding of the concepts and can inform insights for future nursing practice.
Ethical Consideration
Since this conceptual analysis was based on a literature review, we did not apply for ethical approval. However, we still followed the Helsinki Declaration to ensure good practices during the research study.
Results
Search Results
A broad search yielded 100 citations. Various types of quantitative and qualitative studies were reviewed by two researchers independently. Articles that were duplicated, published in languages other than English or Chinese, and irrelevant to the subject matter were excluded. After reviewing the reference list, one additional article was added. Twenty-two articles were selected with high relevance for data extraction and thematic analysis (Figure 1).
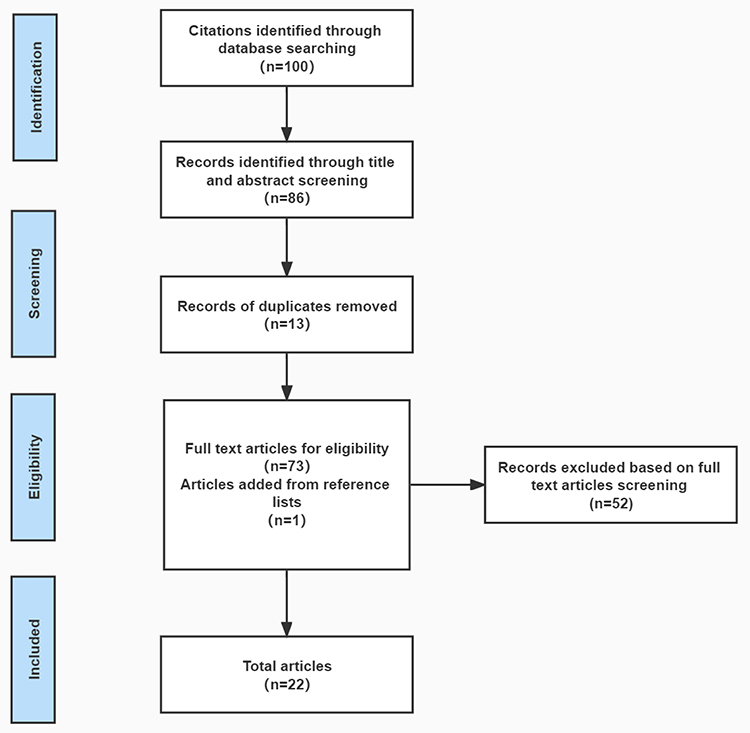 |
Figure 1 Flow diagram showing results of search strategy. |
Concept Uses
According to the Oxford, Merriam-Webster, and other free dictionaries, learned means developed by training or experience and does not exist at birth. Helplessness has two definitions: (i) a feeling of being unable to manage and (ii) powerlessness revealed by an inability to act. We determine the meaning of the concept of learned helplessness from the above combined results. Namely, it refers to a psychological state in which a feeling of losing control or powerlessness is experienced after learning it through negative events or failures.
In related studies, scholars tend to favor learned helplessness as a renal dialysis patient’s psychological phenomenon or an emotional state. In the sample obtained, only three authors gave a definition for it. Devins19 defined learned helplessness as the psychological state of an individual’s perceived loss of control over important life dimensions. Chiang et al20 considered learned helplessness as a negative, desperate emotion exhibited when a person has no choice or meets an unsolvable dilemma. Dec et al21 thought learned helplessness as a psychological phenomenon in which patients believe that the disease outcome is independent of their actions.
Development of Concepts
Learned helplessness is a psychological concept first introduced by Seligman in his animal behavior studies. He found that animals passively accept the current state and no longer actively change behavior after stimulation by external conditions for a long time. In 1978, Abramson further demonstrated that learned helplessness is equally prevalent in humans.22 Learned helplessness has been used to explain the triggers of abandonment behavior and depression and is now widely used in education, psychology, and management. In 1990, Smith6 extended this concept to patients with rheumatoid arthritis and demonstrated that learned helplessness correlated significantly with patients’ depression and disease prognosis. Learned helplessness has been gradually introduced into the medical field, including systemic lupus erythematosus, multiple sclerosis, type 1 diabetes, acute myocardial infarction, and chronic nephrosis. Helplessness has only been studied in patients with glaucoma and traumatic fractures in China.
Attributes
The key to concept analysis is to describe the concept’s attributes. Attributes are the sets of characteristics that establish the true definition of a concept and provide us with greater insight.23 Learned helplessness in renal dialysis patients is multidimensional, with four attributes identified.
Low Self-Concept
Self-concept refers to the beliefs that an individual has about themselves.24 The renal dialysis patients in learned helplessness tend to have a low self-concept and low self-esteem. Their consider themselves unattractive, accompanying the collapse of self-worth and a lack of appropriate self-perception and reasonable self-control.25–27
Perceived Loss
The renal dialysis patients with learned helplessness often mention that they have a sense of loss from all dimensions,20 including perceived loss of emotional relationships (especially intimate relationships with their lover and family), perceived loss of various resources, perceived loss of control, and perceived loss of interest and purpose.20,28,29
Negative Cognitive Set
The cognitive set is a state of readiness or behavioral tendencies for an activity.30 When renal dialysis patients experience a blow of disease or a failure in self-management, if they are accustomed to attributing these to fate or deficiencies in self-efficacy, they will develop the cognitive set that no external factors or person can change the results and tend to fall into a continuous state of helplessness.19–21,27
Abandon Action
The renal dialysis patients with learned helplessness exhibit varying degrees of abandon action, as reflected in stopping health-related behaviors, stopping help-seeking, negative coping, negative acceptance, and avoidance. Once patients identify themselves as a failure and believe that they will not change the outcome of renal failure no matter how hard they try, they will treat therapy and self-management tasks with an abandon action to avoid the next failure.20,25,31
Antecedents
Antecedents are the events or phenomena that should exist before the focus concept arises.23 In summary, antecedents of learned helplessness in renal dialysis patients include sociodemographic characteristics, disease and treatment, and psychological factors.
Sociodemographic Characteristics
Existing studies have mainly reported the effect of gender and native language background variability on renal dialysis patients’ learned helplessness. For example, Tagay32 reported that helplessness was more pronounced in female renal dialysis patients than in males, and female renal dialysis patients tended to have more life-threatening feelings than males. Simoni et al33 found that nonnative English speakers reported more feelings of helplessness among renal dialysis children in America.
Disease and Treatment
The impact of disease and treatment factors on learned helplessness in renal dialysis patients includes ESKD characteristics, treatment modality, comorbidity, physiological function, blood test results, and the experience of disease-related events. The severity, irreversibility, and long-term intensive treatment of ESKD are psychological stressors for patients.34 Although renal dialysis can replace part of kidney function, it does not entirely stop the deterioration of the disease, and life-threatening feelings always affect patients, which leads to emotional problems such as helplessness and depression.35 The strict restrictions on diet and water make patients feel out of control about their future life, making them prone to persistent helplessness.27 Renal dialysis has greatly restricted patients’ education, career, and life, and the accompanying role changes often leave them isolated and helpless.29,36 In addition, their poor health conditions and poor blood test results can magnify the degree of helplessness. For example, in Chiang’s case report,20 he describes a renal dialysis patient who was repeatedly hospitalized due to severe physical failure brought on by complications that left him in learned helplessness. Different treatment modalities also influence renal dialysis patients’ learned helplessness. Devins19 concluded that patients undergoing in-hospital dialysis had a lower sense of self-control than those undergoing home dialysis. Guha37 conducted a focus group interview regarding the suspension of the kidney transplant program due to COVID-19 and found that helplessness was an important psychological problem of patients during this period. If the kidney transplant program goes well, it can reduce the many limitations of renal dialysis for patients, and learned helplessness is expected to be alleviated.
Psychological Factors
Learned helplessness is not exclusively derived from demographic characteristics and personal experiences but is also influenced by psychosocial factors,38,39 including disease uncertainty and expectations, attributional styles, perceived control, and social support. Most renal dialysis patients have experienced multiple cycles of hope and dashed hopes to generate a sense of disease uncertainty and a perceived loss of control, passively accepting the fact that renal failure is incurable and inducing a learned helplessness state where the dilemma cannot be resolved.20,25 Usually, the higher the patients’ negative expectations of disease outcomes are, the stronger the learned helplessness. Attributional style means a specific tendency to choose a causal explanation: when a patient is confronted with an uncontrollable negative event, the likelihood of learned helplessness is greater if he has a stable, pervasive, internal interpretation. Most studies have concluded that social support can help alleviate learned helplessness. Still, it is worth noting that it has been suggested that excessive social support can negatively affect patients’ helplessness as well, as it can make them feel completely manipulated by medical staff.26
Consequences
Consequences describe the situation that follows the “occurrence” of the concept.16 Considering the impact of learned helplessness in renal dialysis patients, most studies emphasize that psychological and physiological problems, quality of life, and health-related behavior should be used as indicators.
Psychological Problems
First, learned helplessness as a persistent negative psychological state can naturally induce more serious psychological problems, such as cognitive biases, embitterment, anxiety and depression, and even suicidal intention.20,33,39–41 For example, in a qualitative study, some patients described their inability to control ESKD effectively and the consequences of renal dialysis, viewing themselves as servants or bystanders to dialysis machines.27 Learned helplessness can also predict patients’ depression and suicidal intention,35 so there is a need to investigate potential suicidal intention in patients with chronic kidney disease, focusing on identifying those with scores ≥9 on the BHS29,40 for early intervention.
Physiological Problem
For possible physiological problems associated with learned helplessness, Elif25 found that helplessness was associated with interdialytic weight gain (IDWG), PO4, and K in a cross-sectional survey of renal dialysis patients in Turkey. In a Japanese multicenter cohort study, a high level of learned helplessness was found to be associated with a high level of sarcopenia in renal dialysis patients,31 which may be related to the ability of helplessness to increase the levels of proinflammatory cytokines.
Quality of Life
A growing number of studies claim that learned helplessness can predict the future quality of life in renal dialysis patients.39,41,42 Tommel39 performed a multiple regression analysis and found that baseline learned helplessness was a relevant predictor of health-related quality of life (HRQOL) 6 months later. Lee41 found that learned helplessness decreased renal dialysis patients’ EQ-5D-VAS scores in an investigation of patients in various stages of chronic kidney disease.
Health-Related Behavior
Due to the irreversibility of ESKD, many renal dialysis patients experience multiple self-management failures. They become fearful and avoidant, falling into a vicious cycle of failure, with the resulting learned helplessness making it more difficult to conduct self-management.25,31,42,43 Helpless renal dialysis patients adhere significantly less to regular treatment and seem to have more difficulty carrying out physicians’ recommendations for diet, water, and physical exercise.20,25,31,44
Measurement Tools
Measurement instruments are tools that define the characteristics of the concept.45 One of the more commonly used in the samples is Beck’s Hopelessness Scale (BHS),25,35 which includes three dimensions of existing apprehension, tendency to give up when making decisions, and negative predictions about the future, including 20 statements of helplessness.46 Tommel39 measured the degree of helplessness in renal dialysis patients using a subscale from the Illness Cognition Questionnaire (ICQ), which contains six items and is positively scored using a Likert 4-point scale with a Cronbach’s α of 0.81–0.91.47 The Powerlessness assessment tool (PAT) was also used to assess the renal dialysis patients’ powerlessness and its source.48 The instrument was scored on a 5-point Likert scale, whose first part consisted of 5 questions, with higher scores associated with a decrease in feelings of helplessness. The second part consisted of 7 questions, with higher scores associated with an increase in the source of powerlessness.44 Simoni33 used the Hopelessness Scale for Children to measure helplessness in HD children, which consists of 17 items, with higher scores reflecting greater hopelessness. The scale has the advantage of being simply worded and easily understood by children.
Interventions
Learned helplessness plays an important role in the commitment of renal dialysis patients to treatment and self-management and has been a major challenge for medicine. In the selected sample, interventions for helpless renal dialysis patients focused on preventive psychological nursing, cognitive therapy, health empowerment, humanistic care, and social support.
Medical staff should prioritize the alleviation of the patient’s physical discomfort and establish a medical relationship of trust.20 Society and hospitals should provide a supportive environment for renal dialysis patients, such as medical, information, family, and peer support.20,44,49 More preventive psychological nursing should be given to renal dialysis patients before their first dialysis to reduce perceived loss of control.21 Goal-oriented health education or multimedia health education can enhance renal dialysis patients’ self-care knowledge and improve health-related behavior, which is an effective option to reduce learned helplessness. Nurses can identify the learned helplessness in renal dialysis patients regarding physical and psychological state and social dimensions, and can integrate humanistic care throughout the nursing process.20 Motivational interviewing, life review and mindfulness-based training can be used to enhance renal dialysis patients’ self-concept and help them eliminate helplessness.28 Based on health empowerment theory, renal dialysis patients are encouraged to participate in self-management. For example, by providing opportunities for self-determination, helping and rewarding them for experiencing self-management successes, it is conducive to increasing their self-efficacy, rebuilding hope, and successfully coping with the helplessness stage.27 In addition, it can also help helpless patients to achieve a gradual internal transformation, acceptance of a new self-state, and willingness to live with ESKD.
Surrogate Terms
Due to similarities in meaning, a surrogate term is used instead of the main concept.45 In selecting samples, one of the most challenging is the seemingly interchangeable use of other terms to describe the phenomenon of learned helplessness. Multiple terms are used throughout the literature, which makes it difficult to explore learned helplessness separately from other concepts. These terms include powerlessness and hopelessness.
Related Concept
A related concept connects or interacts with the target concept but does not share all its characteristics.50 A concept often mentioned in the literature concerning learned helplessness is depression, which is often considered a mood disorder ranging from mild negative emotions to severe.51 Seligman, the proponent of learned helplessness, insisted that it has great similarities in behaviors,52 physical symptoms, etiology, treatment, and prevention with depression, which Abramson supported.22 Researchers in the selected sample have studied learned helplessness in renal dialysis patients while also giving importance to the study of depression.29 They tend to consider learned helplessness as a symptom or an aggravating factor of depression. Therefore, learned helplessness can serve as an explanatory model for depression in renal dialysis patients.29,35
However, some scholars believe that learned helplessness is distinct from depression. Kurita31 considered learned helplessness to be another psychological state that reflects the individual’s loss of self-worth or future goals, in addition to depression. Andrade40 argued that learned helplessness is less severe than depression and that although there is a strong relationship between them, they are also different emotional phenomena.
Model Case
The model case better reflects the concept as a real situation.45 The essence of learned helplessness is understood below through the renal dialysis patient20 suffering from hypertension, diabetes, heart disease, and kidney disease for ten years. After starting dialysis, his health declined rapidly, and he complained, “My whole body is sick. What”s the use of my life?’ He also complained, ‘I have to maintain dialysis twice a week, for four hours at a time, and I usually have to return to the cardiology department. Having spent a lot of time in the hospital, I do not know where is the end?’ His wife said, “Dialysis has hit him hard. He often sits at home all day in frustration and becomes less talkative.” During the interview, the patient had a sad expression, frowned down, and said, “How can I feel good? I cannot even take care of myself. I”m a burden to my family and keep dragging everyone down, it is better to die early, and they will be relaxed.’ The patient believed that even if he followed the doctors’ advice, there was no significant improvement in his physical function. He feels helpless due to his declining sense of control over his life and believes that he is a person waiting to die.
Discussion
Nursing researchers often use concepts from other disciplines directly to measure certain variables. However, it is unclear whether these concepts reflect the phenomena or essence of nursing and contribute to the construction of the nursing discipline, which requires scholars to apply the rigorous steps of concept analysis to define the core concepts in the research. Evolutionary concept analysis provides a structured approach to critically assess knowledge of a concept.53 Learned helplessness has been shown to be prevalent in renal dialysis patients, and the purpose of our study was to provide a clear and comprehensive definition for it (Figure 2). The findings provide a concrete and distinguishable description of learned helplessness in renal dialysis patients, which can help health care providers to understand this psychological phenomenon better. The concept of learned helplessness in renal dialysis patients is multidimensional, reflected in the patient’s low self-concept, perceived loss, negative cognitive set, and abandonment of action. These attributes signify that renal dialysis patients are experiencing learned helplessness, which fits greatly with the learned helplessness model originally proposed by Seligman. Therefore, the concept is also generally applicable to renal dialysis patients.
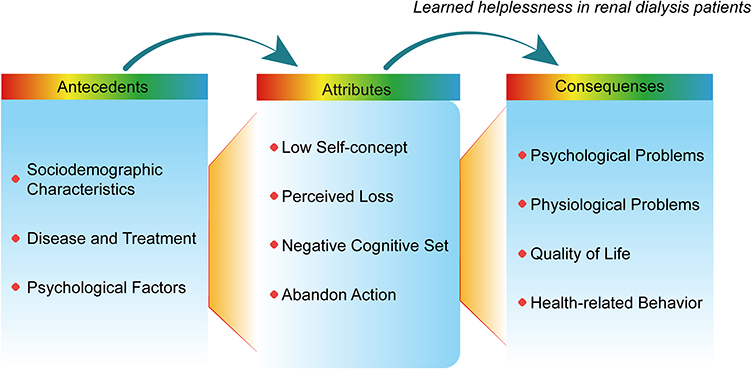 |
Figure 2 Conceptual map of learned helplessness in renal dialysis patients. |
Research on the sociodemographic characteristics of learned helplessness is very limited, and whether other factors, such as age, education, and socioeconomic status, can affect learned helplessness needs to be supported by more primary research. In addition, further exploration is needed to determine what the learned helplessness duration is, whether it changes with the course of treatment, and what the mechanism of this change is.
Once patients develop learned helplessness, it may impair their physical health, mental health, and behavioral patterns. Learned helplessness can effectively predict depression and suicidal intention in renal dialysis patients. Still, the results of this study did not fully distinguish learned helplessness from depression, and future studies focusing on the differences in their antecedents will help determine whether they are two different psychological states in the same continuous regulation process. Learned helplessness can also hinder renal dialysis patients from adopting health-related behaviors, resulting in nonadherence to medical advice and abandonment of self-management. When patients develop learned helplessness, their health interventions become complicated, and, in the long run, this state may even affect their health outcome indicators and quality of life. Therefore, identifying learned helplessness in renal dialysis patients and further exploring effective interventions from nursing care can hopefully improve their health-related outcomes.
According to the results of this study, since helplessness is largely dependent on ESKD and treatment factors, its scope of influence is likely to be limited to self-management, adherence, and other health-related situations. It may not necessarily generalize to all aspects of life, which is particularly prominent in Chinese individuals. For example, in our communication with renal dialysis patients, we found that middle-aged patients often bear the responsibility of raising the family but do not necessarily remain indifferent or abandon their career and child education. However, we will further explain the mechanism of the phenomenon in future qualitative research.
The use of cognitive therapy, empowerment theory, behavior change theory, and humanistic care models for developing and implementing supportive interventions could be expected to reduce renal dialysis patients’ learned helplessness. However, we do not know if these interventions use learned helplessness as the target indicator. In the future, we need to verify further whether the programs use learned helplessness as the target and clarify the mediators and moderators of the intervention outcomes to eliminate the learned helplessness by designing precise intervention programs and ultimately achieve health promotion for renal dialysis patients.
Rodgers noted that the results of the conceptual analysis could be viewed as a starting point rather than a final definition. The antecedents and consequences of learned helplessness identified in this analysis provide the necessary application for further research to guide the design of intervention programs to control these factors. Therefore, the next step is to develop the concept of learned helplessness and use these findings to transfer them to clinical care practice.
Implications for Future Research
Most samples were based on cross-sectional surveys, and the relationship between learned helplessness and many factors may be bidirectional (eg, depression and self-management), so longitudinal studies are needed to understand the interaction of these factors over time. In addition, the relationship between learned helplessness’s attributes, antecedents, consequences, and disease-related indicators will help reveal whether learned helplessness has specific clinical significance. Qualitative studies focusing on a central phenomenon of learned helplessness are scarce and have not yet been able to uncover renal dialysis patients’ deeper information and specific needs, highlighting the need for well-designed mixed studies in the future to complement the interpretation of this concept. The scales used in the samples were not fully adapted to the renal dialysis patients, and the items were too large for clinical generalization. For example, the statements on the BHS are based on descriptions of life and the future. They are not fully applicable to renal dialysis patients’ disease situations, and the “yes or no” scoring method does not fully reflect other degrees of helplessness. To further develop the concept, it is recommended that specific measurement tools be developed based on its attributes, including the best way and time to measure helplessness. The results of this study could provide a reference for the development of instruments.
Limitation
We only included articles published in English and Chinese, and excluding articles published in other languages may limit our understanding of learned helplessness in renal dialysis patients.
Conclusion
With the passage of time and the addition of original studies, there is insufficient evidence to reflect the conceptual content at this stage, so it is meaningful to conduct a conceptual analysis of learned helplessness in renal dialysis patients. The findings can help us to understand and clarify the context of learned helplessness in renal dialysis patients. This study found that learned helplessness in renal dialysis patients is a negative psychological state or behavior mode, which is a feeling of loss of control or powerlessness after learning about disease or disease-related events. The identified attributes, antecedents, consequences, and related concepts allow for learned helplessness to be considered a psychological concept that is independent of and linked to depression, but this still needs further clarification. Analysis of this concept helps develop nursing theories and design specific tools that can help nurses to identify the phenomenon of learned helplessness in renal dialysis patients.
Acknowledgment
This research received grants from the Hunan Provincial Science and Technology Department (No.2021SK2031), and 2022 Central South University Graduate Student Independent Exploration and Innovation Program (No. 1053320213471).
Disclosure
The authors report no conflicts of interest.
References
1. Dunn SL. Hopelessness as a response to physical illness. J Nurs Scholarsh. 2005;37(2):148–154. doi:10.1111/j.1547-5069.2005.00027.x
2. Seligman ME. Learned helplessness as a model of depression. Comment and integration. J Abnorm Psychol. 1978;87(1):165–179. doi:10.1037/0021-843X.87.1.165
3. Huzian O, Baka J, Csakvari E, et al. Stress resilience is Associated with Hippocampal Synaptoprotection in the female rat learned helplessness paradigm. Neuroscience. 2021;459:85–103. doi:10.1016/j.neuroscience.2021.01.029
4. Bruns B, Schmitz T, Diemert N, et al. Learned helplessness reveals a population at risk for depressive‐like behaviour after myocardial infarction in mice. ESC Heart Failure. 2019;6(4):711–722. doi:10.1002/ehf2.12440
5. Günsoy C, Cross SE, Uskul AK, Gercek‐Swing B. The role of culture in appraisals, emotions and helplessness in response to threats. Int J Psychol. 2020;55(3):472–477. doi:10.1002/ijop.12589
6. Smith TW, Peck JR, Ward JR. Helplessness and depression in rheumatoid arthritis. Health Psychol. 1990;9(4):377. doi:10.1037/0278-6133.9.4.377
7. Camacho E, Verstappen S, Symmons D. Association between socioeconomic status, learned helplessness, and disease outcome in patients with inflammatory polyarthritis. Arthritis Care Res Nurs Health Psychol. 2012;64(8):1225–1232. doi:10.1002/acr.21677
8. Camacho EM, Verstappen SMM, Chipping J, et al. Learned helplessness predicts functional disability, pain and fatigue in patients with recent-onset inflammatory polyarthritis. Rheumatology. 2013;52(7):1233–1238. doi:10.1093/rheumatology/kes434
9. Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385(9981):1975–1982.
10. Romagnani P, Remuzzi G, Glassock R, et al. Chronic kidney disease. Nat Rev Dis Primers. 2017;3(1):1–24.
11. Jha V, Martin D, Bargman J, et al. Ethical issues in dialysis therapy. Lancet. 2017;389(10081):1851–1856. doi:10.1016/S0140-6736(16)32408-4
12. Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713–735. doi:10.1053/j.ajkd.2014.01.416
13. Boing AF, Melo GR, Boing AC, Moretti-Pires RO, Peres KG, Peres MA. Associação entre depressão e doenças crônicas: es tudo populacional [Association between depression and chronic diseases: results from a population-based study[J]]. Rev Saúde Pública. 2012;46:617–623. doi:10.1590/S0034-89102012005000044
14. Schick Makaroff KL. The unsayable: a concept analysis. J Adv Nurs. 2014;69(2):481–492. doi:10.1111/j.1365-2648.2012.06083.x
15. Markus KA. Constructs, concepts and the worlds of possibility: connecting the measurement, manipulation, and meaning of variables. Measurement. 2008;6(1–2):54–77.
16. Rodgers B, Jacelon CS, Knafl KA. Concept analysis and the advance of nursing knowledge: state of the science. J Nurs Scholarsh. 2018;50(4):451–459. doi:10.1111/jnu.12386
17. Tofthagen R, Fagerstrom LM, Rodgers’ evolutionary concept analysis - a valid method for developing knowledge in nursing science. Scand J Caring Sci. 2010;24:21–31. doi:10.1111/j.1471-6712.2010.00845.x
18. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(3):77–101. doi:10.1191/1478088706qp063oa
19. Devins GM, Binik YM, Hollomby DJ, Barré PE, Guttmann RD. Helplessness and depression in end-stage renal disease. J Abnorm Psychol. 1981;90(6):531–545. doi:10.1037/0021-843X.90.6.531
20. Chiang YY, Tsai LY. Applying swanson’s caring theory to a patient with end renal stage disease experiencing hopelessness. Hu Li Za Zhi. 2021;68(2):99–106. doi:10.6224/JN.202104_68(2).13
21. Dec E. Impact of locus of control on clinical outcomes in renal dialysis. Adv Chronic Kidney Dis. 2006;13(1):76–85. doi:10.1053/j.ackd.2005.10.009
22. Abramson LY, Seligman ME, Teasdale JD. Learned helplessness in humans: critique and reformulation. J Abnorm Psychol. 1978;87(1):49. doi:10.1037/0021-843X.87.1.49
23. Schwartz-Barcott D, Kim H, Rodgers B, Knafl K. Concept Development in Nursing: Foundations, Techniques, and Applications. Saunders; 2000.
24. Roy C, Andrews HA. The Roy Adaptation Model: The Definitive Statement. Appleton & Lange; 1991.
25. Ok E, Kutlu FY. Hopelessness, anxiety, depression and treatment adherence in chronic hemodialysis patients. Int J Caring Sci. 2019;12(1):423–429.
26. Lowenhaupt E. Psychic reactions to long-term hemodialysis: evaluation in the elderly by means of the draw‐a‐person test. J Am Geriatr Soc. 1977;25(8):358–363. doi:10.1111/j.1532-5415.1977.tb00660.x
27. Duncanson E, Chur-Hansen A, Jesudason S. Psychosocial consequences of gastrointestinal symptoms and dietary changes in people receiving automated peritoneal dialysis. J Ren Care. 2019;45(1):41–50. doi:10.1111/jorc.12265
28. Gerber KE, Nehemkis AM, Farberow NL, Williams J. Indirect self-destructive behavior in chronic hemodialysis patients. Suicide Life Threat Behav. 1981;11(1):31–42. doi:10.1111/j.1943-278X.1981.tb00997.x
29. Ö T, Balaban ÖD, Mutlu C, Şahmelikoğlu Ö, Bali M, Ermis C. Depression and cognitive distortions in hemodialysis patients with end stage renal disease: a case-control study. Eur Psychiatry. 2021;35(4):242–250. doi:10.1016/j.ejpsy.2021.01.001
30. Pope-Caldwell SM, Washburn DA. Overcoming cognitive set bias requires more than seeing an alternative strategy. Sci Rep. 2022;12(1):2179. doi:10.1038/s41598-022-06237-0
31. Kurita N, Wakita T, Fujimoto S, et al. Hopelessness and depression predict sarcopenia in advanced CKD and dialysis: a multicenter cohort study. J Nutr Health Aging. 2021;25(5):593–599. doi:10.1007/s12603-020-1556-4
32. Tagay S, Kribben A, Hohenstein A, Mewes R, Senf W. Posttraumatic stress disorder in hemodialysis patients. Am J Kidney Dis. 2007;50(4):594–601. doi:10.1053/j.ajkd.2007.06.018
33. Simoni JM, Asarnow JR, Munford PR, Koprowski CM, Belin TR, Salusky IB. Psychological distress and treatment adherence among children on dialysis. Pediatr Nephrol. 1997;11(5):604–606. doi:10.1007/s004670050346
34. Lindsay H, MacGregor C, Fry M. The experience of living with chronic illness for the haemodialysis patient: an interpretative phenomenological analysis. Health Sociol Rev. 2014;23(3):232–241. doi:10.1080/14461242.2014.11081976
35. Kim JA, Lee YK, Huh WS, et al. Analysis of depression in continuous ambulatory peritoneal dialysis patients. J Korean Med Sci. 2002;17(6):790–794. doi:10.3346/jkms.2002.17.6.790
36. Bahmani B, Motamed Najjar M, Sayyah M, Shafi-Abadi A, Haddad Kashani H. The effectiveness of cognitive-existential group therapy on increasing hope and decreasing depression in women-treated with haemodialysis. Glob J Health Sci. 2015;8(6):219–225. doi:10.5539/gjhs.v8n6p219
37. Guha C, Tong A, Baumgart A, et al. Suspension and resumption of kidney transplant programmes during the COVID-19 pandemic: perspectives from patients, caregivers and potential living donors – a qualitative study. Transpl Int. 2020;33(11):1481–1490. doi:10.1111/tri.13697
38. Tezel A, Karabulutlu E, Şahin Ö. Depression and perceived social support from family in Turkish patients with chronic renal failure treated by hemodialysis. J Res Med Sci. 2011;16:5.
39. Tommel J, Evers AWM, van Hamersvelt HW, et al. Predicting health-related quality of life in dialysis patients: factors related to negative outcome expectancies and social support. Patient Educ Couns. 2021;104(6):1474–1480. doi:10.1016/j.pec.2020.11.019
40. Andrade SV, Sesso R, Diniz DH. Hopelessness, suicide ideation, and depression in chronic kidney disease patients on hemodialysis or transplant recipients. Braz J Nephrol. 2015;37:55–63. doi:10.5935/0101-2800.20150009
41. Lee K, Song HC, Choi EJ, Pae CU, Kim YK. Posttraumatic embitterment disorder in patients with chronic kidney disease. Clin Psychopharmacol Neurosci. 2019;17(2):183–188. doi:10.9758/cpn.2019.17.2.183
42. Gibson EL, Held I, Khawnekar D, Rutherford P. Differences in knowledge, stress, sensation seeking, and locus of control linked to dietary adherence in hemodialysis patients. Front Psychol. 2016;7:1864. doi:10.3389/fpsyg.2016.01864
43. Tavassoli N, Darvishpour A, Mansour-Ghanaei R, Atrkarroushan Z. A correlational study of hope and its relationship with spiritual health on hemodialysis patients. J Educ Health Promot. 2019;8:146. doi:10.4103/jehp.jehp_461_18
44. Wang LM, Chiou CP. Effectiveness of interactive multimedia CD on self-care and powerlessness in hemodialysis patients. J Nurs Res. 2011;19(2):102–111. doi:10.1097/JNR.0b013e31821b0eff
45. Rodgers BL. Concept analysis: an evolutionary view. Concept Develop Nurs. 2000;14:77–102.
46. Beck AT, Weissman A, Lester D, Trexler L. The measurement of pessimism: the hopelessness scale. J Consult Clin Psychol. 1974;42(6):861–865. doi:10.1037/h0037562
47. Evers AW, Kraaimaat FW, van LW, Jongen PJ, Jacobs JWG, Bijlsma JWJ. Beyond unfavorable thinking: the illness cognition questionnaire for chronic diseases. Consult Clin Psychol. 2001;69(6):1026–1036. doi:10.1037/0022-006X.69.6.1026
48. Kubsch S, Wichowski HC. Restoring power through nursing intervention. Int J Nurs Terminol Classif. 1997;8(1):7–15. doi:10.1111/j.1744-618X.1997.tb00127.x
49. Stapleton S. Powerlessness in persons with end-stage renal disease. In: Coping with Chronic Illness: Overcoming Powerlessness.
50. Goldenberg D, Iwasiw C. Professional socialisation of nursing students as an outcome of a senior clinical preceptorship experience. Nurse Educ Today. 1993;13(1):3–15. doi:10.1016/0260-6917(93)90003-K
51. Tuithof M, Ten Have M, van Dorsselaer S, Kleinjan M, Beekman A, de Graaf R. Course of subthreshold depression into a depressive disorder and its risk factors. J Affect Disord. 2018;241:206–215. doi:10.1016/j.jad.2018.08.010
52. Maier SF, Seligman ME. Learned helplessness: theory and evidence. J Exp Psychol. 1976;105(1):3. doi:10.1037/0096-3445.105.1.3
53. Agenor C, Conner N, Aroian K. Flourishing: an evolutionary concept analysis. Issues Ment Health Nurs. 2017;38(11):915–923. doi:10.1080/01612840.2017.1355945
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.