Back to Journals » Journal of Healthcare Leadership » Volume 18
Leadership-Driven Development of a National Emergency Medical Dispatch and Triage Protocol in Thailand: An Electronic Delphi Expert Consensus
Authors Rojsaengroeng R ![]() , Sri-On J, Huabbangyang T
, Sri-On J, Huabbangyang T ![]() , Thepmanee D, Buaprasert P
, Thepmanee D, Buaprasert P ![]() , Chansomboon P
, Chansomboon P ![]()
Received 15 November 2025
Accepted for publication 31 January 2026
Published 6 February 2026 Volume 2026:18 581816
DOI https://doi.org/10.2147/JHL.S581816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Rapeeporn Rojsaengroeng,1 Jiraporn Sri-On,1 Thongpitak Huabbangyang,2 Duangpon Thepmanee,2 Phudit Buaprasert,3 Pit Chansomboon4
1Department of Emergency Medicine, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2Department of Disaster and Emergency Medical Operation, Faculty of Science and Health Technology, Navamindradhiraj University, Bangkok, Thailand; 3Department of Emergency Medicine, Emory University School of Medicine, Atlanta, GA, USA; 4Department of Emergency Medicine, Udonthani Hospital, Udon Thani, Udonthani Province, Thailand
Correspondence: Thongpitak Huabbangyang, Email [email protected]
Introduction: Effective telephone triage is a critical leadership function within emergency medical systems, supporting timely decision-making, appropriate resource allocation, and improved patient outcomes. This role is particularly important in countries with developing prehospital infrastructures, where emergency medical dispatchers are central to guiding early emergency responses.
Purpose: This study aimed to develop and achieve expert consensus on Thailand’s Emergency Medical Triage Protocol and Criteria-Based Dispatch Code (EMTP-CBDC) using an electronic Delphi expert consensus (EDEC) approach, in order to produce an accurate, up-to-date, and nationally applicable dispatch protocol aligned with international standards.
Methods: A two-round Delphi process was conducted involving 40 emergency medical experts with at least one year of dispatch or prehospital oversight experience. Experts evaluated 30 chief complaints and key operational components of the EMTP-CBDC developed by the National Institute for Emergency Medicine. Round 1 consisted of an onsite panel discussion to review protocol logic and content, followed by structured online assessments across three domains: protocol structure, application, and coding. Items were rated on a 5-point Likert scale, with a mean score ≥ 3.41 indicating acceptance. Revised items were reassessed in Round 2 to confirm clarity, appropriateness, and consensus.
Results: High-to-highest levels of expert agreement were achieved across all protocol domains. Overall structure scored highly (= 4.54 ± 0.48), while pre-arrival instructions received the highest ratings (= 4.77 ± 0.51). Emergency medical conditions and injury categories demonstrated high agreement (= 3.96 and 4.01, respectively). Telephone guidance, triage and dispatch processes, and CBD code application standards also showed strong consensus, confirming clarity and usability for national dispatch operations.
Conclusion: The revised EMTP-CBDC demonstrates high clarity, practicality, and expert consensus, supporting its suitability for nationwide implementation. Adoption of this protocol, alongside continuous dispatcher training and system monitoring, may enhance dispatch accuracy, operational consistency, and overall emergency medical service performance in Thailand.
Keywords: emergency medical services, triage, emergency medical dispatch, Delphi technique, patient care
Introduction
Developing an efficient and effective emergency medical service (EMS) system is a critical public health priority aimed at reducing morbidity and mortality from emergency conditions. This objective aligns with the “Star of Life” framework, which emphasizes key EMS functions including patient access, prehospital care, transportation, referral, and continuity of hospital-based management.1,2 Within this framework, emergency medical dispatch (EMD) serves as a central operational component, functioning as the initial point of contact that determines incident classification, urgency prioritization, and allocation of prehospital resources through standardized triage protocols.
In well-established EMS systems, dispatch protocols are systematically designed to link caller-reported symptoms with structured decision algorithms that guide both urgency determination and resource deployment. For example, the Netherlands employs the Dutch Field Triage Protocol based on standards from the American College of Surgeons Committee on Trauma (ACS-COT),3 while the Medical Priority Dispatch System (MPDS) is widely implemented in the United States, United Kingdom, and Australia.4–9 These systems use structured chief complaint classifications to support consistent dispatch decision-making and appropriate resource allocation, with evidence demonstrating improvements in dispatch efficiency, response times, and alignment of resources with patient acuity.10 Similarly, Norway applies the Norwegian Index for Medical Dispatch,11,12 and Japan utilizes Fire and Disaster Management Agency (FDMA) protocols to standardize emergency severity classification and dispatch prioritization.13 Collectively, these international models highlight the importance of regularly updated, algorithm-driven dispatch systems that integrate clinical logic, operational feasibility, and pre-arrival guidance.
Thailand’s EMS system has developed progressively since 1989 and is currently overseen by the National Institute for Emergency Medicine (NIEMS) under the Emergency Medical Act B.E. 2551.14,15 Despite nationwide coverage and free access to EMS, utilization remains relatively low, with only 14.5% of patients accessing EMS services, largely due to limited public awareness and lack of familiarity with emergency access numbers.16 While Thailand has made substantial efforts to standardize ambulance equipment, personnel qualifications, and service levels, challenges persist, including limited national data on emergency demand patterns and variability in dispatch practices across regions.17
Within this system, EMS responses are organized using a tiered model designed to match patient acuity with appropriate levels of prehospital care. Depending on dispatch priority and regional resources, response units may include paramedic–paramedic teams, nurse–paramedic teams, or physician-led units involving emergency physicians working alongside nurses or paramedics. Consequently, dispatch decisions in Thailand directly influence not only response urgency but also the configuration of personnel and resources deployed to the scene.
Since 2011, Thailand has relied on a criteria-based dispatch (CBD) system comprising 26 chief complaints categorized by color-coded urgency levels (red, yellow, green, and white) to guide dispatch prioritization.18 However, unlike many international dispatch systems, the Thai CBD protocol has undergone limited structural revision and does not fully reflect evolving disease patterns, increasing clinical complexity, or advances in dispatch technology, such as standardized pre-arrival instructions (PAI). Although COVID-19 was added as a chief complaint in 2022,19 the overall framework remains largely unchanged and lacks systematic mechanisms for expert consensus updating, operational validation, and alignment with contemporary international standards.
In response to these limitations, NIEMS initiated the redevelopment of Thailand’s emergency medical triage protocol and criteria-based dispatch code through an electronic Delphi expert consensus (EDEC) process. This structured approach was designed to integrate multidisciplinary expert input, address identified gaps in the existing dispatch system, and establish an updated EMTP-CBDC that is clinically relevant, operationally feasible, and aligned with global best practices in emergency medical dispatch.
Aim
This study aimed to develop Thailand’s EMTP-CBDC using the EDEC process.
Methods
Study Design
This study used a research and development design based on the Delphi technique.
Participants
Data were collected from 40 experts selected by the authors based on qualifications and expertise, representing health regions 1–13 according to Thailand’s public health regional division.
Eligibility Criteria
Eligible participants included dispatch center personnel such as certified emergency physicians with prehospital emergency experience, emergency nurse practitioners, and paramedics. Participants were required to be at least 18 years old and have a minimum of 1 year of experience working in a dispatch center.
Exclusion Criteria
Participants who were unwilling to participate or declined to complete the questionnaires were excluded.
Data Gathering and Rationale for the Delphi Process
The research tool was the latest draft of the EMTP-CBDC, comprising 30 chief complaints that had previously undergone formal content validity assessment and been published by Huabbangyang et al.20 While the prior content validity study primarily evaluated item-level relevance and clarity under expert judgment, it did not address broader operational applicability, workflow integration, or national-level consensus across diverse emergency medical dispatch contexts.
Therefore, the present study employed a Delphi-based expert consensus process to complement the earlier content validity assessment. The Delphi technique was specifically used to achieve multidisciplinary and nationwide consensus, refine the operational structure of the protocol, and evaluate its applicability within real-world emergency medical dispatch workflows. This approach allowed iterative expert review of protocol logic, dispatch sequencing, pre-arrival instruction integration, and criteria-based dispatch code application, thereby strengthening the system-level readiness of the EMTP-CBDC for national implementation.
An initial panel discussion involving five experts was conducted to exchange in-depth opinions, clarify operational issues, and identify areas requiring refinement prior to formal Delphi rounds.
Two-Round Delphi Process
Two rounds of the Delphi technique were conducted to collect expert opinions from professionals in emergency medicine and EMS. The goal was to refine and validate the EMTP-CBDC to ensure clarity, appropriateness, and alignment with real-world practice.
Delphi Round 1
The first round took place on March 29, 2024, through an 8-h onsite panel discussion aimed at reviewing the decision logic and content of the validated EMTP-CBDC draft.
Before the meeting, experts received related documents, including the EMTP-CBDC draft and discussion guidelines under the Chatham House Rule to ensure independent expression of opinions. During the discussion, each item was reviewed to identify unclear or disputed points for later revision. After the meeting, participants completed an online questionnaire via Google Forms consisting of two sections:
Part 1: Closed-ended questions covering three aspects—(1) criteria structure (eg, call handling, dispatch operation, pre-arrival instruction, emergency conditions, injuries, and telephone guidance), (2) application and triage, and (3) code appropriateness. Items were rated on a 5-point Likert scale (5 = highest to 1 = lowest), interpreted according to Best: 1986,21 which determine average score ranges as: 4.21–5.00 = highest, 3.41–4.20 = high, 2.61–3.40 = moderate, 1.81–2.60 = low, and 1.00–1.80 = lowest.
Part 2: Open-ended questions for independent expert feedback.
Items with a mean score ≥3.41 were considered suitable, whereas those scoring below 3.41 or showing significant disagreement were revised for the second round.
Delphi Round 2
In the second round, experts reviewed revised questionnaires based on the first-round results. The questionnaire maintained the same three-part structure to reassess appropriateness, clarity, and applicability. Items were again rated on a 5-point Likert scale and interpreted per Best 1986,21 Items with mean scores ≥3.41 were accepted into the finalized EMTP-CBDC draft, whereas those below 3.41 were excluded due to lack of consensus.
Statistical Analysis
Quantitative data were analyzed using descriptive statistics, including mean, standard deviation, and percentage, to identify opinion trends and consensus levels. Qualitative data from open-ended responses and discussions were analyzed through content analysis to refine wording and criteria descriptions. All analyses were conducted using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY, USA).
Results
Basic Data
The study involved 40 experts representing all 13 health regions of Thailand who participated in developing the EMTP-CBDC through the Delphi technique. Among participants, 50% were male, with a mean age of 38.40 ± 7.59 years. Most participants (72.5%) were aged 35 years or older, and 35% were emergency physicians. The median administrative experience in dispatch centers was six years (interquartile range [IQR]: 5–10), with the majority (35%) having 5–9 years of experience. Most experts (57.5%) were from the 5th and 6th health regions, and each region contributed approximately 10% of participants. The median number of prehospital triaged cases per year was 8750 (IQR: 1000–33,750), and half of the experts handled at least 10,000 cases annually (Table 1).
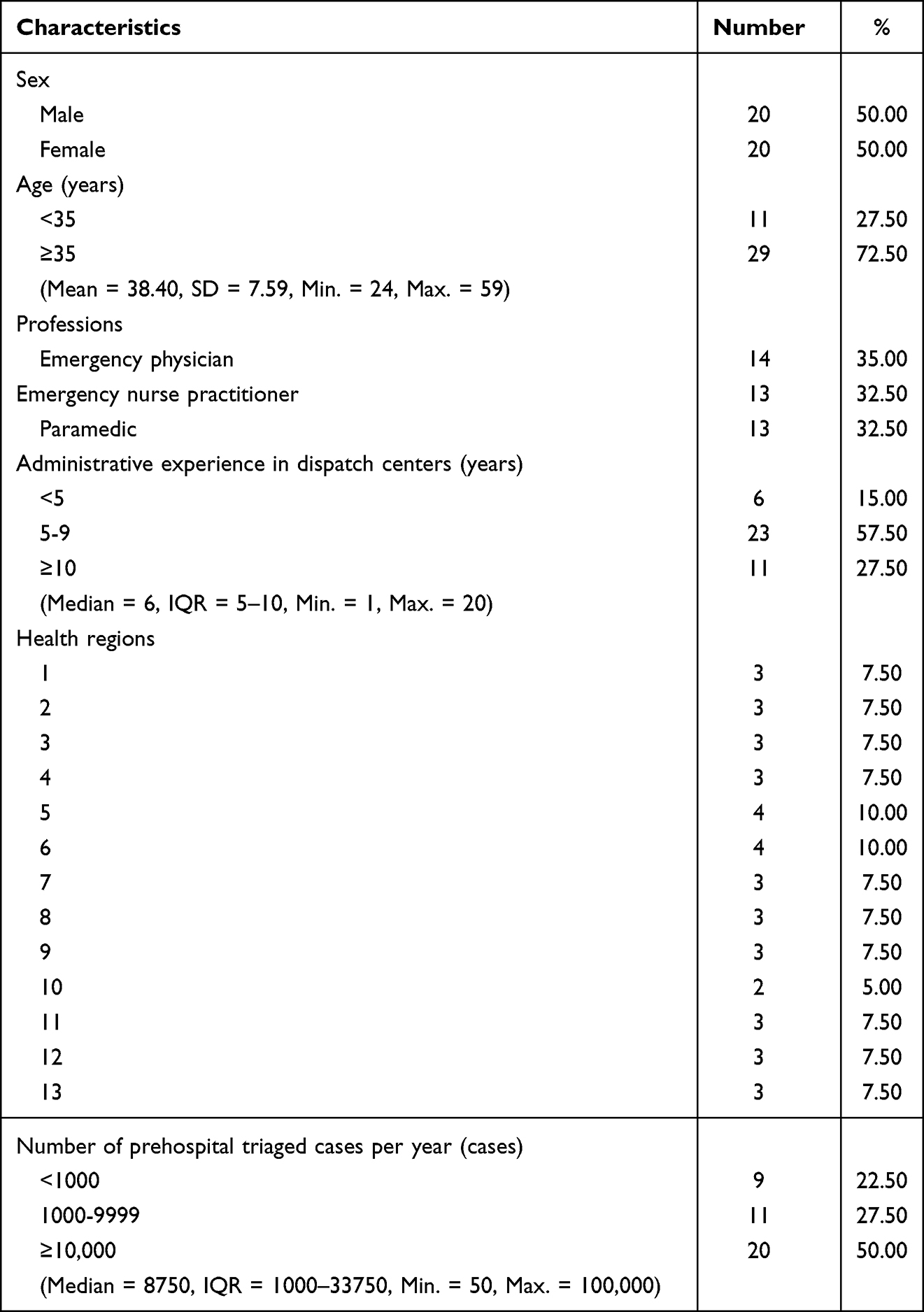 |
Table 1 General Data |
Convenience and Accuracy in EMTP-CBDC Manual Application
Regarding the experts’ opinions on the Thailand EMTP-CBDC manual application, findings are summarized as follows:
For the first aspect—structure—the overall opinion level concerning call handling procedures, emergency operation dispatch, and emergency patient assistance coordination was at the highest level ( = 4.54 ± 0.48). The item “Where is the patient?” achieved the highest mean at the highest level (
= 4.54 ± 0.48). The item “Where is the patient?” achieved the highest mean at the highest level ( = 4.92 ± 0.35), whereas the subitem “What happened?”—(Choking) Cough/breathe? (“You check then tell me what you find”) breathlessness, silent cough, “Don’t hit her/his back” 11-Red-1—received the lowest mean at a high level (
= 4.92 ± 0.35), whereas the subitem “What happened?”—(Choking) Cough/breathe? (“You check then tell me what you find”) breathlessness, silent cough, “Don’t hit her/his back” 11-Red-1—received the lowest mean at a high level ( = 4.02 ± 1.21) (Table S1).
= 4.02 ± 1.21) (Table S1).
For pre-arrival instructions, the overall opinion level was at the highest level ( = 4.77 ± 0.51). The item “If cardiac arrest is suspected, perform chest compression” had the highest mean (
= 4.77 ± 0.51). The item “If cardiac arrest is suspected, perform chest compression” had the highest mean ( = 4.73 ± 0.72), whereas “If unconsciousness or breathlessness/agonal breathing, perform initial treatment with airway-breathing-circulation (ABC)” showed the lowest mean at a high level (
= 4.73 ± 0.72), whereas “If unconsciousness or breathlessness/agonal breathing, perform initial treatment with airway-breathing-circulation (ABC)” showed the lowest mean at a high level ( = 3.87 ± 1.45).
= 3.87 ± 1.45).
Regarding emergency medical conditions, the overall opinion level was high ( = 3.96 ± 1.05). The item “Abdominal pain triage code 1” achieved the highest mean (
= 3.96 ± 1.05). The item “Abdominal pain triage code 1” achieved the highest mean ( = 4.13 ± 1.11), whereas “Ophthalmic problem triage code 13” recorded the lowest mean (
= 4.13 ± 1.11), whereas “Ophthalmic problem triage code 13” recorded the lowest mean ( = 3.62 ± 1.41).
= 3.62 ± 1.41).
For injuries, the overall opinion level was also high ( = 4.01 ± 1.11). The item “Fall/accident/pain triage code 27” had the highest mean (
= 4.01 ± 1.11). The item “Fall/accident/pain triage code 27” had the highest mean ( = 4.10 ± 1.13), whereas “Stabbing, gunshot, or penetrating trauma triage code 29” received the lowest mean (
= 4.10 ± 1.13), whereas “Stabbing, gunshot, or penetrating trauma triage code 29” received the lowest mean ( = 3.90 ± 1.30).
= 3.90 ± 1.30).
In terms of telephone-assisted operation instructions, the overall opinion level was at the highest level ( = 4.35 ± 0.73). The item “Delivery triage” achieved the highest mean (
= 4.35 ± 0.73). The item “Delivery triage” achieved the highest mean ( = 4.47 ± 0.72), whereas “Airway/cardiac arrest/airway obstruction triage (in case of unconsciousness) – in newborns aged <30 days” had the lowest mean (
= 4.47 ± 0.72), whereas “Airway/cardiac arrest/airway obstruction triage (in case of unconsciousness) – in newborns aged <30 days” had the lowest mean ( = 4.28 ± 0.96).
= 4.28 ± 0.96).
For the second aspect—application for triage and dispatch of emergency patients—the overall opinion level was at the highest level ( = 4.28 ± 0.61). The item “Criteria-Based Dispatch (CBD) code application standard examination system should exist” obtained the highest mean (
= 4.28 ± 0.61). The item “Criteria-Based Dispatch (CBD) code application standard examination system should exist” obtained the highest mean ( = 4.70 ± 0.52), whereas “The manual causes under-triage by phone” received the lowest mean at a high level (
= 4.70 ± 0.52), whereas “The manual causes under-triage by phone” received the lowest mean at a high level ( = 3.68 ± 1.00).
= 3.68 ± 1.00).
Regarding the appropriateness of codes, the overall opinion level was at the highest level ( = 4.45 ± 0.62). The item “Red 2 Agonal breathing” had the highest mean (
= 4.45 ± 0.62). The item “Red 2 Agonal breathing” had the highest mean ( = 4.60 ± 0.67), whereas “Red 1 Unconsciousness and breathlessness (only code indicating cardiac arrest from every cause)” and “Pink 2 Difficult breathing or unable to speak a full sentence, requiring pauses to breathe, then differentiating specific codes for each disease” both showed the lowest mean at the highest level (
= 4.60 ± 0.67), whereas “Red 1 Unconsciousness and breathlessness (only code indicating cardiac arrest from every cause)” and “Pink 2 Difficult breathing or unable to speak a full sentence, requiring pauses to breathe, then differentiating specific codes for each disease” both showed the lowest mean at the highest level ( = 4.33 ± 0.94 and 4.33 ± 0.83, respectively) (Table S1).
= 4.33 ± 0.94 and 4.33 ± 0.83, respectively) (Table S1).
Across the two Delphi rounds, all 30 chief complaint categories were retained, and no items were removed due to lack of consensus. However, a subset of protocol components underwent meaningful revision between Round 1 and Round 2 based on expert feedback. These revisions primarily involved clarification of wording, refinement of decision logic, reorganization of dispatch sequencing, and enhancement of pre-arrival instruction content to improve operational clarity and real-world applicability.
Items that demonstrated lower agreement or higher variability during the first round—particularly those related to choking assessment, unconsciousness with abnormal breathing, and selected injury and ophthalmic categories—were substantially revised before reassessment in Round 2. The second Delphi round confirmed improved clarity and expert agreement for these revised items, indicating successful convergence toward national consensus without elimination of any core protocol components.
Additional Opinions or Suggestions
Structural Aspect
The evaluation of the EMTP-CBDC structure revealed expert recommendations to improve the order and format of initial questions in the call handling procedure. Experts suggested beginning with the patients’ main symptom or incident, followed by sex, age, consciousness, breathing pattern, appearance, and movement (eg, ability to sit, lie, or walk to facilitate faster and more accurate assessment of severity. They also emphasized the need to obtain contact numbers because informers are often not at the scene or are bystanders, making call-backs essential for follow-up information and continuous telephone guidance, particularly in choking cases requiring immediate first aid.
Furthermore, some experts noted inconsistencies between certain initial symptoms and the specified CBD codes. They advised integrating “strangulation” into general history-taking instead of treating it as a separate topic to reduce redundancy and simplify data collection.
Pre-Arrival Instructions
Experts suggested refining pre-arrival instruction methods to improve accuracy and alignment with real-world scenarios. For unconscious or cardiac arrest patients, dispatchers should guide informers to assess breathing and, if absent or agonal, initiate cardiopulmonary resuscitation (CPR) immediately following the Circulation–Airway–Breathing (CAB) sequence. They recommended promoting hands-only CPR or alternating with rescue breaths in a 30:2 ratio to enhance survival before emergency units arrive.
For fire or burn cases, experts discouraged the “stop, drop, and roll” method, as it may worsen flames due to wind. Instead, they advised instructing informers to use water or a wet blanket to extinguish flames. Dispatchers should use positive language, such as “Leave that dangerous location”, rather than “Escape quickly”, to prevent panic and ensure safety. Continuous phone communication and coordinated instructions were also emphasized.
Medical Emergencies
Experts recommended revising the classification and severity levels of medical symptoms to align with Thai healthcare contexts and the Emergency Severity Index (ESI) to ensure standardized urgency assessment nationwide. They also advised sequencing module codes based on actual call frequency data to highlight the most common and critical conditions. Prioritizing codes by symptom severity may improve dispatcher–field communication, facilitating faster and more accurate emergency responses.
Trauma-Related Emergencies
Experts proposed enhancing the clarity and practicality of trauma-related EMTP-CBDC components, particularly for traffic accidents, falls, and lacerations. Severity levels—life-threatening, moderate, or mild—should be explicitly defined to improve dispatch prioritization. Key screening questions should address major bleeding, head or chest trauma, abnormal respiration, and partial immobility to guide dispatchers in selecting the appropriate module code. Telephone trauma instructions should be developed to cover hemorrhage control, immobilization, and safe positioning before responders arrive. Experts also suggested prioritizing injury module codes by symptom severity and eliminating redundant or overlapping codes to reduce communication errors between dispatch centers and field units.
Telephone-Assisted Emergency Instructions
Experts emphasized that telephone-assisted instructions should be clear, concise, and sequential, enabling informers to act safely and effectively before emergency responders arrive. Protocols should be adaptable to various situations, including telephone-guided CPR, unconscious patient positioning, bleeding control, and symptom assessment. Dispatchers should use positive reinforcement, remain on the call throughout the incident, and provide continuous evaluation and guidance. Instruction content should also match the severity of the incident and the informer’s role (eg, bystander, patient, or relative) to enhance communication efficiency, reduce panic, and ensure safety for both informers and patients.
Application and Triage of Emergency Patients
Experts generally agreed that EMTP-CBDC is systematic and applicable at the dispatch center level but suggested improving its flexibility to reflect real-world Thai conditions, especially when informer data are incomplete or unclear. They recommended developing user-friendly digital decision support tools to assist Emergency Medical Dispatchers (EMDs) in selecting appropriate module codes and urgency levels. Triage criteria should align with ESI severity levels to maintain consistency across dispatch centers, field units, and hospitals. Continuous EMD training in questioning, condition assessment, and EMTP-CBDC usage was also recommended, along with the establishment of a field monitoring system to evaluate and improve long-term triage accuracy and consistency.
Appropriateness of Codes and Classifications
Experts concurred that the module and chief complaint code structures in EMTP-CBDC should be revised to be more systematic, transparent, and aligned with clinical triage principles. Codes should accurately represent patient conditions and severity levels. Standardized module codes should be compatible with national data reporting systems to enable efficient analysis and quality assessment. Chief complaint codes and terminology should be clear and distinct to minimize ambiguity and ensure mutual understanding among informers, dispatchers, and field responders. Furthermore, code ordering should correspond to clinical urgency—for example, assigning code 1 to cardiac arrest to denote the highest priority—and be informed by national call frequency statistics to ensure evidence-based code organization.
Discussion
The findings of this study demonstrate that the revised EMTP-CBDC achieved “high to highest” levels of expert agreement across all evaluated domains following two rounds of the Delphi process. Importantly, this consensus reflects expert agreement on the clarity, appropriateness, and operational suitability of the protocol, rather than direct evidence of effectiveness or impact on dispatch performance or patient outcomes. Delphi-based consensus represents a critical preparatory step, indicating that a protocol is acceptable and ready for standardized implementation prior to outcome-based evaluation.
The observed expert agreement is consistent with principles underlying established international dispatch systems. For example, Clawson et al reported that structured dispatch systems such as the Medical Priority Dispatch System (MPDS) promote consistency and standardization when supported by appropriate training.22 Similarly, Eberhard et al demonstrated that structured telephone CPR instructions improve outcomes in out-of-hospital cardiac arrest; however, such outcome improvements were derived from implementation and observational studies rather than expert consensus alone.23 In this context, the present study does not claim effectiveness but rather establishes that the revised EMTP-CBDC is considered suitable and applicable by multidisciplinary experts for use in emergency medical dispatch settings.
The findings also highlight system-level considerations relevant to Thailand’s EMS context. Expert feedback underscored limitations in the existing dispatch framework, including inconsistent coding structures and variability in urgency prioritization, which have been previously associated with misclassification and inefficiencies in emergency response systems.24 Studies by O’Hara et al further suggest that dispatcher cognitive load, stress, and uncertainty can contribute to deviations from protocolized decision-making.25 The EMTP-CBDC’s emphasis on structured symptom prioritization and standardized communication may help address these challenges; however, its actual impact on dispatch accuracy, efficiency, or patient outcomes must be evaluated through prospective field implementation studies.
Overall, the strong national expert consensus achieved in this study supports the EMTP-CBDC as a standardized and operationally suitable framework for emergency medical dispatch in Thailand. This consensus provides a necessary foundation for subsequent implementation research, system-level evaluation, and outcome validation.
Policy Implications and Future Directions
The policy considerations arising from this study should be interpreted as future directions informed by expert consensus, rather than direct empirical outcomes of the Delphi process. First, the establishment of a national standard for dispatch coding remains a critical system objective. Adoption of a unified, symptom-based dispatch code across all centers would support consistency and facilitate nationwide quality monitoring, including assessments of over-triage and under-triage in line with ACS-COT recommendations.26
Second, while structured telephone CPR protocols are widely supported by international evidence and guidelines, including the AHA 2025 recommendations,27 their integration within the EMTP-CBDC framework represents a policy and implementation priority rather than a demonstrated outcome of the present study. Future evaluations should examine dispatcher adherence, time to first chest compression, and patient-centered outcomes following implementation.
Third, recommendations regarding decision support systems (DSS) and artificial intelligence–assisted dispatch should be regarded as forward-looking strategies. Although emerging evidence from high-income settings suggests that advanced computerized dispatch systems may reduce cognitive burden and enhance consistency,28,29 empirical evaluation is required to determine their feasibility, safety, and effectiveness within Thailand’s EMS infrastructure.
Finally, continued investment in dispatcher training and competency development remains essential. Simulation-based education and structured performance monitoring are recommended to support effective implementation of the EMTP-CBDC and to ensure that consensus-based protocols translate into consistent real-world practice.30
Limitations
Although this study successfully gathered expert opinions from all health regions across Thailand and achieved consensus on all aspects of the EMTP-CBDC, several limitations should be noted when interpreting the findings. First, the two-round Delphi technique relied on the perspectives of selected experts based on their qualifications and experience, which may have introduced expert bias related to specific experiences or regional differences. Although recruiting participants from all 13 health regions improved representativeness, the sample may not fully reflect the perspectives of all practitioner levels, such as volunteer responders or local communication officers, who play critical roles in field operations. Second, this evaluation focused primarily on the theoretical “appropriateness and clarity of contents” rather than on-field effectiveness. Further studies are required to validate the accuracy and consistency of codes and their impact on patient outcomes through field-based assessments. Additional analyses should also evaluate inter-rater reliability and response time efficiency, especially when applying the DSS, which may produce outcomes different from human judgment.31 Third, using a mean score ≥3.41 as proposed by Best (1986) was appropriate for qualitative research but does not fully capture the degree of statistical agreement. Future studies could employ more rigorous measures, such as Kendall’s coefficient of concordance (W) or Cronbach’s α, to strengthen the reliability of the findings.32 Lastly, the limited study duration—comprising an eight-hour meeting and two Delphi rounds—restricted opportunities for in-depth discussion, particularly regarding complex chief complaint codes, such as cardiac arrest from specific causes or mass casualty incidents. Future research should include workshops or follow-up validations through simulations and real dispatch settings to confirm long-term applicability and accuracy.24 Pilot implementation studies are also recommended to evaluate the revised EMTP-CBDC’s impact on response times, triage accuracy, patient outcomes, and resource management within EMS systems at both provincial and national levels.
Conclusion
This research and development study employed a two-round Delphi process to obtain nationwide expert consensus on the improvement and refinement of the EMTP-CBDC to ensure appropriateness, clarity, and alignment with real-world practice. The findings reveal that expert agreement levels ranged from “high” to “the highest” across all components, including structure, pre-arrival instructions, emergency medical conditions, injuries, telephone-assisted instructions, application, and patient triage, as well as code appropriateness. These results highlight the EMTP-CBDC’s potential to serve as the central standard tool for Thailand’s emergency medical system. Moreover, the study emphasizes key strategies for advancing the national EMS system, including the establishment of a national dispatch coding standard, mandatory implementation of telephone CPR in accordance with the AHA guidelines, integration of a DSS to enhance dispatcher decision-making, and the adoption of ESI mapping to ensure care continuity. In conclusion, the developed EMTP-CBDC demonstrates strong potential to improve Thailand’s emergency medical command system by promoting systematic, transparent, and efficient management of emergency response, resource allocation, and communication between dispatch centers and operation units, ultimately contributing to reduced morbidity and mortality from emergency medical conditions nationwide.
Data Sharing Statement
The datasets are available from the corresponding author with reasonable request.
Ethics Approval and Consent to Participate
The study complied with the principles of the 1975 Declaration of Helsinki and its 2000 revisions. Ethical approval was obtained from the Institutional Review Board of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University (COA no. 065/2567). Participant information was kept strictly confidential, with data reported in aggregate form. The study posed no harm to participants, and written informed consent was obtained after full disclosure of study details and objectives.
Acknowledgments
The authors wish to express their sincere gratitude to the National Institute for Emergency Medicine for funding the development of the EMTP-CBDC, and to the Navamindradhiraj University Research Fund for its generous support of this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Navamindradhiraj University Research Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lincoln EW, Reed-Schrader E, Jarvis JL. EMS Quality Improvement Programs. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.; 2024.
2. Haugland H, Uleberg O, Klepstad P, Krüger A, Rehn M. Quality measurement in physician-staffed emergency medical services: a systematic literature review. Int J Qual Health Care. 2019;31(1):2–10. doi:10.1093/intqhc/mzy106
3. Voskens FJ, van Rein EAJ, van der Sluijs R, et al. Accuracy of prehospital triage in selecting severely injured trauma patients. JAMA Surg. 2018;153(4):322–327. doi:10.1001/jamasurg.2017.4472
4. Olola C, Scott G, Gardett I, Clawson JJ, Broadbent M. Comparison of emergency medical dispatcher stroke identification and paramedic on-scene stroke assessment. Ann Emerg Dispatch Response. 2017;5(1):6–10.
5. Clawson JJ, Scott G, Gardett I, et al. Predictive ability of an emergency medical dispatch stroke diagnostic tool in identifying hospital-confirmed strokes. J Stroke Cerebrovasc Dis. 2016;25(8):2031–2042. doi:10.1016/j.jstrokecerebrovasdis.2016.04.021
6. Oman G, Bury G. Use of telephone CPR advice in Ireland: uptake by callers and delays in the assessment process. Resuscitation. 2016;102:6–10. doi:10.1016/j.resuscitation.2016.02.006
7. Tanner R, Masterson S, Jensen M, et al. Out-of-hospital cardiac arrests in the older population in Ireland. Emerg Med J. 2017;34(10):659–664. doi:10.1136/emermed-2016-206041
8. Dicker B, Davey P, Smith T, Beck B. Incidence and outcomes of out-of-hospital cardiac arrest: a New Zealand perspective. Emerg Med Australas. 2018;30(5):662–671. doi:10.1111/1742-6723.12966
9. Nehme Z, Andrew E, Smith K. Factors influencing the timeliness of emergency medical service response to time critical emergencies. Prehosp Emerg Care. 2016;20(6):783–791. doi:10.3109/10903127.2016.1164776
10. Baabdullah M, Faden H, Alsubhi R, Almalki A, Masri B, Alharbi A. The efficiency of the medical priority dispatch system in improving patient outcomes. SJEMED. 2020;1(2):110–120. doi:10.24911/SJEMed/72-1586163179
11. Ellensen EN, Wisborg T, Hunskaar S, Zakariassen E. Dispatch guideline adherence and response interval-a study of emergency medical calls in Norway. BMC Emerg Med. 2016;16(1):40. doi:10.1186/s12873-016-0105-2
12. Hoikka M, Länkimäki S, Silfvast T, Ala-Kokko TI. Medical priority dispatch codes-comparison with National Early Warning Score. Scand J Trauma Resusc Emerg Med. 2016;24(1):142. doi:10.1186/s13049-016-0336-y
13. Fire and Disaster Management Agency (FDMA), Ministry of Internal Affairs and Communications. Emergency medical system in Japan. Tokyo: FDMA; 2020. Available from: https://www.fdma.go.jp/en/post1.html.
14. Riyapan S, Chantanakomes J, Ruangsomboom O, et al. Assessment of prehospital management of patients transported to a Thai University hospital. Siriraj Med J. 2020;72(4):287–295. doi:10.33192/Smj.2020.39
15. National Institute for Emergency Medicine. Emergency Medical Act B.E. 2551 [Internet]. [cited 2024 Feb 10]. Available from: https://www.niems.go.th/1/SubWebsite/?id=38.
16. Monsomboon A, Chantawatsharakorn P, Suksuriyayothin S, et al. Prevalence of emergency medical service utilisation in patients with out-of-hospital cardiac arrest in Thailand. Emerg Med J. 2016;33:213–217. doi:10.1136/emermed-2015-204818
17. Sutham K, Khuwuthyakorn P, Thinnukool O. Thailand medical mobile application for patients triage base on criteria based dispatch protocol. BMC Med Inform Decis Mak. 2020;20(1):66. doi:10.1186/s12911-020-1075-6
18. Huabbangyang T, Sangketchon C, Ittiphisit S, Uoun K, Saumok C. Predictive factors of outcome in cases of out-of-hospital cardiac arrest due to traffic accident injuries in Thailand; a National Database Study. Arch Acad Emerg Med. 2022;10(1):e64. doi:10.22037/aaem.v10i1.1700
19. National Institute for Emergency Medicine. Criteria for Emergency Patient Triage and Prioritization of Care: symptom Group 26 – coronavirus Disease 2019 (COVID-19), B.E. 2565 [Internet]. [cited 2025 Oct 12]. Available from: https://www.niems.go.th/1/UploadAttachFile/2023/EBook/417975_20230519130242.pdf.
20. Huabbangyang T, Thepmanee D, Buaprasert P, Chansomboon P, Sri-On J, Rojsaengroeng R. Content validity assessment of a newly developed emergency medical dispatch and triage protocol in Thailand. J Clin Med. 2025;14(19):7125. doi:10.3390/jcm14197125
21. Best JW, Kahn JV. Research in Education (9th Ad.). New Delhi: Prentice Hall of India Private Limited; 2007.
22. Clawson JJ, Dernocoeur KB. Principles of Emergency Medical Dispatch.
23. Eberhard KE, Linderoth G, Gregers MCT, Lippert F, Folke F. Impact of dispatcher-assisted cardiopulmonary resuscitation on neurologically intact survival in out-of-hospital cardiac arrest: a systematic review. Scand J Trauma Resusc Emerg Med. 2021;29(1):70. doi:10.1186/s13049-021-00875-5
24. Heward A, Damiani M, Hartley-Sharpe C. Does the use of the advanced medical priority dispatch system affect cardiac arrest detection? Emerg Med J. 2004;21(1):115–118. doi:10.1136/emj.2003.006940
25. O’Hara R, Johnson M, Siriwardena AN, et al. A qualitative study of systemic influences on paramedic decision making: care transitions and patient safety. J Health Serv Res Policy. 2015;20(1 Suppl):45–53. doi:10.1177/1355819614558472
26. Newgard CD, Fischer PE, Gestring M, et al. National guideline for the field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2021. J Trauma Acute Care Surg. 2022;93(2):e49–e60. doi:10.1097/TA.0000000000003627
27. Hirsch KG, Amorim E, Coppler PJ, et al. Part 11: post-cardiac arrest care: 2025 American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2025;152(16_suppl_2):S673–s718. doi:10.1161/CIR.0000000000001375
28. Ventura CAI, Denton EE, David JA. Artificial intelligence in emergency trauma care: a preliminary scoping review. Med Devices. 2024;17:191–211. doi:10.2147/MDER.S467146
29. Binks F, Wallis LA, Stassen W. The triage performance of emergency medical dispatch prioritisation compared to prehospital on-scene triage in the Western Cape Province of South Africa. BMC Emerg Med. 2025;25(1):42. doi:10.1186/s12873-025-01198-9
30. Wayne DB, Didwania A, Feinglass J, Fudala MJ, Barsuk JH, McGaghie WC. Simulation-based education improves quality of care during cardiac arrest team responses at an academic teaching hospital: a case-control study. Chest. 2008;133(1):56–61. doi:10.1378/chest.07-0131
31. Dami F, Golay C, Pasquier M, Fuchs V, Carron PN, Hugli O. Prehospital triage accuracy in a criteria based dispatch centre. BMC Emerg Med. 2015;15:32. doi:10.1186/s12873-015-0058-x
32. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459–467. doi:10.1002/nur.20199
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.