Back to Journals » Psychology Research and Behavior Management » Volume 12
“Was it real or did I imagine it?” Perfectionistic beliefs are associated with dissociative absorption and imaginative involvement in obsessive-compulsive disorder
Received 22 April 2019
Accepted for publication 6 July 2019
Published 1 August 2019 Volume 2019:12 Pages 603—607
DOI https://doi.org/10.2147/PRBM.S212983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Andrea Pozza, Davide Dèttore
Department of Health Sciences, University of Florence, Florence, Italy
Background and objectives: In the literature there are inconsistent data regarding the role of dissociation in OCD. No study explored the association between obsessive beliefs and dissociative symptoms in OCD. It is important to understand which clinical factors are related to dissociation in OCD as more severe dissociative symptoms, particularly absorption, have been found to be predictors of treatment non-response. In the present short report we describe the results of an exploratory study aimed to investigate the role of the obsessive beliefs as predictors of the different dissociative symptoms controlling for anxiety and OCD severity in a group of OCD patients.
Methods: Sixty treatment-seeking patients consecutively referred to psychiatric services were included (mean age=31.17 years, 53.30% females). The Dissociative Experiences Scale-II, the Obsessive Beliefs Questionnaire-46, the Yale-Brown Obsessive-Compulsive Scale, and the Beck Anxiety Inventory were administered.
Results: Higher anxious symptoms predicted higher Dissociative Amnesia, Depersonalization/Derealization, and Absorption/Imaginative Involvement. Higher OCD severity predicted higher Dissociative Amnesia. More severe Perfectionism predicted higher Absorption/Imaginative Involvement.
Conclusion: Perfectionism in OCD patients may be associated with a higher tendency to absorption and imaginative involvement. Future research should explore whether a psychotherapeutic intervention on perfectionism might improve the outcomes of the OCD patients with higher absorption tendencies.
Keywords: obsessive-compulsive disorder, obsessive beliefs, dissociative symptoms, perfectionism, reality monitoring
Introduction
Dissociation encompasses a set of distinct symptoms such as Amnesia (eg, getting somewhere without remembering how you arrived), Depersonalization/Derealization (eg, looking in the mirror and not recognizing oneself, or perceive the environment as behind a glass), and Absorption/Imaginative Involvement (eg, immersion in an external/internal stimulus like a thought resulting in disconnection from the reality).1 The role of dissociation in OCD is equivocal as the current data are inconsistent. Some studies focused on the relation between dissociation and OCD severity: in some of them OCD patients experiencing stronger dissociation had higher OCD severity,2 whereas other studies did not find this result.3 These conflicting findings may be due to the fact that the different dissociative features are differently associated with OCD severity. Absorption and amnesia have been found to be more strongly related to OCD symptoms than Depersonalization/Derealization, despite this evidence was found only in non-clinical samples.4 Less confidence in reality monitoring and stronger memory distrust might be a reason why dissociative symptoms are sometimes present in OCD.5
The role of the obsessive beliefs as vulnerability/maintenance factors in OCD is well-established. These include Overestimation of Threat/Inflated Sense of Responsibility (beliefs regarding the probability of occurrence of a feared event and responsibility for preventing/avoiding its negative outcomes); Importance/Control of Thoughts (beliefs that a thought has the same potential as the actual action imagined, that leads the individuals to perceive their thoughts as extremely important, consequently determining thought control strategies); Perfectionism/Intolerance of Uncertainty (the need to succeed/avoid failure leads OCD patients to set unrelenting standards).6
In the literature, no study explored the association between obsessive beliefs and dissociative symptoms. It is important to understand which clinical factors may be related to dissociation in OCD as more severe dissociative symptoms, particularly absorption, have been found to be predictors of treatment non-response.7 Therefore, in the present short report we describe the results of an exploratory study aimed to investigate the role of the obsessive beliefs as predictors of the different dissociative symptoms controlling for anxiety and OCD severity in a group of OCD patients.
Method
Participants and procedure
Eligibility criteria were having a primary OCD diagnosis and 18–65 year-old age. Exclusion criteria were psychosis, mental retardation, neurological disorders. Sixty treatment-seeking patients consecutively referred to psychiatric services were included (Table 1). Participation was voluntary and uncompensated. All the participants provided written informed consent. Materials containing personal information about participants were kept on electronic supports protected by passwords. In line with the Helsinki Declaration, the study was approved by the Institutional Ethics Committee of the University of Florence.
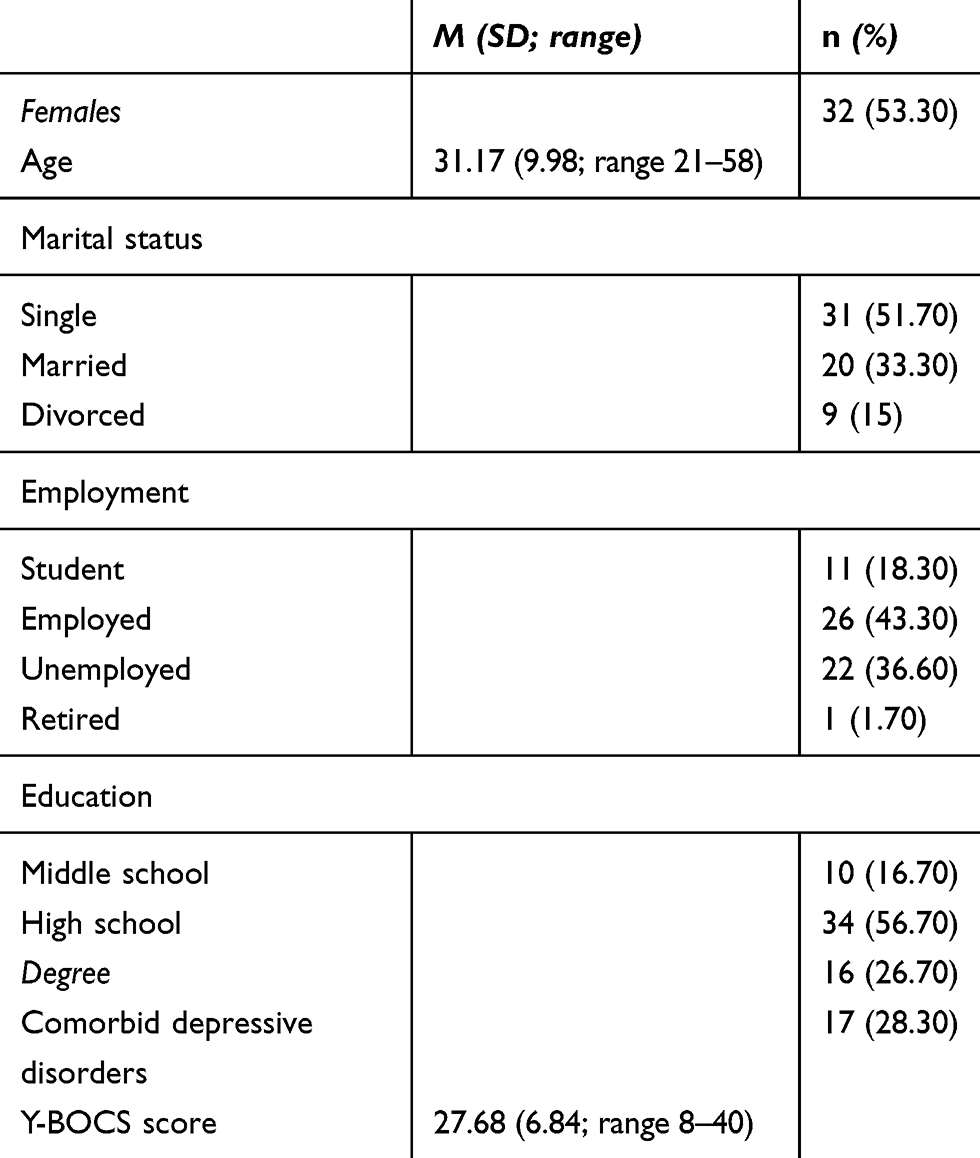 |
Table 1 Sociodemographic and clinical characteristics of the OCD group (n=60) |
Measures
OCD diagnoses were assessed through the Structured Clinical Interview for DSM-IV-TR Axis I Disorders. The official authorized Italian translation of the interview reported in the manual of Mazzi et al8 was used. Comorbid personality disorders were screened by the Structured Clinical Interview for DSM-IV-TR Personality Disorders. The Dissociative Experiences Scale-II (DES-II),1 a 28-item questionnaire on a 11-point scale, was used to assess dissociative symptoms. Three subscales are calculated: Absorption and Imaginative Involvement, Amnesia and Depersonalization/Derealization. It showed excellent reliability. In the present study the official authorized translation reported in Schimmenti et al9 was used and its internal consistency was good for all the subscales. The Obsessive Beliefs Questionnaire-46 (OBQ-46),8 a 46-item questionnaire on a 7-point scale was used to evaluate the obsessive beliefs: Perfectionism, Responsibility for Harm, Control of Thoughts, Responsibility for Omission, Importance of Thoughts. The OBQ-46 presented good internal consistency and the official authorized version is reported in Dorz et al.8 In the present study, internal consistency was good for all the scales. The Yale-Brown Obsessive-Compulsive Scale (Y-BOCS),10 a 10-item interview, was used to assess OCD severity. Higher scores suggest more severe symptoms. It showed excellent reliability.11 The official authorized Italian translation of the scale reported in Hénin12 was used. The Beck Anxiety Inventory (BAI),8 a 21-item questionnaire, was used to assess anxiety symptoms. It showed excellent internal consistency.13 The official authorized Italian translation of the questionnaire reported in Sica et al14 was used. In the present study internal consistency was good.
Statistical analysis
In a first step, partial correlation coefficients were calculated between the scores on the OBQ-46 scales and those on the DES-II controlling for the BAI and Y-BOCS scores. These coefficients were interpreted as follows: 0<r<|0.30|=weak; |0.30|<r<|0.50|= moderate; |0.50|<r<|0.70|= strong; r>|0.70|= very strong. A series of multiple linear regression analyses were conducted entering dissociative symptoms as outcomes by the stepwise procedure and obsessive beliefs, OCD symptoms and anxiety as predictors. The data analysis was conducted using the SPSS software version 21. The significance level was set at p<0.05.
Results
Partial correlation coefficients showed that among the OBQ-46 scales only the scores on the OBQ-46 Perfectionism scale significantly and moderately correlated with the scores on the DES-II subscale, specifically the DES-II Absorption and Imaginative Involvement subscale controlling for the BAI and Y-BOCS scores (Table 2). Higher BAI and Y-BOCS scores predicted higher scores on the DES-II Dissociative Amnesia subscale (R2=0.20). Higher BAI scores predicted higher DES-II Depersonalization/Derealization subscale (R2=0.17). Higher BAI and OBQ-46 Perfectionism scores predicted higher scores on the DES-II Absoprtion and Imaginative Involvement subscale (R2=0.17). No significant effects of the scores on the other predictors emerged. The results of the regression analyses are presented in Table 3.
 |
Table 2 Partial correlations between the DES-II scores and the OBQ-46 scores controlling for BAI and Y-BOCS scores in the OCD group (n=60) |
 |
Table 3 Multiple linear regression analyses of the DES-II scores in the OCD group (n=60) |
Discussion
Previous research showed that amnesia and absorption are dissociative symptoms more strongly associated with OCD symptoms than Depersonalization/Derealization.4 The present exploratory study is the first contribution exploring the association between obsessive beliefs and dissociative symptoms in a group of OCD patients controlling for anxiety and OCD severity. Our findings showed that patients with more severe anxious and OCD symptoms reported more intense amnesia simptoms. This result appears consistent with previous data showing that memory distrust is one of the dissociative symptoms related to OCD severity.5 Consistent with O’Connor and Aardema’s observations,11 it may be that those patients experiencing higher levels of anxiety and more frequent obsessions/compulsions have higher proneness to losing sense of time due to the distracting effects of symptoms. Alternatively, they may be less confident about their capacity to remember whether or not they have done something, a mechanism that might reinforce the obsessional doubt.
Patients with higher anxiety experienced more severe Depersonalization/Derealization symptoms. This result was in line with previous research12 and suggests that Depersonalization/Derealization may be a mental anxiety symptom cluster that needs for a careful psychotherapeutic work in clinical practice. Enteroceptive exposure may be used in combination with the gold standard technique for OCD, exposure and response prevention, to reduce Depersonalization/Derealization feelings. More intense anxious symptoms and more severe perfectionistic beliefs predicted stronger absorption/imaginative involvement. It may be that perfectionism imposes unrelenting standards to the individual about the importance of an extracareful reality monitoring that in turn reinforces the doubt whether or not something was real. Alternatively, absorption/imaginative involvement may be a coping strategy adopted by OCD patients to anticipate potential dangers in order to meet their needs to succeed and/or avoid failure.
Some limitations should be pointed out. Future research should expand the sample size. In addition, the regression models explained a proportion of variance ranging from 17% to 20%. This point suggests that a future work should investigate additional predictors. Moreover, future research should investigate the potential role of perfectionism as mediator of OCD severity/anxiety on dissociative symptoms. Finally, given the frequently observed association between depressive symptoms and OCD,13 a measure of depression should be introduced to control for depressive symptoms in the same way as for anxiety and OCD severity.
In conclusion, the present exploratory study demonstrates that perfectionistic beliefs are associated with dissociative absorption/imaginative involvement in OCD. Perfectionism in OCD patients may be associated with a higher tendency to absorption or imaginal involvement. Clinical work with OCD patients reporting absorption/imaginative involvement might benefit from an intervention on perfectionism. However, whether this may be a promising strategy to improve clinical practice should be supported by additional research assessing treatment effects and mechanisms of change.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Carlson EB, Putnam FW. An update on the dissociative experiences scale. Dissociation. 1993;6:16–27.
2. Belli H, Ural C, Vardar MK, Yesılyurt S, Oncu F. Dissociative symptoms and dissociative disorder comorbidity in patients with obsessive-compulsive disorder. Compr Psychiatry. 2012;53:975–980. doi:10.1016/j.comppsych.2012.02.004
3. Lochner C, Seedat S, Hemmings SM, et al. Dissociative experiences in obsessive-compulsive disorder and trichotillomania: clinical and genetic findings. Compr Psychiatry. 2004;45:384–391. doi:10.1016/j.comppsych.2004.03.010
4. Aardema F, Wu KD. Imaginative, dissociative, and schizotypal processes in obsessive‐compulsive symptoms. J Clin Psychol. 2011;67:74–81. doi:10.1002/jclp.20729
5. Hermans D, Engelen U, Grouwels L, Joos E, Lemmens J, Pieters G. Cognitive confidence in obsessive-compulsive disorder: distrusting perception, attention, and memory. Behav Res Ther. 2008;46:98–113. doi:10.1016/j.brat.2007.11.001
6. Pozza A, Dèttore D. Are inflated responsibility beliefs specific to OCD? Meta-analysis of the relations of responsibility to OCD, anxiety disorders, and depression symptoms. Clin Neuropsychiatry. 2014;11:170–181.
7. Rufer M, Held D, Cremer J, et al. Dissociation as a predictor of cognitive behavior therapy outcome in patients with obsessive-compulsive disorder. Psychother Psychosom. 2006;75:40–46. doi:10.1159/000089225
8. Mazzi F, Morosini P, De Girolamo G, Lussetti M Guaraldi GP. SCID-I: Structured Clinical Interview for DSM-IV Axis I Disorders (Italian edition). Firenze: Giunti OS; 2000.
9. Schimmenti A. Dissociative experiences and dissociative minds: exploring a nomological network of dissociative functioning. J Trauma Dissociation. 2016;17:338–361.
10. Beck AT, Steer RA. Beck Anxiety Inventory Manual. San Antonio, TX: The Psychological Corporation Harcourt Brace Company; 1990.
11. O’Connor K, Aardema F. Living in a Bubble dissociation, relational consciousness, and obsessive compulsive disorder. J Consciousness Stud. 2012;19:216–246.
12. Hénin M. Yale-brown obsessive-compulsive scale. In: Sica C, editor. Disturbo ossessivo-compulsivo. questionari e interviste per la valutazione clinica. Trento: Erickson; 2012:91–120.
13. Pozza A, Coradeschi D, Dèttore D. Do dysfunctional beliefs moderate the negative influence of comorbid severe depression on outcome of residential treatment for refractory OCD? A pilot study. Clin Neuropsychiatry. 2013;10:72–83.
14. Sica C, Coradeschi D, Ghisi M, Sanavio E. Beck Anxiety Inventory. Adattamento italiano: manuale. Firenze: Organizzazioni Speciali; 2006.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.