Back to Journals » Clinical Ophthalmology » Volume 20
Laughter Exercise for Symptomatic Improvement in Dry Eye Following Cataract Surgery: A Randomized Controlled Trial
Authors Tan Y ![]() , Qin D
, Qin D ![]() , Zhou Y, Ru Y
, Zhou Y, Ru Y ![]() , Song X
, Song X ![]()
Received 2 November 2025
Accepted for publication 25 March 2026
Published 7 April 2026 Volume 2026:20 578499
DOI https://doi.org/10.2147/OPTH.S578499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sotiria Palioura
Yuehong Tan, Danyan Qin, Yi Zhou, Yan Ru, Xinxin Song
Department of Nursing, Shanghai Eye Hospital Shanghai Eye Diseases Prevention and Treatment Center, Tongji University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Danyan Qin, Email [email protected]
Background: The effectiveness of laughter exercise in dry eye disease (DED) remains uncertain. This study aimed to evaluate the efficacy and safety of laughter exercise in patients with DED who had undergone cataract surgery.
Methods: This was a parallel-group, randomized controlled trial. A total of 72 participants were randomly assigned to either the laughter exercise group (n=36) or the control group (n=36). Participants in the intervention group performed guided laughter exercises four times a day for 4 weeks. Outcomes were measured preoperatively and at 1, 4, and 12 weeks postoperatively. The primary outcome was the mean change in dry eye symptom scores. Secondary outcomes included tear meniscus height, tear break-up time, health status scores (both physical (PCS) and mental (MCS) component summaries), intervention participation, satisfaction, and incidence of adverse events.
Results: Repeated measures ANOVA was used to analyze dry eye symptom scores. The results showed a significant group×time interaction (P< 0.001). This indicates that the change in dry eye symptom scores in the laughter exercise group was better than that in the control group. Among the secondary outcomes, a significant group×time interaction was also found in the health status scores (both PCS and MCS) (all P< 0.001). Over time, the health status scores of the laughter exercise group improved more than those of the control group. For other secondary outcomes, such as tear meniscus height and tear break-up time, there were no significant differences (P> 0.05). No adverse events were observed in either group.
Conclusion: Laughter exercises can relieve dry eye symptoms in patients who have undergone cataract surgery and improve their physical and mental health. Although this therapy has no significant effect on improving objective clinical symptoms, it can be a safe and effective adjuvant treatment.
Keywords: laughter exercise, dry eye disease, randomized controlled trial, effect analysis
Introduction
Cataract surgery has become increasingly common due to an aging population.1 Dry eye disease (DED) is a common complication following cataract surgery; symptoms include dryness, foreign body sensation, eye fatigue, and decreased tear breakup time.2 The cause of DED after cataract surgery remains unclear and may be due to direct damage from eye surface manipulation and indirect injury from inflammation.3 A 2022 systematic review and meta-analysis of 36 DED studies found that 37.4% of patients without pre-existing DED developed DED after cataract surgery.4 The peak of DED severity occurred 1 day after cataract surgery. It lasts for at least one month and, in some cases, up to 12 months.4 Patients with DED mainly want to relieve eye discomfort and feel more comfortable, which is what they hope to achieve when seeking medical help.
Artificial tears (ATs) are the primary treatment for patients with DED. In fact, 81% of them use ATs as their first treatment.5 ATs mimic the function of natural tears, helping improve tear stability and lubricate the eye surface.6 DED not only affects patients’ quality of life but also imposes a significant economic burden, especially for long-term AT users.7 However, ATs do not always fully relieve all DED symptoms and signs.8 One study surveyed 100 eye care providers; 86% reported that 20% or more of their patients experienced treatment failure with ATs alone, due to either intolerance to the medicine or ineffective relief of eye symptoms.5 Therefore, there is a need for more effective, easily accessible treatment methods.
Several studies have reported a correlation between DED and mental illnesses such as depression and anxiety.9–11 Depression and anxiety are more common in patients with DED. DED has gradually become a biopsychosocial problem. Physicians are paying more attention to the emotional and mental states of patients with DED.12 There is a saying: Laughter is the best medicine. Research shows that laughter may decrease stress hormone levels and reduce the impact of stress on the immune system.13,14 As a result, it can effectively relieve stress, depression, and anxiety in the user. Laughter therapy is a new non-drug psychological treatment. It has gradually attracted the attention of medical staff. Laughter therapy typically involves triggering laughter through stimuli, including includes laughter exercises using humor, such as watching humorous videos or seeing clowns.15 Therefore, can laughter therapy provide therapeutic benefits for DED?
A randomized controlled trial explored the therapeutic potential of laughter therapy in patients with dry eye. These patients had not undergone ophthalmic surgery or experienced eye trauma in the previous 12 months.16 When it came to relieving the subjective symptoms of patients with dry eye disease, laughter exercise was as good as 0.1% sodium hyaluronic acid. In other words, laughter exercises were not worse than this treatment. However, no relevant studies have explored the effectiveness and safety of laughter exercises in DED after cataract surgery. Therefore, in this trial, we aimed to determine whether laughter exercises could relieve discomfort from DED after cataract surgery. The intervention plan designed in this study is simple, low-cost, and easy to implement in clinical wards. This study is expected to provide a feasible non-pharmacological rehabilitation option for patients with postoperative dry eye. We hypothesized that participants who performed the laughter exercise would have greater improvements in their eye symptoms and quality of life than those who received usual care.
Methods
Setting and Design
This two-arm, randomized controlled trial was conducted at the Shanghai Eye Disease Prevention and Treatment Center and lasted for three months (see Figure 1). The study protocol was approved by the Ethics Committee of the Shanghai Eye Disease Prevention and Treatment Center (approval number: EC-20250307-02), registered with the Chinese Clinical Trial Registry (registration number: ChiCTR2500102758) on May 20, 2025, and all participants signed written informed consent after being fully informed of the study details. The trial was conducted in strict accordance with the ethical principles of the Declaration of Helsinki and registration protocol. Additional informed consent was obtained from all participants for the publication of their anonymized data.
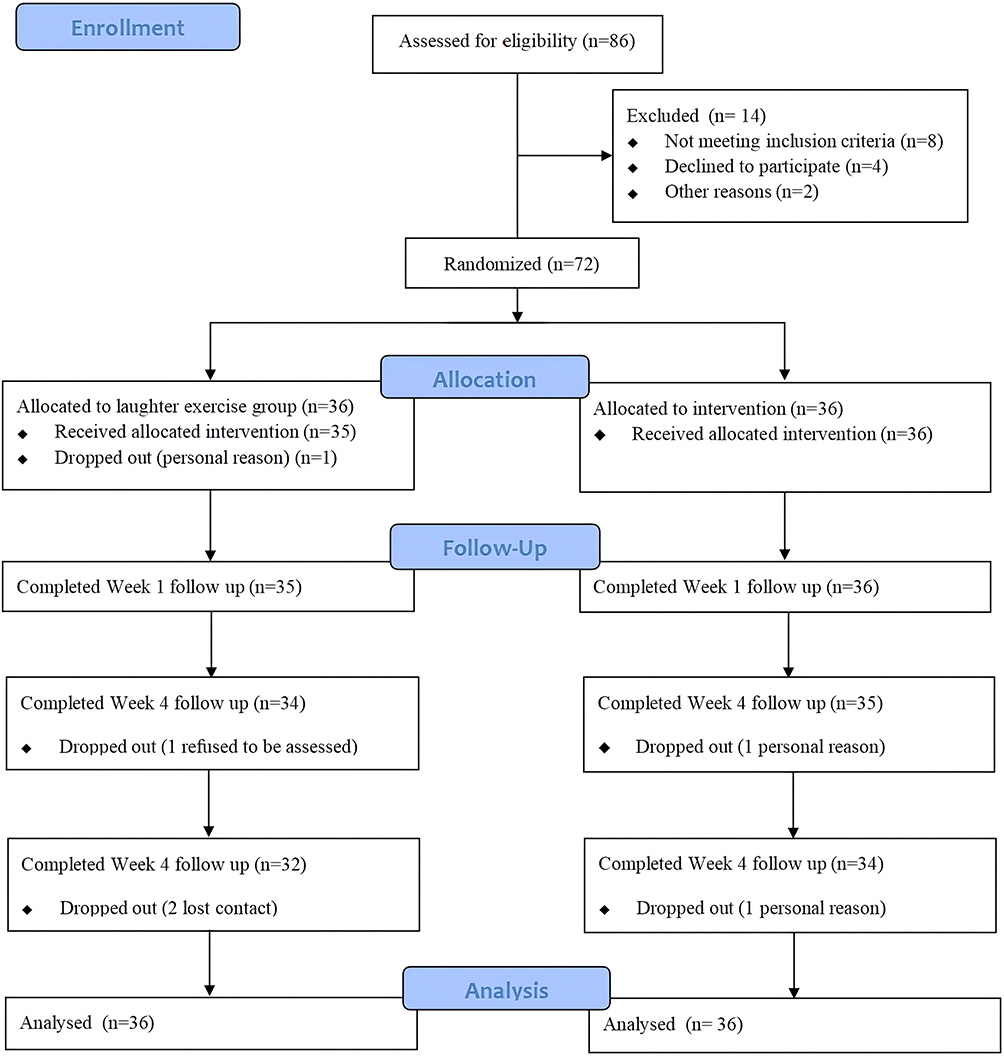 |
Figure 1 CONSORT Flow Diagram. |
Participants
Patients were recruited from the Shanghai Eye Disease Prevention and Treatment Center between May 1 and September 30, 2025. The responsible nurses recommended patients for recruitment. The inclusion criteria were as follows: (1) cataract surgery in one eye, with the other eye being normal. (2) Met the diagnostic criteria for DED according to the “Expert Consensus on Dry Eye Clinical Diagnosis and Treatment (2024)”.17 This involved a comprehensive assessment of subjective symptoms, objective examination results, and classification and grading. (3) No other severe eye or systemic diseases. (4) Willing to provide written informed consent. The exclusion criteria were as follows: (1) Use of medications affecting tear secretion function, such as antihistamines, antidepressants, or artificial tears, within 6 months. (2) History of ophthalmic surgery 6 months before cataract surgery. (3) Presence of a mental disorder. This included depression (scoring < 22 points on the SDS)18 or anxiety (scoring < 40 points on the SAS).19 (4) Had impaired cognitive functioning (scoring < 22 points on the Hong Kong version of the Montreal Cognitive Assessment).20
Interventions
Laughter Exercise Group
In the laughter exercise group, we instructed the patients to perform laughter exercises four times a day for four weeks. Six trained nurses led the laughter exercises. These nurses were trained in laughter therapy. They used consistent verbal cues and movement demonstrations in each session. Before the intervention, our team prepared a standard five-minute humorous video (Video S1). Starting in the first week after surgery, patients watched standard humorous videos with the guidance of their nurses. They practiced making vocalizations like “hee hee hee” and “hah hah hah”. We used observation checklists to record the amount of time each participant spent laughing. We considered that if a participant laughed audibly for at least 5 min, it counted as effective participation. During the intervention, the nurses in charge could use jokes or fun activities to help the patients perform the laughter exercises. In addition, participants watched humorous videos to ensure that the exercise was effective. Patients were required to check in four times a day to complete the exercise. After the patients were discharged, they received the intervention through online meetings.
Control Group
Patients in the control group received usual care. The schedule and duration were the same as those of the intervention group, to match the contact time between nurses and patients. Nurse-patient interactions can produce nonspecific effects. DED education instructors were trained registered nurses. The content of usual care included preoperative preparation, postoperative care, and discharge health guidance. During the intervention, each subject got a training handout about DED symptoms, causes, and daily care instructions. At the start, we allowed patients to share their symptoms. During later education, we answered and discussed patients’ questions about DED daily care. Finally, the instructors checked patients’ understanding of the DED education content.
We told subjects to follow these 5 preoperative preparation steps: (1) Check whether vital signs and chronic diseases like diabetes and hypertension were well-controlled. (2) Clean the eyelids and surrounding skin. Follow the instructions to use antibiotic eye drops to prevent infection. Also, explain the surgical cause, treatment plan, and purpose clearly to patients and their families to alleviate their anxiety and fear, and encourage them to keep a peaceful mindset. (3) Avoid getting a cold, cough, or other upper-respiratory-tract infections. (4) Do not rub your eyes on the day of surgery and follow the intraoperative cooperation requirements. (5) Ensure the surgical etiology, treatment plan, and purpose are clearly explained to patients and their families. There were 6 postoperative care steps: (1) Lie flat or slightly elevate your head. (2) Observe if the dressing is bleeding or exuding. Report it in time. (3) Keep your eye clean and dry. Avoid touching your eye with your hands. (4) Avoid putting pressure on your eye, violent coughing, straining to defecate, and bending down to pick up objects. (5) Have a light and easy - to - digest diet. Avoid spicy food. (6) Follow the instructions to correctly drop eye drops (antibiotics, hormones, or anti-inflammatory drugs). Pay attention to aseptic operation. There were also 5 discharge health guidance steps: (1) Avoid wetting the operated eye when washing your face or hair within 1 week after surgery. (2) Wear protective glasses or a sun hat when going out to protect your eyes from wind, sand, dust, and intense light. (3) Avoid putting pressure on your eyes when sleeping. (4) Follow the instructions to check your vision and eye pressure regularly. (5) If you have severe eye pain, vision loss, redness, tearing, or increased secretions, seek medical attention immediately.
Both patient groups followed the same eye-drop-use rules. All patients in both groups used the eye drops as prescribed by the doctor.
Randomization and Masking
An independent researcher made a table of random numbers using a computer. Another independent researcher sealed the treatment allocation labels in opaque, sequentially numbered envelopes. These envelopes were opened only after participants completed all baseline assessments and after ensuring allocation concealment. The statistician analyzing the data did not know the group allocation until the analysis was done. Outcome assessors were also unaware of the group allocation. We instructed them not to ask about the intervention participants received. We also reminded participants not to tell the assessors which group they were in. To ensure each group had a similar distribution of baseline characteristics, we conducted a post-randomization balance assessment.
Outcomes
Primary Outcome
The primary outcome was the change in the Chinese Dry Eye Symptoms Questionnaire score. This questionnaire assesses the severity of dry eye in three dimensions: medical history, precipitating factors, and ocular symptoms. It was carefully designed to fit the unique characteristics of China’s dry-eye population.21 The scale is a 12-item questionnaire using a 0–4 Likert scale. The total score ranges from 0 to 48 points; higher scores mean more severe dry-eye symptoms.22 The questionnaire has good internal consistency reliability. The Cronbach’s alpha was 0.794.21
Secondary Outcomes
The secondary outcomes were changes in scores on the physical and mental health subscales of the 36-item Short Form Health Survey (SF-36) and changes in DED signs, assessed by tear meniscus height and tear break-up time. The SF-36 is a popular tool for assessing quality of life. It contains 8 domains,23 which can be combined to form two higher-order summary scores: the physical component summary (PCS) and the mental component summary (MCS).24 The PCS score is calculated using a formula validated across four specific domains: physical function, role physical, bodily pain, and general health. In contrast, the MCS score is derived from the remaining four domains: mental health, vitality, social function, and role emotional.25 The PCS and MCS were chosen as primary variables because they have lower inherent variability than the individual domain scores. These scores assess the overall quality of life across both physical and psychological dimensions. Higher scores directly correlate with an enhanced health status. Many studies have shown that the SF-36 scale has good overall and dimensional reliability and validity.25–27 Tear meniscus height and tear break-up time were two other secondary outcomes. They were measured using the Gaush iDea eye-surface interferometer. The manufacturer is SBM Sistemi S.r.l., and the model is Gaush iDea Topo. The Gaush iDea eye-surface interferometer can automatically analyze and measure the tear meniscus height and tear break-up time. We repeated the measurement process three times and averaged the results.
We assessed the above primary and secondary outcomes preoperatively and 1, 4, and 12 weeks after cataract surgery. A research assistant conducted and analyzed specific assessments of the intervention. These included acceptability, engagement, and the record of adverse events. After the intervention, we used a 10-item self-compiled questionnaire (1–5 Likert scale) to assess patients’ acceptability of the laughter exercise. A total score of 35 or higher was considered satisfactory. In our study, we mainly assessed patients’ engagement through their intervention compliance. Patients who completed 80% of the laughter-exercise sessions via the mini-program were considered to have good compliance. Throughout the treatment period, we monitored adverse events (such as eye swelling, conjunctival hyperemia with stinging pain, dry eyes, fatigue, soreness of the periorbital muscles, headache, gastrointestinal discomfort, and blood-pressure fluctuations) at each visit. We used a standard adverse-event case-report form to document, at each visit, the type, severity, and relationship to the intervention of adverse events in patients.
Sample Size Calculation
The formula for sample size calculation using independent samples means comparison is employed to estimate the required sample size.

Here, Uɑ and Uβ represent the U-values corresponding to ɑ and β, δ denotes the difference between the two means, and σ is the combined standard deviation. To initially assess the preliminary findings, a slightly higher ɑ (ɑ=0.10) and moderate power (75%) were selected. As referenced in literature,16 the study employed the tear break-up time for measurement. The mean difference δ was 2.38, and the combined standard deviation σ was 4.38. With 36 cases per group and a 10% dropout rate, the final sample size was determined to be 40 per group, for a total of 80 participants.
Data Analysis
SPSS 26.0 was used for all statistical analyses. We examined differences in dry eye questionnaire scores and other secondary outcomes across time points between groups using a repeated-measures ANOVA. In this study, we performed an intention-to-treat (ITT) analysis. We adopted multiple imputation to handle missing data. We performed sensitivity analyses to assess the influence of imputation on intervention effects. We examined additional between-group comparisons without missing data using independent t-tests. For all analyses, two-tailed P-values of <0.05 were considered statistically significant.
Results
Participant Characteristics
In total, 72 participants were randomized. Table 1 shows that 49 (68.1%) participants were female, with a mean age of 67.28 (3.27) years. Moreover, over 60% of participants have more than 9 years of education. Baseline characteristics were well balanced between the two groups. More participants withdrew from the laughter exercise group (4/36, 11.1%) than from the control group (2/36, 5.6%), but the difference was not significant (chi-square test, P = 0.67).
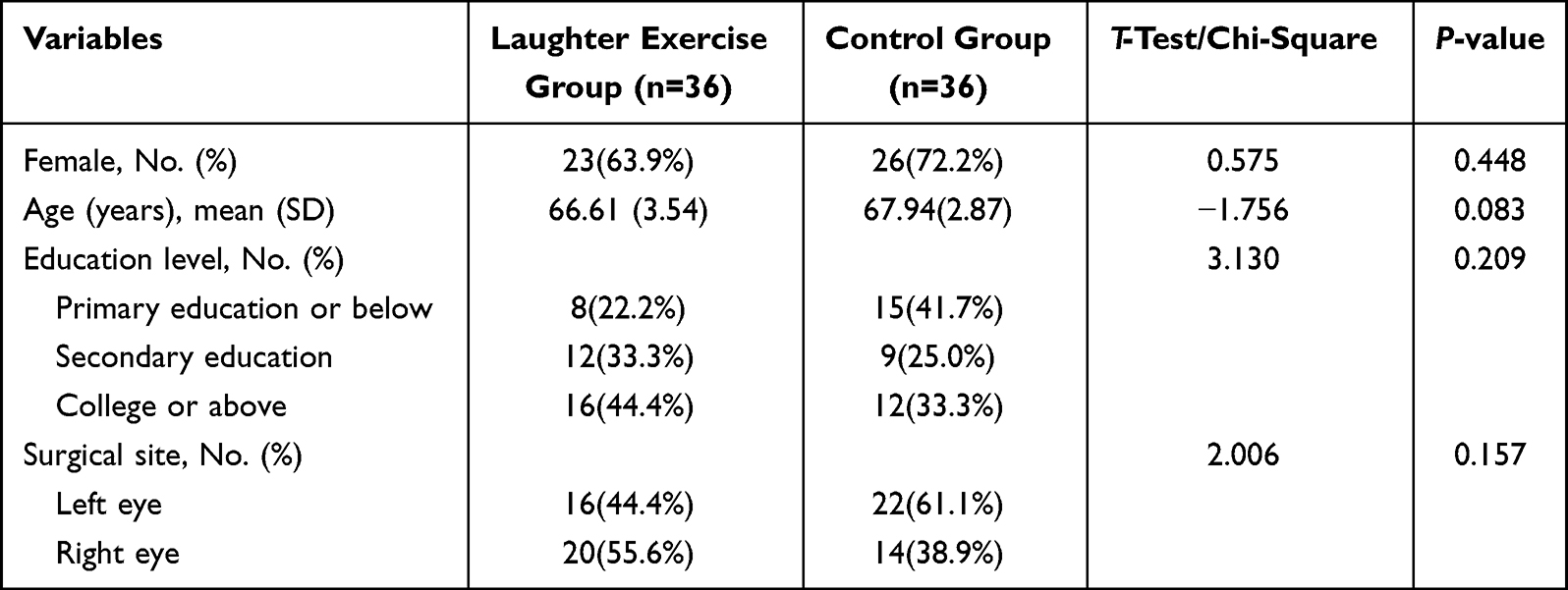 |
Table 1 Socio-Demographic of the Study Participants |
Intervention Compliance
In our study, almost all participants had good compliance. A total of 32 participants in the intervention group completed the research process and follow-up. In the control group, 34 participants did the same. Of the 36 participants in the intervention group, 35 (97.2%) practiced laughter exercises in 80% of the sessions. Moreover, 32 (88.9%) completed the follow-up visit. Based on the mini-program check-in records, the average number of times per day was 3.3, and the total number of times per week was 23.1. Based on participants’ feedback and daily monitoring by responsible nurses, almost all participants in the control group followed at least half of the instructions during the 4 weeks.
Effectiveness
Primary Outcome
In our study, dry eye symptom scores of the two groups have improved over time postoperatively (P<0.001). Moreover, significant interactions between groups and assessment time points were observed in the dry eye symptom scores of the intervention group (P<0.001; Figure 2). Compared with the control group, the laughter exercise group showed significantly greater improvements in dry eye symptom scores (see Table 2).
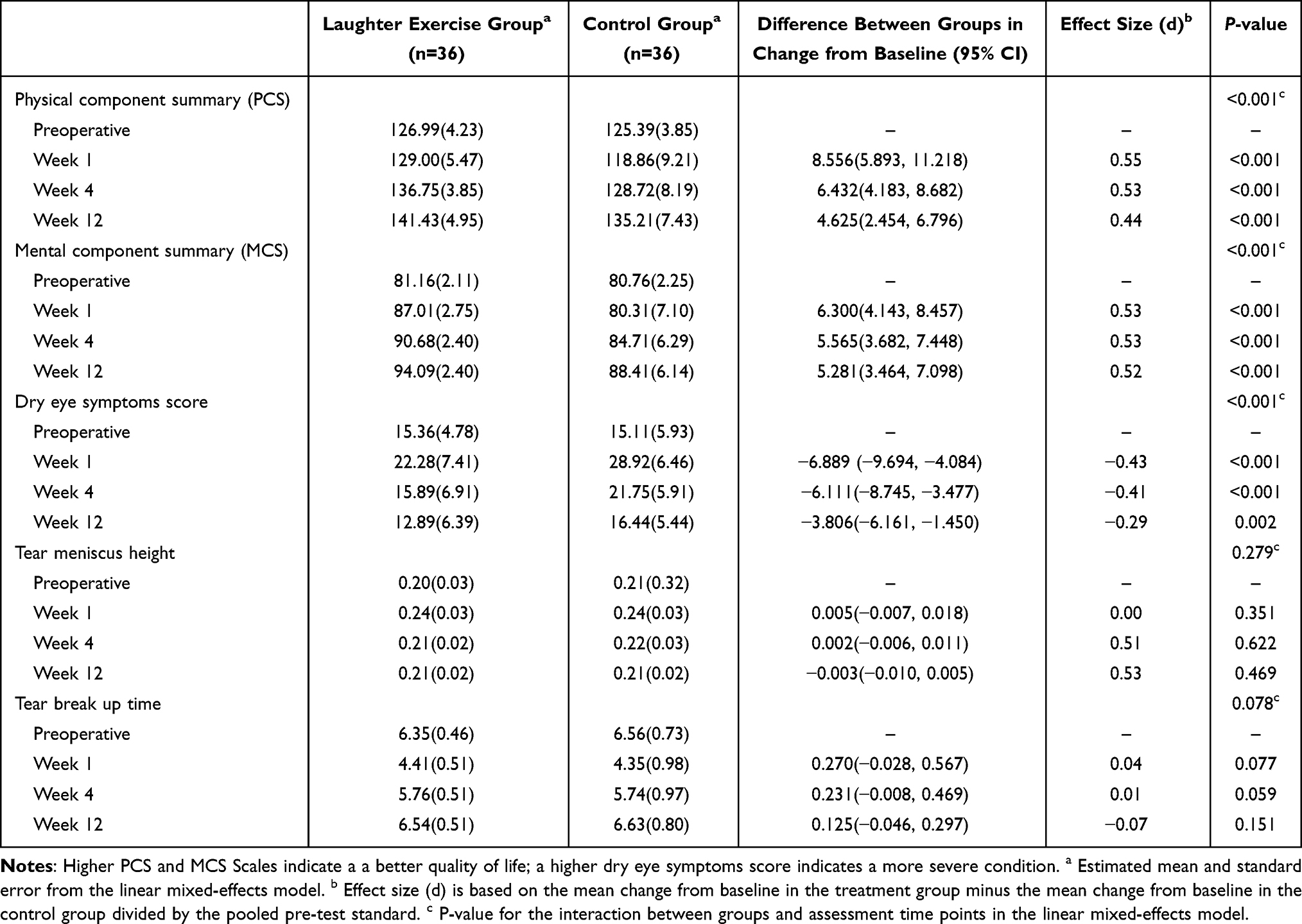 |
Table 2 Intervention Effect on Outcomes Across the Assessment Time Points |
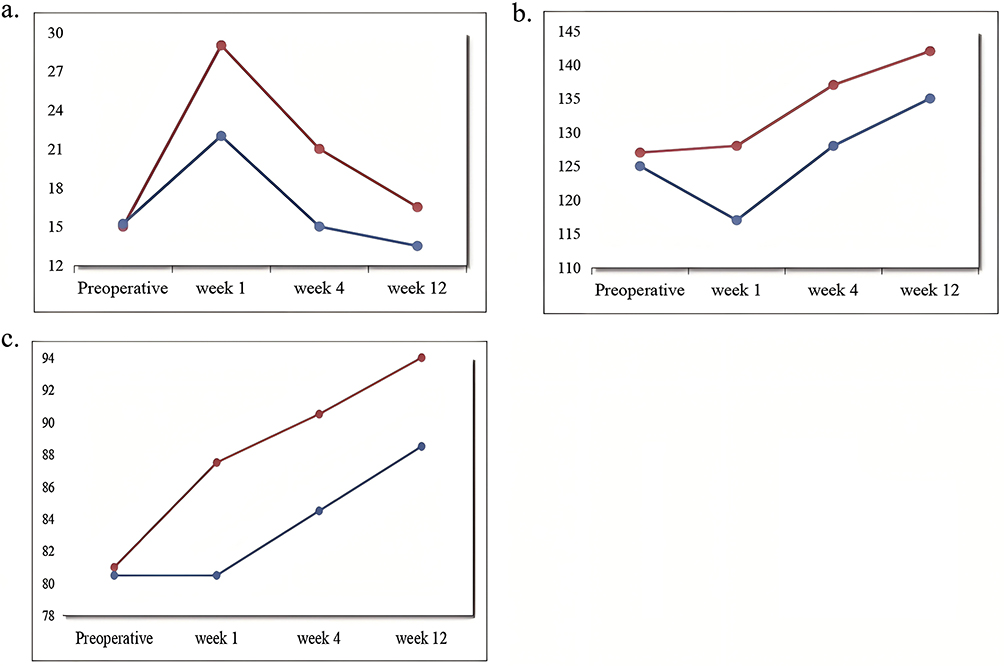 |
Figure 2 Group Comparisons in 4 Measurement Time Points (Repeated-Measures ANOVA). (a) Dry Eye Symptom Scores; (b) PCS; (c) MCS. Note: The red line represents the laughter exercise group, while the blue line represents the control group. |
Secondary Outcomes
The PCS and MCS of the 36-Item Short form Health Survey (SF-36)
In our study, the PCS and MCS have improved over time postoperatively (all P<0.05). There was a significant group×time interaction (all P<0.001; Figure 2), indicating that the change of PCS and MCS differed between the two groups over time. Compared with the control group, the laughter exercise group showed significantly greater improvements in PCS and in MCS (see Table 2). In the sensitivity analysis of missing values, the size of the intergroup difference was similar (P>0.05).
The Tear Meniscus Height and Tear Break-Up Time
In general, the tear meniscus height and tear break-up time have improved over time postoperatively (P<0.05). However, no statistically significant interaction between groups and assessment time points was observed (P>0.05). Both groups showed no difference at the three time points (all P>0.05; Table 2).
Adverse Events
During the 12-week study period, we systematically monitored adverse events. There were no adverse events related to the laughter therapy intervention (eg, eye discomfort, headache) in the intervention group. 97% of participants were satisfied with the intervention.
Discussion
This is the first randomized controlled trial to investigate the efficacy and safety of laughter exercise in alleviating discomfort associated with DED among patients who have undergone cataract surgery. Regular laughter exercises, when done for 4 weeks, can reduce the severity of dry-eye symptoms and boost patients’ physical and mental health. However, tear meniscus height and tear break-up time, which are objective signs of DED, did not change significantly. Our study suggested that laughter exercise is a non-invasive, cost-effective, and easy-to-do way to relieve dry-eye symptoms.
We found that laughter exercise led to significant improvements in dry-eye symptoms and an enhanced quality of life. DED may be a psychosomatic disease. Its management should follow a multifaceted approach.28 Previous studies have shown that laughter exercise can have beneficial effects on various health-related outcomes, including mental health, physical health, and physiological parameters.29,30 This study was the first to explore the value of laughter therapy in patients after cataract surgery, especially in reducing subjective distress associated with DED.
Various pathways help explain the relationship between laughter and DED. When patients smile, contraction of the orbicularis and forehead muscles can enhance local blood circulation and deliver greater amounts of oxygen and nutrients to ocular nerve endings, thereby alleviating patients’ subjective discomfort. There is a significant correlation between DED and emotional problems.9 Laughter exercise may reduce symptom distress. It does this by improving patients’ anxiety and depression. It also diverts their attention from eye discomfort.31,32 Furthermore, laughter increases pleasurable sensations and triggers the release of endogenous opioids in the thalamus, caudate nucleus, and anterior insula.33 Laughter could increase an individual’s tolerance to discomfort. Research has also shown that after laughter therapy, patients’ eating and sleeping habits can be regulated. Also, social media usage was significantly reduced.32 A healthier lifestyle is closely linked to improvements in DED symptoms.34,35 Therefore, when dealing with DED after cataract surgery, clinical practice can focus on patients’ psychological and emotional states, which may be crucial for improving both treatment efficacy and patient quality of life.
In our randomized controlled trial, we saw no significant improvement in tear meniscus height or tear breakup time. Unlike those of Li et al,16 they found that the laughter exercise group showed greater improvement in non-invasive tear breakup time than the control group. It might be due to our choice of research subjects. In our study, we included only patients with DED after cataract surgery. Their dry eye was mainly caused by organic factors like surgical trauma, corneal nerve injury, and inflammatory response. Laughter exercise is a psychological intervention. It affects the brain and emotions, not the tear generation or tear film stabilization system directly. These organic factors may make it hard for these patients to improve tear production and tear-film stability through laughter. Li et al16 included patients with dry eye from various causes. They excluded those who had eye surgery or ocular trauma in the past 12 months. Some of these patients might be more sensitive to psychological interventions. This negative result has important clinical implications. It tells clinicians and patients that laughter exercise cannot be expected to “cure” the physical causes of dry eye or replace artificial tears. Its value is in managing symptoms and improving quality of life. It should be seen as an additional treatment, not a replacement.
Clinical Implications
Laughter exercise intervention is suitable for patients with DED after cataract surgery. These patients might be unwilling to increase their medication burden and want to participate in self-management actively. Laughter exercise is not meant to replace major treatments like ATs. Instead, it serves as a complementary therapy. It helps improve patients’ dry-eye symptoms and quality of life. Nurses can easily teach patients this simple method. It only takes 5–10 minutes during postoperative health education, making it a great standardized, non-pharmaceutical adjunctive care measure. Laughter exercise has direct effects on symptom perception. It may also offer long-term benefits. It can foster a more positive mindset and could encourage patients to make healthier lifestyle choices. Although we did not measure this directly in our study, previous research has shown that laughter exercise can promote a more positive lifestyle.32 So, integrating laughter exercise into clinical practice can do more than relieve symptoms. It can contribute to patients’ overall well-being. However, we need longer follow-up studies to evaluate the long-term effects of laughter exercise and to explore how lifestyle changes might mediate and sustainably enhance well-being.
Advantages and Limitations
The Randomized Controlled Trial (RCT) design is the “gold standard” for evaluating the effectiveness of an intervention. Using laughter exercise in ophthalmic postoperative rehabilitation is a new interdisciplinary approach. This intervention is safe, non-invasive, cost-effective, and has no side effects. It allows patients to participate in their self-rehabilitation actively, and is entirely in line with the modern “biopsychosocial” medical paradigm. The outcome evaluations were comprehensive and objective. Our research uniquely incorporated both subjective indicators and objective metrics. We prioritize subjective indicators as our primary outcome measures. We recognize that improvement in subjective symptoms is the primary demand for most DED patients. In the control group, patients received usual care. The schedule and duration were the same as those of the intervention group, which can help clarify the possible placebo effect.
This study has limitations. The number of patients included was small. There may be a placebo effect; given the nature of the intervention, it is impossible to blind the patients. Humorous videos have varying “laugh-inducing” effects on different people. So, it is hard to standardize the intervention dose fully. The 12-week follow-up period was relatively short. As a result, the long-term effect remains unknown. In the future, researchers can conduct randomized controlled trials with larger samples and more extended follow-up periods (eg, 6–12 months). This will help further explore the impact of laughter exercises on dry eye outcomes. Researchers can also explore the potential mediating role of lifestyle changes in the long-term effects of laughter therapy over a more extended follow-up period.
Conclusion
The findings of this randomized controlled trial suggested that laughter exercise could alleviate dry eye symptoms in patients after cataract surgery and improve patients’ physical and mental health. These benefits were observed, but there was no corresponding improvement in objective clinical signs. Therefore, laughter exercise is a safe, practical, economical, and easily implementable intervention for managing postoperative dry-eye discomfort. It is not a therapeutic approach aimed at reversing the underlying pathophysiological mechanisms. Subsequent research should follow up for at least 6 months to evaluate the long-term effects of laughter exercise. Moreover, researchers can conduct in-depth mechanism studies to clarify the underlying biological pathways through which laughter exercise improves ocular surface health.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The corresponding author will respond to data access requests in a timely manner to ensure the reproducibility and transparency of the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–11. doi:10.1136/bjophthalmol-2011-300539
2. Yu Y, Hua H, Wu M, et al. Evaluation of dry eye after femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2015;41(12):2614–2623. doi:10.1016/j.jcrs.2015.06.036
3. Sutu C, Fukuoka H, Afshari NA. Mechanisms and management of dry eye in cataract surgery patients. Curr Opin Ophthalmol. 2016;27(1):24–30. doi:10.1097/ICU.0000000000000227
4. Miura M, Inomata T, Nakamura M, et al. Prevalence and characteristics of dry eye disease after cataract surgery: a systematic review and meta-analysis. Ophthalmol Ther. 2022;11(4):1309–1332. doi:10.1007/s40123-022-00513-y
5. Williamson JF, Huynh K, Weaver MA, Davis RM. Perceptions of dry eye disease management in current clinical practice. Eye Contact Lens. 2014;40(2):111–115. doi:10.1097/ICL.0000000000000020
6. Labetoulle M, Benitez-Del-Castillo JM, Barabino S, et al. Artificial tears: biological role of their ingredients in the management of dry eye disease. Int J Mol Sci. 2022;23(5). doi:10.3390/ijms23052434
7. Gomes JAP, Santo RM. The impact of dry eye disease treatment on patient satisfaction and quality of life: a review. Ocul Surf. 2018;17(1). doi:10.1016/j.jtos.2018.11.003
8. Serrano-Robles JG, Pérez-Vázquez AK, Vera-Duarte GR, et al. Safety and efficacy of diquafosol compared to artificial tears for the treatment of dry eye: a systematic review and meta-analysis. Int J Mol Sci. 2025;26(17). doi:10.3390/ijms26178113
9. CZ HQ, Xie C, Liu L, Yang H, Wei R. Relationship between dry eye disease and emotional disorder: the mediating effect of health anxiety. Front Public Health. 2022;10:771554. doi:10.3389/fpubh.2022.771554
10. Wan KH, Chen LJ, Young AL. Depression and anxiety in dry eye disease: a systematic review and meta-analysis. Eye. 2016;30(12):1558–1567. doi:10.1038/eye.2016.186
11. Alkozi HA. Ocular surface health in connection with anxiety and depression: a review. J Multidiscip Healthc. 2024;17:2671–2676. doi:10.2147/JMDH.S468878
12. Kaiser TJB, Schrader S, Geerling G. Depressive symptoms, resilience, and personality traits in dry eye disease. Graefes Arch Clin Exp Ophthalmol. 2019;257(3):591–599. doi:10.1007/s00417-019-04241-1
13. Lin G, Yang L, Wang Y, et al. The efficacy of laughter therapy on psychological symptoms in people with cancer: a systematic review and meta-analysis of randomized controlled studies. Psychooncology. 2024;33(11):e70010. doi:10.1002/pon.70010
14. Si S, Çeli KA, Kılınç T. The effect of laughter yoga on perceived stress, burnout, and life satisfaction in nurses during the pandemic: a randomized controlled trial. Complement Ther Clin Pract. 2022;49:101637. doi:10.1016/j.ctcp.2022.101637
15. Brodaty H, Low L-F, Liu Z, et al. Successful ingredients in the SMILE study: resident, staff, and management factors influence the effects of humor therapy in residential aged care. Am J Geriatr Psychiatry. 2013;22(12):1427–1437. doi:10.1016/j.jagp.2013.08.005
16. Li J, Liao Y, Zhang S-Y, et al. Effect of laughter exercise versus 0.1% sodium hyaluronic acid on ocular surface discomfort in dry eye disease: non-inferiority randomised controlled trial. BMJ. 2024;386:e080474. doi:10.1136/bmj-2024-080474
17. Shi WY, Corneal Disease Group of the Ophthalmology Branch of the Chinese Medical Association, Corneal Disease Group of the Ophthalmology Branch of the China Medical Doctor Association. China Dry Eye Clinical Diagnosis and Treatment Expert Consensus (2024) (Chinese Journal). Chin J Ophthalmol. 2024;60(12):968–976. doi:10.3760/cma.j.cn112142-20240517-00227
18. Zung WW, Wonnacott TH. Treatment prediction in depression using a self-rating scale. Biol Psychiatry. 1970;2(4):321–329.
19. Dunstan DA, Scott N. Norms for Zung’s self-rating anxiety scale. BMC Psychiatry. 2020;20(1):90. doi:10.1186/s12888-019-2427-6
20. Wong A, Xiong YY, Kwan PWL, et al. The validity, reliability and clinical utility of the Hong Kong Montreal Cognitive Assessment (HK-MoCA) in patients with cerebral small vessel disease. Dement Geriatr Cognit Disord. 2009;28(1):81–87. doi:10.1159/000232589
21. Zhao H, Liu ZG, Yang WZ, et al. Development and evaluation of a dry eye questionnaire in China (Chinese Journal). Chin J Ophthalmol. 2015;51(9):647–654. doi:10.3760/cma.j.issn.0412-4081.2015.09.003
22. Geng RJ, Wei JJ, Yang KL, Wang SP, Ren SW. A comparative study on the applicability of the China dry eye questionnaire and the corneal disease index questionnaire among college students (Chinese Journal). Int J Ophthalmol. 2023;23(06):972–976. doi:10.3980/j.issn.1672-5123.2023.6.18
23. Aaronson NK, Muller M, Cohen PD, et al. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol. 1998;51(11):1055–1068. doi:10.1016/s0895-4356(98)00097-3
24. Ware JE, Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. Med Care. 1995;33(4 Suppl):AS264–AS279.
25. Wang Y, Zhang X, Dong J, et al. Psychometric properties of the Chinese version of the SF-36v2 in patients with severe mental illnesses in China: factor structure, reliability, and validity. Health Qual Life Outcomes. 2025;23(1):20. doi:10.1186/s12955-025-02350-6
26. Lin Y, Yu Y, Zeng J, Zhao X, Wan C. Comparing the reliability and validity of the SF-36 and SF-12 in measuring quality of life among adolescents in China: a large sample cross-sectional study. Health Qual Life Outcomes. 2020;18(1):360. doi:10.1186/s12955-020-01605-8
27. Zhao L, Liu Z, He Y, Li N, Liu D. Survey on the applicability of SF-36 version-2 (SF-36v2) in assessment quality of life among urban residents in Chengdu city (Chinese Journal). Zhonghua Yu Fang Yi Xue Za Zhi. 2014;48(5):370–374. doi:10.3760/cma.j.issn.0253-9624.2014.05.008
28. Zhao C, Li X. Dry eye disease and psychosomatics-benefits of mind-body therapy for dry eye disease. Front Med Lausanne. 2025;12:1600258. doi:10.3389/fmed.2025.1600258
29. Stiwi K, Rosendahl J. Efficacy of laughter-inducing interventions in patients with somatic or mental health problems: a systematic review and meta-analysis of randomized-controlled trials. Complement Ther Clin Pract. 2022;47:101552. doi:10.1016/j.ctcp.2022.101552
30. Akimbekov NS, Razzaque MS. Laughter therapy: a humor-induced hormonal intervention to reduce stress and anxiety. Curr Res Physiol. 2021;4:135–138. doi:10.1016/j.crphys.2021.04.002
31. Kuru N, Kublay G. The effect of laughter therapy on the quality of life of nursing home residents. J Clin Nurs. 2017;26(21–22):3354–3362. doi:10.1111/jocn.13687
32. Güvener YÖ. The effect of laughter therapy on self-efficacy and psychological well-being in nursing students. Arch Psychiatr Nurs. 2024;52:121–127. doi:10.1016/j.apnu.2024.07.021
33. Manninen S, Tuominen L, Dunbar RI, et al. Social laughter triggers endogenous opioid release in humans. J Neurosci. 2017;37(25):6125–6131. doi:10.1523/JNEUROSCI.0688-16.2017
34. Yang W, Wang H, Li J, et al. Demographic and lifestyle factors associated with dry eye disease in China: a cross-sectional multi-center study. Ocul Surf. 2024;34:146–155. doi:10.1016/j.jtos.2024.07.007
35. Stapleton F, Velez FG, Lau C, Wolffsohn JS. Dry eye disease in the young: a narrative review. Ocul Surf. 2023;31:11–20. doi:10.1016/j.jtos.2023.12.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.