Back to Journals » Journal of Asthma and Allergy » Volume 13
Latex Allergy: Current Status and Future Perspectives
Authors Nucera E, Aruanno A ![]() , Rizzi A
, Rizzi A ![]() , Centrone M
, Centrone M
Received 6 July 2020
Accepted for publication 12 August 2020
Published 28 September 2020 Volume 2020:13 Pages 385—398
DOI https://doi.org/10.2147/JAA.S242058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Eleonora Nucera,* Arianna Aruanno,* Angela Rizzi,* Michele Centrone*
Allergy Unit, Fondazione Policlinico Universitario A. Gemelli IRCSS, Università Cattolica del Sacro Cuore, Rome, Italy
*These authors contributed equally to this work
Correspondence: Eleonora Nucera
Allergy Unit, Fondazione Policlinico Universitario A. Gemelli IRCSS, Largo F. Vito, 1, Rome 00168, Italy
Email [email protected]
Abstract: Allergy to natural rubber latex (NRLA) from Hevea brasiliensis is a relevant public health issue, in particular in healthcare workers and groups at risk. Clinical manifestations of NRLA can range from mild skin disorders to life-threatening systemic reactions. Prevention measures remain the gold-standard treatment for patients suffering from NRLA, but the only etiological therapy able to influence the natural history of NRLA is specific desensitization. This review aims to underline the epidemiological, clinical and diagnostic aspects of NRLA, and carries out a complete and wide-ranging review of the current literature on NRLA management and immunotherapy.
Keywords: latex, immunotherapy, desensitization
Introduction
Natural rubber latex (NRL) is an intracellular cytosol secreted from a rubber tree, Hevea brasiliensis (Hev b), which functions as a protective sealant.
The milky substance is first ammoniated to prevent bacterial contamination and coagulation and then multiple chemicals are added: accelerators, antioxidants and secondary preservatives. Because of its excellent elastic properties, NRL is widely used in the manufacture of medical devices and in a variety of everyday articles such as catheters, gloves, condoms and balloons. The first recorded reactions to NRL date back to 1927, when two German doctors, Stern and Grimm, respectively described a case of urticaria caused by a dental prothesis and a case of professional asthma.1–3
Immediate-type allergic reactions to NRL were epidemiologically silent until 1979, when Nutter reported a case of urticaria after contact with gloves.4
Thereafter, reports linked to latex exposure increased exponentially in the late 1980s and 1990s, simultaneously with the increasing use of latex devices. In general, latex protein components are responsible for type I latex-specific allergy and the accelerators and antioxidants are agents of type IV allergic reactions (contact dermatitis), although rare cases of delayed allergy to latex proteins have been reported.
Undiagnosed latex allergy is potentially very serious for patients and is increasingly recognized as a significant contributor to morbidity and mortality during medical and surgical procedures. The aim of this review is to underline the epidemiological, clinical and diagnostic aspects of natural rubber latex allergy (NRLA), and to carry out a complete and large review of the literature on NRLA management.
Methods
A literature search (PubMed) for articles until June 2020 was conducted using the following key words: “latex”, “latex allergy”, “latex hypersensitivity”, “management”, “primary and secondary prevention”, “immunotherapy”, “desensitization”, “treatment” and “anaphylaxis”.
The following eligibility criteria were used for article inclusion: population: patients with latex allergy and/or at risk for anaphylaxis; intervention: any approaches or protocols that incorporated a strategy for latex allergy and anaphylaxis management; comparator: any studies irrespective of whether there was a comparator included in the study design; outcomes: any related to prevalence, diagnostics, and treatments including primary prevention and immunotherapy; and study design: experimental studies and observational studies. We excluded basic science or animal (non-human) studies. The search focused on English-language articles. Overall, approximately 250 articles were reviewed and 107 of these are included here for reference.
Epidemiology
The current prevalence rate of latex allergy changes according to the population considered.
The highest risk population is represented by patients undergoing repeated surgical interventions (such as spina bifida patients). These groups have a higher chance of being exposed to latex allergens and therefore have a higher risk of developing allergy. The current prevalence of latex allergy and sensitization among susceptible patients are 7.2% and 30.4%, respectively. In particular, the prevalence of latex sensitivity among the spina bifida pediatric population was between 40% and 65%.5–7
Healthcare workers (HCWs) are the occupational group most affected by NRLA owing to their frequent use of latex gloves. The current prevalence of latex allergy and sensitization among HCWs worldwide are 9.7% and 12.4%, respectively.5
Other occupational workers, including rubber industry workers, hairdressers and housekeepers, are also at high risk for latex allergy, although reports have suggested that general populations who have not had occupational contact with latex products can also develop latex sensitization and latex allergy.
Data analysis from limited studies suggests that the current average latex allergy prevalence among the general population worldwide is 4.3%.5
Although the use of latex gloves in surgery became routine after 1920, gloves were not consistently used in other areas of patient care until the late 1980s. The emergence of human-to-human transmission of infectious pathogens, such as hepatitis C and HIV, produced a dramatic increase in the use of latex gloves and other latex devices in all areas of patient care. For these reasons, in the late 1980s and 1990s there was a considerable increase in latex allergy.
Clinical Manifestation
Airborne antigen exposure is an important source of latex sensitization among HCWs. The addition of cornstarch powder to improve the fit of gloves has been shown to increase this latex protein aerosolization; for this reason, the use of powder-free latex gloves markedly reduces the risk of sensitization.8,43
Latex absorption through the skin is another major route of sensitization in HCWs, especially when the skin is damaged. Moreover, susceptible patients can also be latex exposed during surgical procedures.
Non-medical rubber products, such as car tires, have little allergen in them owing to prolonged heating during manufacture and chemical solvent use; consequently, it does not seem necessary to avoid contact. Patients need to be mostly concerned about products made by a dipping method with low heat and minimal vulcanization time (gloves, condoms, etc), which have a high allergenic risk.
Type I Hypersensitivity Reactions
The most frequent clinical manifestations of latex allergy are related to type I hypersensitivity mediated by immunoglobulin E (IgE), and can involve the skin (itching, swelling, pruritus and contact urticaria), the respiratory system (sneezing, wheezing and rhinitis) and the eyes (conjunctivitis). Clinical manifestations can also be systemic, such as bronchospasm, hypotension, cardiorespiratory collapse and shock. Anaphylactic shock is potentially fatal and occurs most commonly in an intraoperative context.9
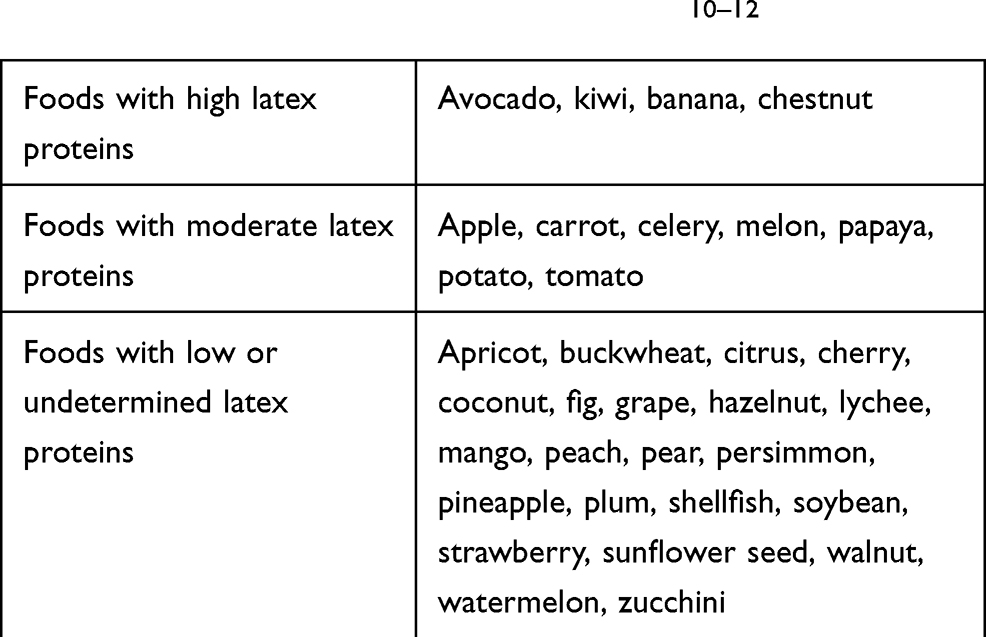
An important clinical manifestation of NRLA is the “latex-fruit syndrome” due to latex proteins that have clinical cross-reactivity with multiple vegetable foods. The ingestion of many fruits or vegetables (Table 1) can cause clinical symptoms ranging from itching and pruritus of the oral cavity (oral allergy syndrome [OAS]) to anaphylaxis.10–12
 |
Type IV Hypersensitivity Reactions
Type IV hypersensitivity reactions typically develop 24–48 hours after exposure. These reactions are generally seen as eczematous dermatitis at the contact site, and are localized and uncomfortable, but not life threatening.
Delayed reactions are usually caused by accelerators and antioxidants (e.g. carbamates, thiurams) added during the manufacturing process of NRL. Only a few cases of delayed allergy to NRL proteins have been reported in the literature.13,14
Relevant Allergens
NRL secreted by Hevea brasiliensis contains more than 240 polypeptides, detected by electrophoresis.15,16
Fifteen allergens (Hev b 1–15) have been characterized and listed by the World Health Organization/International Union of Immunologic Societies Allergen Nomenclature Committee (www.allergen.org) (Table 2). IgE reactivity to Hev b 1 and Hev b 3, membrane-bound elongation proteins, seems to be predominant in patients with spina bifida and urological congenital anomalies, while Hev b 5 and Hev b 6 (with the domains Hev b 6.01 and Hev b 6.02) were recognized as major allergens in HCWs.17,18
 |
Table 2 Allergenic Components of Latex from Hevea brasiliensis www.allergen.org) |
In particular, the isolation and characterization of Hev b 5-specific IgE has resulted in an increase in the sensitivity of the serological assay, and improved allergy diagnostics.19
The other allergens appear to be minor contributors to a genuine sensitization to latex; some of them belong to the families of defense proteins, such as lipid transfer protein (Hev b 12) and profilin (Hev b 8), and are responsible for cross-reactivity with fruits and vegetables. Hev b 15, a serine protease inhibitor, is the last Hev b allergen to be discovered.20–25
Diagnosis
The diagnosis of NRLA is formulated on the basis of an accurate medical history, physical examination, and in vivo and in vitro tests.
Medical History
The medical history is the cornerstone for establishing an accurate diagnosis of latex allergy and for identifying risk factors and a correlation between latex exposure and the appearance of symptoms. It is also fundamental to investigate some key points, such as history of atopy, food allergies (particularly bananas and kiwi fruit), and undiagnosed reactions or complications during dental work or surgical procedures.26
Skin-Prick Test
Skin-prick tests (SPTs) must be carried out in a hospital setting by trained allergist experts in test technique and in interpreting the results. The overall risk of inducing anaphylactic reactions by SPTs is less than 0.02%.27
The first systemic reactions to SPTs were published in 1993, when four of 118 patients with latex allergy reported anaphylactic reactions; since then, further cases have been reported in the literature.28–30
In highly sensitive patients, such as those with spina bifida, latex allergens may induce systemic reactions; in this condition, SPTs are considered a risk and in vitro tests should be performed in order to complete the diagnosis.31
Patch Test
A patch test is used to identify type IV hypersensitivity reactions. Rare cases of delayed allergy to NRL proteins have been reported,14 so this method is helpful in differentiating allergic contact dermatitis from irritant contact dermatitis generally caused by accelerators and antioxidants. The allergens that have most commonly shown positive reactions are carbamates, thiurams mix, 2-mercaptobenzothiazole and 1,3-diphenylguanidine.32
Irritant contact dermatitis occurs when an exogenous substance without previous sensitization causes direct damage to the skin; most cases of hand dermatitis, in particular in HCWs, have this underlying mechanism and may be clinically similar to delayed allergies.
In Vitro Immunoassays and Basophil Activation Test
Serological assays have been developed for the diagnosis of IgE-mediated latex allergy and include IgE testing ImmunoCAP measures. Traditional latex-specific IgE are based upon the quantification of IgE directed against crude natural allergen extract. The Hev b allergens, available in recombinant form, can be identified with ImmunoCAP (Thermo Fisher Scientific, Uppsala, Sweden).
Sensitization to some components (e.g. Hev b 1, Hev b 5, Hev b 6.01 and Hev b 6.02) is associated with severe clinical phenotypes and is expressed as genuine latex allergy whereas sensitization to other components (e.g. Hev b 8) generally results in milder symptoms or is asymptomatic.33,34
The basophil activation test (BAT) is a flow-cytometry-based functional assay that assesses the degree of cell activation after exposure to a stimulus. This test could be useful to evaluate, in vitro, what happens in vivo following the exposure of the immune system to latex.35
Provocation Tests
Provocation tests are important to test the target tissue’s responsiveness to the allergen under controlled conditions.36 It is necessary to carefully evaluate the opportunity to carry out provocation tests if there is a positive anamnesis for anaphylactic reactions or in patients with important comorbidities.37
Several methods of performing challenge tests have been reported (cutaneous, mucous–oral, sublingual, conjunctival, nasal, bronchial and vaginal), although some of them (e.g. vaginal test) have a low sensitivity and many limitations related to the procedure.38,39 Cutaneous challenge was performed by donning a latex glove and recording local symptoms. For sublingual, conjunctival, nasal and bronchial tests, latex solutions were prepared with latex extract, starting with the highest dilution and progressively increasing the concentration to reach the threshold dose.
Management
The management of groups at risk for latex allergy and HCWs is based on a step-by-step process through four possible strategies: preventive measures, symptomatic treatment, immunotherapy and anti-IgE therapy.40,41
Preventive Measures
Primary prevention of latex allergy (NRL) means the reduction of exposure of NRL to prevent sensitization in susceptible workers and at-risk populations.41,42
However, these measures are focused on the use of gloves and, in particular, the total replacement of latex gloves with powder-free low-protein (PFLP) latex gloves or synthetic gloves made of alternative material.43,45 Since 1999, the substitution of powdered NRL gloves with non-powdered NRL sterile gloves in the operating room has resulted in a marked decrease in the number of new cases of latex sensitization.46 In 2005, Korniewicz et al showed that, although the initial cost of conversion may be high, it could help to reduce long-term healthcare costs. In fact, the resulting health expenditure was lower than the level of HCWs’ compensation claims for latex-related disability.45
Furthermore, there have been efforts by the international glove industry to develop innovative protocols in order to reduce the allergenic content, satisfying both consumer demand and regulatory requirements.47 These include deproteinization and purification obtained by the addition of proteolytic and/or surfactant enzymes, chlorination process and high-temperature post-washing.48
Regarding the use of alternative synthetic gloves, manufacturing companies have produced accelerator-free gloves using different materials (polychloroprene, nitrile and polyisoprene thermoplastic elastomers) or after washing in a strong alkaline solution.47 A survey49 of 89 dental practitioners, published in 2020, confirmed that routine use of latex-containing products in UK dental offices was low and that examination gloves in nitrile were replacing the general practice of using NRL gloves.
Nevertheless, at the time, the evidence did not support a total ban on the use of latex gloves. Furthermore, with the exception of a few clinical studies, these latex-free gloves do not seem to have the same characteristics in terms of elasticity, tactile quality, providing a protective barrier against infections, resistance to permeability and cost accessibility.41,50
In 2020, Raulf49 emphasized that most studies demonstrating a decline in the prevalence of latex sensitization following the introduction of powder-free latex gloves have been conducted on healthcare professionals in highly industrialized countries (Europe and North America). In contrast, in developing countries and in those areas where primary prevention policies are not implemented, latex allergy continues to be a serious public health problem.51
Another countermeasure is technological research into potential alternative sources of natural rubber gloves, starting from plant species such the Mexican shrub guayule, which is not botanically related to Hevea brasiliensis, but has a protein content of less than 1% and no cross-reactivity with Hevea latex allergens.52,53
In the USA the Food and Drug Administration (FDA) has approved guayule gloves for use in the general population and has recognized and labeled these gloves as Hevea latex free.54
In March 2020, the FDA released guidance, titled “Process for Making Available Guidance Documents Related to Coronavirus Disease 2019” (available from https://www.govinfo.gov/content/pkg/FR-2020-03-25/pdf/2020-06222.pdf), aimed at increasing the supply of other personal protective equipment (PPE) important in the fight against coronavirus disease 2019 (COVID-19) pneumonia: medical gowns, other apparel and gloves.55 The FDA recommends that HCWs follow current Centers for Disease Control and Prevention (CDC) guidance regarding PPE that should be used during the COVID-19 pandemic. In order to help to ensure the availability of these devices, the FDA does not intend to object to the distribution and use of patient examination and surgeon’s gloves that do not comply with the regulatory requirements (device registration and listing, premarket notification – where applicable – and quality system regulation compliance), provided that these devices are marketed using labeling that 1) expressly delineates the uses for which they are appropriate, 2) warns against uses that may create excessive risk, 3) meets applicable barrier protection/flammability/sterility standards, and 4) does not indicate a use that may increase an undue risk in light of the public health emergency.56
Another crucial strategy of primary prevention in the workplace is the creation of a latex allergy task force and the development of appropriate facility policies, awareness and educational initiatives among HCWs.57
As early as 2002, Allmers et al demonstrated that a joint program of education and regulation in German hospitals was followed by a remarkable change in glove purchase patterns.56 Since children with spina bifida represent the population with the highest risk of developing latex allergy, primary prevention is intended to avoid latex exposure in subjects (not yet sensitized) from birth. Numerous primary prevention studies have demonstrated its effectiveness, with the possibility of reducing the sensitization and, therefore, the appearance of allergic symptoms.56–58
In 2019, Stinkens et al59 highlighted the heterogeneity of recommendations concerning patient safety in the operating room, provided by some scientific societies. Ideally, a latex-safe environment should be used in all healthcare facilities. The guidelines of the American Society of Anesthesiologists60 recommend that high-risk patients are scheduled first on the day of surgery to be treated in an operating room left unused for 3–6 hours, with possible and foreseeable management implications, including postponed surgery, increased patient discomfort and additional financial costs. In contrast, the guidelines of the Australasian Society of Clinical Immunology and Allergy61 suggest that the effect of this specific scheduling is negligible when all powdered latex gloves are removed from the operating room and replaced by PFLP latex or synthetic gloves. According to Stinkens et al, patients with a history of latex allergy can be treated safely without specific scheduling when all powdered latex gloves are substituted with PFLP latex gloves.59
To date, only a few prevalence studies concerning other occupational workers exposed to latex outside the healthcare setting have been conducted, and there is a lack of data on the effects of primary preventive strategies.62–64
Secondary prevention of latex allergy has focused on procedures that prevent the development of reactions in sensitized/allergic patients, and include premedication before carrying out any risky procedures and providing latex-safe environments. However, this is not always possible because of the ubiquity of latex products and the cross-reactions to latex and fruit and vegetables.40
A meta-analysis of 12 studies published between January 1990 and September 2010 highlights that avoidance of NRL powder gloves in the workplace reduces both symptoms and markers of sensitization in latex-allergic subjects, regardless of co-workers’ use of non-latex gloves or PFLP latex gloves. Moreover, the authors concluded that there was
limited evidence that latex-allergic health care workers can continue to use PFLP gloves with no worsening in their symptoms, provided that their co-workers use PFLP latex, or non-latex gloves. 65
On the other hand, only a small case series of nine patients has described the efficacy of accelerator-free medical gloves in the secondary prevention of allergic contact dermatitis (ACD) caused by rubber accelerators in HCWs.66
Gentili et al67 showed that an effective and exemplary example of secondary prevention of latex allergy is feasible for infants born with spina bifida. Previously, a prospective study by Reider’s group68 investigated the effectiveness of secondary prevention strategies in the hitherto largest cohort of subjects at high risk for latex allergy for a comparatively long follow-up period. The authors attributed a significant decrease in latex-specific IgE in latex-sensitized patients with hydrocephalus to medical more than home prophylaxis, which was “un-realistic in everyday life”.
To date, the use of non-latex gloves, catheters and alternative products, usually made of silicone, plastic or vinyl, can be considered the best recommendation for secondary prevention of latex allergy, derived from the scientific literature. Moreover, individuals who have experienced allergic reactions during surgical or medical procedures should consider wearing a MedicAlert bracelet or necklace, carrying auto-injectable epinephrine and sterile non-latex gloves for emergency use, and discussing latex allergy with all healthcare and community providers, including school, day care and camp. In addition, consultation with an allergologist with experience in the management of latex allergy is recommended to fully evaluate the risks and the possible need for preoperative treatment with special medications to suppress the potential for severe allergic reaction. Moreover, the avoidance of all latex-containing items, especially in the operating room, is strongly recommended.9
Finally, regarding prevention, all patients should have a list of substitute latex-safe products for hospital and home duties, cross-reacting fruits and occult sources of NRL exposure.69
Indeed, the concept of “latex-safe” environments versus “latex-free” environments has turned out to be safe, practical and ideal for patients with latex allergy.
Symptomatic Treatment
The management of exposed and symptomatic individuals requires pharmacological treatment depending on the type of reaction that is present – from a mild sensitivity to a life-threatening allergic reaction (anaphylaxis).
If the clinical manifestations consist of irritant dermatitis, removal of the latex and cleaning of the area are the first step. The application of topical steroids is used to reduce inflammation, and evaluation by a dermatologist is recommended. Delayed type IV hypersensitivity reactions require the same treatment.
In case of severe, life-threatening, generalized or systemic hypersensitivity reaction, defined as anaphylaxis, patients should managed and treated according to dedicated guidelines.70–72
Immunotherapy
More than a hundred years ago, Noon and Freeman published the first works on allergen-specific immunotherapy (AIT) using grass pollen extracts.73,74
Since then, AIT has been performed by a large number of modalities and has proven effective and safe in the treatment of allergic diseases, although in some areas of the world (e.g. the USA) no standardized NRL reagent is available. Administration of the allergen at increasing doses results in a shift of T-helper cell polarization from the Th2 to Th1 cell phenotype; this switch is mediated by T-regulatory cells with the production of interleukin-10, tumor necrosis factor-alpha and other chemical mediators.75
Although not all mechanisms of action of specific immunotherapy have been clarified, AIT remains the only etiological and decisive therapy able to modify the natural course of allergic diseases by inducing long-term immunological tolerance (Table 3). The first research tried to desensitize patients with latex allergy belonging to at-risk groups (such as health operators) by the percutaneous route.76
 |
Table 3 Features of Latex Immunotherapy Trials |
Patriarca et al in 2002 suggested a progressively increasing exposure to latex, obtained by wearing latex gloves daily. After the desensitizing treatment, a maintenance latex exposure of at least 60 minutes in both hands three times a week was recommended.77 The proposed percutaneous route seems absolutely safe (although few patients have been treated), and no side effects were highlighted.
In 1999, Pereira et al reported the first experience with subcutaneous immunotherapy (SCIT) for latex. A 31-year-old woman, professionally exposed to latex devices, underwent SCIT for latex up to the maximum tolerated dose.78
Although treatment was effective, systemic reactions related to its administration were reported.
One year later, a randomized, multicenter, double-blind placebo-controlled trial was performed in 17 patients by Leynadier et al; desensitization was effective but the frequency of systemic reactions was higher in the active group, even during the maintenance phase.79
The evidence from these studies, with the experience of a high rate of adverse reactions (even anaphylaxis), was confirmed by further studies; Tabar et al even reported systemic reactions in 81.8% of patients in the active group versus 16.7 % in the placebo group.80,81
For all these reasons, the subcutaneous route of latex immunotherapy administration was largely abandoned.
In the early 2000s, researchers assessed the potential use of sublingual immunotherapy (SLIT) for latex. The published literature regarding latex SLIT began in 2001, when our group described the case report of a patient with NRLA who became able to tolerate 1-hour mucosal and 6-hour cutaneous latex challenge tests after a 3-day rush build-up with latex SLIT.82 From this case, in the following years, numerous works have pursued the study of the sublingual route of administration.83,84 In 2002, Patriarca et al studied 24 patients in a randomized double-blind placebo-controlled trial. Both groups of patients underwent a 4-day rush protocol followed by SLIT maintenance for 3 months. After maintenance, tolerance of latex exposure (confirmed by latex-specific challenges) significantly improved in all patients in the SLIT group compared with the placebo group, and only mild local reactions were reported.85
Although this was a small trial, these preliminary data suggested that SLIT could be safe and efficacious for the treatment of latex allergy. Another study, by Cisterò Bahima et al86 in 2004, enrolled 26 latex-allergic patients treated with a commercial extract for sublingual administration (SLIT-Latex; ALK Abello). According to a rush schedule, the maintenance dose was administered for 9 weeks. A significant improvement in skin reactivity upon cutaneous exposure was reported, but 46.2% of patients experienced at least one systemic reaction. This evidence, together with further, although rare, reports of anaphylaxis, suggest that the induction phase should be performed under medical supervision.87
Nettis et al, in 2007, enrolled 40 adult patients with asthma or urticaria randomized to an ultrarush double-blind, placebo-controlled latex SLIT protocol with the SLIT-Latex extract.88 After a 12-month maintenance phase, patients underwent cutaneous challenge and a statistically significant improvement was again noted compared with the placebo group. Only three patients in the active group reported local side effects, confirming the overall safety of latex SLIT. Other data in the literature also support the long-term safety and efficacy of NRL immunotherapy in children.89–91
The interest in rush protocols has grown over the years; our group in 2008 compared two different rush induction protocols (2 or 3 days) in terms of safety and tolerability, showing no systemic or local reactions in the 3-day protocol patients.92
Buyukoturk et al studied HCWs who remained symptomatic despite attempted avoidance in 2011. This work further confirms the safety and efficacy of latex SLIT.93
Additional confirmation of safety and efficacy was given by Lasa Luaces et al in 2012. They studied 23 latex-allergic children and, after 12 months of SLIT, also underline immunological changes to predict clinical efficacy or safety outcomes. Although some serological changes were observed (the BAT with latex showed a reduction in reactivity after 6 months), this trial did not show significant statistical changes in IgE and IgG4.94
The most recent study regarding latex SLIT is a large observational case series of 76 adult patients with NRLA who underwent SLIT for 3 years of treatment. After desensitization, in this study there was a marked reduction in serum levels of latex-specific IgE and, according to the literature, a reduction in symptoms and scores on provocation tests, while IgG4 levels did not change.95
On the other hand, the literature also describes cases that show a lack of effectiveness of the treatment; for example, Morfin Maciel et al describe the case of a boy who, despite an AIT for latex, experienced anaphylaxis after an airport inspection with latex gloves.96
Gastaminza et al showed no significant difference in specific provocation tests or in vitro testing after a year of SLIT-Latex, with the exception of a reduction in the percentage of basophil activation both in the active group after 2 years of therapy and in the placebo group after 1 year of treatment.97
Long-term latex SLIT complications are less often described in literature; significant is the case of a 38-year-old woman who developed solid food dysphagia, heartburn and dyspepsia after 3 years of the maintenance phase. The esophageal endoscopy and biopsies showed an eosinophilic esophagitis that improved after 3 months of SLIT interruption; this case seems to confirm what has already been highlighted in the literature for other oral or sublingual immunotherapies.98,99
Anti-IgE Therapy
Omalizumab has been shown to be clinically efficacious in the treatment of patients with allergic asthma and chronic spontaneous urticaria (CSU).100,101
Therefore, some authors have studied the role of omalizumab in NRLA treatment. Leynadier et al,102 in a randomized, double-blind, placebo-controlled study, showed a statistically significant reduction in conjunctival and cutaneous responses to latex after omalizumab treatment. Di Leo at al103 also reported an improvement in latex-induced contact urticaria in a patient with uncontrolled chronic spontaneous urticaria. Our case report confirms these findings; in fact, an asthmatic patient who was allergic to latex, during the omalizumab treatment, did not report clinical symptoms after any accidental contact with latex.104
The use of omalizumab can also be extended as an adjunct to latex immunotherapy; its use in conjunction with immunotherapy has shown promising results in the treatment of venom and food allergy, especially in the reduction of adverse reactions.105
Five-Year View
NRLA still represents a substantial health, social and financial problem for society today. Although the prevalence of sensitization to NRL has significantly declined in developed countries over the past few years, NRLA remains a relevant issue, especially among certain professional categories. The lack of data and preventive measures in developing countries means that the problem is still underestimated.
Another important aspect is the heterogeneity of the recommendations concerning primary prevention. It would be desirable that international guidelines (in particular concerning patient safety in the operating room) be drawn up in the coming years.
During 2020, the COVID-19 pandemic has sparked a great deal of interest in how people might avoid becoming infected; for the general population it would seem that a simple solution is to wear disposable gloves, which are often made of latex.
However, the widespread use of latex gloves during the COVID-19 pandemic by both HCWs and lay people could potentially worsen or induce NRLA, as suggested by the first published epidemiological studies.106
The production and the use of alternative synthetic gloves at this time does not seem to be completely regulated because in order to help to ensure the availability of these devices, the FDA does not intend to object to the distribution and use of gloves that do not comply with the regulatory requirements. Given these considerations, an imminent increase in NRLA patients could be expected.
The authors believe that an international call to raise awareness of latex allergy by the world population may help to mitigate the risk of an increase in the incidence of NRLA. This is the first step toward not forgetting the lessons learned in the 1980s and 1990s.
In addition, despite there being reasonable data to support the use of latex SLIT, there is no commercially available latex extract in the USA, and in Europe the production of SLIT has been slowed down by the manufacturer, ALK Abello.
Because of these problems, determining the effectiveness and safety of the percutaneous route, although highlighted only in one case series, may be the strategy to follow to desensitize allergic patients, even if more randomized trials are needed.
The use of omalizumab, already supported by some scientific data, may provide an additional opportunity for therapeutic management, in association with immunotherapy. Further studies on a larger scale are needed to validate this new possible use of omalizumab and to evaluate the persistence of latex tolerability after discontinuation.
Conclusions
Prevention remains the gold-standard treatment for patients suffering from NRLA.107
However, the only etiological and decisive therapy able to influence the natural history of NRLA is specific desensitization. Rush protocols have provided evidence to suggest that effective doses of latex SLIT can be safely and rapidly achieved. Regrettably, there are several limitations to latex studies. The complexity of the clinical manifestations of NRLA continues to limit the power of these studies because patients with differing symptoms are often grouped together when exposed to specific challenge tests. In addition, sample sizes remain small. There is also a lack of long-term data (one case report) to suggest sustained efficacy after the cessation of SLIT.108
The current results show that the NRL SLIT is the only etiological method to resolve NRLA in at-risk patients who cannot avoid this allergen. Moreover, latex SLIT is characterized by a very low incidence of adverse reactions, good patient compliance and a high success rate. At the end of the immunotherapy, almost all patients are able to wear latex gloves, undergo medical examinations or surgery, and stay in environments where latex is present.
Although the tolerability of SLIT has allowed it to remain as the only potential immunotherapy modality, its safety continues to be closely monitored. For these reasons, further investigations in this field are necessary, especially regarding long-term tolerability, safety and efficacy, and the maintenance dosage to be adopted, as the literature still shows a wide variation.
Acknowledgments
The authors are responsible for the content and the writing of this paper.
Funding
The authors declare that no funding was received for the present review.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Dennis R, Ownby A. History of latex allergy. J Allergy Clin Immunol. 2002;110(2):S27–S32. doi:10.1067/mai.2002.125336
2. Stern G. Überempfindlichkeit gegen Kautschuk als ursache von Urticaria und quinckeschem odem. Klin Wochenschr. 1927;6:1096–1097.
3. Grimm A. Uberempfindlichtkeit gegen kautschuk als uorsache von urticaria und quinckeschem ödem. Klin Wochenschr. 1927;6:1479. doi:10.1007/BF01718534
4. Nutter AF. Contact urticaria to rubber. Br J Dermatol. 1979;101(5):597–598. doi:10.1111/j.1365-2133.1979.tb11893.x
5. Wu M, McIntosh J, Liu J. Current prevalence rate of latex allergy: why it remains a problem? J Occup Health. 2016;58:138–144. doi:10.1539/joh.15-0275-RA
6. Cremer R, Mennicken O. Longitudinal study on specific IgE against natural rubber latex, banana and kiwi in patients with spina bifida. Klin Padiatr. 2011;223(06):352–355. doi:10.1055/s-0031-1273752
7. Blumchen K, Bayer P, Buck D, et al. Effects of latex avoidance on latex sensitization, atopy and allergic diseases in patients with spina bifida. Allergy. 2010;65(12):1585–1593. doi:10.1111/j.1398-9995.2010.02447.x
8. Tomazic VJ, Shampaine EL, Lamanna A, Withrow TJ, Adkinson NF
9. Agarwal N, McDonnell S, Khan W. Management of latex hypersensitivity in the perioperative setting. J Perioper Pract. 2020;30(7–8):199–203. doi:10.1177/1750458919882222
10. Brehler R, Theissen U, Mohr C, Luger T. Latex‐fruit syndrome: frequency of cross‐reacting IgE antibodies. Allergy. 1997;52:404–410. doi:10.1111/j.1398-9995.1997.tb01019.x
11. Garcia Ortiz JC, Moyano JC, Alvarez M, Bellido J. Latex allergy in fruit‐allergic patients. Allergy. 1998;53:532–536. doi:10.1111/j.1398-9995.1998.tb04092.x
12. Werfel T, Asero R, Ballmer-Weber BK, et al. Position paper of the EAACI: food allergy due to immunological cross-reactions with common inhalant allergens. Allergy. 2015;70(9):1079–1090. doi:10.1111/all.12666
13. Shaffrali FC, Gawkrodger DG. Allergic contact dermatitis from natural rubber latex without immediate hypersensitivity. Contact Dermatitis. 1999;40:325–326. doi:10.1111/j.1600-0536.1999.tb06084.x
14. Leuzzi M, Vincenzi C, Sechi A, et al. Delayed hypersensitivity to natural rubber latex: does it exist or not? Contact Dermatitis. 2019;81(5):404–405. doi:10.1111/cod.13353
15. Alenius H, Kurup VP, Kelly KJ, Palosuo T, Turjanmaa K, Fink JN. Latex allergy: frequent occurrence of IgE antibodies to a cluster of 11 latex proteins in patients with spina bifida and histories of anaphylaxis. J Lab Clin Med. 1994;123(5):712–720.
16. Kurup VP, Alenius H, Kelly KJ, Castillo L, Fink JN. A two-dimensional electrophoretic analysis of latex peptides reacting with IgE and IgG antibodies from patients with latex allergy. Int Arch Allergy Immunol. 1996;109(1):58–67. doi:10.1159/000237232
17. Lu LJ, Kurup VP, Hoffman DR, Kelly KJ, Murali PS, Fink JN. Characterization of major latex allergen associated with hypersensitivity in spina bifida patients. J Immunol. 1995;155:2721–2728.
18. Bernstein DI, Biagini RE, Karnani R, et al. In vivo sensitization to purified Hevea brasiliensis proteins in health care workers sensitized to natural rubber latex. J Allergy Clin Immunol. 2003;111(3):610–616. doi:10.1067/mai.2003.164
19. Slater J, Vedvick T, Arthur-Smith A, Trybul DE, Kekwick RG. Identification, cloning, and sequence of a major allergen (Hev b 5) from natural rubber latex (Hevea brasiliensis). J Biol Chem. 1996;271(41):25394–25399. doi:10.1074/jbc.271.41.25394
20. Kotovuori A, Poikonen S, Niskanen E, et al. Isolated hevein-like domains, but not 31-kd endochitinases, are responsible for IgE mediated in vitro and in vivo reactions in latex-fruit syndrome. J Allergy Clin Immunol. 2005;115:598–605. doi:10.1016/j.jaci.2004.09.015
21. Blanco C, Diaz-Perales A, Collada C, et al. Class I chitinases as potential panallergenes involved in the latex-fruit syndrome. J Allergy Clin Immunol. 1999;103:507–513. doi:10.1016/S0091-6749(99)70478-1
22. Rolland M
23. Nucera E, Rizzi A, Buonomo A, et al. The clinical meaning of positive latex sige in patients with food/pollen adverse reactions. Int J Immunopathol Pharmacol. 2012;25(2):445–453. doi:10.1177/039463201202500214
24. Chen Z, Cremer R, Posch A, Raulf-Heimsoth M, Rihs HP, Baur X. On the allergenicity of Hev b 1 among health care workers and patients with spina bifida allergic to natural rubber latex. J Allergy Clin Immunol. 1997;100(5):684–769. doi:10.1016/s0091-6749(97)70174-x
25. Rihs HP, Sander I, Heimann H, Meurer U, Brüning T, Raulf M. The new latex allergen Hev b 15: IgE-binding properties of a recombinant serine protease inhibitor. J Investig Allergol Clin Immunol. 2015;25(2):133–162.
26. Woods JA, Lambert S, TAE P-M, Drake DB, Edlich R. Natural rubber latex allergy: spectrum, diagnostic approach, and therapy. J Emerg Med. 1997;15(1):71–85. doi:10.1016/s0736-4679(96)00256-9
27. Liccardi G, D’Amato G, Canonica W, Salzillo A, Piccolo A, Passalacqua G. Systemic reactions from skin testing: literature review. J Investig Allergol Clin Immunol. 2006;16(2):75–78.
28. Kelly KJ, Kurup VP, Zacharisen M, Resnick A, Fink JN. Skin and serologic testing in the diagnosis of latex allergy. J Allergy Clin Immunol. 1993;91:1140–1145.
29. Nicolaou N, Johnston GA. Anaphylaxis following prick testing with natural rubber latex. Contact Dermatitis. 2002;47:251–252. doi:10.1034/j.1600-0536.2002.470422.x
30. Nettis E, Dambra P, Traetta PL, Loria MP, Ferranini A, Tursi A. Systemic reactions on SPT to latex. Allergy. 2001;56:355–356. doi:10.1034/j.1398-9995.2001.00862.x
31. Van Kampen V, Raulf-Heimsoth M, Sander I, Merget R. Diagnostics of occupational type I allergies-comparison of skin prick test solutions from different manufacturers for selected occupational allergens. Pneumologie. 2010;64(5):271–277.
32. Bendewald MJ, Farmer SA, Davis MD. An 8-year retrospective review of patch testing with rubber allergens: the mayo clinic experience. Dermatitis. 2010;21(1):33–40. doi:10.2310/6620.2009.09029
33. Ebo DG, Bridts CH, Rihs HP. Hevea latex associated allergies: piecing together the puzzle of the latex IgE reactivity profile. Expert Rev Mol Diagn. 2020;20(4):367–373. doi:10.1080/14737159.2020.1730817
34. Nowakowska-Świrta E, Wiszniewska M, Walusiak-Skorupa J. Allergen-specific IgE to recombinant latex allergens in occupational allergy diagnostics. J Occup Health. 2019;61(5):378–386. doi:10.1002/1348-9585.12064
35. Sanz ML, García-Avilés MC, Tabar AI, et al. Basophil activation test and specific IgE measurements using a panel of recombinant natural rubber latex allergens to determine the latex allergen sensitization profile in children. Pediatr Allergy Immunol. 2006;17(2):148–156. doi:10.1111/j.1399-3038.2005.00359.x
36. Agache I, Bilò MB, Braunstahl GJ, et al. In vivo diagnosis of allergic diseases–allergen provocation tests. Allergy. 2015;70(4):355–365. doi:10.1111/all.12586
37. Nucera E, Pollastrini E, Sabato V, et al. Challenge tests in the diagnosis of latex allergy. Int J Immunopathol Pharmacol. 2010;23(2):543–552. doi:10.1177/039463201002300216
38. Vandenplas O, Suojalehto H, Aasen TB, et al. Specific inhalation challenge in the diagnosis of occupational asthma: consensus statement. Eur Respir J. 2014;43(6):
39. Chelminska M, Niedoszytko M, Jassem E. Clinical value of conjunctival allergen challenge in diagnosing allergic conjunctivitis related to latex. Int Arch Allergy Immunol. 2011;154(2):
40. Cabañes N, Igea JM, de la Hoz B, et al. Latex allergy: position paper. J Investig Allergol Clin Immunol. 2012;22(5):313–330.
41. Bernstein DI. Management of natural rubber latex allergy. J Allergy Clin Immunol. 2002;110(2):S111. doi:10.1067/mai.2002.125330
42. Palosuo T, Antoniadou I, Gottrup F, Phillips P. Latex medical gloves: time for a reappraisal. Int Arch Allergy Immunol. 2011;156:234–246. doi:10.1159/000323892
43. Kelly KJ, Wang ML, Klancnik M, Petsonk EL. Prevention of IgE sensitization to latex in health care workers after reduction of antigen exposures. J Occup Environ Med. 2011;53(8):934–940. doi:10.1097/JOM.0b013e31822589dc
44. Allergen nomenclature. Available from: http://www.allergen.org/search.php?allergensource=Hevea+brasiliensis . Accessed September 17, 2020.
45. Vandenplas O, Raulf M. Occupational latex allergy: the current state of affairs. Curr Allergy Asthma Rep. 2017;17(3):14. doi:10.1007/s11882-017-0682-5
46. Korniewicz DM, Chookaew N, El-Masri M, Mudd K, Bollinger ME. Conversion to low-protein, powder-free surgical gloves: is it worth the cost? Am Assoc Occup Health Nurses. 2005;53(9):388–393.
47. Yip E, Cacioli P. The manufacture of gloves from natural rubber latex. J Allergy Clin Immunol. 2002;110(Suppl 2):S3–14. doi:10.1067/mai.2002.124499
48. Critchley E, Pemberton MN. Latex and synthetic rubber glove usage in UK general dental practice: changing trends. Heliyon. 2020;6(5):e03889.
49. Raulf M. Current state of occupational latex allergy. Curr Opin Allergy Clin Immunol. 2020;20(2):112–116. doi:10.1097/ACI.0000000000000611
50. Cornish K. Assessment of the risk of type I latex allergy sensitization or reaction during use of products made from latex derived from guayule and other alternative rubber producing species. Rubber Sci. 2012;25:139–155.
51. Caballero ML, Quirce S. Identification and practical management of latex allergy in occupational settings. Expert Rev Clin Immunol. 2015;11(9):977–992. doi:10.1586/1744666X.2015.1059754
52. Crepy MN. Rubber: new allergens and preventive measures. Eur J Dermatol. 2016;26(6):523–530. doi:10.1684/ejd.2016.2839
53. CDC’s recommendations on the use of PPE during the COVID-19 outbreak. Available from: https://www.cdc.gov/coronavirus/2019-ncov/infection-control/controlrecommendations.html.
54. Food and Drug Administration. Enforcement policy for gowns, other apparel, and gloves during the Coronavirus Disease (COVID–19) public health emergency. Guidance for Industry and Food and Drug Administration Staff (March 2020). Docket Number FDA–2020–D–1138. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/enforcement-policy-gowns-other-apparel-and-gloves-during-coronavirus-disease-covid-19-public-health.
55. Food and Drug Administration. Process for Making Available Guidance Documents Related to Coronavirus Disease. 2019. Available from: https://www.govinfo.gov/content/pkg/FR-2020-03-25/pdf/2020-06222.pdf.
56. Allmers H, Schmengler J, Skudlik C. Primary prevention of natural rubber latex allergy in the German health care system through education and intervention. J Allergy Clin Immunol. 2002;110(2):318–323. doi:10.1067/mai.2002.126461
57. Nieto A, Mazon A, Pamies R, et al. Efficacy of latex avoidance for primary prevention of latex sensitization in children with spina bifida. J Pediatr. 2002;140(3):370–372. doi:10.1067/mpd.2002.122732
58. Cremer R, Kleine-Diepenbruck U, Hering F, Holschneider AM. Reduction of latex sensitization in spina bifida patients by a primary prophylaxis programme (five years experience). Eur J Pediatr Surg. 2002;12:S19–S21. doi:10.1055/s-2002-36866
59. Stinkens R, Verbeke N, Van de Velde M, et al. Safety of a powder-free latex allergy protocol in the operating theatre: a prospective, observational cohort study. Eur J Anaesthesiol. 2019;36(4):312–313. doi:10.1097/EJA.0000000000000953
60. American Society of Anesthesiologists Committee on Occupational Health of Operating Room Personnel. Natural Ruber Latex Allergy: Considerations for Anesthesiologists. Park Ridge, IL: American Society of Anesthesiologists; 2005.
61. Australasian Society of Clinical Immunology and Allergy. ASCIA Guidelines – Management of Latex-Allergic Individuals. Balgowlah NSW: Australasian Society of Clinical Immunology and Allergy; 2010.
62. Sussman GL, Lem D, Liss G, Beezhold D. Latex allergy in housekeeping personnel. Ann Allergy Asthma Immunol. 1995;74:415–418.
63. Sanguanchaiyakrit N, Povey AC, de Vocht F. Personal exposure to inhalable dust and the specific latex aero-allergen, Hev b6.02, in latex glove manufacturing in Thailand. Ann Occup Hyg. 2014;58:542–550. doi:10.1093/annhyg/meu013
64. Havmose M, Thyssen JP, Zachariae C, Johansen JD. Use of protective gloves by hairdressers: a review of efficacy and potential adverse effects. Contact Dermatitis. 2020;83(2):75–82. doi:10.1111/cod.13561
65. Madan I, Cullinan P, Ahmed SM. Occupational management of type I latex allergy. Occup Med. 2013;63(6):395–404. doi:10.1093/occmed/kqt055
66. Crepy MN, Lecuen J, Ratour-Bigot C, Stocks J, Bensefa-Colas L. Accelerator-free gloves as alternatives in cases of glove allergy in healthcare workers. Contact Dermatitis. 2018;78(1):28–32. doi:10.1111/cod.12860
67. Gentili A, Lima M, Ricci G, et al. Secondary prevention of latex allergy in children: analysis of results. Pediatr Med Chir. 2006;28:83.
68. Reider N, Kretz B, Menardi G, Ulmer H, Fritsch P. Outcome of a latex avoidance program in a high‐risk population for latex allergy – a five‐year follow‐up study. Clin Exp Allergy. 2002;32(5):708–713. doi:10.1046/j.1365-2222.2002.01390.x
69. Crippa M, Belleri L, Mistrello G, Tedoldi C, Alessio L. Prevention of latex allergy among health care workers and in the general population: latex protein content in devices commonly used in hospitals and general practice. Int Arch Occup Environ Health. 2006;79(7):550–557. doi:10.1007/s00420-005-0080-5
70. Emergency treatment of anaphylactic reactions. Guidelines for healthcare providers. Working Group of the Resuscitation Council (UK). 2016. Available from: www.resus.org.uk.
71. Truhlář A, Deakin CD, Soar J, et al. Cardiac arrest in special circumstances section collaborators. European resuscitation council guidelines for resuscitation 2015: section 4. Cardiac arrest in special circumstances. Resuscitation. 2015;95:148–201. doi:10.1016/j.resuscitation.2015.07.017
72. Kraft M, Dölle-Bierke S, Turner PJ, et al. EAACI task force clinical epidemiology of anaphylaxis: experts’ perspective on the use of adrenaline autoinjectors in Europe. Clin Transl Allergy. 2020;10(1):12. doi:10.1186/s13601-020-00317-y
73. Noon L. Prophylactic inoculation against hay fever. Lancet. 1911;1:1572–1573. doi:10.1016/S0140-6736(00)78276-6
74. Freeman J. Further observation on the treatment of hay-fever by hypodermic inoculation of pollen vaccine. Lancet. 1911;2:814–817. doi:10.1016/S0140-6736(01)40417-X
75. Ring J, Gutermuth J. 100 years of hyposensitization: history of allergen-specific immunotherapy (ASIT). Allergy. 2011;66(6):713–724. doi:10.1111/j.1398-9995.2010.02541.x
76. Nucera E, Schiavino D, Pollastrini E, et al. Desensitization to latex by percutaneous route. J Investig Allergol Clin Immunol. 2002;12:134–135.
77. Patriarca G, Nucera E, Buonomo A, et al. Latex allergy desensitization by exposure protocol: five case reports. Anesth Analg. 2002;94:754–758.
78. Pereira C, Rico P, Lourenço M, Lombardero M, Pinto-Mendes J, Chieira C. Specific immunotherapy for occupational latex allergy. Allergy. 1999;54:291–293. doi:10.1034/j.1398-9995.1999.00954.x
79. Leynadier F, Herman D, Vervloet D, Andre C. Specific immunotherapy with a standardized latex extract versus placebo in allergic healthcare workers. J Allergy Clin Immunol. 2000;106(3):585–590. doi:10.1067/mai.2000.109173
80. Sastre J, Fernández-Nieto M, Rico P. Specific immunotherapy with a standardized latex extract in allergic workers: a double-blind, placebo-controlled study. J Allergy Clin Immunol. 2003;111(5):985–994. doi:10.1067/mai.2003.1390
81. Tabar AI, Anda M, Bonifazi F, et al. Specific Immunotherapy with standardized latex extract versus placebo in latex-allergic patients. Int Arch Allergy Immunol. 2006;141(4):369–376. doi:10.1159/000095463
82. Nucera E, Schiavino D, Buonomo A, et al. Latex rush desensitization. Allergy. 2001;56:86–87. doi:10.1034/j.1398-9995.2001.00904.x
83. Smith DM, Freeman TM. Sublingual immunotherapy for other indications: venom large local, latex, atopic dermatitis, and food. Immunol Allergy Clin North Am. 2020;40(1):41–57. doi:10.1016/j.iac.2019.09.011
84. Nettis E, Delle Donne P, Di Leo E, et al. Latex immunotherapy: state of the art. Ann Allergy Asthma Immunol. 2012;109(3):160–165. doi:10.1016/j.anai.2012.07.004
85. Patriarca G, Nucera E, Roncallo C, et al. Sublingual desensitization: a new approach to latex allergy problem. Anesth Analg. 2002;95:956–960. doi:10.1097/00000539-200210000-00031
86. Cistero Bahima A, Sastre J, Enrique E, et al. Tolerance and effects on skin reactivity to latex of sublingual rush immunotherapy with a latex extract. J Investig Allergol Clin Immunol. 2004;14:17–25.
87. Antico A, Pagani M, Crema A. Anaphylaxis by latex sublingual immunotherapy. Allergy. 2006;61(10):1236–1237. doi:10.1111/j.1398-9995.2006.01155.x
88. Nettis E, Colanardi MC, Soccio AL, et al. Double-blind, placebo-controlled study of sublingual immunotherapy in patients with latex-induced urticaria: a 12-month study. Br J Dermatol. 2007;156(4):674–681. doi:10.1111/j.1365-2133.2006.07738.x
89. Bernardini R, Campodonico P, Burastero S, et al. Sublingual immunotherapy with a latex extract in paediatric patients: a double-blind, placebo-controlled study. Curr Med Res Opin. 2006;22(8):1515–1522. doi:10.1185/030079906X115711
90. Bernardini R, Pecora S, Milani M, Burastero SE. Natural rubber latex allergy in children: clinical and immunological effects of 3-years sublingual immunotherapy. Eur Ann Allergy Clin Immunol. 2008;40(4):142–147.
91. Nucera E, Schiavino D, Pollastrini E, et al. Sublingual desensitization in children with congenital malformations and latex. Allergy Pediatr Allergy Immunol. 2006;17(8):606–612. doi:10.1111/j.1399-3038.2006.00458.x
92. Nucera E, Schiavino D, Sabato V, et al. Sublingual immunotherapy for latex allergy: tolerability and safety profile of rush build-up phase. Curr Med Res Opin. 2008;24(4):1147–1154. doi:10.1185/030079908X291903
93. Buyukozturk S, Gelincik A, Ferhan F, Colakoğlu B, Dal M. Latex sublingual immunotherapy: can its safety be predicted? Ann Allergy Asthma Immunol. 2010;104:339–342. doi:10.1016/j.anai.2010.01.014
94. Lasa Luaces EM, Tabar Purroy AI, García Figueroa BE, et al. Component-resolved immunologic modifications, efficacy, and tolerance of latex sublingual immunotherapy in children. Ann Allergy Asthma Immunol. 2012;108(5):367–372. doi:10.1016/j.anai.2012.03.005
95. Nucera E, Mezzacappa S, Buonomo A, et al. Latex immunotherapy: evidence of effectiveness. Postepy Dermatol Alergol. 2018;35(2):145–150. doi:10.5114/ada.2018.75235
96. Morfin Maciel BM, Castillo Morfin BM. Failure of sublingual immunotherapy to treat latex allergy. A report of a case. Rev Alerg Mex. 2008;55(2):76–81.
97. Gastaminza G, Algorta J, Uriel O, et al. Randomized, double-blind, placebo controlled clinical trial of sublingual immunotherapy in natural rubber latex allergic patients. Trials. 2011;12:191. doi:10.1186/1745-6215-12-191
98. Nucera E, Urbani S, Buonomo A, Andriollo G, Aruanno A. Eosinophilic Esophagitis during latex desensitization. J Investig Allergol Clin Immunol. 2020;30(1):61–63. doi:10.18176/jiaci.0440
99. Alfredo J, Lucendo AJ, Arias A, Tenias JM. Relation between eosinophilic esophagitis and oral immunotherapy for food allergy: a systematic review with meta-analysis. Ann Allergy Asthma Immunol. 2014;113:624–629. doi:10.1016/j.anai.2014.08.004
100. Yoshimichi O, Hisako M, Hiroshi O, Shunsuke T, Kimihiro MH. Roles of Omalizumab in various allergic diseases. Allergol Int. 2020;69(2):167–177. doi:10.1016/j.alit.2020.01.004
101. Incorvaia C, Mauro M, Makri E, Leo G, Ridolo E. Two decades with omalizumab: what we still have to learn. Biologics. 2018;12:135–142. doi:10.2147/BTT.S180846
102. Leynadier F, Doudou O, Gaouar H, et al. Effect of omalizumab in healthcare workers with occupational latex allergy. J Allergy Clin Immunol. 2004;113:360–361. doi:10.1016/j.jaci.2003.11.020
103. Di Leo E, Calogiuri G, Macchia L, Nettis E. Use of omalizumab in uncontrolled chronic spontaneous urticaria also improved latex-induced contact urticaria. J Allergy Clin Immunol Pract. 2019;7(1):300–302. doi:10.1016/j.jaip.2018.05.005
104. Aruanno A, Chini R, Nucera E. Efficacy of omalizumab in reducing latex allergy. Postepy Dermatol Alergol. 2020.
105. Dantzer JA, Wood RA. The use of omalizumab in allergen immunotherapy. Clin Exp Allergy. 2018;48(3):232–240. doi:10.1111/cea.13084
106. Hu K, Fan J, Li X, Gou X, Li X, Zhou X. The adverse skin reactions of health care workers using personal protective equipment for COVID-19. Medicine. 2020;99(24):e20603. doi:10.1097/MD.0000000000020603
107. Raulf M. The latex story. Chem Immunol Allergy. 2014;100:248–255.
108. Pecora V, Aruanno A, Buonomo A, et al. Sublingual immunotherapy with natural rubber latex: a case report with 8-year follow-up. Contact Dermatitis. 2010;63(1):53–54. doi:10.1111/j.1600-0536.2010.01746.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.