Back to Journals » Patient Preference and Adherence » Volume 20
Latent Profiles and Associated Factors of Health Problem-Solving Ability in Patients with Coronary Heart Disease: A Cross-Sectional Study
Authors Hou Q, Xing Q, Duan M, Lan Y
Received 31 March 2026
Accepted for publication 2 June 2026
Published 9 June 2026 Volume 2026:20 613032
DOI https://doi.org/10.2147/PPA.S613032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Qindi Hou, Qiaohong Xing, Meiyi Duan, Yanli Lan
School of Nursing, Gannan Medical University, Ganzhou, Jiangxi, People’s Republic of China
Correspondence: Yanli Lan, School of Nursing, Gannan Medical University, Hexie Avenue No. 1, Ganzhou, Jiangxi, 341000, People’s Republic of China, Email [email protected]
Purpose: To explore the latent profile characteristics of health problem-solving ability in coronary heart disease (CHD) patients and analyze their demographic and clinical determinants, providing empirical evidence for tailored transitional care.
Patients and Methods: A cross-sectional study was conducted among 381 hospitalized CHD patients recruited via convenience sampling from the cardiovascular department of a tertiary hospital in Ganzhou, Jiangxi Province, China, between November 2025 and March 2026. Data were collected using a sociodemographic questionnaire, Health Problem-Solving Scale (HPSS), Cardiac Self-Efficacy Scale (CSES), Coronary Artery Disease Education Questionnaire Short Version (CADE-Q SV), and Perceived Social Support Scale (PSSS). Subgroups were identified via LPA using Mplus 8.3. Multinomial logistic regression explored associated factors using SPSS 27.0.
Results: The mean HPSS score was 13.65 ± 4.84. LPA identified three distinct profiles: Rational-Active Coping (26.8%), Ambivalent-Passive Adaptation (52.2%), and Negative-Impulsive Avoidance (21.0%). Compared to the Rational-Active Coping profile, higher perceived social support (OR=0.897) and self-efficacy (OR=0.825) were independent protective factors against the Ambivalent-Passive Adaptation profile (both P < 0.01). Furthermore, poorer disease knowledge (OR=0.796), lower perceived social support (OR=0.785), and diminished self-efficacy (OR=0.681) emerged as significant independent risk factors for the Negative-Impulsive Avoidance profile.
Conclusion: CHD patients exhibit significant heterogeneity in health problem-solving ability. Profiling these patients provides a practical framework for personalized clinical management. Healthcare providers could target the “Negative-Impulsive” and “Ambivalent-Passive” groups. Enhancing disease knowledge, social support, and self-efficacy can promote active problem-solving, thereby optimizing self-management and long-term clinical outcomes.
Keywords: coronary heart disease, latent profile analysis, health problem-solving, self-efficacy
Introduction
Coronary heart disease (CHD) remains a leading cause of cardiovascular morbidity and mortality globally, necessitating long-term and effective disease management.1 Following discharge, effective self-management serves as a critical determinant of disease recurrence, readmission rates, and long-term quality of life.2 However, secondary prevention for CHD remains a global challenge. Recent large-scale international registries (eg., EUROASPIRE V and INTERASPIRE) indicate that a considerable proportion of patients still face difficulties in achieving cardiovascular risk targets and maintaining long-term lifestyle modifications.3,4 This ongoing challenge suggests that effective daily self-management is a complex process, and traditional health education alone may not fully address the practical needs of patients in their daily lives.
In clinical practice, significant disparities in self-management are often observed when individuals navigate complex situations, such as symptom fluctuations, medication adjustments, or lifestyle modifications.5,6 To better address these challenges, successful home-based self-management is highly contingent on a patient’s “health problem-solving ability”—a comprehensive cognitive process involving the identification of health threats, formulation of strategies, evaluation of outcomes, and subsequent behavioral adjustment.7,8 Proficient problem-solving fosters rational disease management; conversely, avoidant or impulsive strategies significantly elevate the risk of adverse cardiovascular events.9–11
Despite its importance, much of the current literature tends to focus on conditions such as diabetes, leaving health problem-solving within the CHD population relatively underexplored.12 Furthermore, previous studies have largely treated patients as a homogeneous group through mean-centric analyses, thereby neglecting unobserved heterogeneity and latent clustering in individual coping strategies.8
In light of these considerations, the present study is grounded in Hill-Briggs’ problem-solving model of chronic illness self-management, which posits that problem-solving efficacy is driven by internal factors (eg., knowledge, self-efficacy) and external resources (eg., social support).13
To better capture the complex nature of health problem-solving, we employed Latent Profile Analysis (LPA), a person-centered approach, to identify unobserved heterogeneity and distinct latent patterns among the CHD population.14 The specific aims of this study were: (1) to identify these distinct latent profiles; and (2) to examine how the aforementioned internal and external factors predict profile membership. We hypothesized that: (1) distinct, identifiable latent profiles of problem-solving ability exist within this population; and (2) higher levels of disease knowledge, self-efficacy, and social support would be associated with membership in high-performing problem-solving profiles. Ultimately, this study endeavors to provide empirical evidence to inform targeted transitional care interventions for CHD patients.
Material and Methods
Study Design and Participants
A cross-sectional study utilizing convenience sampling was conducted in the cardiovascular departments of a tertiary Grade-A hospital in Ganzhou, Jiangxi Province, China, between November 2025 and March 2026. Inclusion criteria were: (1) a confirmed clinical diagnosis of CHD in a relatively stable condition;15 (2) consciousness with basic reading and communication capacities; and (3) voluntary provision of informed consent. Patients were excluded if they presented with severe hepatic or renal dysfunction, severe sequelae of cerebrovascular accidents, or significant cognitive/psychiatric disorders. Based on Kendall’s rule of thumb (5 to 10 cases per independent variable), we counted a total of 27 variables in our analysis: 12 sociodemographic items and 15 dimensions across the four scales used. Factoring in a 20% potential rate for invalid questionnaires and attrition, the required sample size was calculated to range from 169 to 338. Our final sample of 381 patients effectively exceeded this threshold, ensuring adequate statistical power.16 After a strict review to exclude questionnaires with patterned responses or missing information, 381 valid questionnaires were ultimately recovered, yielding an effective response rate of 93.02%.
Measures
Sociodemographic and Clinical Characteristics
A self-designed questionnaire captured patient data, including gender, age, residence, educational level, employment status, marital status, monthly per capita family income, smoking/drinking status, number of comorbidities, and history of percutaneous coronary intervention (PCI).
Health Problem-Solving Scale (HPSS)
The HPSS, originally developed by Hill-Briggs et al13 and adapted by Wang et al,17 was used to assess health problem-solving abilities Extended from diabetes to cardiovascular populations (eg., hypertension),18 the scale evaluates six dimensions—rational/effective, positive/forward transfer, avoidance, impulsive/careless, negative transfer, and negative motivation—using a 5-point Likert scale (0–4). A transformed total score (range: 0–24) is calculated using the formula: Total Score = (Rational / 5) + (Positive Transfer / 6) + [(20 - Avoidance) / 5] + [(20 - Impulsive) / 5] + [(16 - Negative Transfer) / 4] + [(20 - Negative Motivation) / 5]. Higher scores reflect stronger capabilities. In this study, the overall Cronbach’s α coefficient was 0.70, and those for the six dimensions ranged from 0.80 to 0.94.
Cardiac Self-Efficacy Scale (CSES)
Self-efficacy was measured using the Chinese version of the CSES, originally compiled by Sullivan19 and translated by Xie.20 It comprises 16 items divided into two dimensions: symptom control and maintain function. Each item is rated on a 5-point Likert scale (0–4), yielding a total score from 0 to 64. Higher scores represent higher levels of self-efficacy in disease management. The Cronbach’s α coefficient in the current study was 0.963.
Coronary Artery Disease Education Questionnaire Short Version (CADE-Q SV)
Disease-related knowledge was assessed using the Chinese version of the CADE-Q SV, originally developed by Ghisi21 as a validated, disease-specific short-form instrument for coronary patients, and translated by Li et al22 The questionnaire includes 20 items covering five domains: medical condition, risk factors, exercise, nutrition, and psychosocial risk. Correct answers are scored as 1, while incorrect or “I don’t know” responses are scored as 0 (total score range: 0–20). Higher scores indicate better mastery of CHD knowledge. The Cronbach’s α coefficient in this study was 0.853.
Perceived Social Support Scale (PSSS)
The PSSS, developed by Zimet,23 and revised by Jiang in China,24 was used to evaluate patients’ perceived social support. It consists of 12 items assessing support from family, friends, and significant others. Responses are recorded on a 7-point Likert scale (total score range: 12–84), with higher scores reflecting greater perceived social support. The Cronbach’s α coefficient in this study was 0.975.
Data Collection and Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of The First Affiliated Hospital of Gannan Medical University (Approval No.: LLSC-2025567). All procedures were performed in strict compliance with relevant institutional guidelines and regulations. Prior to the investigation, all eligible patients were informed about the study’s purpose, procedures, and their right to withdraw at any time. Written informed consent was obtained from all participants. Data were collected face-to-face in the wards. To counteract potential investigator-induced bias and ensure strict standardization, all data administrators completed prerequisite training to align their screening protocols and the delivery of survey instructions. To mitigate social desirability bias, the surveys were intentionally conducted in a private bedside setting. In instances where participants required clarification on ambiguous items, researchers repeated the text exactly as written, deliberately refraining from providing any subjective elaborations or suggestive guidance. Questionnaires were distributed and recovered immediately on-site to preserve data completeness.Prior to the formal study, a preliminary pilot test was conducted among CHD patients to verify the scale’s comprehensibility and clinical applicability, with no modifications made to the original items.
Statistical Analysis
Analyses were performed using SPSS 27.0 and Mplus 8.3. Missing data were handled using complete case analysis, where questionnaires with incomplete sociodemographic information or missing responses to scale items were excluded from the final analysis. LPA was executed via Mplus to identify unobserved subgroups of health problem-solving abilities. Model fit was evaluated using AIC, BIC, aBIC, Entropy, LMRT, and BLRT. Group differences in general characteristics were assessed using ANOVA or Chi-square tests. Pearson correlation analyzed relationships among continuous variables. Prior to the regression analysis, multicollinearity among the independent variables was assessed using the Variance Inflation Factor (VIF). Variables with VIF < 5 were considered free of severe multicollinearity. Significant variables from univariate analyses were subsequently entered into a multinomial logistic regression model to identify independent predictors of the latent profiles. Statistical significance was set at a two-tailed P < 0.05.
Results
Participant Characteristics and HPSS Scores
The sample comprised 381 CHD patients (65.9% male) with a mean age of 64.43 ± 11.23 years. The overall mean HPSS score was 13.65 ± 4.84, indicating a suboptimal level of problem-solving ability. Among the sub-dimensions, positive/forward transfer scored the highest (mean item score: 2.38 ± 0.86), followed by rational/effective (2.20 ± 0.92). Conversely, negative dimensions (avoidance, impulsive/careless, negative transfer, and negative motivation) yielded lower mean item scores ranging from 1.56 to 2.00 (Table 1).
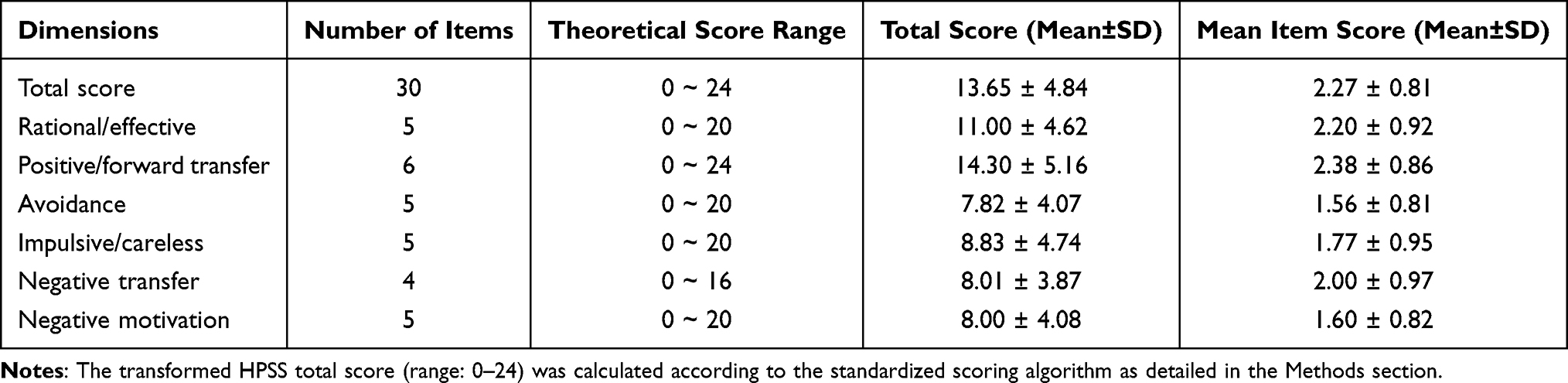 |
Table 1 Scores of Health Problem-Solving Ability and Its Dimensions (n=381) |
Latent Profile Analysis of Health Problem-Solving Ability
To determine the optimal number of latent profiles, models ranging from one to five classes were sequentially estimated (Table 2). Although the AIC, BIC, and aBIC values continued to decrease with additional profiles, the 5-profile model yielded a non-significant LMRT (P = 0.2628). Although the 4-profile model demonstrated acceptable statistical fit, the additional profile primarily represented a quantitative split of the intermediate subgroup without clear conceptual distinction. Moreover, one subgroup accounted for fewer than 10% of the sample (8.9%), potentially compromising profile stability.14 Therefore, considering statistical fit, parsimony, stability, and clinical interpretability, the 3-profile solution (Entropy = 0.950; LMRT and BLRT, both P < 0.001) was retained.
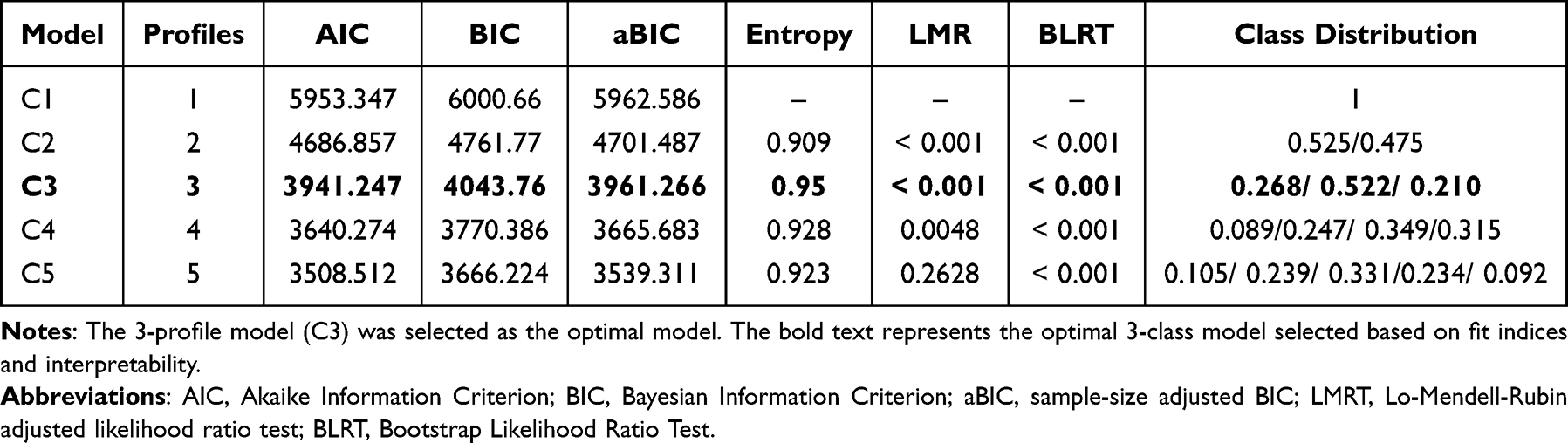 |
Table 2 Fit Indices of the Latent Profile Models for Health Problem-Solving Ability |
Based on the dimensional scoring patterns (Figure 1), Profile 1 (Rational-Active Coping, n=102, 26.8%) was characterized by prominent scores in rational/effective and positive/forward transfer dimensions, alongside the lowest scores across all negative dimensions. Conversely, Profile 3 (Negative-Impulsive Avoidance, n=80, 21.0%) demonstrated the opposite pattern, exhibiting significantly elevated scores in negative motivation, impulsive/careless, avoidance, and negative transfer. Profile 2 (Ambivalent-Passive Adaptation, n=199, 52.2%) served as a transitional group, demonstrating intermediate scores across all evaluated dimensions.
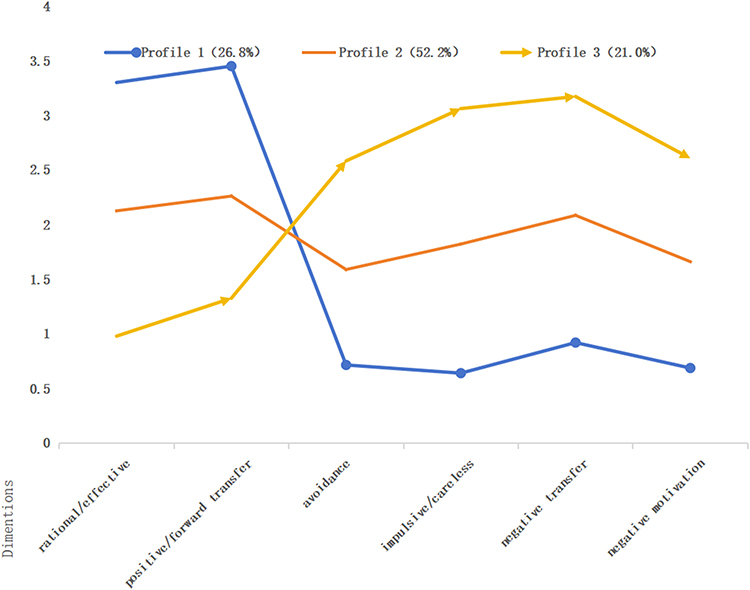 |
Figure 1 Latent profile characteristics of health problem solving in patients with coronary heart disease. |
Univariate and Correlation Analyses
Univariate analyses (Table 3) revealed that profile membership was significantly associated with several sociodemographic factors—including residence, educational level, employment, drinking status, and monthly income—as well as clinical burdens such as the number of comorbidities (all P < 0.05 or P < 0.01). Additionally, Pearson correlations (Table 4) demonstrated that patients with higher disease knowledge, stronger perceived social support, and greater self-efficacy exhibited significantly better overall health problem-solving scores (all P < 0.01).
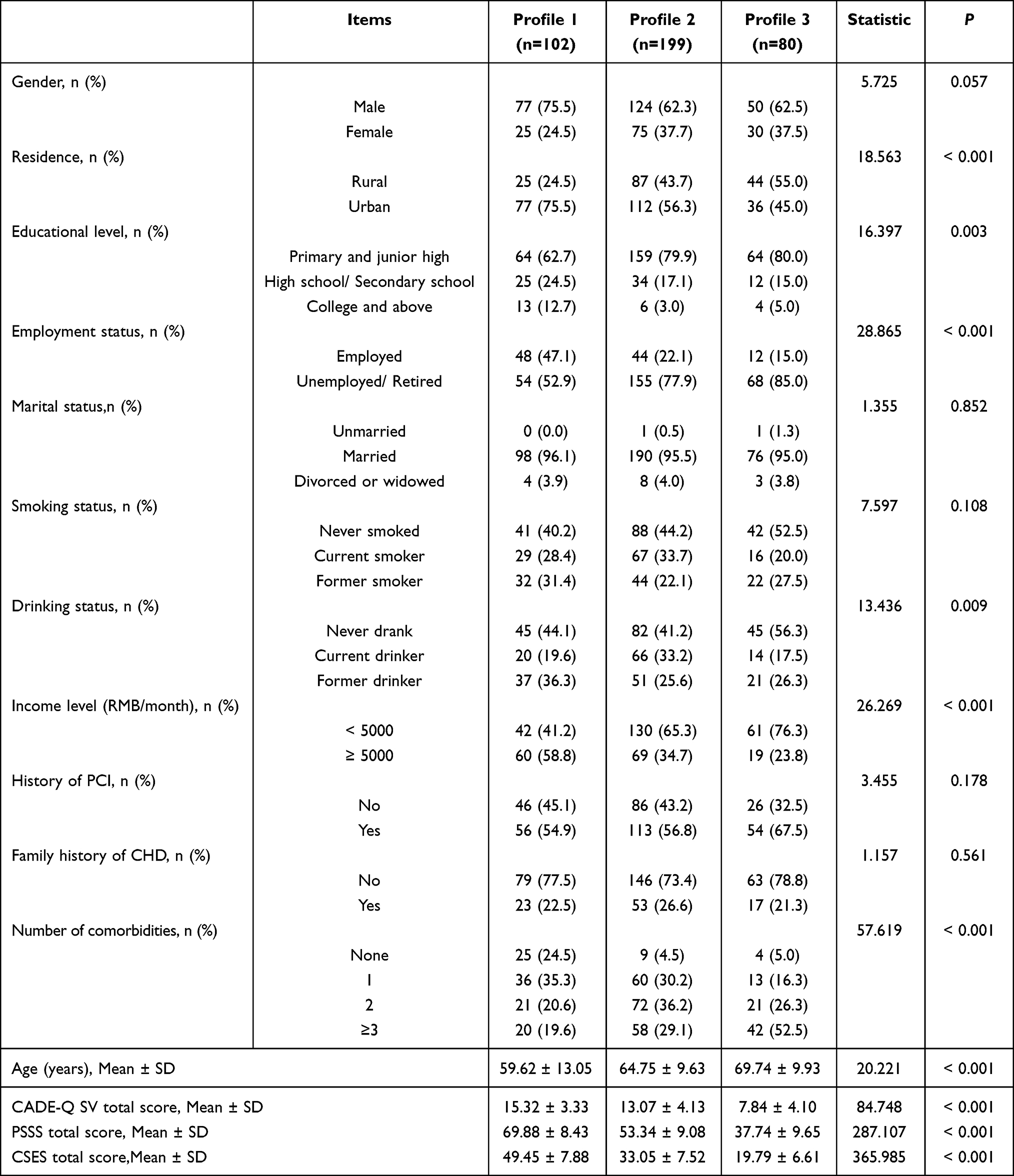 |
Table 3 Univariate Analysis of Characteristics Across the Three Latent Profiles |
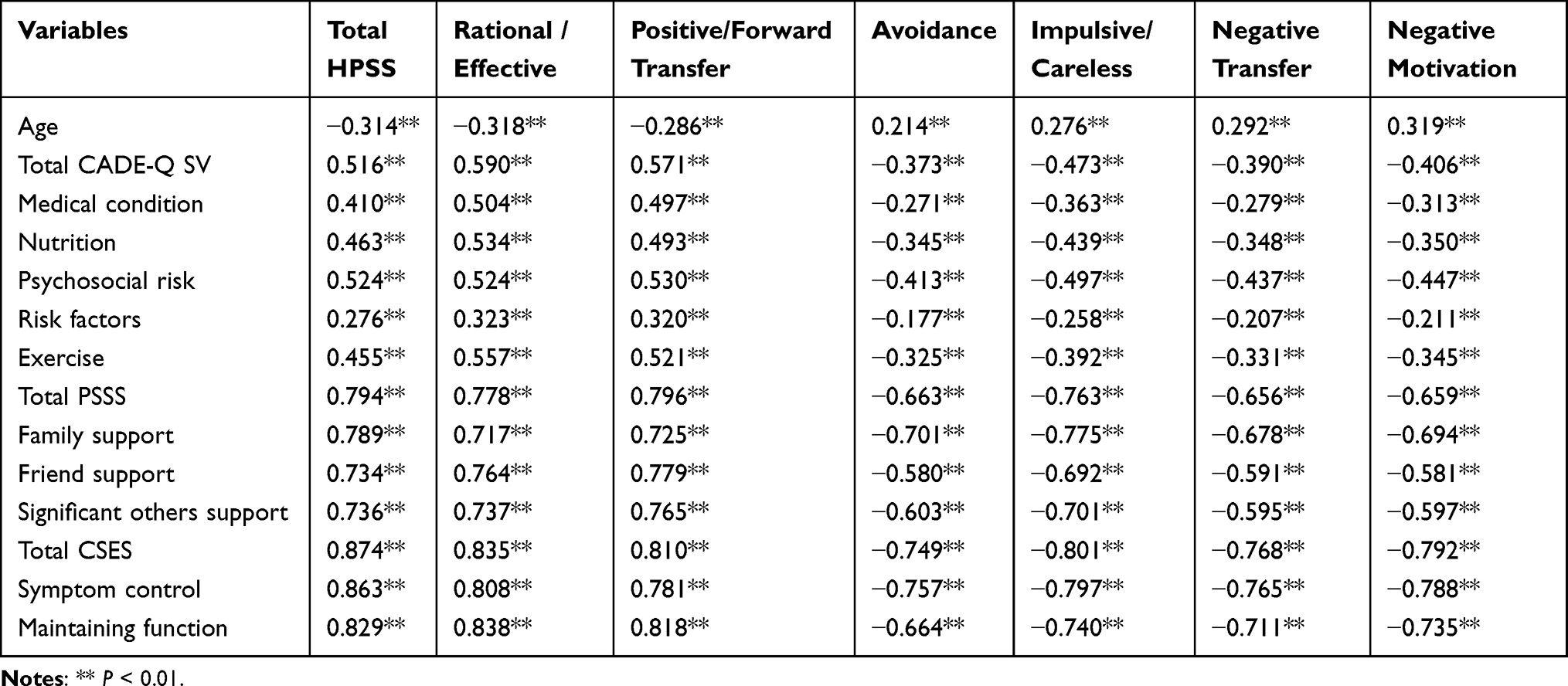 |
Table 4 Correlations Between Health Problem-Solving Ability and Other Continuous Variables |
Multinomial Logistic Regression Analysis
A multinomial logistic regression model was constructed using the three latent profiles as the dependent variable, with the “Rational-Active Coping” profile serving as the reference group. Variables that were statistically significant in the univariate and correlation analyses were incorporated as independent variables (assignments detailed in Table 5). Prior to regression analysis, multicollinearity diagnostics confirmed that no severe multicollinearity existed among the independent variables, with Variance Inflation Factor (VIF) values ranging from 1.085 to 2.795 (all below 5). The model demonstrated an excellent overall fit (x2 = 500.414, P < 0.001, Nagelkerke R2 = 0.840). As shown in Table 6, higher perceived social support (OR = 0.897, 95% CI: 0.843–0.954) and greater self-efficacy (OR = 0.825, 95% CI: 0.767–0.888) were significant protective factors negatively associated with classification into the Ambivalent-Passive Adaptation profile. Conversely, lower disease knowledge (OR = 0.796), lower perceived social support (OR = 0.785), and lower self-efficacy (OR = 0.681) were identified as independent factors positively associated with the Negative-Impulsive Avoidance profile. In addition, a lower educational level (primary and junior high vs. college and above; OR = 0.031, P = 0.019) exhibited a significant inverse association in this adjusted model.
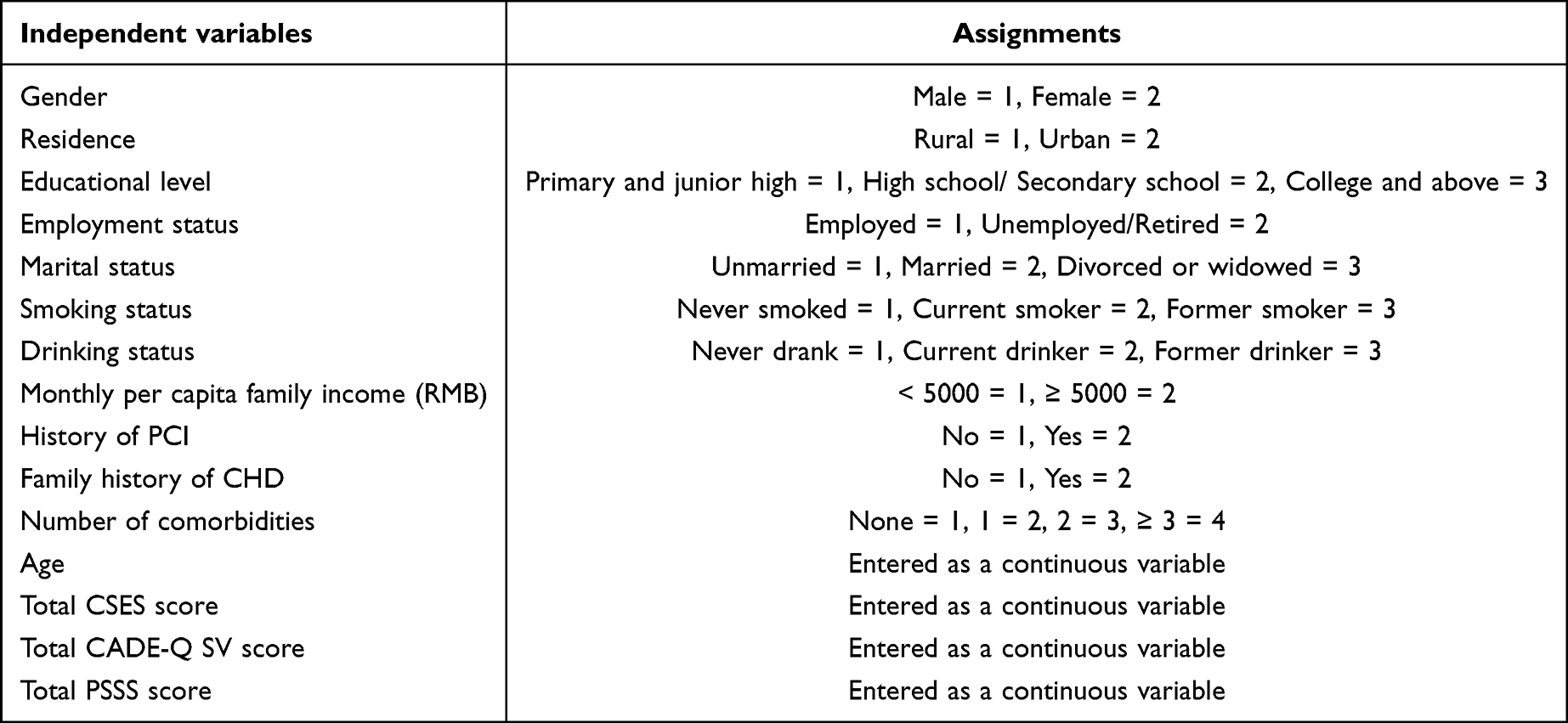 |
Table 5 Assignments of Independent Variables |
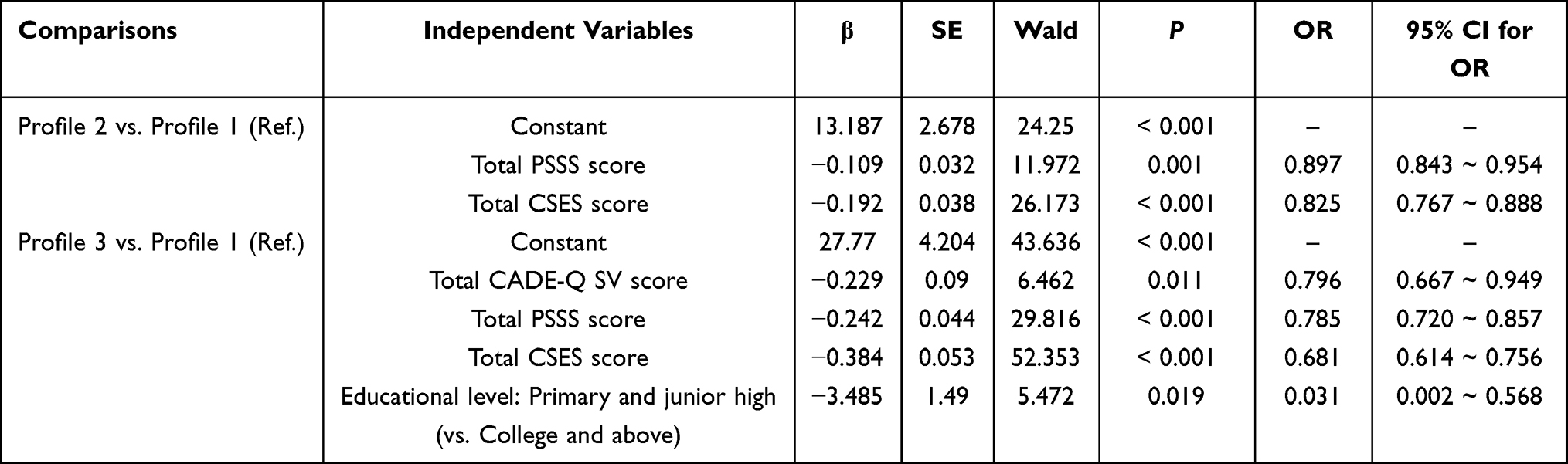 |
Table 6 Multinomial Logistic Regression Analysis of Associated Factors for the Latent Profiles |
Discussion
Heterogeneity and the Suboptimal Level of Health Problem-Solving Ability in CHD Patients
The findings of this study demonstrate that the mean HPSS score among CHD patients was 13.65 ± 4.84, reflecting a suboptimal level of health problem-solving ability. Since this study utilized the Chinese version of the 30-item HPSS adapted by Wang et al,17 direct and methodologically homogeneous comparisons can be drawn with domestic populations managing other chronic conditions. Notably, our sample’s score is lower than that reported by Zhan et al,18 who observed a median HPSS score of 16.53 among elderly hypertensive patients in China using the identical instrument. Furthermore, our LPA revealed substantial population heterogeneity, identifying three distinct subgroups: “Rational-Active Coping” (26.8%), “Ambivalent-Passive Adaptation” (52.2%), and “Negative-Impulsive Avoidance” (21.0%). This distribution indicates that the vast majority (73.2%) fell into suboptimal or maladaptive coping patterns. Clinically, these derived profiles are not merely statistical artifacts; they closely reflect distinct subgroups frequently encountered in cardiovascular wards—patients who either vacillate due to a disconnect between health awareness and behavioral execution, or resort to impulsive evasion during acute cardiac events.
This pronounced deficit and heterogeneity in problem-solving capacity within the CHD population, even when compared to general cardiovascular conditions like hypertension, may be primarily attributed to the distinct clinical trajectory of coronary events. While hypertension management largely relies on routine, predictable, and often asymptomatic daily self-care tasks (such as blood pressure monitoring and scheduled medication adherence), CHD frequently involves episodic, acute, and potentially life-threatening symptom fluctuations.1 Rational problem-solving in the context of CHD demands that patients rapidly appraise complex and ambiguous warning signs—such as differentiating atypical chest pain—and make immediate, time-sensitive medical decisions. This unpredictable nature imposes a severe cognitive and informational load that can easily overwhelm patients’ existing health literacy, leading to a higher inclination toward ambivalent-passive hesitation or impulsive evasion during acute cardiac events. This interpretation is broadly consistent with real-world outcomes documented in large-scale international registries, such as EUROASPIRE V and INTERASPIRE,3,4 where a substantial proportion of CHD patients fail to achieve secondary prevention targets or maintain long-term lifestyle modifications, although direct numerical comparisons are limited by differences in measurement instruments.
Consistent with previous findings across various chronic conditions (eg., Zhan et al18 in hypertension and Ji et al8 in diabetes populations), our findings suggest that self-efficacy and social support were independently associated with profile membership. Consequently, this unobserved heterogeneity suggests that conventional transitional care could be further enhanced by incorporating targeted strategies tailored to specific cognitive and coping profiles.
Mechanism Analysis Based on the Chronic Illness Problem-Solving Model
The present findings are broadly consistent with Hill-Briggs’ problem-solving model of chronic illness self-management.13 In the long-term management of CHD, the strategies adopted by patients may be associated with both internal individual factors and external environmental resources.
Internal Drivers: Disease Knowledge and Self-Efficacy
Disease knowledge and educational attainment provide the informational foundation for rational decision-making. While univariate analysis indicated that a lower educational level was associated with a higher risk of avoidant coping, its independent effect inverted in the multivariate model after adjusting for cognitive factors (OR = 0.031, P = 0.019). This statistical shift may suggest that the relationship between educational attainment and health problem-solving ability could be partly explained through more proximal cognitive resources, such as disease knowledge and self-efficacy. However, given the cross-sectional nature of the study, this interpretation should be considered exploratory, and mediation pathways require further validation. Given the relatively small number of participants with higher educational attainment across profiles, this finding should also be interpreted cautiously and further validated in larger multicenter studies.These findings may imply that strengthening modifiable cognitive resources, such as disease knowledge and self-efficacy, could potentially mitigate educational disparities in health problem-solving. However, this possibility requires confirmation in future longitudinal or intervention studies. This is primarily because a deficit in health literacy impedes the accurate interpretation of cardiovascular warning signs. Lacking essential medical literacy (eg., angina triggers, emergency medication protocols), these patients struggle to evaluate sudden symptom onset effectively, frequently resorting to impulsive actions or avoidant procrastination. Previous research indicates that acute cardiac symptom onset coupled with low health literacy can easily induce psychological distress, which significantly amplifies non-rational coping mechanisms.25 Notably, the strong correlations observed between HPSS, cardiac self-efficacy (r = 0.874), and perceived social support (r = 0.794) may reflect close interrelationships among psychosocial resources and health problem-solving behavior in CHD patients. Consistent with Hill-Briggs’ theoretical framework, self-efficacy may function as an internal cognitive resource, whereas social support may serve as an external contextual facilitator jointly associated with adaptive problem-solving.
External Buffer: Perceived Social Support
The theoretical model posits that an external social support system can significantly optimize problem-solving pathways. Our findings confirmed that lower perceived social support increases the risk of patients adopting ambivalent-passive or negative-impulsive strategies. CHD is characterized by a prolonged disease course accompanied by the constant risk of acute cardiovascular events, imposing a psychological burden on patients during home-based management. Emotional resonance and daily care from spouses and children, coupled with professional informational support from healthcare providers and peers, serve as a vital psychological buffer.26,27 This external support network not only alleviates the cognitive load associated with disease management but also provides timely psychological counseling and behavioral supervision during setbacks, effectively mitigating negative behaviors such as avoidance.
Implications for Tailored Transitional Care Interventions
Based on these findings, healthcare professionals may consider implementing differentiated, precision intervention strategies tailored to the latent profile characteristics of CHD patients:
(1) For “Negative-Impulsive Avoidance” patients: Interventions could prioritize foundational cognition building and family support reinforcement. Given their limited health literacy and susceptibility to negative emotions, traditional one-way health education is often ineffective. Healthcare providers are encouraged to utilize the “Teach-back” method combined with intuitive visual materials to ensure mastery of core emergency skills and critical medication protocols.28 Concurrently, a family-inclusive intervention model is highly recommended. Encouraging core family members (eg., spouses) to actively participate in the co-management process can compensate for the patient’s intrinsic problem-solving deficits through robust external supervision.29
(2) For “Ambivalent-Passive Adaptation” patients: Care might focus on stimulating internal self-efficacy and facilitating the translation of knowledge into action. Although these patients possess basic disease awareness, they lack execution capability. Incorporating motivational interviewing techniques can assist patients in identifying and overcoming underlying psychological barriers to non-adherence.30 Furthermore, leveraging a peer support model—where successfully rehabilitated patients share their experiences—can utilize the role-model effect to boost self-efficacy.31 Nurses can collaborate with these patients to set feasible, phased health goals, guiding them progressively toward a rational and active problem-solving paradigm. Regarding feasibility, resource-prohibitive full-scale motivational interviewing can be streamlined by integrating condensed motivational prompts into routine health education and discharge counseling, and leveraging established hospital-mediated digital peer groups (eg., WeChat) to provide scalable, low-cost behavioral reinforcement.
Limitations
This study has several limitations that warrant consideration. First, the cross-sectional design precludes establishing temporal ordering or causal inferences, and cannot fully capture the underlying motivations behind patients’ behavioral choices; thus, future research should integrate qualitative methodologies (eg., in-depth interviews) to explore their authentic experiences. Second, single-center convenience sampling limits generalizability and introduces selection bias, failing to fully represent patients from other geographic regions or primary care settings. Third, data were collected entirely via self-reported scales, which are highly susceptible to recall bias, social desirability bias, and common method variance. Fourth, we lacked quantitative adjustments for the clinical severity of CHD (eg., comorbidity indexes) and direct psychological evaluations, which restricts our mechanistic depth. Furthermore, our variable selection strategy combined with the relatively small sample sizes in certain profiles introduces a risk of potential overfitting. Finally, the profiles derived via LPA represent statistical approximations of unobserved heterogeneity, which requires further validation through robust longitudinal studies.
Conclusion
This study highlights significant population heterogeneity in the health problem-solving ability of CHD patients, identifying three latent profiles: Rational-Active Coping, Ambivalent-Passive Adaptation, and Negative-Impulsive Avoidance. Diminished self-efficacy, insufficient perceived social support, and a lack of disease knowledge reserves are critical factors significantly associated with patients’ inclination toward passive or negative coping mechanisms. Guided by the chronic illness problem-solving model, these profiles offer a practical screening tool to optimize limited transitional care resources through targeted interventions tailored to distinct coping subgroups, which may ultimately contribute to reducing post-discharge readmission risks and improving long-term disease management.
Ethical Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of The First Affiliated Hospital of Gannan Medical University (Approval No.: LLSC-2025567). Written informed consent was obtained from all participants.
Acknowledgments
We would like to express our deepest gratitude to Ms. Yanli Lan for her continuous guidance and invaluable support throughout this research. We also extend our sincere appreciation to the participating hospital for facilitating this study, as well as to our fellow research group members for their dedicated efforts in data collection. Finally, we are profoundly grateful to all the patients with coronary heart disease who volunteered their time to participate in this research.
Author Contributions
All authors made substantial contributions to the conception and design of the study, data acquisition, or data analysis and interpretation. Furthermore, all authors participated in drafting the manuscript or revising it critically for important intellectual content, gave final approval for the current version to be published, agreed to submit it to this journal, and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Galli M, Abbate A, Bonaca MP, et al. Residual cardiovascular risk in coronary artery disease: from pathophysiology to established and novel therapies. Nat Rev Cardiol. 2026;2026:1.
2. Zhang Y, Yan F, Jiang W. Relationship between self-management behaviors and health-related quality of life among Chinese patients with coronary heart disease: a cross-sectional study. Contemp Nurse. 2019;55(6):554–11. doi:10.1080/10376178.2020.1731316
3. McEvoy JW, Jennings C, Kotseva K, et al. Variation in secondary prevention of coronary heart disease: the INTERASPIRE study. Eur Heart J. 2024;45(39):4184–4196. doi:10.1093/eurheartj/ehae558
4. Kotseva K, De Backer G, De Bacquer D, et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur J Prev Cardiol. 2019;26(8):824–835. doi:10.1177/2047487318825350
5. De Bacquer D, Astin F, Kotseva K, et al. Poor adherence to lifestyle recommendations in patients with coronary heart disease: results from the EUROASPIRE surveys. Eur J Prev Cardiol. 2022;29(2):383–395. doi:10.1093/eurjpc/zwab115
6. Shang S, Zheng X, Xu Z, et al. Mediation effect of hope on the relationship between inner strength and self-management in patients after percutaneous coronary intervention. Front Psychol. 2024;15:1268598. doi:10.3389/fpsyg.2024.1268598
7. Hill-Briggs F, Gemmell L, Kulkarni B, et al. Associations of patient health-related problem solving with disease control, emergency department visits, and hospitalizations in HIV and diabetes clinic samples. J Gen Intern Med. 2007;22(5):649–654. doi:10.1007/s11606-006-0091-2
8. Ji M, Sereika SM, Dunbar-Jacob J, et al. Correlation of symptom distress, self-efficacy, and social support with problem-solving and glycemic control among patients with type 2 diabetes. Sci Diabetes Self Manag Care. 2021;47(1):85–93. doi:10.1177/0145721720983222
9. Chen CY, Lo FS, Wang RH. Roles of emotional autonomy, problem-solving ability and parent-adolescent relationships on self-management of adolescents with type 1 diabetes in Taiwan. J Pediatr Nurs. 2020;55:e263–e269. doi:10.1016/j.pedn.2020.05.013
10. Shin N, Hill-Briggs F, Langan S, et al. The association of minor and major depression with health problem-solving and diabetes self-care activities in a clinic-based population of adults with type 2 diabetes mellitus. J Diabetes Complications. 2017;31(5):880–885. doi:10.1016/j.jdiacomp.2017.01.026
11. Witty TE, Heppner PP, Bernard CB, et al. Problem-Solving appraisal and psychological adjustment of persons with chronic low-back pain. J Clin Psychol Med Settings. 2001;8(3):149–160. doi:10.1023/A:1011361418436
12. Wu K, Wen A, Jin P, et al. Characteristics and correlates of health information literacy among patients with type 2 diabetes and metabolic syndrome: a cross-sectional study. Sci Diabetes Self Manag Care. 2024;50(6):546–562. doi:10.1177/26350106241290443
13. Hill-Briggs F. Problem solving in diabetes self-management: a model of chronic illness self-management behavior. Ann Behav Med. 2003;25(3):182–193. doi:10.1207/S15324796ABM2503_04
14. Berlin KS, Williams NA, Parra GR. An introduction to latent variable mixture modeling (part 1): overview and cross-sectional latent class and latent profile analyses. J Pediatr Psychol. 2014;39(2):174–187. doi:10.1093/jpepsy/jst084
15. Dey S, Wang A, McMaster M, et al. Clinical management of patients with stable ischemic heart disease. Cardiol Rev. 2023. doi:10.1097/CRD.0000000000000557
16. Kendall MG, Stuart A. The Advanced Theory of Statistics. London: Charles Griffin & Company; 1961.
17. Wang XJ, Jin PN, Ji MH. Translation and reliability and validity testing of the Health Problem-Solving Scale. J Nurs Sci. 2023;38(15):35–39. In Chinese.
18. Zhan XY, Zhao X, Cai P, et al. Current status and influencing factors of health problem-solving ability in elderly patients with hypertension. Mod Med J. 2025;53(7):1149–1157. In Chinese.
19. Sullivan MD, LaCroix AZ, Russo J, et al. Self-efficacy and self-reported functional status in coronary heart disease: a six-month prospective study. Psychosom Med. 1998;60(4):473–478. doi:10.1097/00006842-199807000-00014
20. Xie BQ, Xu LH. Current status and predictive factors of self-management behaviors in patients with coronary heart disease. Nurs J Chin PLA. 2011;28(6):3–7. In Chinese.
21. Ghisi G, Sandison N, Oh P. Development, pilot testing and psychometric validation of a short version of the coronary artery disease education questionnaire: the CADE-Q SV. Patient Educ Couns. 2016;99(3):443–447. doi:10.1016/j.pec.2015.11.002
22. Li JJ, Wang Z, Chen N, et al. Translation, reliability, and validity of the short version of the Coronary Artery Disease Education Questionnaire. Acad J Second Mil Med Univ. 2021;42(3):294–300. In Chinese.
23. Zimet GD, Powell SS, Farley GK, et al. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. J Pers Assess. 1990;55(3–4):610–617.
24. Jiang QJ. Perceived social support scale. Chin J Behav Med Sci. 2001;10(10):41–43. In Chinese.
25. Svavarsdóttir MH, Halapi E, Ketilsdóttir A, et al. Changes in disease-related knowledge and educational needs of patients with coronary heart disease over a six-month period between hospital discharge and follow-up. Patient Educ Couns. 2023;117:107972. doi:10.1016/j.pec.2023.107972
26. Smith TW. Intimate relationships and coronary heart disease: implications for risk, prevention, and patient management. Curr Cardiol Rep. 2022;24(6):761–774. doi:10.1007/s11886-022-01695-4
27. Zhu Y, Song Y, Wang Y, et al. Relationships among social support, self-efficacy, and patient activation in community-dwelling older adults living with coronary heart disease: a cross-sectional study. Geriatr Nurs. 2022;48:139–144. doi:10.1016/j.gerinurse.2022.09.008
28. Liu Y, Luo X, Ru X, et al. Impact of a multimodal health education combined with teach-back method on self-management in hemodialysis patients: a randomized controlled trial. Medicine. 2024;103(52):e39971. doi:10.1097/MD.0000000000039971
29. Nelson LA, Spieker AJ, Greevy RJ, et al. Glycemic outcomes of a family-focused intervention for adults with type 2 diabetes: main, mediated, and subgroup effects from the FAMS 2.0 RCT. Diabet Res Clin Pract. 2023;206:110991. doi:10.1016/j.diabres.2023.110991
30. Zhang BR, Yang X. Motivational interviewing in postoperative rehabilitation and chronic disease management: current findings and future research directions. World J Psychiatry. 2025;15(1):102737. doi:10.5498/wjp.v15.i1.102737
31. Cooper RE, Saunders K, Greenburgh A, et al. The effectiveness, implementation, and experiences of peer support approaches for mental health: a systematic umbrella review. BMC Med. 2024;22(1):72. doi:10.1186/s12916-024-03260-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pathways of Media Contact to Health Literacy in Middle-Aged and Older People: The Chain Mediation Effect of Perceived Social Support and Self-Efficacy
Jiang MM, Xiao YW, Liao ZL
Journal of Multidisciplinary Healthcare 2024, 17:111-121
Published Date: 6 January 2024
The Serial Mediation Effects of Social Support and Self-Efficacy on Health Literacy and Self-Management Behaviors Among Young and Middle-Aged Cardiac Patients After Percutaneous Coronary Intervention: A Cross-Sectional Study in China
Liu W, Qian S, Hu Y, Zhang R
Risk Management and Healthcare Policy 2024, 17:2893-2906
Published Date: 22 November 2024
Confirmatory Factor Analysis of the Malay Version of the Malaysia Medication Adherence Assessment Tool (MyMAAT) Among Patients with Chronic Medications
Ong GT, Abdullah S, Bachok NB
Patient Preference and Adherence 2024, 18:2609-2620
Published Date: 21 December 2024
Mediating Effects of Health Literacy, Self-Efficacy, and Social Support on the Relationship Between Disease Knowledge and Patient Participation Behavior Among Chronic Ill Patients: A Cross-Sectional Study Based on the Capability-Opportunity-Motivation and Behavior (COM-B) Model
Wu M, Wang W, He H, Bao L, Lv P
Patient Preference and Adherence 2025, 19:1337-1350
Published Date: 8 May 2025
Psychosocial and Clinical Factors That Differentiate and Predict Patients’ Adaptation to Chronic Diseases
Laza R, Al Ghazi L, Lustrea A, Lazureanu VE, Oancea CI, Luput-Andrica IM, Poplicean EI, Ilina R, Cireap N, Bob F, Olariu N, Ionita I, Lazar S, Dehelean L, Romosan RS, Romosan AM
Patient Preference and Adherence 2025, 19:1539-1556
Published Date: 24 May 2025