Back to Journals » International Journal of General Medicine » Volume 19
Latent Profile Analysis of Illness Perception and Its Association with Fear of Progression in Chronic Kidney Disease
Authors Chen L, Wu Y, Yang JH, Zhou MJ, Lv XL, Lin Z, Cui Y
Received 29 September 2025
Accepted for publication 29 January 2026
Published 25 February 2026 Volume 2026:19 571208
DOI https://doi.org/10.2147/IJGM.S571208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David E. Stec
Lu Chen,1,2,* Yue Wu,1,3,* Jia-hui Yang,4 Mei-jing Zhou,5 Xiao-lin Lv,4 Zheng Lin,1,2 Yan Cui2
1Department of Nursing, The First Affiliated Hospital with Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 2School of Nursing, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3School of Nursing and Midwifery, University College Cork, Cork, Ireland; 4Department of Nephrology, The First Affiliated Hospital with Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 5Department of Endocrinology, The First Affiliated Hospital with Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Cui, School of Nursing, Nanjing Medical University, No. 101, Longmian Avenue, Jiangning District, Nanjing, Jiangsu, 211166, People’s Republic of China, Tel +86 13951916137, Email [email protected] Zheng Lin, School of Nursing, Nanjing Medical University, No. 101, Longmian Avenue, Jiangning District, Nanjing, Jiangsu, 211166, People’s Republic of China, Tel +86 13851770340, Email [email protected]
Background: Fear of progression (FoP) is one of the most prevalent psychological responses among patients with chronic kidney disease (CKD), impairing mental health and quality of life. However, research on the heterogeneity of illness perceptions among CKD patients remains limited, and the relationship between distinct perception profiles and FoP is not yet well understood. This study aimed to identify latent profiles of illness perception in CKD patients and examine their associations with FoP.
Methods: In this cross-sectional study, a total of 428 CKD patients were recruited from four tertiary hospitals through convenience sampling between May 1, 2023, and April 30, 2024. Participants completed questionnaires assessing demographic and clinical characteristics, illness perception, FoP, psychological flexibility, family resilience, and social support. Latent profile analysis was conducted to identify illness perception profiles, multinomial logistic regression was used to examine predictors of profile membership, and stratified regression analyses were performed to assess the associations between illness perception profiles and FoP.
Results: Latent profile analysis identified three distinct illness perception profiles. Multinomial logistic regression analysis indicated that CKD stage, number of concomitant symptoms, psychological flexibility, family resilience, and social support significantly predicted the latent profiles of illness perception (P < 0.05). Stratified regression analysis further demonstrated that illness perception profiles were independently predicted FoP after controlling for key demographic and clinical variables.
Conclusion: CKD patients exhibit heterogeneity in illness perception. Illness perception profiles were associated with FoP. Distinct illness perception profiles are associated with FoP, and are influenced by key psychosocial factors. These findings support the development of tailored, perception-based interventions to reduce FoP among CKD patients.
Keywords: chronic kidney disease, fear of progression, illness perception, latent profile analysis
Introduction
The prevalence of chronic kidney disease (CKD) has increased in recent decades, now affecting 8% to 16% of the global population.1,2 CKD is a progressive disease, and as it advances to end-stage renal disease (ESRD), patients typically require dialysis, which may be lifelong in many cases.3 Due to its long-term, incurable nature and associated complications, CKD imposes a significant burden on both the physical and psychological well-being of patients.4 Most patients reaching the dialysis stage experience a significant decline in quality of life, accompanied by increased risk of mortality. Compared with the general population of similar age, the five-year survival rate of people with ESRD undergoing dialysis is significantly lower, ranging between 13% and 60%.5
In clinical settings, patients frequently express concern about the severity of their current condition, especially fearing progression to end-stage renal disease.6,7 Compared with many other chronic conditions, CKD patients are particularly vulnerable to fear of progression (FoP) due to the irreversible nature of the disease, the uncertainty of its trajectory, and the anticipation of renal replacement therapy, which is often accompanied by substantial lifestyle disruption and financial burden.
One of the most common psychological responses among CKD patients facing disease uncertainty is FoP. Dankert et al8 defined FoP as the fear of disease advancement and its associated physical, psychological, and social consequences or recurrence. A moderate level of fear regarding disease progression may be adaptive, motivating patients to restrain harmful behaviors and adopt healthier lifestyles.9 However, excessive FoP may impair mental health, manifesting as heightened levels of worry, anxiety, and depression.10 This can lead to harmful behaviors such as increased alcohol consumption, reduced physical activity, excessive health-seeking behavior, or non-adherence to treatment regimens, avoidance of dialysis planning, and frequent cancellation or postponement of follow-up visits.10 Over time, these behaviors can affect patient health outcomes, increase the financial burden on patients, and in severe cases, lead to mental disorders.11
The FoP experience by patients with CKD is influenced by numerous factors,12–14 among which illness perception (IP) may be an important potential determinant. The Common-Sense Model of Self-Regulation (CSM) is a widely used theoretical framework in research on both FoP and illness perception.15–17 According to the CSM, individuals’ perceptions of physical symptoms or health threats activate cognitive and emotional processing systems, which guide coping responses and generate feedback loops through outcome appraisal, ultimately forming a self-regulatory system.15,18–21 Illness perception refers to patients’ cognitive and emotional representations of their disease, including their understanding of the condition and its perceived consequences.17,22 Within this framework, FoP is conceptualized as an emotional response shaped by illness perception.23
Previous studies have reported associations between illness perception and FoP in various chronic disease populations, including patients with cancer, diabetes, and those undergoing maintenance hemodialysis, with more negative or threatening illness perceptions being linked to higher FoP.16,24,25 However, most existing studies in CKD have relied on variable-centered analytic approaches, using total scores derived from standardized illness perception scales. This approach assumes homogeneity across dimensions of illness perception and may overlook clinically meaningful individual differences, thereby limiting the applicability of findings in the context of personalized care.26,27
Illness perception is a multidimensional construct comprising both cognitive and emotional components.28 The Brief Illness Perception Questionnaire (BIPQ) is commonly used to evaluate patients’ illness perceptions. The BIPQ evaluates six cognitive representations—consequences, timeline, personal control, treatment control, identity, and coherence—and two emotional representations—emotional responses and concern.17 The majority of studies have analyzed the BIPQ’s results at the variable level, treating each dimension as a separate scale or aggregating items into composite scores.22 However, in recent years, more researchers have recognised these limitations and advocated for person-centered analytic approaches to re-examining illness perception. Person-centered approaches include methods such as traditional mean-splitting and cluster analysis, as well as model-based techniques such as latent profile analysis (LPA), which has emerged as a robust method for identifying homogeneous subgroups based on response patterns.29–32 Prior studies suggest that LPA can facilitate more precise subgroup identification and support the development of tailored interventions.26,28,33 Although previous studies have examined associations between positive psychological qualities, family resilience, social support, and illness perception,11,34–36 it remains unclear whether these factors influence the latent profile structure of illness perception in patients with CKD.
Grounded in the Common-Sense Model of Self-Regulation, this study assumes that individuals’ cognitive and emotional representations of illness, reflected by distinct illness perception profiles, are closely associated with FoP among patients with CKD. Specifically, profiles characterized by more negative cognitive and emotional illness perceptions are expected to be associated with higher levels of FoP.
Accordingly, this study was designed with three primary aims: (1) to examine whether heterogeneity exists in illness perception among patients with CKD; (2) to identify psychosocial and clinical factors influencing different illness perception profiles; and (3) to determine whether these profiles are associated with FoP in CKD patients. These objectives are intended to advance understanding of illness perception in CKD and to support the development of personalized interventions.
Methods
Study Design and Sample
A cross-sectional descriptive study was conducted between May 1, 2023, and April 30, 2024, in the nephrology departments of four tertiary hospitals in Jiangsu Province, China. Participants were recruited using convenience sampling. The inclusion criteria were: 1) meeting the diagnostic criteria outlined by the Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group for identifying CKD patients;37 2) having clear consciousness, with the ability to understand and express themselves sufficiently to complete the survey questionnaire independently or with assistance; and 3) providing informed consent to voluntarily participate in the study. Exclusion criteria included: 1) the presence of another type of malignant tumor; 2) having serious heart, brain, or other functional disorders; 3) having a mental disability such as schizophrenia; and 4) being pregnant or breastfeeding. These details were obtained from electronic medical records.
Ethical Considerations
This survey was approved by the Institutional Review Board (IRB) of Nanjing Medical University in March 2023, (IRB No: (2023)494#). In accordance with the Declaration of Helsinki, all participants provided written informed consent prior to participating in this study.
Instruments
Demographic and Clinical Characteristics Questionnaire
The demographic and clinical characteristics questionnaire developed by the research team was used to collect demographic data (age, sex, marital status, fertility status, place of residence, educational level, occupational status and monthly disposable household income) and disease-related data (CKD stage and number of concomitant symptoms). Demographic data were self-reported by the patients, while disease-related data were extracted from the hospital’s electronic medical record system.
Brief Illness Perception Questionnaire
The Brief Illness Perception Questionnaire (BIPQ) consists of nine items used to measure patients’ perspective of their illness.17 The first eight items are scored on an 11-point Likert scale ranging from 0 to 10, with a total score ranging from 0 to 80. The first five items pertain to disease-related domains: disease consequences, timeline (duration of the disease), personal control (self-control of the disease), treatment control, and identity. The next two items are related to emotions, namely concern and emotional response, and the eighth item is illness comprehensibility (ie, the extent to which the illness is understood). The ninth item is an open-ended question, asking patients to list the three most important perceived causes of their disease. Higher total scores reflect a greater perceived psychological burden of illness. The Chinese version of the BIPQ exhibits strong internal reliability among CKD patients, as evidenced by a Cronbach’s alpha coefficient of 0.70.23 In this study, the overall Cronbach’s alpha for the entire scale was 0.756.
Fear of Progression Questionnaire
The Fear of Progression Questionnaire (FoP-Q), developed by Herschbach et al,38 consists of 43 items and yields two total scores: one for all anxiety subscales and another for the coping subscale. The total score of the anxiety subscale, representing FoP, is categorized into four dimensions consisting of 34 items. These dimensions include affective reactions, partnership/family, occupation, and loss of autonomy. The “coping with anxiety” subscale was excluded from the analysis, as it did not contribute to the total FoP-Q assessment in this study. Each item was rated on a 5-point Likert scale ranging from 1 to 5, with 1 indicating “never” and 5 indicating “very often”. Higher total scores on FoP-Q indicate a greater level of FoP. The Chinese version of the FoP-Q has demonstrated good internal reliability, with a Cronbach’s alpha of 0.969 for the entire scale.39 In this study, the overall Cronbach’s alpha for the FoP-Q was 0.966.
Comprehensive Assessment of Acceptance and Commitment Therapy Processes
The Comprehensive Assessment of Acceptance and Commitment Therapy Processes (CompACT), developed by Francis et al,40 evaluates psychological flexibility through 23 items across three dimensions: openness to experience, behavioral awareness, and valued action. Each item was rated on a 7-point Likert scale ranging from 1 (“strongly disagree” to 7 (“strongly agree”), with 12 items reverse scored. The total CompACT score ranges from 23 to 161, with higher scores indicating better psychological flexibility. The Chinese version of the CompACT demonstrates strong internal reliability, with a Cronbach’s alpha of 0.91 for the entire scale.41 In this study, however, the overall Cronbach’s alpha for the entire scale was 0.624.
Family Resilience Questionnaire
The Family Resilience Questionnaire (FaRe), developed by Faccio et al,42 comprises 24 items organized into four dimensions: communication and cohesion, perception of social support, perception of family coping, and religious beliefs. Participants rated each item on a 7-point Likert scale, ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). Total scores ranged from 24 to 168, with higher scores indicating higher levels of family resilience. The Chinese version of FaRe has shown good internal consistency, with a Cronbach’s alpha of 0.909 in a previous study.43 In the present study, the “religious beliefs” dimension was excluded because the majority of participants reported no religious affiliation, and responses to this dimension showed limited variability, which could compromise the interpretability and validity of the scale in this population. Therefore, analyses were conducted using the remaining three dimensions, and total scores were calculated based on these dimensions only. The Cronbach’s alpha for the revised scale in this study was 0.964.
Social Support Rating Scale
The Social Support Rating Scale (SSRS), developed by Xiao,44 includes 10 items across three dimensions: objective support, subjective support, and utilization of support. Scoring for the items in question follows this structure: Items 1–4 and 8–10 are rated on a 4-point scale. Item 5 is evaluated across five dimensions (A, B, C, D, and E), each receiving 1–4 points. For Items 6 and 7, 0 points are given if no support source is identified, and 1 point is awarded for each additional source. Total scores range from 12 to 66 points. Higher scores on the scale indicate the greater the level of social support. The SSRS demonstrated good internal consistency, with a Cronbach’s alpha of 0.89045 in previous studies and 0.717 in this study.
Data Analysis
Statistical analyses were conducted using SPSS 22.046 and Mplus 8.3 software.47 Latent profile analysis (LPA) of illness perception in CKD patients was performed using Mplus 8.3, with scores in the eight illness perception items as observed variables. Starting from a one-class model, we progressively increased the number of classes, comprehensively evaluating model fit indices and clinical applicability to determine the optimal solution. Model fit indices included the following: 1) Information indices: Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and adjusted Bayesian Information Criterion (aBIC). Lower values indicate a better model fit. 2) Classification index: Entropy. Values range from 0 to 1, with higher values indicating a more accurate classification. An entropy value above 0.8 implies classification accuracy exceeding 90%. 3) Likelihood ratio test: The Lo-Mendell-Rubin (LMR) and the bootstrap-based likelihood ratio test (Bootstrap Likelihood Ratio Test, BLRT). A p-values < 0.05 indicates that the models with k classes fits significantly better than the model with k-1 categories. Regarding sample size adequacy for LPA, there is no fixed minimum sample size requirement, as adequacy depends on factors such as the number of indicators, class separation, and model complexity. Methodological literature indicates that LPA studies are commonly conducted with sample sizes in the several-hundred range, and that stable and reliable profile solutions can be obtained when model fit indices and classification quality are satisfactory.48 With a final sample of 428 participants, eight indicator variables, and acceptable entropy and fit indices, the present study provides adequate support for reliable latent profile identification.
Continuous data were presented as mean (M) ± standard deviation (SD), and categorical data were summarized using frequencies and percentages. Analysis of variance (ANOVA) was employed for continuous variables, with p < 0.05 indicating statistical significance. Categorical unordered variables were analyzed using the chi-square test or Fisher’s exact test, while the Kruskal–Wallis H-test was used for ordered categorical variables. Variables with p-values < 0.20 in the univariate analyses were included as independent variables in the multinomial regression model. Hierarchical multiple regression analysis was used to explore the relationship between illness perception and FoP.
Results
Demographic and Clinical Disease Characteristics
Of the 455 questionnaires distributed, 428 were returned with complete information, resulting in an effective retrieval rate of 94.07%. Participant characteristics are presented in Table 1. The mean age of the CKD patients was 46.61 ± 16.16 years, with approximately 56.54% were male. Regarding educational level, 64 participants (14.95%) had a low level of education, while 170 participants (39.72%) had a college degree or above. The majority of patients surveyed (72.66%) resided in urban areas. Additionally, 330 participants (77.10%) were married, 343 (80.14%) had children, and 404 (94.39%) reported no religious affiliation. Economically, more than three-fourths (75.70%) of households had a monthly disposable income below 5000 RMB. Regarding disease characteristics, 180 participants (42.06%) were in CKD stage 5, and half of the participants (52.33%) reported experiencing concomitant symptoms.
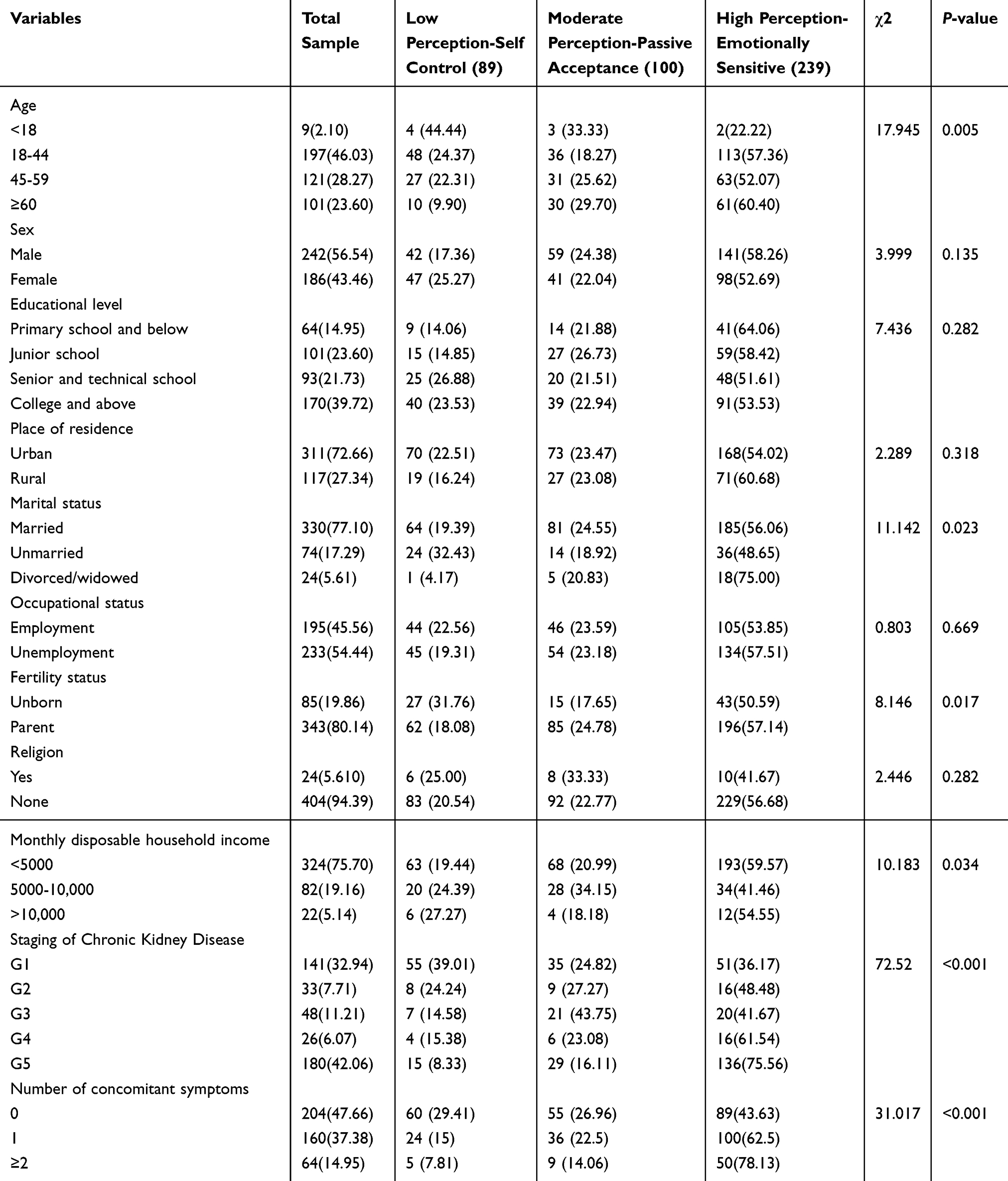 |
Table 1 Comparison of Demographic and Clinical Characteristics Among Latent Illness Perception Profiles in CKD Patients [n (%)] |
Latent Profile Analysis of Illness Perception in CKD Patients
An exploratory latent profile analysis (LPA) was conducted on the illness perception of CKD patients based on the eight items of the BIPQ. 1 to 5 potential profile models were established successively, as shown in Table 2. In models 1 to 5, AIC, BIC, and aBIC values exhibited a decreasing trend with an increasing number of latent profiles. However, only models 2 and 3 demonstrated significant levels (p < 0.05) for both the LMRT and BLRT tests, indicating that Model 4 was not superior to Model 3, and Model 3 was superior to Model 2. The two-profile model was excluded due to its lowest entropy value of 0.771 (entropy value < 0.8), while the three-profile model had an entropy value of 0.841. This suggests that the three-profile model provided a more accurate classification compared to the two-profile model. After comprehensively evaluating all fitting indicators and considering clinical significance, Model 3 was selected as the optimal solution. Therefore, three potential profiles were retained: Profile1, Profile 2 and Profile 3, and the probability of the total sample was 20.8% (n = 89), 23.4% (n = 100) and 55.8% (n = 239), respectively.
 |
Table 2 Fit Indices for Latent Profile Analysis of Illness Model |
Characteristics and Nomenclature of Latent Profiles
Based on the three-profile model, line plots for each BIPQ item score were generated according to their feature patterns, as illustrated in Figure 1. The characteristic attributes of each profile were named based on the fluctuations observed in the average line chart of each item. Overall, the three profiles reflected distinct patterns of illness perception: Profile 1 was characterized by low overall illness perception with relatively strong perceived control, Profile 2 by moderate illness perception with passive acceptance, and Profile 3 by high illness perception accompanied by pronounced emotional sensitivity. The specific characteristics of each profile are described below.
 |
Figure 1 The characteristic distribution of 3 latent profiles of illness perception in CKD patients. |
Profile 1 demonstrated a low overall BIPQ score, with an average of 31.36 ± 6.32. The scores for disease consequences, timeline, identity, and emotional response were relatively low. However, the scores for personal control (self-management of the disease), treatment control, concern, and understanding were high. Therefore, this profile was labeled as “Low Perception-Self Control”, comprising 89 patients (20.8%). Profile 2 exhibited a moderate overall score of 42.19 ± 4.42, positioning it between Profile 1 and Profile 3 in terms of overall score levels. The scores for all items were relatively moderate, but compared with Profiles 1 and 3, the scores for personal control, treatment control, concern, and understanding were the lowest. Thus, this profile was named “Moderate Perception-Passive Acceptance”, with 100 patients (23.4%).
Profile 3 had the highest overall BIPQ score of 49.68 ± 6.06. The scores for personal control and treatment control were between those of Profile 1 and Profile 2. The scores for disease consequences, timeline, identity, concern, understanding, and emotional response were relatively high. This indicates that patients in this profile believe they have some control over the disease and recognize the impact of medication or treatment on its progression. However, they also acknowledge that the disease significantly affects their emotional state, deeply influenced by its symptoms. Consequently, this profile was labeled as “High Perception-Emotionally Sensitive”, comprising 239 patients (55.8%).
Influencing Factors of Different Latent Profiles
The general demographic and disease-related characteristics of the three different latent profiles were analyzed, revealing significant differences in age, marital status, fertility status, monthly disposable household income, CKD stage, and the number of concomitant symptoms (P<0.05), as shown in Table 1. Moreover, significant differences in psychological flexibility, family resilience, and social support were observed among patients with different latent profiles (P<0.05), as illustrated in Table 3.
 |
Table 3 Comparison of Scores of CompACT, FaRe, and SSRS Among 3 Latent Profiles (M±SD) |
A multinomial logistic regression analysis was conducted with the three latent profiles of illness perception in CKD patients as dependent variables, using Profile 1 (Low Perception–Self Control Type) as the reference category. Variables with P values<0.2 in the univariate analysis were chosen as independent variables. The results indicated that CKD stage, the number of concomitant symptoms, psychological flexibility, family resilience, and social support were significant influencing factors for the latent profiles of illness perception in CKD patients (P<0.05), as shown in Table 4.
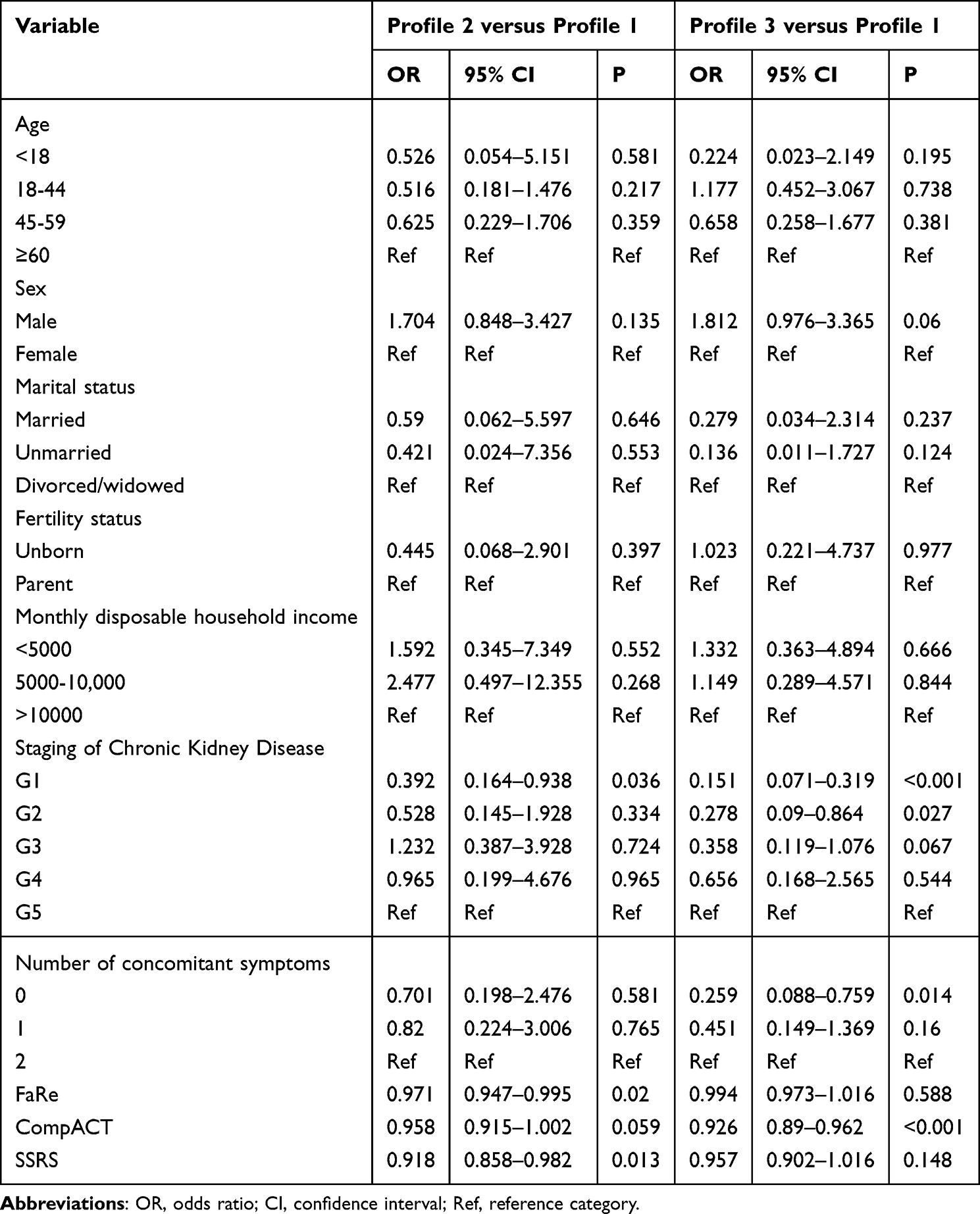 |
Table 4 Multivariate Logistic Regression Analysis of Profiles |
Relationship Between the Latent Profiles and FoP
One-way ANOVA and correlation analysis showed that the number of concomitant symptoms (F=4.045, P=0.018), psychological flexibility (r=−0.431, P<0.001), family resilience (r=−0.154, P<0.001), social support (r=−0.218, P<0.001), and the latent profiles of illness perception (F=43.550, P<0.001) were significant factors affecting the FoP. Hierarchical regression analysis was conducted to examine whether illness perception latent profiles independently predicted FoP after controlling for relevant clinical and psychosocial variables. In Model 1, the number of concomitant symptoms, psychological flexibility, family resilience, and social support were entered as predictors and jointly explained 22.5% of the variance in FoP (R2=0.225, F=30.638, p<0.001). In Model 2, latent profile membership was added to the model using dummy coding, with the Low Perception–Self Control profile as the reference group. The inclusion of latent profiles resulted in a significant increase in explained variance (ΔR2 = 0.074, F change = 22.091, p < 0.001), raising the total explained variance to 29.8% (R2 = 0.298). Compared with the reference group, patients classified as Moderate Perception–Passive Acceptance and High Perception-Emotionally Sensitive profiles exhibited significantly higher levels of FoP (both p < 0.01). These findings indicate that illness perception latent profiles make an independent and meaningful contribution to FoP beyond established clinical and psychosocial factors, as shown in Table 5.
 |
Table 5 Hierarchical Regression Analysis of the Effect of Illness Perception Latent Profile on FoP in Patients with CKD |
Discussion
Illness Perception Profiles Identified by LPA
The LPA identified three distinct latent profiles of illness perception among patients with CKD: Low Perception-Self Control Type (20.8%), Moderate Perception-Passive Acceptance Type (23.4%), and High Perception-Emotionally Sensitive Type (55.8%). The classification results were comparable to those reported in previous studies.27,33 However, this study used LPA to extract latent categories of illness perception with a larger sample size, which is likely to support more precise and stable classifications and enhance the interpretability of the findings. Importantly, the adoption of a person-centered analytical approach moves beyond traditional variable-centered analyses and highlights clinically meaningful heterogeneity in illness perception among CKD patients.
Furthermore, the identified profiles demonstrated distinct and independent associations with FoP after adjustment for disease-related and psychosocial factors, underscoring the potential clinical relevance of illness perception profiling for psychological risk stratification and care planning.
Characteristics of the Low and Moderate Illness Perception Profiles
Patients in the Low Perception-Self Control Type profile held a positive outlook toward their illness. They perceived CKD as having a limited impact on their lives and emotional well-being, reported fewer physical symptoms, and demonstrated relatively high perceived control over disease management and treatment. Despite their lower perceived disease impact, these patients did not ignore their condition and maintained a certain level of attentiveness and understanding.
In contrast, Patients from the Moderate Perception-Passive Acceptance Type profile exhibited illness perception score that fell between the low and high perception groups but demonstrated the lowest levels of perceived disease control, treatment control, concern, and understanding. One possible reason is that they perceive CKD as having minimal impact on their life and emotional well-being, with relatively mild or non-salient symptoms, leading to insufficient engagement in disease management. It is also possible that they lack adequate self-regulation capacity and passively accept the effects of the disease. This phenomenon has also been observed in cancer patients,26 suggesting that such individuals may require greater clinical attention and support.
Predominance and Clinical Meaning of the High Perception-Emotionally Sensitive Profile
Patients categorized as High Perception-Emotionally Sensitive Type profile constituted 55.8% of the sample, indicating that the majority of CKD patients tend to exhibit higher levels of illness perception. This predominance may reflect key characteristics of CKD, particularly the coexistence of disease irreversibility and uncertainty regarding disease progression, together with persistent symptoms that continuously draw patients’ attention to bodily changes. As a result, many patients remain highly vigilant toward their illness, which may amplify emotional responses and render emotional sensitivity a common psychological state rather than an exceptional one.
Notably, patients in this profile not only perceived their illness as having a substantial impact on their lives and emotional well-being, but also tended to maintain relatively high levels of attention to and understanding of their condition. Compared with patients in the Moderate Perception-Passive Acceptance Type, they reported greater perceived treatment effectiveness and disease controllability. This pattern suggests that heightened emotional sensitivity does not necessarily indicate disengagement from disease management but may coexist with active cognitive engagement.49 Nevertheless, excessive concern about illness may increase emotional distress and negatively affect self-management and quality of life.18,50
Clinical and Psychosocial Determinants of Illness Perception Profiles
The Common-Sense Model of Self-Regulation serves as the theoretical basis for understanding illness perception.17 It was developed to explain patients’ lay perceptions of illness threats and to guide their coping strategies. It also proposes the regulatory role of individual and social factors in this process.19 Guided by this theoretical framework, we included psychological flexibility, family resilience, and social support, in addition to demographic and clinical characteristics, as potential factors associated with illness perception profiles. Multinomial logistic regression analyses indicated that CKD stage, number of concomitant symptoms, psychological flexibility, family resilience, and social support were significant determinants of patient grouping.
Patients with CKD stages 4 and 5, as well as those experiencing disease-related discomfort symptoms, were more likely to be included in the High Perception-Emotionally Sensitive Type. Disease progression and symptom burden may heighten awareness of illness severity and associated stress, thereby amplifying emotional responses.49,51
Role of Psychological Flexibility, Family Resilience, and Social Support
Psychological flexibility, as a positive psychological attribute, was significantly associated with illness perception.52 However, given the relatively modest internal consistency of the CompACT scale in this study, the observed associations between psychological flexibility and illness perception profiles should be interpreted with caution. Individuals with higher psychological flexibility are generally better able to engage with the present moment and maintain value-consistent behaviors, which may facilitate more effective illness management.53,54 Consistent with this conceptualization, patients with higher psychological flexibility were more likely to belong to the Low Perception–Self Control Type. Psychological inflexibility has been conceptualized as involving processes such as cognitive fusion and experiential avoidance.53,55 In the present study, patients in the Moderate Perception–Passive Acceptance Type and High Perception-Emotionally Sensitive Type exhibited lower levels of psychological flexibility. These findings suggest that psychological flexibility may represent a potential focus for future supportive strategies in CKD care.
Family resilience and social support are also closely related to illness perception. Although previous studies have reported a negative association between illness perception and both family resilience and social support.35,36 Our findings revealed that patients with lower levels of family resilience and social support were more likely to be in the moderate perception group rather than the high perception group. Family resilience refers to the ability of family members to cope with and adapt to significant stressful events.56 Family members’ perceptions and beliefs when facing adversity may also interact with patients’ adaptation processes.57 Low family resilience means that patients may lack an effective family response and support system when facing disease threats, leaving them feeling isolated and without essential emotional support and psychological comfort. Consequently, patients may struggle to effectively cope with and manage their illness.35 Low social support means that patients lack sufficient external resources and assistance. Consequently, patients may struggle with confidence and motivation to actively understand and manage their disease, often leaning towards passively receiving medical advice and treatment decisions.36,58
Illness Perception Profiles and FoP
In the present study, latent profiles of illness perception emerged as the primary predictors of FoP among patients with CKD and remained significantly associated with FoP after adjustment for key clinical and demographic variables. This finding is consistent with previous evidence indicating a close association between illness perception and FoP in chronic disease populations.16,25 Patients in the High Perception–Emotionally Sensitive Type tend to perceive their illness as having a substantial impact on their lives, which may heighten vigilance toward disease-related threats and increase concerns about disease progression.59 In contrast, patients in the Moderate Perception-Passive Acceptance Type profile may feel less capable of effectively managing or coping with disease progression, thereby amplifying feelings of fear and anxiety.51
Contextual factors such as marital status and CKD stage may be related to differences in FoP partly through their associations with patients’ illness perceptions. From a psychosocial perspective, married patients may experience greater concern due to family and economic responsibilities, while patients in earlier stages of CKD may anticipate future treatments, such as hemodialysis, and their associated financial burden. These anticipatory concerns and uncertainties may contribute to more negative illness perceptions, thereby increasing FoP. Overall, FoP can be understood as complex and multidimensional psychological response arising from the interaction between clinical characteristics and patients’ cognitive and emotional representations of illness.60–62
Taken together, these findings highlight the importance of identifying heterogeneity in illness perception and adopting personalized approaches to reduce FoP in clinical renal care. Importantly, illness perceptions are not static and may be shaped by contextual and interpersonal factors during clinical care.20 In this context, healthcare providers play a central role in influencing patients’ illness perceptions through communication styles, clinical decision-making, and ongoing interactions.63 Clear, consistent, and empathetic communication may facilitate more adaptive illness perceptions, whereas overly technical or inconsistent information may exacerbate uncertainty and emotional distress.64
Despite the potential value of personalized interventions based on illness perception profiles, several practical barriers may limit their implementation in routine clinical care. Time constraints, limited staffing, insufficient training in psychosocial profiling, and variability in patient engagement and access to resources may all pose challenges. Addressing these barriers will be essential for translating profile-based interventions into real-world renal care.
Limitations
This study has several limitations that should be acknowledged. First, convenience sampling was employed, and participants were recruited exclusively from four tertiary hospitals in Jiangsu Province, China. Although the sample size was sufficient for the planned statistical analyses, the generalizability of the findings to the broader CKD population may be limited.
Second, this study adopted a cross-sectional design, which precludes causal inference and limits the ability to capture temporal changes in illness perception profiles and FoP. Longitudinal studies are therefore warranted to examine the dynamic evolution of illness perception and its relationship with FoP over time. In addition, retrospective or longitudinal data on participants’ premorbid personality traits or baseline anxiety levels prior to CKD diagnosis were not available, and thus the potential influence of pre-existing temperament cannot be fully ruled out.
Third, although CKD stage was identified as an important factor associated with illness perception profiles, disease progression over time was not assessed, which may influence patients’ cognitive and emotional representations of illness.
Finally, the internal consistency of the psychological flexibility measure (CompACT) in this study was relatively low, with a Cronbach’s alpha of 0.624, which is below the conventional threshold of 0.70. Although this value is considered acceptable in exploratory research, it may have affected the precision of the psychological flexibility assessment and should be taken into account when interpreting the related findings.
Conclusion
This study identified three distinct patterns of illness perception among patients with CKD using latent profile analysis, providing a person-centered perspective on heterogeneity in illness perception. In addition, we examined clinical and psychosocial factors influencing profile membership and found that CKD stage, number of concomitant symptoms, psychological flexibility, family resilience, and social support were significant determinants of illness perception profiles. Moreover, the findings demonstrate that latent profiles of illness perception were independently associated with FoP in CKD patients and explained additional variance beyond key clinical and demographic variables. Importantly, these results highlight the clinical value of identifying specific subgroups of patients. In particular, patients characterized by a Moderate Perception-Passive Acceptance profile may benefit from targeted interventions aimed at enhancing illness awareness, psychological flexibility, and engagement in disease management. Furthermore, the predominance of emotionally sensitive profiles underscores the need for routine psychological screening in renal care. Future longitudinal and intervention studies are warranted to examine changes in illness perception over time and to evaluate the effectiveness of profile-based psychological interventions in reducing FoP and improving psychological outcomes in patients with CKD.
Data Sharing Statement
The datasets generated and/or analyses during the present investigation are not public available since they are also being used for ongoing study. However, they can be obtained from the corresponding author (Yan Cui) upon reasonable request.
Ethics Approval and Consent to Participate
This survey was approved by the Institutional Review Board (IRB) of Nanjing Medical University in March 2023, (IRB No: (2023)494#). In accordance with the Declaration of Helsinki, all patients provided written informed consent prior to participating in this study.
Acknowledgments
The authors would like to thank all the participants. We also gratefully acknowledge the contributions of Head Nurse Meiling Chen from Yifu Hospital of Nanjing Medical University, Head Nurse Wenjuan Chen from Jingjiang People’s Hospital, and Nurse Wenjie Shi from Jiangsu Provincial Hospital of Traditional Chinese Medicine for their valuable assistance in data collection.
Funding
Jiangsu Provincial People’s Hospital Clinical Competency Enhancement Project – Nursing Program, No. JSPH-NC-2022-3.
Disclosure
The authors declare that they have no competing interests.
References
1. Chen TK, Knicely DH, Grams ME. Chronic kidney disease diagnosis and management: a review. JAMA. 2019;322(13):1294–15. PMID: 31573641; PMCID: PMC7015670. doi:10.1001/jama.2019.14745
2. Tuttle KR, Hauske SJ, Canziani ME, et al; ASi in CKD Group. Efficacy and safety of aldosterone synthase inhibition with and without empagliflozin for chronic kidney disease: a randomised, controlled, phase 2 trial. Lancet. 2024;403(10424):379–390. PMID: 38109916. doi:10.1016/S0140-6736(23)02408-X
3. Evans M, Lewis RD, Morgan AR, et al. A narrative review of chronic kidney disease in clinical practice: current challenges and future perspectives. Adv Ther. 2022;39(1):33–43. PMID: 34739697; PMCID: PMC8569052. doi:10.1007/s12325-021-01927-z
4. Huang CW, Wee PH, Low LL, et al. Prevalence and risk factors for elevated anxiety symptoms and anxiety disorders in chronic kidney disease: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2021;69:27–40. PMID: 33516963. doi:10.1016/j.genhosppsych.2020.12.003
5. Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet. 2017;389(10075):1238–1252. PMID: 27887750. doi:10.1016/S0140-6736(16)32064-5
6. Allen K, Damery SL, Sein K, et al. How do patients and their family members experience the transition from peritoneal dialysis to incentre haemodialysis? A multisite qualitative study in England and Australia. Perit Dial Int. 2022;42(3):297–304. PMID: 33331224. doi:10.1177/0896860820975596
7. Frontini R, Sousa H, Ribeiro Ó, Figueiredo D. “What do we fear the most?”: exploring fears and concerns of patients, family members and dyads in end-stage renal disease. Scand J Caring Sci. 2021;35(4):1216–1225. PMID: 33615525. doi:10.1111/scs.12940
8. Dankert A, Duran G, Engst-Hastreiter U, et al. Progredienzangst bei patienten mit tumorerkrankungen, diabetes mellitus und entzündlich-rheumatischen erkrankungen [Fear of progression in patients with cancer, diabetes mellitus and chronic arthritis]. Rehabilitation. 2003. 42(3):155–163. German. PMID: 12813652. doi:10.1055/s-2003-40094
9. Simon R, Latreille J, Matte C, Desjardins P, Bergeron E. Adherence to adjuvant endocrine therapy in estrogen receptor-positive breast cancer patients with regular follow-up. Can J Surg. 2014;57(1):26–32. PMID: 24461223; PMCID: PMC3908992. doi:10.1503/cjs.006211
10. Sharpe L, Michalowski M, Richmond B, Menzies RE, Shaw J. Fear of progression in chronic illnesses other than cancer: a systematic review and meta-analysis of a transdiagnostic construct. Health Psychol Rev. 2023;17(2):301–320. PMID: 35132937. doi:10.1080/17437199.2022.2039744
11. Wu J, Lan X, Liao Z, Chen J, Wu Y, Hu R. Comparison of the sense of spousal support, anxiety, depression and their relationship to fear of cancer recurrence between lymphoma patients and their spouses: a cross-sectional study in China. J Cancer Surviv. 2025;19(1):1–11. PMID: 37610477. doi:10.1007/s11764-023-01443-9
12. Zheng W, Hu M, Liu Y. Social support can alleviate the fear of cancer recurrence in postoperative patients with lung carcinoma. Am J Transl Res. 2022;14(7):4804–4811. PMID: 35958474; PMCID: PMC9360850.
13. Li MC, Cheng HL. Fear of cancer recurrence, supportive care needs, and the utilization of psychosocial services in cancer survivors: a cross-sectional survey in Hong Kong. Psychooncology. 2021;30(4):602–613. PMID: 33247969. doi:10.1002/pon.5609
14. Xiong J, Qin J, Gong K. Association between fear of progression and sleep quality in patients with chronic heart failure: a cross-sectional study. J Adv Nurs. 2023;79(8):3082–3091. PMID: 36978259. doi:10.1111/jan.15657
15. Lee-Jones C, Humphris G, Dixon R, Hatcher MB. Fear of cancer recurrence--a literature review and proposed cognitive formulation to explain exacerbation of recurrence fears. Psychooncology. 1997;6(2):95–105. PMID: 9205967. doi:10.1002/(SICI)1099-1611(199706)6:2<95::AID-PON250>3.0.CO;2-B
16. Chen R, Yang H, Zhang H, Chen J, Liu S, Wei L. Fear of progression among postoperative patients with newly diagnosed lung cancer: a cross-sectional survey in China. BMC Psychol. 2023;11(1):168. PMID: 37217966; PMCID: PMC10201766. doi:10.1186/s40359-023-01211-5
17. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. PMID: 16731240. doi:10.1016/j.jpsychores.2005.10.020
18. Hagger MS, Koch S, Chatzisarantis NLD, Orbell S. The common sense model of self-regulation: meta-analysis and test of a process model. Psychol Bull. 2017;143(11):1117–1154. PMID: 28805401. doi:10.1037/bul0000118
19. Leventhal H, Diefenbach M, Leventhal EA. Illness cognition using common sense to understand treatment adherence and affect cognition interactions. Cognit Ther Res. 1992;6(2):143–163. doi:10.1007/BF01173486
20. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. PMID: 27515801. doi:10.1007/s10865-016-9782-2
21. Hagger MS, Orbell S. The common sense model of illness self-regulation: a conceptual review and proposed extended model. Health Psychol Rev. 2022;16(3):347–377. PMID: 33461402. doi:10.1080/17437199.2021.1878050
22. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the brief illness perception questionnaire. Psychol Health. 2015;30(11):1361–1385. PMID: 26181764. doi:10.1080/08870446.2015.1070851
23. Duan D, Yang L, Zhang M, Song X, Ren W. Depression and associated factors in Chinese patients with chronic kidney disease without dialysis: a cross-sectional study. Front Public Health. 2021;9:605651. PMID: 34123983; PMCID: PMC8192721. doi:10.3389/fpubh.2021.605651
24. Zhu B, Wu H, Lv S, Xu Y. Association between illness perception and social alienation among maintenance hemodialysis patients: the mediating role of fear of progression. PLoS One. 2024;19(4):e0301666. PMID: 38564570; PMCID: PMC10986954. doi:10.1371/journal.pone.0301666
25. Shim EJ, Lee JW, Min YH. Does depression decrease the moderating effect of self-efficacy in the relationship between illness perception and fear of progression in breast cancer? Psychooncology. 2018;27(2):539–547. PMID: 28816370. doi:10.1002/pon.4532
26. Ma H, Hu K, Wu W, et al. Illness perception profile among cancer patients and its influencing factors: a cross-sectional study. Eur J Oncol Nurs. 2024;69:102526. PMID: 38401348. doi:10.1016/j.ejon.2024.102526
27. Kajiwara Y, Morimoto M. Identification of illness representational patterns and examining differences of self-care behavior in the patterns in chronic kidney disease. PLoS One. 2023;18(3):e0283701. PMID: 37000861; PMCID: PMC10065431. doi:10.1371/journal.pone.0283701
28. Valentine TR, Presley CJ, Carbone DP, Shields PG, Andersen BL. Illness perception profiles and psychological and physical symptoms in newly diagnosed advanced non-small cell lung cancer. Health Psychol. 2022;41(6):379–388. PMID: 35604701; PMCID: PMC9817475. doi:10.1037/hea0001192
29. Wang X, Li X, Zhang Z, et al. A latent profile analysis of psychological resilience in gastric cancer survivors: a cross-sectional study. Eur J Oncol Nurs. 2024;70:102612. PMID: 38795446. doi:10.1016/j.ejon.2024.102612
30. Zhou XY, Wang YF, Yang JM, et al. Latent profile analysis and influencing factors of quality of life in pregnant women with gestational diabetes mellitus. BMC Pregnancy Childbirth. 2023;23(1):785. PMID: 37951868; PMCID: PMC10638685. doi:10.1186/s12884-023-06079-2
31. Jamali J, Ayatollahi SM. Classification of Iranian nurses according to their mental health outcomes using Ghq-12 questionnaire: a comparison between latent class analysis and K-means clustering with traditional scoring method. Mater Sociomed. 2015;27(5):337–341. PMID: 26622202; PMCID: PMC4639329. doi:10.5455/msm.2015.27.337-341
32. Steinley D, Brusco MJ. Evaluating mixture modeling for clustering: recommendations and cautions. Psychol Methods. 2011;16(1):63–79. PMID: 21319900. doi:10.1037/a0022673
33. Rivera E, Tintle N, Townsend RR, et al. Characterization of CKD illness representation profiles using patient-level factors. J Nephrol. 2024;37(3):671–679. PMID: 38727894. doi:10.1007/s40620-024-01955-2
34. TTimkova V, Mikula P, Fedicova M, Szilasiova J, Nagyova I. Psychological well-being in people with multiple sclerosis and its association with illness perception and self-esteem. Mult Scler Relat Disord. 2021;54:103114. PMID: 34217996. doi:10.1016/j.msard.2021.103114
35. Xu X, Chen X, Wang T, Qiu C, Li M. Relationship between illness perception and family resilience in gynecologic cancer patients: the mediating role of couple illness communication. Support Care Cancer. 2023;31(9):522. PMID: 37581695. doi:10.1007/s00520-023-07992-0
36. Hu N, Wang A, Chang T. Social support mediates the relationship between illness perception and psychosocial adaptation among young and middle-aged kidney transplant recipients in China. Front Psychol. 2023;14:1062337. PMID: 36910788; PMCID: PMC9998938. doi:10.3389/fpsyg.2023.1062337
37. Disease K; Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117–S314. PMID: 38490803. doi:10.1016/j.kint.2023.10.018
38. Herschbach P, Berg P, Dankert A, et al. Fear of progression in chronic diseases: psychometric properties of the fear of progression questionnaire. J Psychosom Res. 2005;58(6):505–511. PMID: 16125517. doi:10.1016/j.jpsychores.2005.02.007
39. Huang Y, Luo Y, Liu J, Qiaoying F. Chinese version and reliability and validity test of Fear of Progression Questionnaire. Chin J Mod Nurs. 2022;28:155–161. doi:10.3760/cma.j.cn115682-20210325-01318
40. Francis AW, Dawson DL, Golijani-Moghaddam N. The development and validation of the comprehensive assessment of acceptance and commitment therapy processes (CompACT). J Context Behav Sci. 2016;5(3):134–145. doi:10.1016/j.jcbs.2016.05.003
41. Ge HY. Study on Psychological Flexibility and Its Influencing Factors in Patients with Atrial Fibrillation. Tianjing Medical University; 2020.
42. Faccio F, Renzi C, Crico C, et al. Development of an eHealth tool for cancer patients: monitoring psycho-emotional aspects with the Family Resilience (FaRe) Questionnaire. Ecancermedicalscience. 2018;12:852. PMID: 30079114; PMCID: PMC6057659. doi:10.3332/ecancer.2018.852
43. Li MM. The Chinese Localization of the Family Resilience Questionnaire and the Application in Patients with Breast Cancer. Zhengzhou University; 2021.
44. Xiao S. The theoretical basis and applications of social support rating scale (SSRs). J Clin Psychiatry. 1994;4:98–100.
45. Luo B, Luo Z, Zhang X, Xu M, Shi C. Status of cognitive frailty in elderly patients with chronic kidney disease and construction of a risk prediction model: a cross-sectional study. BMJ Open. 2022;12(12):e060633. PMID: 36572488; PMCID: PMC9806025. doi:10.1136/bmjopen-2021-060633
46. IBM Corp. IBM SPSS statistics for windows, version 22.0. Armonk, NY IBM Corp; 2013 [Cited May 13, 2025]. Available from: https://www.ibm.comproductsspss-statistics.pdf.
47. Muthén LK, Muthén BO. Mplus Version 8.3 [software]. Los Angeles, CA Muthén & Muthén; 2019 [Cited May 13, 2025]. Available from: https://www.statmodel.com.
48. Nylund-Gibson K, Choi AY. Ten frequently asked questions about latent class analysis. Transl Issues Psychol Sci. 2018;4(4):440–461. doi:10.1037/tps0000176
49. Meuleman Y, de Goeij MC, Halbesma N, Chilcot J, Dekker FW, van Dijk S; PREPARE-2 Study Group. Illness perceptions in patients on predialysis care: associations with time until start of dialysis and decline of kidney function. Psychosom Med. 2015;77(8):946–954. PMID: 26230483. doi:10.1097/PSY.0000000000000220
50. Wright HH, Kickbusch H, Swanepoel E, Gray N. Factors influencing low sodium intake in people with non-dialysis dependent chronic kidney disease. J Ren Care. 2020;46(2):95–105. Epub 2019 Dec 22. PMID: 31867867. doi:10.1111/jorc.12311
51. Meuleman Y, van der Bent Y, Gentenaar L, et al. Exploring patients’ perceptions about chronic kidney disease and their treatment: a qualitative study. Int J Behav Med. 2024;31(2):263–275. Epub 2023 May 24. PMID: 37226037; PMCID: PMC10208195. doi:10.1007/s12529-023-10178-x
52. Zukerman G, Maor M, Reichard T, Ben-Itzhak S. Beyond illness perception: the effects of psychological flexibility when coping with a chronic medical condition. Psychol Health Med. 2023;28(7):1795–1802. Epub 2022 Apr 19. PMID: 35440254. doi:10.1080/13548506.2022.2067344
53. Cherry KM, Hoeven EV, Patterson TS, Lumley MN. Defining and measuring “psychological flexibility”: a narrative scoping review of diverse flexibility and rigidity constructs and perspectives. Clin Psychol Rev. 2021;84:101973. Epub 2021 Jan 21. PMID: 33550157. doi:10.1016/j.cpr.2021.101973
54. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44(1):1–25. PMID: 16300724. doi:10.1016/j.brat.2005.06.006
55. Thomas KN, Bardeen JR, Witte TK, Rogers TA, Benfer N, Clauss K. An examination of the factor structure of the multidimensional psychological flexibility inventory. Assessment. 2022;29(8):1714–1729. Epub 2021 Jul 7. PMID: 34232088. doi:10.1177/10731911211024353
56. Walsh F. Family resilience: a framework for clinical practice. Fam Process. 2003;42(1):1–18. PMID: 12698595. doi:10.1111/j.1545-5300.2003.00001.x
57. Kuang Y, Wang M, Yu NX, et al. Family resilience of patients requiring long-term care: a meta-synthesis of qualitative studies. J Clin Nurs. 2023;32(13–14):4159–4175. PMID: 36030397. doi:10.1111/jocn.16500
58. Ding YM, Liu CP, Xu HX, et al. Effect of social support on illness perception in patients with atrial fibrillation during “Blanking Period”: mediating role of sense of mastery. Nurs Open. 2023;10(1):115–122. Epub 2022 Jul 19. PMID: 35855521; PMCID: PMC9748061. doi:10.1002/nop2.1284
59. Muscat P, Weinman J, Farrugia E, Callus R, Chilcot J. Illness perceptions predict distress in patients with chronic kidney disease. BMC Psychol. 2021;9(1):75. PMID: 33962685; PMCID: PMC8105921. doi:10.1186/s40359-021-00572-z
60. Yang Y, Sun H, Liu T, et al. Factors associated with fear of progression in Chinese cancer patients: sociodemographic, clinical and psychological variables. J Psychosom Res. 2018;114:18–24. Epub 2018 Sep 7. PMID: 30314574. doi:10.1016/j.jpsychores.2018.09.003
61. Wang Y, Yu Q, Zeng Z, et al. Predictors of fear of diabetes progression: a multi-center cross-sectional study for patients self-management and healthcare professions education. Front Public Health. 2022;10:910145. PMID: 36600932; PMCID: PMC9806215. doi:10.3389/fpubh.2022.910145
62. Li B, Lin X, Chen S, et al. The association between fear of progression and medical coping strategies among people living with HIV: a cross-sectional study. BMC Public Health. 2024;24(1):440. PMID: 38347483; PMCID: PMC10860317. doi:10.1186/s12889-024-17969-1
63. Iroegbu C, Tuot DS, Lewis L, Matura LA. The influence of patient–provider communication on self-management among patients with chronic illness: a systematic mixed studies review. J Adv Nurs. 2025;81(4):1678–1699. doi:10.1111/jan.16492
64. Gong SA, Ao SH, Chen YS. The influence of patient-centered communication on psychological distress: the chain mediating role of health-related self-efficacy and healthy lifestyle behaviors and the moderating role of social media use. Front Psychiatry. 2025;16:1562414. doi:10.3389/fpsyt.2025.1562414
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.