Back to Journals » Patient Preference and Adherence » Volume 19
Latent Profile Analysis for Patient Activation in Patients with Essential Hypertension
Received 25 February 2025
Accepted for publication 22 July 2025
Published 26 August 2025 Volume 2025:19 Pages 2635—2645
DOI https://doi.org/10.2147/PPA.S524968
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Video abstract presented by Wang.
Views: 127
Qingqing Wang,1 Xiao Xin,2 Xianhua Li1,3
1School of Nursing, Shanghai Jiao Tong University, School of Nursing, Shanghai, People’s Republic of China; 2Department of Oncology, Ruijin Hospital, Shanghai Jiao Tong University, School of Nursing, Shanghai, People’s Republic of China; 3Outpatient Department, Ruijin Hospital, Shanghai Jiao Tong University, School of Nursing, Shanghai, People’s Republic of China
Correspondence: Xianhua Li, Outpatient Department, Ruijin Hospital, Shanghai Jiao Tong University, School of Nursing, Shanghai, People’s Republic of China, Tel/Fax +8617775437057, Email [email protected]
Purpose: Hypertension constitutes a significant global health issue, requiring active patient participation in self-management and health-related behaviors. Patient activation is defined as the knowledge, skills, and confidence in the management of their health. Prior studies have primarily employed total-score methods, potentially overlooking the variability in patient engagement. This study employs Latent Profile Analysis (LPA) to identify distinct patient activation profiles and investigate key predictors influencing activation levels in individuals with hypertension.
Patients and Methods: A convenience sampling method was employed to select 301 patients with essential hypertension from an outpatient clinic in a tertiary care hospital located in Shanghai for a cross-sectional study. A general demographic questionnaire, the Patient Activation Measure (PAM), the General Self-Efficacy Scale (GSES), the Health Literacy Scale for patients with chronic diseases (HLSCP), and the Hypertension Adherence Scale (TASHP) were utilized. Latent profile analysis was employed to investigate the latent profiles of patient activation, while univariate analysis and binomial logistic regression were used to identify significant predictors of patient activation types, based on factors found significant in univariate analysis.
Results: The research revealed two distinct latent profiles of patient activation in individuals with essential hypertension: High Cognition-Proactive Action Type (33.9%) and Passive Cognition-Low Skills Type (66.1%). The logistic regression analysis indicated that monthly income (OR=1.725, p< 0.05), self-efficacy (OR=1.162, p< 0.01), and health literacy (OR=1.027, p< 0.05) are significant predictors of patient activation.
Conclusion: Patients with essential hypertension exhibit diverse activation levels, with a majority (66.1%) demonstrating low skills and passive cognition, indicating the need for targeted interventions. Increased income, health literacy and self-efficacy facilitate activation. Interventions must improve self-efficacy and refine health education to enhance patient engagement and self-management.
Keywords: essential hypertension, patient activation, patient participation, latent profile analysis, health literacy, self-efficacy
Introduction
Essential hypertension has emerged as one of the chronic non-communicable diseases with the greatest global disease burden.1 The incidence of essential hypertension is rising every year, and the morbidity and mortality rates associated with cardiovascular and cerebrovascular illnesses are persistently escalating.2 Effective control of blood pressure is essential for reducing the risk of cardiovascular disease. However, clinical interventions alone are insufficient; long-term management requires active patient engagement in health-related behaviors. In this context, the concept of patient activation becomes particularly relevant.3
Patient activation refers to the knowledge, skills, and confidence individuals possess to take charge of their health and health care.4 It plays a key role in promoting self-care and health-related behaviors, especially among patients with chronic conditions such as hypertension.5 Enhancing patient activation is essential for achieving improved blood pressure control and increasing treatment adherence.6 Patients with higher activation are more likely to actively monitor their blood pressure, adhere to medication regimens, and modify their diet and exercise habits, resulting in significantly improved treatment adherence.7 Simultaneously, individuals exhibit an increased willingness to engage with their physicians regarding their needs during consultations, obtain tailored health recommendations, and effectively execute treatment strategies, thereby fostering healthier lifestyles and enhancing health outcome.8–10 These factors are crucial for attaining blood pressure regulation in individuals with essential hypertension,11,12 The transition from passive patient care to active patient involvement in health management significantly influences health outcomes and the quality of care.13 The Quadruple Aim encompasses the enhancement of population health, cost-effectiveness of the healthcare system, patient experience, and job satisfaction of healthcare professionals, which can be realized through the promotion of patient activation.14–17
Although patient activation is recognized as a key driver of self-management in chronic disease care, studies consistently report that many individuals with hypertension exhibit low activation levels.18 This discrepancy underscores the importance of identifying context-specific determinants that influence activation. Previous studies have primarily employed the total-score method of questionnaires, representing a variable-centered approach that may overlook inter-individual variability.12,19 Latent Profile Analysis (LPA) is a person-centered statistical approach used to uncover latent subgroups within a population based on similar response patterns. Unlike total-score methods, LPA captures unobserved heterogeneity and facilitates the development of profile-specific interventions.20 This study applied LPA to identify distinct activation profiles and examine their associated demographic and contextual determinants. The social-ecological model posits that health behaviors arise from a confluence of multilevel factors.21 This study categorizes the factors influencing patient activation into three groups, namely demographic factors, disease-related factors, and psychosocial factors. The objective of this study was to delineate the current status of activation in patients with essential hypertension and to utilize LPA for identifying subgroups of patients exhibiting activation along with their influencing factors.
Methods
Study Design and Participants
This study chose outpatients with essential hypertension from a tertiary care hospital in Shanghai between October and December 2024, using a convenience sampling method. Participants completed paper-based questionnaires on-site, with trained research staff available to provide clarification when needed. Data collection and quality assurance procedures are detailed in the subsequent section. Inclusion criteria: (a) age ≥18 years; (b) physician-confirmed diagnosis of essential hypertension according to the 2023 International Society of Hypertension Global Hypertension Practice (ISH) Guidelines,22 defined as: office blood pressure (BP) ≥140/90mmHg (or home BP ≥135/85mmHg) without antihypertensive treatment; secondary causes excluded based on routine clinical evaluations documented in electronic medical records (EMR), with no restriction on the timing of diagnosis, provided documentation was available in the electronic medical records;(c) ability to communicate independently, as assessed by trained staff through verbal interaction and observation; and (d) informed agreement for participation. Exclusion criteria: (a) patients with significant problems, such as severe cardiac, pulmonary, and renal insufficiency; (b)patients with secondary hypertension were excluded based on the 2023 ISH Guidelines,22 which recommend etiological screening in cases of resistant hypertension or suggestive clinical features (e.g., renal artery stenosis, primary aldosteronism). Sample size calculations for logistic regression analyses suggest that the sample size should be 5 to 10 times the number of independent variables.23 With 15 independent variables, a minimum sample size of 165 is necessary, accounting for a 10% missing rate. For the latent profile analysis (LPA), a larger sample of at least 200 participants was considered appropriate.20 A total of 309 questionnaires were distributed in this study, with 8 incomplete responses excluded. A total of 301 self-administered, paper-based questionnaires were included, yielding a return rate of 97.41%.
Data Collection and Quality Control
The corresponding author first contacted the head nurses of the participating hospital departments, who nominated nurses with strong clinical experience to serve as field data collectors. After obtaining departmental approval, the research team explained the study objectives and procedures to eligible participants, and written informed consent was obtained prior to questionnaire administration. Prior to the start of the study, they received standardized training conducted by the investigators.The training covered participant eligibility screening, survey administration procedures, communication protocols, and techniques for minimizing data errors. To ensure procedural consistency, the training incorporated case-based discussions and short role-play exercises. A written assessment was conducted to evaluate comprehension, and a refresher session was held immediately before formal data collection. Participant completed self-administered paper-based questionnaires during their outpatient visit, consisting of single-choice and Likert-scale items, with responses marked by ticking the predefined options on the questionnaire. Trained staffs were available to clarify questions without influencing responses. All completed questionnaires were reviewed on-site by a second trained staff member to check for completeness and legibility. Subsequently, trained staff members independently entered the data into an electronic database. Discrepancies between entries were resolved through cross-checking. The finalized dataset was imported into SPSS version 26.0 and Mplus version 8.3 software for analysis. All procedures were carried out in accordance with predefined protocols to minimize bias and maintain data integrity.
Measurements
Data collection encompassed three domains:
Demographic and Disease-Related Characteristics
Data included sex, age, marital status, residency status, income, education level, and Body Mass Index (BMI). Disease-related variables covered comorbid chronic diseases, first diagnosis status, disease duration, hypertension classification, and family history of essential hypertension.
Psychosocial Dimensions
Psychosocial factors were assessed using validated scales:
Patient Activation Measure (PAM-13)
PAM-13 was created by Hibbard to evaluate patients’ beliefs, knowledge, skills, and confidence in managing their health and health care.24 The scale consists of 13 items and encompasses four dimensions: perceptions, skills, behaviors, and beliefs. It encompasses a total of 13 items rated on a 5-point Likert scale, where 1–4 indicates a range from strongly disagree to strongly agree. The aggregate of the components constitutes the raw scale score, which is logarithmically transformed to a 0–100 scale. Scores of 47.0 denote the first level; 47.1–55.1 indicate the second level; 55.2–67.0 indicate the third level; and ≥67.1 corresponds to the fourth level, with higher scores reflecting greater patient activation. Patients in Level 1 (score ≤ 47) tend to lack confidence in their ability to manage their health and possess limited knowledge about their condition and necessary self-care practices. In Level 2 (47.1–55.1), patients recognize the importance of self-management and have basic knowledge of their condition, but they lack the skills and confidence to effectively manage their health. Level 3 patients (55.2–67.0) are able to take active steps to manage their symptoms and prevent further issues, although they may still lack the confidence to maintain long-term health. Finally, Level 4 patients (score > 67) have the knowledge, skills, and confidence to manage their health, but may struggle to sustain their health practices in the face of stress or unexpected challenges. The use of this instrument has been validated in chronic disease populations in China.16 The raw scores of all elements were aggregated, and the total scores were computed by conversion, yielding a range of 0–100. The Cronbach’s α coefficient for the scale in this study was 0.903, indicating strong reliability and validity.
General Self-Efficacy Scale (GSES)
The Generalized Self-Efficacy Scale (GSES) was created by Schwarzer et al, in 1981 to evaluate individuals’ confidence in their capacity to function competently in diverse stressful or challenging circumstances.25 The scale has 10 items and is evaluated using a 4-point Likert scale, where responses range from “completely incorrect” to “completely correct” assigning scores from 1 to 4. The total score ranges from 10 to 40, with higher scores reflecting greater self-efficacy. A higher score indicates greater self-efficacy in the individual. The Cronbach’s α coefficient for this scale in the present investigation was 0.886.
Health Literacy Scale for Chronic Patients (HLSCP)
The Health Literacy Skills and Competency Profile (HLSCP),26 developed by Professor Jordan, effectively assesses patients’ health literacy levels through 24 items across four dimensions: information acquisition (9 items), communication and interaction (9 items), willingness to enhance health status (4 items), and willingness to offer financial support (4 items). A 5-point Likert scale was employed, yielding a total score range of 24 to 120; a higher score indicates a greater level of patient health literacy. A score of 96 or above indicated proficient health literacy, whereas a score below 96 signified inadequate health literacy. The Cronbach’s α coefficient for this scale in the study was 0.780.
Treatment Adherence Scale for Hypertensive Patients (TASHP)
This Treatment Adherence Scale for Hypertensive Patients (TASHP) scale was created by Tang Honeying in 2011 to evaluate the extent of compliance with medical recommendations, pharmacotherapy, and lifestyle modifications in hypertension patients undergoing treatment.27 The measure comprised medication adherence behaviors (5 items), adverse medication behaviors (8 items), daily life management behaviors (10 items), and tobacco and alcohol addiction management behaviors (2 items), totaling 25 items across 4 dimensions. A 5-point Likert scale was employed, spanning from “no or very little time” to “all the time” with scores ranging from 1 to 5, where items 1 and 6–13 were negatively graded. The overall score ranged from 25 to 125, with elevated scores indicating superior treatment adherence. The Cronbach’s α coefficient for this scale was 0.841.
Analysis of Data
Data analysis was conducted utilizing SPSS version 26.0 and Mplus version 8.3 software. Categorical variables were reported as frequencies and percentages. Continuous variables were assessed for normality using the Shapiro–Wilk test (p > 0.05 indicating normality). Normally distributed variables were presented as mean and standard deviation, while non-normally distributed data were represented as median and interquartile range. LPA was conducted using Mplus to identify potential categories of patient activation among hypertensive patients. Initially, a single-category model was employed, and additional categories were incorporated incrementally until the optimal model was identified. Assessment metrics included the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and adjusted BIC (aBIC), where lower values indicate a better fit. An entropy value of ≥ 0.8 signifies high classification accuracy.28 Additionally, the Lo-Mendell-Rubin adjusted likelihood ratio test (LMRT) and Bootstrap likelihood ratio test (BLRT) were employed, with p < 0.05 indicating a superior model. LMRT and BLRT were employed to assess the fit of the class k model relative to the class k-1 model, with p-values less than 0.05 signifying a statistically significant improvement for the class k model. The p-value of 0.05 indicates that the class k model outperformed the class k-1 model significantly.29 The distribution of categories and the differences in characteristics among them were utilized to assist in model selection. Furthermore, to enhance the robustness of the results, the analysis was conducted multiple times with various randomized initial values for validation purposes. The significance level was established at α = 0.05.
Ethical Considerations
This study obtained approval from Ruijin Hospital, Shanghai Jiao Tong University, School of Nursing, under ChiCTR registration number ChiCTR2500095173, and was conducted by the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
Results
Characteristics of Hypertensive Patients
This study included 301 hypertensive patients, with a mean age of 58.37 ± 15.1 years and a mean Body Mass Index (BMI) of 24.79 ± 3.02. Among the participants, 165 (54.8%) were male. A total of 277 patients (92%) had a history of essential hypertension. While 168 patients (55.8%) exhibited normal blood pressure. A total of 247 patients (82.1%) resided in urban areas.126 patients (41.9%) held a bachelor’s degree or college diploma in education.135 patients (44.8%) reported a monthly income ranging from 0 to 5000 RMB. A total of 254 patients (84.4%) were identified as married. 232 patients (77.1%) were not newly diagnosed, while 202 patients (67.1%) presented with one comorbid chronic diseases. 126 patients (41.9%) had a disease duration of less than 5 years.
Potential Profiles of Patient Activation
The overall patient activation score for 301 patients was 60.63 ± 11.32, indicating a third level of patient activation. The cognitive dimension is measured at 10.34 ± 2.27, the skill dimension at 27.68 ± 6.02, the action dimension at 13.79 ± 2.98, and the beliefs dimension at 8.82 ± 2.31. Four latent profile analyses were conducted based on the initial model (refer to Table 1). The Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and adjusted BIC (aBIC) values exhibited a decrease as the number of latent classes increased, suggesting enhanced model fit. In the Lo-Mendell-Rubin adjusted likelihood ratio test (LMRT), the p-value of 0.133 (p > 0.05) for the comparison between the 2-class and 3-class models suggests that the improvement in model fit achieved by including a third class was not statistically significant. The entropy value of the 2-category model is 0.867, exceeding 0.8, indicating high classification quality. The classification probability is balanced at 0.668 versus 0.332, mitigating instability associated with overly small categories. Despite the 3-class model showing a marginally reduced BIC value, the entropy value decreased, and one of the supplementary subgroups comprised a minimal fraction of the sample, complicating interpretation and raising concerns about reliability. Likewise, the 4-class model further divided the sample, resulting in subgroups with minimal practical distinction. In the analysis, the BIC value was minimized at 9243.466 for the 2-category model, and the Bootstrap Likelihood Ratio Test (BLRT) yielded a significant result (p < 0.001), thereby reinforcing the superiority of the 2-category model. Table 2 presents the attribution probability matrices for the two potential categories, with attribution probabilities for each category ranging from 98% to 99.8%, demonstrating a high level of reliability in the classification results. Consequently, by integrating the goodness-of-fit metrics of AIC, BIC, and aBIC, the significance tests of LMRT and BLRT, along with the clarity of classification (entropy values and probability distributions), the two-category latent trait model was identified as the optimal solution, with its feature map presented in Figure 1.
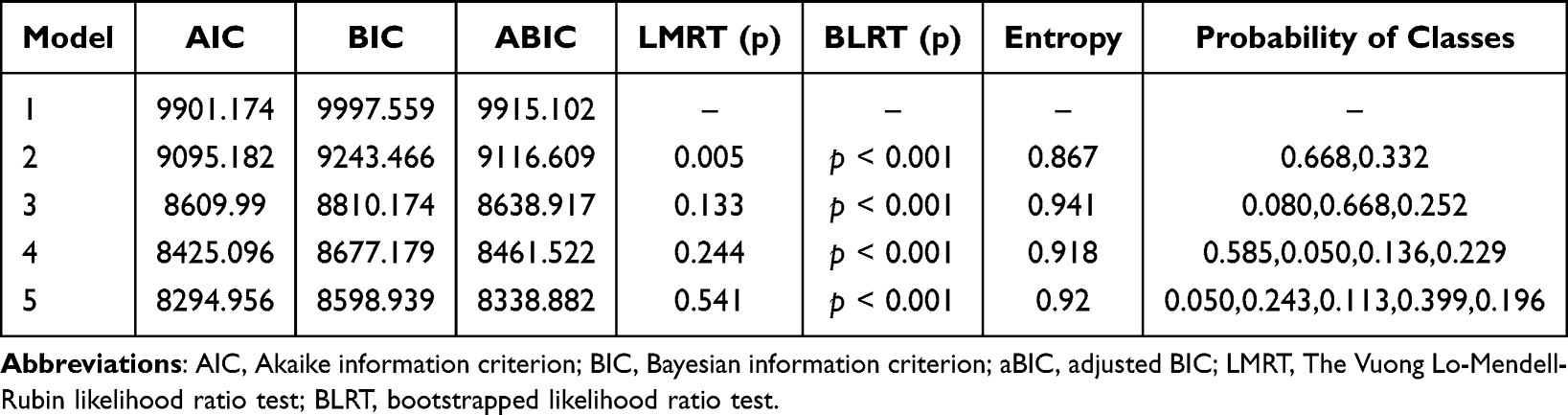 |
Table 1 Model Fit Statistics for LPA Models of Patient Activation in Patients with Essential Hypertension |
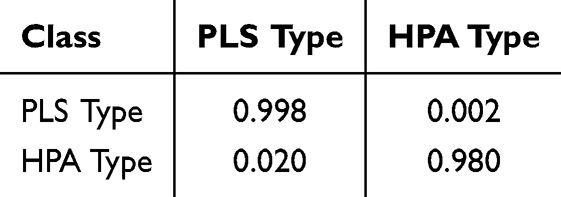 |
Table 2 Attribution Probabilities for Each Latent Profile of Subjects |
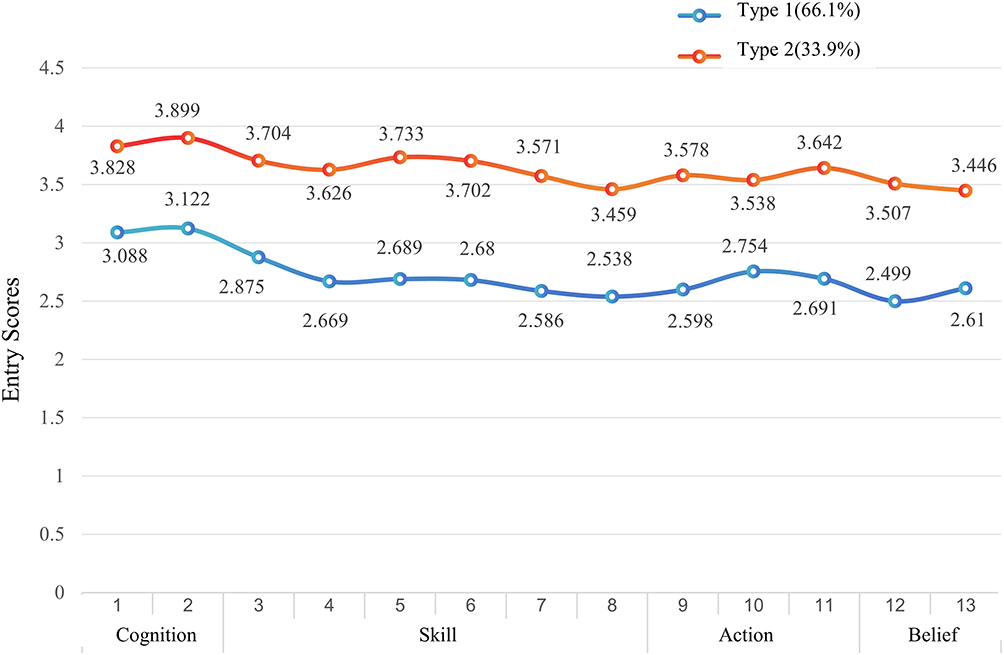 |
Figure 1 Two latent profiles of patient activation in essential hypertension patients. |
Naming and Characterization of Potential Categories
The Patient Activation Theory (PAT) and the PAM-13 scale indicate that the activation levels of hypertensive patients were distinctly stratified in the current study.24,30 The total PAM score for patients in Stage 1 was 54.38±7.84, indicating that they fell within the second level of PAM (Stage 2: Becoming Aware but Still Struggling), reflecting an overall state of passive acceptance of healthcare services. The potential profile analysis revealed a rapid decline in scores for this patient group following the “Cognitive” dimension, particularly in the “Skills” dimension. This suggests that while they recognized the significance of health management, they lacked the necessary learning abilities and self-management skills to convert their understanding into practical behavior. This suggests that while they started to recognize the significance of health management, they did not possess the necessary learning abilities and self-management skills, preventing them from translating their understanding into actionable behavior. This characteristic aligns with the second stage of the Precaution Adoption Model (PAM), indicating that while patients possess some health awareness, they encounter challenges in effectively managing their health. This patient category was designated as “passive cognition-low skills Type” comprising a total of 199 cases (66.1%). In contrast, the total PAM score of patients in Category 2, 72.82 ± 5.74, corresponds to the fourth level of PAM (Stage 4: Maintaining Behaviors and Pushing Further). This indicates that these patients not only exhibit a high level of health cognition but also demonstrate stable health management behaviors over time and engage proactively in self-management. The profile indicates that these patients maintain stable scores in the “Skills” and “Actions” dimensions, highlighting their initiative and sustainability in health management. This characteristic aligns with the fourth stage of PAM, where patients can autonomously manage their health and continuously enhance their self-care practices. Consequently, this cohort of patients was designated as the “High Cognition-Proactive Action Patient Activation Type”.
Univariate Analysis of Latent Profile Categories
The study results indicated statistically significant differences (p < 0.05) between age, monthly income, disease duration, self-efficacy, and health literacy across the two potential profile Types of patient activation in hypertensive patients. Refer to Tables 3 and 4.
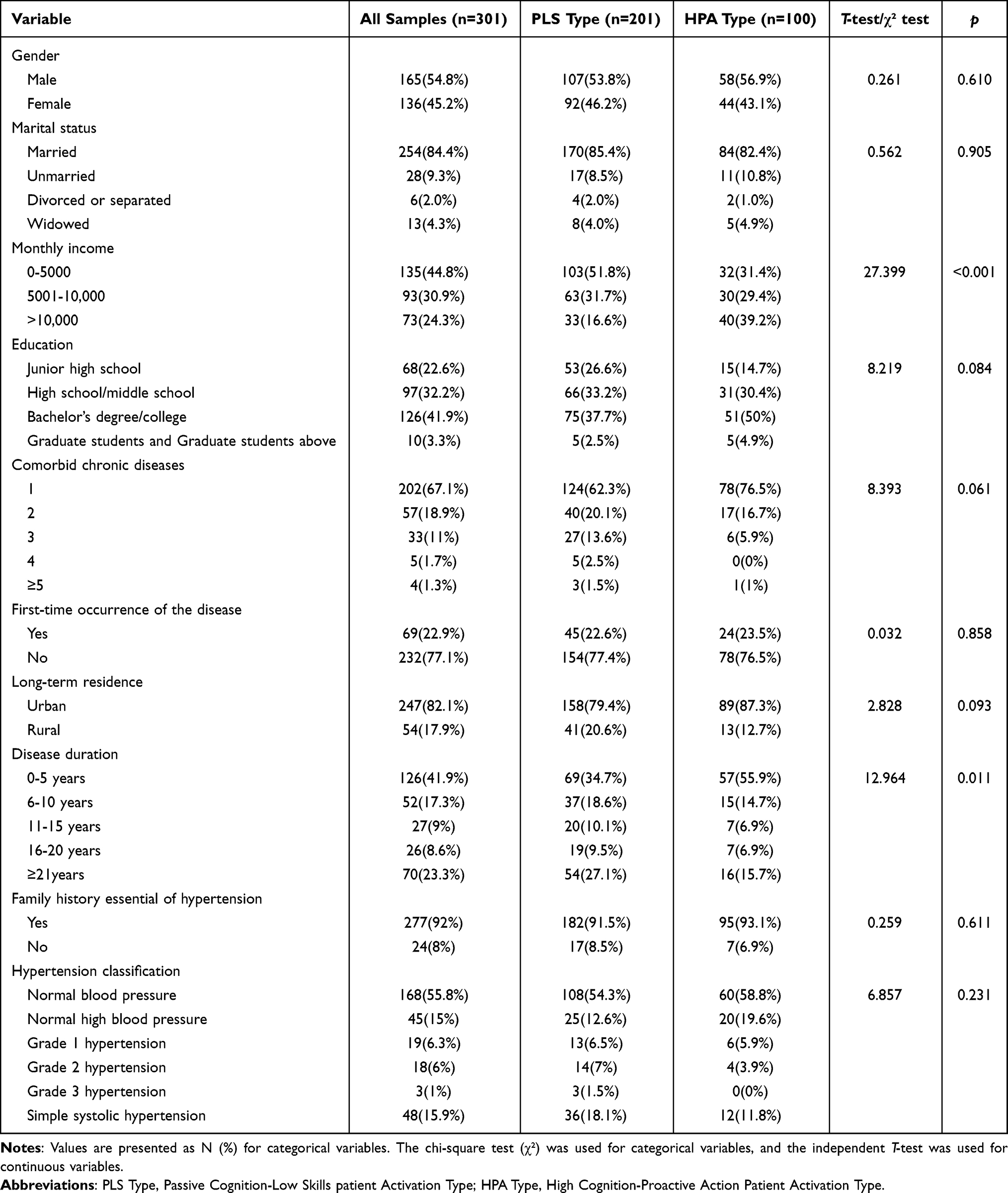 |
Table 3 Univariate Analysis of Demographic Factors Associated with Patient Activation Profiles (n=301) |
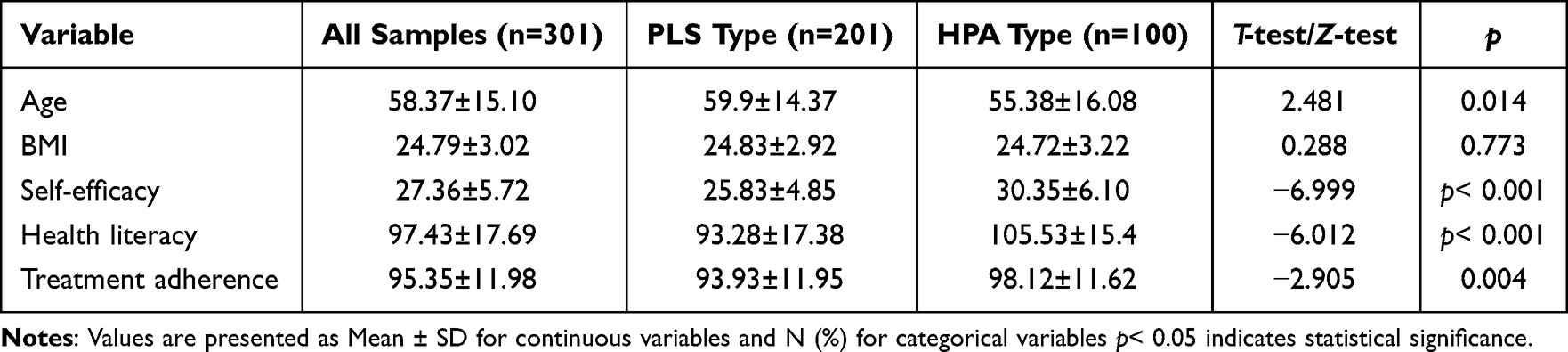 |
Table 4 Comparison of Age, BMI, Self-Efficacy, Health Literacy, and Treatment Adherence Between Patient Activation Profiles (n=301) |
Binary Logistic Regression Analysis of Latent Profile Categories
This study utilized potential profile categories of patient activation as dependent variables, assigning a value of 0 to the “Passive Cognition-Low Skills Patient Activation Type” and a value of 1 to the “High Cognition-Proactive Action Patient Activation Type”. The binary logistic regression model was employed to analyze statistically significant variables across various potential categories, yielding the following values: The disease duration was categorized as follows:0–5 years = 1, 6–10 years = 2, 11–15 years = 3, 16–20 years = 4, and ≥21 years = 5. The monthly income was categorized as follows: <3000 = 1, 3001–5000 = 2, 5001–10,000 = 3, >10,000 = 4. Age, self-efficacy, treatment adherence, and health literacy were recorded using their original values. The model fit test results indicated that the regression model achieved statistical significance at the p<0.05 level. The Hosmer-Lemeshow test produced a p-value of 0.236, suggesting a satisfactory alignment between predicted and observed values, with a model fit of 32.8%. Logistic regression analysis, as presented in Table 5 at the end of the manuscript identified income, sense of self-efficacy, and health literacy as independent predictors of potential categories of patient activation (p < 0.05). Among the identified predictors, higher monthly income, greater self-efficacy, and higher health literacy were significantly associated with classification into the High Cognition–Proactive Action Patient Activation profile. Specifically, participants with higher income levels were 1.72 times more likely to be classified into this group (OR = 1.725, 95% CI:1.225–2.429, p = 0.014). For each unit increase in self-efficacy score, the odds of being in the high activation group increased by 16.2% (OR:1.162, 95% CI = 1.098–1.231, p < 0.01). Similarly each additional point in health literacy was associated with a 2.7% higher likelihood (OR = 1.027, 95% CI: 1.005–1.049, p < 0.05).
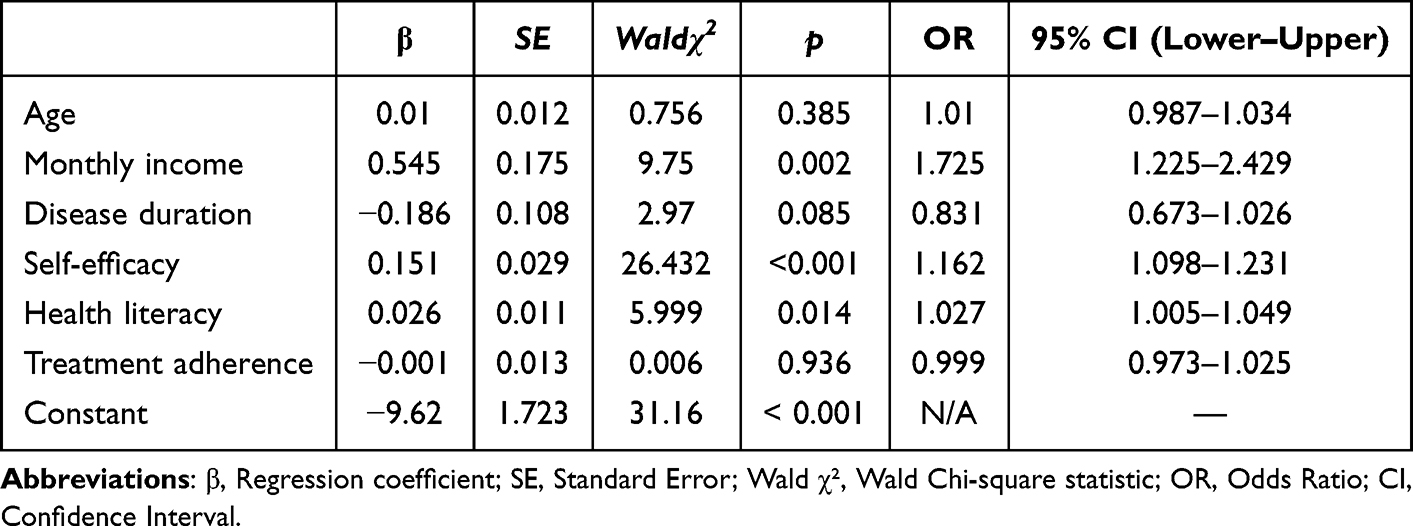 |
Table 5 Two Latent Profiles Probability Matrices of Patient Activation in Essential Hypertension Patients |
Discussion
The findings of this study indicated that 301 individuals with essential hypertension exhibited a patient activation score that was higher than previously reported.12,19 This disparity may reflect differences in participant recruitment settings. The elevated patient activation noted in this study can be ascribed to the recruitment of participants from outpatient clinics, which typically offer more systematic access to healthcare resources, structured education, and disease management than community-based settings.19,31
This study identified two latent patient activation profiles via LPA: the Passive Cognition–Low Skills group and the High Cognition–Proactive Action group, with the former representing the majority of participants. The overall low activation levels of the former group, particularly the reduced scores in cognitive and skill dimensions, indicate deficiencies in disease management awareness and skill acquisition. Intervention strategies must focus on improving cognitive engagement and self-management skills through structured patient education and customized behavioral reinforcement methods.32,33 The integration of cognitive enhancement, skill development, and behavioral reinforcement is crucial for sustainable health management.34
Behavioral triggers such as daily blood pressure reminders and clinician feedback may contribute to improved disease self-management. Incorporating skills training into daily routines can further enhance feasibility and support behavior adoption.35 Income, self-efficacy, and health literacy emerged as key factors differentiating activation subgroups, with lower levels consistently associated with the Passive Cognition–Low Skills profile. These findings suggest that financial constraints may limit access to health resources and increase psychological distress.36,37 Accordingly, expanding affordable management strategies is critical to supporting hypertension control among low-income populations. This includes promoting free or low-cost blood pressure monitoring devices and utilizing telemedicine and mobile health applications to deliver personalized health education, thereby mitigating the influence of economic factors on patients’ health management.38,39
Similar to previous findings, self-efficacy may influence patient activation levels in this study.40,41 In alignment with Bandura’s self-efficacy theory,42 this study demonstrated that patients exhibiting higher self-efficacy displayed increased initiative and adherence to disease management, thereby reinforcing a positive cycle of health behaviors.43 Patients exhibiting low self-efficacy demonstrated a lack of confidence and a higher propensity to abandon management efforts following setbacks. Interventions for these patients should prioritize the establishment of progressive, attainable goals, including daily blood pressure monitoring or enhanced physical activity, to foster confidence through incremental successes.44–46 Moreover, self-management training and behavioral interventions, such as cognitive behavioral therapy (CBT), assist patients in acquiring fundamental health skills and overcoming anxiety-related obstacles to effective disease management.47 This investigation revealed that health literacy significantly influences patient activation levels, with patients exhibiting poorer health literacy more frequently categorized as low-activation types, corroborating prior research.18,48,49 Reduced health literacy impairs patients’ understanding of their condition, adherence to treatment, and self-management skills, thus resulting in inadequate illness control. Moreover, health literacy training must be enhanced in primary care and community health services to facilitate patients’ access to and utilization of health information, hence improving chronic disease management proficiency.50,51
Several limitations should be acknowledged. First, the cross-sectional nature of the study precludes any inference of causality between patient activation levels and associated factors. Second, as the sample was limited to a single tertiary care hospital, the findings may not be generalizable to primary care or rural settings. Third, reliance on self-reported activation levels may introduce reporting bias. Lastly, excluding individuals with impaired communication may have limited the representativeness of the study population and introduced potential selection bias. Future research should adopt longitudinal designs, include more diverse clinical settings, and utilize mixed-method approaches to validate and extend these findings across broader hypertensive populations.
Conclusion
This research delineated two unique patient activation profiles: “Passive Cognition–Low Skills” (66.1%) and “High Cognition–Proactive Action” (33.9%). The latter demonstrated effective health management, whereas the former showed health awareness but lacked self-management skills. This study employed binary logistic regression analysis and determined that income, self-efficacy, and health literacy strongly impacted patient activation levels (p < 0.05). Individuals with elevated income had greater involvement in health management; those with strong self-efficacy exhibited increased confidence and capability in managing their health. Similarly, higher health literacy facilitated better understanding of medical information, improved adherence to treatment plans, and enhanced engagement in self-care practices. Consequently, in essential hypertension care, emphasis should be placed on patients categorized as “Passive Cognition–Low Skills Patient Activation Type” particularly those impacted by financial limitations, low health literacy, or diminished self-efficacy. Accessible health education, coupled with skills training, individualized follow-up, and psychological support, is advised to assist patients in identifying essential information, alleviating anxiety, and enhancing self-management abilities to optimize long-term blood pressure control measures. This study’s identification of distinct activation profiles and their psychosocial predictors offers a preliminary basis for stratified intervention design in essential hypertension care. Targeting low-activation subgroups through tailored education and behavioral support may improve engagement and clinical outcomes. Future studies employing longitudinal and randomized designs are warranted to validate these profiles and assess the effectiveness of profile-specific intervention strategies.
Acknowledgments
We acknowledge the contributions of participants who facilitated data collection.
Ethical Considerations
This study obtained approval from Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, under ChiCTR registration number ChiCTR2500095173, and was conducted by the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
Funding
This work was supported by the Shanghai Shenkang Hospital Development Center under the research grant “Exploratory Study on Outpatient System Optimization under the Background of High-Quality Development of Public Hospitals” (Project No. SHDC12024607).
Disclosure
The authors declare that they have no conflicts of interest related to this study.
References
1. McEvoy JW, McCarthy CP, Bruno RM, et al. ESC guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024;45(38):3912–4018. doi:10.1093/eurheartj/ehae178
2. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi:10.1016/S0140-6736(21)01330-1
3. McCarthy CP, Bruno RM, Rahimi K, Touyz RM, McEvoy JW. Global and European landscape of major hypertension guidelines. Lancet. 2025;(24):2795–2798. doi:10.1016/S0140-6736(24)02795-8
4. Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. 2005;40(6):1918–1930. doi:10.1111/j.1475-6773.2005.00438.x.
5. Satti DI, Chan JSK, Mszar R, et al. Social determinants of health, cardiovascular health, and mortality in sexual minority individuals in the United States. J Am Coll Cardiol. 2025;85(5):515–525. doi:10.1016/j.jacc.2024.11.026
6. Thiboutot J, Sciamanna CN, Falkner B, et al. Effects of a web-based patient activation intervention to overcome clinical inertia on blood pressure control: cluster randomized controlled trial. J Med Internet Res. 2013;15(9):e158. doi:10.2196/jmir.2298
7. Innab A, Kerari A, Alqahtani N, Albloushi M, Alshammari A. Patient activation, adherence to hypertension treatment plans and blood pressure control in Saudi Arabia: a cross-sectional study. BMJ Open. 2023;13(1):e067862. doi:10.1136/bmjopen-2022-067862
8. Acquati C, Hibbard JH, Miller-Sonet E, Zhang A, Ionescu E. Patient activation and treatment decision-making in the context of cancer: examining the contribution of informal caregivers’ involvement. J Cancer Surviv. 2022;16(5):929–939. doi:10.1007/s11764-021-01085-9
9. Mirpuri KK. Three pounds and seven ounces: my patient activation journey. Am J Kidney Dis. 2022;80(5):A14–A15. doi:10.1053/j.ajkd.2022.04.012
10. Sacks RM, Greene J, Hibbard J, Overton V, Parrotta CD. Does patient activation predict the course of type 2 diabetes? A longitudinal study. Patient Educ Couns. 2017;100(7):1268–1275. doi:10.1016/j.pec.2017.01.014
11. Bu F, Fancourt D. How is patient activation related to healthcare service utilisation? Evidence from electronic patient records in England. BMC Health Serv Res. 2021;21(1). doi:10.1186/s12913-021-07115-7
12. Innab A, Kerari A. Impact of behavioral interventions on patient activation in adults with hypertension: a systematic review and meta-analysis. Inquiry. 2022;59:469580221090408. doi:10.1177/00469580221090408
13. Schwarzer R, Bäßler J, Kwiatek P, Schröder K, Zhang JX. The assessment of optimistic self-beliefs: comparison of the German, Spanish, and Chinese versions of the general self-efficacy scale. Appl Psychol Int Rev. 1997;46(1):69–88.
14. Jordan JE, Buchbinder R, Briggs AM, et al. The health literacy management scale (HeLMS): a measure of an individual’s capacity to seek, understand and use health information within the healthcare setting. Patient Educ Couns. 2013;91(2):228–235. doi:10.1016/j.pec.2013.01.013
15. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037//0033-295X.84.2.191
16. Zhang A, Wang J, Wan X, et al. The mediating effect of self-efficacy on the relationship between diabetes self-management ability and patient activation in older adults with type 2 diabetes. Geriatr Nurs. 2023;51:136–142. doi:10.1016/j.gerinurse.2023.02.017
17. Liu CF, Kuo KM. Does information overload prevent chronic patients from reading self-management educational materials? Int J Med Inform. 2016;89:1–8. doi:10.1016/j.ijmedinf.2016.01.012
18. Blakemore A, Hann M, Howells K, et al. Patient activation in older people with long-term conditions and multimorbidity: correlates and change in a cohort study in the United Kingdom. BMC Health Serv Res. 2016;16(1):582. doi:10.1186/s12913-016-1843-2
19. Hibbard JH, Mahoney E. Toward a theory of patient and consumer activation. Patient Educ Couns. 2010;78(3):377–381. doi:10.1016/j.pec.2009.12.015
20. Wang J, Wang X. Structural Equation Modeling: Applications Using Mplus.
21. Kazak AE. Families of chronically ill children: a systems and social-ecological model of adaptation and challenge. J Consult Clin Psychol. 1989;57(1):25–30. doi:10.1037//0022-006x.57.1.25
22. Unger T, Borghi C, Charchar FJ, et al. International society of hypertension global hypertension practice guidelines. Hypertension. 2023;80(6):e1–e132. doi:10.1161/HYPERTENSIONAHA.123.21108
23. Hsieh FY, Bloch DA, Larsen MD. A simple method of sample size calculation for linear and logistic regression. Stat Med. 1998;17(14):1623–1634. doi:10.1002/(SICI)1097-0258(19980730)17:14<1623::AID-SIM871>3.0.CO;2-S
24. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the patient activation measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4):1005–1026. doi:10.1111/j.1475-6773.2004.00269.x
25. Schwarzer R, Jerusalem M. Generalized Self-Efficacy Scale. In: Weinman J, Wright S, Johnston M, editors. Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs. Windsor, UK: NFER-NELSON; 1995:35–37.
26. Jordan JE, Buchbinder R, Osborne RH. Conceptualising health literacy from the patient perspective. Patient Educ Couns. 2010;79(1):36–42. doi:10.1016/j.pec.2009.10.001
27. Tang H, Du W, Jiang Y, et al. Development and psychometric testing of the therapeutic adherence scale for hypertensive patients. Eur J Cardiovasc Nurs. 2015;15(2):150–156. doi:10.1177/1474515114563414
28. He J, Fan X. Latent Profile Analysis. In: Zeigler-Hill V, Shackelford TK editors. Encyclopedia of Personality and Individual Differences. Springer; 2018:1–4. doi:10.1007/978-3-319-28099-8_2316-1
29. Wang MC, Deng Q, Bi X, Ye H, Yang W. Performance of the entropy as an index of classification accuracy in latent profile analysis: a monte carlo simulation study. Acta Psychol Sin. 2017;49(11):1473–1482. doi:10.3724/SP.J.1041.2017.01473
30. Demiray O, Gunes ED, Kulak E, et al. Classification of patients with chronic disease by activation level using machine learning methods. Health Care Manag Sci. 2023;26(4):626–650. doi:10.1007/s10729-023-09653-4
31. Xiao B, Chen J. Analysis of patient activation levels and influencing factors among community hypertension patients [in Chinese]. J Clin Nurs. 2021;20(5):13–16. doi:10.3969/j.issn.1671-8933.2021.05.004
32. Chaturvedi A, Zhu A, Gadela NV, Prabhakaran D, Jafar TH. Social determinants of health and disparities in hypertension and cardiovascular diseases. Hypertension. 2024;81(3):387–399. doi:10.1161/HYPERTENSIONAHA.123.21354
33. Lee AYL, Wong AKC, Hung TTM, Yan J, Yang S. Nurse-led telehealth intervention for rehabilitation (telerehabilitation) among community-dwelling patients with chronic diseases: systematic review and meta-analysis. J Med Internet Res. 2022;24(11):e40364. doi:10.2196/40364
34. Carey RM, Muntner P, Bosworth HB, Whelton PK. Prevention and control of hypertension: JACC Health Promotion Series. J Am Coll Cardiol. 2018;72(23): 1278–1293. doi:10.1016/j.jacc.2018.10.022
35. O’Regan SA, Ekelund K, Watterson LM. Emotional activation in simulation: measuring the influence of participant roles and scenario design. Simul Healthc. 2022;17(6):394–402. doi:10.1097/SIH.0000000000000615
36. Hussain A, Umair M, Khan S, et al. Exploring sustainable healthcare: innovations in health economics, social policy, and management. Heliyon. 2024;10(13):e33186. doi:10.1016/j.heliyon.2024.e33186
37. Chen W, Bai X, Liu D, et al. Public satisfaction with healthy china action plan implementation: a web-based cross-sectional survey in southwest China. BMJ Open. 2025;15(2):e091039. doi:10.1136/bmjopen-2024-091039
38. Bos-Touwen I, Schuurmans M, Monninkhof E, et al. Patient and disease characteristics associated with activation for self-management in patients with diabetes, chronic obstructive pulmonary disease, chronic heart failure and chronic renal disease: a cross-sectional survey study. PLoS One. 2015;10(5):e0126400. doi:10.1371/journal.pone.0126400
39. Korpershoek Y, Vervoort S, Nijssen L, et al. Factors influencing exacerbation-related self-management in patients with COPD: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2016;11:2977–2990. doi:10.2147/copd.s116196
40. Liu F, Song T, Yu P, et al. Efficacy of an mHealth app to support patients’ self-management of hypertension: randomized controlled trial. J Med Internet Res. 2023;25:e43809. doi:10.2196/43809
41. Lightfoot CJ, Wilkinson TJ, Sohansoha GK, et al. The effects of a digital health intervention on patient activation in chronic kidney disease. NPJ Digit Med. 2024;7(1):318. doi:10.1038/s41746-024-01296-1
42. Bonetti L, Tolotti A, Anderson G, et al. Nursing interventions to promote patient engagement in cancer care: a systematic review. Int J Nurs Stud. 2022;133:104289. doi:10.1016/j.ijnurstu.2022.104289
43. Mirmazhari R, Ghafourifard M, Sheikhalipour Z. Relationship between patient activation and self-efficacy among patients undergoing hemodialysis: a cross-sectional study. Renal Replac Ther. 2022;8(1):40. doi:10.1186/s41100-022-00431-6
44. Young L, Kupzyk K, Barnason S. The impact of self-management knowledge and support on the relationships among self-efficacy, patient activation, and self-management in rural patients with heart failure. J Cardiovasc Nurs. 2017;32(4):e1–e8. doi:10.1097/jcn.0000000000000390
45. Hübner J, Welter S, Ciarlo G, et al. Patient activation, self-efficacy and usage of complementary and alternative medicine in cancer patients. Med Oncol. 2022;39(12):192. doi:10.1007/s12032-022-01796-8
46. Denecke K, Schmid N, Nüssli S. Implementation of cognitive behavioral therapy in e-mental health apps: literature review. J Med Internet Res. 2022;24(3):e27791. doi:10.2196/2779
47. Rademakers J, Nijman J, van der Hoek L, Heijmans M, Rijken M. Measuring patient activation in The Netherlands: translation and validation of the American short form Patient Activation Measure (PAM13). BMC Public Health. 2012;12(1):577. doi:10.1186/1471-2458-12-577
48. Smith SG, Curtis LM, Wardle J, von Wagner C, Wolf MS. Skill set or mind set? Associations between health literacy, patient activation and health. PLoS One. 2013;8(9):e74373. doi:10.1371/journal.pone.0074373
49. Nutbeam D, Lloyd JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. 2021;42(1):159–173. doi:10.1146/annurev-publhealth-090419-102529
50. Hersh L, Salzman B, Snyderman D. Health literacy in primary care practice. Am Fam Physician. 2015;92(2):118–124.
51. Hasannejadasl H, Roumen C, Smit Y, Dekker A, Fijten R. Health literacy and eHealth: challenges and strategies. JCO Clin Cancer Inform. 2022;
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pathways of Media Contact to Health Literacy in Middle-Aged and Older People: The Chain Mediation Effect of Perceived Social Support and Self-Efficacy
Jiang MM, Xiao YW, Liao ZL
Journal of Multidisciplinary Healthcare 2024, 17:111-121
Published Date: 6 January 2024
The Serial Mediation Effects of Social Support and Self-Efficacy on Health Literacy and Self-Management Behaviors Among Young and Middle-Aged Cardiac Patients After Percutaneous Coronary Intervention: A Cross-Sectional Study in China
Liu W, Qian S, Hu Y, Zhang R
Risk Management and Healthcare Policy 2024, 17:2893-2906
Published Date: 22 November 2024
Mediating Effects of Health Literacy, Self-Efficacy, and Social Support on the Relationship Between Disease Knowledge and Patient Participation Behavior Among Chronic Ill Patients: A Cross-Sectional Study Based on the Capability-Opportunity-Motivation and Behavior (COM-B) Model
Wu M, Wang W, He H, Bao L, Lv P
Patient Preference and Adherence 2025, 19:1337-1350
Published Date: 8 May 2025