")
Back to Journals » Open Access Emergency Medicine » Volume 15
Lasting Effects of COVID-19 Pandemic on Prehospital Emergency Medical Service Missions
Authors Metelmann I , Nagel M, Schneider B, Krämer B, Kraemer S
Received 9 June 2023
Accepted for publication 30 August 2023
Published 18 September 2023 Volume 2023:15 Pages 325—332
DOI https://doi.org/10.2147/OAEM.S425272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Isabella Metelmann,1 Matthes Nagel,2 Bastian Schneider,2 Bernd Krämer,3 Sebastian Kraemer1
1Department of Visceral, Transplant, Thoracic and Vascular Surgery, University Hospital of Leipzig, Leipzig, Saxony, 04103, Germany; 2Simba n3 GmbH, Oelsnitz, Saxony, 08606, Germany; 3Rettungszweckverband Südwestsachsen, Plauen, Saxony, 08529, Germany
Correspondence: Isabella Metelmann, Department of Visceral, Transplant, Thoracic and Vascular Surgery, University Hospital of Leipzig, Liebigstrasse 20, Leipzig, Saxony, 04103, Germany, Tel + 49 341 97 17200, Email [email protected]
Purpose: The COVID-19 pandemic confronted prehospital emergency medical services (PHEMS) with immense challenges. This study aimed to investigate the development of PHEMS mission numbers and times in the COVID-affected region of Southwest Saxony (SWS).
Patients and Methods: This was a retrospective analysis of PHEMS in SWS during lockdown periods and equal time spans in the previous and following years. Differences were tested for statistical significance using the chi-squared test and one-way analysis of variance (ANOVA).
Results: The total number of missions showed a substantial drop during the first (− 16.6%) and the second (− 4.5%) lockdown period compared with the previous year. Next-year periods showed a recovery that was nearly equivalent to the starting point. The first lockdown period was not associated with longer overall mission times. The minutes spent at the scene differed significantly between the first lockdown period (31.1 ± 3.52 min), previous year (28.4 ± 4.84 min), and follow-up period (31.8 ± 0.98 min). During the second lockdown, the overall mission times (71.6 ± 2.91 min), response times in minutes (8.9 ± 0.49 min), and minutes spent at the scene (31.4 ± 2.99 min) were significantly longer. The minutes spent at the scene (32.3 ± 18.68 min) and the overall mission time (69.6 ± 1.92 min) remained significantly longer during the control period.
Conclusion: Our data confirm the impact of the SARS-CoV-2 pandemic on German PHEMS. It can be concluded that nationwide lockdown measures led to lasting effects regarding a reduction in the total mission number, transport-on-site released-ratio, and emergency time intervals in the following year, without lockdown restrictions. The lasting effects on the transport-on-site released-ratio and emergency time intervals call for a re-evaluation of the delivery of emergency services during pandemics. These findings can inform future policy decisions and resource allocations to ensure optimal emergency medical services.
Keywords: SARS-CoV-2, emergency mission times, emergency medicine, prehospital emergency medical services, COVID
Introduction
The eruption of the COVID-19 pandemic put every part of the health system in place to test and forced adjustments to processes and operating procedures. Several studies from earlier pandemics such as Ebola in 2014 have shown that nationwide-imposed security measures increase public perception of public health emergencies and influenced people’s health behavior leading to a reduced use of health services due to fear from infection or overloaded health systems.1–4 During the pandemic spread of COVID-19, the utilization of prehospital emergency health services (PHEMS) decreased substantially during the lockdown periods all over the world.5–10 PHEMS are essential to the functionality of health systems. The challenging conditions of the COVID-19 pandemic, including special requirements for personal protective equipment (PPE) and patient transport, have put PHEMS under immense pressure to adapt. This study aimed to investigate the development of mission numbers and mission times of PHEMS during lockdown periods in the COVID-affected region of Southwest Saxony (SWS) by applying the study protocol introduced by Eskol et al.7
Study Setting
The SWS region is a rural area of eastern Germany. Figure 1 shows a map of the study region. The PHEMS covers an area of 2400 km2 with 660,000 inhabitants. The population density is 275 inhabitants per square kilometer, which is slightly above the German average (233/km²). Ambulances with state-approved paramedics were stationed at 28 rescue stations, of which 14 were staffed with specialized emergency medical doctors. They interact in a rendezvous system, where an emergency physician is not necessarily alarmed for any emergency, but for certain indications. In-patient care was provided by 13 hospitals, including one supranational trauma care center. SWS was strongly affected in the second pandemic wave from November 2020 to February 2021 but not in the first pandemic wave as depicted in Figure 2. Nationwide lockdown measures and restrictions were implemented in calendar weeks (CW) 13–18 of 2020 (lockdown 1) and CW 45/2020–06/2021 (lockdown 2).
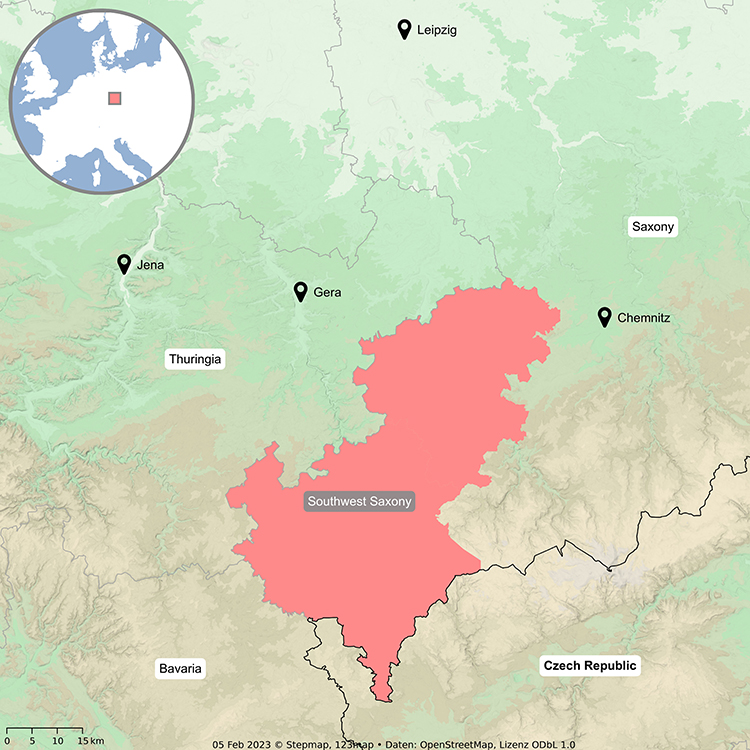 |
Figure 1 Map of the study region. |
 |
Figure 2 Investigation periods concerning incidence rates of SARS-CoV-2 in SWS and Saxony. Notes: Light grey: Lockdown 1 and post-period 1, Light blue: Lockdown 2 and post-period 2; blue line: 7-day incidence of SARS-CoV2 per 100,000 inhabitants in Southwest-Saxony; orange line: 7-day incidence of SARS-CoV2 per 100,000 inhabitants in Saxony. |
The PHEMS in Germany is federally organized and publicly funded. The German PHEMS is a paramedic and emergency medicine doctor-based system dispatched by centralized rescue centers specified for fire and emergency departments. An indication decision refers to several defined criteria queried by approved dispatchers. Mission details were digitally recorded and entered into an electronic patient medical record system providing information on patient details, mission indication, and mission time intervals, including response minutes, time spent at the scene, and transport time.
Materials and Methods
This study was designed as a retrospective analysis of data concerning PHEMS in SWS during lockdown periods and equal time spans in previous and following years.
Data were retrieved from an electronic patient medical record system (Rescue Track, RND 1110, 1010; Rescue Track GmbH, Reutlingen). Mission times were recorded and differentiated into response times and the time spent at the scene, as described by Eskol et al.7
All statistical analyses were performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA). Differences between the study periods were tested for statistical significance using the chi-square test. Mission times were tested for statistically significant differences using one-way analysis of variance (ANOVA). Effect size was measured using Cohen’s f.11 Scheffe’s test was used to determine significant differences between the groups. Differences were considered statistically significant at p <0.05. This study was conducted in compliance with the International Conference on Harmonization Guidelines for Good Clinical Practice and principles of the Declaration of Helsinki. The need for ethical approval for this retrospective evaluation of archived, anonymized, and aggregated patient data was waived by the Scientific Ethical Committee of the Medical Faculty of Leipzig University.
Results
Mission Numbers
The total number of missions showed a substantial drop of 16.6% (‒1110 in total) during the first and 4.5% (‒742 in total) during the second lockdown period compared to the previous year. Next-year periods showed a recovery in mission numbers, with nearly equivalent numbers to the starting point.
Number of Patients Released at Scene
During the lockdown periods, the number of patients released at the scene was significantly higher than that in previous years (p<0.01). The number of patients released at the scene in the following year was significantly higher than before the COVID-19 pandemic (p<0.01), although it decreased significantly in comparison with the lockdown periods (p<0.01). In a complementary way, the number of patients who were transported to the emergency departments showed a statistically significant decrease during the lockdown periods (p<0.01) and remained significantly lower during the following year compared to pre-COVID times (p<0.01). Effect size of all comparisons was low (w<0.04). Table 1 details the development of mission numbers during the first and second lockdowns and the control periods, respectively.
 |
Table 1 Development of Mission Numbers, Numbers of Patients Released at Scene or Transported to Hospital |
Mission Times
The first lockdown period was not associated with longer overall mission times. However, the minutes spent at the scene were significantly longer. This effect continued in 2021. The Scheffe test showed a statistically significant difference between the minutes spent at the scene between the first lockdown period (31.1 ± 3.52 min) and the previous year (28.4 ± 4.84 min) and a significant prolongation in the follow-up period in 2021 (31.8 ± 0.98 min) in comparison to 2019 with a large effect size (f=0.88). During the second lockdown, there was a substantial increase in the duration of the overall mission time, response time (in minutes), and time spent at the scene. The response time in minutes was significantly longer during the second lockdown in 2020 (8.9 ± 0.49 min) than in the previous (7.9 ± 0.23 min) and the following year (8.1 ± 1.17 min). The length of response time recovered in 2021 showed no significant difference compared with the pre-COVID period. Minutes spent at the scene remained significantly longer during the control period (32.3 ± 18.68 min) than during the pre-COVID period (25 ± 25.66 min). This affected the overall mission time, remaining significantly longer in the control period (69.6 ± 1.92 min) than in the pre-COVID period (68.2 ± 3.25 min). Table 2 summarizes the development of mission times, minutes spent at the scene, and response times during the two lockdown phases and their comparison periods during the previous and following years.
 |
Table 2 Development of Mission Times During the Investigation Periods in Minutes |
Discussion
Mission Number Drop
Our findings complement those of Eskol et al, who showed a substantial decrease in PHEMS missions during lockdown periods.7 Similar studies from Italy, Iran, Finland and the USA on the influence of the SARS-CoV-2 pandemic on emergency medical services confirmed our described decline in total mission numbers, with rates from 5.7% to 23%.5,6,8,9 In accordance with our results, another German study that investigated the area of Bavaria found the most substantial decrease of mission numbers during the first lockdown period.10
The reasons for the drop in mission numbers are multifaceted: reaching from a change in lifestyle habits that led to a lowered risk of accidents, to the avoidance of reaching for health services because of the fear of facing an infectious disease or getting infected in the emergency department or hospitals, and to worry and ambitions not to overload the health system. A study group from the USA examined the injury severity score (ISS) of prehospital trauma patients before and during COVID-19 and found out, that patients had a significantly higher ISS during COVID-19 indicating that patients with less severe injury used private transport instead of PHEMS.9 However, several conditions, such as cerebral stroke or myocardial infarction, require emergency medical services and are independent of lockdown restrictions. A decrease in the number of patients presenting with transient ischemic attack or cerebral stroke was reported early during the pandemic.12 Reasons for this are commonly seen in the public and media transport advice to stay at home and limit the utilization of health services.13 Additionally, neurological symptoms, such as dysarthria or neglect, are often recognized only by relatives or friends, and contact bans may have led to missed recognition of symptoms.12 Our data do not allow for the differentiation of the reasons for emergency missions. However, the severe drop suggests that an unknown number of actual necessary missions were not triggered. This highlights the need to strengthen educational programs to help people identify necessary emergency calls. Efforts made to educate the public on emergency symptoms of cerebral strokes and myocardial infarction have increased awareness of seeking PHEMS at the earliest possible point.14–16
Rise of Patient Numbers Released at Scene
Our data show a lasting rise in the number of patients released at the scene over a period of 1 year following the lockdown measures. Herein, reasons might be seen in the ongoing educational effect of lockdown restrictions and the previously described causes. Releasements at the emergency scene may have been accepted more generously to prevent the collapse of hospital emergency capacity. Hence, the SARS-CoV-2 pandemic may have served as an unexpected opportunity for prehospital medical service providers to re-evaluate the indication catalog for a reasonable release at the emergency scene. For example, patients with elevated blood pressure without cardiological or neurological symptoms are not transported to the emergency department without an elevated risk of end-organ failure.17
Treatment at the scene and release without transport in the hospital increase the risk of second missions for the same reasons or overseen critical cases. Breeman et al described a request for secondary attention for the same complaints in 24.7% of patients released at the scene in a paramedic-based system.18 However, the proportion of secondary missions seemed to depend on the constitution of the PHEMS team. Højfeldt et al reported successful release at a scene without the need for a second healthcare contact in 93% of a merely anesthesiologist-based PHEMS team.19 In Germany, release at the scene must be approved by an emergency doctor. This may lower the risk of secondary missions while obviating overload in emergency departments. Although these results are promising, further investigation is needed concerning concrete criteria that are suitable for not being transported to the hospital.19,20
Mission Times
The number of PHEMS missions significantly increased during the COVID-19 pandemic.6 The total mission time increased significantly during the second lockdown and its aftermath. Similarly, an Italian group described a prolongation of mission times during phases of high incidences of COVID-19 in the study area.8 In Iran, response time, on-scene time and transfer time were significantly longer during COVID-19 pandemic.21 In contrast to that, a study from the USA described no statistically significant different prehospital times of trauma patients during the early phase of COVID-19.9 Reason for that may be found in the Anglo-American PHEMS model of “scoop and run”: the teams consist of paramedics and Emergency Medical Technicians and every patient needs to be transported to the Emergency Department unless the patient refuses to. Hence, prehospital times are minimized and the effect of on-scene time on overall mission times is relatively small.
While the prolongation seems to be negligible in absolute numbers (3 min, less than 5%), it may influence patient care and prognosis. When disaggregated into mission phases, the time spent at the scene increased the most. The time spent at the scene was the only phase that was significantly longer during the first lockdown period. The main reason for this prolongation may be the increased proportion of people treated solely at emergency sites. However, there was a short and significant prolongation of the response time during the second lockdown. This may be due to the comparatively lower drop in mission numbers in the second lockdown and consecutive overload of PHEMS, while preparation for missions may have been more complex than during pre-COVID times. The use of PPE under SARS-CoV-2 pandemic circumstances had an impact on the daily work routine of every healthcare provider, as well as on prehospital staff, with a substantial influence on mission times.21 While it is considered that the prehospital mission time is strongly associated with patients outcome and mortality in various diseases,22–28 reliable data on whether and how this affects the number of avoidable deaths, disability-adjusted life years or health care spending is still missing revealing potential for future research.
Limitations
There are some limitations in the interpretation of the presented data. First, our data do not represent the German PHEMS as a whole but reflect only SWS. Second, the German PHEMS was a physician-based system. Hence, the results on patient numbers released at the scene cannot be transferred to other countries with paramedic-only systems. Third, we did not have information on the number of second missions after the release at the scene. Finally, our data did not allow us to derive information on the indications for PHEMS missions. Thus, we cannot fully interpret whether the decrease in mission numbers includes a decrease in missions that would have been necessary.
Conclusion
Our data confirmed the impact of the SARS-CoV-2 pandemic on the German PHEMS. Furthermore, it can be concluded that the nationwide lockdown measures led to lasting effects regarding a reduction in the total mission number, transport-on-site released-ratio, and emergency time intervals in the following year without lockdown restrictions. Supposed population educational effects on the use of PHEMS and/or the development of PHEMS orders on how and when patients are to be released at the scene should be studied further. Our results invite future research projects to study the impact of the prolongation of mission times and increase of on-scene treatments on patients’ outcome as well as disease-specific differences. Additionally, the changes of PHEMS in SWS emphasize how the COVID-19 specific political security measures influenced people’s health behavior and usage of health services.
Funding
Funded by the Open Access Publishing Fund of Leipzig University supported by the German Research Foundation within the program Open Access Publication Funding.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Elston JWT, Moosa AJ, Moses F, et al. Impact of the Ebola outbreak on health systems and population health in Sierra Leone. J Public Health. 2016;38(4):673–678. doi:10.1093/pubmed/fdv158
2. Bali S, Stewart KA, Pate MA. Long shadow of fear in an epidemic: fearonomic effects of Ebola on the private sector in Nigeria. BMJ Glob Health. 2016;1(3):e000111. doi:10.1136/bmjgh-2016-000111
3. Bannister-Tyrrell M, Gryseels C, Delamou A, D’Alessandro U, van Griensven J, Grietens KP. Blood as medicine: social meanings of blood and the success of Ebola trials. Lancet. 2015;385(9966):420. doi:10.1016/S0140-6736(14)62392-8
4. Thiam S, Delamou A, Camara S, et al. Challenges in controlling the Ebola outbreak in two prefectures in Guinea: why did communities continue to resist? Pan Afr Med J. 2015;22(Suppl 1):22. doi:10.11694/pamj.supp.2015.22.1.6626
5. Hasani-Sharamin P, Saberian P, Sadeghi M, Mireskandari SM, Baratloo A. Characteristics of emergency medical service missions in out-of-hospital cardiac arrest and death cases in the periods of before and after the COVID-19 pandemic. Prehosp Disaster Med. 2021;36(6):676–683. doi:10.1017/S1049023X21001138
6. Laukkanen L, Lahtinen S, Liisanantti J, Kaakinen T, Ehrola A, Raatiniemi L. Early impact of the COVID-19 pandemic and social restrictions on ambulance missions. Eur J Public Health. 2021;31(5):1090–1095. doi:10.1093/eurpub/ckab065
7. Eskol JR, Zegers FD, Wittrock D, Lassen AT, Mikkelsen S. Increased ambulance on-scene times but unaffected response times during the first wave of the COVID-19 pandemic in Southern Denmark. BMC Emerg Med. 2022;22(1):61. doi:10.1186/s12873-022-00623-7
8. Stirparo G, Ristagno G, Bellini L, et al. Changes to the major trauma pre-hospital emergency medical system network before and during the 2019 COVID-19 pandemic. J Clin Med. 2022;11(22). doi:10.3390/jcm11226748
9. Jarvis S, Salottolo K, Berg GM, et al. Examining emergency medical services’ prehospital transport times for trauma patients during COVID-19. Am J Emerg Med. 2021;44:33–37. doi:10.1016/j.ajem.2021.01.091
10. Hegenberg K, Althammer A, Gehring C, Prueckner S, Trentzsch H. Pre-hospital emergency medical services utilization amid COVID-19 in 2020: descriptive study based on routinely collected dispatch data in Bavaria, Germany. Healthcare. 2023;11(14). doi:10.3390/healthcare11141983
11. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
12. Bersano A, Kraemer M, Touzé E, et al. Stroke care during the COVID-19 pandemic: experience from three large European countries. Eur J Neurol. 2020;27(9):1794–1800. doi:10.1111/ene.14375
13. Baracchini C, Pieroni A, Viaro F, et al. Acute stroke management pathway during Coronavirus-19 pandemic. Neurol Sci. 2020;41(5):1003–1005. doi:10.1007/s10072-020-04375-9
14. Coventry LL, van Schalkwyk JW, Thompson PL, Hawkins SA, Hegney DG. Myocardial infarction, patient decision delay and help-seeking behaviour: a thematic analysis. J Clin Nurs. 2017;26(13–14):1993–2005. doi:10.1111/jocn.13607
15. Tan J, Ramazanu S, Liaw SY, Chua WL. Effectiveness of public education campaigns for stroke symptom recognition and response in non-elderly adults: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. 2022;31(2):106207. doi:10.1016/j.jstrokecerebrovasdis.2021.106207
16. Ueda Y, Tahara Y, Itoh T, et al. New strategy to prevent acute myocardial infarction by public education - A position statement of the committee on public education about emergency medical care of the Japanese circulation society. Circ J. 2021;85(3):319–322. doi:10.1253/circj.CJ-20-1308
17. McAlister FA, Youngson E, Rowe BH. Elevated blood pressures are common in the emergency department but are they important? A retrospective cohort study of 30,278 adults. Ann Emerg Med. 2021;77(4):425–432. doi:10.1016/j.annemergmed.2020.11.005
18. Breeman W, Poublon NA, Verhofstad MHJ, van Lieshout EMM. Safety of on-scene medical care by EMS nurses in non-transported patients: a prospective, observational study. Scand J Trauma Resusc Emerg Med. 2018;26(1):79. doi:10.1186/s13049-018-0540-z
19. Højfeldt SG, Sørensen LP, Mikkelsen S. Emergency patients receiving anaesthesiologist-based pre-hospital treatment and subsequently released at the scene. Acta Anaesthesiol Scand. 2014;58(8):1025–1031. doi:10.1111/aas.12347
20. Tohira H, Fatovich D, Williams TA, et al. Is it appropriate for patients to be discharged at the scene by paramedics? Prehosp Emerg Care. 2016;20(4):539–549. doi:10.3109/10903127.2015.1128028
21. Sabbaghi M, Namazinia M, Miri K. Time indices of pre-hospital EMS missions before and during the COVID-19 pandemic: a cross-sectional study in Iran. BMC Emerg Med. 2023;23(1):9. doi:10.1186/s12873-023-00780-3
22. Elkbuli A, Dowd B, Sanchez C, Shaikh S, Sutherland M, McKenney M. Emergency medical service transport time and trauma outcomes at an urban level 1 trauma center: evaluation of prehospital emergency medical service response. Am Surg. 2022;88(6):1090–1096. doi:10.1177/0003134820988827
23. Harmsen AMK, Giannakopoulos GF, Moerbeek PR, Jansma EP, Bonjer HJ, Bloemers FW. The influence of prehospital time on trauma patients outcome: a systematic review. Injury. 2015;46(4):602–609. doi:10.1016/j.injury.2015.01.008
24. Dharap SB, Kamath S, Kumar V. Does prehospital time affect survival of major trauma patients where there is no prehospital care? J Postgrad Med. 2017;63(3):169–175. doi:10.4103/0022-3859.201417
25. Fiehler J, Cognard C, Gallitelli M, et al. European recommendations on organisation of interventional care in acute stroke (EROICAS). Int J Stroke. 2016;11(6):701–716. doi:10.1177/1747493016647735
26. Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
27. Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med. 2006;355(22):2308–2320. doi:10.1056/NEJMsa063117
28. Welsh RC, Armstrong PW. It’s a matter of time: contemporary pre-hospital management of acute ST elevation myocardial infarction. Heart. 2005;91(12):1524–1526. doi:10.1136/hrt.2004.055616
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.