Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Laryngeal Responses During Non-Invasive Ventilation in Stable Chronic Obstructive Pulmonary Disease: An Observational Study
Authors Brekka AK ![]() , Solli PV, Indrekvam S, Engeset MS, Røksund OD, Lehmann S
, Solli PV, Indrekvam S, Engeset MS, Røksund OD, Lehmann S ![]() , Clemm HH, Halvorsen T
, Clemm HH, Halvorsen T ![]() , Heimdal JH, Murphy PB, Vollsæter M, Andersen TM
, Heimdal JH, Murphy PB, Vollsæter M, Andersen TM
Received 26 January 2026
Accepted for publication 13 May 2026
Published 28 May 2026 Volume 2026:21 596874
DOI https://doi.org/10.2147/COPD.S596874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Anne Kristine Brekka,1,2 Petrine Veierød Solli,2,3 Solfrid Indrekvam,1 Merete Salveson Engeset,2 Ola Drange Røksund,2,3 Sverre Lehmann,1,4 Hege Havstad Clemm,3,5 Thomas Halvorsen,3,4 John-Helge Heimdal,6,7 Patrick Brian Murphy,8,9 Maria Vollsæter,3,4 Tiina Maarit Andersen1,2
1Thoracic Department, Haukeland University Hospital, Bergen, Norway; 2The Faculty of Health and Social Sciences, Western Norway University of Applied Sciences, Bergen, Norway; 3Department of Pediatrics, Haukeland University Hospital, Bergen, Norway; 4Department of Clinical Medicine, University of Bergen, Bergen, Norway; 5Department of Sports Medicine, Norwegian School of Sport Science, Oslo, Norway; 6Department of Surgical Science, University of Bergen, Bergen, Norway; 7Department of Otolaryngology, Haukeland University Hospital, Bergen, Norway; 8Lane Fox Clinical Respiratory Physiological Center, Guy’s and St Thomas’ NHS Foundation Trust, London, UK; 9Center for Human and Applied Physiological Sciences (CHAPS), King’s College London, London, UK
Correspondence: Anne Kristine Brekka, Thoracic Department, Haukeland University Hospital, Helse-Bergen HF, Postboks 1400, Bergen, 5021, Norway, Tel +4790651406, Email [email protected]
Purpose: Long-term non-invasive ventilation (NIV) is an established therapy for hypercapnic chronic obstructive pulmonary disease (COPD); however, many patients remain challenging to ventilate effectively. We hypothesized that NIV-induced laryngeal obstruction (NIV-ILO), observed during laryngoscopy, may contribute to reduced ventilatory effectiveness, and that this obstruction can be identified using laryngeal ultrasound (US).
Patients and Methods: This exploratory cross-sectional study included 15 participants with stable COPD receiving long-term NIV. Laryngeal responses were assessed using transnasal flexible laryngoscopy (TFL) and US. Assessments began during spontaneous breathing, followed by NIV at each participant’s prescribed settings. Inspiratory positive airway pressure (IPAP) was increased in 2 cmH2O increments to the device’s maximum. Laryngeal responses were assessed in real time and reassessed retrospectively from video recordings. The participants rated discomfort using a numeric rating scale (0– 10).
Results: Fifteen participants (40% female) were included. The prescribed IPAP ranged from 7 to 30 cmH2O, with NIV-ILO observed in 5 of 15 participants at a median of 22.0 cmH2O. During subsequent pressure increments, additional 6 of 15 developed NIV-ILO at a median (range) IPAP of 20.5 cmH2O (16.0– 30.0), yielding 11 participants (73.3%) developing NIV-ILO within the pressure range of their device. US was assessable in 11 participants, with the structures of interest visualized during 54 of 63 pressure increments. The two methods demonstrated complete concordance for all assessable findings.
Conclusion: NIV-ILO was common in patients with COPD using long-term NIV, occurring within the pressure range typically applied to achieve effective ventilation. US can serve as a less invasive diagnostic alternative to TFL.
Keywords: COPD, NIV, ILO, TFL, NIV-ILO, laryngeal US
Introduction
Non-invasive ventilation (NIV) constitutes the mainstay of respiratory support in both the acute and long-term management of severe chronic obstructive pulmonary disease (COPD). Effective ventilation during NIV requires maintaining an open and functionally intact upper airway, and high inspiratory pressures are often recommended to achieve optimal outcomes.1,2 However, adherence to long-term NIV in patients with COPD often remains suboptimal.3,4 Several factors have been proposed to explain this, including patient discomfort, intolerance and patient-ventilator asynchrony.
A potential but underexplored contributor to poor adherence and reduced effectiveness of NIV is laryngeal obstruction induced by the applied positive airway pressures, as shown both in healthy individuals and amyotrophic lateral sclerosis patients.5–7 According to consensus terminology,8,9 this phenomenon should be referred to as NIV-induced laryngeal obstruction (NIV-ILO), reflecting NIV as the inducer of laryngeal obstruction. NIV-ILO may reflect laryngeal structural or reflex responses to airflow under positive pressure, whereby mechanical stimulation of the laryngeal mucosa can provoke inspiratory narrowing.10 Consistent with this, studies in healthy individuals have shown that nasal positive-pressure ventilation can induce inspiratory glottic narrowing, increasing upper airway resistance and reducing effective tidal volume delivery, particularly during sleep.11,12 Although laryngeal closure reflexes are well documented, the underlying mechanisms are incompletely understood, and likely vary between individuals.11–16 Given the larynx’s role as a dynamic gatekeeper of airflow, understanding its behaviour during NIV is a key area of respiratory medicine.5,6,17–21
Data on laryngeal patency during NIV in awake patients with COPD are limited, fragmented, and partly conflicting, making it difficult to form a coherent understanding of how the larynx responds to positive airway pressures applied by respiratory support devices.22–26 The effect of NIV pressure titration on laryngeal behaviour in stable COPD therefore remains unresolved.
We have previously shown that transnasal flexible laryngoscopy (TFL) provides detailed information on laryngeal behaviour across different pressure conditions, treatment modalities, and clinical settings.5,6,17 However, the invasive nature of TFL limits its routine clinical use. Laryngeal ultrasound (US) has recently been proposed as a non-invasive method for assessing laryngeal anatomy and may represent a more feasible approach for evaluating airway behaviour during NIV.7,27–29
We hypothesised that unrecognised adverse laryngeal responses to positive-pressure support may contribute to poor adherence to long-term NIV in COPD. Thus, the primary aim of this study was to characterise laryngeal responses during stepwise NIV pressure titration in awake individuals with stable COPD and to explore the occurrence of NIV-ILO at usual home NIV settings. A secondary aim was to assess the feasibility of laryngeal US by comparing its findings with parallel TFL assessments.
Materials and Methods
This explorative cross-sectional observational study included participants with COPD recruited from the respiratory failure outpatient clinic at Haukeland University Hospital, Bergen, Norway. Eligible patients were listed in the Norwegian Registry for Long-Term Mechanical Ventilation and had appointments between April 1, 2023, to December 31, 2024. Inclusion criteria were COPD with pCO2 ≥ 6.0 kPa as the primary indication for NIV initiation and clinically stable disease, defined as no hospital admission within the precenting 4–6 weeks. Exclusion criteria were age <18 years, a history of laryngospasm, pneumothorax or pronounced nasal obstruction. The study was conducted in accordance with the amended Declaration of Helsinki30 and approved by the Regional Committee for Medical and Health Research Ethics in Western Norway (ID: 2022–536,829). All participants were initially approached for inclusion by their attending physician, subsequently, contacted by phone, and then scheduled for the examination. Written informed consent was obtained from all participants prior to their inclusion.
Baseline Measurements
Spirometry was performed using Vyntus spirometer (CareFusion, Vyntys, Hoechberg, Bavaria, Germany) and raw data transformed to percentages of predicted following the European Respiratory Society guidelines.31
Examination Set-Up
The previously described experimental setup27 with parallel data sources was used to record synchronized data, allowing retrospective evaluation and verification of the NIV cycle phase. The participants were assessed while awake, in a supine position in a reclining chair, using their home-based NIV device with usual settings (Resmed, Lumis ST 100/150, San Diego, California, USA). For those using intelligent volume assured pressure support, the settings were standardized by conversion to spontaneous-timed mode, applying their starting pressures. Thereafter, inspiratory positive airway pressure (IPAP) was increased in 2.0 cmH2O increments according to the predefined protocol, until the device limit was reached (25.0 or 30.0 cmH2O).
Transnasal Fiberoptic Laryngoscopy
A lubricated flexible laryngoscope (diameter 2.6 mm, Olympus, ENF-V3, Tokyo, Tokyo Prefecture, Japan) was inserted through a full-face mask (Phillips Respironics, Fitlife, Amsterdam, North Holland, Netherlands) into the nasopharynx until a satisfactory view of the larynx was achieved. A pneumotachograph (Fleisch, No. 3, Lausanne, Vaud, Switzerland) and differential pressure transducer (± 100 cmH2O, Validyne, MP 45, Northridge, California, USA) positioned within the circuit between the facemask and the NIV device measured airflow and pressure during the intervention.
The participants were premedicated with their prescribed acute medication, as directed by their pulmonologist, before application of a local anaesthetic spray (0.1 mL of 4% lidocaine, Accord Healthcare, Lidocaine, Middlesex, United Kingdom). Supplemental oxygen was provided to participants using long-term oxygen therapy, with the humidifier attached during the examination. Continuous pulse oximetry monitoring (Masimo Corporation, Rad-5, Irvine, California, USA) was maintained throughout the examination.
Laryngeal Ultrasound
After application of US gel, the linear transducer (frequency 5–10 MHz) of the portable US device (GE Healthcare, Vscan Air, Chicago, Illinois, USA) was used in 2-dimensional mode.27 First, the transducer was placed anteriorly and transverse over the middle section of the thyroid cartilage imaging the bilateral VFs and AEFs. Secondly, the transducer was placed vertically parallel to the lateral border of the thyroid cartilage on the right side for imaging of the indirectly right AEF; ie arytenoid cartilage (Figure 1).
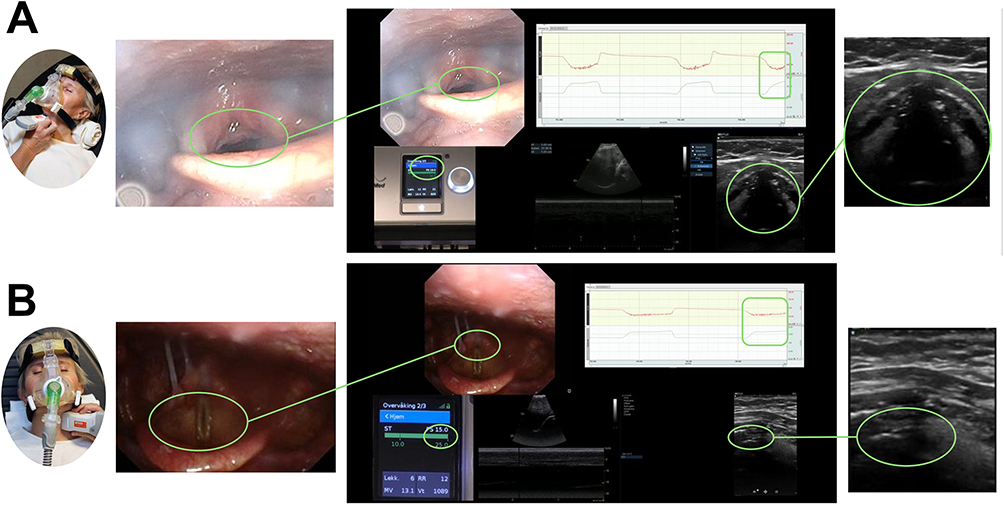 |
Figure 1 The laryngeal US probe placement is illustrated during NIV where image (A) shows anterior approach and image (B) lateral approach (right lateral approach is used during examination). The video recording of the parallel TFL and laryngeal US is shown in the middle with the structure of interest marked and enlarged. The inspiratory plateau pressure phase is indicated by green geometric shapes. Image A shows abduction of VFs and AEFs during IPAP 25 cmH2O and EPAP 6 cmH2O, whereas image B shows NIV-ILO with adduction of VFs and AEFs during IPAP 25 cmH2O and EPAP 10 cmH2O. Abbreviations: VFs, vocal folds; AEFs, aryepiglottic folds: NIV-ILO, non-invasive ventilation-induced laryngeal obstruction; IPAP, inspiratory positive airway pressure; EPAP, expiratory positive airway pressure; TFL, transnasal fberoptic laryngoscopy; US, ultrasound. |
Data Collection
Throughout the data collection the TFL was displayed on a television screen, the US transducer outputs was visualized on a mounted portable tablet (Samsung, Galaxy Tab S7, Seoul, South Korea) via Bluetooth, and the NIV device’s control panel was video-recorded by an external camera (Sony Computer Science Laboratories, Sony SRG-300HW, Tokyo, Tokyo Prefecture, Japan) for visualization during the entire examination. Airflow and pressure curve signals were digitalized and sampled for analysis (Biopac Systems, MP100, Goleta, California, USA) and run on a computer with appropriate software (Acknowledge Software, Acknowledge, East Palo Alto, California, USA). All the sources were routed via HDMI cables to a shared screen through a switcher (Blackmagic design, ATEM Mini Extreme ISO, South Melbourne, Victoria, Australia). The software recorded all the parallel recordings as one video file that was stored on the research server, allowing retrospective investigation. To ensure quality of the recordings, the complete setup was shown in real time and supervised throughout the procedure.
Visual Analysis of the Laryngeal Responses
The TFL assessment was described verbally in real time by the operator, while the video recordings of both the TFL and laryngeal US examinations were reviewed retrospectively in slow motion by two trained raters.7,27 Each pressure increment was followed by a short adaptation period (≈5 breaths) prior to observational assessment. The NIV respiratory cycles were analysed during inspiration (IPAP) and expiration (EPAP). The observations were categorised as occurring either at the onset of the inspiratory phase with rapid pressure rise (initial NIV-ILO) or later in the respiratory cycle during the stable pressurisation period (plateau pressure NIV-ILO), verified from the parallel video recorded setup (Figure 2). Observations were first categorised by the presence or absence of NIV-ILO, and then according to the anatomical level at which laryngeal adduction occurred: the laryngeal structures (VFs, AEFs, and epiglottis), the tongue base, and the hypopharynx.5,6 Observations involving high-standing epiglottis, tongue base, or the hypopharynx were registered but not classified as NIV-ILO.
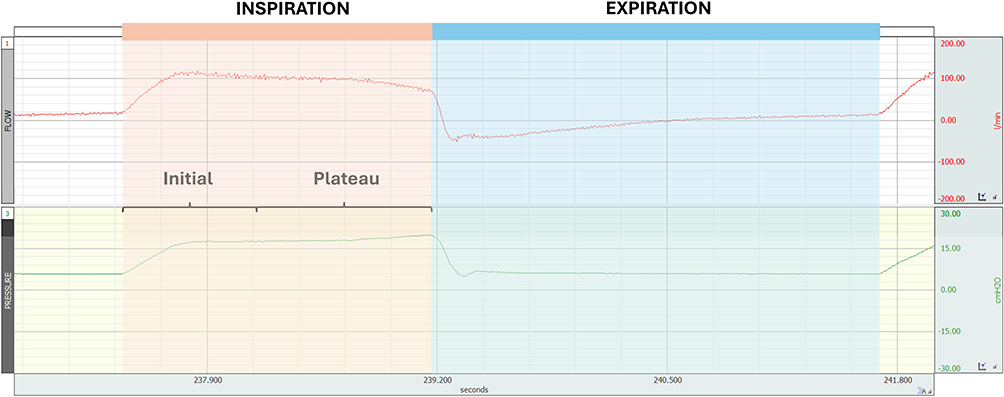 |
Figure 2 The pressure and flow waveforms from the parallel video recording were used to verify the inspiratory phase and to distinguish between the initial and plateau pressure phases. |
Tolerability
A numeric rating scale (NRS) from 0 (“not unpleasant at all”) to 10 (“worst imaginable discomfort”), was used to assess the participants’ experiences of the examination with TFL, US, and NIV settings.
Statistical Analysis
In the absence of prior studies to inform a formal sample size calculation, the study pragmatically included all eligible patients within the available time frame, guided by expert opinion and comparable physiological descriptive studies. Continuous sample characteristics are reported as medians with minimum-maximum, whereas dichotomous characteristics were reported as counts and percentages. Group comparisons between NIV-ILO and no NIV-ILO were performed using the Mann–Whitney U-test for continuous data or Fisher’s exact test for dichotomous data, as appropriate. A p-value of <0.05 was considered statistically significant. Descriptions of the laryngeal responses during NIV were reported as counts and percentages of participants. All statistical analyses were performed using Stata version 18 (StataCorp LLC, College Station, Texas, USA).
Results
Fifteen participants were included (40% female); their characteristics are given in Table 1. Three additional participants were eligible and scheduled for examinations; one cancelled due to acute infection, one did not attend, and one was excluded because of time constraints. There were no reported adverse events. Nine participants used a device with a maximum IPAP limit of 25.0 cmH2O while six participants used a device with a maximum limit of 30.0 cmH2O. The prescribed IPAP ranged from 7.0 to 30.0 cmH2O with a median of 17.0 cmH2O.
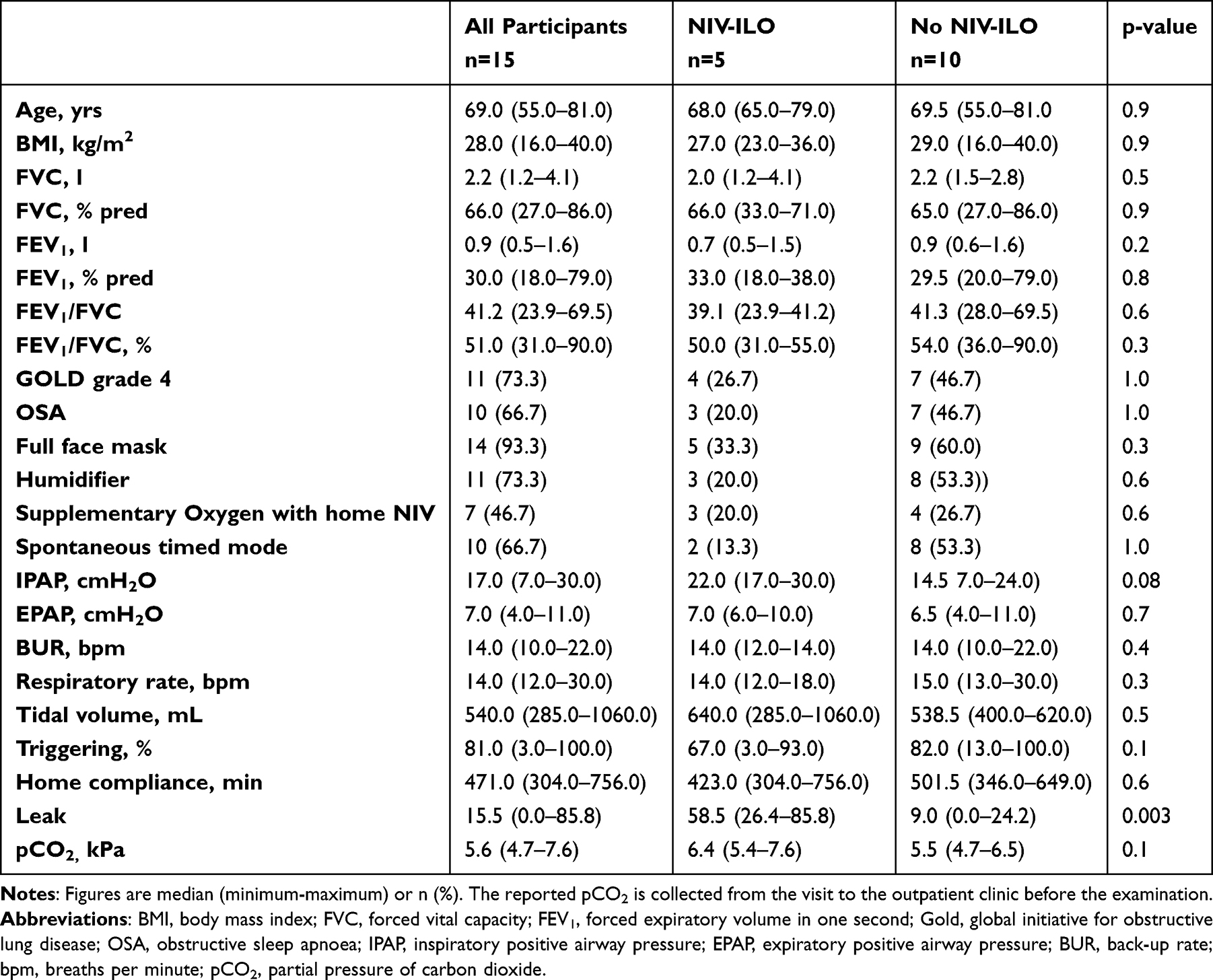 |
Table 1 Participant Characteristics and Home NIV Settings Stratified by Presence or Absence of NIV-ILO at the Usual Home Pressure Setting |
During spontaneous breathing 6 of 14 participants (42.9%) had a high-standing epiglottis throughout the respiratory cycle, including two with a juvenile epiglottis. In one of these, the AEFs were also rotated towards adduction during inspiration, indicating ILO.
While using the usual home NIV settings, the larynx was open at the onset of the initial inspiratory phase in all fifteen participants. During plateau pressure, NIV-ILO occurred in five participants (33.3%) at a median IPAP of 22.0 cmH2O (Table 2). The measured respiratory parameters included a median (minimum-maximum) respiratory rate of 16 (11–24) breaths per minute, tidal volume of 802.0 (477.0–1085.0) mL and SpO2 93.0 (85.0–98.0) %.
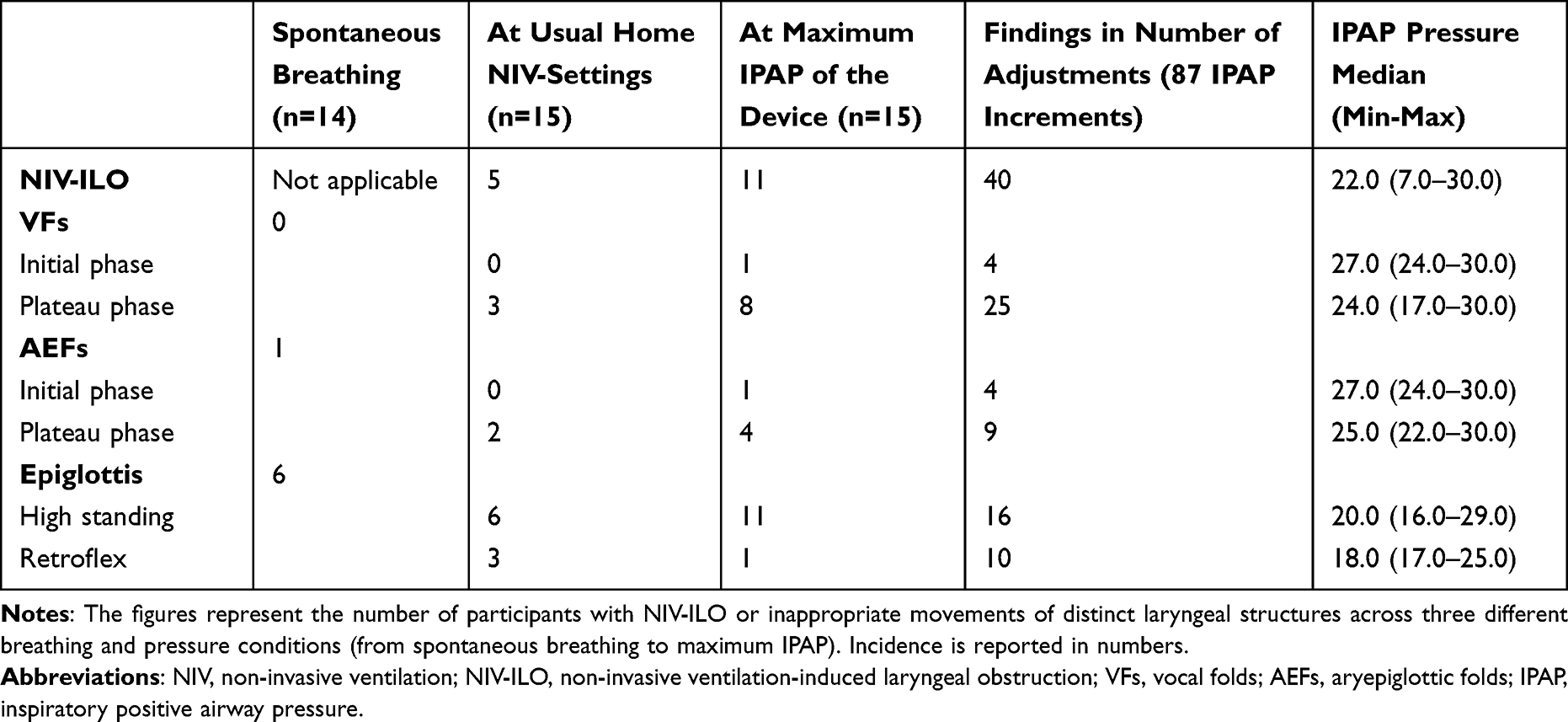 |
Table 2 Upper-Airway Movements Indicative of NIV-ILO Observed Across Three Different Breathing and Pressure Conditions (n=15) |
After evaluation of the home settings, IPAP was increased with 1 to 12 pressure adjustments per participant (Figure 3). NIV-ILO emerged in six additional participants during these increments, at a median IPAP of 20.5 cmH2O. This yielded a total of 11 participants (73.3%) with NIV-ILO, at a median IPAP of 22.0 cmH2O (minimum-maximum 16.0–30.0). The measured respiratory parameters at maximum IPAP included a median (minimum-maximum) respiratory rate of 16 (12–24) breaths per minute, tidal volume of 989.0 (646.0–1348.0) mL and SpO2 96.0 (90.0–99.0) %.
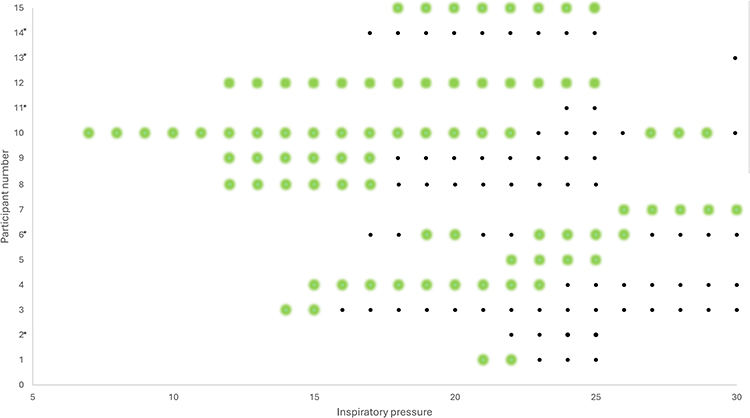 |
Figure 3 Dot chart visualizing the presence or absence of NIV-ILO at increasing pressures, starting from the prescribed home NIV setting and raised in 2 cmH2O increments up to the device’s maximum pressure (n=15). During unmeasured pressure increments (per 1 cmH2O), NIV-ILO presence or absence was categorized based on observations from the preceding measured increment. Black dots represent observations with NIV-ILO present, whereas green dots indicate its absence (no NIV-ILO). *=NIV-ILO at usual home NIV-pressures. Abbreviations: NIV-ILO, non-invasive ventilation-induced laryngeal obstruction. |
The laryngeal inlet showed dynamic behaviour, with adducting movements involving multiple laryngeal subsites in 7 of 11 participants (63.6%) (Figure 4). In some participants, obstructive responses also involved upper airway structures not included in the NIV-ILO definition. Backward movement the tongue base was observed in three participants, in two of whom the movement appeared during pressure increments. The oesophageal inlet became visible in three participants. In 9 of 15 participants (60%) expansion of the hypopharynx occurred during increases in the IPAP, and in six of these, a concomitant NIV-ILO was observed (Figure 5).
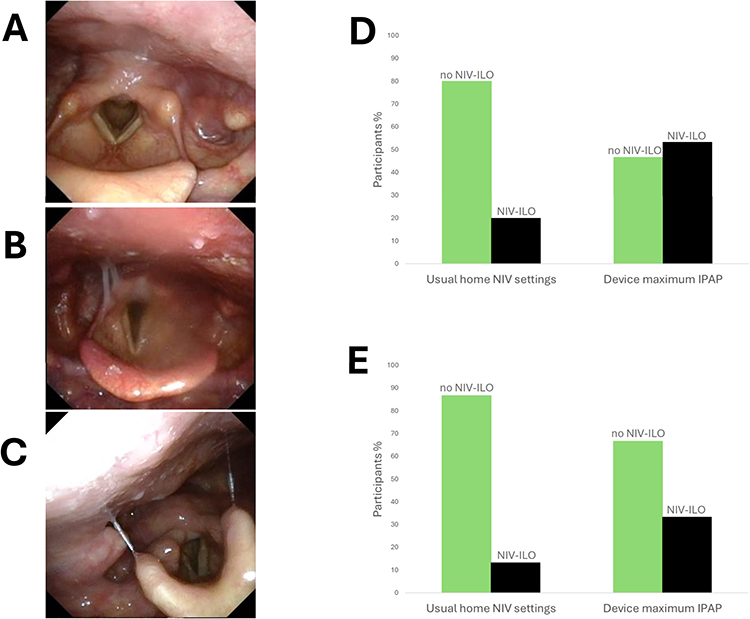 |
Figure 4 Laryngeal observations during inspiration from the VFs or AEFs indicating NIV-ILO visualized in pictures and graphs: Image (A) shows no NIV-ILO, image (B) indicates plateau pressure NIV-ILO (VF/AEF adduction, high raised epiglottis) and image (C) indicates initial pressure NIV-ILO (VF/AEF adduction, juvenile and high raised epiglottis). The bar graphs represent percentages of the total sample (n=15) with the described observation. Image (D) indicates VFs responses and image (E) the AEFs responses. Green colour represents laryngeal abduction of the VFs and AEFs (no NIV-ILO), while black represents presence of NIV-ILO. Abbreviations: VFs, vocal folds; AEFs, aryepiglottic folds; NIV-ILO, non-invasive ventilation induced laryngeal obstruction. |
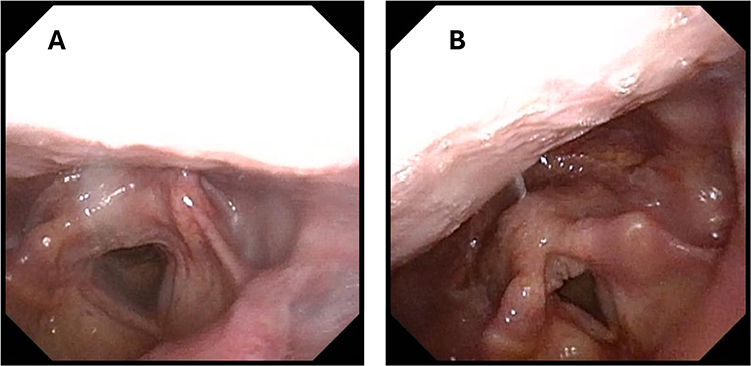 |
Figure 5 Example from a single participant showing occurence of NIV-ILO with increased pressure at the VFs with simultaneous expansion of the hypopharynx. (A) is captured at the individual’s usual home NIV-settings (IPAP 12 cmH2O), while (B) is from the highest applied IPAP (25 cmH2O), where VF adduction is observed along with a marked expansion of the hypopharynx. Abbreviations: IPAP, inspiratory positive airway pressure, NIV-ILO, non-invasive ventilation induced laryngeal obstruction; VFs, vocal folds. |
Ultrasound Detection of Obstructive Laryngeal Responses
The laryngeal structure was assessable with US for assessment of ILO in 11 of 15 participants (73.3%). Four participants were only assessable with lateral view, one participant was only assessable with anterior view, whereas six participants were assessable with both views.
In assessable participants, a total of 63 IPAP increments were conducted, of which 54 (85.7%) allowed visualization of the structures of interest. Visualization was achieved in 25 of 47 increments (53.2%) using anterior view and in 51 of 61 increments (83.6%) using lateral view. For US observations in the assessable participants (n=11), there was a 100% concordance with TFL.
Both assessment methods were well tolerated, with no discomfort reported by 6 of 15 for TFL (mean (minimum-maximum) score 0.9 (0.0–3.0)), by 11 of 15 for US (mean (minimum-maximum) score 0.2 (0.0–2.0)), and by 12 of 15 (mean (minimum-maximum) score 0.2 (0.0–2.0)) during NIV.
Discussion
In this study of awake participants with stable COPD receiving long-term NIV, we found that NIV-ILO was frequently observed at patients’ usual home pressure settings and was more frequent at higher IPAP levels. The upper airway responses to increasing IPAP were heterogenous rather than uniform across patients and structures. At lower pressures, obstruction was more frequently characterized by retroflexion of the epiglottis, while at higher pressures involvement of the AEFs was more commonly observed. Overall, the VFs represented the most common site of NIV-ILO.
Visualization of multiple upper airway structures during NIV confirmed that NIV-ILO was a frequent finding in patients with stable COPD receiving long-term NIV. The heterogeneous responses to positive pressure observed in this study may help explain the variable clinical success of long-term NIV in COPD. Although laryngeal responses to positive pressure have been explored in animal models,32 healthy volunteers,11,12,15,16 and amyotrophic lateral sclerosis,18,21 this phenomenon has received little scientific attention in COPD. To date, the study by Oppersma et al24 remains the only work published. They examined eight awake participants with COPD exacerbation receiving acute NIV and used laryngoscopy to quantify the glottic angle during pressure support ventilation and neurally adjusted ventilatory assist. Their hypothesis, similar to ours, was that glottic patency would decrease with rising inspiratory pressure. However, they found no change in glottic angle with increasing pressure or between modes. The discrepancy between findings may reflect differences in patient characteristics, clinical context, NIV modes and settings or interpretation of laryngeal behavior. Both studies included small samples, increasing the risk of Type II error and underscoring the need for cautious interpretation.
Our study revealed that most NIV-ILO events were dynamic, emerging with increasing inspiratory pressure rather than appearing as fixed obstructions. Similar dynamic laryngeal behaviour in response to devices applying positive pressure has also been reported in other chronic clinical contexts,18,19,21 and during disease exacerbations,24 suggesting that laryngeal responses to NIV are heterogeneous across conditions and individuals. These findings reinforce the concept of the larynx as an active valve to the lower airways balancing opposing demands required to optimize ventilation, airway protection, and phonation. Finely tuned reflex mechanisms are vital to this interplay, and interference from positive pressure may easily disturb the delicate equilibrium of the system.33
Home NIV in COPD aims to reduce PaCO2 and improve outcomes through effective ventilatory support.1,2 Studies indicate that higher inspiratory pressures enhance ventilatory efficacy and improve survival when titrated to reduce hypercapnia.34,35 In routine practice, however, pressures are often kept lower to improve patient tolerance as in our cohort. In our data, NIV-ILO became more frequent as inspiratory pressure increased, providing a plausible mechanistic link between pressure escalation and reduced adherence. High-intensity NIV, as defined by Windisch et al,36 employed very high inspiratory pressures (>28.0cmH2O) and backup rates to normalise PaCO2. Subsequent studies have refined this concept, demonstrating that similar physiological and clinical benefits can be achieved with lower pressures.37,38 Changes in PaCO2 have been proposed as a trigger for NIV-ILO.11,12,39 As CO2 was not measured, its potential contribution to NIV-ILO cannot be unequivocally determined. However, there was no evidence of hyperventilation based on respiratory rate, suggesting that a pure CO2-driven mechanism is unlikely. Instead, our findings suggest that NIV-ILO represents a form of heterogeneous laryngeal vulnerability, in which varying susceptibility to externally applied pressure and flow leads to transient adduction. These findings support an individualized, physiology-based approach to NIV aimed at optimizing control of hypercapnia, while recognizing that upper-airway behaviour may influence both ventilation and tolerance. Assessment of upper-airway responses during pressure titration may therefore be valuable in patients with poor adherence or difficulty tolerating NIV.
TFL is the reference standard for visualizing laryngeal responses,20 with VF angle used in prior NIV studies.11,12,24 In this study, NIV-ILO was defined as obstruction involving the VFs, AEFs, and retroflex epiglottis, but responses at the tongue base and in the hypopharynx were also observed – regions not fully encompassed by existing TFL-based classification systems. Accordingly, qualitative comparison with laryngeal US was warranted.
US is a validated diagnostic method for detecting VF paralysis postoperatively.40 In the context of NIV, its utility lies in real-time, non-invasive monitoring of laryngeal responses during treatment. Previous work by our group showed good concordance between US and TFL in healthy individuals,7 consistent with the current findings, although 26.7% of participants were non-assessable with laryngeal US. Despite this limitation, laryngeal US shows promise as a first-line tool to assess VFs and AEFs responses during ongoing positive pressure therapy, particularly when adjustments are required.
Strengths and Limitations
The main limitation of this study is the sample size. By using data from the Norwegian Registry for Long-Term Mechanical Ventilation, we were able to identify the eligible population and successfully include the majority of those who met the inclusion criteria. Nonetheless, the limited sample size precluded strict inferential statistical analysis, particularly regarding exploring associations and conducting subgroup comparisons.41 Despite this, the sample size is comparable to similar studies.5,6,17,21,24,25
Although participant discomfort during the examination was evaluated, no specific evaluation was conducted to assess how the participants perceived NIV-ILO events themselves. Consequently, patient-reported experience of NIV-ILO was not captured, and the relationship between observed laryngeal obstruction and subjective sensation remains unclear.
The study did not include a detailed analysis of the NIV pressure and flow waveforms recorded by the ventilator, which could have provided valuable insight into the functional consequences of the observed findings. A more comprehensive assessment, including synchronised measurements of flow and pressure with resistance calculations throughout the upper airway, would have allowed a deeper understanding of the underlying physiology.42,43
The described technical setup represents the major strength of the study. Parallel recording of multiple data sources enabled retrospective analysis of the respiratory phases.44 However, CO2 monitoring was not included, which could have informed the interpretation of laryngeal responses, as CO2 levels are known to affect laryngeal behavior in healthy individuals.39 All participants were examined using a full-face mask, regardless of individual preference, which may have contributed to the high frequency of NIV-ILO. Although nasal masks are increasingly recommended due to their lower risk of upper airway obstruction,45 this interface was not evaluated, as 14 of 15 participants used a full-face mask at home. The laryngeal responses associated with nasal mask use in stable COPD remain unclear and warrant further investigation.
Conclusion
This study demonstrates that NIV-ILO is common among stable COPD patients receiving long-term NIV, and that laryngeal US can serve as a practical first-line tool to assess laryngeal patency during NIV and to support individualised titration of ventilatory settings.
Acknowledgments
The authors would like to express their gratitude to medical photographer Thor Andre Ellingsen, Department of Pediatrics, Haukeland University Hospital, Bergen, Norway, for valuable help with the setup.
Norwegian Registry for Long-Term Mechanical Ventilation in collaboration with the Norwegian Centre of Excellence in Home Mechanical Ventilation, Department of Thoracic Medicine, Haukeland University Hospital, Bergen, also contributes to this work. The register is funded by the Western Norway Regional Health Authority.
Funding
This study was supported by the Western Norway Regional Health Authority (grant F-12817-D10980). Additional support was provided by the Western Norwegian Regional Health Authority General Research Fund for the HelpILO project (grant F12564).
Disclosure
Hege Clemm is the Chair of Global Initiative for ILO (unpaid). Patrick Murphy discloses a relationship with Breas, Philips, ResMed (grants or contracts, honoraria for lectures and support for attending meetings), GSK, Fischer & Paykel (grants or contracts and honoraria for lectures), Löwenstein (honoraria for lectures and support for attending meetings), Santhera and Chiesi (honoraria for lectures). Tiina Andersen discloses a relationship with Breas (member of Advisory Board and honoraria for lectures), ABM Respiratory Care (member of Advisory Board and honoraria for lectures), Löwenstein and Air Liquide (honoraria for lectures). The other authors report no conflicts of interest in this work.
References
1. Raveling T, Vonk J, Struik FM, et al. Chronic non-invasive ventilation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;8(
2. Ergan B, Oczkowski S, Rochwerg B, et al. European Respiratory Society guidelines on long-term home non-invasive ventilation for management of COPD. Eur Respir J. 2019;54(
3. Volpato E, Banfi P, Pagnini F. Promoting acceptance and adherence to noninvasive ventilation in chronic obstructive pulmonary disease: a randomized controlled trial. Psychosom Med. 2022;84(
4. Raveling T, Vonk JM, Hill NS, et al. Home noninvasive ventilation in severe COPD: in whom does it work and how? ERJ Open Res 2024;10(
5. Andersen T, Sandnes A, Hilland M. Laryngeal response patterns to mechanical insufflation-exsufflation in healthy subjects. Am J Phys Med Rehabil. 2013;92(10):920–929. doi:10.1097/PHM.0b013e3182a4708f
6. Andersen T, Sandnes A, Brekka AK, et al. Laryngeal response patterns influence the efficacy of mechanical assisted cough in amyotrophic lateral sclerosis. Thorax. 2017;72(3):221–229. doi:10.1136/thoraxjnl-2015-207555
7. Brekka AK, Ntoumenopoulos G, Røksund OD, et al. Use of laryngeal ultrasound to observe laryngeal movements during noninvasive ventilation in healthy volunteers. Respir Care. 2024:
8. Christensen PM, Heimdal JH, Christopher KL, et al. ERS/ELS/ACCP 2013 international consensus conference nomenclature on inducible laryngeal obstructions. Eur Respir Rev. 2015;24(137):445–450. doi:10.1183/16000617.00006513
9. Halvorsen T, Walsted ES, Bucca C, et al. Inducible laryngeal obstruction: an official joint European Respiratory Society and European Laryngological Society statement. Eur Respir J. 2017;50(3):1602221. doi:10.1183/13993003.02221-2016
10. Ludlow CL. Laryngeal reflexes: physiology, technique, and clinical use. J Clin Neurophysiol. 2015;32(4):284–293. doi:10.1097/wnp.0000000000000187
11. Jounieaux V, Aubert G, Dury M, Delguste P, Rodenstein DO. Effects of nasal positive-pressure hyperventilation on the glottis in normale sleeping subjects. J Appl Physiol. 1995;79(1):186–193. doi:10.1152/jappl.1995.79.1.186
12. Jounieaux V. Effects of nasal positive-pressure hyperventilation on the glottis in normal awake subjects. J Appl Physiol. 1995;79(1):176–185. doi:10.1152/jappl.1995.79.1.176
13. Bhabu P, Poletto C, Mann E, Bielamowicz S, Ludlow CL. Thyroarytenoid muscle responses to air pressure stimulation of the laryngeal mucosa in humans. Ann Otol Rhinol Laryngol. 2003;112(10):834–840. doi:10.1177/000348940311201002
14. Jounieaux V, Rodenstein DO. Glottic patency during noninvasive ventilation in patients with chronic obstructive pulmonary disease. Respir Physiol Neurobiol. 2019;259:178. doi:10.1016/j.resp.2018.09.001
15. Parreira VF, Delguste P, Jounieaux V, Aubert G, Dury M, Rodenstein DO. Glottic aperture and effective minute ventilation during nasal two-level positive pressure ventilation in spontaneous mode. Am J Respir Crit Care Med. 1996;154(6):1857–1863. doi:10.1164/ajrccm.154.6.8970381
16. Parreira VF, Jounieaux V, Aubert G, Dury M, Delguste PE, Rodenstein DO. Nasal two-level positive-pressure ventilation in normal subjects. Effects of the glottis and ventilation. Am J Respir Crit Care Med. 1996;153(5):1616–1623. doi:10.1164/ajrccm.153.5.8630611
17. Andersen TM, Sandnes A, Fondenes O, et al. Laryngeal responses to mechanically assisted cough in progressing amyotrophic lateral sclerosis. Respir Care. 2018;63(5):538–549. doi:10.4187/respcare.05924
18. Georges M, Attali V, Golmard JL, et al. Reduced survival in patients with ALS with upper airway obstructive events on non-invasive ventilation. J Neurol Neurosurg Psych. 2016;87(10):1045–1050. doi:10.1136/jnnp-2015-312606
19. Sayas Catalán J, Jiménez Huerta I, Benavides Mañas P, et al. Videolaryngoscopy with noninvasive ventilation in subjects with upper-airway obstruction. Respir Care. 2017;62(2):222–230. doi:10.4187/respcare.04784
20. Conde B, Martins N, Brandão M, Pimenta AC, Winck JC. Upper airway video endoscopy: assessment of the response to positive pressure ventilation and mechanical in-exsufflation. Pulmonology. 2019. 25.
21. Sarasate M, Córdoba-Izquierdo A, Farrero E, et al. Effect of noninvasive ventilation on the upper airway in patients with amyotrophic lateral sclerosis: the role of upper-airway endoscopy. Respir Care. 2025;70(9):1075–1083. doi:10.1089/respcare.12791
22. Oppersma E, Doorduin J, van der Heijden EH, van der Hoeven JG, Heunks LM. Noninvasive ventilation and the upper airway: should we pay more attention? Crit Care. 2013. 17.
23. Ruane L, Daley C, D’Souza D, et al. Vocal cord dysfunction (VCD) in hospitalised exacerbations of asthma and chronic obstructive pulmonary disease (COPD). Eur Resp Soc. 2019;2019:1.
24. Oppersma E, Doorduin J, Gooskens PJ, et al. Glottic patency during noninvasive ventilation in patients with chronic obstructive pulmonary disease. Respir Physiol Neurobiol. 2019;259:53–57. doi:10.1016/j.resp.2018.07.006
25. Baz M, Haji GS, Menzies-Gow A, et al. Dynamic laryngeal narrowing during exercise: a mechanism for generating intrinsic PEEP in COPD? Thorax. 2015;70(3):251–257. doi:10.1136/thoraxjnl-2014-205940
26. Miki K, Tsujino K, Fukui M, et al. Laryngeal widening and adequate ventilation by expiratory pressure load training improve aerobic capacity in COPD: a randomised controlled trial. Thorax. 2023;79(1):23–34. doi:10.1136/thorax-2022-219755
27. Brekka AK, Vollsæter M, Ntoumenopoulos G, et al. Adjustments of non-invasive ventilation and mechanically assisted cough by combining ultrasound imaging of the larynx with transnasal fibre-optic laryngoscopy: a protocol for an experimental study. BMJ Open. 2022;12(5):e059234. doi:10.1136/bmjopen-2021-059234
28. Slinger C, Leong P, Spencer S, Slinger R, Govender R. Is trans-laryngeal ultrasound (TLUS) an accurate and acceptable tool in the assessment of inducible laryngeal obstruction? A protocol for the ILOTUS: a cross-sectional, two-stage feasibility study. Adv Commun Swallow. 2024;27(2):131–141. doi:10.3233/acs-230003
29. Chatwin M, Sancho J, Lujan M, Andersen T, Winck J-C. Waves of precision: a practical guide for reviewing new tools to evaluate mechanical in-exsufflation efficacy in neuromuscular disorders. J Clin Med. 2024;13(9):2643. doi:10.3390/jcm13092643
30. Pp R. Human experimentation: code of ethics of W.M.A. Br Med J. 1964;2(5402):177. doi:10.1136/bmj.2.5402.177
31. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
32. Moreau-Bussière F, Samson N, St-Hilaire M, et al. Laryngeal response to nasal ventilation in nonsedated newborn lambs. J Appl Physiol. 2007;102(6):2149–2157. doi:10.1152/japplphysiol.00891.2006
33. Andersen TM, Hov B, Halvorsen T, Røksund OD, Vollsæter M. Upper airway assessment and responses during mechanically assisted cough. Respir Care. 2021;66(7):1196–1213. doi:10.4187/respcare.08960
34. Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD exacerbation: a randomized clinical trial. JAMA. 2017;317:2177–2186. doi:10.1001/jama.2017.4451
35. Köhnlein T, Windisch W, Köhler D, et al. Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. Lancet Resp Med. 2014;2(9):698–705. doi:10.1016/S2213-2600(14)70153-5
36. Windisch W, Haenel M, Storre JH, Dreher M. High-intensity non-invasive positive pressure ventilation for stable hypercapnic COPD. Int J Med Sci. 2009;6(2):72. doi:10.7150/ijms.6.72
37. Patout M, Lhuillier E, Kaltsakas G, et al. Long-term survival following initiation of home non-invasive ventilation: a European study. Thorax. 2020;75(11):965–973. doi:10.1136/thoraxjnl-2019-214204
38. Murphy PB, Brignall K, Moxham J, Polkey MI, Davidson AC, Hart N. High pressure versus high intensity noninvasive ventilation in stable hypercapnic chronic obstructive pulmonary disease: a randomized crossover trial. Int J Chron Obstruct Pulmon Dis. 2012;7:811. doi:10.2147/COPD.S36151
39. Jounieaux V, Parreira VF, Aubert G, Dury M, Delguste P, Rodenstein DO. Effects of hypocapnic hyperventilation on the response to hypoxia in normal subjects receiving intermittent positive-pressure ventilation. Chest 2002;121(
40. Patel A, Spychalski P, Aszkiełowicz A, Mikaszewski B, Kobiela J. Transcutaneous laryngeal ultrasound for vocal cord paralysis assessment in patients undergoing thyroid and parathyroid surgery-a systematic review and meta-analysis. J Clin Med. 2021. 10.
41. Brekka AK, Solli PV, Indrekvam S, et al. Inspiratory laryngeal observations during non-invasive ventilation titration in individuals with COPD. Eur Respir J. 2025;66(suppl 69):PA2074. doi:10.1183/13993003.congress-2025.PA2074
42. Brekka AK, Vollsæter M, Fretheim-Kelly Z, et al. Exploring upper airway and laryngeal resistance to noninvasive ventilation in healthy awake adults. Physiolog Rep 2025;13(
43. Andersen TM, Brekka AK, Fretheim-Kelly Z, et al. Upper airway and translaryngeal resistance during mechanical insufflation-exsufflation. Chest. 2024;167:188–201. doi:10.1016/j.chest.2024.08.022
44. Andersen TM, Conde B, Vollsæter M. Seeing in synchrony: toward personalized noninvasive ventilation in amyotrophic lateral sclerosis through dynamic upper-airway visualization. Respir Care. 2025. doi:10.1089/respcare.13193
45. Vrijsen B, Buyse B, Belge C, Testelmans D. Upper airway obstruction during noninvasive ventilation induced by the use of an oronasal mask. J Clin Sleep Med. 2014;10:1033–1035. doi:10.5664/jcsm.4046
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.