Back to Journals » International Journal of General Medicine » Volume 18
Lactate Dehydrogenase Indicates Development From Fulminant Myocarditis to Chronic Persistent Myocarditis: A Multicenter Retrospective Cohort Study in China
Authors Zhao Q, Li Z, Wang DW, Li F, Zhang L, Jiang J
Received 29 November 2024
Accepted for publication 28 February 2025
Published 6 March 2025 Volume 2025:18 Pages 1333—1344
DOI https://doi.org/10.2147/IJGM.S509291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Qu Zhao,1,2 Zeping Li,1,2 Dao Wen Wang,1,2 Fan Li,1,2 Li Zhang,3 Jiangang Jiang1,2
1Division of Cardiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 2Hubei Key Laboratory of Genetics and Molecular Mechanisms of Cardiological Disorders, Wuhan, 430030, People’s Republic of China; 3Division of Cardiology, Minda Hospital of Hubei Minzu University, Enshi, 445099, People’s Republic of China
Correspondence: Jiangang Jiang, Division of Cardiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China, Email [email protected]
Background: Fulminant myocarditis (FM) is a critical manifestation of myocarditis. However, the clinical features and risk factors associated with its adverse outcomes are not fully understood. Given the high mortality and potential for long-term complications, it is crucial to identify factors that could predict the progression of FM to chronic persistent myocarditis. We hypothesize some clinical or laboratory markers may be predictive of this progression. This study aims to identify clinical factors that may help predict the progress of FM to chronic persistent myocarditis.
Methods: A total of 82 patients with FM treated based on Chinese protocol were included. Kaplan–Meier curve and regression analysis were used to determine the clinical features and prognostic predictors of chronic persistent myocarditis in patients with 24 months of follow-up.
Results: Chronic persistent myocarditis was observed in 20 patients during the follow-up. ROC curve showed that the critical value for chronic persistent myocarditis caused by lactate dehydrogenase (LDH) was 577.00U/L (sensitivity 75.0%, specificity 74.2%). Time from onset to admission over 6 days and LDH > 577.00U/L were identified as risk factors for chronic persistent myocarditis in patients with FM in both univariate and multivariate cox analysis. The hazard ratio and 95% Confidence intervals were 3.35 (1.32– 8.50) (p = 0.011) and 6.11 (2.02– 18.48) (p < 0.001), respectively. The per standard deviation of increment in LDH was associated with the 55% (1.55, 1.11– 2.18) in HR and 95% CI of the occurrence of chronic persistent myocarditis.
Conclusion: About 24.4% of the patients with FM treated based on the life support measures proposed in the consensus of Chinese Society of Cardiology have been observed chronic persistent myocarditis. Time from onset to admission over 6 days and LDH levels > 577.00 U/L at admission may serve as risk factors for the progression from FM to chronic persistent myocarditis.
Keywords: fulminant myocarditis, chronic persistent myocarditis, prognosis
Introduction
Fulminant myocarditis (FM) is the most dangerous form of acute myocarditis with low morbidity and high mortality and can progress suddenly and rapidly to severe heart failure, refractory arrhythmias, cardiogenic shock and even death in as little as several days.1,2 Acute lymphocytic myocarditis represents the predominant pathological subtype of fulminant myocarditis.3,4 The swift advancement of the disease poses challenges for patients to receive a prompt and accurate diagnosis, leading to delayed diagnosis, misdiagnosis, or even fatality. Nevertheless, timely mechanical support and immunoregulatory therapy are believed to considerably decrease in-hospital mortality rates in patients with fulminant myocarditis.5
The prognosis of FM is a topic of debate. A single-center retrospective cohort study with average period of follow-up was 5.6 years in 20006 reported that FM has a better prognosis than non-fulminant myocarditis (NFM). However, the results of this study are now thought to be affected by the low incidence of endomyocardial biopsy (EMB) and limited choice of mechanical circulatory support (MCS) devices.7 This can lead to differential diagnosis and misleading pathological diagnosis, which may result in an incorrect conclusion. Recently, a retrospective, international, multicenter cohort study8 have shown that impaired haemodynamics at presentation is a major determinant of both short and long-term prognosis in FM patients, with the incidence of cardiac death or heart transplantation (HTx) being 28% at day 60 and 47.7% at 7 years. Histological subtype4,9 and QRS width on electrocardiogram (ECG)8 of FM patients may also had independent prognostic value. However, the factors that contribute to chronic persistent myocarditis in FM patients require further investigation.
This study aims to identify clinical factors that may influence the progression of fulminant myocarditis to chronic persistent myocarditis after treatment. The findings will provide valuable information for predicting the risk of chronic persistent myocarditis for FM patients after hospitalization.
Methods
Study Population
This multicenter retrospective cohort study included acute myocarditis patients admitted to Tongji Hospital Tongji Medical College of Huazhong University of Science and Technology and Minda Hospital of Hubei Minzu University from February 2017 to June 2023. The diagnosis of acute myocarditis was made by an experienced clinician and requires at least one clinical manifestation and one diagnostic criteria, or at least two diagnostic criteria, and the exclusion of other diseases with similar manifestations.10 The clinical manifestation10 goes to: (1) acute chest pain, pericarditic, or pseudo-ischaemic; (2) new-onset or worsening of dyspnoea at rest or exercise, and/or fatigue, with or without left and/or right heart failure signs; (3) subacute/chronic or worsening of fatigue, with or without left and/or right heart failure signs and/or dyspnoea at rest or exercise; (4) aborted sudden cardiac death, and/or palpitation, and/or unexplained arrhythmia symptoms and/or syncope; (5) unexplained cardiogenic shock. The diagnostic criteria10 go to: (1) newly abnormal 12 lead ECG and/or Holter and/or stress testing; (2) elevated TnT/TnI; (3) functional and structural abnormalities on cardiac imaging; (4) tissue characterization by cardiac magnetic resonance (CMR). Fulminant myocarditis, as previous studies have reported,8 was defined as acute presentation with hemodynamic compromise requiring inotropes and/or MCS, such as intra-aortic balloon pump (IABP) and extracorporeal membrane oxygenation (ECMO).8,11 The inclusion criteria for this study were as follows: (1) clinical diagnosis of FM; (2) hospitalization of more than 48 hours. Exclusion criteria for this study were as follows: (1) not confirmed by EMB or CMR; (2) death or HTx during hospitalization; (3) refusal of follow-up; (4) history of ischaemic cardiomyopathy, myocarditis, cardiomyopathy, malignant tumor/cancer and other diseases affecting cardiac function and prognosis; (5) time from onset to hospitalization longer than 30 days; (6) children (<15 years old).
End Points
The end point of this study was chronic persistent myocarditis. According to the guideline from Japanese Circulation Society (JCS)3 and the expert consensus document of acute myocarditis and chronic inflammatory cardiomyopathy in 2020,1 chronic persistent myocarditis was defined as highly sensitive cardiac troponin levels in the blood of FM patients continuously elevated for more than 30 days after discharge. In this study, we defined highly sensitive cardiac troponin level as high-sensitivity cardiac troponin I (hs-cTnI) >15.6 pg/mL according to the test standard of the clinical lab of the hospital. Outpatient follow-up was scheduled at 1, 3, and 6 months post-discharge, with subsequent visits every 6 months for patients in stable condition. These follow-up appointments included adjustments to medications, hs-cTnI testing and echocardiographic evaluations. In the event of acute episodes or special conditions, patients have access to dedicated communication channels for the timely identification and management of emergencies. Two or more times of increased hs-cTnI detected within the 6-month follow-up was considered as the occurrence of the endpoint. The time when hs-cTnI elevation was first detected was taken as the time the end point occurred.
Laboratory methods
Laboratory tests for blood samples were collected and tested within two hours of admission. Laboratory tests included routine blood tests, aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, high-sensitive cardiac troponin I (hs-cTnI), N-terminal pro-B-type natriuretic peptide (NT-proBNP), lactate dehydrogenase (LDH), Creatine Kinase MB isoenzyme (CK-MB) or Creatine Kinase (CK), high-sensitive C-reactive protein (hs-CRP), erythrocyte sedimentation rate (ESR), procalcitonin (PCT), Interleukin-1β (IL-1β), Interleukin-2 receptor (IL-2R), Interleukin-6 (IL-6), Interleukin-8 (IL-8), Interleukin-10 (IL-10), tumor necrosis factor α (TNF-α), Procalcitonin (PCT), Lactic Acid (LA), D-D Dimer, activated partial thromboplastin time (APTT) and prothrombin time (PT).
Endomyocardial Biopsy
EMB was done as previous described.12 The bioptome was accurately positioned on the apical left ventricular septum. Ideally, the specimens should measure between 2 and 3 mm³ in size. A minimum of 3 to 5 biopsy samples should be obtained to ensure adequate sampling. The specimens are routinely processed for staining and subsequent histological examination. The diagnosis of pathological classification was based on the Dallas criteria.13
Cardiac Magnetic Resonance Imaging
CMR was conducted during the hospital stay using a 1.5-T system equipped with a 32-channel cardiac coil. The CMR protocol included cine imaging, T2-weighted sequences, first-pass perfusion, and breath-held late gadolinium enhancement (LGE), consistent with previously reported.14
Treatment of Patients
We implemented a comprehensive treatment plan based on the life support measures proposed in the consensus of the Chinese Society of Cardiology5,15 in both hospitals. The treatment plan was mainly based on the following 4 principles: (1) mechanical life support, including the utilization of mechanical ventilators and circulatory support systems such as ECMO, IABP, continuous renal replacement therapy (CRRT), temporary pacemakers, etc.; (2) immunomodulation through appropriate administration of corticosteroids and intravenous immunoglobulin (IVIG); (3) antiviral therapy. Patients were given oral glucocorticoids tablets after discharge for months. The complications of the patient at discharge and other drug use during follow-up were shown in Table S1.
Statistical Analysis
The baseline characteristics of the analyzed samples were summarized based on the occurrence of chronic persistent myocarditis. Categorical variables were presented as frequencies and percentages, while continuous variables were reported as medians with interquartile ranges (IQR). The chi-square test was employed for categorical variables, and the Student’s t-test was used to compare baseline characteristics in terms of continuous variables. Differences in categorical data were analyzed using the Fisher exact test. Predictive mean matching was used to interpolate for variables with missing values of 5–20%. To identify clinically relevant prognostic factors, logistic and cox regression analysis was used to identify predictors associated with outcome. In the regression analysis, variables with p < 0.05 were included in the regression model.
The p-value of the interaction was calculated to assess the consistency of the patterns observed in the main results. Analyses and plotting were conducted using GraphPad Prism version 10.0.0 for Windows (GraphPad Software, Boston, MA, www.graphpad.com, USA) and R software (the R Foundation, http://www.r-project.org, version 4.0.2) with a two-sided significance threshold of p < 0.05.
Results
The Population of FM Patients
A total of 82 FM patients were selected from a group of 304 patients who had received clinical diagnosis for acute myocarditis from February 2017 to June 2023 in Tongji Hospital affiliated to Huazhong University of Science and Technology and Minda Hospital of Hubei Minzu University from China. The flow chart is presented in Figure S1. The mean age of patients enrolled was 34 years old (IQR 24–47 years old) and 41.5% were male, with a median hospitalization of 12 days (IQR 9–17 days) and a median time from onset to hospital admission of 3 days (IQR 2–5 days). A total of 45 patients (54.9%) underwent EMB, all of whom were diagnosed with lymphocytic myocarditis. Additionally, 75 patients (91.5%) underwent CMR. Notably, 38 patients (46.3%) received both EMB and CMR examinations. Chronic persistent myocarditis was observed in 20 patients (24.4%) during follow-up. The main characteristics of the patients did not develop chronic persistent myocarditis (n = 62) and those developed chronic persistent myocarditis (n = 20) are shown in Tables 1 and S2. At baseline, the patients did not develop chronic persistent myocarditis were found lower levels of hs-cTnI, AST and LDH compared with those developed chronic persistent myocarditis. There were no significant differences in age, sex, clinical manifestation, medical history, blood pressure, left ventricular ejection fraction (LVEF), NT-proBNP, leukocytosis, neutrophil count, lymphopenia, hs-CRP, ESR, PCT and serum inflammatory parameters (IL-1β, IL-2R, IL-6, IL-8, IL-10 and TNF-α) between the two groups.
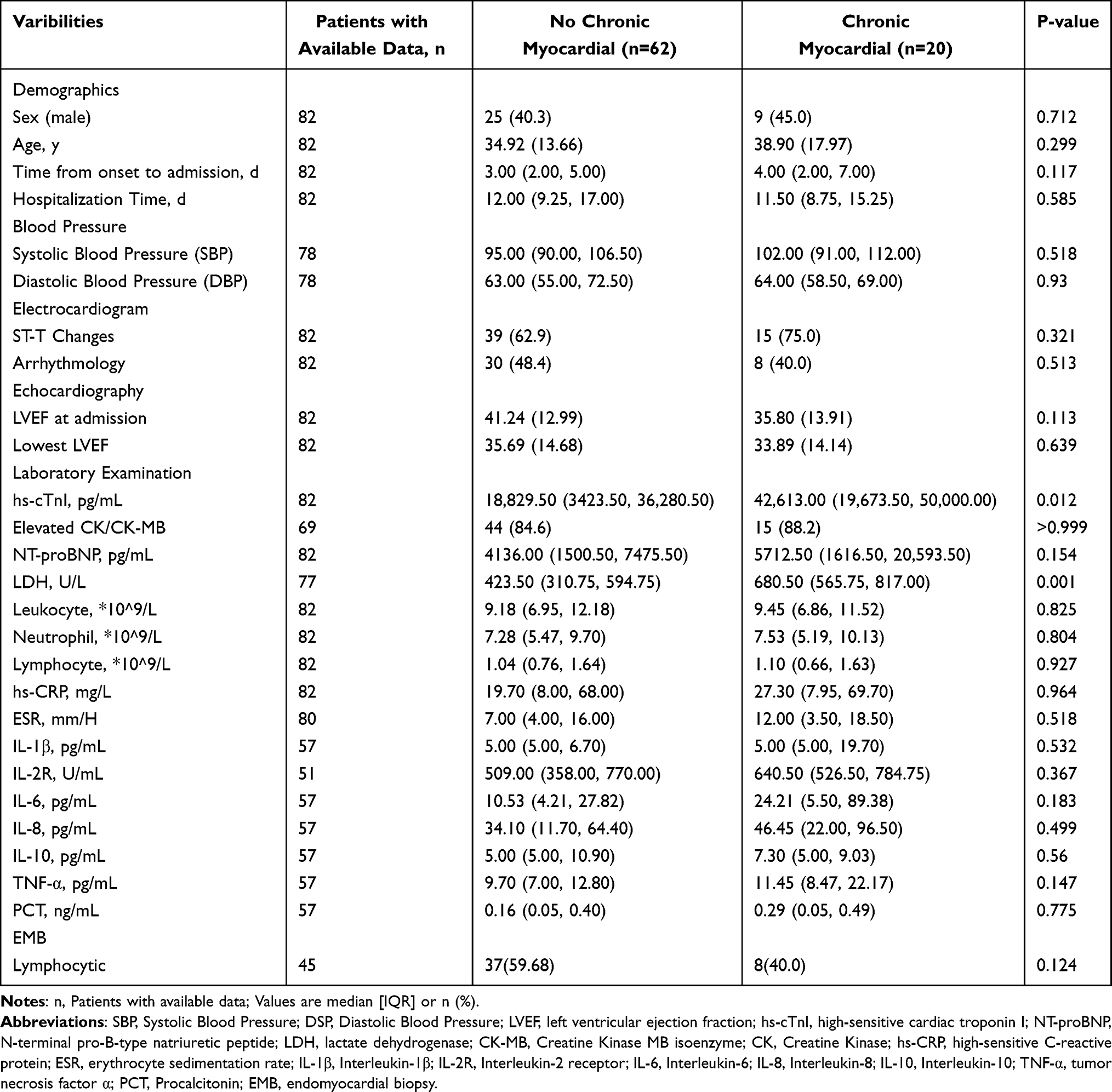 |
Table 1 Baseline Characteristics of Patients in the Study |
Outcome of Patients With FM
In-hospital management of the patients is detailed in the Table S3. All patients received immunosuppressive therapy. Glucocorticoids were used in all patients and IVIG in 79 patients, with no difference in dose between the two groups. Regarding mechanical circulatory support, IABP was the most common MCS used in 93.9% of patients developed chronic persistent myocarditis (median time 4 days, IQR: 3–6 days) and 81.5% of those did not (median time 4 days, IQR: 2–7 days), showing no difference between the two groups. The use of temporary external pacing, CRRT and ECMO also showed no difference.
We did not find a strong association between hs-cTnI and cardiac function (presented as LVEF) during the follow-up (Table S4). The changes in hs-cTnI and LVEF of two typical patients were depicted in Figure S2, one with chronic persistent myocarditis (Figure S2a) and one with complete recovery (Figure S2b), showing LVEF to improve as hs-cTnI decreased.
Analysis of Factors Associated With Chronic Persistent Myocarditis
To identify clinically relevant prognostic factors for the occurrence of chronic persistent myocarditis in patients with FM, we performed both univariate logistic and univariate cox regression analysis of baseline data and hospital admissions factors in the two groups to get a more stable and reliable results (Table S5). Time from onset to admission over 6 days, hs-cTnI, NT-proBNP, LDH and IL-6 were significantly associated with the occurrence of chronic persistent myocarditis in both univariate logistic and univariate cox analysis. The ROC curve (Figure 1) showed that the LDH and hs-cTnI were predictive values for chronic persistent myocarditis compared with other laboratory results statistically significant in univariate analysis. The cutoff value of LDH was 577.00U/L (sensitivity 75.0%, specificity 74.2%). The cutoff value of hs-cTnI was 34991.50pg/mL (sensitivity 74.2%, specificity 60.0%).
 |
Figure 1 ROC curve for chronic persistent myocarditis. Abbreviations: AUC, area under the curve; CI, confidence interval; LDH, lactate dehydrogenase; IL-6, Interleukin-6; hs-cTnI, high-sensitive cardiac troponin I; NT-proBNP, N-terminal pro-B-type natriuretic peptide. |
The results of stepwise multivariable cox regression analysis (Table 2) showed that time from onset to admission over 6 days and LDH > 577.00U/L were identified as risk factors for chronic persistent myocarditis in patients with FM after discharge in multivariate cox analysis. We adjusted these two factors with sex and age as demographic confounding factors in Model 2 and used EMB16 and LVEF at admission4 as clinically relevant confounding factors according to previous research in Model 3. Time from onset to admission over 6 days and LDH > 577.00U/L still showed statistical significance in these two models. The HR and 95% Confidence intervals were 3.35 (1.32–8.50) (p = 0.011) and 6.11 (2.02–18.48) (p < 0.001), respectively in model 1. The per standard deviation (SD) of increment in LDH was associated with the 55% (1.55, 1.11–2.18) in HR and 95% confidence interval (CI) of the occurrence of chronic persistent myocarditis. The unadjusted Kaplan–Meier survival curve showed a significant difference between the groups of patients with different levels of time from onset to admission and LDH (Figure 2a and b). Compared to patients admitted within 6 days after onset, those who admitted over than 6 days were more likely to develop chronic persistent myocarditis (p = 0.029), with post-hoc power 58.6%. Patients with LDH > 577.00U/L (divided according to the cutoff value of ROC curve) were more likely to develop chronic persistent myocarditis than those with LDH ≤ 577.00U/L (p < 0.001), with post-hoc power 98.7%.
 |
Table 2 Multivariate Cox Analysis of Factors Associated With the Occurrence of Chronic Persistent Myocarditis |
 |
Figure 2 Unadjusted K-M curve of chronic persistent myocarditis in sub group of time from onset to admission (a) and LDH (b). Abbreviation: LDH, lactate dehydrogenase. |
Discussion
Acute myocarditis can be caused by infection with viruses, parasites, mycoplasmas and fungi. Viruses are the most common cause of infection, including Coxsackievirus B3, parvovirus B19, human herpesvirus 617 and upper respiratory viruses such as SARS-CoV-2.18 HIV, toxins, drugs and autoimmune phenomena can also cause acute myocarditis. The pathophysiological process of acute myocarditis caused by coxsackie virus infection in humans can be divided into three stages:17 (1) Coxsackie virus binds to corresponding receptors on the cell surface, and the resultant complex is internalized by the cell, leading to the activation of the host innate immunity. Then, virus replication in cardiomyocytes leads to cell lysis, which triggers a cascade of reactions resulting in cytokine release. (2) Specific immunity is activated, and natural killer cells, macrophages, and virus-specific T cells converge at the site of infection. High levels of cytokines, including TNFα, IL-1α, IL-1β, IL-2, and interferon-gamma (IFN-γ), can even cause inflammatory storms,7 leading to autoimmune-mediated damage. (3) Inflammation generally resolves after a few weeks, and in most patients, the myocardial damage completely resolves with the elimination of the virus. Early and timely use of MCS and corticosteroids and IVIG can effectively control the inflammatory storm caused by immune overactivation in FM patients.7,15 However, there are still a small number of patients develop chronic inflammation and dilated cardiomyopathy (DCM).
The pathophysiological mechanism leading to the transformation of acute myocarditis into chronic inflammatory is not yet clear, and chronic persistent myocarditis can be regarded as a transitional stage between acute myocarditis and chronic inflammatory cardiomyopathy.1 One possible reason is the persistence of the viral genome.17 Clinical studies have demonstrated that clearance of the viral genome can substantially enhance both the left ventricular end diastolic and end systolic diameters, as well as LVEF in myocarditis patients.19,20 Host genetics also plays a significant role in the progression of myocardial inflammation into chronic inflammation. In human, the polymorphism of MHC,21,22 CD4523 are associated with an increased risk of acute myocarditis developing into chronic inflammation. In animal models, studies have shown that deletion of certain key genes, such as TLR3,24 ISG15,25 TRIM18,26 may lead to a weakened innate immune response to enterovirus infection in individuals, resulting in reduced viral clearance and an increased risk of chronic inflammation. Genetic predispositions and environmental factors can work together to drive chronic inflammation. In addition to viral genomes, cardiotoxic agents and hemodynamic changes are also contributors to this process.27 However, eliminating the virus, even with favorable genetic and environmental factors, does not guarantee the resolution of chronic inflammation. Studies show that myocardial inflammation can persist in mice after virus clearance,28 possibly due to over-activation of autoimmune reactivity. Pro-inflammatory Th17 cells and regulatory T (Treg) cells, which suppress inflammation, play pivotal roles in the chronic progression of myocarditis.29 Th17 cells contribute to the overactivation of autoimmune responses by secreting pro-inflammatory cytokines such as IL-17, TNF-α, and IL-1β. An increased presence of Th17 cells has been associated with myocardial fibrosis and a worsening of functional status, as indicated by the New York Heart Association (NYHA) classification.30 In contrast, Treg cells exhibit protective effects by suppressing excessive inflammation and were shown to inhibit the development of cardiomyopathy in murine models of myocarditis induced by CVB3 infection.31 Beyond the Th17/Treg balance, targeting other immune components, including NLRP3 inflammasome,32 complement pathways, NK cells,33 and mast cells34 may also help reduce inflammation and prevent chronic inflammation progression. The role of TGF-β in viral myocarditis is particularly complex. While it supports Treg function to suppress immune responses against heart tissue and maintain antiviral immunity,35 it also promotes myofibroblast formation and myocardial fibrosis progression through the Wnt/β-catenin pathway.36
The innovation of this study is that we examine the end point of chronic persistent myocarditis, which has never been used as a prognostic outcome for FM patients, with most studies of acute myocarditis have focused on death, HTx or DCM. Our study identified that prolonged time from onset to admission and high LDH as risk factor for FM patients to develop chronic persistent myocarditis. It is easy to understand that a short time from onset to admission, which is nearly equivalent to early treatment, may reduce the risk of chronic persistent myocarditis in FM patients – it allows early intervention in this rapidly progressing disease. A number of studies have also provided evidence for early treatment in the acute stage of FM, and early treatment was strongly recommended in the Chinese guidelines for the diagnosis and treatment of adult fulminant myocarditis.15 This finding also indicates that clinicians should devote greater attention to patients with prolonged time from onset to admission, thereby facilitating the earlier detection of potential chronic progression.
Imaging techniques differ in sensitivity and applicability for effective myocarditis monitoring, depending on their specific function. Traditional echocardiography, while accessible and useful for assessing cardiac structure and function, lacks the sensitivity needed to detect inflammation. Two- and three-dimensional speckle-tracking echocardiography is a valuable tool for predicting adverse prognosis in acute myocarditis patients,37 though its use may be restricted to non-critical cases.38 Advanced methods like FDG-PET and CMR are effective in identifying early myocardial damage, edema, and fibrosis1 and they offer predictive value for adverse outcomes in acute myocarditis.39 However, their high costs and the need for specialized expertise limit their use in resource-constrained settings, making them not ideal for routine follow-up. CT is primarily employed to evaluate structural changes or exclude other conditions but is not routinely used for myocarditis. Additionally, certain patient factors, such as physical limitations or contraindications like metal implants, may restrict the use of these imaging modalities. Therefore, there is a need to identify reliable biological markers to monitor the prognosis of myocarditis patients.
Biomarkers that indicate myocardial injury were not only used in the clinical diagnosis of myocarditis,2,40 but also were frequently mentioned in the prognosis of myocarditis. Study from Ekstrom et al41 and Okura et al42 found that elevated NT-proBNP and cardiac troponin, and reduced LVEF were predictors of a poor prognosis in patients with giant cell myocarditis. Decrease in hs-cTnI within 24h was also found to be associated with in-hospital mortality of FM patients.43 Hs-cTnI is widely recognized as a biomarker for myocardial injury in clinical practice. Although, in our study, there was significant difference in hs-cTnI between patients who developed chronic persistent myocarditis and those who did not, it remains unsignificant in multivariate cox analysis. Instead, another biomarker suggesting myocardial injury, LDH, was found significant in both univariate and multivariate analysis, indicating that LDH may be a more sensitive prognostic biomarker than troponin in FM. LDH is an enzyme that catalyzes the conversion between lactic acid and pyruvate and may have proinflammatory or anti-inflammatory effects in different pathophysiological environments.44 It was wildly detected high level in acute myocarditis patients45 and animals.46,47 Lei et al48 and Xu et al49 reported that LDH as the risk factor for severe immune checkpoint inhibitor-induced myocarditis compared with the mild one. In the study of Stasa et al,50 LDH > 1780 mmol/l was regarded as the cutoff value for pediatric acute myocarditis to develop DCM, with larger specificity than CK, CK-MB and AST. However, they found no statistically significant difference in LDH levels observed in the univariate cox analysis between the patients who developed DCM and those who did not. Our results found LDH > 577.0 U/L a potential risk factor for occurrence of chronic persistent myocarditis in adult patients with FM. Elevated LDH levels at admission may indicate the need for enhanced post-discharge monitoring and care for patients with FM. Continuous monitoring of LDH during follow-up may provide clinicians with reliable reference information regarding disease progression and recovery, thereby facilitating more informed clinical decision-making.
Limitation
This study has several limitations. First, as a retrospective study, it inherently lacks the ability to establish a definitive causal relationship between the potential impact factors and the observed outcomes. Our findings suggest that time from onset to admission and LDH may serve as potential predictors of chronic persistent myocarditis in patients with FM. However, causal inferences cannot be drawn, and these findings require validation in prospective studies. Secondly, the small sample size limits the statistical power of the analysis, making it challenging to detect subtle differences or small effects within the population. This increases the risk of Type II errors and may lead to biased results, ultimately undermining the study’s overall robustness and reliability. Furthermore, the study’s follow-up period of only 24 months may be insufficient to fully capture the long-term progression of myocarditis, potentially resulting in an incomplete assessment of its long-term prognosis. Large scale studies were needed. Thirdly, only 54.9% of the participants were diagnosed with myocarditis through EMB, which is the gold standard for confirming myocarditis. The remaining participants were diagnosed using CMR, which may introduce misclassification bias. Last, we determined the time from onset to admission based on the initial occurrence of clinical symptoms as described in the patient’s chief complaint. However, individual differences in symptom perception, such as variations in pain sensitivity, and variations in pathogen incubation periods may introduce unavoidable random errors into our measurements of the time from onset to admission.
Conclusion
About 24.4% of the patients with fulminant myocarditis treated based on the life support measures proposed in the consensus of the Chinese Society of Cardiology have been observed the occurrence chronic persistent myocarditis. Time from onset to admission over 6 days and LDH >577.0 U/L at admission may be risk factors from FM to chronic persistent myocarditis in adult patients.
Abbreviations
FM, Fulminant myocarditis; K-M, Kaplan-Meier; EMB, Endomyocardial biopsy; MCS, Mechanical circulatory support; HTx, heart transplantation; CMR, Cardiac magnetic resonance; IABP, Intra-aortic balloon pump; ECMO, Extracorporeal membrane oxygenation; CRRT, Continuous renal replacement therapy; IVIG, intravenous immunoglobulin; DCM, Dilated cardiomyopathy.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due reason why data are not public but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study has received approval from the Research Ethics Commissions of Tongji Hospital Tongji Medical College of Huazhong University of Science and Technology (TJ-C20160202). The Executive Committee planned and oversaw the study’s execution as well as its data analysis. Following the guidelines set out by the International Conference on Harmonization of Guidelines for Good Clinical Practice51 and the Declaration of Helsinki,52 all procedures and methodologies underwent ethical review and approval by local ethics committees.
Consent for Publication
As this is a retrospective study using de-identified data, the Institutional Review Board did not require patient consent.
Acknowledgments
The authors thank to the participating subjects and follow-up staff for their valuable assistance in this study. Additionally, the authors acknowledge Minda Hospital of Hubei Minzu University for providing the subjects.
Author Contributions
All authors made substantial contributions to the work, including the conception, study design, execution, data acquisition, analysis, or interpretation. They were involved in drafting, revising, or critically reviewing the manuscript, approved the final version for publication, agreed on the journal for submission, and take full responsibility for all aspects of the work.
Funding
Open access publication fees were funded by the Tongji Hospital affiliated to Huazhong University of Science and Technology, and there were no other sources of funding.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Ammirati E, Frigerio M, Adler ED, et al. Management of acute myocarditis and chronic inflammatory cardiomyopathy: an expert consensus document. Circ Heart Fail. 2020;13(11):e007405. doi:10.1161/CIRCHEARTFAILURE.120.007405
2. Ammirati E, Veronese G, Cipriani M, et al. Acute and fulminant myocarditis: a pragmatic clinical approach to diagnosis and treatment. Curr Cardiol Rep. 2018;20(11):114. doi:10.1007/s11886-018-1054-z
3. Nagai T, Inomata T, Kohno T, et al. JCS 2023 guideline on the diagnosis and treatment of myocarditis. Circ J. 2023;87(5):674–754. doi:10.1253/circj.CJ-22-0696
4. Kanaoka K, Onoue K, Terasaki S, et al. Features and outcomes of histologically proven myocarditis with fulminant presentation. Circulation. 2022;146(19):1425–1433. doi:10.1161/CIRCULATIONAHA.121.058869
5. Li S, Xu S, Li C, et al. A life support-based comprehensive treatment regimen dramatically lowers the in-hospital mortality of patients with fulminant myocarditis: a multiple center study. Sci China Life Sci. 2019;62(3):369–380. doi:10.1007/s11427-018-9501-9
6. McCarthy RE 3rd, Boehmer JP, Hruban RH, et al. Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med. 2000;342(10):690–695. doi:10.1056/NEJM200003093421003
7. Hang W, Chen C, Seubert JM, Wang DW. Fulminant myocarditis: a comprehensive review from etiology to treatments and outcomes. Signal Transduct Target Ther. 2020;5(1):287. doi:10.1038/s41392-020-00360-y
8. Ammirati E, Veronese G, Brambatti M, et al. Fulminant versus acute nonfulminant myocarditis in patients with left ventricular systolic dysfunction. J Am Coll Cardiol. 2019;74(3):299–311. doi:10.1016/j.jacc.2019.04.063
9. Kondo T, Okumura T, Shibata N, et al. Differences in prognosis and cardiac function according to required percutaneous mechanical circulatory support and histological findings in patients with fulminant myocarditis: insights from the CHANGE PUMP 2 study. J Am Heart Assoc. 2022;11(4):e023719. doi:10.1161/JAHA.121.023719
10. Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European society of cardiology working group on myocardial and pericardial diseases. Eur Heart J. 2013;34(33):2636–48,48a–48d. doi:10.1093/eurheartj/eht210
11. Ammirati E, Cipriani M, Lilliu M, et al. Survival and left ventricular function changes in fulminant versus nonfulminant acute myocarditis. Circulation. 2017;136(6):529–545. doi:10.1161/CIRCULATIONAHA.117.026386
12. Porcari A, Baggio C, Fabris E, et al. Endomyocardial biopsy in the clinical context: current indications and challenging scenarios. Heart Fail Rev. 2023;28(1):123–135. doi:10.1007/s10741-022-10247-5
13. Aretz HT, Billingham ME, Edwards WD, et al. Myocarditis. A histopathologic definition and classification. Am J Cardiovasc Pathol. 1987;1(1):3–14.
14. Grigoratos C, Di Bella G, Aquaro GD. Diagnostic and prognostic role of cardiac magnetic resonance in acute myocarditis. Heart Fail Rev. 2019;24(1):81–90. doi:10.1007/s10741-018-9724-x
15. Jiang J, Shu H, Wang DW, et al.; Chinese Society of Cardiology CMAWG. Chinese society of cardiology guidelines on the diagnosis and treatment of adult fulminant myocarditis. Sci China Life Sci. 2024;2024:1.
16. Huang F, Ammirati E, Ponnaiah M, et al. Fulminant myocarditis proven by early biopsy and outcomes. Eur Heart J. 2023;44(48):5110–5124. doi:10.1093/eurheartj/ehad707
17. Pollack A, Kontorovich AR, Fuster V, Dec GW. Viral myocarditis--diagnosis, treatment options, and current controversies. Nat Rev Cardiol. 2015;12(11):670–680. doi:10.1038/nrcardio.2015.108
18. Bearse M, Hung YP, Krauson AJ, et al. Factors associated with myocardial SARS-CoV-2 infection, myocarditis, and cardiac inflammation in patients with COVID-19. Mod Pathol. 2021;34(7):1345–1357. doi:10.1038/s41379-021-00790-1
19. Kuhl U, Pauschinger M, Seeberg B, et al. Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation. 2005;112(13):1965–1970. doi:10.1161/CIRCULATIONAHA.105.548156
20. Kuhl U, Pauschinger M, Schwimmbeck PL, et al. Interferon-beta treatment eliminates cardiotropic viruses and improves left ventricular function in patients with myocardial persistence of viral genomes and left ventricular dysfunction. Circulation. 2003;107(22):2793–2798. doi:10.1161/01.CIR.0000072766.67150.51
21. Carlquist JF, Ward RH, Husebye D, Feolo M, Anderson JL. Major histocompatibility complex class II gene frequencies by serologic and deoxyribonucleic acid genomic typing in idiopathic dilated cardiomyopathy. Am J Cardiol. 1994;74(9):918–920. doi:10.1016/0002-9149(94)90586-X
22. Liu W, Li WM, Yang SS, et al. Association of HLA class II DRB1, DPA1 and DPB1 polymorphism with genetic susceptibility to idiopathic dilated cardiomyopathy in Chinese Han nationality. Autoimmunity. 2006;39(6):461–467. doi:10.1080/08916930600893709
23. Tchilian EZ, Gil J, Navarro ML, et al. Unusual case presentations associated with the CD45 C77G polymorphism. Clin Exp Immunol. 2006;146(3):448–454. doi:10.1111/j.1365-2249.2006.03230.x
24. Gorbea C, Makar KA, Pauschinger M, et al. A role for Toll-like receptor 3 variants in host susceptibility to enteroviral myocarditis and dilated cardiomyopathy. J Biol Chem. 2010;285(30):23208–23223. doi:10.1074/jbc.M109.047464
25. Rahnefeld A, Klingel K, Schuermann A, et al. Ubiquitin-like protein ISG15 (interferon-stimulated gene of 15 kDa) in host defense against heart failure in a mouse model of virus-induced cardiomyopathy. Circulation. 2014;130(18):1589–+. doi:10.1161/CIRCULATIONAHA.114.009847
26. Fang ML, Zhang A, Du Y, et al. TRIM18 is a critical regulator of viral myocarditis and organ inflammation. J Biomed Sci. 2022;29(1). doi:10.1186/s12929-022-00840-z.
27. Poller W, Kuhl U, Tschoepe C, Pauschinger M, Fechner H, Schultheiss HP. Genome-environment interactions in the molecular pathogenesis of dilated cardiomyopathy. J Mol Med. 2005;83(8):579–586. doi:10.1007/s00109-005-0664-2
28. Barin JG, Rose NR, Cihakova D. Macrophage diversity in cardiac inflammation: a review. Immunobiology. 2012;217(5):468–475. doi:10.1016/j.imbio.2011.06.009
29. Jensen LD, Marchant DJ. Emerging pharmacologic targets and treatments for myocarditis. Pharmacol Ther. 2016;161:40–51. doi:10.1016/j.pharmthera.2016.03.006
30. Myers JM, Cooper LT, Kem DC, et al. Cardiac myosin-Th17 responses promote heart failure in human myocarditis. JCI Insight. 2016;1(9). doi:10.1172/jci.insight.85851.
31. Huber SA, Feldman AM, Sartini D. Coxsackievirus B3 induces T regulatory cells, which inhibit cardiomyopathy in tumor necrosis factor-alpha transgenic mice. Circ Res. 2006;99(10):1109–1116. doi:10.1161/01.RES.0000249405.13536.49
32. Toldo S, Abbate A. The role of the NLRP3 inflammasome and pyroptosis in cardiovascular diseases. Nat Rev Cardiol. 2024;21(4):219–237. doi:10.1038/s41569-023-00946-3
33. Fairweather D, Kaya Z, Shellam GR, Lawson CM, Rose NR. From infection to autoimmunity. J Autoimmun. 2001;16(3):175–186. doi:10.1006/jaut.2000.0492
34. Fairweather D, Frisancho-Kiss S, Rose NR. Viruses as adjuvants for autoimmunity: evidence from Coxsackievirus-induced myocarditis. Rev Med Virol. 2005;15(1):17–27. doi:10.1002/rmv.445
35. Shi Y, Fukuoka M, Li G, et al. Regulatory T cells protect mice against coxsackievirus-induced myocarditis through the transforming growth factor beta-coxsackie-adenovirus receptor pathway. Circulation. 2010;121(24):2624–2634. doi:10.1161/CIRCULATIONAHA.109.893248
36. Blyszczuk P, Muller-Edenborn B, Valenta T, et al. Transforming growth factor-beta-dependent Wnt secretion controls myofibroblast formation and myocardial fibrosis progression in experimental autoimmune myocarditis. Eur Heart J. 2017;38(18):1413–1425. doi:10.1093/eurheartj/ehw116
37. Hsiao JF, Koshino Y, Bonnichsen CR, et al. Speckle tracking echocardiography in acute myocarditis. Int J Cardiovasc Imaging. 2013;29(2):275–284. doi:10.1007/s10554-012-0085-6
38. Caspar T, Fichot M, Ohana M, El Ghannudi S, Morel O, Ohlmann P. Late detection of left ventricular dysfunction using two-dimensional and three-dimensional speckle-tracking echocardiography in patients with history of nonsevere acute myocarditis. J Am Soc Echocardiogr. 2017;30(8):756–762. doi:10.1016/j.echo.2017.04.002
39. Lee JW, Jeong YJ, Lee G, et al. Predictive value of cardiac magnetic resonance imaging-derived myocardial strain for poor outcomes in patients with acute myocarditis. Korean J Radiol. 2017;18(4):643–654. doi:10.3348/kjr.2017.18.4.643
40. Scicchitano P, Grazioli Gauthier L, D’Agostino C, et al. The diagnosis of acute myocarditis in emergency (DAME) score: improving diagnostics within the emergency department. Eur J Intern Med. 2021;85:56–62. doi:10.1016/j.ejim.2021.01.011
41. Ekstrom K, Lehtonen J, Kandolin R, Raisanen-Sokolowski A, Salmenkivi K, Kupari M. Long-term outcome and its predictors in giant cell myocarditis. Eur J Heart Fail. 2016;18(12):1452–1458. doi:10.1002/ejhf.606
42. Okura Y, Dec GW, Hare JM, et al. A clinical and histopathologic comparison of cardiac sarcoidosis and idiopathic giant cell myocarditis. J Am Coll Cardiol. 2003;41(2):322–329. doi:10.1016/S0735-1097(02)02715-8
43. Liu C, Wang Z, Chen K, et al. The absolute and relative changes in high-sensitivity cardiac troponin I are associated with the in-hospital mortality of patients with fulminant myocarditis. BMC Cardiovasc Disord. 2021;21(1):571. doi:10.1186/s12872-021-02386-8
44. Certo M, Tsai CH, Pucino V, Ho PC, Mauro C. Lactate modulation of immune responses in inflammatory versus tumour microenvironments. Nat Rev Immunol. 2021;21(3):151–161. doi:10.1038/s41577-020-0406-2
45. Du Q, Yu J, Chen Q, et al. Clinical characteristics and influencing factors of severe fever with thrombocytopenia syndrome complicated by viral myocarditis: a retrospective study. BMC Infect Dis. 2024;24(1):240. doi:10.1186/s12879-024-09096-4
46. Wang YF, Wang XY, Ren Z, et al. Phyllaemblicin B inhibits Coxsackie virus B3 induced apoptosis and myocarditis. Antiviral Res. 2009;84(2):150–158. doi:10.1016/j.antiviral.2009.08.004
47. Gou W, Zhang Z, Yang C, Li Y. MiR-223/Pknox1 axis protects mice from CVB3-induced viral myocarditis by modulating macrophage polarization. Exp Cell Res. 2018;366(1):41–48. doi:10.1016/j.yexcr.2018.03.004
48. Lei Y, Zheng X, Huang Q, Li X, Qiu M, Liu M. Intrinsic differences in immune checkpoint inhibitor-induced myocarditis: a retrospective analysis of real world data. Front Pharmacol. 2022;13:914928. doi:10.3389/fphar.2022.914928
49. Xu L, Xu M, Sun W, Zhang W, Song Z. Clinical characteristics and prognostic impact of immune checkpoint inhibitor-associated myocarditis in advanced non-small cell lung cancer. Invest New Drugs. 2023;41(6):816–824. doi:10.1007/s10637-023-01400-4
50. Krasic S, Prijic S, Ninic S, et al. Could the unfortunate outcome of pediatric acute myocarditis be predicted? Factors contributing to a poor outcome in myocarditis. Rev Port Cardiol. 2021;40(9):631–638. doi:10.1016/j.repc.2020.10.015
51. Dixon JR Jr. The international conference on harmonization good clinical practice guideline. Qual Assur. 1998;6(2):65–74. doi:10.1080/105294199277860
52. Human D. Declaration of Helsinki. Lancet. 2001;357(9251):236. doi:10.1016/S0140-6736(05)71342-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.