Back to Journals » Infection and Drug Resistance » Volume 15
Lack of Correlation Between Soluble Angiotensin-Converting Enzyme 2 and Inflammatory Markers in Hospitalized COVID-19 Patients with Hypertension
Authors Louisa M ![]() , Cahyadi D, Nilasari D, Soetikno V
, Cahyadi D, Nilasari D, Soetikno V
Received 14 April 2022
Accepted for publication 10 August 2022
Published 24 August 2022 Volume 2022:15 Pages 4799—4807
DOI https://doi.org/10.2147/IDR.S369771
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Melva Louisa,1 Daniel Cahyadi,2 Dina Nilasari,3,4 Vivian Soetikno1
1Department of Pharmacology and Therapeutics, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 2Master Program in Biomedical Sciences, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 3Department of Clinical Research, Siloam Hospitals, Jakarta, Indonesia; 4Faculty of Medicine, University of Hasanuddin, Makassar, South Sulawesi, Indonesia
Correspondence: Melva Louisa, Department of Pharmacology and Therapeutics Faculty of Medicine Universitas Indonesia, Jl. Salemba Raya No. 6, Jakarta Pusat, Jakarta, Indonesia, Tel +62-21-319 30481, Email [email protected]
Purpose: This study aimed to investigate the correlation of plasma soluble angiotensin-converting enzyme 2, sACE2, and several inflammatory markers in COVID-19 patients requiring hospitalization with hypertension. Additionally, we analyzed the effects of renin-angiotensin-aldosterone-system, RAAS, inhibitors on the levels of sACE2 and inflammatory marker levels in patients with COVID-19.
Patients and Methods: This cross-sectional study involved patients with COVID-19 who required hospitalization on a stable dose of antihypertensive drugs. The study included three hospitals in Jakarta and Tangerang, Indonesia, between December 2020 and June 2021. We classified eligible subjects into two groups: patients with COVID-19 treated with antihypertensive RAAS inhibitors or non-RAAS inhibitors.
Results: We found no correlation between sACE2 and all the inflammatory and coagulation markers studied (high-sensitivity C-reactive protein, IL-6, IL-10, IL6/IL10, tumor necrosis factor-α, neutrophil-to-lymphocyte ratio, and D-dimer) in COVID-19 patients with hypertension. Further analysis showed lower sACE2 concentrations and IL-6/IL-10 ratio in patients treated with RAAS inhibitors vs those treated with non-RAAS inhibitors.
Conclusion: We found no correlation between ACE2 and inflammatory markers. Using RAAS inhibitors resulted in a lower sACE2 and IL-6/IL-10 ratio. The type of antihypertensive treatments has a neutral effect on disease severity and outcome in COVID-19 patients with hypertension. However, to firmly-established these effects, our findings should be confirmed in a much larger population.
Keywords: antihypertensive drugs, cytokines, interleukins, neutrophil-to-lymphocyte ratio, renin-angiotensin-aldosterone system inhibitors
Introduction
The coronavirus disease 2019 (COVID-19) outbreak, caused by SARS-CoV-2, has infected more than 560 million people worldwide.1 People with comorbidities such as hypertension, diabetes mellitus (DM), chronic kidney diseases, or any other significant illnesses are at greater risk of COVID-19 and have been linked to a more severe illness.2–5 Based on the evidence that SARS-COV-2 spike (S) protein attaches to angiotensin-converting-enzyme 2 receptor as the mode of entry to human cells, controversies are ongoing regarding its correlation with hypertension and the use of renin-angiotensin-aldosterone inhibitors.6
Membrane-bound angiotensin-converting enzyme 2, ACE2, is found in an enzyme that controls blood pressure homeostasis by interacting with the renin-angiotensin-aldosterone system, RAAS activation. ACE2 acts in the degradation process of Ang II by cleaving angiotensin into Angiotensin (1–7), Ang (1–7). ACE/Ang II/Ang II receptor type 2 (AT1R) promotes vasoconstriction and pro-thrombosis effects, whereas ACE/Ang (1–7)/MasR has the opposite impact on the cardiovascular system.7,8 As a membrane-bound enzyme, the extracellular part of ACE2 is shed into the plasma by a protease known as sheddase. Thus, ACE2 in soluble form is detectable at low levels in the bloodstream.9,10
Angiotensin-converting enzyme inhibitors, ACEIs, and angiotensin II receptor blockers, ARBs, have been demonstrated to increase the level of soluble angiotensin-converting enzyme 2, sACE2, raising concerns about their potential risk of increasing disease severity.6,11 Concurrently, SARS- CoV-2ʹs attachment to the ACE2 receptor causes sACE2 to accumulate in the blood and urine, triggering a cytokine storm that releases interleukin-6, IL-6, from the host macrophage. These occurrences lead to hypercoagulation, increased morbidity, and poor survival rates in severely ill patients with COVID-19.12,13
Observational studies and two recent clinical trials have suggested that using RAAS inhibitors did not increase disease severity or death.14–18 However, other extensive studies have shown that patients with COVID-19 who received ACEIs or ARBs were more likely to have better clinical outcomes than those who used other antihypertensive drugs.19,20
Studies continue to examine the mechanisms of COVID-19 and the contributions of ACE2, disease manifestations, organ damage, and mortality and morbidity.11,21 In their previous study, Lundstrom et al demonstrated that the level of sACE2 in patients with COVID-19 was increased and correlated with several markers of inflammation.22 Additionally, in a study by Wu in patients with COVID-19 with hypertension, treatment with ACEI/ARB resulted in lower inflammatory and organ damage markers.19 Taken together, we suggested that the variable results of clinical outcomes in patients with hypertension are related to the levels of sACE2 and related inflammatory markers. Thus, we aimed to study the correlations between the levels of sACE2 with inflammatory markers and disease severity in hypertensive COVID-19 patients requiring hospitalizations.
Materials and Methods
Study Design, Period, and Setting
This cross-sectional study was conducted in three Siloam Hospitals in Jakarta and Tangerang, Indonesia, between December 2020 and June 2021. RT-PCR confirmed the diagnosis of COVID-19 in patients who required hospitalization with a stable dose of antihypertensive drugs. Ethical approval was obtained from the Ethics Committee of the Faculty of Medicine Universitas Indonesia (no KET-926/UN2.F1/ETIK/PPM.00.02/2020). This study was conducted in full compliance with the Declaration of Helsinki, which was mandatory for all clinical research submitted to Ethics Committee in our institution. All patients provided informed consent before participating in the study.
Population and Sample
The sample size was calculated based on the correlation,23 which was expected to be 0.43 between sACE2 and inflammatory markers.22 Type I error (α two-sided) was set at 0.05, whereas type II error (β) was 0.2. The result of the sample size calculation was 40.
We included adult patients with RT-PCR confirmed COVID-19 requiring hospitalizations with hypertension. Patients were required to undergo treatment with a stable dose of antihypertensive drugs for a minimum of 1 month. Exclusion criteria include pregnant and nursing mothers, patients with morbid obesity, on treatment with anti-inflammatory drugs such as corticosteroids/chloroquine/hydroxychloroquine/monoclonal antibody, history of chronic kidney disease or malignancy, COVID-19-vaccinated individuals, and resistant hypertension. Blood samples and routine hematology were drawn from eligible patients to quantify the levels of sACE2, hs-CRP, TNF-α, IL-6, IL-10, and interferon-γ, IFN-γ.
Variables
Soluble ACE2 and hs-CRP were quantified using an enzyme-linked immunosorbent assay (ELISA) (CusabioTM, Houston, Texas, USA). Levels of IL-6, IL-10, TNF-α, and IFN-γ were quantified using LuminexTM instruments with antibody panels from R&D systems (Minneapolis, USA). Collected patient data included routine examinations, such as hemoglobin, hematocrit, lymphocytes, platelets, neutrophils, neutrophil-to-lymphocyte ratio, NLR, and D-dimer.
Data Collection
We collected demographic data from available medical records, including age, sex, comorbidities, and medication history. COVID-19 severity was determined based on the Management of COVID-19 Protocol released by the Ministry of the Health Republic of Indonesia.
Statistical Analysis
Correlations between plasma sACE2 concentrations and inflammatory, coagulation, liver, and kidney function markers were analyzed using Spearman correlation coefficient. Independent t-tests were used to identify significant differences between patients treated with RAAS and those treated with non-RAAS inhibitors. A P-value of <0.05 is regarded as statistically significant.
Results
Patient Characteristics
The mean age of the patients recruited was 57.3 years in mild to moderate cases. All patients were on a stable dose of antihypertensives, and most were diagnosed for more than 1 year. Most admitted patients had clinical symptoms of fever and cough; 12/40 patients had dyspnea, and 9/40 patients had low oxygen saturation. Both groups had similar lengths of hospital stay, and all patients were discharged with clinical improvements or complete recovery (Table 1). Of the 40 patients, 25 were on a stable dose of RAAS inhibitors (ACEIs or ARBs), whereas 15 were on a stable dose of calcium channel blockers.
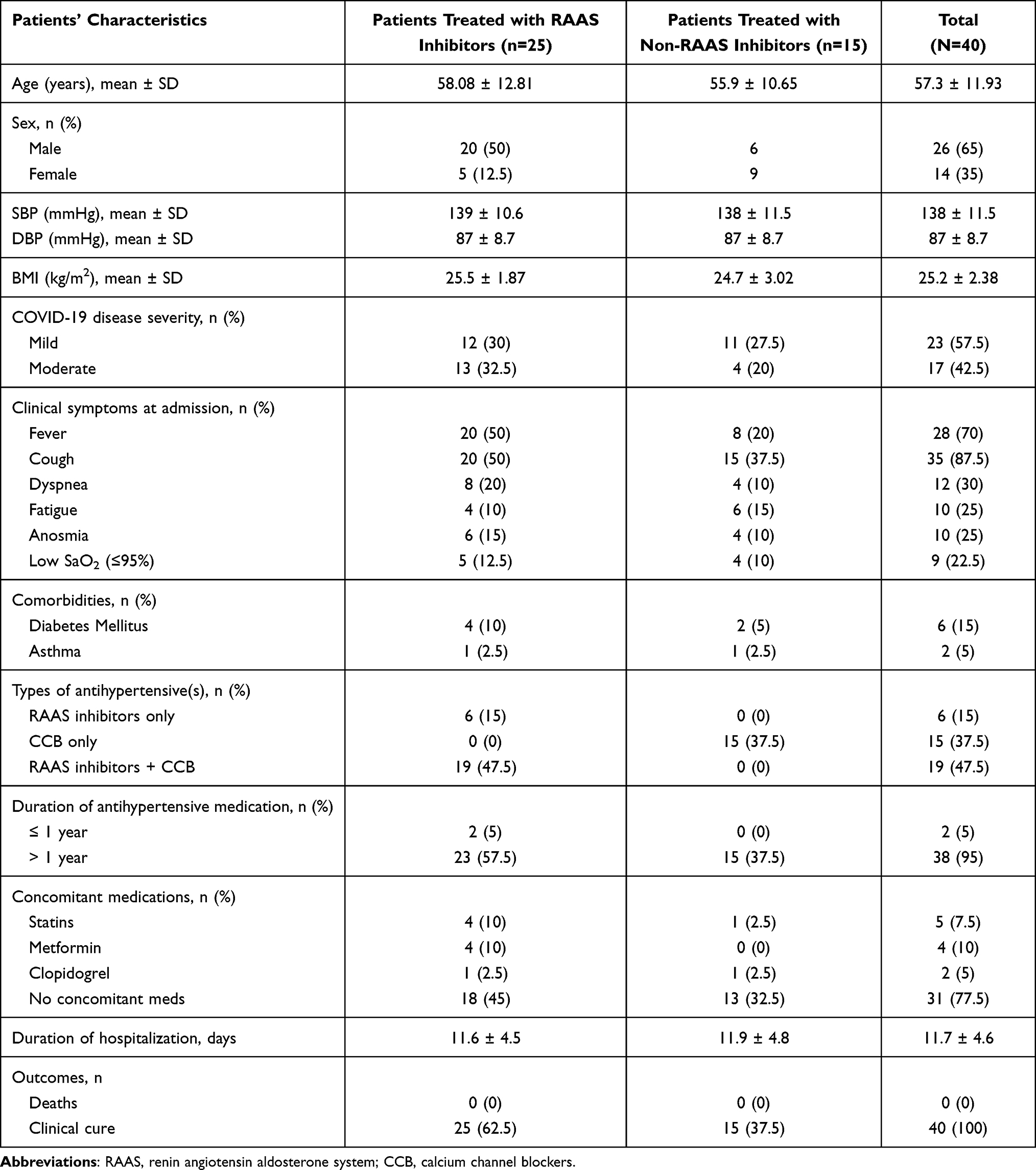 |
Table 1 Patients’ Characteristics (N = 40) Upon Hospital Admission |
Lack of Correlation Between sACE2 Concentrations and Inflammation and Coagulation Markers
We analyzed the correlation between the concentrations of sACE2 in patients and several markers of interest, including inflammatory cytokines, kidney function, and liver function markers. None of the 12 markers studied was correlated with sACE2 concentrations (Table 2).
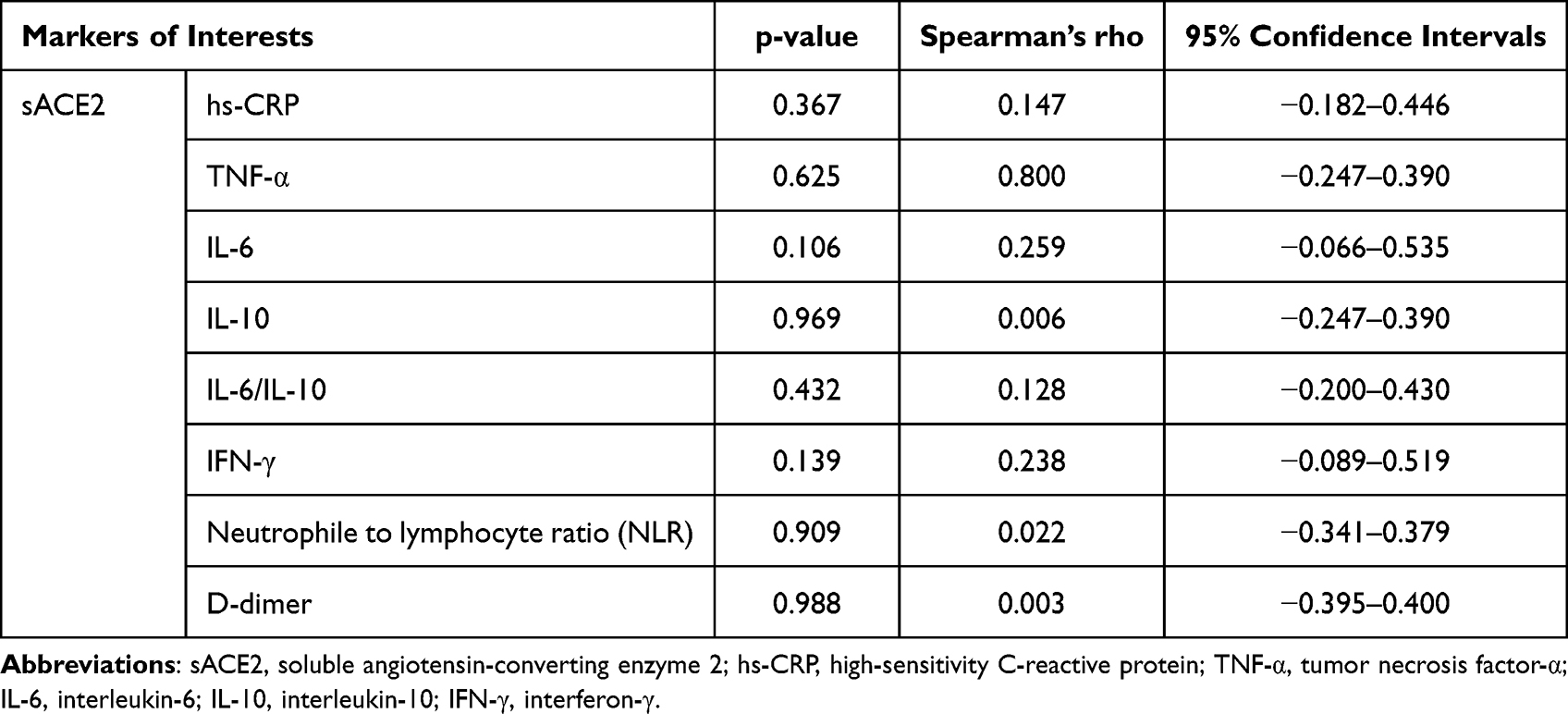 |
Table 2 Correlation Analysis Between sACE2 Inflammatory and Coagulation Markers |
Lower sACE2 Concentrations and IL-6/IL-10 Ratio in Hypertensive COVID-19 Patients Treated with RAAS Inhibitors
We found significantly higher sACE2 concentrations in COVID-19 patients with hypertension treated with non-RAAS inhibitors than those treated with RAAS inhibitors (Table 3). Despite the lower sACE2 concentrations in patients treated with RAAS inhibitors, we found no differences in pro-inflammatory markers (hs-CRP, TNF-α, IL-6, NLR, and IFN-γ). However, there were marked differences in the anti-inflammatory cytokine concentrations, IL-10, and a lower ratio of IL-6/IL-10 between the two groups. Similar hematologic markers were also observed in the two groups (Table 3).
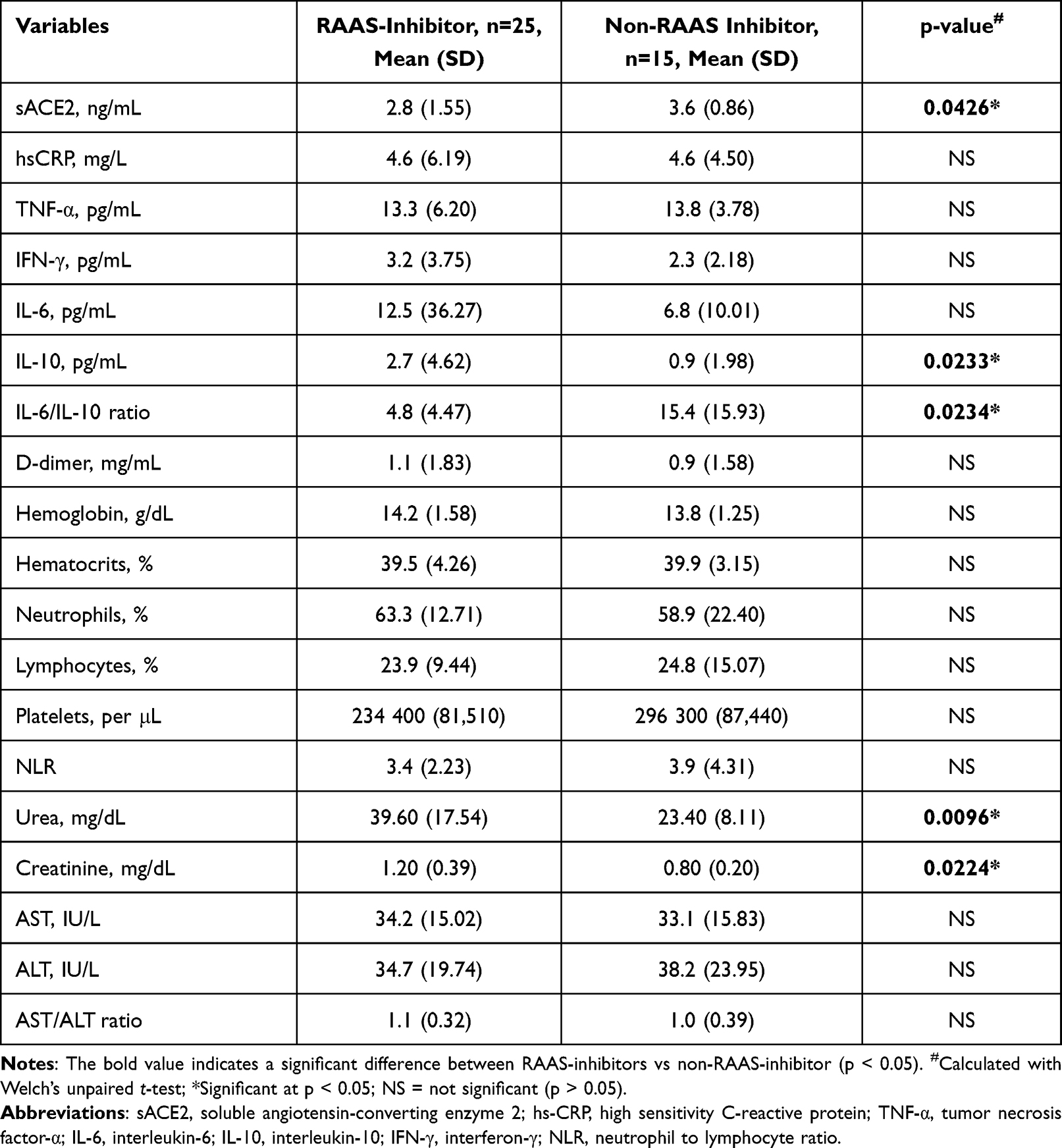 |
Table 3 Soluble ACE2 and Inflammation, Coagulation, and Hematology Markers in COVID-19 Hypertensive Patients Given RAAS-Inhibitors and Non-RAAS Inhibitors |
Discussion
The findings of this study are consistent with previous studies that revealed that RAAS inhibitor use does not result in increased inflammation and disease severity.14–18 Our results also confirmed that the antihypertensive drugs used by patients with COVID-19, RAAS inhibitors, or non-RAAS inhibitors have a neutral effect on the disease severity and hospitalization duration.
In a previous study of severely ill patients with COVID-19 requiring ICU treatment, cytokines, chemokines, and regulatory proteins were elevated. Among those highly increased were CRP, IL-6, TNF-α, IFN-α, IFN-γ, and ferritin, all elevated in the blood of patients who need admission to ICUs due to the cytokine storm.24
In earlier studies, both SARS-COV and SARS-COV-2 infectivity were reduced by high sACE2 levels.25,26 The studies had suggested that high sACE2 levels might inhibit secondary viral establishment in the event of a viral infection.25,26 ACE2 was long considered an interferon-stimulated gene based on its inducible expression in cells treated with interferons or infected with viruses that trigger IFN responses, such as influenza. Therefore, increased ACE2, a tissue-protective mediator following lung damage, may be exploited by SARS-CoV-2 to promote infection.27
Our study did not discover any correlation between the concentration of sACE2 with IFN-γ and several markers of inflammation. Osman et al might explain our results, which proved a modulatory activity in the expressions of ACE2, sACE2, and Ang (1–7) in patients with COVID-19. They showed that ACE2 expression and Ang II plasma levels might vary in SARS-CoV-2-infected individuals. Patients with COVID-19 had lower levels of ACE2 mRNA in their blood cells than healthy individuals. The deregulation of the ACE2 gene caused the decreased production of membrane ACE2 protein. Osman et al also discovered a greater quantity of Ang II and Ang I in the plasma of long-term viral shedders. Even when Ang (1–7) plasma levels were almost constant in long-term shedders, they were inadequate to counteract the negative consequences of Ang II increase.28 Additionally, a study by Onabajo et al proved that changes in the ACE2 isoform produced by the interferons-induced gene caused by SARS-COV2 are shortened. The new, truncated version of ACE2, designated by Onabajo et al as dACE2, was the type of ACE2 that increased IFNs and viruses.29 Further, the hypothesis by researchers displayed the importance of ACE/ACE2 balance that may explain some of the comorbidities that contribute to the severity in patients with COVID-19.30,31 Thus, measurement of sACE2 alone might not give the complete picture of the expressions of ACE2-related genes in COVID-19 patients with hypertension.
Our results agreed with findings by Lundstrom et al in hospitalized patients with COVID-19, and their findings also showed no correlations between sACE2 and the levels of interleukins and TNF-α. Lundstrom et al argued that the absence of correlation between sACE2 with markers of inflammation was caused by the variability in the number of patient’s risk factors and the overall comorbidities.22 In contrast, in our study, only 20% of patients had other comorbidities. Thus, our results were slightly affected by other comorbidities. Notably, none of the participants in our research received any corticosteroids or COVID-19 vaccination throughout the observation. Thus, the status of inflammatory markers in our study was not affected by corticosteroids and vaccines.
Despite the lack of statistical significance of sACE2 correlation with TNF-α, Spearman’s rho was 0.800, possibly due to the limited sample in this study. TNF-α is the main pro-inflammatory cytokine that acts as a connection between inflammation and RAAS.12 Although not statistically significant, this study found higher TNF-α levels in patients treated with non-RAAS inhibitors, possibly because upon the binding of Ang II to AT1R, a signal forms and triggers immune cells such as macrophages and T-cells to produce IFN-γ, which then stimulates the release of TNF-α. Increased sACE2 will convert Ang II to Ang (1–7) and block the interaction of Ang II with the AT1R.32 In patients treated with non-RAAS inhibitors, the inhibition of Ang II does not occur, so it can still bind to its receptors and produce inflammatory cytokines. Increased inflammatory cytokines are associated with activation of the coagulation system, which is a typical response in patients with COVID-19.11,22
In the present study, the patients treated with RAAS inhibitors significantly decreased sACE2 levels. Studies have shown that ACE2 modulates the RAAS to regulate tissue microcirculation and inflammation.33,34 We also found higher concentrations of the pro-inflammatory cytokine IL-6 in patients treated with RAAS inhibitors. The ACE2 and IL-6 genes have been identified as non-canonical interferon-stimulated genes, ISGs, due to their unusual reactions to interferons and inflammatory stimuli through an epigenetic cascade.35 A study of epithelial cells demonstrated that in the presence of SARS-CoV-2 spike protein, IL-6 signaling was started via AT1 axis activation to commence coordination of a hyper-inflammatory response.36
However, the higher concentrations of IL-6 were counterbalanced by the higher concentrations of the anti-inflammatory cytokine, IL-10. Subsequently, we found a marked reduction in the ratio of IL-6/IL-10 in patients treated with RAAS inhibitors.
Several significant clinical findings in COVID-19 were that patients with poor prognoses had increased levels of IL-10 in addition to the two pro-inflammatory cytokines, IL-6 and IL-1β. Given the cytokine’s immunoregulatory capabilities, this might indicate an alarm from the host organism.37 Furthermore, higher IL-10 levels were more closely associated with positive outcomes than higher levels of pro-inflammatory IL-6 and IL-8.38 Hence, studies have inferred that the two cytokine indicators may be better predictors of COVID-19 disease severity compared with IL-6 alone.39,40 Similarly, a recent systematic review and meta-analysis confirmed that IL-6 and IL-10 concentrations, not TNF-α, might better predict the severity and outcomes of patients with COVID-19.41
Our study found no correlations between sACE2 concentrations and D-dimers or NLR. We also did not find any association between D-dimers and NLR in the two groups of patients with different antihypertensive treatments. Our results agreed with Gormez et al’s study of the association between clinical outcomes in patients with COVID-19 using ACEIs or ARBs. Their study showed that NLR and D-dimer concentration were closely linked to the essential outcomes of patients. However, the outcomes were not connected with ACEI/ARB usage.42
Although patients with RAAS inhibitors have lower inflammatory markers of IL-6/IL-10 and NLR, we found that hs-CRP concentrations were similar in both groups. Contrary to our results, Yang et al demonstrated that patients in the ARBs/ACEI group had considerably lower amounts of hs-CRP, followed by a decreased mortality rate; however, these changes were not statistically significant.43 A case series presented by Lee et al also indicated that patients treated with ARBs had reduced CRP following clinical improvement.44
Studies have demonstrated that the level of CRP measured upon admission is a straightforward and independent indicator that could be helpful for the early diagnosis of severity during COVID-19.45,46 Yet; several studies suggested that rather than a single parameter, multiple markers should be used as predictors of severity and mortality in patients with COVID-19.47,48
Regardless of all the above findings, the incomplete knowledge of the association between COVID and ACE2 has led to debates concerning the use of RAAS inhibitors. Our study found no concern regarding the inflammatory markers; we even found a better ratio of IL-6/IL-10 in patients treated with RAAS inhibitors.
Our study has some limitations. We include a limited number of samples due to the strict eligibility criteria. Our study only included patients requiring hospitalization to facilitate blood sampling and confirm RT-PCR results and outcome observations, which would have been challenging to perform in outpatient settings.
Several patients were already subjected to high-dose corticosteroids before informed consent could be obtained. Despite recent recommendations and protocols that do not endorse the use of steroids in mild COVID-19, systemic corticosteroids were commonly used for patients with COVID-19 despite their baseline clinical status in the first year of the pandemic in Indonesia. The use was allowed to address the possibility of hyperinflammatory conditions in patients with comorbidities. At the time, most clinical staff members were almost entirely preoccupied with saving patients’ lives.49 Several studies had also shown that although corticosteroids administered to hospitalized patients with COVID-19 did not improve their clinical state after Day 14, they shortened the amount of time it took for radiological findings to improve for all patients regardless of illness severity.50–52
The commencement of the vaccination program also limited our access to patients. The first vaccination program for health-care providers was ongoing when the study started. At that time, only a limited number of patients had been vaccinated. A study showed that upon vaccination, there was a substantial increase in the levels of the cytokines IL-2, IL-6, and IFN-γ.53,54 Thus, we excluded vaccinated patients to avoid interference with the analysis of inflammatory markers.
Conclusion
In conclusion, in hospitalized COVID-19 patients with hypertension, inflammatory markers, illness severity, and outcome were not associated with the types of antihypertensive medications administered. Patients treated with RAAS inhibitors had a significantly lower sACE2 concentration, thereby improving the IL-6/IL-10 ratio. Considering the limited sample size in this study, our findings should be confirmed in larger populations.
Acknowledgments
The English language review was provided by Enago (www.enago.com). This study was funded by the Grants from PUTI 2020 Contract No. PUTI NKB 1292/UN2.RST/PPM.00.03.01/2020.
Author Contributions
All authors made a substantial contribution to the work presented, whether that is in the idea, design of the study, execution, collection of data, analysis, and interpretation, or in all these areas; they took part in writing, revising, or critically reviewing the article; provided final approval of the paper; agreed on the submission to the journal; and agree to be responsible for all elements of the work.
Disclosure
The authors declare no conflicts of interest regarding this manuscript.
References
1. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int.
2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
3. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. 2020;323(18):1775–1776. doi:10.1001/jama.2020.4683
4. Ng WH, Tipih T, Makoah NA, et al. Comorbidities in SARS-CoV-2 patients: a systematic review and meta-analysis. mBio. 2021;12(1). doi:10.1128/mBio.03647-20
5. Bajgain KT, Badal S, Bajgain BB, Santana MJ. Prevalence of comorbidities among individuals with COVID-19: a rapid review of current literature. Am J Infect Control. 2021;49(2):238–246. doi:10.1016/j.ajic.2020.06.213
6. Saba L, Gerosa C, Fanni D, et al. Molecular pathways triggered by COVID-19 in different organs: ACE2 receptor-expressing cells under attack? A review. Eur Rev Med Pharmacol Sci. 2020;24(23):12609–12622. doi:10.26355/eurrev_202012_24058
7. Tikellis C, Thomas MC. Angiotensin-Converting Enzyme 2 (ACE2) is a key modulator of the renin-angiotensin system in health and disease. Int J Pept. 2012;2012:256294. doi:10.1155/2012/256294
8. Oz M, Lorke DE, Kabbani N. A comprehensive guide to the pharmacologic regulation of angiotensin-converting enzyme 2 (ACE2), the SARS-CoV-2 entry receptor. Pharmacol Ther. 2021;221:107750. doi:10.1016/j.pharmthera.2020.107750
9. Epelman S, Shrestha K, Troughton RW, et al. Soluble angiotensin-converting enzyme 2 in human heart failure: relation with myocardial function and clinical outcomes. J Card Fail. 2009;15(7):565–571. doi:10.1016/j.cardfail.2009.01.014
10. Epelman S, Tang WH, Chen SY, Van Lente F, Francis GS, Sen S. Detection of soluble angiotensin-converting enzyme 2 in heart failure: insights into the endogenous counter-regulatory pathway of the renin-angiotensin-aldosterone system. J Am Coll Cardiol. 2008;52(9):750–754. doi:10.1016/j.jacc.2008.02.088
11. Loganathan S, Kuppusamy M, Wankhar W, et al. Angiotensin-converting enzyme 2 (ACE2): COVID 19 gate way to multiple organ failure syndromes. Respir Physiol Neurobiol. 2021;283:103548. doi:10.1016/j.resp.2020.103548
12. Iwasaki M, Saito J, Zhao H, Sakamoto A, Hirota K, Ma D. Inflammation triggered by SARS-CoV-2 and ACE2 augment drives multiple organ failure of severe COVID-19: molecular mechanisms and implications. Inflammation. 2021;44(1):13–34. doi:10.1007/s10753-020-01337-3
13. Bitker L, Burrell LM. Classic and nonclassic renin-angiotensin systems in the critically Ill. Crit Care Clin. 2019;35(2):213–227. doi:10.1016/j.ccc.2018.11.002
14. Mancia G, Rea F, Ludergnani M, Apolone G, Corrao G. Renin–angiotensin–aldosterone system blockers and the risk of Covid-19. New Engl J Med. 2020;382(25):2431–2440. doi:10.1056/NEJMoa2006923
15. Reynolds HR, Adhikari S, Pulgarin C, et al. Renin–angiotensin–aldosterone system inhibitors and risk of covid-19. New Engl J Med. 2020;382(25):2441–2448. doi:10.1056/NEJMoa2008975
16. Park J, Lee S-H, You SC, Kim J, Yang K. Effect of renin-angiotensin-aldosterone system inhibitors on Covid-19 patients in Korea. PLoS One. 2021;16(3):e0248058. doi:10.1371/journal.pone.0248058
17. Lopes RD, Macedo AVS, de Barros ES, et al. Effect of discontinuing vs. continuing angiotensin-converting enzyme inhibitors and Angiotensin II receptor blockers on days alive and out of the hospital in patients admitted with COVID-19: a Randomized Clinical Trial. JAMA. 2021;325(3):254–264. doi:10.1001/jama.2020.25864
18. Bauer A, Schreinlechner M, Sappler N, et al. Discontinuation versus continuation of renin-angiotensin-system inhibitors in COVID-19 (ACEI-COVID): a prospective, parallel-group, randomized, controlled, open-label trial. Lancet Respir Med. 2021;9(8):863–872. doi:10.1016/S2213-2600(21)00214-9
19. Wu C, Qu G, Wang L, et al. Clinical characteristics and inflammatory immune responses in COVID-19 patients with hypertension: a retrospective study. Front Pharmacol. 2021;12:2333. doi:10.3389/fphar.2021.721769
20. Semenzato L, Botton J, Drouin J, et al. Antihypertensive drugs and COVID-19 risk. Hypertension. 2021;77(3):833–842. doi:10.1161/HYPERTENSIONAHA.120.16314
21. Kumar A, Narayan RK, Prasoon P, et al. COVID-19 mechanisms in the human body-what we know so far. Front Immunol. 2021;12:693938. doi:10.3389/fimmu.2021.693938
22. Lundström A, Ziegler L, Havervall S, et al. Soluble angiotensin-converting enzyme 2 is transiently elevated in COVID-19 and correlates with specific inflammatory and endothelial markers. J Med Virol. 2021;93(10):5908–5916. doi:10.1002/jmv.27144
23. Negida A. Sample size calculation guide - Part 7: how to calculate the sample size based on a correlation. Adv J Emerg Med. 2020;4(2):e34–e34. doi:10.22114/ajem.v0i0.344
24. Olbei M, Hautefort I, Modos D, et al. SARS-CoV-2 causes a different cytokine response compared to other cytokine storm-causing respiratory viruses in severely ill patients. Front Immunol. 2021;12:629193. doi:10.3389/fimmu.2021.629193
25. Hofmann H, Geier M, Marzi A, et al. Susceptibility to SARS coronavirus S protein-driven infection correlates with expression of angiotensin-converting enzyme 2, and infection can be blocked by soluble receptor. Biochem Biophys Res Commun. 2004;319(4):1216–1221. doi:10.1016/j.bbrc.2004.05.114
26. Monteil V, Kwon H, Prado P, et al. Inhibition of SARS-CoV-2 infections in engineered human tissues using clinical-grade soluble human ACE2. Cell. 2020;181(4):905–913.e907. doi:10.1016/j.cell.2020.04.004
27. Ziegler CGK, Allon SJ, Nyquist SK, et al. SARS-CoV-2 receptor ACE2 is an interferon-stimulated gene in human airway epithelial cells and is detected in specific cell subsets across tissues. Cell. 2020;181(5):1016–1035.e1019. doi:10.1016/j.cell.2020.04.035
28. Osman IO, Melenotte C, Brouqui P, et al. Expression of ACE2, soluble ACE2, Angiotensin I, Angiotensin II and Angiotensin-(1–7) is modulated in COVID-19 patients. Front Immunol. 2021;12. doi:10.3389/fimmu.2021.625732
29. Onabajo OO, Banday AR, Stanifer ML, et al. Interferons and viruses induce a novel truncated ACE2 isoform and not the full-length SARS-CoV-2 receptor. Nat Gen. 2020;52(12):1283–1293. doi:10.1038/s41588-020-00731-9
30. Bank S, De SK, Bankura B, Maiti S, Das M. ACE/ACE2 balance might be instrumental to explain the certain comorbidities leading to severe COVID-19 cases. Biosci Rep. 2021;41(2). doi:10.1042/BSR20202014
31. Ferrara F, Vitiello A. Scientific hypothesis for treatment of COVID-19ʹs lung lesions by adjusting ACE/ACE2 imbalance. Cardiovasc Toxicol. 2021;21(6):498–503. doi:10.1007/s12012-021-09649-y
32. Vaduganathan M, Vardeny O, Michel T, McMurray JJV, Pfeffer MA, Solomon SD. Renin-angiotensin-aldosterone system inhibitors in patients with Covid-19. N Engl J Med. 2020;382(17):1653–1659. doi:10.1056/NEJMsr2005760
33. Datta PK, Liu F, Fischer T, Rappaport J, Qin X. SARS-CoV-2 pandemic and research gaps: understanding SARS-CoV-2 interaction with the ACE2 receptor and implications for therapy. Theranostics. 2020;10(16):7448–7464. doi:10.7150/thno.48076
34. Abassi Z, Higazi AAR, Kinaneh S, Armaly Z, Skorecki K, Heyman SN. ACE2, COVID-19 infection, inflammation, and coagulopathy: missing pieces in the puzzle. Front Physiol. 2020;11. doi:10.3389/fphys.2020.574753
35. Sang ER, Tian Y, Miller LC, Sang Y. Epigenetic evolution of ACE2 and IL-6 genes: non-canonical interferon-stimulated genes correlate to COVID-19 susceptibility in vertebrates. Genes. 2021;12(2):154. doi:10.3390/genes12020154
36. Patra T, Meyer K, Geerling L, et al. SARS-CoV-2 spike protein promotes IL-6 trans-signaling by activation of angiotensin II receptor signaling in epithelial cells. PLoS Pathog. 2020;16(12):e1009128. doi:10.1371/journal.ppat.1009128
37. Albini A, Calabrone L, Carlini V, et al. Preliminary evidence for IL-10-induced ACE2 mRNA expression in lung-derived and endothelial cells: implications for SARS-Cov-2 ARDS pathogenesis. Front Immunol. 2021;12. doi:10.3389/fimmu.2021.718136
38. Han H, Ma Q, Li C, et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg Microbes Infect. 2020;9(1):1123–1130. doi:10.1080/22221751.2020.1770129
39. Dhar SK, Damodar S, Gujar S, Das M. IL-6 and IL-10 as predictors of disease severity in COVID-19 patients: results from meta-analysis and regression. Heliyon. 2021;7(2):e06155. doi:10.1016/j.heliyon.2021.e06155
40. Luporini RL, Rodolpho JMA, Kubota LT, et al. IL-6 and IL-10 are associated with disease severity and higher comorbidity in adults with COVID-19. Cytokine. 2021;143:155507. doi:10.1016/j.cyto.2021.155507
41. Udomsinprasert W, Jittikoon J, Sangroongruangsri S, Chaikledkaew U. Circulating levels of Interleukin-6 and Interleukin-10, but not tumor necrosis factor-alpha, as potential biomarkers of severity and mortality for COVID-19: systematic review with meta-analysis. J Clin Immunol. 2021;41(1):11–22. doi:10.1007/s10875-020-00899-z
42. Gormez S, Ekicibasi E, Degirmencioglu A, et al. Association between renin–angiotensin–aldosterone system inhibitor treatment, neutrophil–lymphocyte ratio, D-Dimer and clinical severity of COVID-19 in hospitalized patients: a multicenter, observational study. J Human Hypertens. 2021;35(7):588–597. doi:10.1038/s41371-020-00405-3
43. Yang G, Tan Z, Zhou L, et al. Effects of Angiotensin II receptor blockers and ACE (Angiotensin-Converting Enzyme) inhibitors on virus infection, inflammatory status, and clinical outcomes in patients with COVID-19 and hypertension. Hypertension. 2020;76(1):51–58. doi:10.1161/HYPERTENSIONAHA.120.15143
44. Lee SJ, Kim T, Cho WH, Jeon D, Lim S. Possible benefit of Angiotensin II receptor blockers in COVID-19 patients: a case series. J Renin-Angiotensin-Aldosterone Syst. 2021;2021:9951540. doi:10.1155/2021/9951540
45. Ahnach M, Zbiri S, Nejjari S, Ousti F, Elkettani C. C-reactive protein as an early predictor of COVID-19 severity. J Med Biochem. 2020;39(4):500–507. doi:10.5937/jomb0-27554
46. Sadeghi-Haddad-Zavareh M, Bayani M, Shokri M, et al. C-Reactive protein as a prognostic indicator in COVID-19 patients. Interdiscip Perspect Infect Dis. 2021;2021:5557582. doi:10.1155/2021/5557582
47. Gopalan N, Senthil S, Prabakar NL, et al. Predictors of mortality among hospitalized COVID-19 patients and risk score formulation for prioritizing tertiary care—An experience from South India. PLoS One. 2022;17(2):e0263471. doi:10.1371/journal.pone.0263471
48. de Jong VMT, Rousset RZ, Antonio-Villa NE, et al. Clinical prediction models for mortality in patients with covid-19: external validation and individual participant data meta-analysis. Br Med J. 2022;378:e069881. doi:10.1136/bmj-2021-069881
49. Lim MA, Pranata R. Worrying situation regarding the use of dexamethasone for COVID-19. Ther Adv Respir Dis. 2020;14:1753466620942131. doi:10.1177/1753466620942131
50. El-Saber Batiha G, Al-Gareeb AI, Saad HM, Al-Kuraishy HM. COVID-19 and corticosteroids: a narrative review. Inflammopharmacology. 2022;30(4):1189–1205. doi:10.1007/s10787-022-00987-z
51. Ikeda S, Misumi T, Izumi S, et al. Corticosteroids for hospitalized patients with mild to critically-ill COVID-19: a multicenter, retrospective, propensity score-matched study. Sci Rep. 2021;11(1):10727. doi:10.1038/s41598-021-90246-y
52. Berton AM, Prencipe N, Giordano R, Ghigo E, Grottoli S. Systemic steroids in patients with COVID-19: pros and contras, an endocrinological point of view. J Endocrinol Invest. 2021;44(4):873–875. doi:10.1007/s40618-020-01325-2
53. Souza-Silva GA, Aquino RCA, Sousa GF, et al. Memory elicitation, T-cell response and antibody production: an independent study of an inactivated entire virus vaccine (Coronavac). An Acad Bras Cienc. 2022;94(3):e20211590. doi:10.1590/0001-3765202220211590
54. Szabó GT, Mahiny AJ, Vlatkovic I. COVID-19 mRNA vaccines: platforms and current developments. Mol Ther. 2022;30(5):1850–1868. doi:10.1016/j.ymthe.2022.02.016
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.