Back to Journals » Journal of Pain Research » Volume 15
Knowledge, Practices, and Perceived Barriers in Cancer Pain Management at Oncology Units: A Cross-Sectional Survey of Medical Staff in China
Authors Yu Z, Li W, Shangguan X, Cai Y, Gao Q, Wang X, Chen Y, Liu D, Zhang C
Received 22 September 2021
Accepted for publication 30 December 2021
Published 21 January 2022 Volume 2022:15 Pages 159—169
DOI https://doi.org/10.2147/JPR.S339377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Zaoqin Yu,1,* Wei Li,1,* Xiaofang Shangguan,2 Yuanxuan Cai,2 Qianyan Gao,1 Ximin Wang,1 Yuan Chen,3 Dong Liu,1 Chengliang Zhang1
1Department of Pharmacy, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 2School of Pharmacy, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China; 3Department of Oncology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dong Liu; Chengliang Zhang
Department of Pharmacy, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430030, People’s Republic of China
Tel/Fax +86-27-83663643
; +86-27-83663519
Email [email protected]; [email protected]
Background: Despite the great signs of progress in cancer pain management in China, the associated pain remains under-treated. Poor knowledge among the medical staff is an important factor contributing to the under-treatment of cancer pain. This study aimed to evaluate the knowledge, practices, and perceived barriers in cancer pain management among the medical staff at oncology units in China.
Patients and Methods: A cross-sectional survey was conducted with the medical staff (including physicians, nurses, and pharmacists) at oncology units in tertiary hospitals of China between December 2020 and January 2021. The questionnaire assessed the knowledge, practices, and perceived barriers in cancer pain management.
Results: A total of 1262 medical staff responded to the questionnaire; the response rate was 94.2%. Most participants had good knowledge of the three-step analgesic ladder of the World Health Organization (WHO) and the National Comprehensive Cancer Network (NCCN) guidelines for Adult Cancer Pain. Knowledge deficit was prominent in questions on opioid dose titration and rotation and adverse effects of opioids; the correct response rate was less than 40%. Training, work experience in oncology, and education level were significantly related to knowledge of cancer pain management (all P < 0.001). In clinical practice for cancer pain management, approximately 57.2% of medical staff were unfamiliar with opioid dose titration and rotation; only 14.4% treated cancer pain through multidisciplinary collaboration. Poor medication compliance, difficult individualized analgesia protocols, and insufficient multidisciplinary participation were the most frequently perceived barriers by the medical staff for pain management.
Conclusion: These findings suggested a further need for integrating recent guidelines to strengthen continued training (especially among juniors and those with low education levels) and patient education to improve the knowledge and clinical practices of cancer pain management among the medical staff in China. Multi-disciplinary management is required for the effective treatment of cancer pain.
Keywords: cancer pain, medical staff, knowledge, practices, barriers, multi-disciplinary management
Introduction
Globally, cancer is one of the major causes of death.1 Pain is one of the most common and feared symptoms among cancer patients, with a prevalence of 25% at the first diagnosis and 66.4% among patients with advanced cancer; approximately one-third of patients experience moderate-to-severe pain.2,3 In addition to the physical harm, cancer pain causes psychosocial, behavioral, emotional, and spiritual problems, thus resulting in a significant impact on the quality of life of the patients.4–6 Therefore, cancer pain continues to be a worldwide issue.
In 1986, WHO developed a three-step analgesic ladder for pain management, which recommends non-opioid analgesics for mild pain, and opioids as the first line of treatment for moderate-to-severe cancer pain.7 According to the WHO guidelines, several other guidelines for the management of cancer pain have been established to aid in clinical decision-making, including those by NCCN and the American Society of Clinical Oncology (ASCO).8–11 This suggests that the attention to cancer pain treatment has greatly increased, and many efforts have been made to improve the treatment of cancer pain. Following these evidence-based guidelines, it is estimated that more than 70% of cancer patients can achieve adequate pain relief.7–11
Despite the significant progress in cancer pain treatment, evidence shows that many patients with cancer pain still experience unacceptable pain due to inadequate pain treatment.12,13 A previous study has demonstrated that more than one-third of patients reported moderate-to-severe pain after curative treatment.3 Sharkey et al14 found that nearly 56–82.3% of patients with cancer pain were under-treated, and these figures are worse in low- and middle-income countries. The inherent reasons for the undertreatment of cancer pain are multifactorial and related to the medical professional, patient, society, and the healthcare system.15 Unfortunately, poor knowledge in cancer pain management among medical professionals is an important barrier to effective control.16–18 Studies have found knowledge deficits among medical professionals in cancer pain management in Jordan,19 Palestine,20 Korea,21 Spain,22 and Italy.23 Jho et al reported that physicians, especially oncologists, seemingly lacked knowledge regarding the calculation of opioid dosages, adverse effects, and alternative therapies. Moreover, access to opioid use was also limited and sometimes challenging as it changed according to each country’s protocols, thereby resulting in lower cancer pain control.21
In China, it is estimated that approximately 4.3 million people are diagnosed with cancer, annually, and there were more than 2.9 million cancer-related deaths in 2018.24 According to the ACHEON survey, 88% of patients with advanced cancer reported moderate-to-severe pain, and even though the drug and non-drug interventions were administered, pain management remained inadequate in 43.8% of patients in China.25 Given this situation of under-treatment, why pain treatment is insufficient in China and the current challenges, need to be addressed. At present, in China, some studies also have investigated the factors among medical staff that influence the treatment of cancer pain.26–28 For instance, in a multi-center survey in Shandong, China, a high incidence of cancer pain was attributed to insufficient assessment, treatment, and patient education on cancer pain.26 However, these studies have a relatively small sample size (mostly limited to certain areas), and focus on a single medical profession, either physicians or nurses. Therefore, a large-scale investigation of knowledge and practices among medical staff for cancer pain management in China is needed. In the current study, we conducted a nationwide cross-sectional survey to investigate the knowledge, practices, and barriers in cancer pain management among different medical professionals at oncology units including physicians, nurses, and pharmacists. We also evaluated the related factors that influenced their knowledge.
Patients and Methods
Survey Design and Participants
This nationwide cross-sectional survey was performed using convenience sampling between December 2020 and January 2021. Medical staff (including physicians, nurses, and pharmacists) working at oncology units were recruited. These participants were from tertiary Hospitals spanning 22 provinces, 4 municipalities, and 4 autonomous regions in China. According to the geographical regions, these provinces, municipalities, and autonomous regions were divided into eastern China (10 provinces and 3 municipalities), central China (6 provinces), and western China (6 provinces, 1 municipality, and 4 autonomous regions).
This study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology. Before the questionnaire survey, the surveyors were required to confirm and explain the purpose and significance of the study. All medical staff participating in the survey were guaranteed confidentiality and anonymity to ensure that their rights were respected. All participants provided written informed consent before completing the survey. The participants who participated in the study were asked to complete the questionnaire that took approximately 10–20 min.
Questionnaire
The self-designed questionnaire was prepared by researchers based on literature review and expert consultation. The questionnaire was revised by a group of experts which consisted of 2 physicians, 2 pharmacists, and 2 nurses working in the oncology ward or palliative care unit. The questionnaire was comprised of four parts (Supplementary Material). The first part included the demographic characteristics of medical staff, including gender, region, education level, years of working experience in oncology, profession, occupation, and cancer pain-related training. In the second part, the questions were regarding the knowledge of guidelines for cancer pain management. These responses were structured on a 5-point Likert scale ranging from 1 (very unfamiliar) to 5 (very familiar). The part on knowledge of cancer pain management consisted of 10 true/false, 15 single-choice, and 5 multiple-choice questions (k=30). These focused on the principles of cancer pain management, pain assessment, analgesic drug properties, opioid dose titration and calculation, routes of administration, and the safety profile of opioids. Thus, the total scores for the correct answers could range from 0 to 30, and the mean scores of more than 18 were considered as “good knowledge” in cancer pain management.
The third section was regarding the current practices in cancer pain management; these included pain assessment, pain management, opioid dose calculation, and multidisciplinary diagnosis and treatment (MDT). Questions about perceived barriers in the fourth section were classified into three groups as follows: patient-, medical staff-, and healthcare system-related barriers.
Statistical Analysis
The database was established using EpiData version 3.1 (Atlanta, GA, USA). All data entry and statistical analyses were carried out using SPSS version 24.0 (SPSS Inc. Chicago, IL, USA). Descriptive analyses were used to describe the background characteristics of medical staff and their responses to questions related to knowledge, practices, and barriers in cancer pain management. Categorical variables are presented as frequencies and percentages. The chi-square analysis was used to examine the differences between categorical variables. Analysis of variance (ANOVA) was utilized to examine the differences in the knowledge for demographic variables that consisted of more than two groups. Logistic regression was used to identify the correlation between background characteristics and the knowledge of cancer pain management. A P-value of < 0.05 was considered statistically significant for all tests.
Results
Sample Characteristics
A total of 1262 medical staff completed the questionnaire survey in China; the response rate was 94.2%. A summary of participants’ background characteristics is presented in Table 1. The medical staff consisted of 459 physicians, 486 nurses, and 317 pharmacists. The majority of the respondents were female (69.4%) and had either an undergraduate or masters’ degree (88.8%). About half (45.1%) of participants had 3–10 years of working experience at oncology units. Approximately 81.4% of participants were in primary and middle levels in their occupation. 55.3% of the respondents were from Central China. More than 78% of medical staff reported that they had received training for standardized treatment of cancer pain, whereas 21.6% had never received any cancer pain-related training.
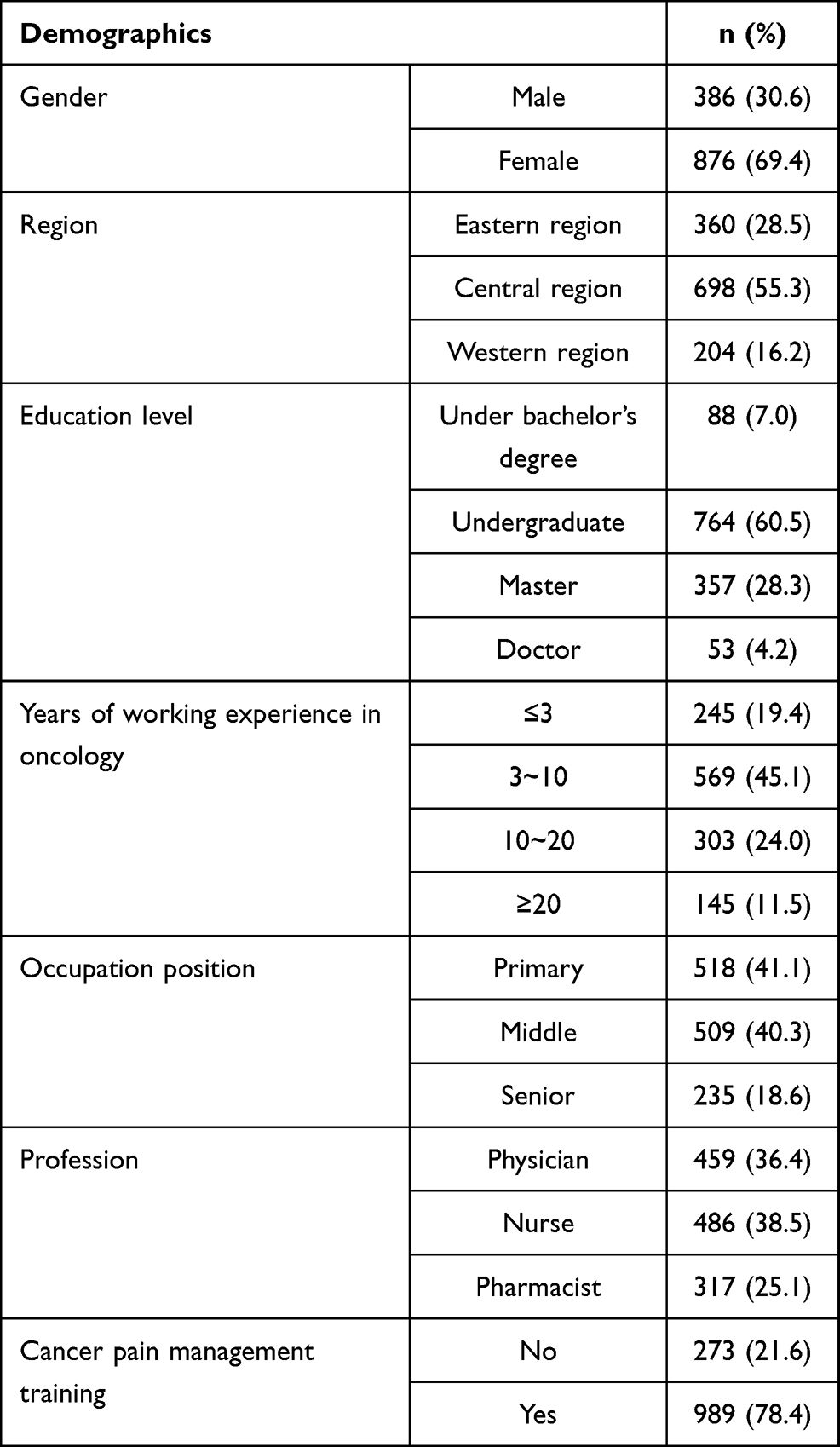 |
Table 1 Demographic Characteristics of Medical Staffs (n=1262) |
Knowledge of Cancer Pain Management
Table 2 describes the knowledge of cancer pain guidelines among the medical staff. Approximately 85% of respondents reported a comprehensive knowledge of the three-step analgesic ladder proposed by the WHO for cancer pain management. More than half of the medical staff were familiar with the clinical practice of NCCN guidelines for Adult Cancer Pain. As shown in Table 3, the rate of correct responses for each question which assessed the knowledge of cancer pain management was calculated. For medical staff, knowledge deficit was prominent in questions on opioid dose titration, and rotation, and adverse effects of opioids, with correct response rates of less than 40% (questions 11, 12, 21, 22, and 29). The rate of correct responses was higher for the questions on WHO three-ladder analgesic principle (questions 1 and 3), pain assessment (questions 17 and 24), route of administration (question 10), and analgesic drug properties (questions 5, 13, 26, 27, and 30).
 |
Table 2 Medical Staff’ Knowledge of Cancer Pain Guidelines |
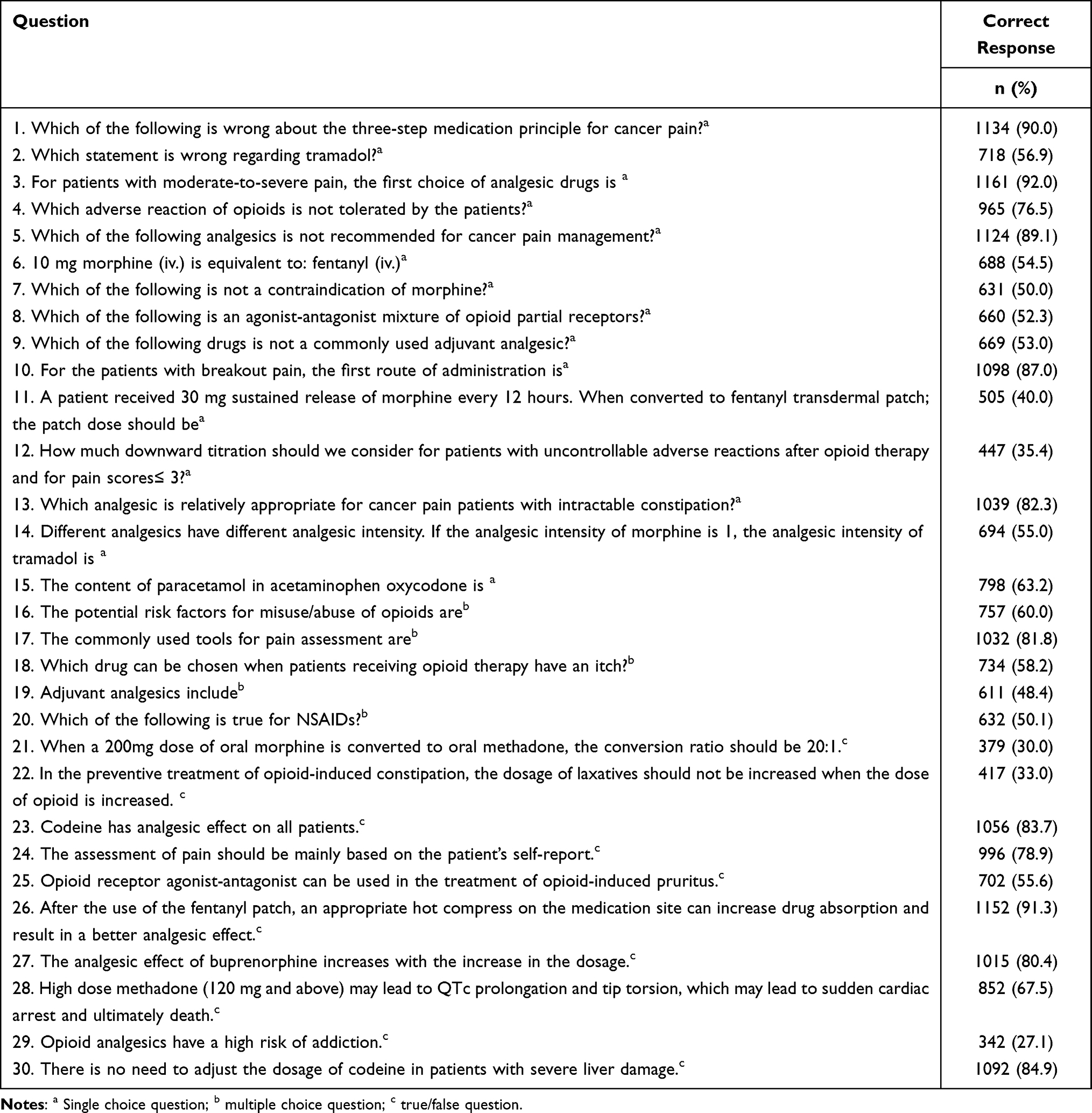 |
Table 3 Correct Response Rate for Knowledge of Cancer Pain Management |
Factors Associated with Knowledge of Cancer Pain Management
The knowledge of medical staff toward cancer pain management varied with education level, region, years of work experience in oncology, profession, and occupation, as shown in Table 4. Among them, the higher the education level, the higher was the knowledge of cancer pain management; the knowledge of physicians was higher than those of nurses. Medical staff who had worked for more than 3 years had better knowledge. In addition, the knowledge of respondents who had received training was higher than those who were not trained.
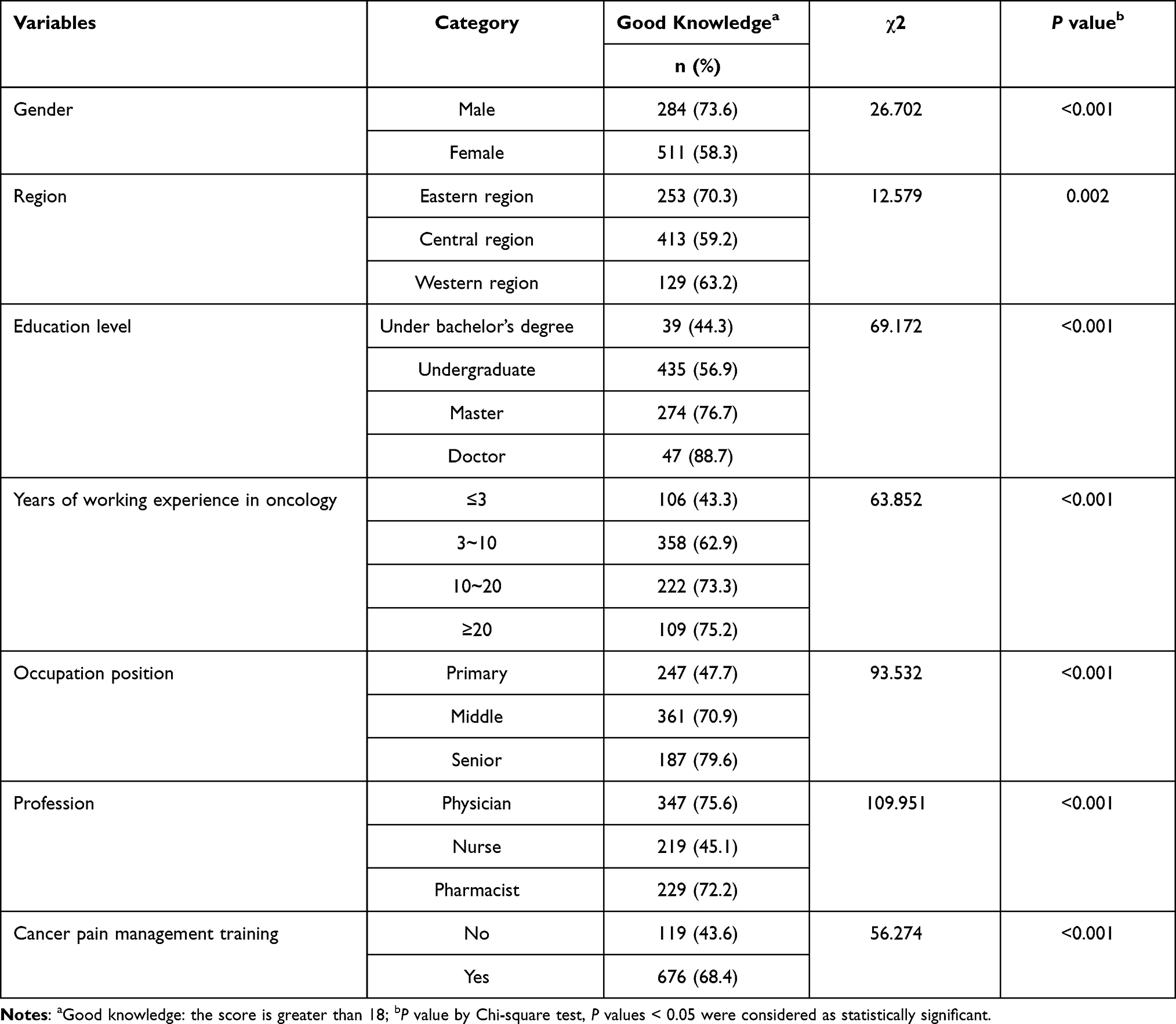 |
Table 4 The Related Factors That Influence Knowledge of Medical Staffs on Cancer Pain Management |
To identify the association of background characteristics with knowledge of cancer pain management, further analysis was performed using multiple logistic regression. The results showed that training, work experience in oncology, and education level were significantly positively correlated with the knowledge of cancer pain management (Table 5).
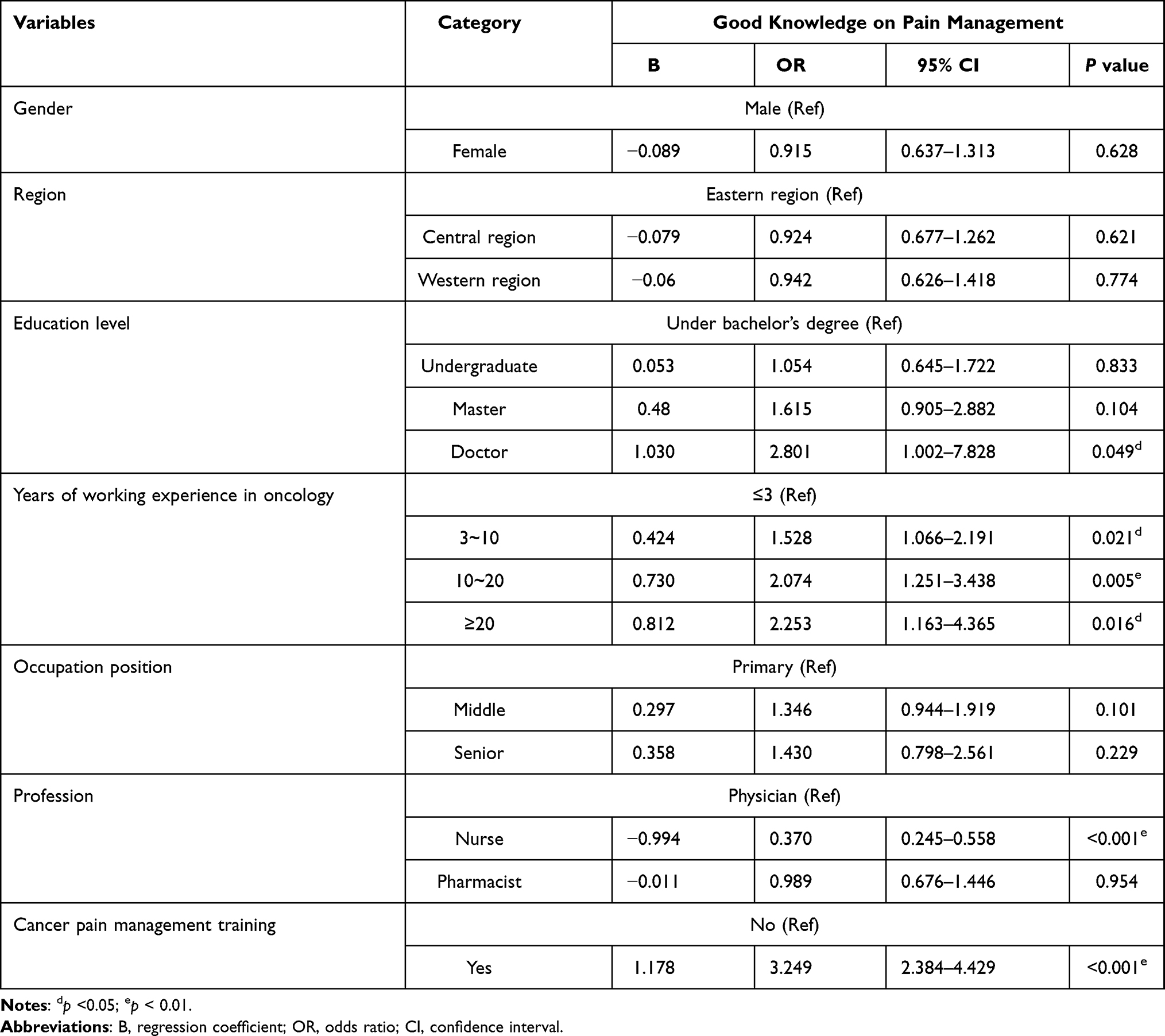 |
Table 5 Logistic Regression Analysis of Related Factors Associated with Good Knowledge of Cancer Pain Management |
The stratified analysis of training for different demographic characteristics is described in Table 6. Compared with participants who had not received the training, the knowledge among medical staff who had received training was significantly higher, especially for those who held doctor degrees (OR=22.5; 95% CI=2.655–190.678), in the western region (OR=6.21; 95% CI=3.279–11.761) and a senior position (OR=6.776; 95% CI=3.033–15.142). Trained medical staff who had an undergraduate degree or above and had worked for more than 3 years had better knowledge than those who had never received any training.
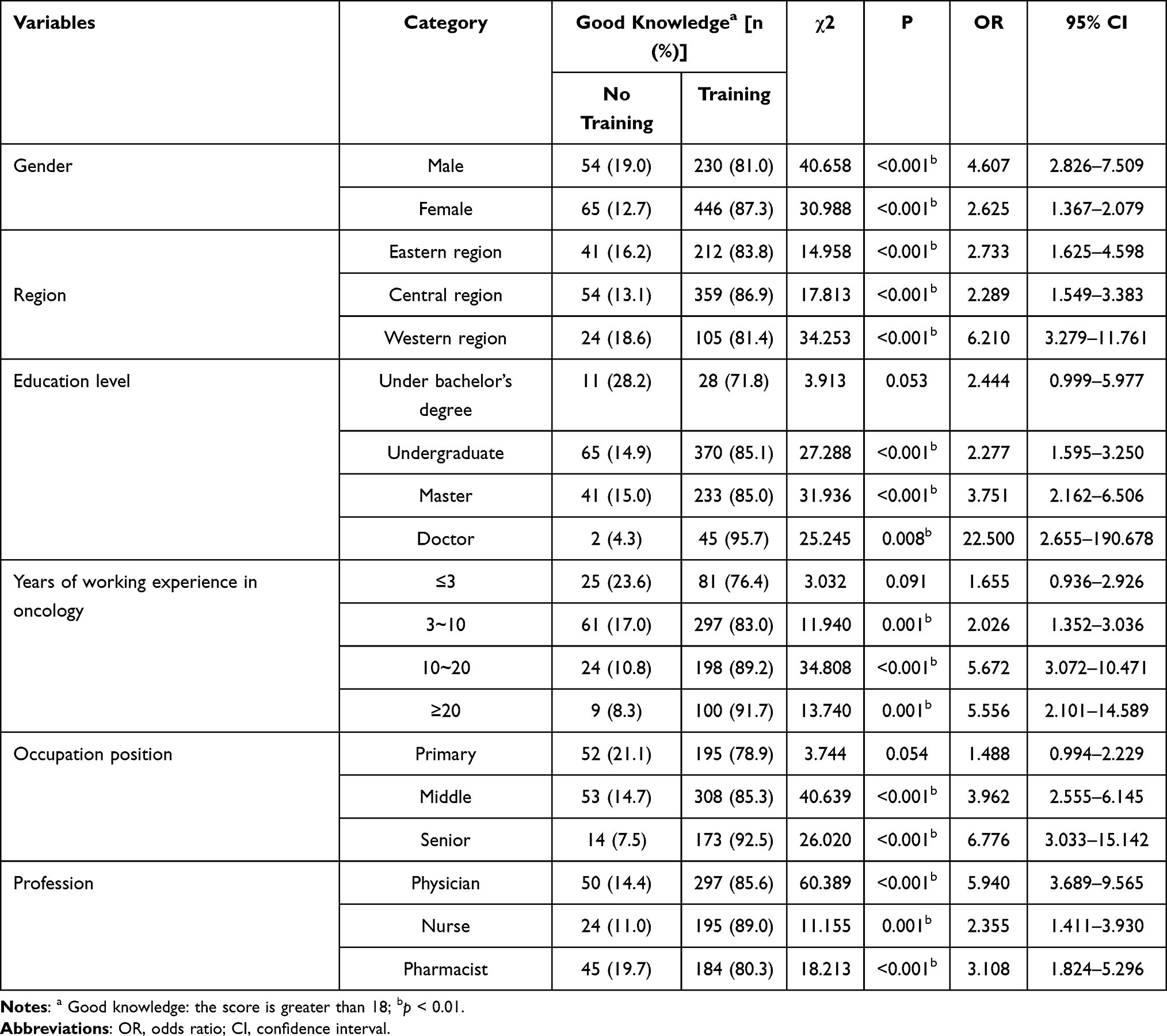 |
Table 6 Stratified Analysis of Cancer Pain-Related Training Among Different Demographic Factors |
Clinical Practices in Cancer Pain Management
Overall, more than half (58.9%, n=743) of respondents stated that they assessed the patients’ cancer pain every day. Approximately, 62.3% (n=785) of participants used the international guidelines to manage cancer pain, and most of them (80.2%, n=1010) responded that opioid therapy was the first-line therapy for cancer patients with moderate-to-severe pain. However, only 14.4% (n=181) of the medical staff treated the patients’ pain by multidisciplinary collaboration. For cancer pain treatment using opioids, 57.2% of medical staff were not familiar with the titrations of opioid doses and dosage calculation when switching between oral and parenteral routes of opioid administration.
Barriers to Cancer Pain Management
Barriers to cancer pain management are listed in Table 7. Insufficient multidisciplinary participation (61.8%) was the major barrier in health care systems. Medical staff-related barriers mainly included difficulty in individualized analgesia protocols (78.3%), lack of a good solution for refractory cancer pain (78.0%), and insufficient knowledge of pain management (68.0%). Among patient-related factors, the lack of knowledge in cancer pain management (80.6%), poor drug adherence (81.5%), and fear of addiction (73.5%) were the main barriers to cancer pain management.
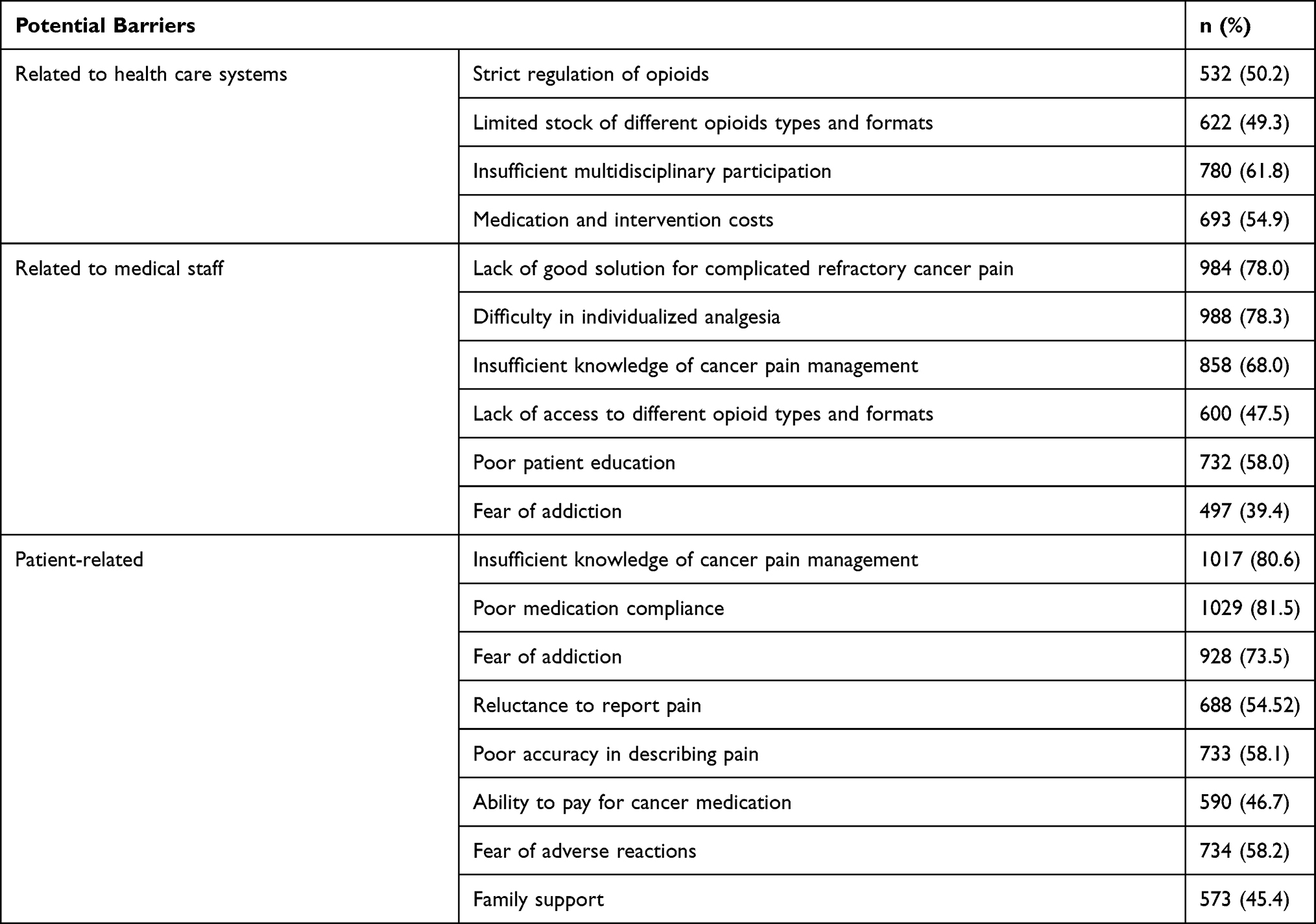 |
Table 7 Medical Staff’ Perceived Barriers to Cancer Pain Management |
Discussion
This study aimed to evaluate the knowledge, practices, and perceived barriers in cancer pain management from the perspective of the medical staff at oncology units. Such an investigation contributes to the understanding of the current status of cancer pain management and hence improves the management strategies of pain control in China. Overall, results demonstrated that medical staff, in general, had good knowledge of cancer pain management but lacked experience in multi-disciplinary collaboration which was among the perceived barriers in cancer pain management. In addition, training, work experience in oncology, and education levels were significantly positively related to the knowledge among medical staff regarding cancer pain management.
Pain management guidelines play an important role in the assessment, management, and standardized treatment of cancer pain. This study showed that 85.3% of medical staff had a better knowledge of the WHO three-step analgesic guideline; 53.4% had good knowledge of NCCN guidelines for Adult Cancer Pain. These were similar to those reported in previous studies in China.25,26,28,29 This indicated that the WHO and NCCN guidelines for cancer pain are widely used in China and considered as the primary references for the treatment of cancer pain. In China, many efforts have been taken to improve pain management.
Familiarity with the knowledge of cancer pain, such as pain assessment, opioid use, and adverse reactions is essential for effective pain control. In this study, medical staff had good knowledge, especially in the principle of cancer pain treatment and characteristics of analgesics, similar to results from previous studies.20–22 Our study also found that medical staff displayed substantial knowledge deficits for opioid-induced adverse effects, titration, and calculation of opioid dosages, which may be important factors leading to inadequate pain relief among some patients.19–21,30 If more attention is given to the adverse reaction of opioids, the patient’s quality of life will improve. The low rate of correct responses for opioid dose titration and calculation indicated a limited understanding of the specialist areas, which suggested that their understanding should be strengthened.
Socio-demographic factors have an important impact on the perception of cancer pain treatment. Several studies have shown that education level and working years in a cancer ward were positively associated with the knowledge of cancer pain management.19–21,30–32 In our study, the results showed that indeed the medical staff who received higher education and had more experience in the care of patients with cancer pain had significantly higher knowledge of pain management as compared to than who did not have the higher education or experience. Therefore, educational programs targeted to the medical staff with lower education and shorter experience are needed to improve their knowledge of cancer pain management. Clinical practice in a pain treatment team allows them to improve their knowledge of cancer pain management. However, many hospitals in China still lack pain treatment teams. Thus, the clinical decision-makers should pay attention to the importance of initiating the formation of pain treatment teams because it is highly effective in relieving the patient’s pain and improving the quality of life.33
In general, the training is necessary for medical staff to improve cancer pain management.19–21,30,34 The results in this study also showed that the knowledge of medical staff among those who received cancer pain-related training was higher than those who did not. However, training in China varies between schools and hospitals; many hospitals do not provide continued educational training to the staff involved in the care of cancer patients.35 These findings indicated that training in this field needs to be strengthened. Interestingly, the influence of training on knowledge was significantly different among different demographics. Thus, innovative and different training strategies targeted to the medical staff should be developed to effectively improve their knowledge and practices in cancer pain management.
Furthermore, our study confirmed that most medical staff often assess patients’ cancer pain and treat the pain by referring to international guidelines; however, the majority of the respondents did not follow a multi-disciplinary approach, were not familiar with dose titration, and rotation of opioids. This is similar to the findings from previous studies.22,25,26 This suggested a gap between existing treatment guidelines and real-world clinical practice. Thus, hospitals should provide timely and continuous education and training for updated guidelines to the medical staff, particularly for opioid dose calculation and conversion from oral to parenteral routes of administration.
Identifying barriers is crucial for improving cancer pain management. This study showed that medical staff-related barriers were mainly due to the difficulty in individualized analgesia protocols and treatment of refractory pain; these may be due to the complexity of cancer pain and less physician-patient communication. Inadequate knowledge of pain management and poor drug adherence were highlighted as important patient-related barriers perceived by medical staff. From the perspective of patients with cancer pain, our previous study also showed that patients’ lack of knowledge of cancer pain and poor drug adherence were crucial factors of poor pain control.36 In addition, patient factors, such as cancer stage (curative vs non-curative) and timing (during or after cancer treatment) can also affect pain control and should be addressed by the medical staff. These findings indicated that education programs for medical staff and patients and relevant guidelines on cancer pain are needed to overcome these obstacles that hinder effective pain management.
Insufficient multidisciplinary participation was also the main barrier to cancer pain management. Reddy et al reported that cancer patients with complex and refractory pain, who responded poorly to analgesia, experienced significant improvement in symptoms after management by an interdisciplinary palliative care team.37 In recent years, several studies have demonstrated that multidisciplinary treatment team, including surgeon, oncologist, radiotherapist, pain physicians, psychologists, nutritionist, nurse specialists, and pharmacist, is critical for improving pain control.38,39 A recent survey in China also showed that multidisciplinary interventions had beneficial effects on cancer pain management, especially in patients with moderate-to-severe pain.40 Meanwhile, multi-disciplinary collaboration should be integrated into comprehensive care to improve pain management and change the awareness and attitudes of medical staff toward pain treatment.41 Hence, multidisciplinary treatment should be strongly recommended to improve cancer pain management and the patient’s quality of life.
This nationwide cross-sectional study conducted in China explored knowledge, practices, and perceived barriers among the medical staff at oncology units relating to the management of cancer pain and identified the relationships between knowledge and their related factors. These contribute to the development of effective training programs for the improvement of pain management. However, this study also has some limitations. The convenience sample used in this study had a potential bias, and thus the results may not represent all the medical staff of China. Moreover, clinical practices among medical staff were influenced by various factors, leading to a discrepancy in the responses. Thus, further studies are needed to accurately assess the actual practice process and development of cancer pain management strategies in clinics based on the relevant influencing factors.
Conclusion
In conclusion, our study showed that medical staff at oncology units generally had good knowledge of pain treatment principles and the characteristics of analgesics. The knowledge deficits were prominent in dose titration, rotation, and adverse effects of opioids. Training, work experience in oncology, and education levels were significantly associated with the knowledge of cancer pain management. Multidisciplinary collaboration with other specialties remained deficient and problematic. From a global perspective, these findings highlighted the need for widespread and effective education programs and a multidisciplinary team-based approach for improving the management of cancer pain. With increasing attention given to cancer pain worldwide, we hope that the findings encourage researchers from other countries to conduct similar studies, to better control cancer pain and improve the quality of life of patients suffering from it.
Data Sharing Statement
The authors confirm that the data underlying the findings described in this manuscript are available from the corresponding author (Chengliang Zhang, E-mail [email protected]) upon reasonable request.
Acknowledgments
The authors would like to thank all experts involved in the design of the survey questionnaire and all medical staff who participated in the study.
Funding
The authors have no sources of funding to declare for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5–29. doi:10.3322/caac.21254
2. van den Beuken-van Everdingen MH, de Rijke JM, Kessels AG, et al. Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol. 2007;18(9):1437–1449. doi:10.1093/annonc/mdm056
3. van den Beuken-van Everdingen MH, Hochstenbach LM, Joosten EA, Tjan-Heijnen VC, Janssen DJ. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manag. 2016;51(6):1070–1090. doi:10.1016/j.jpainsymman
4. Al Qadire M, Al Khalaileh M. Prevalence of symptoms and quality of life among cancer patients. Clin Nursing Res. 2016;25(2):174–191. doi:10.1177/1054773814564212
5. Li P, Wu X, Liu D, et al. Beijing cancer pain management guideline (2017 edition). Chin J Pain Med. 2017;23(12):881–889. doi:10.3969/j.issn.1006-9852.2017.12.001
6. Leadley RM, Armstrong N, Reid KJ, et al. Healthy aging in relation to chronic pain and quality of life in Europe. Pain Pract. 2014;14(6):547–558. doi:10.1111/papr.12125
7. Carlson CL. Effectiveness of the World Health Organization cancer pain relief guidelines: an integrative review. J Pain Res. 2016;9:515–534. doi:10.2147/JPR.S97759
8. Swarm RA, Paice JA, Anghelescu DL, et al. Adult cancer pain, Version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(8):977–1007. doi:10.6004/jnccn.2019.0038
9. Paice JA, Portenoy R, Lacchetti C, et al. Management of chronic pain in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2016;34(27):3325–3345. doi:10.1200/JCO.2016.68.5206
10. Fallon M, Giusti R, Aielli F, et al. Management of cancer pain in adult patients: ESMO clinical practice guidelines. Ann Oncol. 2018;29(Suppl4):iv166–iv191. doi:10.1093/annonc/mdy152
11. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58–e68. doi:10.1016/S1470-2045(12)70040-2
12. Greco MT, Roberto A, Corli O, et al. Quality of cancer pain management: an update of a systematic review of undertreatment of patients with cancer. J Clin Oncol. 2014;32(36):4149–4154. doi:10.1200/JCO.2014.56.0383
13. Sherlyn V, Natalie P, Carlo DA, et al. Inadequate pain management in cancer patients attending an outpatient palliative radiotherapy clinic. Support Care Cancer. 2016;24(2):887–892. doi:10.1007/s00520-015-2858-7
14. Sharkey L, Loring B, Cowan M, Riley L, Krakauer EL. National palliative care capacities around the world: results from the World Health Organization noncommunicable disease country capacity survey. Palliat Med. 2018;32(1):106–113. doi:10.1177/0269216317716060
15. Kwon JH. Overcoming barriers in cancer pain management. J Clin Oncol. 2014;32(16):1727–1733. doi:10.1200/JCO.2013.52.4827
16. Eid T, Manias E, Bucknall T, Almazrooa A. Nurses’ knowledge and attitudes regarding pain in Saudi Arabia. Pain Manag Nurs. 2014;15(4):e25–e36. doi:10.1016/j.pmn.2014.05.014
17. Breuer B, Fleishman SB, Cruciani RA, Portenoy RK. Medical oncologists’ attitudes and practice in cancer pain management: a national survey. J Clin Oncol. 2011;29(36):4769–4775. doi:10.1200/JCO.2011.35.0561
18. D’ Emeh W, Yacoub M, Darawad M, Al-Badawi T, Shahwan B. Pain-related knowledge and barriers among Jordanian nurses: a national study. Health. 2016;8(6):548.
19. Darawad M, Alnajar MK, Abdalrahim MS, El-Aqoul AM. Cancer pain management at oncology units: comparing knowledge, attitudes and perceived barriers between physicians and nurses. J Cancer Educ. 2019;34(2):366–374. doi:10.1007/s13187-017-1314-4
20. Toba HA, Samara AM, Zyoud SH. Nurses’ knowledge, perceived barriers, and practices regarding cancer pain management: a cross-sectional study from Palestine. BMC Med Educ. 2019;19(1):167. doi:10.1186/s12909-019-1613-z
21. Jho HJ, Kim Y, Kong KA, et al. Knowledge, practices, and perceived barriers regarding cancer pain management among physicians and nurses in Korea: a nationwide multicenter survey. PLoS One. 2014;9(8):e105900. doi:10.1371/journal.pone.0105900
22. Garcia-Mata J, Alamo C, de Castro J, et al. A survey of perceptions, attitudes, knowledge and practices of medical oncologists about cancer pain management in Spain. Clin Transl Oncol. 2018;20(8):1061–1071. doi:10.1007/s12094-017-1826-8
23. Prandi C, Garrino L, Mastromarino P, et al. Barriers in the management of cancer-related pain and strategies to overcome them: findings of a qualitative research involving physicians and nurses in Italy. Ann Ist Super Sanita. 2015;51(1):71–78. doi:10.4415/ANN_15_01_13
24. Feng RM, Zong YN, Cao SM, Xu RH. Current cancer situation in China: good or bad news from the 2018 global cancer statistics? Cancer Commun. 2019;39(1):22. doi:10.1186/s40880-019-0368-6
25. Kim YC, Ahn JS, Calimag MMP, et al.; The ACHEON Working Group. Current practices in cancer pain management in Asia: a survey of patients and physicians across 10 countries. Cancer Med. 2015;4(8):1196–1204. doi:10.1002/cam4.471.
26. Tan B, Li B, An Y, et al. A multicentre survey of pain management in cancer patients and physicians attending radiotherapy clinics in Shandong Province, China. J Int Med Res. 2019;47(11):5711–5722. doi:10.1177/0300060519867168
27. Liao Z, Hao J, Guo Y, Reyes-Gibby C, Guo H. Assessment of cancer pain management knowledge in Southwest China: a survey of 259 physicians from small city and county hospitals. J Palliat Med. 2013;16(6):692–695. doi:10.1089/jpm.2012.0418
28. Zhang Q, Yu C, Feng S, et al. Physicians’ practice, attitudes toward, and knowledge of cancer pain management in China. Pain Med. 2015;16(11):2195–2203. doi:10.1111/pme.12819
29. Xia Z. Cancer pain management in China: current status and practice implications based on the ACHEON survey. J Pain Res. 2017;10:1943–1952. doi:10.2147/JPR.S128533
30. Yu W, Li D, Lu Y, Yang H, Ma X. Knowledge and attitudes of Chinese oncology nurses regarding cancer pain management-a cross-sectional study. J Cancer Educ. 2020. doi:10.1007/s13187-020-01743-z
31. Samarkandi OA. Knowledge and attitudes of nurses toward pain management. Saudi J Anaesth. 2018;12(2):220–226. doi:10.4103/sja.SJA_587_17
32. Gretarsdottir E, Zoëga S, Tomasson G, Sveinsdottir H, Gunnarsdottir S. Determinants of knowledge and attitudes regarding pain among nurses in a university hospital: a cross-sectional study. Pain Manag Nurs. 2017;18(3):144–152. doi:10.1016/j.pmn.2017.02.200
33. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119–130. doi:10.1037/a0035514
34. Germossa GN, Sjetne IS, Helleso R. The impact of an inservice educational program on nurses’ knowledge and attitudes regarding pain management in an Ethiopian University hospital. Front Public Health. 2018;6:229. doi:10.3389/fpubh.2018.00229
35. Lu Y, Gu Y, Yu W. Hospice and palliative care in China: development and challenges. Asia Pac J Oncol Nurs. 2018;5(1):26–32. doi:10.4103/apjon.apjon_72_17
36. Shangguan X, Yu Z, Ji L, et al. Cognition and sociodemographic determinants for effective pain control in patients with cancer pain: a cross-sectional survey in China. Curr Med Sci. 2020;40(2):249–256. doi:10.1007/s11596-020-2167-3
37. Reddy A, Hui D, Bruera E. A successful palliative care intervention for cancer pain refractory to intrathecal analgesia. J Pain Symptom Manage. 2012;44(1):124–130. doi:10.1016/j.jpainsymman.2011.07.010
38. Perez J, Olivier S, Rampakakis E, Borod M, Shir Y. The McGill University Health Centre Cancer Pain Clinic: a retrospective analysis of an interdisciplinary approach to cancer pain management. Pain Res Manag. 2016;2016:2157950. doi:10.1155/2016/2157950
39. Geum MJ, Ahn JH, Kim JS, et al. Interprofessional collaboration between a multidisciplinary palliative care team and the team pharmacist on pain management. Am J Hosp Palliat Care. 2019;36(7):616–622. doi:10.1177/1049909119829047
40. Yang B, Cui Z, Zhu X, et al. Clinical pain management by a multidisciplinary palliative care team: experience from a tertiary cancer center in China. Medicine. 2020;99(48):e23312. doi:10.1097/MD.0000000000023312
41. Liu WC, Zheng ZX, Tan KH, Meredith GJ. Multidimensional treatment of cancer pain. Curr Oncol Rep. 2017;19(2):10. doi:10.1007/s11912-017-0570-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.