Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Knowledge, Perceptions, Satisfaction, and Readiness of Health-Care Providers Regarding COVID-19 in Northern Ethiopia
Authors Wuneh A ![]() , Kahsay A
, Kahsay A ![]() , Tinsae F, Ashebir F, Giday G
, Tinsae F, Ashebir F, Giday G ![]() , Mirutse G, Gebretsadik G
, Mirutse G, Gebretsadik G ![]() , Gebremedhin G
, Gebremedhin G ![]() , Weldearegay H
, Weldearegay H ![]() , Berhe K
, Berhe K ![]() , Woldegebriel M, Weldeselassie T, Berhane Y, Hadis Z
, Woldegebriel M, Weldeselassie T, Berhane Y, Hadis Z ![]()
Received 26 September 2020
Accepted for publication 17 May 2021
Published 8 June 2021 Volume 2021:14 Pages 1349—1359
DOI https://doi.org/10.2147/JMDH.S284106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alem Wuneh,1 Amaha Kahsay,2 Fitiwi Tinsae,3 Fisseha Ashebir,4 Gebreamlak Giday,5 Gebremeskel Mirutse,6 Gebremedhin Gebretsadik,7 Getachew Gebremedhin,3 Haftom Weldearegay,8 Kalayou Berhe,9 Manay Woldegebriel,10 Tesfay Weldeselassie,11 Yemane Berhane,3 Zinabu Hadis6
1Health System, Mekelle University College of Health Sciences, Mekelle, Tigrai, Ethiopia; 2Nutrition and Dietetics, Mekelle University College of Health Sciences, Mekelle, Tigrai, Ethiopia; 3Nursing, Adigrat University College of Health Sciences, Adigrat, Tigrai, Ethiopia; 4Maternal and Child Health, Tigrai Regional Health Bureau, Mekelle, Tigrai, Ethiopia; 5Midwifery, Axum University College of Health Sciences, Axum, Tigrai, Ethiopia; 6Environmental and Behavioral Sciences, Mekelle University College of Health Sciences, Mekelle, Tigrai, Ethiopia; 7Midwifery, Adigrat University College of Health Sciences, Adigrat, Tigrai, Ethiopia; 8Midwifery, Mekelle University College of Health Sciences, Mekelle, Tigrai, Ethiopia; 9Nursing, Mekelle University College of Health Sciences, Mekelle, Tigrai, Ethiopia; 10Public Health, Axum University College of Health Sciences, Axum, Tigrai, Ethiopia; 11Research Monitoring, Training and Publication, Tigrai Health Research Institute, Mekelle, Tigrai, Ethiopia
Correspondence: Kalayou Berhe Tel +251 91-211-7719
Email [email protected]
Background: To protect health-care providers (HCPs) from COVID-19, the WHO recommends applying basic principles of infection prevention and control measures at all health-care facilities. This study aimed to assess the knowledge, perceptions, satisfaction, and readiness of HCPs regarding COVID-19 in Tigrai, Ethiopia in 2020.
Methods: This cross-sectional study was conducted from June 1 to July, 2020. Data were collected using a self-administered structured questionnaire. Multistage sampling followed by purposive sampling were used to recruit study subjects. SPSS 21 was used to compute proportions and χ2 to identify risk factors.
Results: Of 765 participants, 88% had adequate knowledge, close to a third showed positive perceptions and were satisfied with their job and nearly a quarter demonstrated readiness to prevent and control COVID-19. Education, knowledge, readiness, perceptions, and job satisfaction with associated with type and readiness of health facilities.
Conclusion: Despite adequate knowledge of the HCPs about COVID-19, their perceptions and job satisfaction are a concern for the health-care system. Only one in five HCPs was found to be ready to prevent and control COVID-19. Efforts should be exerted to improve perceptions, job satisfaction, and readiness of HCPs to fight COVID-19.
Keywords: knowledge, perception, satisfaction, readiness of HCPs, Tigrai, Ethiopia
Introduction
COVID-19 is an acute respiratory illness caused by a novel human coronavirus (SARS-CoV2) that causes higher mortality in people aged ≥60 years and those with underlying medical conditions, such as cardiovascular disease, chronic respiratory disease, diabetes, and cancer.1,2 Clinical symptoms include fever, cough, shortness of breath, and pneumonia. Severe cases show respiratory, hepatic, gastrointestinal, and neurological complications, and acute respiratory distress syndrome and cytokine storm, which can lead to mortality. Transmission of COVID-19 is human to human transmission via respiratory droplets or direct contact with infected patients.3,4 As of May 2020, the magnitude of the disease was escalating worldwide in terms of morbidity and mortality according to the WHO,5 and it had spread to 213 countries and territories around the world.6
In fighting this pandemic, health-care workers (HCWs) are at the front line of the response, and as such are exposed to hazards that put them at risk of infection.7,8,8 As a result, it is expected that all HCWs have the right to necessary preventive and protective measures to minimize occupational safety and health risks and adequate infection-prevention and -control and personal protective equipment (PPE) supplies, such as masks and sanitizer.7 The WHO recommends that the basic principles of infection prevention and control and standard precautions be applied in all health-care facilities, including outpatient care and primary care.9
However, as reported in Reuters by Mantovani in 2020, at least 90,000 HCWs worldwide are believed to have been infected with COVID-19, possibly twice that, amid a shortage of PPE, with 3.5 million cases of COVID-19 having been reported worldwide. He said that based on the average HCW-infection rate of 6%, there might be >200,000 HCWs infected globally.10 A report has also shown that >1,000 health-care providers (HCPs) had died as of May 1, 2020 from dozens of countries,8 which can be related to their exposure to risk of infection and emotional breakdown.11 As a result, readiness of HCWs to provide care for COVID-19 patients in resource-poor settings becomes unpredictable. Therefore to provide successful treatment for COVID-19, the physical and mental health of frontline HCWs needs to be protected.12
In Africa, as of June 24, 2020, there haxd been 324,559 confirmed cases and 8,621 deaths from of COVID-19.13 A government report showed that in Tigrai regional state, as of first the week of August 2020, more than 100 HCWs were infected. The level of COVID-19 infection in Ethiopia, from when the first case was detected in March 2020, has been surging as high as tenfold to reach the current number of cases.14 There are about 24 testing laboratory sites in the country performing >5,600 tests a day. About 18,000 health professionals, including students and retirees, have been mobilized of which 5000 began serving.15 However, there is a paucity of evidence about the readiness of HCPs in the country, despite this massive mobilization. Therefore, this study aimed ti assess Knowledge, perceptions, satisfaction, and readiness of HCPs regarding COVID-19 in northern Ethiopia. The findings from this study will used to guide policy-makers and serve as a baseline for other researchers.
Methods
Study Area and Period
This study was conducted in Tigrai from September to December 2019. Tigrais is one of the ten regional states of Ethiopia. Ethiopia’s health system is divided into three levels. Level one is a district health system comprised of a primary hospital (for 60,000–100,000 people), health centers (for 15,000–25,000), and five satellite health posts (for 3,000–5,000), connected to one another by two referral systems. The primary hospital, health centers and health posts form a primary health–care unit. Level two is a general hospital meant to serve 1–1.5 million people and level three a specialized hospital that serves 3.5–5 million people.16
As of 2020 in Tigrai, there were two specialized hospital, 15 general hospitals, 22 primary hospitals, 214 health centers, and 712 health posts. There were also 629 private health institutions, and health-care coverage is around 92% With regard to the number and composition of health professionals, there were 618 physicians, 3,092 nurses, 792 midwives, 562 health officers, and 1,539 health-extension workers17 The study was conducted from June 1, 2020 to June 21, 2020 in 26 health-care facilities.
Study Design
This was an institution-based cross-sectional study.
Source Population and Study Participants
All HCPs and sampled nurses, midwives, physicians, and other allied HCPs who were directly involved in the provision of health service and working in selected private and public health institutions of Tigray during the data-collection period were the source population and study participants, respectively.
Inclusion and Exclusion Criteria
All HCPs who were on duty during data collection, had direct involvement in COVID-19 prevention and control, and had volunteered to participate were included. All HCPs who were on night duty, sick leave, maternity leave, or in managerial positions were excluded.
Sample-Size Determination
The sample size was determined using a single-population proportion and computation made via the StatCalc component of EpiInfo 7.1.5 with 95% confidence level, a margin of error (d) of 5%, unknown proportion of readiness among HCPsP=50%), design effect of 2, and a 10% for nonresponse rate gave a final sample size of 846.
Sampling Procedure
Multistage sampling was used. in the first stage, districts were selected based on high risk of COVID-19 and highly populated urban areas. In the second stage, from the total public and private health facilities found in the region, 27 facilities who fulfilled the aforementioned criteria were selected purposefully. We used convenience sampling to recruit each participant from those who were on duty during the data-collection period.
The health facilities selected were two public referral hospitals (Ayder Comprehensive and Axum), six public general hospitals (Kahsay Abera, Lemlem Carl, Abi Adi, Mekelle, Adigrat, and Alamata), one private general hospital (Meskerem Ben), eight public primary hospitals (Tsegedie, Entecho, Rama, Tanqua Abergele, Atsebi, Hewo, Mekoni, and Samre), two private primary hospitals (Abi Dera and Romanat), and seven public health centers (Mykadra, Nebellet, Haykimeshal, Kasech, Quiha, Chercher, and Membere Kudisan)
Data Collection
Data were collected using a pretested self-administered questionnaire from previous studies and guidelines. The data-collection tool had five parts: socio demographic characteristics, HCP knowledge, perception, satisfaction, and readiness of HCPs to fight COVID-19.
Data-Collection Technique
Fourteen research assistants were assigned to facilitate the data-collection process. This was supervised by four health professionals with MPH/MSc degrees. Eligible HCPs for the study were identified with the help of managers. All HCPsproviders who were on duty were approached by the data collectors and managers, verified for eligibility, and adata collected.
Study Variables
Independent variables were facility type, age, sex, marital status, parenthood, religion, education, profession, and work experience, and dependent variables were knowledge, perceptions, job satisfaction, and readiness of HCPs regarding COVID-19 prevention and control.
Measurement
Readiness of HCPs was measured using principal-component analysis, the most common technique to create a single or composite quality index, which is a variable-reduction method to obtain a smaller set of uncorrelated variables from a large list of correlated variables. Each component is a linear combination of the observed variables optimally weighted to account for the maximum variance. As such, according to principal-component analysis, readiness of HCPs was defined as a binary variable of “lacks readiness” to “high readiness” on a continuous scale from 0 to 100. If HCPs scored 75% and above, it was classified as high readiness and otherwise “lacks readiness”. The knowledge section consisted of 20 items using “yes,” “no,” or “I don’t know” options. Knowledge was classified as adequate for ≥75% and above or inadequate for less <75%).18
Perceptions were assessed with five items and responses scored using a five-point Likert scale (strongly agree, agree, neutral, disagree, and strongly disagree). Then, perceptions were categorized as positive (≥75%) or negative (<75%). Finally, satisfaction was measured using seven items, categorized as satisfied (score ≥60%) or not satisfied (<60%).
Data Quality
To assure data quality, training and orientation were provided for the data collectors and supervisors by investigators. The questionnaire was tested and checked for its validity and reliability prior to actual data collection on 5% of the sample size 2 weeks before actual data collection and necessary amendments made. Data collected were checked for completeness and consistency on a daily basis at the spot during the data-collection period.
Data Analysis
Data were cleaned and checked for completeness and consistency before analysis. Data entry and analysis were performed using SPSS 21. Descriptive statistics were computed and cross-tabulation with χ2 tests applied to compare differences in HCPs’ knowledge, perceptions, job satisfaction, and readiness regarding COVID-19 prevention and control by demographic characteristics, profession, and facility type. P<0.05 was considered statistically significant. Results are presented using tables, figures, and text based on the data obtained.
Ethics Clearance
The verbal informed consent procedure was approved by the institutional review board of Mekelle University College of Health Sciences (May 19, 2020, EA 1729/2020), and the study was conducted in accordance with the Declaration of Helsinki. Letters of permission were secured from the Tigrai Regional State Health Bureau and administrative bodies of the area to communicate with relevant bodies at the health facilities. All participants were informed about the purpose of the survey, their right to participate or pull out at any time, and respondents assured of the confidentiality of information obtained. Respondents were asked not to write their name, to answer the questions only, and assued that individual responses would not be reported.
Results
Sociodemographic Characteristics and Facility-Related Factors
A total of 765 participants completed the questionnaire for a response rate of 90%. In sum, 774 (97.3%) were from public hospitals, 63% (n=483) aged of 20–29 years, 394 (51.5%)male, 378 (49.45%) married, and 392 (51.2%) did not have children. Most were nurses 367 (48.0%) by profession, and 481 (62.9%) had ≤5 years work experience (Table 1).
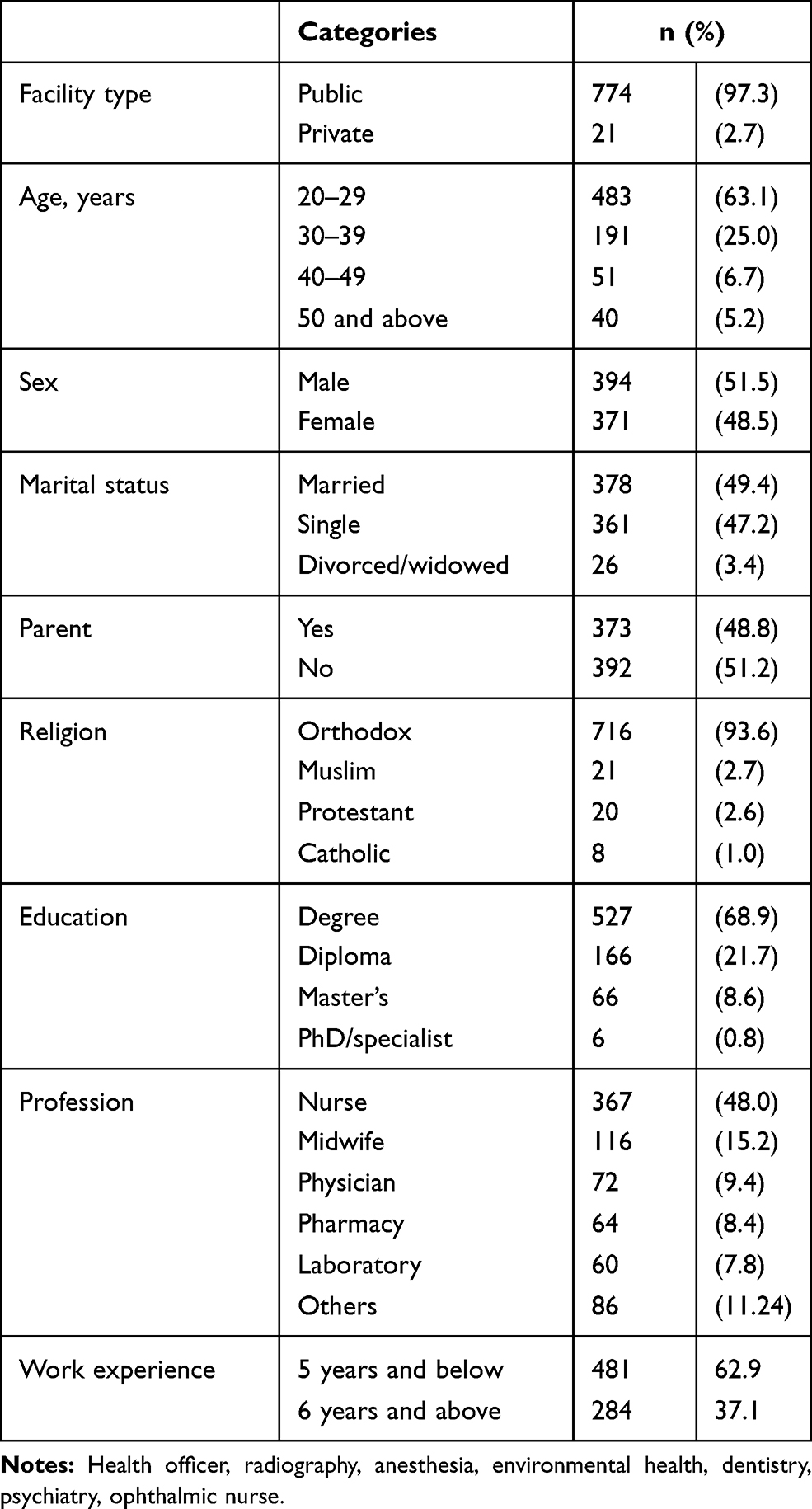 |
Table 1 Characteristics of HCPs in Selected Heath Facilities (n=765) |
HCPs’ Knowledge about COVID-19
Nearly nine in ten of HCPs (87.8%, 95% CI 85%–90%) had adequate knowledge about COVID-19. The most common signs and symptoms of COVID-19 mentioned by the participants were fever (735, 96.1%), coughing (718, 93.9%), and difficulty breathing (720, 94.1%). Contact with COVID cases was mentioned by 713 (93.2%) participants as a means of disease transmission. A majority of agreed that maintaining handwashing (733, 95.8%) help to prevent COVID-19 transmission. The most commonly mentioned high-risk groups fwas people with chronic diseases 723 (94.5%). Eight of ten (81.8%, n=626) participants answered correctly regarding incubation period (1–14 days, Table 2)
 |
Table 2 HCPs’ Knowledge About COVID-19 (n=765) |
Perceptions of HCPs about COVID-19
Of the participants, 284 (37.1%, 95% CI 33.4%–40.5%) exhibited positive perceptions about COVID-19 prevention and control strategies. Of the six perception items, risk of infection when there is confirmed cases and unavailability of PPE while caring for a suspected case were the greatest concerns of HCPs (Table 3).
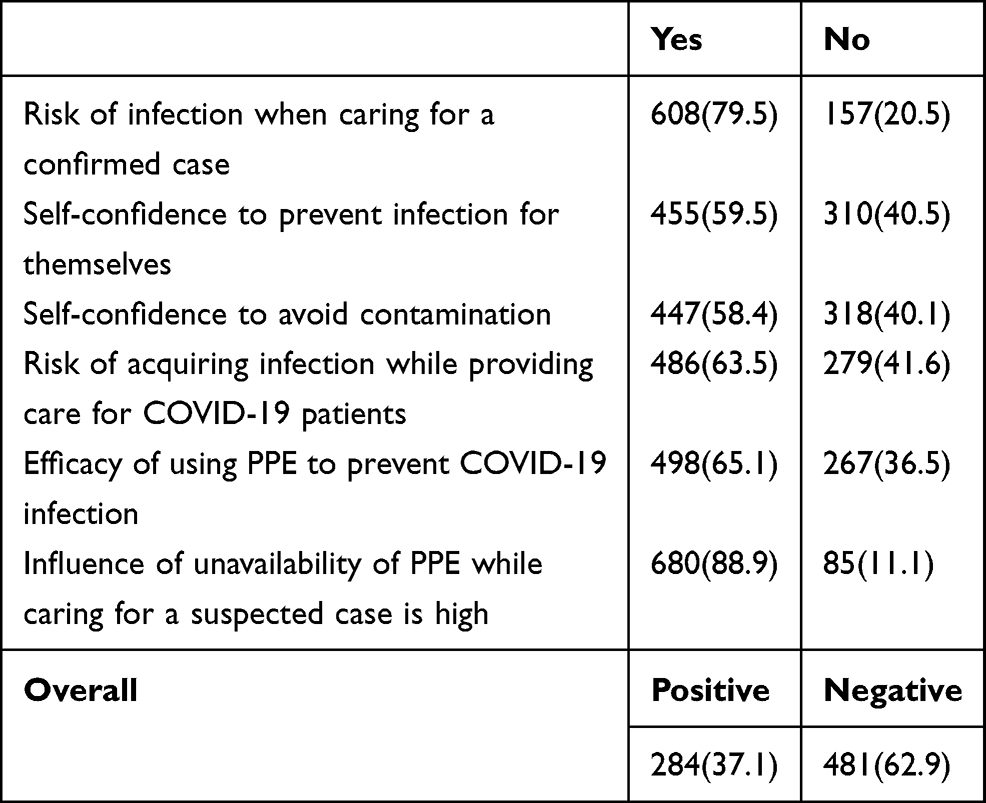 |
Table 3 HCPs’ Perceptions About COVID-19(n=765) |
HCPs’ Job Satisfaction in Prevention and Control of COVID-19
In sum, 242 (32.0%) of HCPs were satisfied with their job in the prevention and control of COVID-19. Almost all HCPs, 94.2% (n=721) were dissatisfied with the availability of medical equipment and supplies, including PPE. Only three in ten (29.7%, n=227) reported that they were satisfied working in teams (Table 4).
 |
Table 4 HCPs’ Job Satisfaction in Fighting COVID-19 (n=765) |
HCPs’ Readiness to Provide Care and Treatment for COVID-19
About a quarter (n=178) of the HCPs demonstrated readiness to provide care and treatment for COVID-19 patients: 649 (84.8%) were ready to be on duty to provide care for COVID-19 patients to the same extent as their routine activity. Also, 61.2% (n=468) of the participants were ready to provide psychological support to other HCPs in case they get infected while caring for COVID-19 cases (Table 5).
 |
Table 5 Readiness of HCPs to Treat and Manage COVID-19 Cases (n=765) |
Overall Scores of HCPs’ Knowledge, Perception, Satisfaction, and Readiness
The overall score for knowledge showed that 88% of the HCPs had adequate knowledge on the prevention and control of COVID-19. Close to a third had positive perceptions and were satisfied with their job in fighting COVID-19. ForNearly a quarter demonstrated readiness to prevent and control COVID-19. (Figure 1).
 |
Figure 1 Overall scores for knowledge, perceptions, satisfaction, and readiness of health-care providers regarding the prevention and control of COVID-19 in selected health facilities. |
Factors Affecting HCPs’ Knowledge in Prevention and Control of COVID-19
Knowledge of HCPs was higher among those working at public health facilities, married, parents, nurses, the highly educated, and those with work experience <5 years. Only education showed a statistically significant association with HCPs’ knowledge (Table 6).
 |
Table 6 Associations of Knowledge About Fighting COVID-19 with Facility Type, Sociodemographic Characteristics, and Profession (n=1,158) |
Factors Affecting HCPs’ Perceptions of Prevention and Control of COVID-19
Overall, HCPs showed positive perceptions of COVID-19 prevention and control: 19% of nurses and nearly 3% of midwives and physicians. No variables showed a statistically significant association for perceptions (Table 7)
 |
Table 7 Associations of Perception of Fighting COVID-19 with Facility Type, Sociodemographic Characteristics, and Profession (n=1,158) |
Factors Affecting HCPs’ Job Satisfaction in Prevention and Control of COVID-19
The number of HCPs who had job satisfaction was higher among among those working at public health facilities, married, parents, nurses, BSc holders, and work experience <5 years. No variables showed statistically significant association for HCPs’ perceptions (Table 8).
 |
Table 8 Association of Job Satisfaction to Fight COVID-19 with Facility Type, Sociodemographic Characteristics, and Profession (n=1,158) |
Factors Affecting HCPs’ Readiness in Prevention and Control of COVID-19
The readiness of HCPs to fight COVID-19 was higher among those working at public health facilities than those working at private facilities. Readiness was lower among parents, the highly educated, health officers, and physicians. Readiness scores for those with adequate knowledge, positive perceptions and satisfied with their current work indicated slightly higher readiness to fight COVID-19 (Table 9).
 |
Table 9 Association of Readiness to Fight COVID-19 with Facility Type, Sociodemographic Characteristics, and Profession (n=1,158) |
Discussion
COVID-19 is top of the agenda of discussion worldwide in the media and among the public, particularly among health professionals and patients. At present, the transmission of COVID-19 is increasing, which results in pressures for everyone, including health-care leaders and health systems. Knowledge is a requirement in prevention, forming positive perceptions, promoting practices, and individuals’ cognition and attitudes toward disease, which affect the effectiveness of their coping strategies and behavior to a certain extent.19 The aim of this study was to investigated HCPs’ knowledge, perceptions, job satisfaction, and readiness regarding the prevention and control of COVID-19 in selected public hospitals of Tigrai, Ethiopia.
The results revealed that a majority of the HCPs has adequate knowledge about COVID-19. Around four in ten participants had positive perceptions of COVID-19 prevention and control. Around a third of participants were satisfied with their job in providing care for patients with COVID-19, and nearly a quarter were ready to provide care for patients with COVID-19.
There was adequate knowledge among HCPs on COVID-19 prevention and control, consistent with studies conducted in Iran20,21 and China.22 However, this was higher than research from Uganda.23 A possible reason for this discrepancy might be associated with information acquired from social and conventional medias
This study also provides evidence of the extent of knowledge of HCWs regarding the symptoms, transmission, prevention, treatment, incubation period, and risk groups of COVID-19. Almost all HCPs identified “difficulty in breathing” as the main symptom of SARS-CoV2 infection, along with cough and fever, which is in line with a study in India.24 About nine in ten HCWs responded that contact with a COVID patient was a means of transmission, higher than a study from Vietnam,25 but lower than findings from Iran.20
A majority of the HCPs agreed that maintaining hand hygiene, physical/social distance, staying at home, covering the nose and mouth while coughing, not touching one’s eyes, nose, or mouth, and wearing a face mask can help prevent COVID-19 transmission, in line with studies from India and globally,24,26 and higher than one from Libya.27 In this study, a majority of HCPs identified people with chronic disease as being at high risk of COVID-19, similar to findings from Iran, where almost all participants knew that people with underlying diseases were more likely to become infected by the virus or even die from it.20 Eight of ten of the participants answered correctly about the incubation period (1–14 days) of COVID-19, in line with results from India and Vietnam indicatating that a majority were aware of the infectious and asymptomatic periods and knew that symptoms appeared in 2–14 days.24,25
This study revealed that more than a third of participants had positive perceptions of prevention and control measures, which is higher than a study from Uganda,23 but lower than studies from other countries.20,22,24–26 This difference can be explained in terms of supply of PPE and other medical equipment.
Only one of three respondents were satisfied with in the prevention and control of COVID-19, different from a cross-sectional study done in a hospital in Nepal, unlike ours, which was undertaken at all levels of health-care facilities. That study found relatively better satisfaction, attributed to information dissemination within the hospital,28 which was identified as a barrier in our study. A shortage of medical equipment and supplies, inadequate training and coaching, and lack of benefit packages were found to cause dissatisfaction among the respondents on their job, which was also found in a qualitative study from China.29 As such, improving the work environment complemented with institutional support and reward should enhance satisfaction.30 Otherwise, they will develop depression and stress, which will negatively affect their readiness to fight the disease.
This study revealed that more than three quarters of the HCPs lacked readiness to fight COVID-19, similar to a study from China.29 For example, as we drafted this manuscript, nearly 100 confirmed cases and deaths were reported among HCPs in the country. According to this study, lack of readiness is particularly worsened when it is reinforced by negative perceptions, lack of job satisfaction, and shortage of PPE, which may increase the infectivity and death of HCPs. These in turn impede the provision of routine services and care and treatment of COVID-19 cases as the HCPs get infected. The study also revealed being knowledgeable would not be a guarantee of readiness to fight an outbreak of infectious diseases. This calls for further study on why HCPs with adequate knowledge lack readiness to fight COVID-19 and perhaps also other outbreaks.
Conclusion
This study found that knowledge of HCPs on COVID-19 prevention and control measures was adequate. However, they had negative perceptions about COVID-19 and were not satisfied on their current job. Combined with the shortage of PPE, this negatively affects the readiness of HCPs to fight the disease. Therefore, to improve readiness of the HCPs to fight the disease, there should be provision of incentive packages, continued managerial support, PPE and psychological reassurance. Further research should be done to improve the readiness of HCPs. Monitoring and evaluation should also be strengthened.
Further research should aim to gain in-depth understanding for policy formulation regarding possible barriers to HCP’s readiness and perceptions through longitudinal/qualitative study that can avoid the limitations of this study. This was a cross-sectional study and conducted during lockdown, so data collection was difficult and said data partly affected by the recall ability of the participants, and thus may subject to recall bias.
Accessibility of Data and Materials
The results of this research were extracted from the data gathered and analyzed based on the stated methods and materials. There are no supplementary files. The original data supporting this finding will be accessible at any time upon request.
Abbreviations
HCPs, health-care providers; HCWs, health-care workers; PPE, personal protective equipment.
Ethics Approval and Consent to Participate
Ethics approval to conduct the assessment was obtained from the institutional review board of Mekelle University (May 19, 2020, EA 1729/2020), and an official letter of permission was obtained from Tigrai Regional Health Bureau.
Consent to Publish
Consent to publish is not applicable for this manuscript, because there are no individual data details like images or videos.
Acknowledgments
First and foremost, we would like to express our deepest gratitude and appreciation to Tigrai Regional Health Bureau for financial support to do this work. We would like to extend our thanks to the heads of the selected health facilities for the support they provided us in conducting this research.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Tigrai Regional Health Bureau (TRHB), but they had no other role in the manuscript.
Disclosure
The authors affirm that there is no conflict of interest concerning the publication of this manuscript. The authors report no conflicts of interest for this work.
References
1. Huber K, Goldstein P. Covid-19: implications for prehospital, emergency and hospital care in patients with acute coronary syndromes. Eur Heart J Acute Cardiovasc Care. 2020;2048872620923639.
2. World Health Organization. Infection prevention and control guidance for long-term care facilities in the context of COVID-19: interim guidance. World Health Organization; 2020.
3. Shanmugaraj B, Siriwattananon K, Wangkanont K, Phoolcharoen W. Perspectives on monoclonal antibody therapy as potential therapeutic intervention for Coronavirus disease-19 (COVID-19). Asian Pac J Allergy Immunol. 2020;38(1):10–18. doi:10.12932/AP-200220-0773
4. Guo Y-R, Cao Q-D, Hong Z-S, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Military Med Res. 2020;7(1):1–10. doi:10.1186/s40779-020-00240-0
5. World Health Organisation. Coronavirus Disease (COVID-19) Dashboard. Geneva: World Health Organisation; 2020. Available from: https://covid19.who.int/.
6. Worldometer. Countries where COVID-19 has spread; 2020. Available from: https://www.worldometers.info/coronavirus/countries-where-coronavirus-has-spread/.
7. World Health Organisation. Coronavirus disease (covid-19) outbreak: rights, roles and responsibilities of health workers, including key considerations for occupational safety and health. Geneva: WHO; 2020.
8. Medscape. In Memoriam: healthcare workers who have died of COVID‐19; 2020.
9. World Health Organization. Infection prevention and control during health care when COVID-19 is suspected: interim guidance. World Health Organization; 2020.
10. Mantovani C. Over 90,000 health workers infected with COVID-19 worldwide: nurses group. Reuters; 2020. Available from: https://www.reuters.com/article/us-health-coronavirus-nurses/over-90000-health-workers-infected-with-covid-19-worldwide-nurses-group-idUSKBN22I1XH.
11. Organization WH. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): interim guidance. World Health Organization; 2020.
12. World Health Organization. Strengthening the health system response to COVID-19: technical guidance# 1: maintaining the delivery of essential health care services while mobilizing the health workforce for the COVID-19 response. World Health Organization. Regional Office for Europe; 2020.
13. Shaban ARA. Coronavirus in Africa; 2020. Available from: https://www.africanews.com/2020/06/24/coronavirus-in-africa-breakdown-of-infected-virus-free-countries/.
14. covid19.et. Covid-19 Updates Ethiopian Governmet; 2020. Available from: https://www.covid19.et/covid-19/.
15. Shigute ZMA, Alemu G, Bedi A, Bedi A. Containing the spread of COVID-19 in Ethiopia. J Glob Health. 2020;10(1). doi:10.7189/jogh.10.010369
16. FMOH. Reference HSTP final draft document. Planning H, editor. Addis Ababa FMOH; 2007.
17. TRHB. Tigray regional health bureau (TRHB) Health System. Mekelle City: TRHB; 2020. Available from: https://tigrayrhb.org/mission/.
18. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hospital Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
19. McEachan RTN, Lawton R, Lawton R, Gardner P, Conner M, Conner M. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors.;. Ann Behav Med. 2016;50(592):592–612. doi:10.1007/s12160-016-9798-4
20. Maleki SNF, Farhadi K, Fakhri M, Hosseini F, Naderi M. Knowledge, attitude and behavior of health care workers in the prevention of COVID-19. Res Square.
21. Taghrir MHBR, Shiraly R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. 2020;23(4):249–254.
22. Zhou MTF, Wang Y, Nie H, Zhang L, You G, Zhang M. Knowledge, attitude and practice regarding COVID-19 among health care workers in Henan, China. J Hospital Infect. 2020.
23. Olum RCG, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus disease-2019. knowledge, attitude, and practices of health care workers at makerere university teaching Hospitals, Uganda. Front Public Health. 2020;30(8):181. doi:10.3389/fpubh.2020.00181
24. Parikh PASB, Phatak AG, Vadnerkar AC, Uttekar S, Thacker N, Nimbalkar SM. COVID-19 pandemic: knowledge and perceptions of the public and healthcare professionals. Cureus. 2020;12(5).
25. Huynh G, Nguyen TH, Tran V, Vo K, Vo V, Pham,L. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260. doi:10.4103/1995-7645.280396
26. Akshaya Srikanth Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Mohammadjavad ashrafi mahabadi and deepak kumar bandari. knowledge and perceptions of COVID-19 among health care workers: cross-Sectional Study. JMIR Public Health Surveill. 2020;6(2):e19160. doi:10.2196/19160
27. Elhadi M, Ahmed Msherghi A, Alkeelani M. Assessment of healthcare workers’ levels of preparedness and awareness regarding COVID-19Infection in low-resource settings. Am J Trop Med Hyg. 2020;103(2):828–833. doi:10.4269/ajtmh.20-0330
28. Samita Acharya S, K. M, Dongol D, Ghimire A. Awareness of COVID-19 and perception of work satisfaction among healthcare workers at Patan Hospital, Nepal. J Patan Acad Health Sci. 2020;7(1):31–36. doi:10.3126/jpahs.v7i1.28860
29. Liu QLD, Luo D, Haase JE, et al. The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob Heal. 2020;8:e790–e798. doi:10.1016/S2214-109X(20)30204-7
30. Theorell T. COVID-19 and working conditions in health care. Psychother Psychosom. 2020;89:193–194. doi:10.1159/000507765
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.