Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Knowledge on and Attitude toward Silver Diamine Fluoride among Saudi Dental Practitioners in Riyadh Public Hospitals
Authors Alajlan G, Alshaikh H ![]() , Alshamrani L
, Alshamrani L ![]() , Alanezi M, Alarfaj S, AlSwayyed T
, Alanezi M, Alarfaj S, AlSwayyed T ![]()
Received 3 July 2020
Accepted for publication 27 August 2020
Published 30 September 2020 Volume 2020:12 Pages 399—407
DOI https://doi.org/10.2147/CCIDE.S270562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Ghadah Alajlan,1,* Hessa Alshaikh,2,3,* Lamar Alshamrani,1,* Malak Alanezi,4,* Salma Alarfaj,5,* Tariq AlSwayyed3,6
1Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 4Buraydah Private Colleges, Qassim, Saudi Arabia; 5Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 6King Abduaziz Medical City/King Saud Bin Abdulaziz University for Health Sciences, Ministry of National Guard, Riyadh, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Tariq AlSwayyed
King Abduaziz Medical City/King Saud Bin Abdulaziz University for Health Sciences, Ministry of National Guard, Riyadh 11426, Saudi Arabia
Tel +966554428965
Email [email protected]
Aim: This study assessed the knowledge on and attitude toward silver diamine fluoride among Saudi dental practitioners in Riyadh public hospitals.
Materials and Methods: A cross-sectional study was done, data were collected between July and October 2019 using a validated, and the published questionnaire was analyzed. A sample size of 278 public hospital dental practitioners in Riyadh, Saudi Arabia, was used. Participants who agreed to the study completed a 3-section questionnaire of Likert scale comprising multiple questions regarding demographic data, knowledge on silver diamine fluoride, potential, and actual use of SDF in dental practitioner’s own professional life. Finally, respondents were asked about the future usage of SDF.
Results: A total of 278 Saudi dentists in Riyadh public hospitals completed the survey. The mean knowledge of SDF among participants was averagely 3.1. About half of the participants (50.4%) agreed that SDF could be used to arrest cavitated lesions. The majority of respondents showed a positive attitude toward SDF by accepting it as a good alternative treatment for individuals with behavioral problems or medical issues (> 50%). The most frequently reported barrier to the use of SDF was black discoloration (55.39%). A high number of respondents have not experienced the application of SDF, in their practice (> 60%), or dental school (65.5%). However, 57.9% expect an increase in the future use of SDF. The correlation between knowledge and attitude among different dental specialties was statistically significant (P< 0.05). The restorative specialty was observed to have the highest mean of knowledge (3.26), while advanced education general dentistry had the highest mean (3.67) of attitude toward SDF.
Conclusion: The aim of the study was achieved as the knowledge on, and attitude toward silver diamine fluoride among Saudi dental practitioners in Riyadh public hospitals was assessed. The response was average, with means of 3.1 and 3.3 for knowledge and attitude, respectively, among the participants.
Keywords: silver diamine fluoride, dental caries, public hospitals, knowledge, attitude, SDF approval and future usage
Introduction
Dental caries is one of the most common conditions which has an enormous public health impact on the overall health, social wellness, income of individuals, and healthcare systems.1 The prevalence of dental caries was the highest among all conditions of Global Burden of Disease 2015.2 The current review on the incidence and severity of caries over the past decades indicated that caries is a highly prevalent condition that adversely affects various age groups in Saudi Arabia. Also, secular trends show a dramatic increase in decayed, missing, filled teeth (DMFT) prevalence rates.1 According to a systematic review done by Al Ayyan et al,3 the mean DMFT range in children in Saudi Arabia was between 0.91 and 8.6, and the prevalence range was between 20.8% and 96%. In the United Arab Emirates in preschool children, the mean DMFT range was between 3.07 and 10.9 with a prevalence range of 41.5–99.4%. In primary dentitions of Omani children, the mean DMFT was 4.61, and the prevalence was 84.5%. Furthermore, the mean DMFT of Qatari children was 7.6, and the prevalence was 89.2%. Hence the conclusion that the prevalence of caries in the primary dentition in the Gulf Cooperation Council (GCC) State was high both in terms of mean DMFT (5.14) and incidence (80.95%). Caries estimation is alarming over the past 24 years in all GCC countries both primary and permanent dentitions, and is much higher than those observed in many other countries.3
Traditionally, dental caries is handled through treatment or prevention. One of the recent conservative preventive measures is the use of silver diamine fluoride (SDF).4,5 It was first discovered in Japan by Mizuho Nishino in 1970.5 However, it has been recently approved by the Food and Drug Administration (FDA) in August 2014,6 as well as by the Saudi FDA in January 2020. Consequently, SDF is recognized as caries arresting treatment since it has silver and fluoride particles. The interaction of the silver particles with the microorganisms’ sulfhydryl groups obstructs the bacterial metabolism, resulting in the bactericidal effect. In addition, the formation of a layer composed of silver salts and silver phosphate causes dentinal tubules blockage, whereas the fluoride particles of the SDF act as a remineralizing agent.7 It has been reported that the application of 38% SDF biannually is recommended for obtaining the maximum benefits.8
The validity of SDF in both primary and permanent teeth caries management is documented. A series of systematic reviews have indicated that SDF is more effective in controlling childhood caries compared to other treatments.7,9 Evidence supports the use of SDF in primary teeth, especially in children with high caries risk, including those with intellectual or developmental disabilities. Moreover, SDF can be used in arresting and preventing coronal and root caries in adults with high caries risk, limited access to dental care, and who require multiple visits. Also, SDF can be used to reduce teeth sensitivity.9–11
The main advantages of SDF are affordability and ease of application. SDF is a non-invasive alternative treatment to conventional methods (drill and fill) in dental caries management. Standard dental restorative treatment required sophisticated procedures that involve the use of rotary burs under local anesthesia and the need for highly trained dental health professionals.12 “The pain and discomfort associated with conventional cavity preparation methods have resulted in many patients being reluctant to seek dental treatment”.13 As a conservative approach, SDF can prevent extensive repair, eliminate postoperative pulpal symptoms, and weakening of the tooth that result from invasive caries removal. Furthermore, applying SDF in deeply cavitated teeth can preserve the vitality of pulpal tissue and avoid the need for a root canal treatment or extraction.14 However, dentists may hesitate to choose this type of treatment since its major drawback is the esthetic outcome that manifests as a black stain on arrested carious teeth.9
Due to the lack of studies conducted in Saudi Arabia about knowledge and attitude toward SDF among dentists, formulating a baseline data toward a relatively new accepted material would offer an opportunity to improve the provided oral healthcare services regarding dental caries in Saudi Arabia. The healthcare system in Saudi Arabia can be described as a primary public system, 80% of healthcare was through public services in 2019 (60% through Ministry of Health and the other 20% through other governmental sectors).15 In addition, dental residency and postgraduate programs provided by the Saudi universities and training centers approved by the Saudi Council of health specialties, are provided by governmental organizations.
Therefore, this study aimed to assess knowledge on and attitude toward silver diamine fluoride among Saudi dental practitioners in Riyadh public hospitals.
Materials and Methods
This is a cross-sectional study conducted to assess knowledge on and attitude toward Silver diamine fluoride among Saudi dental practitioners in Riyadh public hospitals. The questionnaire-based on a previously validated and published questionnaire after taking permission from the authors.16 To meet the study’s purpose certain adjustments were done on the questionnaire. The background section was re-established, and the education section was eliminated. The questionnaire included three parts of 40 questions with Likert scale. The first section sought demographic details, including sex, age group, specialty, and clinical title. The second section was designed to estimate the general thoughts on SDF among dental practitioners. The third section was about the potential and actual use of SDF in the dental practitioner’s own professional life. Finally, respondents were asked about the future usage of SDF.
Ethical approval was obtained from the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC) on 10 July 2019. Online Informed consent was obtained as the IRB approved this consent process since an online agreement button (Yes or No) to participate in the survey was available, and participants who agree to informed consent were directed to the survey. The aims of the study were explained, and the respondents were assured that the data will be completely anonymous and will be used for professional purposes only which include this manuscript; hence the participation was voluntary and in accordance to the Helsinki declaration.
The study included Saudi dental practitioners working in Riyadh public hospitals. Whereas non-Saudi dental practitioners, dental students, and Saudi dental practitioners who work only in the private sector, or other cities in Saudi Arabia were excluded.
A sample size of 278 from an assumed population of 1000 practitioners produces a two-sided 95% confidence interval with a precision (half-width) of 0.0500 when the actual proportion is near 66.35%.17 The sample size was calculated using Power Analysis and Sample Size (PASS) software (PASS 15 Power Analysis and Sample Size Software (2017). NCSS, LLC. Kaysville, UT, USA, ncss.com/software/pass).18
A simple random sampling technique was considered to select the 278 Saudi dental practitioners from public hospitals in Riyadh. The sampling frame was Saudi dental practitioners working in Riyadh public hospitals who used social media or emails.
The questionnaire was converted to an electronic form using Google Forms (Google Forms, 2019; a free web-based survey generator). A link to the questionnaire was distributed in English language via email and social media platforms. A reminder to participate was sent 5 days after the initial invitation.
The Likert scale direction was used, in Tables 1 and 2, the scale direction ranged from 5–1, where 5 denoted strongly agree and 1 strongly disagree. Exceptions were in some questions where it was reversed. This was in the following cases; SDF used prior to all restoration, in high risk patients, in the esthetic zones for both primary and permanent teeth, and in patients treated under general anesthesia. In Table 3, the scale was from 7–1, where 7 represented very appealing and 1 represented a large barrier. Exceptions were in three questions regarding black discoloration, restoring the natural teeth anatomy and patient satisfaction, where the scale was reversed. In Table 4, the scale was from 5–1, where 5 represented very often and 1 represented never. An exception was in the last question, though the scale was maintained from 5–1, where 5 represented increase a lot and 1 represented decrease a lot.
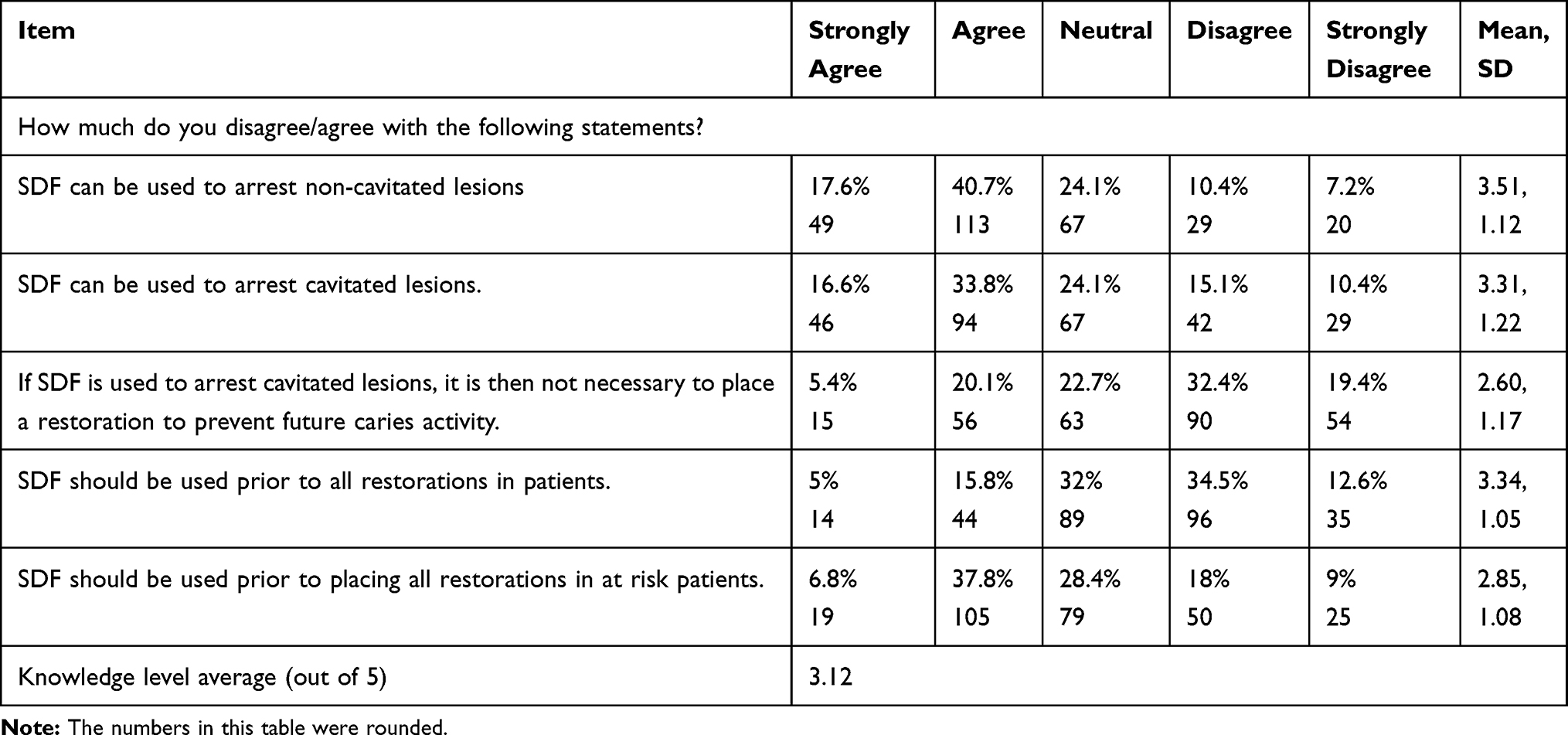 |
Table 1 Participating Pediatric Dentists’ Responses About Their Silver Diamine Fluoride (SDF) Knowledge, by Percentage of Respondents to Each Item |
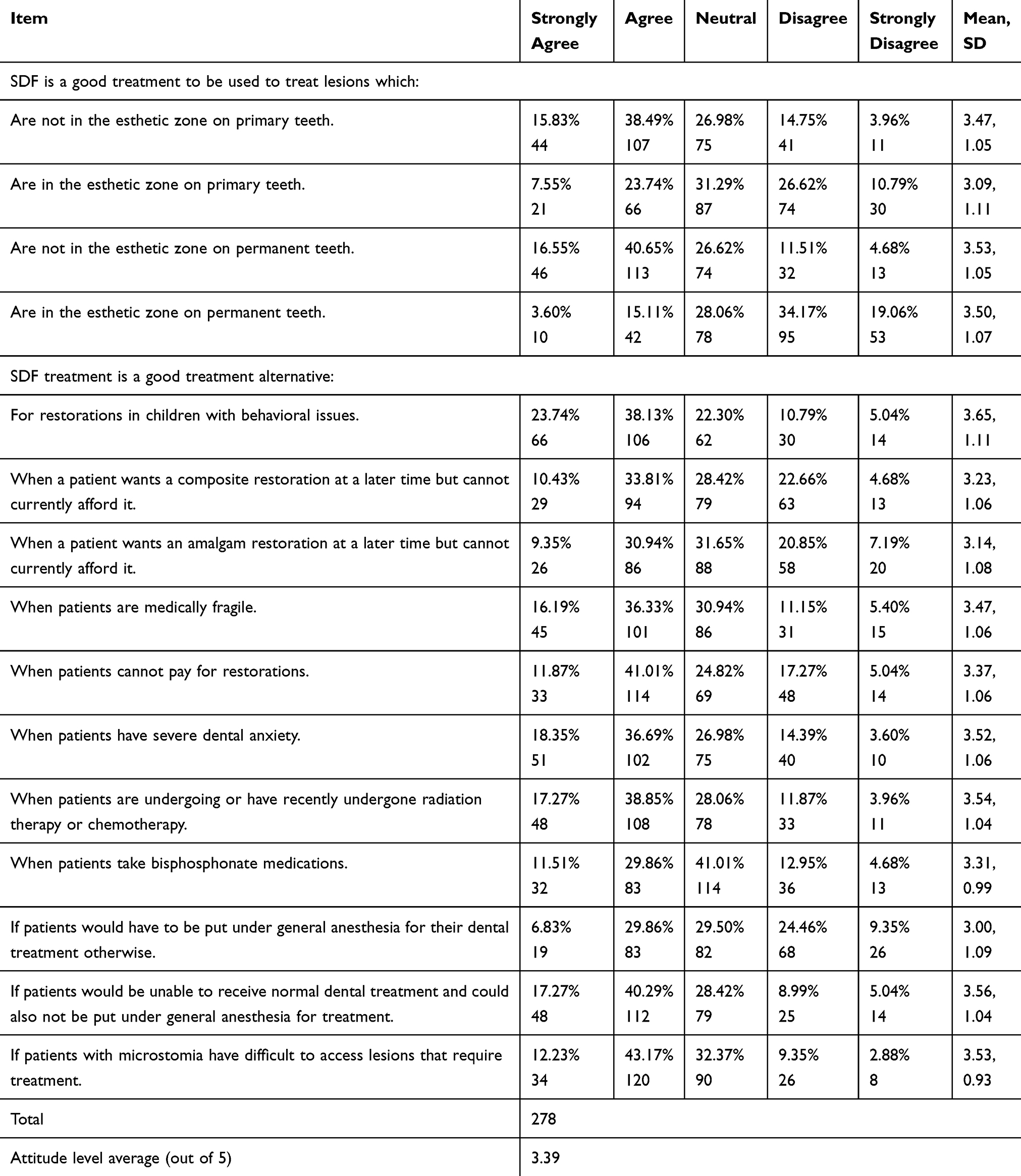 |
Table 2 Participating Saudi Dentists’ Responses Regarding Silver Diamine Fluoride (SDF) Considerations/Attitudes, by Percentage of Respondents to Each Item |
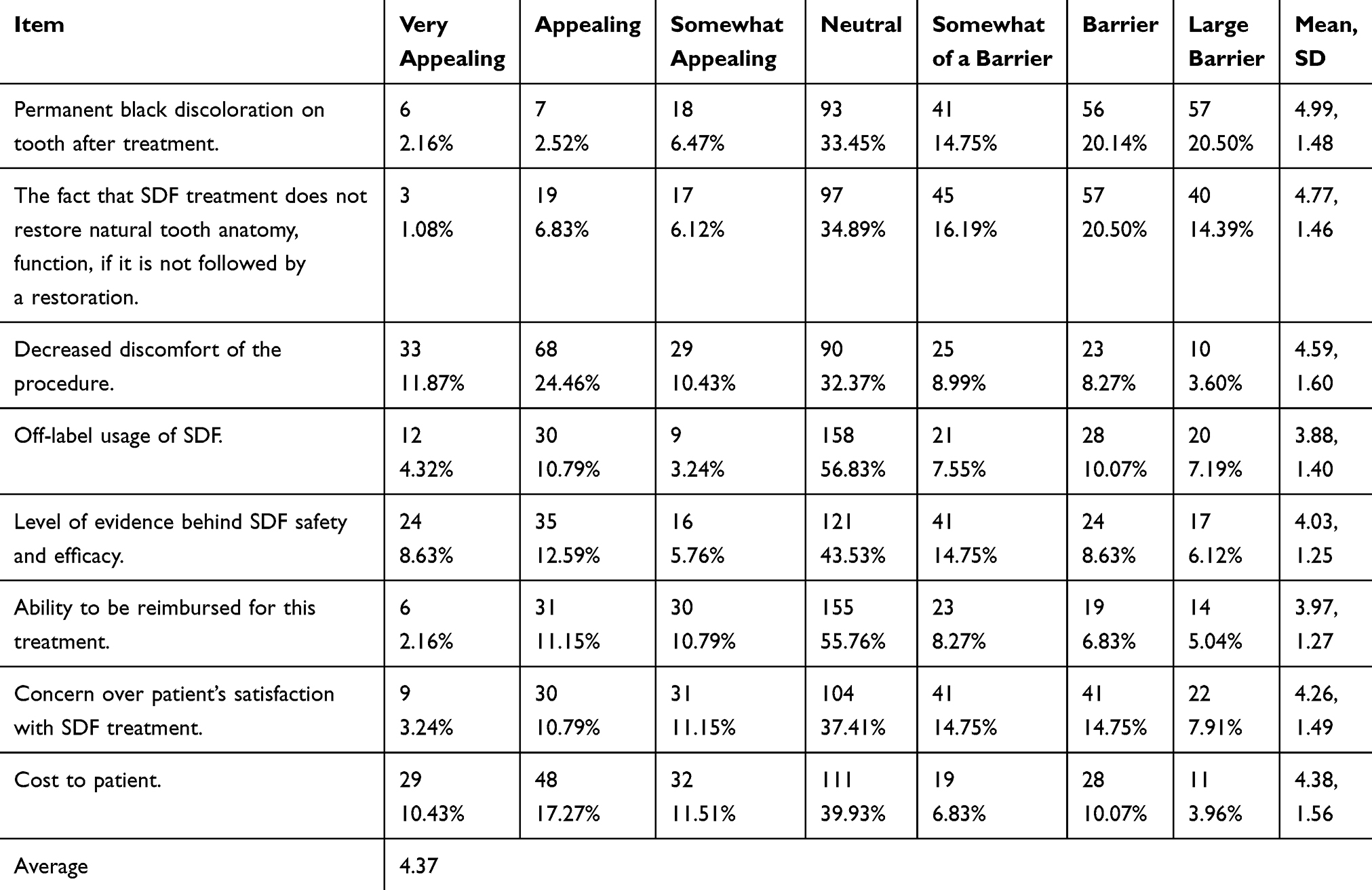 |
Table 3 Participating Saudi Dentists’ Responses Regarding Considerations to Silver Diamine Fluoride (SDF) Barriers, by Percentage of Respondents to Each Item |
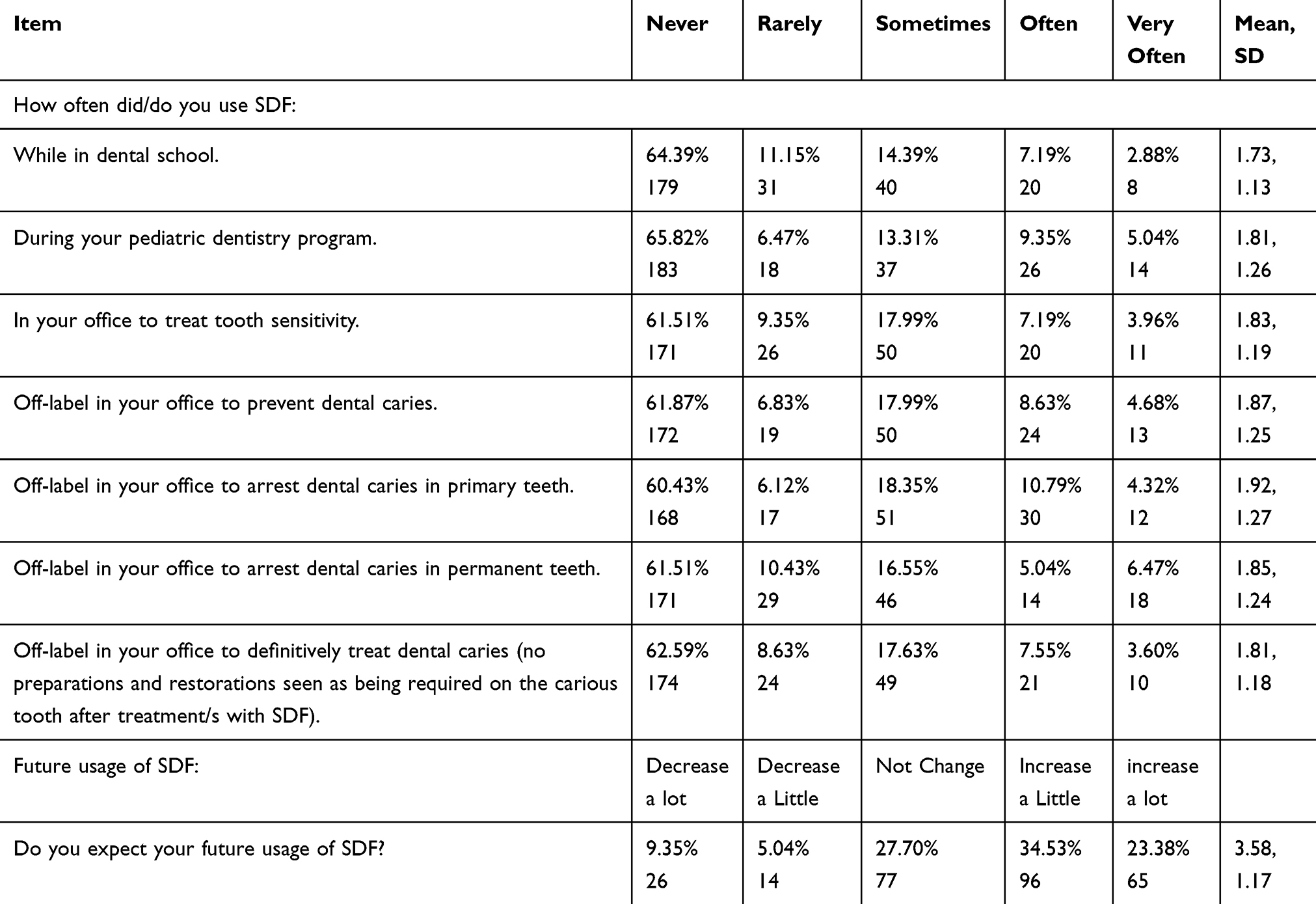 |
Table 4 Participating Saudi Dentists’ Responses Regarding Silver Diamine Fluoride (SDF) Usage, by Percentage of Respondents to Each Item |
The collected data from 278 Saudi dentists between July and October 2019 were analyzed using SAS version 9.4. Continuous variables were expressed as mean±standard deviations. Categorical variables are presented as frequencies (%). For evaluation of risk factors, 95% confidence interval for proportion, and a binomial test for one proportion were applied. For comparison and correlation purposes, tests such as the Pearson coefficient test were used. All P-values <0.05 were considered significant.
Results
In this study, a total of 278 Saudi dentists in Riyadh public hospitals completed the survey and provided their demographic information (Table 5). Out of the 278 participants, 111 (39.9%) were males and 167 (60.07%) were females, their ages ranged from 24 to over 45 years. The great majority of the participants were in the age range from 24–35 years, representing 209 (75%), followed by the age range from 36–45 (17.27%). The majority of respondents were general dentists (50.36%) followed by consultants (21.2%).
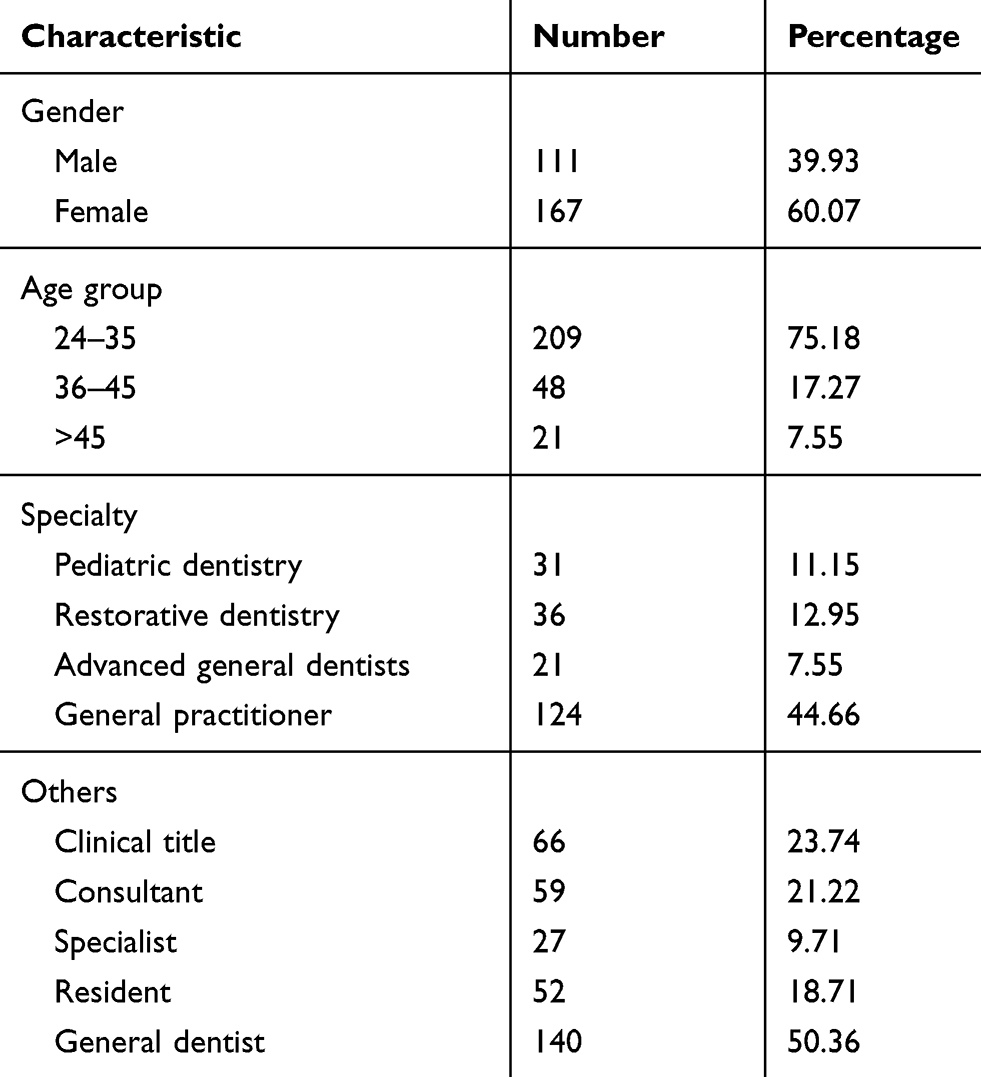 |
Table 5 Characteristics of Saudi Dentists Participating in Survey About Silver Diamine Fluoride (N=278) |
Five items were used to assess knowledge concerning SDF (Table 1). The majority agreed and strongly agreed that SDF can be used to arrest cavitated lesions (50.4%). When asked about non-cavitated lesions, 56.31% agreed and strongly agreed that SDF can be used to arrest non-cavitated lesions. Only 25.5% agreed and strongly agreed that it is not necessary to place restoration to prevent caries after application of SDF, while 47.1% disagreed and strongly disagreed that SDF should be used prior to all restorations, and 44.6% agreed and strongly agreed that SDF should be used prior to all restorations in at-risk patients followed by neutral response (28.42%).
The responses regarding the attitude toward SDF are shown in Table 2. Approximately 54% of the respondents agreed that SDF is a good treatment for primary teeth not in the esthetic zone. In contrast, only 37.41% agreed in the esthetic zone. More than half of the participants, when asked about permanent teeth not in the esthetic zone, agreed that SDF is a good treatment (57.2%). Few respondents disagreed with the statements; SDF is a good alternative treatment for children with behavioral issues (15.8%), patients who are medically fragile (16.55%), patients with severe dental anxiety (17.99%), patients undergoing chemotherapy or
radiotherapy (15.8%), patients on bisphosphonate medication (17.6%), and patients with microstomia (12.23%).
Regarding factors that make SDF appealing or a barrier for usage on patients (Table 3), the responses about permanent black discoloration on the tooth after treatment were somewhat barrier/large barrier (55.39%), followed by neutral responses (33.45%). Furthermore, 51.08% of respondents found the fact that SDF treatment does not restore natural tooth anatomy and function if it is not followed by a restoration as a somewhat barrier/large barrier. Nearly half of the participants (46.76%) responded that decreased discomfort of the procedure is somewhat appealing/very appealing. For the level of evidence behind SDF safety and efficacy, 43.53% responded with a neutral response. Concerning patient’s satisfaction with SDF treatment, 37.41% of dentists were neutral on that point. Regarding the cost of SDF to patients, 39.21% found it as a somewhat appealing/very appealing feature.
Table 4 illustrates the usage of SDF, approximately 60% of the participating dental practitioners had never used SDF neither to prevent nor to arrest dental caries in primary and permanent teeth. However, among those, 15.1% often/very often used SDF to arrest caries in primary teeth, with only 11.5% in permanent teeth. Regarding the future usage of SDF, 57.9% expected that it would increase a little or would increase a lot.
The secondary objective of the study was to explore multiple correlations between the respondents’ age, specialties, and clinical titles and knowledge level on as well as attitude toward SDF (Table 6). Thus, the analysis of the correlations showed there was no significant difference between age, gender, clinical titles, and respondents’ current level of SDF knowledge at 95% confidence level. However, as for the knowledge and attitude level, there were significant differences across the different specialties with a P-value <0.05. The highest level of knowledge among the specialties was observed in restorative dentistry (3.26), while advanced general dentistry and pediatric dentistry showed similar findings, 3.10 and 3.09, respectively. Moreover, advanced education general dentists (AEGD) had the highest mean (3.67) of attitude toward SDF followed by pediatric dentists. A significant difference was found in the correlation between the clinical titles and the level of attitude toward SDF with a P-value of 0.0048. The highest mean of attitude was found in the residents compared with other clinical titles.
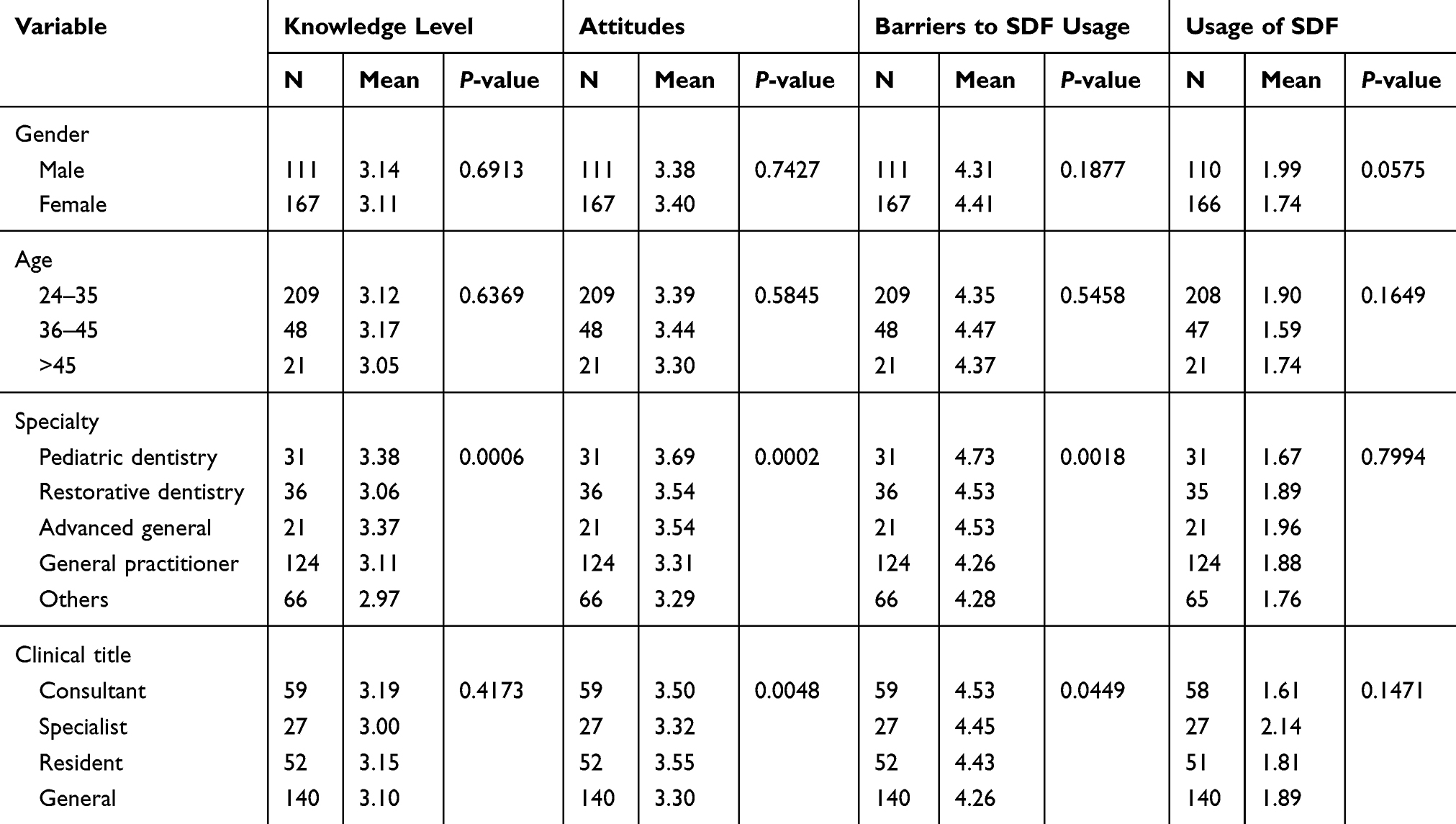 |
Table 6 Comparison of Knowledge, Attitude, Barriers to SDF, and Usage of SDF Across Different Variables |
Discussion
Few studies have discussed SDF material in Saudi Arabia. None of which concentrated on measuring SDF knowledge and attitude amongst dentists in the Riyadh region. SDF material has recently been approved in Saudi Arabia, thus its impact and usage among the Saudi dental society were unknown. Accordingly, the knowledge of SDF use was relatively low-to-average, and several responses were not consistent with empirical evidence. This could be due to their unfamiliarity and limited educational experiences with the material.
According to the American Dental Association (ADA) guidelines, SDF material is recommended to be used to arrest advanced cavitated lesions in primary teeth. Also, to arrest occlusal carious lesions in permanent teeth.19 Despite the established high level of evidence, only 50.4% of the respondents stated that they agreed/strongly agreed that SDF can be used to arrest cavitated lesions. Furthermore, evidence supports the use of SDF material as a preventive agent for new carious lesions in primary teeth and permanent molars.4 In this regard, 56.3% agreed/strongly agreed with that. The preventive effect of the SDF outperformed fluoride varnish.20,21 In contrast, SDF compared to resin or glass-ionomer cement sealants are less effective but has greater cost-effectiveness.4,16
The majority of the respondents were either against placing SDF prior to all restoration (47.1%), or neutral (32%). In accordance with the present results, the evidence behind the placement of SDF prior to restoration to prevent secondary caries is still limited and further studies are needed.5,16
In the current study, there were few agreement responses regarding treating lesions on permanent teeth in the esthetic zone with SDF, similar to a study conducted in the US.16 This finding is reasonable due to the permanent black discoloration after the SDF application.22 Accordingly, 55.39% of the participants considered it as a substantial barrier. Furthermore, 91.8% of pediatric dentistry program directors in the US were concerned about parental acceptance to the implementation of SDF.23 In Saudi Arabia, the parental acceptance of teeth discoloration found to be on the anterior teeth 90% strongly refuse, while on posterior teeth 28.4% refuse and 68.5% strongly refuse.14 Also, a study demonstrated that parents’ acceptance and decisions differ depending on whether it is a posterior or anterior tooth.16 Despite parental intolerance of the black discoloration, a wide range of them would still accept SDF application to avoid extensive dental behavioral management such as general anesthesia or sedation.5,24
Consistent with the American Academy of Pediatric Dentistry guidelines,22 this research found that more than half of the participants agreed that SDF is a good alternative treatment for individuals with behavioral or medical issues, whereas only a few disagreed. These results are similar to those reported by Antonioni et al.16
Regarding the cost of SDF, several factors should be taken into consideration, the low cost of the material, and the short time of application for the practitioner as well as for the caregivers, also the longevity of the treatment or the disease-free years.22 In this study, only 39.21% of the respondents found the cost of SDF material as an appealing feature, and 39.9% were neutral about it.
With respect to the frequency of SDF usage (Table 4), a greater number of respondents have not experienced the application of SDF in their practice or dental school. Contrarily, a previous study showed that the majority of their respondents had used SDF to arrest carious lesions in primary teeth.16 Possible explanations for this might be that our participants were from various dental specialties as well as different clinical experiences, while in the above-mentioned study, their participants were only pediatric dentists. Also, as mentioned earlier, the Saudi FDA has recently approved the material. However, over half of those who answered the question regarding the expectation of the future use of SDF were positive and expected it would increase.
The observed results of the correlation between knowledge and attitude among different dental specialties were statistically significant. Whereas, among clinical titles, only attitude means showed significant correlation. Contrary to expectation, the restorative specialty was observed to have a higher mean of knowledge toward SDF compared to those in pediatric dentistry. These results among dental specialties and clinical titles may have been influenced by the lack of adequate samples representing each group.
The study encountered multiple limitations. Firstly, the most important limitation lies in the fact that “I don’t know” was not included as an option in the original version of the questionnaire, which might contribute to the high percentage of neutral responses among participants. Secondly, SDF is only recently approved in Saudi Arabia, thus a lack of long exposure and clinical experience of SDF might affect dentists’ decisions and preferences regarding such treatment. In addition, the scope of this study was confined to dental practitioners from governmental sectors only, which may not reflect those of other sectors in Saudi Arabia.
Further studies with more focus on larger samples including dentists from other sectors and different regions are needed to provide more conclusive and generalized findings is therefore suggested. Moreover, this study raises many questions and sheds light on areas that should be explored in future studies. Including, areas of education experience and teaching practices can provide very helpful information that can identify the source of gaps in the current knowledge of dentists.
Conclusion
The aim of the study was achieved as the knowledge on and attitude toward Silver diamine fluoride among Saudi dental practitioners in Riyadh public hospitals was assessed. The response was on average with means of 3.1 and 3.3 for knowledge and attitude, respectively, among the respondents. As previously stated, SDF material is an affordable caries management method with minimal equipment and operator training required. This study has been one of the first attempts to thoroughly assess the dental practitioners’ knowledge on and attitude toward SDF in Riyadh, Saudi Arabia. Overall, it strengthens the idea that raising awareness on SDF material is needed to have more implementation into dentists’ clinical practice in Saudi Arabia which in return will improve the knowledge and attitude towards SDF among Saudi dental practitioners.
Acknowledgments
The authors wish to thank the Research Summer School Program at King Abdullah.
International Medical Research Center for giving them the opportunity to do this project. All the efforts by Dr. Ramesh Vishwakarma in sample size calculation and Dr. Omar Aldibasi in data analysis are highly appreciated.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Al-Ansari AA. Prevalence, severity, and secular trends of dental caries among various Saudi populations: a literature review. Saudi J Med Med Sci. 2014;2(3):142. doi:10.4103/1658-631X.142496
2. Kassebaum NJ, Smith AG, Bernabé E, et al. GBD 2015 oral health collaborators. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96(4):380–387.
3. Al Ayyan W, Al Halabi M, Hussein I, Khamis AH, Kowash M. A systematic review and meta-analysis of primary teeth caries studies in gulf cooperation council states. Saudi Dent J. 2018;30(3):175–182. doi:10.1016/j.sdentj.2018.05.002
4. Horst JA, Heima M. Prevention of dental caries by silver diamine fluoride. Compend Contin Educ Dent. 2019;40(3):158–163.
5. Crystal YO, Niederman R. Evidence-based dentistry update on silver diamine fluoride. Dent Clin. 2019;63(1):45–68.
6. Sarvas E. The history and use of silver diamine fluoride in dentistry: a review. CAC J. 2018;46:19–22.
7. Chibinski AC, Wambier LM, Feltrin J, Loguercio AD, Wambier DS, Reis A. Silver diamine fluoride has efficacy in controlling caries progression in primary teeth: a systematic review and meta-analysis. Caries Res. 2017;51(5):527–541. doi:10.1159/000478668
8. Fung MHT, Duangthip D, Wong MCM, Lo ECM, Chu CH. Randomized clinical trial of 12% and 38% silver diamine fluoride treatment. J Dent Res. 2018;97(2):171–178. doi:10.1177/0022034517728496
9. Contreras V, Toro MJ, Elías-Boneta AR, Encarnación-Burgos MA. Effectiveness of silver diamine fluoride in caries prevention and arrest: a systematic literature review. Gen Dent. 2017;65(3):22.
10. Sinha N, Gupta A, Logani A, Shah N. Remineralizing efficacy of silver diamine fluoride and glass ionomer type VII for their proposed use as indirect pulp capping materials–Part II (A clinical study). J Conserv Dent. 2011;14(3):233. doi:10.4103/0972-0707.85796
11. Castillo JL, Rivera S, Aparicio T, et al. The short-term effects of diammine silver fluoride on tooth sensitivity: a randomized controlled trial. J Dent Res. 2011;90(2):203–208. doi:10.1177/0022034510388516
12. Subbiah GK, Gopinathan NM. Is silver diamine fluoride effective in preventing and arresting caries in elderly adults? A systematic review. J Int Soc Prev Community Dent. 2018;8(3):191. doi:10.4103/jispcd.JISPCD_99_18
13. Martinez-Zapata MJ, Walsh T, Marinho VC, Sheiham A, Zaror C, Dorri M. Atraumatic restorative treatment versus conventional restorative treatment for managing dental caries. Cochrane Database Syst Rev. 2017;2017(12).
14. Alshammari AF, Almuqrin AA, Aldakhil AM, Alshammari BH, Lopez JNJ. Parental perceptions and acceptance of silver diamine fluoride treatment in Kingdom of Saudi Arabia. Int J Health Sci. 2019;13(2):25.
15. MOH. Ministry of Health – Saudi Arabia. Statistical Book for 2019. Riyadh: Ministry of Health; 2019.
16. Antonioni MB, Fontana M, Salzmann LB, Inglehart MR. Pediatric dentists’ silver diamine fluoride education, knowledge, attitudes, and professional behavior: a national survey. J Dent Educ. 2019;83(2):173–182. doi:10.21815/JDE.019.020
17. AlBaker AM, Al-Ruthia YS, AlShehri M, Alshuwairikh S. The characteristics and distribution of dentist workforce in Saudi Arabia: a descriptive cross-sectional study. Saudi Pharm J. 2017;25(8):1208–1216. doi:10.1016/j.jsps.2017.09.005
18. Machin D, Campbell M, Tan SB, Tan SH. Sample Size Tables for Clinical Studies.
19. Slayton RL, Urquhart O, Araujo MW, et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: a report from the American dental association. J Am Dent Assoc. 2018;149(10):837–849. doi:10.1016/j.adaj.2018.07.002
20. Tan HP, Lo EC, Dyson JE, Luo Y, Corbet EF. A randomized trial on root caries prevention in elders. J Dent Res. 2010;89(10):1086–1090. doi:10.1177/0022034510375825
21. Horst JA, Ellenikiotis H, Milgrom PM, UCSF Silver Caries Arrest Committee. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016;44(1):16.
22. Crystal YO, Marghalani AA, Ureles SD, et al. Use of silver diamine fluoride for dental caries management in children and adolescents, including those with special health care needs. Pediatr Dent. 2017;39(5):135E–45E.
23. Nelson T, Scott JM, Crystal YO, Berg JH, Milgrom P. Silver diamine fluoride in pediatric dentistry training programs: survey of graduate program directors. Pediatr Dent. 2016;38(3):212–217.
24. Crystal YO, Janal MN, Hamilton DS, Niederman R. Parental perceptions and acceptance of silver diamine fluoride staining. J Am Dent Assoc. 2017;148(7):510–518. doi:10.1016/j.adaj.2017.03.013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.