Back to Journals » International Journal of General Medicine » Volume 13
Knowledge of Basic Neonatal Resuscitation and Associated Factors Among Midwives and Nurses in Public Health Institutions in Eastern Ethiopia
Authors Sintayehu Y ![]() , Desalew A
, Desalew A ![]() , Geda B
, Geda B ![]() , Shiferaw K
, Shiferaw K ![]() , Tiruye G
, Tiruye G ![]() , Mulatu T
, Mulatu T ![]() , Mezmur H
, Mezmur H ![]()
Received 28 March 2020
Accepted for publication 12 May 2020
Published 27 May 2020 Volume 2020:13 Pages 225—233
DOI https://doi.org/10.2147/IJGM.S255892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yitagesu Sintayehu, Assefa Desalew, Biftu Geda, Kasiye Shiferaw, Getahun Tiruye, Teshale Mulatu, Haymanot Mezmur
Haramaya University College of Health and Medical Sciences, School of Nursing and Midwifery, Harar, Ethiopia
Correspondence: Yitagesu Sintayehu Email [email protected]
Background: Neonatal resuscitation is a means to restore life to a baby from the state of asphyxia. It is a single intervention of birth asphyxia. Over 1.2 million African babies are supposed to die in the first four weeks of their life and many of them in the first 24 hours of birth in Sub-Saharan Africa. The major cause of early neonatal death is neonatal asphyxia, which can be prevented by neonatal resuscitation. However, there is limited evidence on midwives’ and nurses’ knowledge of neonatal resuscitation in the study area. Therefore, this study aimed to assess the knowledge of midwives and nurses about neonatal resuscitation and its associated factors.
Methods: This facility-based cross-sectional study was done on 427 midwives and nurses, who were selected using simple random sampling technique. Data were collected on facility type, availability of essential equipment, socio-demographic characteristics, working unit, professional experience, in-service training, and knowledge of neonatal resuscitation. First-degree holder midwives collected the data using a pre-tested face-to-face interviewer-administered questionnaire. Bivariate and multivariate logistic regression was used to analyze the association between the dependent and independent variables.
Results: The study showed that 9.8% of the study participants had good knowledge about neonatal resuscitation. Factors significantly associated with knowledge of neonatal resuscitation were being trained on newborn resuscitation (AOR = 3.79, 95% CI: 1.73, 8.32), being unmarried (AOR = 2.36, 95% CI: 1.11, 5.02), holding bachelor sciences degree or above (AOR = 2.67, 95% CI: 1.11, 6.47), and working under West Hararghe health institutions (AOR = 0.30, 95% CI: 0.10, 0.88).
Conclusion: The study participants had low knowledge of neonatal resuscitation. Being unmarried, holding bachelor sciences degree or above, being trained on neonatal resuscitation, and working under West Hararghe health institutions were factors associated with the knowledge of the study participants on neonatal resuscitation.
Keywords: neonate, neonatal resuscitation, newborn, knowledge
Background
Neonatal resuscitation (NR) is a means to restore life to a baby from the state of asphyxia. It is a single intervention of birth asphyxia.1 Resuscitation of a neonate is more challenging than that of an adult or even older infant or child.2 Basic newborn resuscitation refers to airway clearing (suctioning if required), head positioning, and positive pressure ventilation with bag and masks.3
Annually, approximately four million babies die within the first month of life, of these deaths about 99% occur in low-middle income countries, where most births occur at home, without a skilled attendant.3 Nearly 1.2 million African babies are assumed to die in the first four weeks of their life, and half of the deaths occur in the first 24 hours of birth. This is particularly true in Sub-Saharan African countries.4,5
Neonatal mortality is an indicator of a country’s socio-economic condition and quality of life. A large proportion of maternal and neonatal deaths occur during the 48 hours after delivery, which is a critical time for monitoring complications arising from the delivery.6,7
In the short term, asphyxia could lead to multi-organ dysfunction or even death, whereas in the long term, childhood survivors of neonatal hypoxic-ischemic encephalopathy might develop cerebral palsy, developmental delay, visual, hearing, and intellectual impairments; epilepsy, and learning and behavioral problems.8 Despite the important advances in perinatal care in the past decades, neonatal mortality and morbidity have remained a serious problem, and thus it is critical to address its main causes, which often differ from the causes of death for older children. Preterm birth, intrapartum-related complications (birth asphyxia or lack of breathing at birth), infections and birth defects cause most neonatal deaths.9
Immediate newborn assessment and stimulation reduce both intrapartum related and preterm related deaths by 10%.10 However, studies done in Kenya and Nepal have reported that a shortage of equipment and health provider’s knowledge are problems with NR performance.11,12 Additionally, maintaining knowledge of resuscitation is a challenge, particularly in settings where providers attend very few deliveries and infrequently resuscitate newborns.13,14 Current trends predict that close to 26 million newborns will die between 2019 and 2030. These deaths can be prevented through quality antenatal care, skilled care at birth, postnatal care for mothers and babies, and care of small and sick newborns.15 Neonatal resuscitation and comprehensive emergency obstetric care are among those recommended to reduce deaths due to intrapartum-related events.16 In short, knowledge of health care providers about NR is of crucial importance.17 In resource-poor areas, nurses and midwives are the medical persons available to perform neonatal resuscitation.18
Midwives and nurses are health care providers who are able to provide promotive, preventive, curative and rehabilitative services at all levels of the health care system. Midwifery and nursing training in Ethiopia offered in three ways in both public and private science and higher educations: the diploma, the post-basic, and the direct BSc (Bachelor of Sciences) degree qualification in midwifery and nurse. Diploma and direct BSc degree in midwifery and nurse is open to all senior high school graduates depending on their achieved score of national exam criteria. The post-basic entry is available as post-diploma. The diploma and the post-basic program runs for three years and four years for the direct BSc degree program and given their certificate when they attain the requirement per Ministry of Science and Higher Education of Ethiopia. In addition to these, some midwives and nurses are given in-service training that can help them to give quality care at where they assigned.
However, there is limited evidence on midwives’ and nurses’ knowledge of neonatal resuscitation (ie, crucial to overcome death due to asphyxia) and its associated factors in Eastern Ethiopia. Therefore, this study aimed to identify knowledge of basic neonatal resuscitation and associated factors among midwives and nurses in public health institutions in Eastern Ethiopia.
Methods and Materials
Study Area
The study was conducted in the eastern part of Ethiopia (i.e., Harari Regional State, Dire Dawa City Administration, and West and East Hararghe zones of the Oromia Regional state). There were 14 public hospitals and 221 public health centers in the study area. These public health institutions have 7816 health care workers (of whom 3256 were midwives and nurses) who serve 6,565,406 populations.
Study Design and Population
A health facility-based cross-sectional study was employed among midwives and nurses who were working in public health institutions in Eastern Ethiopia from October 1 to December 15, 2018.
Sample Size Determination and Procedure
After calculating the sample size for both objectives, we selected larger sample size. A single population proportion formula; n = (Zα/2)2pq/d2 whereas, P (78.8%) was the prevalence of knowledge taken from a previous study.19 95% confidence level, and 5% margin of error and 1.5 design effect. By adding 15% non-response, the final sample size was 442 study participants. There were four clusters in the study area: Harari regional state, Dire Dawa city administration, East Hararghe, and West Hararghe zones of the Oromia Regional state. From these four clusters, 28 public health institutions were selected using a simple random sampling method. Then midwives and nurses were selected using a simple random sampling method with proportional allocation to sample size to health facilities.
Data Collection and Quality Control
Data were collected from the study subjects (as well as the heads of the selected health institutions) in a pre-selected comfortable setting and using a pre-tested face-to-face interview administered questionnaire using paper printed English version language. Data were collected on facility type, availability of essential resuscitation equipment, socio-demographic characteristics of participants, current working unit, years of professional experience, whether a nurse or midwife received in-service training and knowledge related to neonatal resuscitation. We adopted a questionnaire based on model assessment forms in the Needs Assessment Toolkit (based on the Averting Maternal Death and Disability Program’s Needs Assessment taken from another study).20 The questionnaire was pre-tested on a similar population and corrections were made accordingly. Also, regular supervision has been done and filled questionnaires were checked daily. The data were cleaned and double data entry was done. The data collectors, who were BSc holders and experienced on maternal and neonatal care, and the supervisors (MPH graduates), were given a five-day training on the objectives, method, ethical issue of the study and questionnaire.
Measurement of Knowledge
Knowledge of midwives and nurses on neonatal resuscitation was determined using a set of 25 Yes/No questions. Each correct answer was valued at one point, and a wrong answer given zero points. Questions not answered were considered as wrong answers. Eventually, participants were then grouped into two categories based on their total score on the knowledge scale: good knowledge (score 80% or higher) and poor knowledge (score less than 80%), which have been used in different studies.11,20-23 after the overall cumulative mean score and the cumulative mean percentage score were calculated.
Data Processing and Analysis
After the data had been checked for completeness and internal consistency, they were coded and entered into the Epi data Version 3.1-computer software package and cleaned for inconsistency. Then, they were exported to SPSS Version 23 for further data cleaning and analysis. The respondents who answered more than 80% of the knowledge questions correctly were coded 1 (good knowledge) and 0 (poor knowledge) otherwise. Descriptive statistics were used to summarize the facility and provider characteristics. Also, a binary logistic regression was used to see the association between good knowledge and each independent variable. Variables that showed p ≤ 0.25 in the bivariate analysis were considered as candidates for multivariable logistic regression analysis; this was to control all possible confounders and to detect associated factors of good knowledge. Hosmer and Lemeshow goodness-of-fit tests were used to assess whether the necessary assumptions were fulfilled. The direction and strength of the statistical associations were measured by the odds ratio with 95% CI. Adjusted odds ratio (AOR) with 95% confidence intervals (CI) using a P-value< 0.05 was considered as statistically significant association with the outcome.
Ethical Considerations
Institutional ethical clearance was first sought from the Institutional Health Research Ethics Review Committee (IHRERC) at Haramaya University, College of Health and Medical Sciences. Next, permission letters were collected from Regional and City administration Health Bureaus, zonal and Woreda health offices, and health facility officials. During data collection with each participant was informed about the aim of the study. The data collectors discussed the issue of confidentiality and were taken informed, voluntary, written, and signed consent before the start of data collection. The respondents were assured of confidentiality by excluding their names during data collection.
Results
Socio-Demographic Characteristics
A total of 427 nurses and midwives participated in the study, with a 96.6% response rate. Two hundred fifty-three (59.5%), participants were in the age range of 25–34 years with mean age ± SD (28.4 ± 7.05), female (60%), and married (57%). Moreover, 46.8% were Orthodox Christians, 66.7% were nurses, and 68.4% were bachelor degrees and above education. Two hundred sixty-three nurses and midwives had 1–5 years of work experience (Table 1).
 |
Table 1 Socio-Demographic Characteristics of a Study Conducted on Knowledge of Basic Neonatal Resuscitation and Associated Factors Among Midwives and Nurses Working in the Public Health Institutions in Eastern Ethiopia, 2018 [n = 427] |
Exposure of Nurses and Midwives to Neonatal Resuscitation
The study showed that only one-fourth (25%) of the respondents were taken additional training on neonatal resuscitation. Nearly half of the study participants had performed resuscitation at least once with the basic training they took in college before graduation, and had ever worked in the delivery room (Figure 1).
 |
Figure 1 Exposure of a study conducted on knowledge of basic neonatal resuscitation among midwives and nurses working in the public health institutions in Eastern Ethiopia, 2018 [n = 427]. |
Health Facilities Characteristics
In this study, almost all the health facilities had neonatal resuscitation corners; 63% had sufficient newborn resuscitation guidelines and 85% had essential equipment for newborn resuscitation. The study participants were selected from these facilities: 29.7%, 25.1%, 23.2%, and 22% were from Dire Dawa city administration health facilities, Harari health facilities, East Hararghe health facilities, and West Hararghe health facilities, respectively. Nearly 80% of the study participants were working in a hospital setting whereas the rest were working in health centers (20%).
Knowledge of Neonatal Resuscitation
The study revealed that only one in ten of the nurses and the midwives had good knowledge of neonatal resuscitation (Figure 2).
 |
Figure 2 Level of knowledge of a study conducted on knowledge of basic neonatal resuscitation and associated factors among midwives and nurses working in the public health institutions, in Eastern Ethiopia, 2018 [n=427]. |
Additionally, most of the midwives and nurses scored high the variable depressed breathing for the birth asphyxia diagnosis and scored lowest the variable call for help for the response of preliminary steps of newborn resuscitation (Table 2).
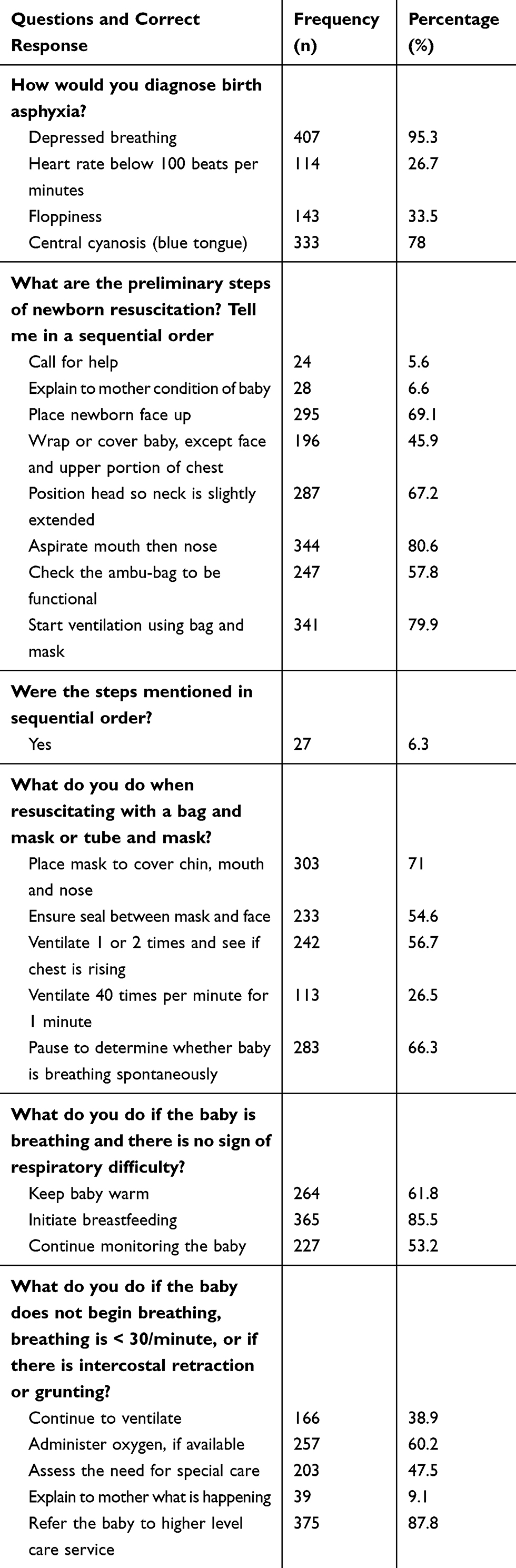 |
Table 2 Provider Knowledge: Percent of Providers Who Gave Correct Responses to Each Knowledge Questions Items on Newborn Resuscitation [427] |
Factors Associated with Knowledge of Neonatal Resuscitation
In the multivariable logistic regression analysis, the nurses and midwives who received in-training on newborn resuscitation were 3.79 times (AOR = 3.79, 95% CI: 1.73, 8.32) more likely to be knowledgeable about neonatal resuscitation compared to their counterparts. The analysis also revealed that the unmarried respondents were 2.36 times (AOR = 2.36, 95% CI: 1.11, 5.02) more likely to be knowledgeable than married ones. Moreover, the midwives and the nurses who had a bachelor’s degree and above in educational level were 2.67 times (AOR = 2.67, 95% CI: 1.11, 6.47) more likely to be knowledgeable about neonatal resuscitation compared to those on diploma level. Furthermore, midwives and nurses working in west Hararghe health facilities were (AOR = 0.30, 95% CI: 0.10, 0.88) less likely to be knowledgeable than those working in Dire Dawa city administration (Table 3).
 |
Table 3 Bivariate and Multivariate Analysis of a Study Conducted on Knowledge of Basic Neonatal Resuscitation and Associated Factors Among Midwives and Nurses Working in the Public Health Institutions, in Eastern Ethiopia, 2018 [n = 427] |
Discussion
Birth is a major challenge for a newborn to negotiate successfully from intrauterine to extrauterine life. The first few hours after birth is the most crucial period in the life of an infant for further growth and development, which is largely determined by the quality of care that the newborn receives.21
There was inadequate knowledge (9.8%) of basic neonatal resuscitation among the study subjects. The lack of knowledge and inability to cope with emergencies can lead to loss of life. In the multivariate analysis, being never married, BSc degree and above in educational status, receiving in-service neonatal resuscitation training, and working under West Hararghe health office health facilities were factors associated with the knowledge of the midwives and nurses about neonatal resuscitation.
This study revealed that about 9.8% of nurses and midwives had good knowledge of neonatal resuscitation. This finding is in the argument with the study Mangalore.2 But lower than the studies in Pune City, India, Northern Ethiopia, Kenya, Nigeria, Afghanistan, Poland, India, central Ethiopia, and Uganda.1,10,19-29 The difference might be due to the fact that most of the listed studies were conducted in a single facility and single urban town facilities. However, this finding was from a multi-facility level including the rural area which had no access to updated neonatal resuscitation information, had a shortage of supplies due to transportation problems, even no internet access. In contrast, it is higher than the study conducted in Tamale, Ghana.22 This difference might be due to that our sample size is higher and most of our participants are BSc degree and above in educational level.
After adjustment of logistic regression, the study showed that neonatal resuscitation training had a statistically significant association with the knowledge of the nurse and the midwives that is, the participants who had newborn resuscitation training were more likely to have a good knowledge when compared to those who did not have neonatal resuscitation training. This is probably because the trained providers had more updated information than the untrained participants. This finding is supported by studies conducted in Kenya, Nepal, Afghanistan, Tamale, India, Ghana, Tanzania, Ethiopia.11,12,20,22,23,30-33
Those who were unmarried were almost two times more likely to have good knowledge than their counterparts’ had. This is probably because most of the unmarried midwives and nurses have more time to read different updated resources/information on neonatal resuscitation than the married midwives and nurses. This is because married midwives and nurses might spars there time with their partners/children, but unmarried one uses this time to their reading. Also, unmarried are expected to be younger than married which implies that they have better capacity of retaining the reading materials and nearer to their educational award time. The BSc degree and above respondents were about two times more likely to have good knowledge than the diploma nurses and midwives had. This might be due to the fact that BSc degree and above providers could have a better chance of evidence-based reviewed information than diploma level providers. This finding is supported by a study conducted in Tamala.22
Nurses and midwives working in the health facilities of West Hararghe health facilities were less likely knowledgeable than nurses and midwives working in the Dire Dawa city administration health office. This might be due to the fact that the health facilities under Dire Dawa City Administration’s health facility might have access to more up to date information and close follow-up since most of their facilities were in the town, where there were easy transport accesses available. In addition, they might have close support from NGO’s while almost all facilities of West Harerghe were found in a rural area. The above variables were not reported or were not tested in other studies. Therefore, these associated variables will be one input for other studies that will be conducted in the future.
Conclusion
The level of knowledge among the midwives and nurses was very low. Being unmarried, holding BSc degree and above in educational status and received in-service neonatal resuscitation training had a positive influence on the knowledge of midwives and nurses about neonatal resuscitation, whereas working in West Hararghe health facility had less influence on the respondents knowledgeable on neonatal resuscitation. The governing office and providers should try to plan neonatal resuscitation training and upgrade nurses and midwives with a diploma education level to a BSc degree or higher level.
Data Sharing Statement
All related data has been presented within the manuscript. The dataset supporting the conclusions of this article is available from the authors upon reasonable request.
Acknowledgment
First and for most, we thank CIRHT-Ethiopia for funding and Haramaya University, College of Health and Medical Sciences for their initiative idea and support to develop this work. We would like to thank all the respective Health Bureau for their support to give us the necessary data for the proposal development and department of midwifery for coordinating this project. Our thanks also go to our data collectors, the participants involved in the study and Mr. Asfachew Balcha for English language revision.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Devi S, Upendra S, Barde S. A study to assess the effectiveness of Neonatal resuscitation Programme, First Golden minute certified training Course on knowledge and skill set of Nurses working in selected Hospital of Pune city. Int J Sci Res. 2015;4(2277):432–435.
2. Benazeera SGS, Umarani J. Assessment of student’s knowledge on neonatal resuscitation. J Biomed Pharm Res. 2014;3(2):67–71.
3. Agravat N. mHealth and Neonatal Resuscitation. A Review of Interventions, Approaches, and Applications; United Nations Foundation. 2013:1–40.
4. Oza S, Lawn JE, Hogan DR, Mathers C, Cousens SN. Neonatal cause-of-death estimates for the early and late neonatal periods for 194 countries: 2000–2013. Bull World Health Organ. 2015;93(1):19–28. doi:10.2471/BLT.14.139790
5. Lawn J, Mongi P, Cousens S. Africa’s Newborns-Counting Them and Making Them Count. Opportunities for Africa’s Newborns: Practical Data, Policy, and Programmatic Support for Newborn Care in Africa. The Partnership for Maternal, Newborn and Child Health;2006:12.
6. Central Statistical Agency (CSA) [Ethiopia]. Ethiopia Mini Demographic and Health Survey 2014, Addis Ababa, Ethiopia; 2014:1–81
7. United Nations Development Programme. Measuring Human Development, a Primer; 2007:1–173
8. Chiabi A, Nguefack S, Mah E, et al. Risk factors for birth asphyxia in an urban health facility in Cameroon. Iran J Child Neurol. 2013;7(3):46–54. doi:10.22037/ijcn.v7i3.3473
9. United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Levels & Trends in Child Mortality: Report 2019, Estimates Developed by the United Nations Inter-Agency Group for Child Mortality Estimation. New York: United Nations Children’s Fund; 2019.
10. Lee AC, Cousens S, Wall SN, et al. Neonatal resuscitation and immediate newborn assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect. BMC Public Health. 2011;11(Suppl 3):S12. doi:10.1186/1471-2458-11-S3-S12
11. Murila F, Obimbo MM, Musoke R. Assessment of knowledge on neonatal resuscitation amongst health care providers in Kenya. Pan Afr Med J. 2012;8688:4–9.
12. Kc A, Wrammert J, Nelin V, Clark RB, Ewald U, Peterson S. Evaluation of Helping Babies Breathe Quality Improvement Cycle (HBB-QIC) on retention of neonatal resuscitation skills six months after training in Nepal. BMC Pediatr. 2017;1–9. doi:10.1186/s12887-017-0853-5
13. Wall SN, Lee AC, Niermeyer S, et al. Neonatal resuscitation in low-resource settings: what, who, and how to overcome challenges to scale up? Int J Gynaecol Obstet. 2010;107(Suppl1):S47–S64. doi:10.1016/j.ijgo.2009.07.013
14. Coffey P, Kak L, Narayanan I, et al. Newborn Resuscitation Devices, Prepared for the United Nations Commission on Life-Saving Commodities for Women and Children; New York: United Nations. 2012:32.
15. World Health Organization. Child Mortality 2019. Levels & Trends in Child Mortality; 2019.
16. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–3035. doi:10.1016/S0140-6736(16)31593-8
17. Berglund S, Norman M. Neonatal resuscitation assessment: documentation and early paging must be improved! Arch Dis Child Fetal Neonatal Ed. 2012;97(3):F204–8. doi:10.1136/archdischild-2011-300295
18. Basu M. A study on knowledge and practice of neonatal resuscitation among nursing staff. Sri Lanka J Child Health. 2014;43(1):38–40. doi:10.4038/sljch.v43i1.6660
19. Ogunlesi T, Dedeke O, Adekanmbi F, Fetuga B, Okeniyi A. Neonatal resuscitation: knowledge and practice of nurses in western Nigeria. South African J Child Heal. 2008;2(1):23–25. doi:10.7196/sajch.80
20. Kim YM, Ansari N, Kols A, et al. Assessing the capacity for newborn resuscitation and factors associated with providers’ knowledge and skills: a cross-sectional study in Afghanistan. BMC Pediatr. 2013;13:140. doi:10.1186/1471-2431-13-140
21. Gebreegziabher E, Aregawi A, Getinet H. Knowledge and skills of neonatal resuscitation of health professionals at a university teaching hospital of Northwest Ethiopia. World J Emerg Med. 2014;5(3):
22. Alhassan A, Fuseini AG, Osman W, Basour Adam A. Knowledge and experience of neonatal resuscitation among midwives in tamale. Nurs Res Pract. 2019;2019:3652608. doi:10.1155/2019/3652608
23. Abrha MW, Asresu TT, Araya AA, Woldearegay HG. Healthcare Professionals’ Knowledge of Neonatal Resuscitation in Ethiopia: analysis from 2016 National Emergency Obstetric and Newborn Care Survey. Int J Pediatr. 2019;2019:8571351. doi:10.1155/2019/857
24. El Fattah NA, Zein El Dein NA. Assessment of Quality of Nursing Care Provided Immediately after Birth at University Hospital in El kom-Minoufiya, Egypt. Life Sci J. 2012;9(4):2115–2166.
25. Szarpak Ł. What we know about neonatal resuscitation? Randomized survey study. Emerg Med. 2013;3:59–66.
26. Chandregowda DC, Prakash GM, Anikethan GV. A cross-sectional study on awareness of Basic Life Support among final year students and interns in a medical college in Mandya, Karnataka. Sch J Appl Med Sci. 2016;4(6):2278–2281. doi:10.21276/sjams.2016.4.6.84
27. Currie S, de Graft-johnson J, Galloway R, Sheehan C, Smith J Interventions for impact in essential obstetric and newborn care.
28. Mirkuzie AH, Sisay MM, Reta AT, Bedane MM. Current evidence on basic emergency obstetric and newborn care services in Addis Ababa, Ethiopia; a cross sectional study. BMC Pregnancy Childbirth. 2014;14:354. doi:10.1186/1471-2393-14-354
29. Ayiasi RM, Criel B, Orach CG, Nabiwemba E, Kolsteren P. Primary healthcare worker knowledge related to prenatal and immediate newborn care: a cross sectional study in Masindi, Uganda. BMC Health Serv Res. 2014;14:65. doi:10.1186/1472-6963-14-65
30. Vijayan A. Effect of structured teaching programme on knowledge and skills on neonatal resuscitation. Int J Adv Res. 2015;3(7):1200–1205.
31. Subbiah N, Sarin J, Geetanjali JS. Effectiveness of educational intervention on neonatal resuscitation among nursing personnel. TT -. Heal Popul Perspect Issues. 2012;35(1):36–45.
32. Bookman L, Engmann C, Srofenyoh E, et al. Educational impact of a hospital-based neonatal resuscitation program in Ghana. Resuscitation. 2010;81(9):1180–1182. doi:10.1016/j.resuscitation.2010.04.034
33. Makene CL, Plotkin M, Currie S, et al. Improvements in newborn care and newborn resuscitation following a quality improvement program at scale: results from a before and after study in Tanzania. BMC Pregnancy Childbirth. 2014;14:381. doi:10.1186/s12884-014-0381-3
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.