Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Knowledge of and Attitudes Towards Standard Care in Patients with COPD
Authors Zimmermann M ![]() , von Plessen CM
, von Plessen CM ![]() , Kroppen D, Stanzel SB, Berger M, Wollsching-Strobel M, Feldmeyer F, Kellner C, Mathes T, Windisch W
, Kroppen D, Stanzel SB, Berger M, Wollsching-Strobel M, Feldmeyer F, Kellner C, Mathes T, Windisch W ![]() , Majorski DS
, Majorski DS ![]()
Received 30 July 2024
Accepted for publication 22 March 2025
Published 29 April 2025 Volume 2025:20 Pages 1287—1297
DOI https://doi.org/10.2147/COPD.S489395
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Maximilian Zimmermann,1 Charlotte Maria von Plessen,2 Doreen Kroppen,1 Sarah B Stanzel,1 Melanie Berger,1 Maximilian Wollsching-Strobel,1 F Feldmeyer,3 Cornelius Kellner,3 Tim Mathes,4 Wolfram Windisch,1,2 Daniel S Majorski1
1Department of Pneumology, Cologne Merheim Hospital Kliniken der Stadt Köln gGmbH, University Hospital of Witten/Herdecke University, Lung Clinic, Cologne, Germany; 2Faculty of Health, Witten/Herdecke University, Witten, Germany; 3Gemeinschaftspraxis Dr. Feldmeyer /Dr. Kellner Hagen, Germany; 4Biometry and Statistics, Georg-August-University Göttingen, Göttingen, Germany
Correspondence: Wolfram Windisch, Department of Pneumology, Cologne Merheim Hospital Kliniken der Stadt Köln gGmbH, Ostmerheimer Strasse 200, Cologne, North Rhine Westphalia, Germany, Email [email protected]
Objective: Health-related-quality-of-life is frequently reduced following intensive care treatment. Unwarranted or unwanted therapeutic interventions should be avoided at all costs. Since COPD patients are often faced with difficult decisions, an assessment was made of their desire for disease education. Our aim was to identify patients understanding of their disease and what their attitudes are towards different treatment options and whether this correlates to demographic factors.
Methods: The COPD-Assessment-Test (CAT) was used to measure subjective disease burden. The COPD-Questionnaire (COPD-Q) was used to assess subjects’ own knowledge of their disease. In addition, a specifically designed questionnaire was used to assess patient’s subjective level of desire to be educated on COPD-specific topics. A multiple linear regression analysis was performed to identify the demographic factors associated with a greater desire for disease-specific information.
Results: 127 patients (67.2± 8.8 years) were prospectively enrolled. Mean CAT score was 21.3± 8.9 (95% CI:1– 40). The desire for medical consultation was highly individual. In terms of vaccination, 31.5% of patients wished for more information while 34.6% wished for less. This also held true for information on long-term pharmacological therapy (29.1% vs 30.7%, respectively). Information on behaviour in case of emergencies as well as smoking cessation were wished for 38% and 42% of patients, respectively. Results of the COPD-Q showed that subjects were well-informed about specific topics (vaccination, etiology, emergency-inhaler) and less informed about long-term pharmacotherapy. In linear regression analyses, age (p=0.086), sex (p=0.906), education (p=0.833), health literacy (p=0.336) and burden of disease (p=0.296) did not influence patients´ desire for disease-specific information.
Conclusion: Based on our cohort, COPD patients wish for more medical information related to behaviour in emergency situations and smoking cessation. The desire for education on disease-specific topics did not naturally correlate with demographic characteristics. The provision of medical information to patients remains a highly individualized and essential part of patient care.
Trial Registration: German Clinical Trials Registry (DRKS00022109).
Keywords: COPD, medical education, CAT-score, COPD-Q, advanced care planning
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the three leading causes of death worldwide. Despite it being a preventable and treatable disease, COPD accounts for 6% of all deaths globally and poses a critical challenge to public health. Moreover, the burden of COPD is expected to increase due to continued exposure to risk factors and an ageing population.1 Modern medicine has been one of the main drivers of increased life expectancy, which has led to an ageing population, although many epidemiologically important diseases such as COPD remain incurable. It is, therefore essential to focus not only on prolonging survival, but also on achieving an acceptable health-related quality of life (HRQL) in patients with advanced chronic diseases. To assess disease burden in patients the COPD Assessment Test (CAT) was used. It is imperative that unwarranted or unwanted therapies are avoided at all costs. Modern healthcare is based on the historic approach to the treatment of acute injuries and illnesses, where healthcare professionals were regarded as experts and patients as passive recipients of medical care.2 However, in the context of chronic diseases such as COPD, a different model for high-quality healthcare is required in which more focus is placed on patient self-management and patient education.3 Subsequently, patients should be prepared to make informed decisions about interventions such as end-of-life and emergency therapies. However, for this purpose it is crucial that patients are adequately informed. Nonetheless, the extent to which COPD patients understand their disease, as well as how they view it, remains poorly understood, particularly when it comes to making decisions about treatment approaches. Therefore, the present study was designed to assess how well patients with COPD understand their disease and what their attitudes are towards different treatment options. The study aims to investigate potential associations between participants’ level of knowledge and their expressed desire for medical consultation or education.
Materials and Methods
Study Design and Measurements
This trial was designed as a prospective observational cross-sectional trial. Patients were interviewed either in an outpatient setting (hospital outpatient clinic) or at a private pneumology practice to reduce single-center bias from 06/2020 to 01/2021. Patients were screened consecutively for eligibility to minimize patient selection bias. Patients received detailed written and verbal information about the study. All patients were informed that there would be no detriment or changes to their therapy if they refused to participate. After demographic data were collected, patients completed the three questionnaires described above. If patients were unable to read or write their answers on the questionnaires, the questions were read out aloud by an interviewer and the patient’s responses were documented accordingly. Relatives and caregivers were not allowed to answer the questionnaires. In order to minimize information bias the questionnaires were not handled by anyone involved in the day-to-day care of the patients.
The study protocol was approved by the ethics committee at the Witten/Herdecke University (Processing number 188/2019). All participants were informed about the purpose of the trial. The study was performed in accordance with the ethical standards laid down in the Declaration of Helsinki and was registered at the German Clinical Trials Registry (DRKS00022109). The study was undertaken at the Department of Pneumology, Lung Clinic, Cologne Merheim Hospital, Witten/Herdecke University, Germany as well as at a private pneumology practice in Hagen, Germany, led by Dr. Feldmeyer, MD and Dr. Kellner, MD.
Inclusion and Exclusion Criteria
Adult COPD patients (≥18 years) at different GOLD stages (I to IV; FEV1/IVC <70%) were included in the study upon signing the written consent form. Patients already established on long-term invasive ventilation were excluded. Further exclusion criteria were mental retardation and deafness.
Questionnaires
To assess disease burden in patients, a specialized questionnaire known as the COPD Assessment Test (CAT) was employed.4 The CAT encompasses eight key aspects: energy levels, sleep quality, confidence in leaving the home, capability of engaging in household activities, experience of breathlessness, chest tightness, mucus production, and frequency of coughing. Each component is evaluated using a five-point Likert scale, where 0 indicates that the statement does not apply at all, and 5 indicates that the statement applies very well to the individual, leading to a score range from 0 = no symptom burden to 40 = maximum of COPD symptom burden.
In order to assess patients’ knowledge of their own disease, the COPD Questionnaire (COPD-Q) was employed. The COPD-Q is designed to assess how patients comprehend their condition. Developed by Maples et al in 2010, the COPD-Q is specifically tailored to individuals with low health literacy.5 It comprises 13 questions pertaining to the disease, with participants being prompted to respond with “true”, “false”, or “not sure.” The inclusion of this questionnaire in the study serves the purpose of delving into the participants’ overall knowledge about their illness. The focus is on identifying specific areas where further information may be required or where there is already a well-informed understanding.
To assess participants’ level of desire to be educated about their disease, a specifically designed questionnaire developed by an expert committee was used, whereby a range of topics of interest to COPD patients were covered. This questionnaire was designed by single person interviews and comprised a committee of respiratory therapists, pulmonologists, intensive care specialists, patients and psychologists. Answers upon relevant topics of possible interest for patients were accumulated and the 5 topics mentioned most were included. The 5 topics included at the end were: “Medical education in general”, “More medical education on vaccines”, “More medical education on behaviour in case of emergency”, “More medical education on long-term pharmacological-therapy options” “More medical education on modern therapies for smoking cessation”.
Analysis
This study was designed as a pilot study. A predominantly descriptive analysis of the data was planned, with a multifactorial analysis of variance to determine any correlations between the captured data. Confidence intervals of 95% were used for all questionnaire analyses. Due to the lack of comparable studies in the literature, it was not possible to statistically calculate the power and, in turn, sample size. To represent the different COPD-stages, at least 20 patients were included from each GOLD category (ranging from I to IV). Statistical relevance was assumed at a p-value <0.05.
The study was based on the principle of random sampling. A multifactorial analysis of variance was used to assess factors associated with the subjective wish for medical consultation/information. The dependent variable was the preference for medical consultation/information, and the independent variables used to identify a statistical correlation with this preference were age, sex, health-literacy (COPD-Q), level of education and perceived disease burden (CAT score). IBM SPSS 28.0 was used for all analyses.
Results
A total of 139 COPD patients were screened for eligibility and 127 patients were consecutively enrolled in the study (Figure 1). Demographic data and COPD symptom burden (CAT score) are shown in Table 1. The level of schooling completed by each patient was determined and summarised in Figure 2. The cohort represented each COPD GOLD stage with the least number of patients in GOLD stage I (n = 21; 16.6%) and the most in GOLD stage II (n = 45; 35.4%). Twenty-four subjects (18.9%) represented GOLD stage III and 37 patients (29.1%) represented GOLD stage IV, respectively. At the time of enrollment, around 50% of subjects were undergoing treatment for chronic hypoxemic respiratory failure in the form of either non-invasive ventilation (NIV) alone (n=17;13.4%), long-term oxygen therapy (LTOT) alone (n=14; 11.0%), or a combination of both (n=33; 26.0%). The primary source of COPD-related information for the patient was the pneumologist, followed by the internet (Figure 3). Regarding patient wish for disease-specific medical information, topic-related differences were found. While 36% (14% agree; 22% strongly agree) wished for more medical information in general, 54% desired more education on how to behave in the case of an emergency (16% agreed; 38% strongly agreed). Half the patient cohort said they did not require more education on long-term pharmaceutical options (19% disagree; 31% strongly disagree) (Figure 4). In terms of health literacy on the subject of COPD, most patients correctly answered question (Q) 9 (“People with COPD may feel short of breath”) and Q11 (“People with COPD should have a flu shot every year”), whereas Q4 (“COPD can be prevented”), Q5 (“People can stop taking their long-acting breathing medications (inhalers) when their COPD symptoms get better”) and Q13 (“COPD can be reversed”) were the most frequently incorrectly answered questions (Figure 5).5
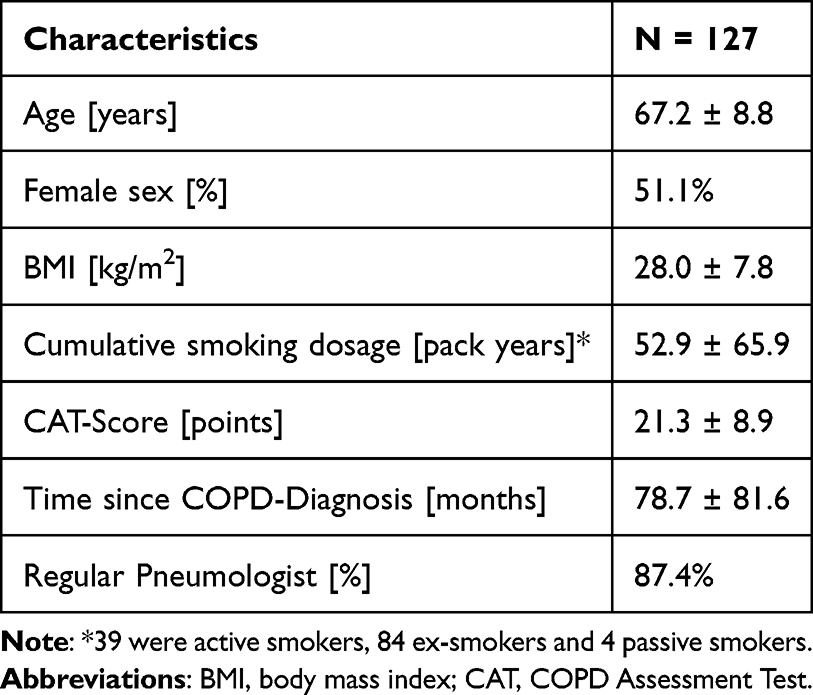 |
Table 1 Demographical Data |
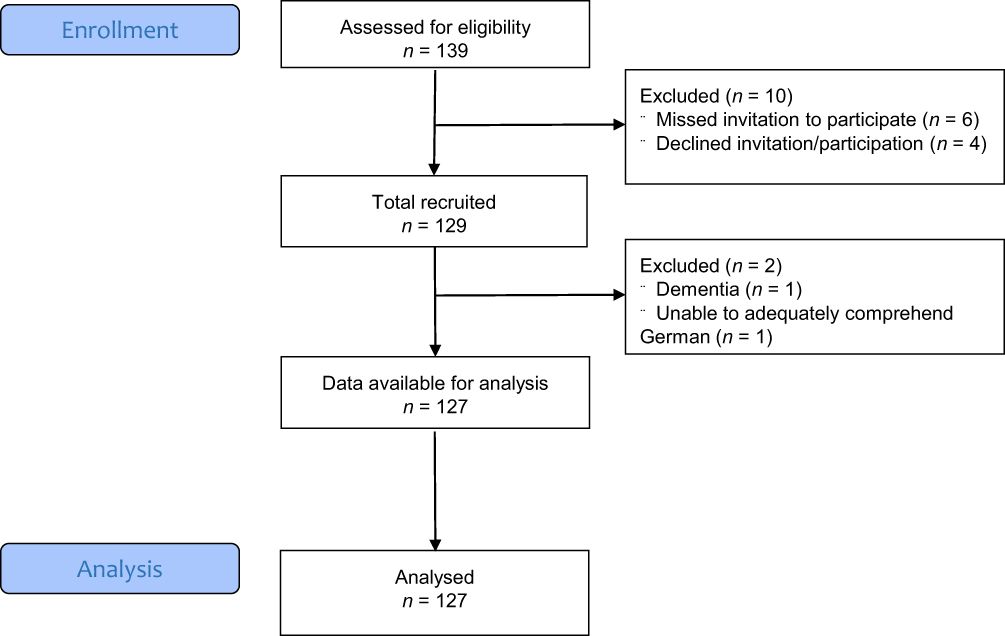 |
Figure 1 Study flow chart. |
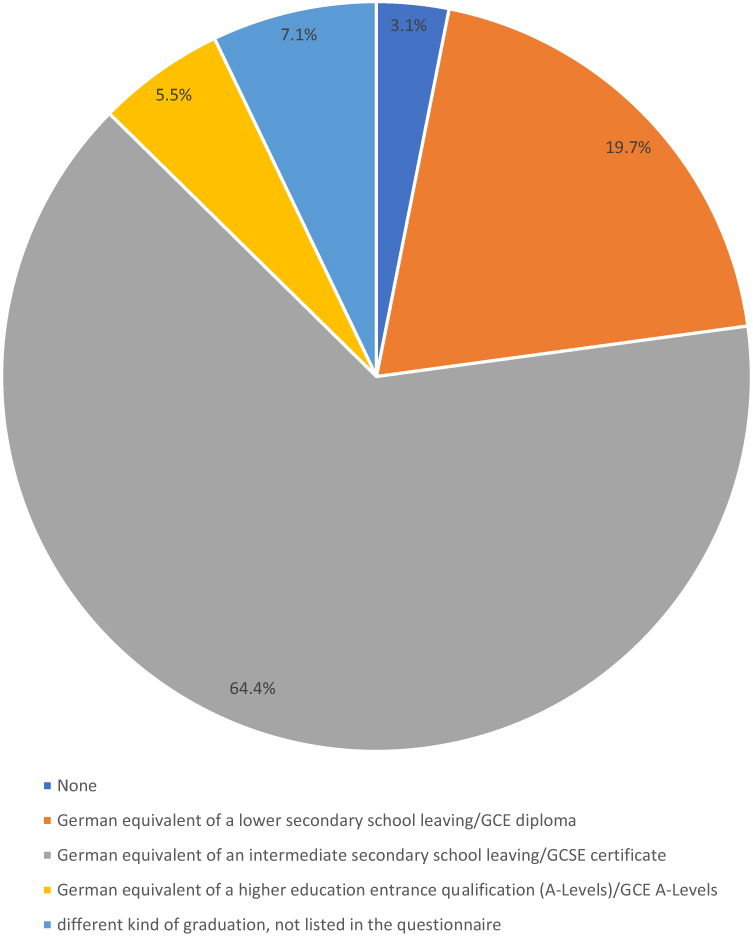 |
Figure 2 Distribution of educational levels within patient cohort. |
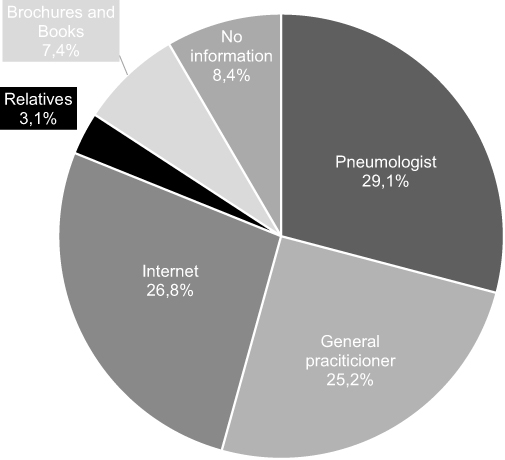 |
Figure 3 Primary source of medical information. |
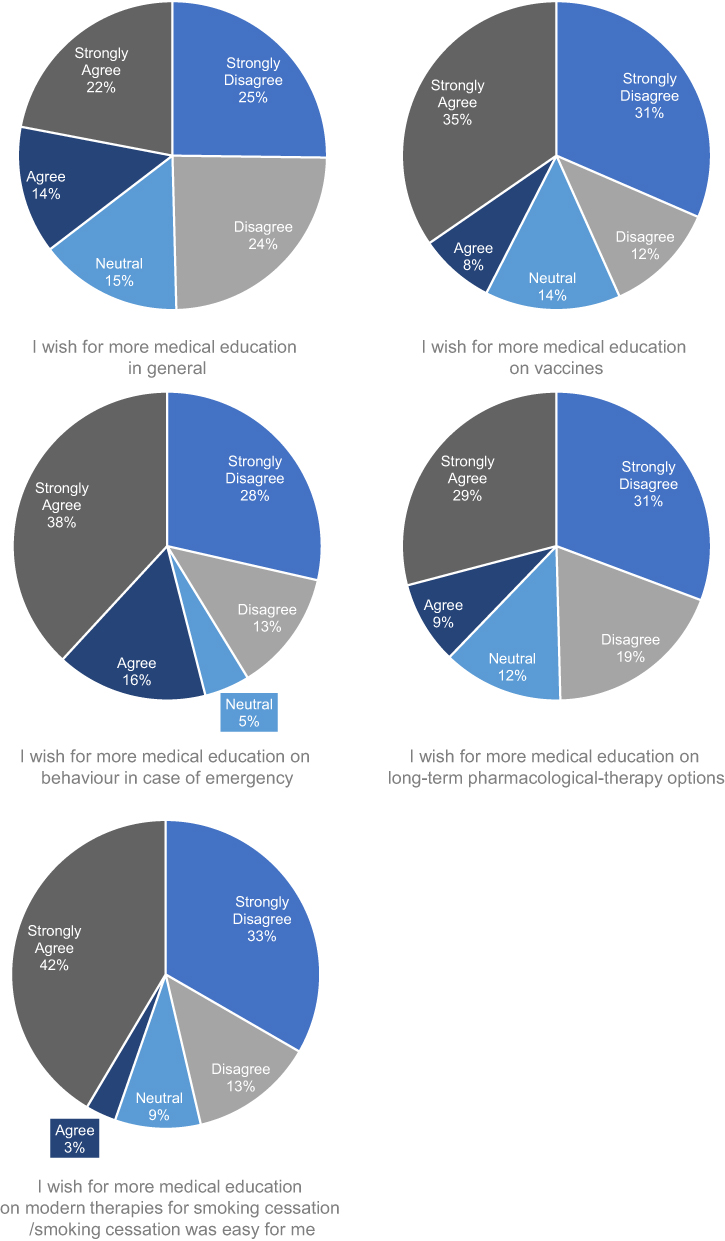 |
Figure 4 Subjective desire for disease education structured according to topics. |
 |
Figure 5 Distribution of correctly and incorrectly answered responses to the COPD-Q Questionnaire5 (expressed as percentages). True items are 1, 2, 4, 6, 8, 9, 10, 11. False items are 3, 5, 7, 12, 13. |
In terms of the patient’s wish for disease-specific medical information, multifactorial analysis of variance did not show a statistically significant interaction between the effects of the subject sex (F (1,117) = 0.014, p = 0.906), subject level of education (F (4,117) = 0.306, p = 0.833) or subject age (F (1,117) = 3.005, p = 0.086). Given the high correlation between COPD GOLD stage and CAT score, an explicit correlation analysis between the wish for medical consultation and COPD stage was not performed. Kendall’s tau-b correlation between the wish for medical consultation and cohort health literacy (Kendall’s tau-b coefficient (τb) = −0.067, p = 0.336 and subjects’ CAT Score (τb = 0.07, p = 0.296) did not demonstrate a significant statistical difference. Explorative correlation analyses revealed that patients who wanted more general medical information about their disease trended towards also wanting it for all the items tested, namely, vaccines (τb = 0.497), behavior in case of an emergency (τb = 0.539), long-term pharmacological-therapy options (τb = 0.506) and options for smoking cessation (τb = 0.227).
Discussion
The main findings of the study are as follows: Firstly, a significant number of patients with a rather high symptom burden have the wish – or, in some cases, even a strong wish – to receive more medical information about their disease in general (36%). This general trend is even more pronounced for topics that are subjectively considered to be highly relevant, such as how to behave in emergency situations (54.3%), and modern approaches to smoking cessation (46.5%). On the other hand, and even larger proportion (49.3%) of patients had no desire for further medical education in general either feeling informed well enough or perhaps being disappointed with the healthcare system and their own state of health.
Secondly, the desire for medical information does not seem to correlate with demographic factors such as age, disease state, educational status, health literacy, or perceived disease burden. Therefore, this sensitive issue is highly individual and needs to be addressed in an equal and consistent manner in every patient constellation. Indeed, this observation is in contrast to our hypothesis that the desire for medical information would be higher in the later stages of the disease (GOLD III–IV). This also slightly contradicts prior research showing that the motivation to complete an advanced care plan is influenced by old age, female sex, a higher level of education or a longer disease duration.6 We were then again able to demonstrate that participants who actually wanted to receive more medical information, tended to want it to focus on all the areas explored in the present study (vaccines, emergency behavior, long-term pharmacological therapy, and smoking cessation options).
Thirdly, a significant proportion of participants (27%) indicated that they primarily obtain disease-specific information from the internet, with this medium being second place after the pneumologist (29.1%) for information, surpassing other information sources such as acquaintances and relatives (3.1%), brochures or books (9.4%) and even their own general practitioners (25.2%). Although it remains true, that more than half the patients have a health care provider as their primary source of information (27% pulmonologist, 25.2% general practitioner), the important role of the internet in providing disease-specific information is supported by several scientific trials, which demonstrated that it is increasingly being used by patients for this purpose, even those from older age groups.7–9 This is an important and emerging trend in medicine, especially because although we observe an increase in internet use, the quality of medical information is rather heterogeneous.10 The internet may therefore, if proper information sources are being used, play an exceptional role in providing low-threshold learning opportunities such as viewing video footage on open platforms.11
Analysis of the COPD-Q results in the present study revealed that most patients had a good appreciation of the need for vaccination (pneumonia and influenza), the degenerative nature of their disease, and that albuterol is a drug that can be used to treat shortness of breath. Notably, patients exhibited less certainty regarding the differential effects of their emergency/long-term-inhalers. This finding is of particularly importance, given that half the patient cohort indicated a lack of desire for further education about long-term pharmaceutical options. This suggests that patients are inadequately informed about long-term pharmaceutical therapy, despite this being an important treatment aspect. As a consequence, alternative forms of explanation and education must be established because the amount of accessible information appears to be limited, even when patient desire for information also appears to be low. Future patient education should therefore place greater emphasis on the differential effects of emergency inhalers versus long-term-inhalers, as well as the importance of continued long-term inhaler use. This could result in an increase in use of long-term inhalers among COPD patients, which has been demonstrated to reduce exacerbations.12 Finally, most participants (67.7%) had the understanding that COPD is primarily caused by smoking (or passive smoking), while many patients (43.9%) still believed that COPD cannot be prevented. A question that remains unanswered is why a certain group of patients did not wish to receive further medical information related to their disease. While these patients might deem it unnecessary because they already feel sufficiently informed, it is also possible that there are barriers such as fears, negative experiences, or feeling overwhelmed or embarrassed, which could lead to the refusal of disease education.13 Further research is needed to identify the reasons behind patients’ refusal of further education and to identify effective strategies for addressing them. With regard to specific one-off intervention procedures, a study by James et al found that most patients are interested in the same topics, which include pain management, rehabilitation and who will perform the intervention.14 In contrast, when it comes to long-term education of patients with chronic diseases, patient wishes often differ and are more individualistic. An illustrative example is the concept of advanced care planning, which is based on patients and doctors discussing future care plans in alignment with the patient’s wishes, goals and values, often in the later stages of life.15 Our findings confirm that providing patients with an education in chronic diseases such as COPD is highly individualistic and must be tailored to the patient’s wishes and needs. The current study has several limitations. As this was a pilot study, no primary endpoints could be designed and tested in advance; as a consequence, the results must be treated as explorative. Data collection was conducted using interviewer-administered and self-administered questionnaires. This may have introduced a performance bias. In addition, the study group decided against an exact interview script, which may have introduced an interview bias, although only three interviewers were involved and all received the same interview training beforehand. Nevertheless, this may have influenced participant responses and, in turn, the data.16 Approximately half of the participants were interviewed in a private pneumology practice, while the other half were interviewed in a lung clinic that collaborated closely with local pneumologists. This may have resulted in a sample that is not necessarily representative of the general COPD population, as plenty of COPD patients in the general population do not have regular visits with a pneumologist. Furthermore, the proportion of participants who indicated that they had received medical information from their pneumologist (29.1%) may also be disproportionately high in comparison to what the general population of patients with COPD has experienced. The self designed questionnaire was established by an expert committee in small group interviews, but wasn´t validated beforehand, which must be taken into consideration. The COPD-Q is a specifically designed questionnaire for a low health literacy collective and is hereby used in this trial close to, but not directly aligned with the specific goal in this study.
Conclusion
The desire for disease education among patients with COPD is highly individual and should be approached accordingly. Fundamental aspects of therapy that are clear to healthcare providers may not be understood by patients in the same way, such as the correct use of inhalation therapy, regardless of time since diagnosis. It is therefore recommended that caregivers regularly offer patients the chance to discuss relevant medical topics and proactively engage with the patients who express an interest learning more about their own disease. This can be achieved either through face-to-face meetings or online media, with the latter holding the possibility of being a reliable source of information.
Abbreviations
BMI, Body Mass Index; CAT-Score, COPD Assessment Test; COPD, Chronic obstructive pulmonary disease; COPD-Q, COPD-Questionnaire; DRKS, German Registry for clinical trials (German: Deutsches Register für klinische Studien); GOLD, Global Initiative for Chronic Obstructive Lung Disease; GCE, General Certificate of Education; GCSE, General Certificate of secondary Education; FEV1, Forced expiratory volume in 1 second; FVC, Forced vital capacity; LLN, Lower limit of normal; LTOT, Long-term oxygen therapy; NIV, Non-invasive ventilation; SD, Standard Deviation.
Data Sharing Statement
Data are available upon request from the corresponding author.
Ethical Data Sharing Statement
The authors do not intend to share individual de-identified participant data. The authors do only, without exception, share anonymized data with written permission given by each participant. The authors intend to publish an original and will not share any other information concerning this trial on other platforms. The data will be accessible through the publishing journal only.
Acknowledgments
We acknowledge all participants for the effort they devoted to this study. Furthermore, we thank Dr Sandra Dieni for helpful comments on the manuscript prior to submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors state that neither the study design, results, interpretation of the findings, nor any other subject discussed in the submitted manuscript was dependent on financial support.
Disclosure
The Cologne study group (SBS, MWS, DSM, DK, MZ, WW) received open research grants from Löwenstein Medical/Germany and GCE group/UK and by the Innovation Fund for Health Services Research (01VSF1905) of the German Federal Joint Committee. SBS, DSM, MWS, MZ received travel grants from companies dealing with mechanical ventilation products; MB, CVP, DK, FF, CK, TM have nothing to declare. DSM: received travel grants and speaking fees from companies dealing with mechanical ventilation and companies dealing with pharmaceutical therapeutics. MWS reports non-financial support from Chiesi GmbH, non-financial support from AstraZeneca GmbH, personal fees from Novartis AG, personal fees from CSL Behring, grants from Löwenstein medical SE&Co KG, outside the submitted work. MZ reports personal fees from Löwenstein medical, personal fees from Resmed medical, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD Science Committee Report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
2. Lawn S, Schoo A. Supporting self-management of chronic health conditions: common approaches. Patient Educ Couns. 2010;80(2):205–211. doi:10.1016/j.pec.2009.10.006
3. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
4. Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
5. Maples P, Franks A, Ray S, et al. Development and validation of a low-literacy Chronic Obstructive Pulmonary Disease knowledge Questionnaire (COPD-Q). Patient Educ Couns. 2010;81(1):19–22. doi:10.1016/j.pec.2009.11.020
6. Inoue M. The influence of sociodemographic and psychosocial factors on advance care planning. J Gerontol Soc Work. 2016;59(5):401–422. doi:10.1080/01634372.2016.1229709
7. Cutilli CC. Seeking health information: what sources do your patients use? Orthop Nurs. 2010;29(3):214–219. doi:10.1097/NOR.0b013e3181db5471
8. Lee K, Hoti K, Hughes JD, et al. Consumer use of “Dr Google”: a survey on health information-seeking behaviors and navigational needs. J Med Internet Res. 2015;17(12):e288. doi:10.2196/jmir.4345
9. Swoboda CM, Van Hulle JM, McAlearney AS, et al. Odds of talking to healthcare providers as the initial source of healthcare information: updated cross-sectional results from the Health Information National Trends Survey (HINTS). BMC Fam Pract. 2018;19(1):146. doi:10.1186/s12875-018-0805-7
10. Abdel-Wahab N, Rai D, Siddhanamatha H, et al. A comprehensive scoping review to identify standards for the development of health information resources on the internet. PLoS One. 2019;14(6):e0218342. doi:10.1371/journal.pone.0218342
11. Wollsching-Strobel M, Butt U, Majorski DS, et al. Evolution of web-based training videos provided by the German respiratory league for the correct inhalation technique. Respiration. 2022;101(8):757–765. doi:10.1159/000524712
12. Vogelmeier C, Buhl R, Burghuber O, et al. [Guideline for the diagnosis and treatment of COPD patients - issued by the German Respiratory Society and the German Atemwegsliga in Cooperation with the Austrian Society of Pneumology]. Pneumologie. 2018;72(4):253–308. doi:10.1055/s-0043-125031
13. Bester J, Cole CM, Kodish E. The limits of informed consent for an overwhelmed patient: clinicians’ role in protecting patients and preventing overwhelm. AMA J Ethics. 2016;18(9):869–886.
14. James JT, Eakins DJ, Scully RR. Informed consent, shared-decision making and a reasonable patient’s wishes based on a cross-sectional, national survey in the USA using a hypothetical scenario. BMJ Open. 2019;9(7):e028957. doi:10.1136/bmjopen-2019-028957
15. Dingfield LE, Kayser JB. Integrating advance care planning into practice. Chest. 2017;151(6):1387–1393. doi:10.1016/j.chest.2017.02.024
16. Pannucci CJ, Wilkins EG. Identifying and avoiding bias in research. Plast Reconstr Surg. 2010;126(2):619–625. doi:10.1097/PRS.0b013e3181de24bc
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.