Back to Journals » Infection and Drug Resistance » Volume 15
Knowledge, Attitudes, and Practices Toward the Coronavirus Disease 2019 (COVID-19) Pandemic in a Population Under Community-Wide Containment Measures in Southern Thailand
Authors Rerkswattavorn C ![]() , Chanprasertpinyo W
, Chanprasertpinyo W ![]()
Received 18 December 2021
Accepted for publication 4 June 2022
Published 1 November 2022 Volume 2022:15 Pages 6391—6403
DOI https://doi.org/10.2147/IDR.S354512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chaiwat Rerkswattavorn,1,2 Wandee Chanprasertpinyo1,2
1School of Medicine, Walailak University, Nakhon Si Thammarat, Thailand; 2Walailak University Hospital, Nakhon Si Thammarat, Thailand
Correspondence: Wandee Chanprasertpinyo, School of Medicine, Walailak University, Thai Buri, Tha Sala, Nakhon Si Thammarat, 80160, Thailand, Email [email protected]
Background: The coronavirus disease 2019 (COVID-19) outbreak has had a significant impact on public health and the socioeconomic system. While governments established community-wide containment measures to prevent further transmission, the number of patients continued to increase. For a better COVID-19 outbreak response, there is a need to better understand communities’ knowledge, attitudes and practices toward COVID-19.
Objective: Our main objective is to describe knowledge, attitudes, and practices toward COVID-19 in a population under community-wide containment measures.
Participants and Setting: Eligible participants affected by community-wide containment measures living in southern Thailand were included. A convenience sampling strategy was used to include the participants.
Methods: A descriptive cross-sectional survey was used in this study. We developed an online self-administered Thai-language questionnaire that included the respondents’ demographic profiles and questions regarding their knowledge, attitudes, and practices toward COVID-19. Piloting the questionnaire was performed in a small sample at Walailak University, Nakhon Si Thammarat.
Results: In total, 717 subjects were included in this study. Regarding the knowledge and practice assessments, most respondents knew about COVID-19 by browsing websites. The respondents were confident in their knowledge, understood the situation causing the COVID-19 outbreak and knew how to prevent it. However, there were still misunderstandings. Regarding the attitude assessment, only 56.4% (405/717) of the subjects scored greater than or equal to 80%.
Conclusion: COVID-19 misunderstandings render disease outbreaks more difficult to control. These misunderstandings may result from outdated or inaccurate online information. It is essential to gain knowledge from a reliable source for proper understanding.
Keywords: coronavirus disease 2019, COVID-19, knowledge, attitudes, practices, pandemic
Introduction
In December 2019, an outbreak of the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) responsible for coronavirus disease 2019 (COVID-19) occurred in Wuhan City, Hubei Province, China.1 In January 2020, the World Health Organization (WHO) declared the outbreak a public health emergency of international concern.2 The first officially confirmed COVID-19 patient in Thailand was reported on January 13, 2020.3 In March 2020, patients from among a cluster of patients with COVID-19 in Iran and Malaysia traveled to the southern provinces in Thailand, Nakhon Si Thammarat and Surat Thani (Walailak University is located between these two provinces) and were potentially exposed to numerous persons.4 As of July 17, 2020, there were 744 confirmed cases of COVID-19 distributed throughout southern Thailand (Figure 1).4
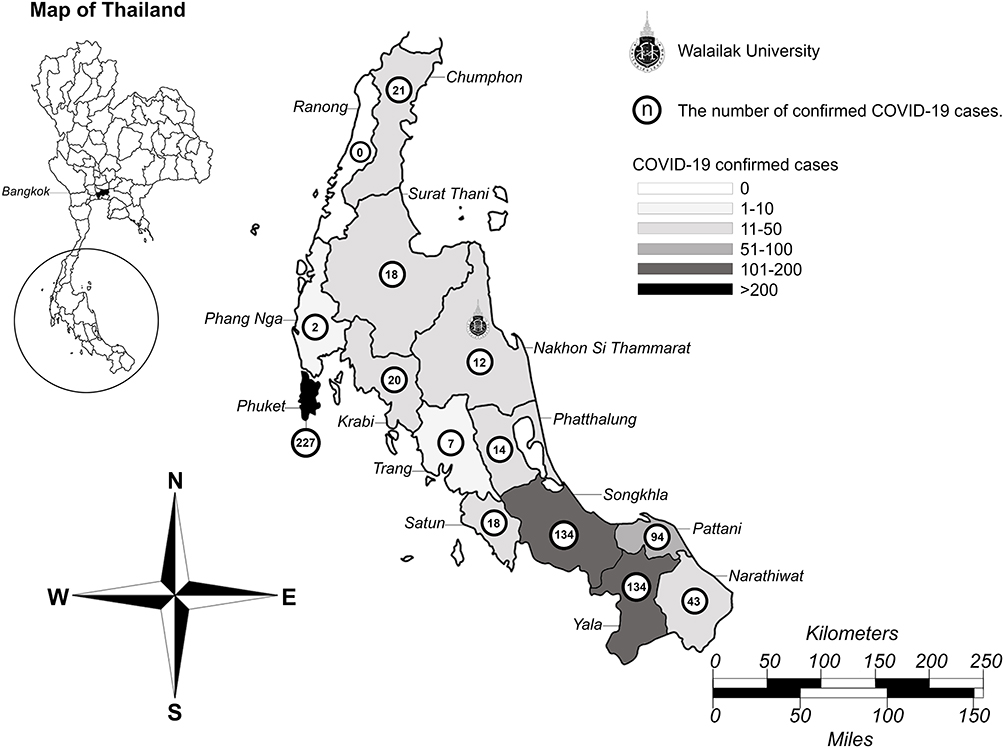 |
Figure 1 Distribution of the COVID-19 outbreak in southern Thailand. A map of southern Thailand showing the location of confirmed COVID-19 cases. There were 744 confirmed cases of COVID-19 in southern Thailand as of July 17, 2020. Source: Department of Disease Control (DDC), Ministry of Public Health (MOPH), Thailand. |
The current COVID-19 pandemic has affected people of all ages, including children, adults, and elderly individuals. COVID-19 can affect children, especially those under five years of age, in several ways. In addition to physical illness, many young children’s mental, emotional, and social well-being have been affected. Trauma faced at this developmental stage may have long-term consequences across their lifespan.5 Among adults and elderly individuals, the risk of severe illness with COVID-19 (hospitalization, admission to the intensive care unit (ICU), intubation or mechanical ventilation, or death) increases with age; however, adults of any age with certain underlying medical conditions (eg, type 2 diabetes mellitus, obesity, heart failure, chronic kidney disease, etc.) are also at an increased risk of severe illness.6
Usually, outbreaks of deadly infectious diseases trigger considerable fear and anxiety among the public, especially when the death toll rapidly climbs. The COVID-19 outbreak has had a significant impact on public health and the socioeconomic system in many countries. Many resources (eg, funds, laboratory testing, and medical personnel) are needed to respond to the outbreak. Having recognized the risk of the COVID-19 outbreak, health authorities should be on alert and re-examine their capacity to manage an epidemic if such a mishap should recur in the future.7 Many governments established various control measures to prevent any further transmission and minimize the number of additional cases. The Thai government applied community-wide containment measures, including increased social distancing among community members, cancelling public gatherings, and implementing mandatory 14-day self-quarantine periods for individuals at risk of infection or those with COVID-19.
As a lesson from the past, quarantine measures have been used to control and eradicate the spread of infectious diseases, such as severe acute respiratory syndrome (SARS), with success. SARS was eventually controlled by interrupting all human-to-human transmission, ie, prompt isolation of patients, strict enforcement of the quarantine of all contacts, and community-level quarantine.8 Although quarantine measures were effective against the SARS outbreak, they were tarnished by the negative influences of socioeconomic issues, generalized fear, lack of understanding, posttraumatic stress disorder (PTSD), depression, discrimination, and rebellion.9–12
For a better COVID-19 outbreak response, there is a need to understand communities’ knowledge, attitudes, and practices toward COVID-19. The results of a previous study concerning severe respiratory tract infections due to viral pandemics other than COVID-19 suggested that extensive standardized educational health campaigns and assessment of prior knowledge are necessary for preventing disease outbreaks by improving public awareness.13–15 In addition, mitigating fear and discrimination directed toward persons infected with SARS can be important in controlling outbreaks.16
Therefore, our main objective is to describe the knowledge, attitudes, and practices toward COVID-19 in a population under community-wide containment measures, especially in southern Thailand, where our university is located. Our research findings may be essential for designing information, education, and communication materials and policy making. These are crucial components for responding to future pandemics and improving health outcomes.
Methods
Study Design
In brief, we conducted a descriptive cross-sectional survey of the population under community-wide containment measures in southern Thailand from May 1 to July 31, 2020. Due to social distancing measures during the COVID-19 pandemic, we developed an online self-administered Thai-language questionnaire using Microsoft Forms® (see Appendix). The questionnaire included the respondents’ demographic profiles and questions regarding their knowledge, attitudes, and practices toward COVID-19. The question types consisted of Likert-type scale questions, short-answer questions (SAQs), and multiple-choice questions (MCQs). We designed the questions in the questionnaire based on a literature review1,17–20 and guidelines from the WHO,21 Department of Disease Control, Ministry of Public Health, Thailand (DDC-Thailand).4 The questionnaire was piloted to ensure the questionnaire’s validity and reliability using a small sample at Walailak University, Nakhon Si Thammarat.
Study Population and Sampling Strategy
The required sample size was calculated using Epi Info® software version 7.2.4.0, statistical software for epidemiology developed by the Centers for Disease Control and Prevention (CDC), based on an expected proportion of the population that knows about COVID-19 of 50%, an acceptable margin of error of 5%, and a confidence level of 95%. The results showed that 384 subjects were required for this study. People affected by community-wide containment measures living in southern Thailand were eligible participants enrolled in the study. A convenience sampling strategy was used to include the participants. Only participants who voluntarily consented to participate were given the questionnaire, and other participants were excluded from the study.
Questionnaire
The questionnaire consisted of the following three parts: 1) demographic data, 2) knowledge and practices assessment and 3) attitude questions. The demographic data included date of birth, gender, religion, province, type of community, education, occupation, salary, and number of people living in their house. For the knowledge and practices assessment, we used questions with multiple correct answers to allow the participants to choose more than one answer to assess their basic knowledge, practices, and preferred channels for receiving information related to COVID-19. Each selected answer was calculated as a percentage score and 95% confidence interval. To assess attitudes, we applied closed-ended items to assess people’s attitudes regarding COVID-19ʹs signs and symptoms, risk factors, mode of transmission, and prevention and control of the disease. There were ten Likert-type questions related to COVID-19 rated on a 3-point Likert scale (“Agree”, “Neither agree nor disagree”, and “Disagree”). The participants had to choose the answer that achieved the best possible fit with their agreement level to a particular statement. All answers were equally weighted; correct answers were scored as one (1), while incorrect answers and missing responses were scored as zero (0). The maximum score of the attitude assessment was 10. We confirmed the validity and reliability of the questionnaire, resulting in an item-objective congruence (IOC) index of 0.87 and Cronbach’s alpha reliability coefficient (α) of 0.809, respectively.
Statistical Analysis
All statistical analyses were performed by using IBM® SPSS® Statistics version 22 for Windows®. The categorical variables are presented as frequencies and percentages, and the continuous variables are presented as averages and standard deviations. Confidence intervals are shown where appropriate. Statistical significance was accepted at a p value < 0.05.
Ethical Statement
Participation in this study was completely voluntary. Permission and informed consent were obtained from individual respondents before conducting the survey. Regarding online survey consent, the participants and minor participants had to click a “button” in a response indicating that they read the consent information and agreed to participate before being allowed to complete the online self-reporting questionnaire. In addition, parental informed consent was obtained for minor participants using valid signatures and returned to the researchers. Confidentiality and anonymity were maintained throughout the study. The Declaration of Helsinki was adequately addressed, and the study was approved by the Human Research Ethics Committee of Walailak University (certification ID number WU-EC-MD-0-179-63).
Results
General Characteristics of the Study Subjects
Between May 1 and July 31, 2020, in total, 717 subjects were included in this study. Four hundred eighty-four subjects were female (67.5%), and 233 subjects were male (32.5%). Most subjects were aged between 18 and 30 years (49.2%), were Buddhists (68%), graduated with a bachelor’s degree (81%), were not working in healthcare jobs (55.6%), and lived in the urban community (58%). The other general baseline characteristics of the study subjects are described in detail in Table 1.
 |
Table 1 Summary of the General Characteristics of the Study Subjects |
Knowledge Assessment of COVID-19
The details of the questionnaire responses to the COVID-19 knowledge assessment are shown in Table 2. More than half of the respondents knew that the most common early signs and symptoms of COVID-19 (based on the WHO21) were fever (94.1%), cough (80.7%), and tiredness (65.5%), while 6.4% and 3.3% thought that the early signs and symptoms were death and multiorgan failure, respectively. Regarding the mode of transmission, most respondents knew that the disease was transmitted by close contact with respiratory droplets (94.9% via saliva, 87.4% via snot, and 79.3% via sputum), and 95.4% knew that asymptomatic COVID-19 patients could spread coronavirus to others. Regarding people at risk of severe COVID-19 illness, most respondents knew that only older people (89.5%) and people with chronic medical conditions (79.9%) were at a higher risk of becoming seriously ill from COVID-19.
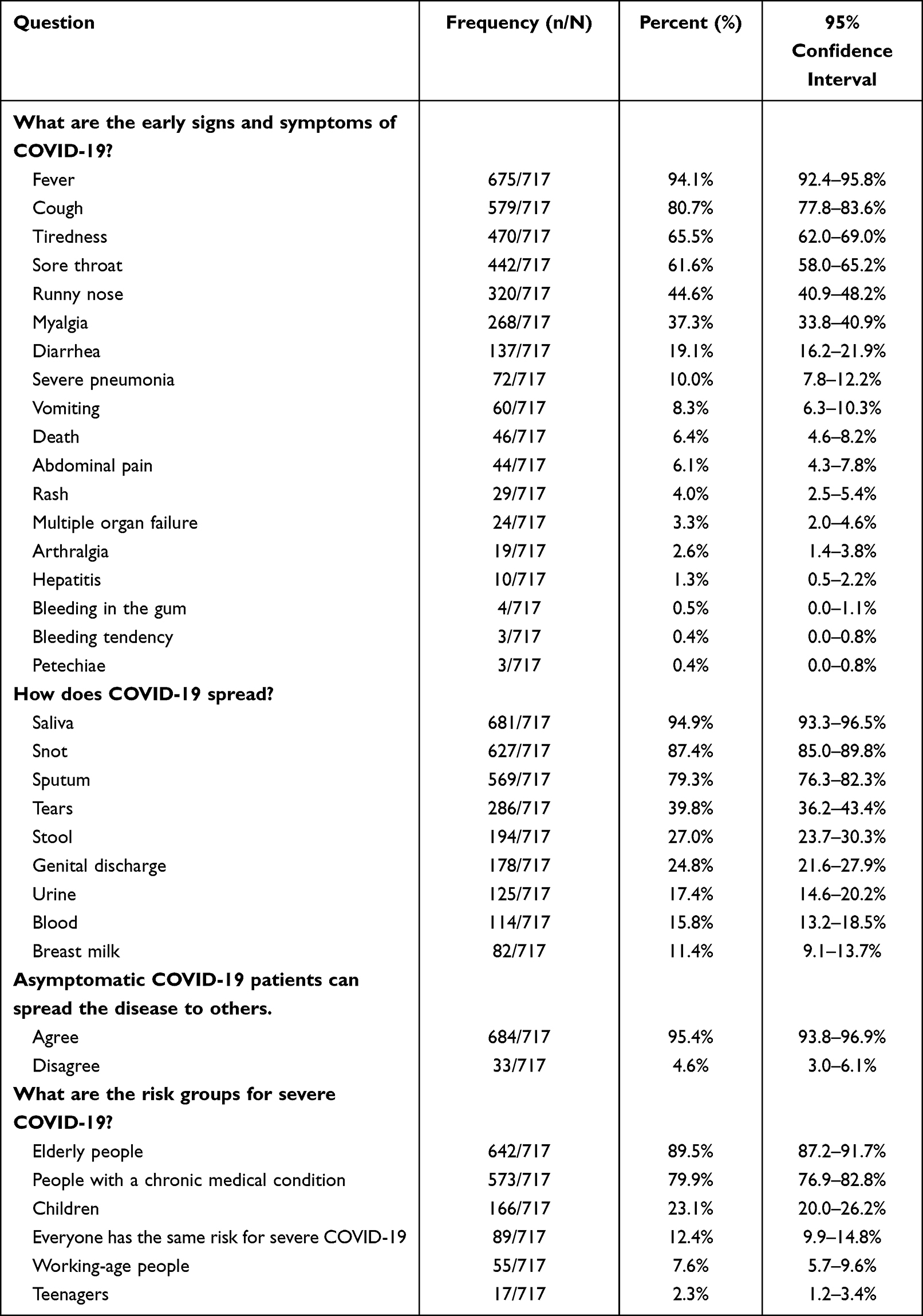 |
Table 2 Knowledge Assessment of COVID-19 |
Practices Related to the Control and Prevention of COVID-19
Table 3 shows the results of the respondents’ practices related to the control and prevention of COVID-19. Almost all respondents knew about COVID-19 by browsing websites (87%) and watching television (72.2%). Most respondents understood the example in the questionnaire regarding the situation causing the COVID-19 outbreak and knew how to prevent it. Nevertheless, 2.6% thought that COVID-19 was transmitted by mosquito bites, and 5.4% thought it was transmitted by dogs. In total, 14.9% believed that the spread of COVID-19 could be prevented by using particular herbs, 1.3% thought that amulets, talismans, or charms could prevent the spread of COVID-19, and 1.8% thought that only wind drying of the contaminated surface area was good enough to disinfect COVID-19.
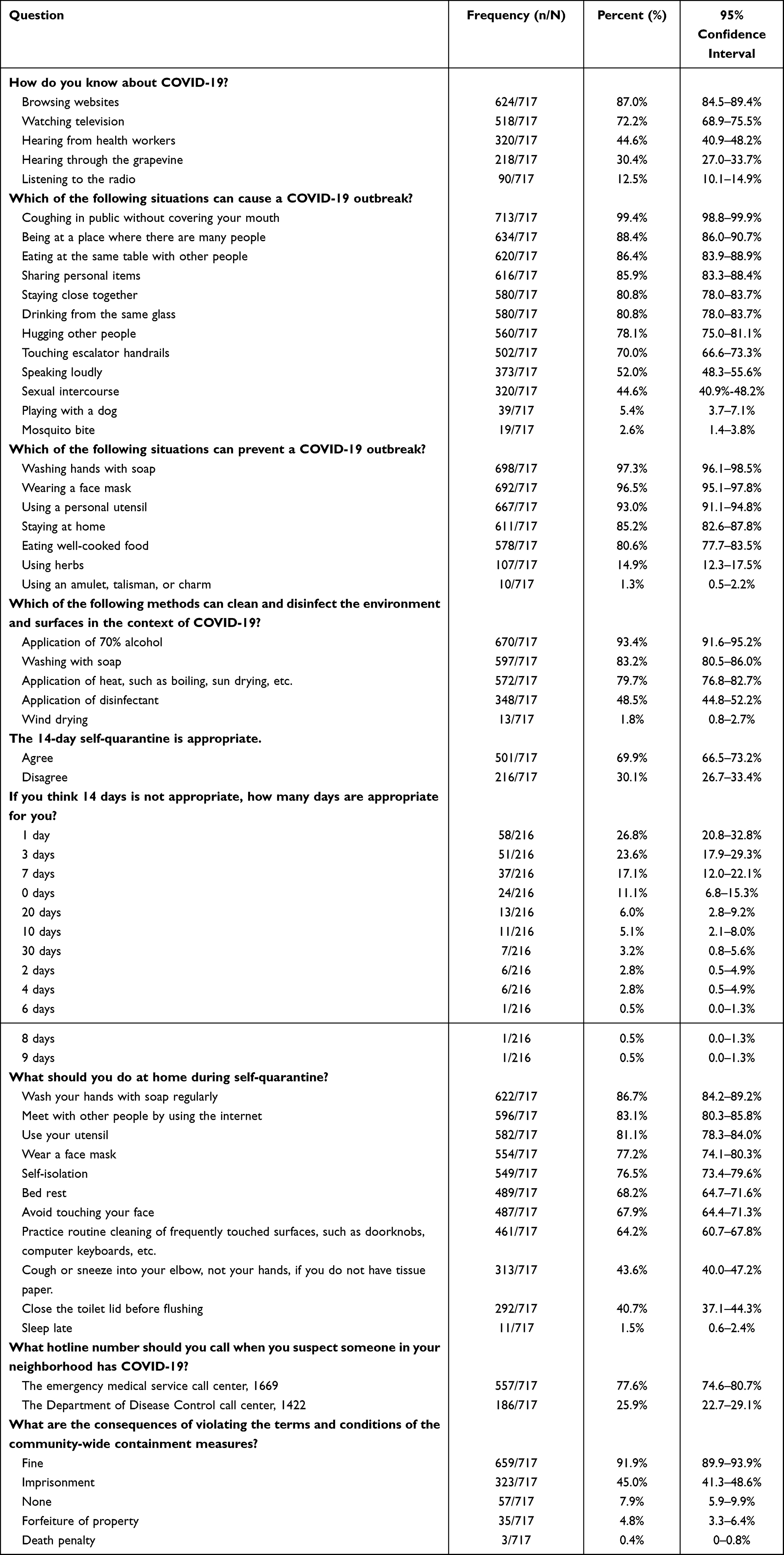 |
Table 3 Practices Related to the Control and Prevention of COVID-19 |
Regarding the practice of self-quarantine, 69.9% of the respondents accepted that 14 days is appropriate for self-quarantine. Among the respondents who disagreed with the 14-day duration of self-quarantine, 26.8% said that only one day was adequate, 23.6% said three days were adequate, 17.1% said one week was adequate, and 11.1% said self-quarantine was unnecessary. Of all respondents answering questions about their practices during self-quarantine periods, 86.7% regularly washed their hands with soap, 83.1% met other people by using the internet, 81.1% used a personal utensil, 77.2% wore face masks at home, 76.5% self-isolated at home, 67.9% avoided touching their face, and 64.2% routinely cleaned and disinfected high-touch surfaces to lower the chance of spreading COVID-19. Only 40.7% of the respondents closed the toilet lid before flushing, and 43.6% covered their mouth and nose with an elbow when lacking tissue paper while coughing or sneezing.
In total, 77.6% of the respondents reported that they knew the hotline number of the emergency medical service call center (1669), while only 25.9% said they knew the hotline number of the Department of Disease Control call center (1422). Regarding punishment, 91.9% of the respondents knew that a fine or mulct was the law’s consequence for not following the rules, but only 45% knew that a prison sentence was also a possible repercussion for noncompliance.
Attitudes Toward COVID-19
Regarding attitudes toward the COVID-19 pandemic, 25.2% believed that people were too concerned about COVID-19. The results showed that 84.2% of the respondents were confident in transferring knowledge about COVID-19 into practice, 55.2% thought they were at risk of COVID-19 infection, and 13.1% believed that COVID-19 could be treated with an alternative method in addition to conventional medicine. Regarding issues of stigmatization from their community, 66.0% would welcome a cured patient back into their community, and 5.3% would keep the fact of having friends infected with COVID-19 a secret. Regarding the community-wide containment measures, most respondents (91.9%) felt that they could complete a 14-day quarantine, but 3.3% thought that community-wide containment measures were unnecessary, 28.6% would live a regular life even against the government recommendation, and 2.2% were willing to travel internationally as shown in Table 4.
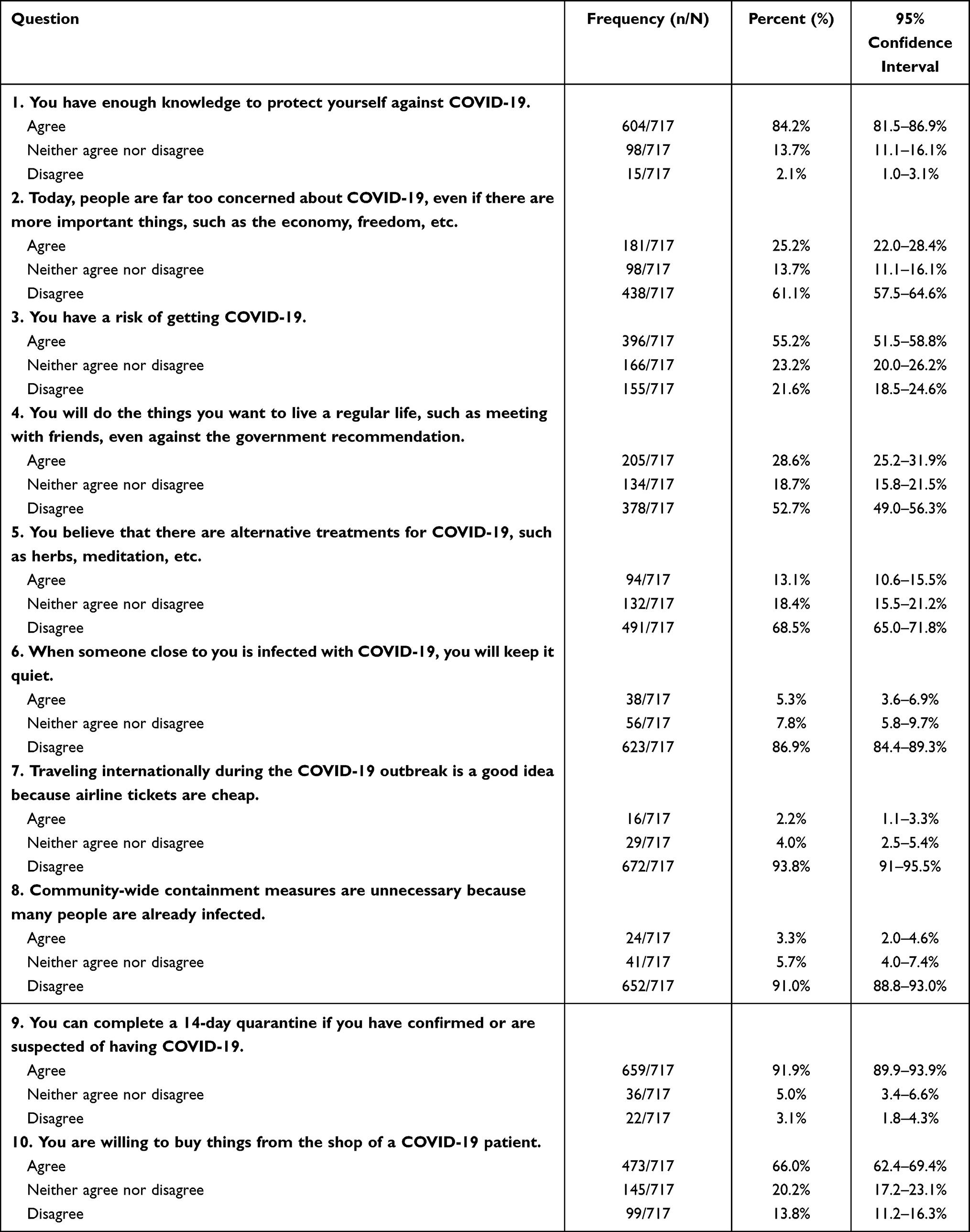 |
Table 4 Attitudes Toward COVID-19 |
Overall, only 56.4% (405/717) of the subjects had scores greater than or equal to 80% (8 of 10) in the attitudes assessment toward COVID-19 (Figure 2).
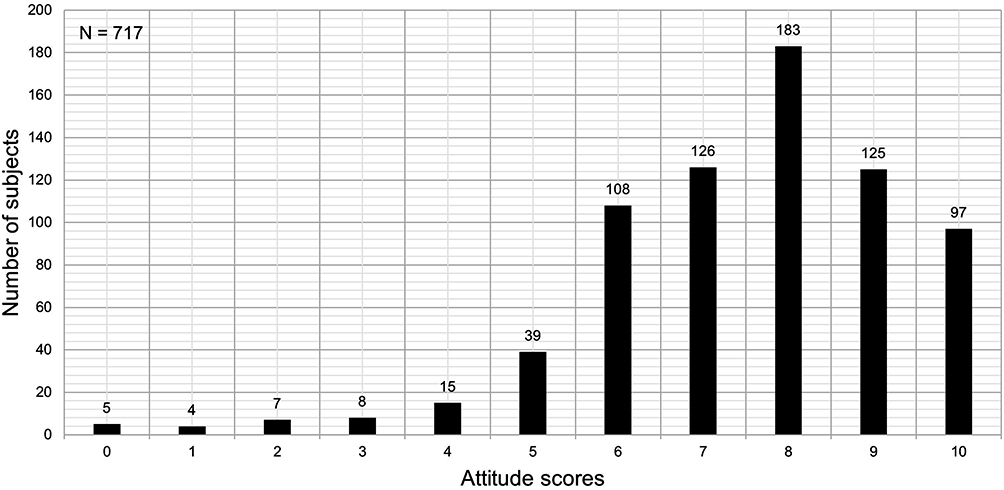 |
Figure 2 Distribution of attitude scores among the subjects. The total number of subjects (N) was 717. The number over the bar indicates the number of subjects. |
Discussion
The COVID-19 pandemic has unleashed a massive global crisis in our lifetime. This crisis caused a large-scale change in social and human behavior, and although countries worldwide have responded with unprecedented action, the situation is far from over. While COVID-19 vaccine development is still ongoing, many governments established several measures to reduce the transmission of COVID-19. In Thailand, these efforts included announcements concerning preventive measures (eg, social distancing, regular hand washing, avoiding touching the face, wearing masks when visiting crowded places, and coughing only into a folded elbow or a tissue), active case surveillance, case investigation and contact tracing, and community-wide containment.4,22
Given this situation, conducting research during the pandemic was difficult due to the policies regarding infectious disease prevention, especially the social distancing policies. Therefore, conducting internet-based research was appropriate because it followed social distancing guidelines and considered the safety of both the participants and researchers. However, online studies have disadvantages in many aspects, such as sample bias, psychometric distortions, technophobia, and lower response rates.23 Our study results showed that most participants were working-age adults, received a middle-income salary range, and graduated with a bachelor’s degree. These data showing bias in the sample variance were predictable because most people with internet access opportunities in Thailand meet the characteristics mentioned above. However, the participants showed relatively similar proportions living in rural areas and urban areas and similar percentages earning a living by working in the healthcare sector (compared to nonhealthcare sector workers and unemployed individuals).
While our research data were being collected (May to July 2020), our results showed that most participants believed that the elderly and people with chronic medical conditions were at a high risk of severe illness. The respondents also believed that the presenting symptoms were limited to fever, cough, tiredness, and sore throat and that respiratory droplets (eg, saliva, knot, and sputum) were the only transmission routes. This belief was based on the available knowledge at that time. However, over time, the global experience of the COVID-19 pandemic was continually developing, and several new findings emerged. Many published studies updated these issues, including recognizing that children and adolescents were also at risk of severe illness, the temporary loss of smell was a new presenting symptom, and nonrespiratory body fluids could transmit the disease.
Regarding the update concerning people at an increased risk for severe disease, children and adolescents were at risk of severe illness similar to the elderly and people with chronic medical conditions. These new data were reported in late 2020 as it was found that COVID-19 could have severe illness consequences in children and adolescents by causing conditions, such as multisystem inflammatory syndrome in children (MIS-C) and stroke in the young.24,25 Regarding updates concerning the transmission of SARS-CoV-2, new scientific evidence emerged showing other possible transmission routes via nonrespiratory body fluids from an infected person, including blood, urine, feces, sputum, tears, and semen, which could contain viable virus.26 Finally, the updates concerning the presenting symptoms of COVID-19 showed that the temporary loss of smell or anosmia emerged as a presenting symptom during this pandemic.27 Because COVID-19 knowledge has been continuously changing and this study was conducted before some of these updates, we assume that the participants had sufficient background knowledge even if they did not consider the updated data. However, some participants still misunderstood that all persons infected with COVID-19 would suffer from severe illnesses, such as severe pneumonia, multiorgan failure, and even death.
Regarding COVID-19-related practices, the results showed that most participants learned about the disease by using the internet. The respondents understood the situations that can lead to a high risk of disease transmission and prevent it. The respondents also knew the financial penalties and potential jail time for noncompliance with government advice concerning COVID-19. However, some misunderstandings due to personal opinions and beliefs were also found in this study. For example, some participants believed that a mosquito bite can spread the disease, that herbs and talisman could cure the disease, and that contaminated surfaces can be disinfected only by drying. These findings may suggest that gathering information related to COVID-19 from the internet sometimes provides incorrect information, leading to misunderstandings and malpractices regarding COVID-19 prevention. In addition, although the results show that only 44.6% of the participants obtained COVID-19 information from health workers, it is still important because many people in the community cannot access media sources, eg, the internet and television, to gain knowledge regarding COVID-19. Furthermore, the Thai context shows that “health workers” played a crucial role in educating the community during the pandemic.28 Therefore, strengthening the community network of health workers and encouraging on-site knowledge sharing by health workers are essential for preventing misunderstandings leading to incorrect practices.
Another interesting issue related to practices regarding COVID-19 was the 14-day self-quarantine period and contacts for emergency support and government services. Regarding the 14 days of self-quarantine, only 69.9% of the study participants thought that 14 days was an appropriate duration. This finding may reflect the problem that most participants did not understand the concept behind the 14-day quarantine, which was based on estimates of the upper bounds of the COVID-19 incubation period.29 Concerning contacts for emergency support and government services, the results showed that only 25.9% knew the Department of Disease Control’s hotline number (1422). This finding could be due to inadequate advertising and the choice of the wrong channels for establishing media publicity.
Regarding attitudes toward COVID-19, the results showed that most participants were confident in their COVID-19 knowledge and their ability to care for themselves, but only 56.4% had high attitude scores. Many believed that COVID-19 has nothing to do with them and felt that they could return to everyday life, even against the government’s recommendation. Moreover, some respondents accused the government of overreacting to the coronavirus crisis. This finding may indicate that misunderstandings occur among people under community-wide containment measures and that the government’s education for their citizens alone is not enough. We suggest that education and social engagement from another part of society, such as the private sector and nongovernment organizations (NGOs), may fulfill citizens’ education needs.
Regarding stigma and discrimination issues, only 66% of the study participants accepted recovering patients back into society. This finding is consistent with a previous study showing that COVID-19 was still stigmatizing healthcare workers, COVID-19 patients, and survivors of this pandemic worldwide.30 This result may have been caused by the participants gaining knowledge from anonymous sources without a proper analysis, leading to misunderstandings and confusion. Finally, we believe that education from a reliable source is critical for stopping the spread of misinformation and minimizing stigma and discrimination.
In summary, our findings of the knowledge, attitudes, and practices of COVID-19 in our study’s participants did not differ from those of previous studies. For example, a study conducted in Malaysia, a country in southern Thailand, found that people have good knowledge, but attitudes and practices regarding COVID-19 remain problematic.31 Therefore, it is the duty of everyone from the government to all citizens to spread accurate and up-to-date information regarding the coronavirus pandemic. In addition, using only opinions concerning COVID-19 without supporting evidence can compromise the control of the pandemic because it causes misunderstandings, negative attitudes, and malpractice.
Limitations
Finally, several significant limitations need to be considered. First, the research relied on an online survey; thus, it was difficult to reach participants who did not have internet access. Therefore, only certain types of study participants were included, leading to a sample bias. The second limitation is that the research was conducted only in the southern part of Thailand, especially near Walailak University; therefore, the subjects may not represent the general population. Finally, the survey length was too long for the participants to complete. It was challenging to stay fully motivated while completing the questionnaire such that the respondents may have refused to continue cooperating in the research or made mistakes. Further studies are recommended.
Conclusion
COVID-19 is no longer a disease of elderly individuals and persons with underlying disease. This crisis can affect people of all ages and lead to a drastic loss of human life. Currently, COVID-19 information is widely shared globally because effective communication technology, especially the internet, is accessible. This technology has resulted in most participants having adequate knowledge, positive attitudes, and good practices against COVID-19. However, there were some misunderstandings among the participants, rendering disease outbreaks more difficult to control. These mistakes may result from outdated or inaccurate online information. It is essential to gain knowledge from a reliable source for proper understanding such that this information can be used to prevent, control, and provide an effective public health response to outbreaks of COVID-19.
Disclosure
The authors report no conflicts of interest in this study.
References
1. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
2. Burki TK. Coronavirus in China. Lancet Respir Med. 2020;8(3):238.
3. Okada P, Buathong R, Phuygun S, et al. Early transmission patterns of coronavirus disease 2019 (COVID-19) in travellers from Wuhan to Thailand, January 2020. Euro Surveill. 2020;25(8):2000097. doi:10.2807/1560-7917.ES.2020.25.8.2000097
4. Department of Disease Control Thailand (DDC). Coronavirus disease (COVID-19); 2019. Available from: https://covid19.ddc.moph.go.th/en.
5. Centers for Disease Control and Prevention (CDC). COVID-19 parental resources kit; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/parental-resource-kit/index.html.
6. Centers for Disease Control and Prevention (CDC). People at increased risk and other people who need to take extra precautions; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html.
7. Bener A, Al-Khal A. Knowledge, attitude and practice towards SARS. J R Soc Promot Health. 2004;124(4):167–170. doi:10.1177/146642400412400408
8. Wilder-Smith A, Chiew C, Lee V. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. 2020;20(5):e102–e107. doi:10.1016/S1473-3099(20)30129-8
9. Centers for Disease Control and Prevention (CDC). Use of quarantine to prevent transmission of severe acute respiratory syndrome–Taiwan, 2003. MMWR Morb Mortal Wkly Rep. 2003;52(29):680–683.
10. Hawryluck L, Gold WL, Robinson S, Pogorski S, Galea S, Styra R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis. 2004;10(7):1206–1212. doi:10.3201/eid1007.030703
11. Mandavilli A. SARS epidemic unmasks age-old quarantine conundrum. Nat Med. 2003;9(5):487. doi:10.1038/nm0503-487
12. Twu S-J, Chen T-J, Chen C-J, et al. Control measures for severe acute respiratory syndrome (SARS) in Taiwan. Emerg Infect Dis. 2003;9(6):718–720. doi:10.3201/eid0906.030283
13. Chan EYY, Cheng CKY, Tam G, Huang Z, Lee P. Knowledge, attitudes, and practices of Hong Kong population towards human A/H7N9 influenza pandemic preparedness, China, 2014. BMC Public Health. 2015;15(1):943. doi:10.1186/s12889-015-2245-9
14. Dauda Goni M, Hasan H, Naing NN, et al. Assessment of knowledge, attitude and practice towards prevention of respiratory tract infections among Hajj and Umrah Pilgrims from Malaysia in 2018. Int J Environ Res Public Health. 2019;16(22). doi:10.3390/ijerph16224569
15. Deng JF, Olowokure B, Kaydos-Daniels SC, et al. Severe acute respiratory syndrome (SARS): knowledge, attitudes, practices and sources of information among physicians answering a SARS fever hotline service. Public Health. 2006;120(1):15–19. doi:10.1016/j.puhe.2005.10.001
16. Person B, Sy F, Holton K, Govert B, Liang A. National center for infectious diseases SCOT fear and stigma: the epidemic within the SARS outbreak. Emerg Infect Dis. 2004;10(2):358–363. doi:10.3201/eid1002.030750
17. Zhai P, Ding Y, Wu X, Long J, Zhong Y, Li Y. The epidemiology, diagnosis and treatment of COVID-19. Int J Antimicrob Agents. 2020;55(5):105955. doi:10.1016/j.ijantimicag.2020.105955
18. Singhal T. A review of coronavirus disease-2019 (COVID-19). Indian J Pediatr. 2020;87(4):281–286. doi:10.1007/s12098-020-03263-6
19. Vicerra PMM. Disparity between knowledge and practice regarding COVID-19 in Thailand: a cross-sectional study of older adults. PLoS One. 2021;16(10):e0259154. doi:10.1371/journal.pone.0259154
20. The United Nations Population Fund (UNFPA). COVID-19 and older persons: evidence from the survey in Thailand; 2021. Available from: https://thailand.unfpa.org/sites/default/files/pub-pdf/covid-19_report-online-revised_2021.pdf.
21. World Health Organization (WHO). Coronavirus disease (COVID-19) pandemic; 2019. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
22. World Health Organization (WHO). WHO Thailand situation report; 2020. Available from: https://www.who.int/docs/default-source/searo/thailand/2020_12_26_tha-sitrep-106-covid19.pdf.
23. Hunter L. Challenging the reported disadvantages of e-questionnaires and addressing methodological issues of online data collection. Nurse Res. 2012;20(1):11–20. doi:10.7748/nr2012.09.20.1.11.c9303
24. Ahmed M, Advani S, Moreira A, et al. Multisystem inflammatory syndrome in children: a systematic review. EClinicalMedicine. 2020;26:100527. doi:10.1016/j.eclinm.2020.100527
25. Fifi JT, Mocco J. COVID-19 related stroke in young individuals. Lancet Neurol. 2020;19(9):713–715. doi:10.1016/S1474-4422(20)30272-6
26. Mohseni AH, Taghinezhad-S S, Xu Z, Fu X. Body fluids may contribute to human-to-human transmission of severe acute respiratory syndrome coronavirus 2: evidence and practical experience. Chin Med. 2020;15(1):58. doi:10.1186/s13020-020-00337-7
27. Meng X, Deng Y, Dai Z, Meng Z. COVID-19 and anosmia: a review based on up-to-date knowledge. Am J Otolaryngol. 2020;41(5):102581. doi:10.1016/j.amjoto.2020.102581
28. Vicerra PMM. Knowledge-behavior gap on COVID-19 among older people in rural Thailand. Gerontol Geriatr Med. 2021;7:2333721421997207. doi:10.1177/2333721421997207
29. Centers for Disease Control and Prevention (CDC). Science brief: options to reduce quarantine for contacts of persons with SARS-CoV-2 infection using symptom monitoring and diagnostic testing; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/more/scientific-brief-options-to-reduce-quarantine.html.
30. Bagcchi S. Stigma during the COVID-19 pandemic. Lancet Infect Dis. 2020;20(7):782. doi:10.1016/S1473-3099(20)30498-9
31. Chai CS, Ng DL, Chua WJ, et al. Knowledge, attitude, and practices among the general population during the later stage of the COVID-19 pandemic in Malaysia: a cross-sectional study. Risk Manag Healthc Policy. 2022;15:389–401. doi:10.2147/RMHP.S349798
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.