Back to Journals » Risk Management and Healthcare Policy » Volume 13
Knowledge, Attitudes and Practices Toward Prevention and Early Detection of COVID-19 and Associated Factors Among Religious Clerics and Traditional Healers in Gondar Town, Northwest Ethiopia: A Community-Based Study
Authors Asmelash D ![]() , Fasil A
, Fasil A ![]() , Tegegne Y, Akalu TY
, Tegegne Y, Akalu TY ![]() , Ferede HA
, Ferede HA ![]() , Aynalem GL
, Aynalem GL ![]()
Received 19 August 2020
Accepted for publication 1 October 2020
Published 20 October 2020 Volume 2020:13 Pages 2239—2250
DOI https://doi.org/10.2147/RMHP.S277846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Daniel Asmelash, 1 Alebachew Fasil, 1 Yalewayker Tegegne, 2 Temesgen Yihunie Akalu, 3 Habtamu Asfaw Ferede, 4 Getie Lake Aynalem 5
1Department of Clinical Chemistry, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Parasitology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Epidemiology and Biostatistics, School of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Department of Nursing, University of Gondar Referral Hospital, Gondar, Ethiopia; 5School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Daniel Asmelash Email [email protected]
Background: COVID-19 control measures efforts are affected by the knowledge, attitudes, and practices of the public, particularly religious clerics and traditional healers, who have close contact and are widely accepted by a significant number of community members.
Methods: A community-based cross-sectional study was conducted to determine knowledge, attitudes and practices towards COVID-19 and its associated factors among religious clerics and traditional healers in Gondar town. Study participants who met our inclusion criteria were selected using a simple random sampling technique. Data were collected by trained data collectors through face-to-face interviews. The reliability of the questionnaire was assessed using Cronbach’s alpha. Knowledge, attitudes and practices scores were calculated to give the overall knowledge, attitude and practice score. Binary logistic regression was fitted to identify associated factors and odds ratio was used to measure the strength of the association.
Results: A total of 410 religious clerics and traditional healers were included in the study with a response rate of 97.1%. Of the total participants, 60.7% (95%: CI (56– 65%)) had good knowledge, 34.1% (95%: CI (30– 39%)) had a positive attitude and 15.6% (95%: CI (12– 19%)) had good practices towards prevention and early detection of COVID-19. Less than one third of the participants practiced physical distancing (28%) and facemask use (17.8%). In multivariate logistic regression, age, educational status and marital status were significantly associated with knowledge score. Likewise, age and marital status were significantly associated with the positive attitude score. In addition, age, educational status, and the presence of underlying disease were significantly associated with the good practice score.
Conclusion: Majority of the participants had poor practice and negative attitudes. Therefore, there should be a sensitization program to fill the gap in the knowledge, attitudes and practice measures of COVID-19 especially for elderly and illiterates.
Keywords: knowledge, attitude, practice, COVID-19, religious clerics, traditional healers, Ethiopia
A Letter to the Editor has been published for this article.
Introduction
In the last two decades, epidemics of severe acute respiratory infections have been identified as one of the most serious risks to global health.1 An emerging acute respiratory disease named Coronavirus Disease 2019 (COVID-19) was reported in Wuhan, China, on December 2019.2 And a total of 9,653,048 diagnosed cases of COVID-19 and 491,128 deaths were reported as of 27 June, 2020, according to data compiled by the World Health Organization (WHO). The COVID-19 pandemic has spread very quickly and the world needs to prepare for the prevention of the pandemic.3,4
The COVID-19 epidemics are mainly associated with respiratory diseases and symptoms range from mild to severe illness and are mainly characterized by fever, dry cough, dyspnea, headache, sore throat and rhinorrhea and sometimes hemoptysis.5 To date, no successful treatment or vaccine has been used for COVID-19. Therefore, the only intervention is the implementation of preventive measure to control the infection of COVID-19.6
A study in China showed that residents had a high level of awareness of the main symptoms, transmission routes, use of masks, hand washing and treatment information for COVID-19, while a low level of awareness of the atypical symptoms. Also, 92.6% of the subjects thought that the outbreak was scary and 71.9% of the residents were satisfied with the local epidemic control measures.7
Health education programs aimed at improving COVID-19 knowledge are reported helpful for Chinese to hold optimistic attitudes and maintain appropriate practices.8 The presence of COVID-19 in low-and middle-income countries raises pressing issues about the effective pandemic response and preparedness in the setting of fragile health systems. The response to the COVID-19 pandemic has exposed that basic disease prevention and control systems are insufficient in terms of human resources and laboratory testing capacity.9
Being the most populous African nation, Ethiopia could certainly be associated with a higher risk of increased morbidity and mortality due to COVID-19. Thus, there is a need to examine knowledge, attitudes and practice, and associated factors towards the COVID-19 pandemic especially for religious clerics and traditional healers (THs). Because attitudes and practices shared by the religious clerics and THs could be widely adopted by large numbers of community members in Ethiopia. They have also contact with a large number of clients and followers. Therefore, targeting this population would be essential in order to develop an effective intervention plan and propose an effective policy.
Methods
Study Area, Design
The study was conducted in Gondar town, located in the regional state of Amhara and approximately 741 kilometers northwest of Addis Ababa, the capital city of Ethiopia. A community-based cross-sectional study was conducted to determine the level of knowledge, attitudes and practices towards prevention and early detection of COVID-19 and its associated factors among religious cleric and THs from 25 May to 30 June 2020.
Study Population
Religious clerics and THs, who were aged 18 years and above living in Gondar town were included in the study after written informed consent was obtained. Eligible religious clerics and THs living in the selected sub-city of Gondar town at the time of data collection, who were willing to participate and willing to provide appropriate information, were included in the study. Individuals who were not willing to take part in the study, individuals with mental disabilities and those who were unable to provide adequate information were excluded.
Religious clerics are religious leaders who conduct ceremonial religious services in churches and mosques, advise individuals or families in times of distress, and sanctify marriage and birth. THs, referred to as those who practice a wide range of spiritual healing, healing, surgical, and preventive practices locally. Because religious rituals are deeply rooted in healing practices in Ethiopia, a boundary demarcation between clerics and THs is difficult. Religious clerics and THs were therefore allowed to self-identify when they had both clerical and healing functions.10 Therefore, THs with clerical function were categorized as dual Traditional healers, THs without clerical functions were categorized as sole traditional healers, and clerics without traditional healing function were categorized as sole clerics.
Data Collection Tool and Procedure
The data collection tool for the assessment of the knowledge, attitudes and practices towards prevention and early detection of COVID-19 was based on the questions adapted from published literature9,11,12 and by the recommendations of WHO and Communicable Disease Control (CDC).3,13 Finally, 46 questions were generated to assess the knowledge, attitudes and practices towards COVID-19 using a closed-ended questionnaire.
The questionnaire was divided into 4 portions: the first portion deals with socio-demographic characteristics; the remaining three portions contain questions on the assessment of participants knowledge (16 questions), attitudes (14 questions) and practices (16 questions) of the religious clerics and THs. Each response was scored as “1” for the correct/positive response and “0” for the incorrect/negative response. Knowledge, attitudes and practice scores of individuals were calculated to give the total knowledge, attitudes and practice score. Then negative attitudes, poor knowledge and poor practice levels were categorized based on a 60% Bloom’s cutoff point.6
A pilot study was done on 22 religious clerics and the reliability of the questionnaire was assessed using Cronbach’s alpha (α) (Cronbach’s alpha (α) for knowledge, attitudes and practice were found to be 0.826, 0.744 and 0.704 respectively).14 Face validity was performed to evaluate the comprehension towards understanding of the questionnaire and to assess how important it was to target study participants. A revised version of the questionnaire was developed based on the feedbacks from face-validation. Finally, the questionnaire was modified and re-evaluated to fit the study population based on the feedbacks of the pilot study. The data generated from the pilot study and incomplete responses were excluded from the final analysis.
Four sub-cities (Jantekel sub-city, Mahal Arada sub-city, Azezo Tseda sub-city and Maraki sub-city) were selected using a simple random sampling technique. Eligible religious clerics and THs living within the selected sub-cities were enrolled using simple random sampling technique.
Data were collected by trained data collectors through face-to-face interviews using constructed questionnaire. The interview was completed in accordance with the WHO standard for the prevention of COVID-19. The questionnaire was first prepared in English and then translated into local Amharic language with the assistance of a language expert. The collected data were checked daily for consistency and accuracy.
Statistical Methods
The cleaned data were analyzed by using Statistical Package for Social Science (SPSS) version 21 software. Numerical data were summarized as means and standard deviations and categorical variables were summarized in frequency and percentage and the result was presented using tables. Knowledge, attitudes and practices scores were calculated to give the overall knowledge, attitude and practice score. The bivariate and multivariate logistic regression model was used to identify factors associated with good knowledge, good attitude and good practice towards COVID-19. The variables in the bivariable analysis with p < 0.25 were entered in the multivariable logistic regression.15,16 Crude odds ratio (COR) and the adjusted odds ratio (AOR) were used to measure the strength of association. Besides, the Pearson correlation between knowledge, attitude and practice scores was assessed. Finally, P < 0.05 is considered statistically significant.
Results
Sociodemographic and Clinical Characteristics of the Study Participants
A total of 410 religious clerics and THs were included in the study with a response rate of 97.1%. Of these, 323 (78.7%) were sole religious clerics, followed by the dual traditional healers 65 (15.9%), and 22 (5.4%) were sole traditional healers. Of the total study participants, 122 (29.8%) were between 31–45 years age group with a mean age of 47 ±17 (µ± SD). Also, the majority of the study participants were male 379 (92.4%) and 294 (71.7%) were living with more than two family members (Table 1).
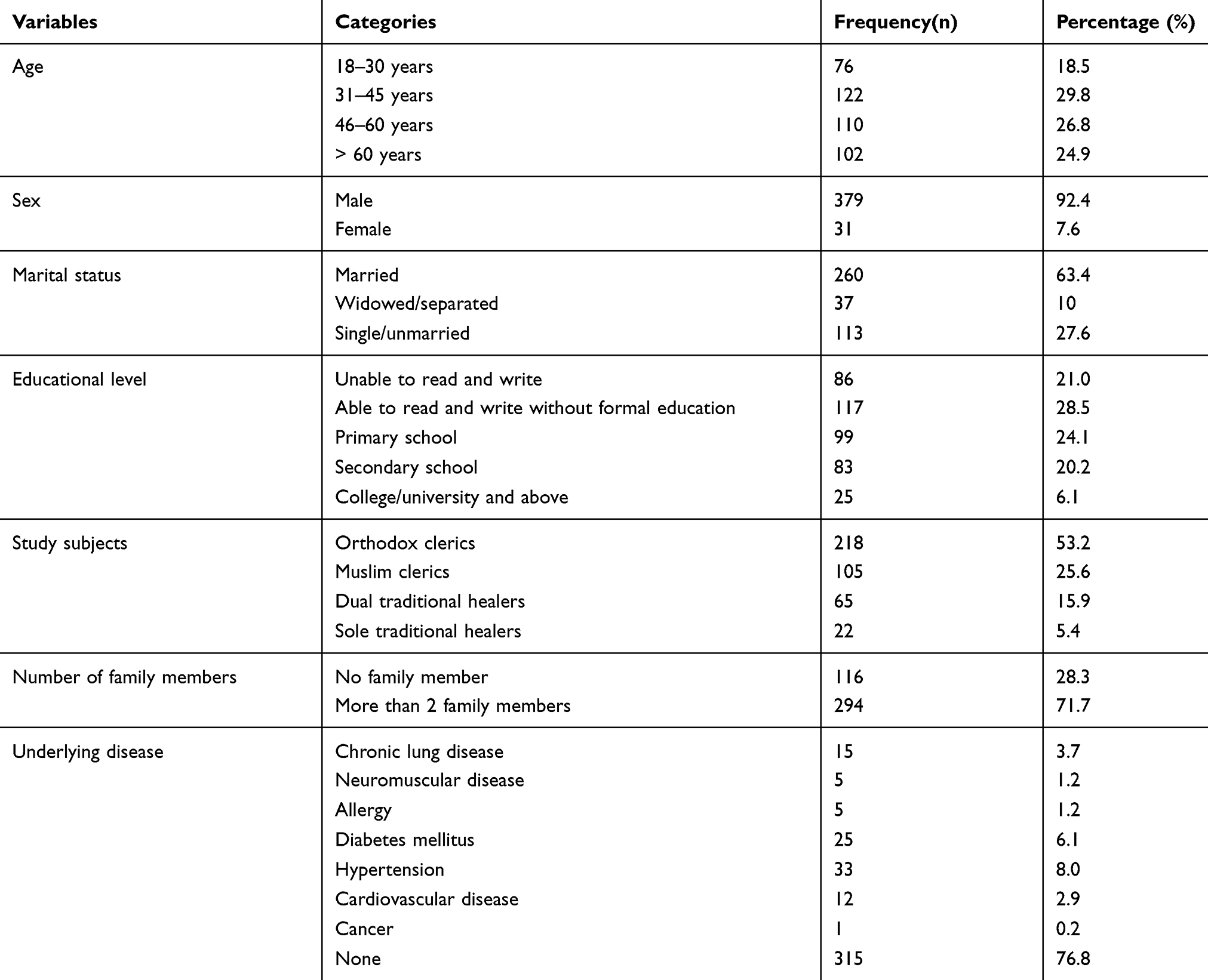 |
Table 1 Socio-Demographic Characteristics of the Religious Clerics and Traditional Healers in Gondar Town |
Knowledge Toward Prevention and Early Detection of COVID-19 and Associated Factors
Out of the total study participants, 60.7% (95%: CI (56–65%)) had a good knowledge toward COVID-19 with a knowledge mean score of 10.22 ± 3.4. Almost all 404 (98.5%) of religious clerics and THs had heard about COVID-19, whereas only 148 (36.1%) knew that the disease was a viral illness and 249 (60.7%) knew it could be fatal.
Besides, more than one third of participants were not aware of the importance of facemask usage 196 (47.8%), physical distancing 148 (36.1%) and quarantine or isolation 201 (49%) for COVID-19 prevention, while more than three fourths 308 (75.1%) were aware of the importance of proper hand washing for COVID-19 prevention. In addition, 321 (78.3%) of the participants were aware of the main transmission routes and 369 (90%) were also aware of at least one sign and symptomof COVID-19 (Table 2).
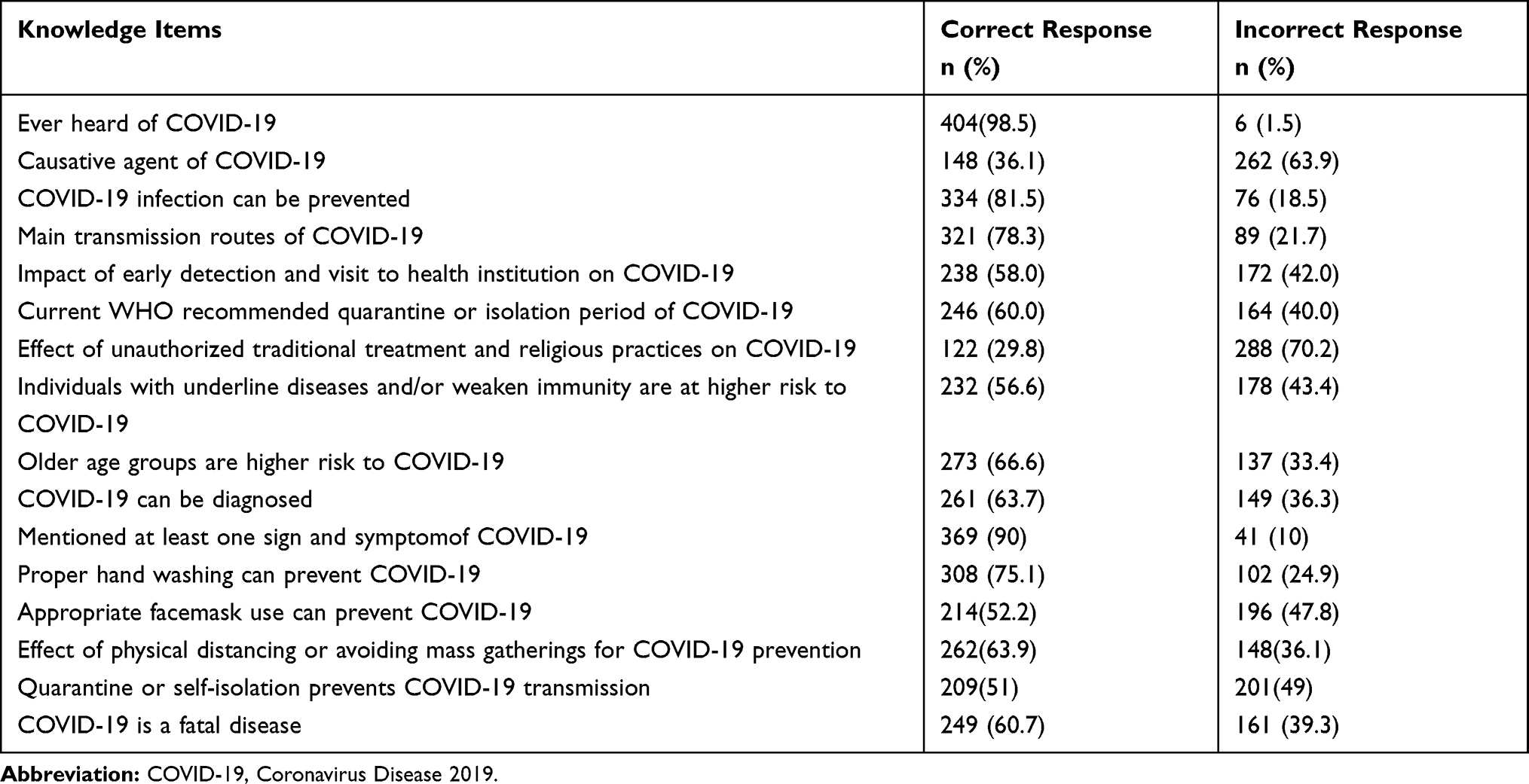 |
Table 2 Knowledge Items Toward COVID-19 Among Religious Cleric and Traditional Healers in Gondar, 2020 |
The bivariate analysis showed that sex, age, educational status, marital status and presence of underlying disease were significantly associated with the knowledge score. In multivariate logistic regression: age, educational status and marital status were significantly associated with the knowledge level of participants towards COVID-19. Accordingly, the 18–30 age group participants were 7.33 (AOR=7.33; 95% CI: 2.76–19.49) times knowledgeable compared to the above 60 years age groups. In addition, participants with educational status of able to read and write, completed primary school, completed secondary school, university/college and above were 2.94 (AOR=2.94; 95% CI: 1.56–5.51), 5.91 (AOR=5.91; 95% CI: 2.94–12.10), 8.59 (AOR=8.59; 95% CI: 3.84–19.19) and 6.57 (AOR=6.57; 95% CI: 2.00–21.52) times higher knowledge score compared with those study participants whose educational status was to unable to read and write. Moreover, married participants were 2.82 (AOR=2.82; 95% CI: 1.13–7.03) times higher knowledge score compared with separated and or widowed participants (Table 3).
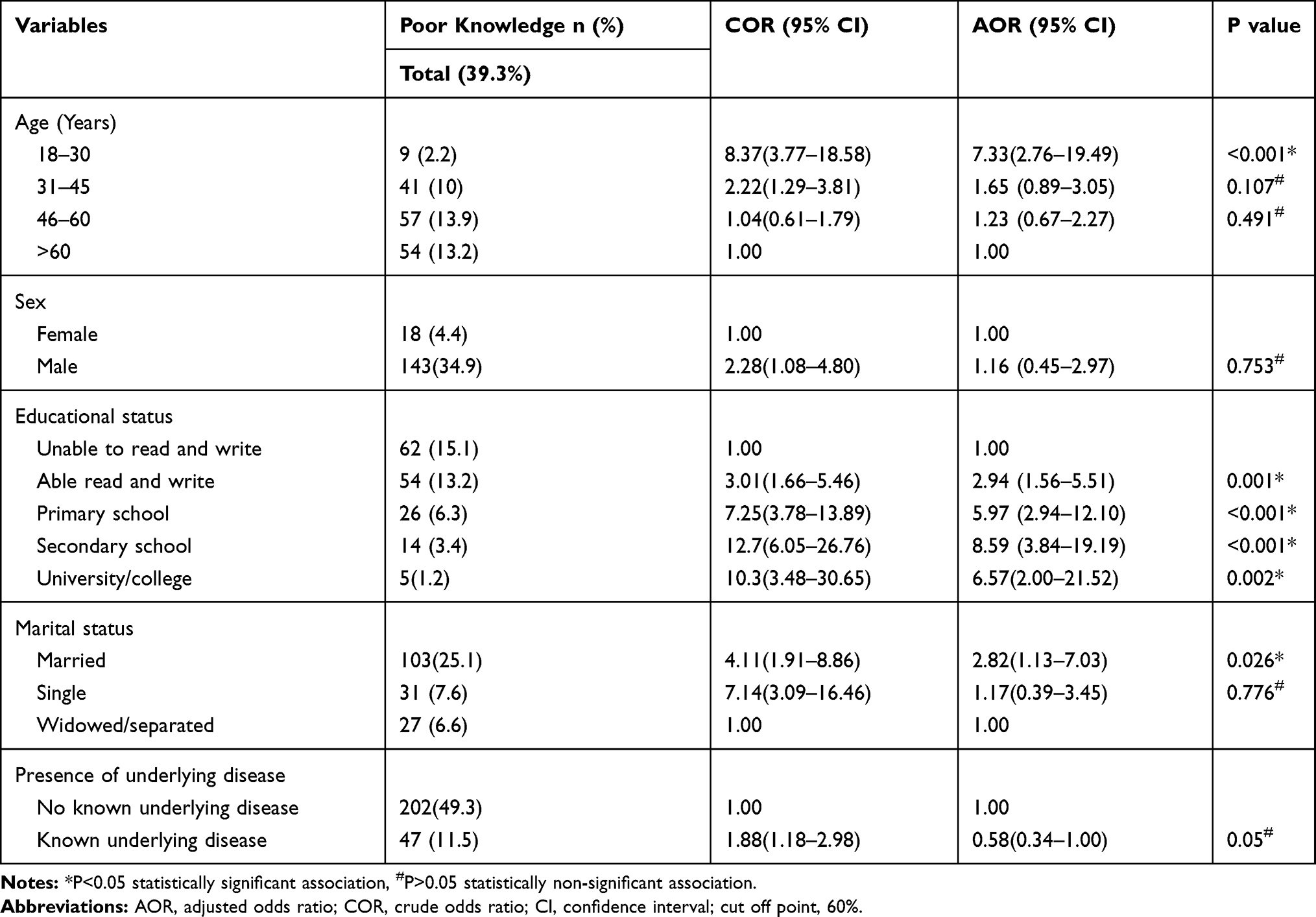 |
Table 3 Bivariate and Multivariate Analysis of Factors Associated with Knowledge Toward COVID-19 |
Attitude Toward Prevention and Early Detection of COVID-19 and Associated Factors
Only 34.1% (95%: CI (30–39%)) of the participants had a positive attitude score towards prevention and early detection of COVID-19, and the mean attitude score was 6.5 ± 3.3. More than two thirds of 273 (66.6%) of the study participants believed that they would recover if they had acquired COVID-19 and only 155 (36.1%) of the participants perceived that they were at risk of infection. Less than half of participants believed that practicing physical distance 181 (44.1%), avoiding mass gatherings 189 (46.1%) and avoiding touching eyes, mouth and noses 175 (42.7%) with the unclean hand, was necessary for COVID-19 prevention. The majority of the respondents believed that COVID-19 was due to the punishment of God 356 (86.8%) and TH/religious clerics 278 (67.8%) were better than physicians for the management of COVID-19 (Table 4).
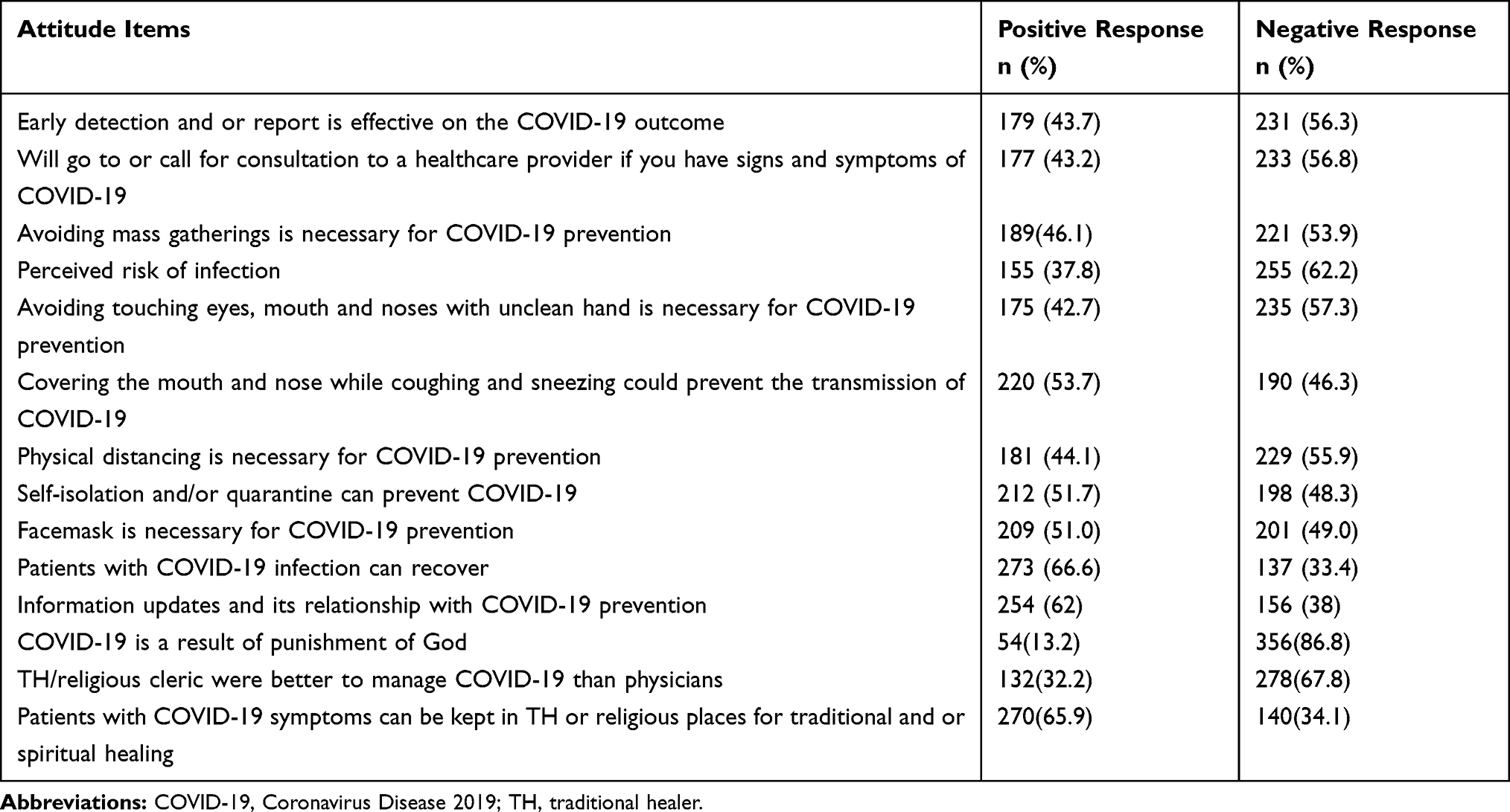 |
Table 4 Attitude Items Toward COVID-19 Among Religious Cleric and Traditional Healers in Gondar Town, 2020 |
In the bivariate analysis; sex, age and marital status were found to be significantly associated with attitudes towardprevention and early detection of COVID-19. Multivariate analysis showed that age and married participants were significantly associated with a positive attitude towards prevention and early detection of COVID-19. Participants in the 18–30 and 30–45-year age groups had 3.01 (AOR=3.01; 95% CI: 1.38–6.59) and 1.82 (AOR=1.82; 95% CI: 1.02–3.27) times higher positive attitude score than those above 60 years old age. Moreover, married participants were 5.65 (AOR=5.65; 95% CI: 1.28–24.83) times higher positive attitude score compared to separated and or widowed study participants. However, sex, the number of family members and the presence of underlying disease were not significantly associated with the attitude level of participants towards COVID-19 pandemic (Table 5).
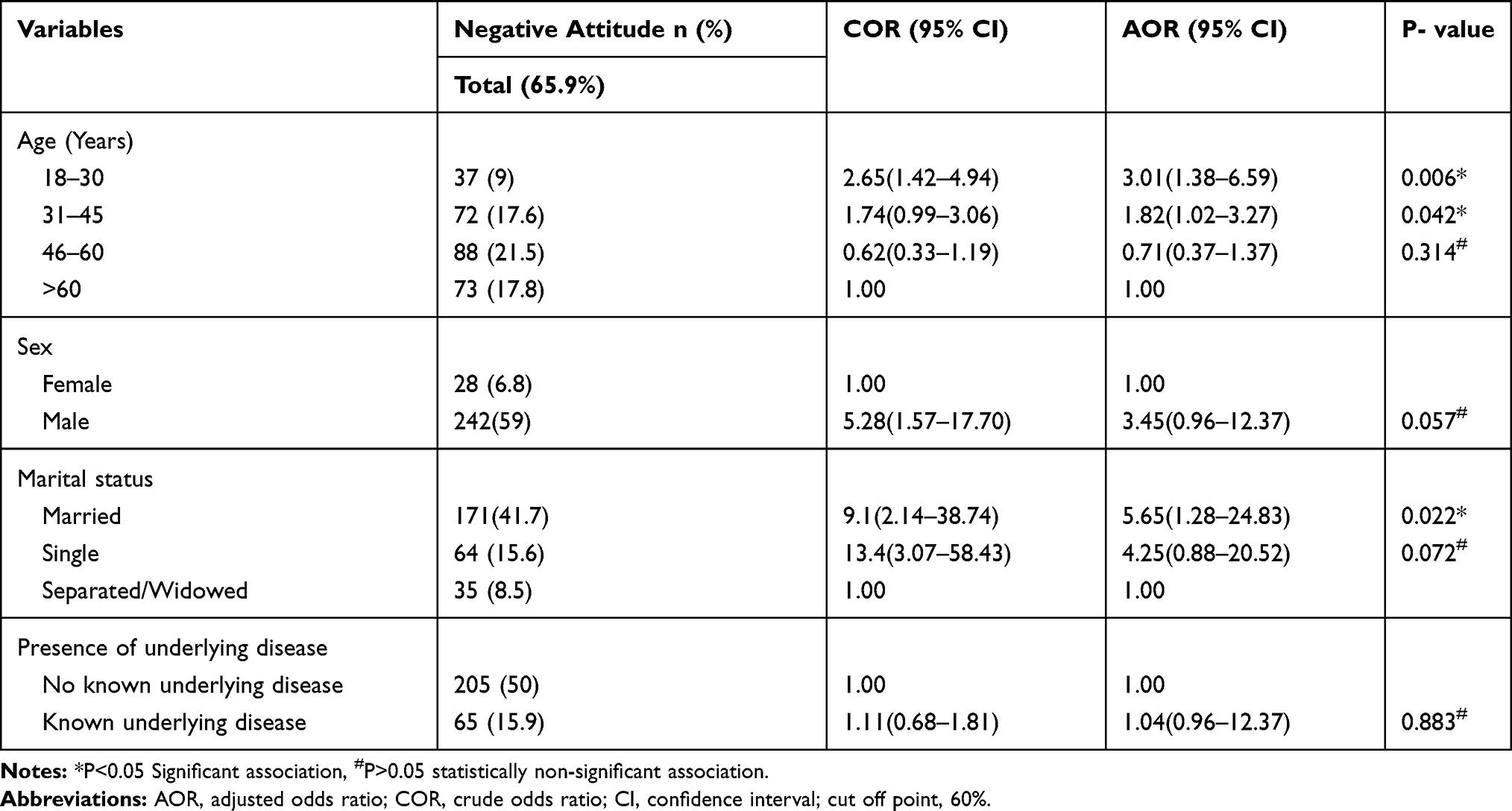 |
Table 5 Bivariate and Multivariate Analysis of Factors Associated with Attitude Toward COVID-19 |
Practices Toward Prevention and Early Detection of COVID-19 and Associated Factors
Of the total participants, 15.6% (95%: CI (12–19%)) had good practice towards the prevention and early detection of COVID-19 with a mean practice score of 4.69 ± 2.9. Two thirds (65.5%) of the study participants reported proper hand washing practice. However, less than one third of the participants practiced physical distancing 115 (28%), avoided mass gatherings 105 (25.6) and 73 (17.8%) used facemasks properly in the weeks before. The majority of the study participants, 402 (92.6%) did not practice dietary balance and hygiene, 402 (98%) did not perform regular exercise and were extremely scared about COVID-19,338 (82.4%) (Table 6)
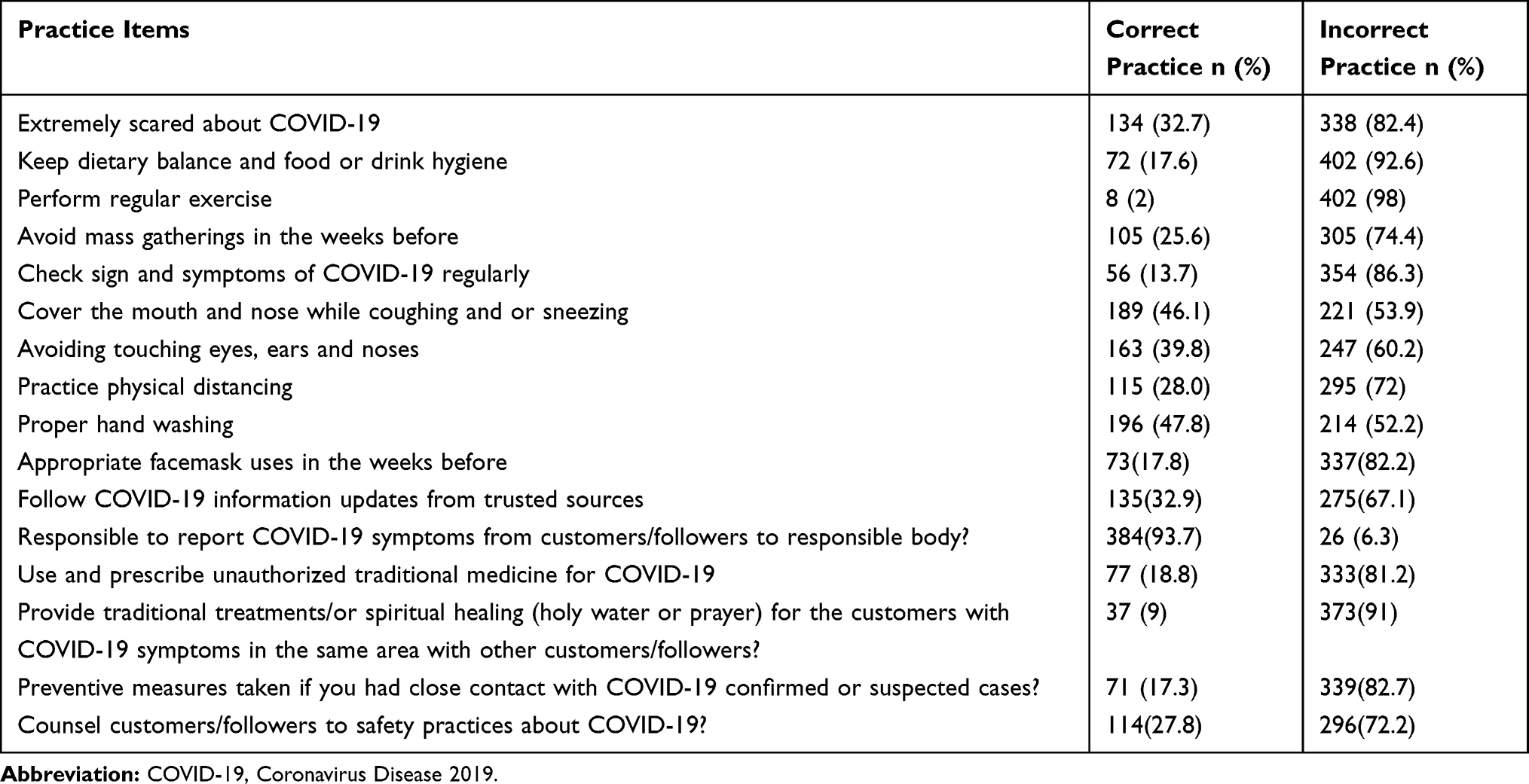 |
Table 6 Practice Items Toward COVID-19 Among Religious Clerics and THs at Gondar Town, 2020 |
In the bivariate analysis; age, educational status, marital status, number of family members and presence of underlying disease were found to be significantly associated with practice score towardprevention and early detection of COVID-19. Multivariate logistic regression analysis revealed that age, educational status and presence of underlying disease were significantly associated with good practice towards COVID-19.
The odds of good practice among 18–30 and 31–45 years age groups were 4.75 (AOR=4.75; 95% CI: 2.04–11.08) and 4.37 (AOR=4.37; 95% CI: 1.33–14.33) times higher compared to above 60 years age groups, respectively. Also, participants who were able to read and write, completed secondary school and university/college were had 4.03 (AOR=4.03; 95% CI: 1.35–12.04), 4.15 (AOR=4.15; 95% CI: 1.28–13.24) and 5.42 (AOR=5.42; 95% CI: 1.24–23.76) times more likely to have good practice towards COVID-19 compared to participants who were unable to read and write. Moreover, the study participants with the known underlying disease were 5.2 (AOR=5.2; 95% CI: 2.66–10.04) times higher good practice than those with without known underlying disease (Table 7).
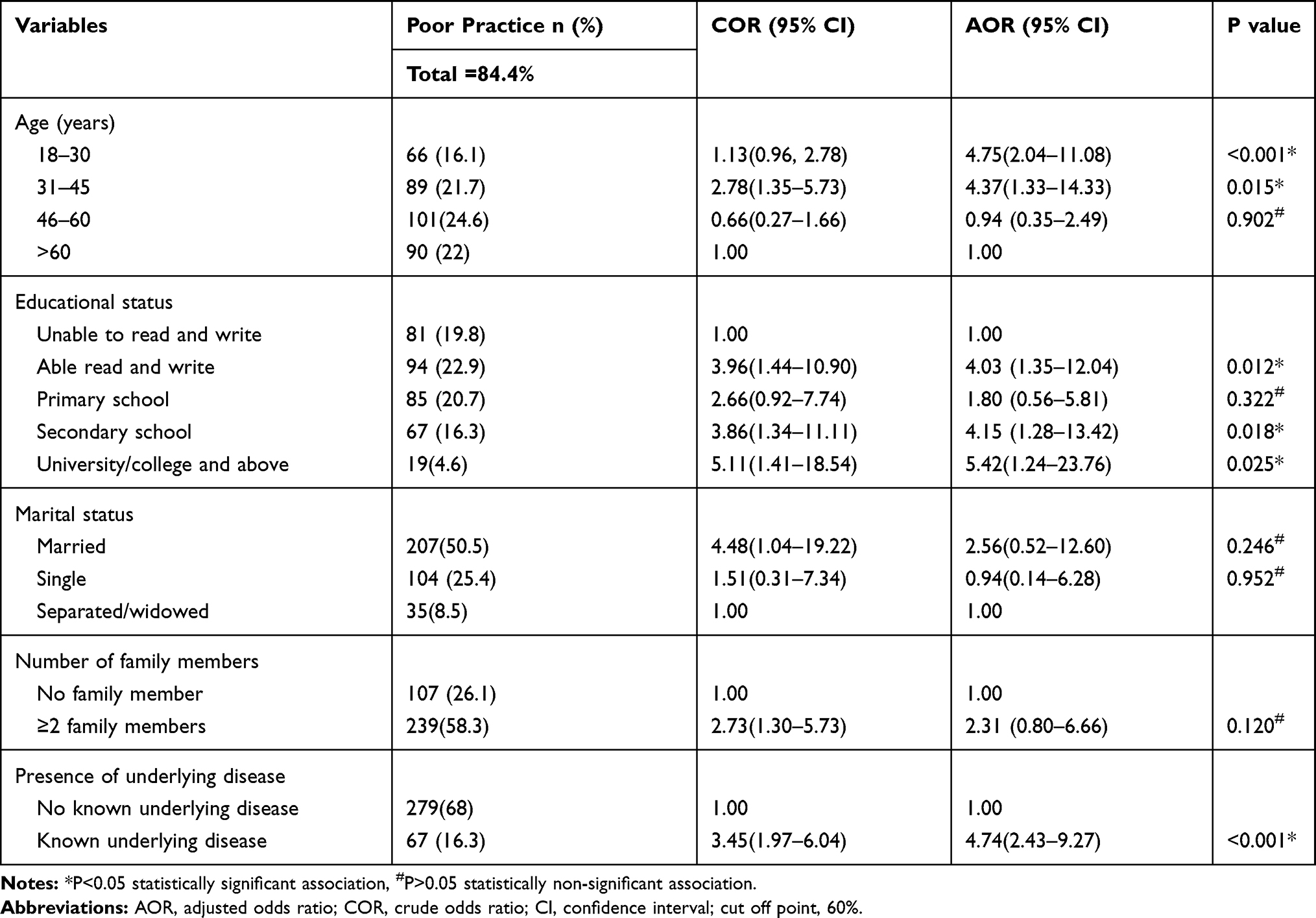 |
Table 7 Bivariate and Multivariate Analysis of Factors Associated with Practice Toward COVID-19 |
In addition, the Pearson correlation revealed that there was a positive correlation between knowledge, attitude and practice scores towards prevention and early detection of COVID-19. (between knowledge and practice (r = 0.294, p < 0.001), between knowledge and attitude (r =0.708, p < 0.001), and between attitude and practice scores (r = 0.327, p < 0.001)).
Discussion
The current study was conducted among religious clerics and THs respondents who are in close contact and widely accepted by a large number of community members and/or customers.
Most of the participants (60.7%) had a good knowledge toward prevention and early detection of COVID-19. This finding was consistent with a community-based bi-national survey in Egypt and Nigeria (61.6%).17 However, this finding was lower than studies in Ethiopia,6,18–21 China8 and Iran.11 The discrepancies may be due to differences in socio-demographic factors, such as educational status, sample size and study population. In the current study, only 26.3% of the study participants had completed secondary school and higher education.
Almost all, 98.5% of religious clerics and THs had heard about COVID-19, which was higher than studies in Ethiopia (91.2%),18 Nepal (91.6%)22 and the Philippines (94%).9 This may be due to the difference in the time of the study and the current study was conducted late after a lot of information was disseminated to the population compared to those studies. However, about one third of the participants (36.1%) reported that virus is the cause of the COVID-19. And this finding was lower than studies in Cameroon (77.1%)23 and Nigeria (91.9%)12 of the participants reported that COVID-19 is caused by a virus. The possible reason for the disparity may be that half of the study participants did not have formal education and also, they have no access to newspapers and the Internet. This reflects limited COVID-19 information updates on preventive measures through government officials, social media and the Internet.
Age was significantly associated with the knowledge level of participants towards COVID-19. Participants of the 18–30 years age group were three times more knowledgeable compared to the over 60 years age groups. This finding was supported by the studies done in Ethiopia,6 Egypt24 and China.25 However, the current finding was inconsistent with the study done in Saudi Arabia, which showed that the older age participants were significantly associated with good knowledge.26 This may be because a significant numberof older age participants in the current study were unable to read and write. In addition, aging-associated loss of cognition, loss of hearing and visual ability might be challenging to read or understand new information updates. These conditions are considered a challenge to access to information and result in poor knowledge.
In addition, participants who completed primary school, secondary school, college and above were significantly associated with higher knowledge score compared to those who were unable to read and write. This finding was supported by the study conducted in Iran in which the lower level of education was significantly associated with lower knowledge scores.11 This may be due to the fact that individuals with higher formal education would be self-sufficient and more likely to receive different sources of information updates than those unable to read and write participants. Access to reliable information could help prevent misinformation, misconception and ignorance about the COVID-19 pandemic.
In addition, married participants were significantly associated with higher knowledge and attitude score compared to widowed and separated study participants. This may be due to the fact that most married participants could share additional information with their partner. In addition, the lack of shared information, motivation and responsibility from the partner in unmarried participants may have an effect on the level of knowledge.
About one third (34.1%) and one sixth (15.6%) of the participants had a positive attitude and good practice score towards prevention and early detection of COVID-19, respectively. This finding was much lower than previous studies in Ethiopia,6,19,21,27 China,8 Iran11 and a bi-national survey in Africa.17 This may be due to difference in the level of education, age group and access to information such as newspapers and internet. In this study, significant numbers of study participants were older age and had no formal education that could affect the level of knowledge and attitude towards prevention and early detection of COVID-19.
Regarding attitude, about half of participants had a positive attitude towards physical distancing (44.1%), facemask use (51%) and avoiding mass gatherings (46.1%) for COVID-19 prevention. This finding was much lower than the study in India28 and Nigeria.12 This may be due to differences in educational status that may have an effect on the level of attitudes. In addition, religious clerics and THs have had strict adherence and beliefs in GOD and traditional medicines, which may have an effect on the level of attitudes towards COVID-19 preventive measures.
In the current study, only 28% and 17.8% of religious clerics and THs practiced physical distancing and facemasking, respectively. This finding was far lower than that of studies in Ethiopia,6,18 Malaysia,29 Nepal22 and the bi-national survey in Africa.17 Furthermore, 47.8% practiced proper hand washing and only 25.6% avoided mass gatherings in the weeks before. This finding was much lower than studies in Ethiopia,6,18 the Philippines9 and Malaysia.29 This may be due to the difference in the level of education, age group, information seeking behavior and access to information which could affect the level of practice. In this study half of the study participants did not have formal education and these participants had limited access to COVID-19 information updates on preventive measures. In addition, significant numbers of participants were old age group which have aging-associated loss of cognition and loss of hearing and visual ability which might be challenging to read or understand new information updates. These factors could result in poor knowledge and practice. This might be due to the reason that knowledge is the main modifier of attitudes and this could affect the level of practice towards prevention and early detection of COVID-19. Moreover, the majority of the study population may believe that God will prevent them from contracting COVID-19 infection and fail to practice properly.
In this study, the odds of good practice in the 18–30 and 31–45 age groups were 4.75 and 4.37 times higher compared to above 60 years old age group, respectively. These findings were consistent with the Iran study in which poor practices were associated with older age.11 This may be due to the majority of the older age group participants (68%) had no formal education in the current study, which may affect the level of knowledge, attitude and practice. Since the Pearson correlation showed that knowledge, attitude and practice scores were positively correlated, the effect on the level of knowledge also had an impact on the level of practice.
In addition, participants who were able to read and write, completed secondary school and university/college scored 4.03, 4.15 and 5.42 times more likely to have good practice scores, respectively, compared to those who were unable to read and write. This finding was in agreement with the studies in Ethiopia6 and Iran.11 Moreover, the study participants with known underlying disease were 5.2 times more likely to have good practice compared with participants without known underlying disease. This may be due to the fact that individuals with higher formal education would be self-sufficient and more likely to receive different sources of information updates than those unable to read and write participants. As a result, access to reliable information could help to improve preventive practices, because knowledge is positively correlated with practice score. In addition, participants with known underlying disease had more access to health education and had more health concerns that would help to have better practice score than those without underlying disease.
The positive correlations between knowledge-attitude, attitude-practice and knowledge-practice in this study reaffirm the relationship between knowledge attitude and practice towards prevention and early detection of COVID-19. It is concluded that good knowledge can lead to a positive attitude, resulting in good practices. The findings are in line with the results of previous studies in Nigeria and China.12,30 A person’s intention to a specific behavior is a function of their attitude towards that behavior.31 In the current study, the practices related to prevention and early detection of COVID-19 were dependent on the attitude of the participants. In addition, the attitude was shaped by the knowledge they possess towards prevention and early detection of COVID-19. Hence, it is inferred that good knowledge leads to a positive attitude and this positive attitude brings about a good practice.
Limitation
The response of the participants might be affected by the interviewers’ bias, and the cross-sectional nature of the study did not show the cause and effect relationship.
Conclusion
More than half of the participants had good knowledge towards prevention and early detection of COVID-19. However, less than one fourth and about one third of the participants had a good practice and attitude scores, respectively. In multivariate logistic regression: age, educational status and marital status were significantly associated with good knowledge score. In addition, age and marital status were significantly associated with a positive attitude score and age, educational status, and the presence of underlying disease were significantly associated with good practice scores.
The sensitization program should be in place to fill a gap in the knowledge, attitude and practice measures of COVID-19, specifically older age groups and those unable to read and write. Since, the attitude and practices shared by religious cleric and THs could be widely adopted by a significant number of community members in Ethiopia. Therefore, targeting this population would be essential in the fight against COVID-19, which would enable the dissemination of reliable information about COVID-19 among followers and or customers. The findings of the study could contribute to the design and implementation of COVID-19 prevention strategies.
Abbreviations
AOR, adjusted odds ratio; CDC, Communicable Disease Control; CI, confidence interval; COR, crude odds ratio; COVID-19, Coronavirus Disease 2019; EPHI, Ethiopia Public Health Institute; SPSS, Statistical Package for Social Science; TH, traditional healer; WHO, World Health Organization.
Data Sharing Statement
Most of the data generated during this study are included in this published article and additional data will be made available upon request to the corresponding author.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Board of the University of Gondar. All eligible study participants were informed about the purpose of the study, and interviews were held only with those who agreed to give written consent to participate. The study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
All participants provided written informed consent to publish this study.
Acknowledgments
The authors gratefully acknowledge the University of Gondar for technical and financial support and sincerely thank the study participants for their voluntary participation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by the University of Gondar. The University of Gondar was not involved in the study design, data collection, analysis, interpretation and manuscript writing.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Li B, Yang J, Zhao F, et al. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin Res Cardiol. 2020;109(5):531–538. doi:10.1007/s00392-020-1626-9
2. Jing Yang YZ, Gou X, Pu K, et al. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020.
3. WHO. COVID-2019 situation report 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200627-covid-19-sitrep-159.pdf?sfvrsn=93e027f6_2.
4. Novel CP. [The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China]. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(2):145–151.
5. Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Features, Evaluation and Treatment Coronavirus (COVID-19). Statpearls [internet]: StatPearls Publishing; 2020.
6. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S258736
7. Chen Y, Jin YL, Zhu LJ, et al. The network investigation on knowledge, attitude and practice about Novel coronavirus pneumonia of the residents in Anhui Province. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54:E004–E.
8. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
9. Lau LL, Hung N, Go DJ, et al. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: a cross-sectional study. J Glob Health. 2020;10(1). doi:10.7189/jogh.10.011007.
10. Gugssa SA, Haidar J. Knowledge, attitude, and practice towards epilepsy among religious cleric and traditional healers of Addis Ababa, Ethiopia. Seizure. 2020;78:57–62. doi:10.1016/j.seizure.2020.03.006
11. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ. 2020;30.
12. Reuben RC, Danladi MM, Saleh DA, Ejembi PE. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. 2020;1–14.
13. CDC. Coronavirus disease 2019. Information for healthcare professionals about Coronavirus (COVID-19) 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/index.html.
14. Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48(6):1273–1296. doi:10.1007/s11165-016-9602-2
15. Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3(1):17. doi:10.1186/1751-0473-3-17
16. Agresti A. Building and applying logistic regression models. Categorical Data Anal. 2007;211–266.
17. Elnadi H, Odetokun IA, Bolarinwa O, Ahmed Z, Okechukwu O, Al-Mustapha AI. Knowledge, attitude, and perceptions towards the 2019 Coronavirus Pandemic: a bi-national survey in Africa. medRxiv. 2020.
18. Bekele D, Tolossa T, Tsegaye R, Teshome W. The knowledge and practice towards COVID-19 pandemic prevention among residents of Ethiopia. An online cross-sectional study. BioRxiv. 2020.
19. Tadesse AW, Melese N, Eshetie S, Chane M, Ali A. Knowledge, attitude, and practice and associated factors towards COVID-19 among college students in Amhara Region, Ethiopia; a cross-sectional study. 2020.
20. Tadesse DB, Gebrewahd GT, Demoz GT. Knowledge, attitude, practice and psychological response toward COVID-19 among nurses during the COVID-19 outbreak in Northern Ethiopia, 2020. 2020.
21. Aynalem YA, Akalu TY, Gebresellassie B, Sharew NT, Shiferaw WS. Assessment of undergraduate student knowledge, practices, and attitude towards COVID-19 in Debre Berhan University, Ethiopia. 2020.
22. Vaidya B, Bhochhibhoya M, Baral R, Nakarmi S. Knowledge, attitude and practice towards COVID-19 among patients with musculoskeletal and rheumatic diseases in Nepal: a web-based cross-sectional study. 2020.
23. Nicholas T, Mandaah FV, Esemu SN, et al. COVID-19 knowledge, attitudes and practices in a conflict affected area of the South West Region of Cameroon. Pan Afr Med J. 2020;35(Supp 2). doi:10.11604/pamj.supp.2020.35.2.22963.
24. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;1–10.
25. Wolf MS, Serper M, Opsasnick L, et al. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the US outbreak: a cross-sectional survey. Ann Internal Med. 2020.
26. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Health. 2020;8. 10.3389/fpubh.2020.00217
27. Jemal B, Ferede ZA, Mola S, et al. Knowledge, attitude and practice of healthcare workers towards COVID-19 and its prevention in Ethiopia: a multicenter study. 2020.
28. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
29. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E, Tu W-J. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
30. Peng Y, Pei C, Zheng Y, et al. A cross-sectional survey of knowledge, attitude and practice associated with COVID-19 among undergraduate students in China. BMC Public Health. 2020;20(1):1–8. doi:10.1186/s12889-020-09392-z
31. Fisher WA, Fisher JD, Rye BJ. Understanding and promoting AIDS-preventive behavior: insights from the theory of reasoned action. Health Psychol. 1995;14(3):255. doi:10.1037/0278-6133.14.3.255
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.