Back to Journals » Nature and Science of Sleep » Volume 18

Knowledge, Attitudes, and Practices Toward Obstructive Sleep Apnea in China: A Structural Equation Modeling Study
Authors Wang Y ![]() , Zhou H, Huang J, Yin M, Li Y
, Zhou H, Huang J, Yin M, Li Y
Received 21 October 2025
Accepted for publication 4 January 2026
Published 17 January 2026 Volume 2026:18 565615
DOI https://doi.org/10.2147/NSS.S565615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yina Wang,1 Hu Zhou,2 Jing Huang,1 Meilong Yin,3 Yayong Li3
1Department of Geriatrics, The Second Xiangya Hospital of Central South University, Changsha, 410011, People’s Republic of China; 2College of Information Science and Engineering, Hunan University, Changsha, Hunan, People’s Republic of China; 3Department of Emergency, The Third Xiangya Hospital of Central South University, Changsha, 410013, People’s Republic of China
Correspondence: Yayong Li, Department of Emergency, The Third Xiangya Hospital of Central South University, Changsha, 410013, People’s Republic of China, Email [email protected]
Background: Self-management is essential for the management of obstructive sleep apnea (OSA); however, the general public’s understanding of OSA in China remains unclear. This study aimed to investigate the knowledge, attitudes, and practices (KAP) concerning OSA among Chinese adults. This information is essential for informing population-level prevention strategies and strengthening public health responses to OSA.
Methods: This cross-sectional study was conducted between October 2022 and October 2023 among Chinese adults. Based on a knowledge–attitude–practice conceptual framework, we hypothesized that knowledge would directly influence attitudes, attitudes would directly influence practices, and knowledge would exert both direct and indirect effects on practices.
Results: A total of 1,145 questionnaires were collected, and 850 valid responses were analyzed (valid response rate: 74.76%). The mean scores for knowledge, attitudes, and practices were 20.84 (0– 42), 37.96 (9– 45), and 38.03 (10– 50), respectively. Knowledge was positively associated with attitude (r = 0.502, P < 0.001) and practice (r = 0.434, P < 0.001), while attitude showed a strong correlation with practice (r = 0.722, P < 0.001). Structural equation modeling showed that education positively affected knowledge (β = 0.166, P = 0.005). Knowledge directly influenced attitude (β = 0.502, P < 0.001) and practice (β = 0.096, P < 0.001), and indirectly affected practice through attitude (β = 0.338, P = 0.012). Attitude had a strong direct effect on practice (β = 0.674, P < 0.001).
Conclusion: Chinese adults demonstrated a limited understanding of OSA; however, they generally exhibited positive attitudes and moderate engagement in related practices. This study emphasized the need to strengthen public knowledge about OSA, which may support improvements in attitudes and practices. The observed pathways among knowledge, attitudes, and practices suggest that increasing public awareness could play an important role in shaping health-related behaviors.
Keywords: knowledge, attitudes, practices, obstructive sleep apnea, cross-sectional study, structural equation modeling
Introduction
Obstructive sleep apnea (OSA) is a prevalent sleep disorder characterized by recurrent episodes of upper airway obstruction during sleep, leading to intermittent hypoxia and disrupted sleep architecture. OSA considerably impairs quality of life and is associated with an elevated risk of cardiovascular diseases, cognitive deficits, and motor vehicle accidents.1–7 Approximately 936 million adults aged 30 to 69 globally are affected by OSA, with China bearing the highest burden, accounting for 176 million cases. In China, the estimated prevalence of OSA is 23.6% for mild to severe cases (apnea-hypopnea index [AHI] ≥5 events/hour) and 8.8% for moderate to severe cases (AHI ≥15 events/hour).8
Despite its high prevalence, only approximately 1% of individuals diagnosed with OSA in China receive appropriate treatment. This low treatment rate is primarily attributable to the limited availability of diagnostic modalities, such as polysomnography, and therapeutic interventions like continuous positive airway pressure (CPAP), which are often resource-intensive and predominantly available in specialized medical facilities.1 Furthermore, nearly two-thirds of diagnosed patients opt not to pursue treatment, mainly due to the perception that their condition is not severe (53.4%) or due to the inconveniences associated with CPAP devices, including mask discomfort and nasal congestion (15.3%).9
Public awareness of OSA is markedly insufficient, with approximately 90% of affected individuals unaware of their diagnosis before medical evaluation.9,10 A 2022 study indicated that although 62.8% of the general Chinese population had heard of OSA, only 37.2% could accurately identify its key characteristics, underscoring a significant knowledge gap.11 Additionally, the study revealed that 89.4% of respondents expressed a willingness to receive education about OSA, primarily through the internet and new media platforms.11
Given China’s substantial population (approximately 1.4 billion) and its status as the country with the highest incidence of OSA, it is imperative to understand the knowledge, attitudes, and practices (KAP) regarding OSA among Chinese adults to develop effective public health interventions and improve treatment adherence. To guide this investigation, the KAP framework provides a widely used behavioral model that conceptualizes how awareness shapes beliefs and subsequently influences health-related actions, making it appropriate for examining OSA-related behaviors.12 SEM has been widely applied in public health research to examine directional pathways among behavioral constructs.13 While previous KAP studies have predominantly focused on healthcare providers, such as primary care physicians and dentists,14,15 there exists a notable paucity of research targeting the general population. This study aims to address this gap by investigating the KAP related to OSA among Chinese adults, utilizing a structural equation model to analyze the interrelationships among these variables. Moreover, focusing on the general adult population, rather than only high-risk subgroups, is essential because most individuals with OSA remain undiagnosed and asymptomatic, and population-level prevention requires understanding awareness and behaviors across the broader community.16
Material and Methods
Study Design and Participants
This cross-sectional study was conducted between October 2022 and October 2023 among Chinese adults, using a self-administered questionnaire. Participants aged 18 years or older were invited to complete an electronic questionnaire either during their hospital visit or through links shared by researchers and their social media contacts. The study received ethical approval from the Medical Ethics Committee of Xiangya Second Hospital, Central South University (No. 735, 2022), and informed consent was obtained from all participants.
Questionnaire
The questionnaire (Supplementary Material) was designed based on the OSA screening study in the general population, conducted by Sia et al,17 and the OSAKA questionnaire proposed by Schotland and Jeffe,18 as well as the Chinese OSA diagnosis and treatment guidelines.19 The valid questionnaire responses demonstrated satisfactory reliability and validity (Cronbach’s α = 0.941, KMO = 0.967), indicating good validity and reliability. In addition, a confirmatory factor analysis (CFA) was performed to further evaluate the construct validity of the questionnaire. The overall model demonstrated acceptable fit (Chi-square fit statistic/degrees of freedom (CMIN/DF) = 3.686; root mean square error of approximation (RMSEA) = 0.056; incremental fit index (IFI) = 0.892; Tucker-Lewis index (TLI) = 0.886; CFI = 0.892) (Supplementary Figure 1).
The finalized questionnaire comprised four components: demographic characteristics, knowledge, attitude, and practice. The knowledge component included 42 items, each scored as 1 for a correct response and 0 for an incorrect or unclear one, giving a possible total score between 0 and 42. The attitude component contained nine items assessed on a five-point Likert scale, ranging from strongly agree (5) to strongly disagree (1), with an overall score span of 9 to 45. The practice component consisted of 12 items, also rated on a five-point Likert scale from “strongly agree/always” (5 points) to “strongly disagree/never” (1 point). Items 9 and 10 were excluded from the total practice score, resulting in a possible range of 10 to 50 points. To assess participants’ overall Knowledge, Attitude, and Practice (KAP) levels, knowledge scores were categorized as poor (≤60%), moderate (60–80%), and good (>80%). Similarly, attitude was classified as negative (≤60%), neutral (60–80%), and positive (>80%), while practice was defined as inappropriate (≤60%), acceptable (60–80%), and appropriate (>80%), in accordance with modified Bloom’s cut-off criteria.20
The questionnaire was distributed via “Questionnaire Star” (https://questionstar.com), a Chinese web-based survey platform. A secure assessment page was created, and a quick response (QR) code was generated for dissemination. To ensure data quality and response completeness, each IP address was limited to one submission, and all items were mandatory. The research team reviewed all returned questionnaires for completeness, internal consistency, and appropriateness. Participants who were unable to access the online platform independently received assistance from family members, guardians, or healthcare personnel, who facilitated completion of the electronic questionnaire through oral inquiry. Incomplete, inconsistent, or duplicate responses were excluded from the final analysis.
Sample Size Estimation
The required sample size for this study was calculated based on Cochran’s sample size estimation equation and the expected proportion, as determined in a previous KAP study.21 The single population proportion formula was used, based on the assumption that the probability of having low K, A, and P scores was 50.0%, with a 95% CI and a 5% margin of error. The result was determined to be at least 384. By adding a non-response rate of 10%, the total required sample size was 423.
Statistical Analysis
Statistical analyses were conducted using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means and standard deviations (SD), whereas categorical variables were summarized as frequencies and percentages (n, %). For normally distributed continuous variables, comparisons were made using independent sample t-tests or one-way analysis of variance (ANOVA). Non-normally distributed variables were analyzed with the Wilcoxon-Mann–Whitney test or Kruskal–Wallis ANOVA. Spearman correlation analysis was used to assess the relationships among KAP scores. Structural equation modeling (SEM) was further applied to evaluate interrelations among KAP dimensions. The SEM hypotheses were: (1) knowledge directly affects attitude, (2) attitude directly affects practice, and (3) knowledge exerts both direct and indirect effects on practice. In the structural equation modeling (SEM) analysis, baseline characteristics including age, education level, occupation, and chronic disease status were incorporated as covariates to reduce potential confounding. These variables were selected based on prior evidence suggesting their relevance to health literacy and health-related behaviors. The hypothesized model was constructed according to the KAP framework, specifying paths from knowledge to attitude, from attitude to practice, and both direct and indirect effects from knowledge to practice. Alternative path specifications were evaluated, but the final model was retained based on theoretical rationale and superior model fit indices. All tests were two-sided, and a P-value < 0.05 was considered statistically significant.
Results
Demographic Characteristics
A total of 1145 questionnaires were collected, of which 295 were excluded due to logical conflicts or all questions being answered with the same response. After exclusion, 850 valid questionnaires remained, corresponding to the effectiveness rate of 74.76%. Among the included participants with valid questionnaire responses, the majority (61.65%) were female, residing in the city area (79.88%), and of Han ethnicity (95.29%), with a level of education of college or above (75.65%) (Supplementary Table 1). The knowledge, attitudes, and practices scores were 20.84 ± 14.13 (possible range: 0–42), 37.95 ± 6.26 (possible range: 9–45), and 38.03 ± 6.97 (possible range: 10–50), respectively (Table 1).
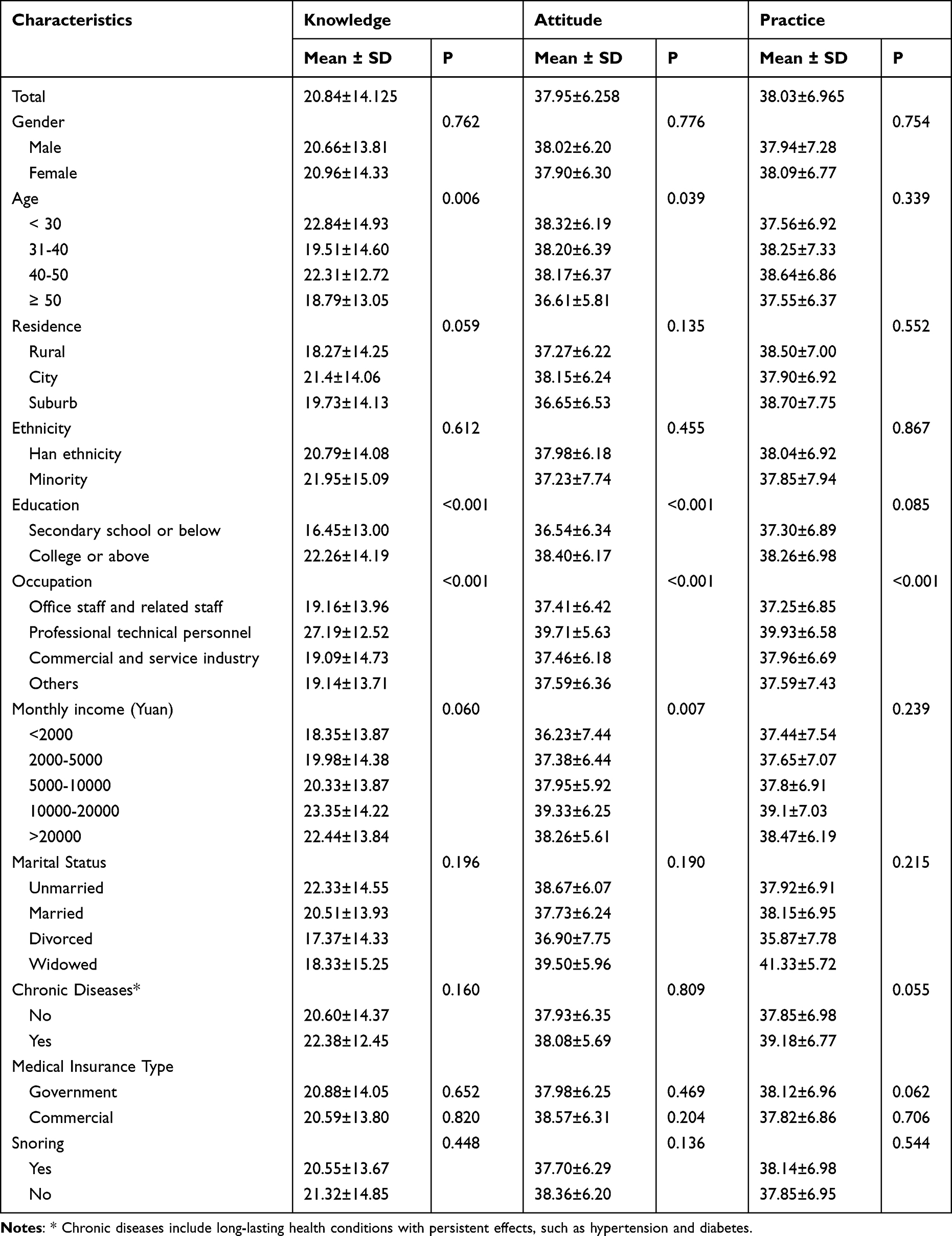 |
Table 1 The Knowledge, Attitude, and Practice Towards Obstructive Sleep Apnea |
Distribution of Knowledge, Attitude, and Practice Dimension
KAP responses showed that 84.83% of participants identified at least one risk factor for OSA, most commonly obesity (75.5%) and nasal congestion (68.1%). A total of 79.53% recognized at least one symptom, with snoring (70.2%) and apnea (62.6%) being the most frequently reported. Awareness of OSA-related hazards reached 68.00%, and increased mortality was the most familiar consequence (53.3%). For treatment, 69.76% identified at least one option, most commonly weight loss (59.6%) and exercise (58%). The least known items included nocturia (31.8%), atrial fibrillation (27.2%), and continuous positive airway pressure (44.8%). Most respondents demonstrated neutral or positive attitudes toward OSA prevention, and although few routinely paid attention to snoring, willingness to seek medical evaluation or treatment when experiencing OSA-related symptoms was relatively high (Supplementary Tables 2–4).
Spearman Correlation Analysis
Spearman correlation analysis revealed significant positive associations between knowledge and attitude (r = 0.502, P < 0.001), knowledge and practice (r = 0.434, P < 0.001), and attitude and practice (r = 0.722, P < 0.001) (Table 2).
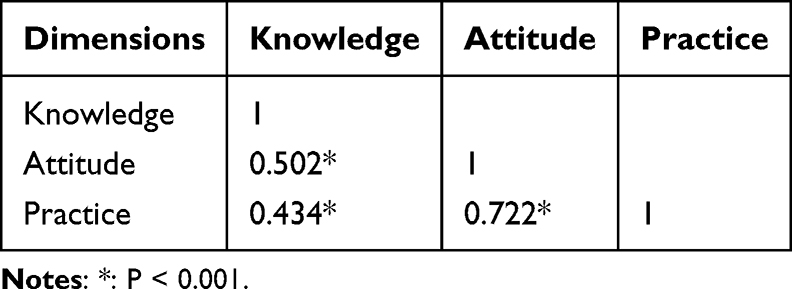 |
Table 2 Spearman Correlation Between Knowledge, Attitude, and Practice |
Structural Equation Model Analysis
The SEM demonstrated highly favorable model fit indices: CMIN/DF = 2.653 (reference: 1–3 excellent, 3–5 good), RMSEA = 0.034 (reference < 0.08), IFI = 0.983 (reference > 0.80 good), TLI = 0.968 (reference > 0.80 good), and comparative fit index = 0.983 (reference > 0.80 good), indicating an excellent model fit (Supplementary Table 5). The SEM results showed that education exerted a direct positive effect on knowledge (β = 0.166, P = 0.005), whereas occupation and age showed no significant associations. Knowledge had a direct positive influence on attitude (β = 0.502, P < 0.001) and practice (β = 0.096, P < 0.001). Attitude also demonstrated a strong direct effect on practice (β = 0.674, P < 0.001). In addition, knowledge exerted a significant indirect effect on practice through attitude (β = 0.338, P = 0.012). Chronic diseases, occupation, and age did not exhibit significant direct effects on practice. (Figure 1, Table 3, and Supplementary Table 6).
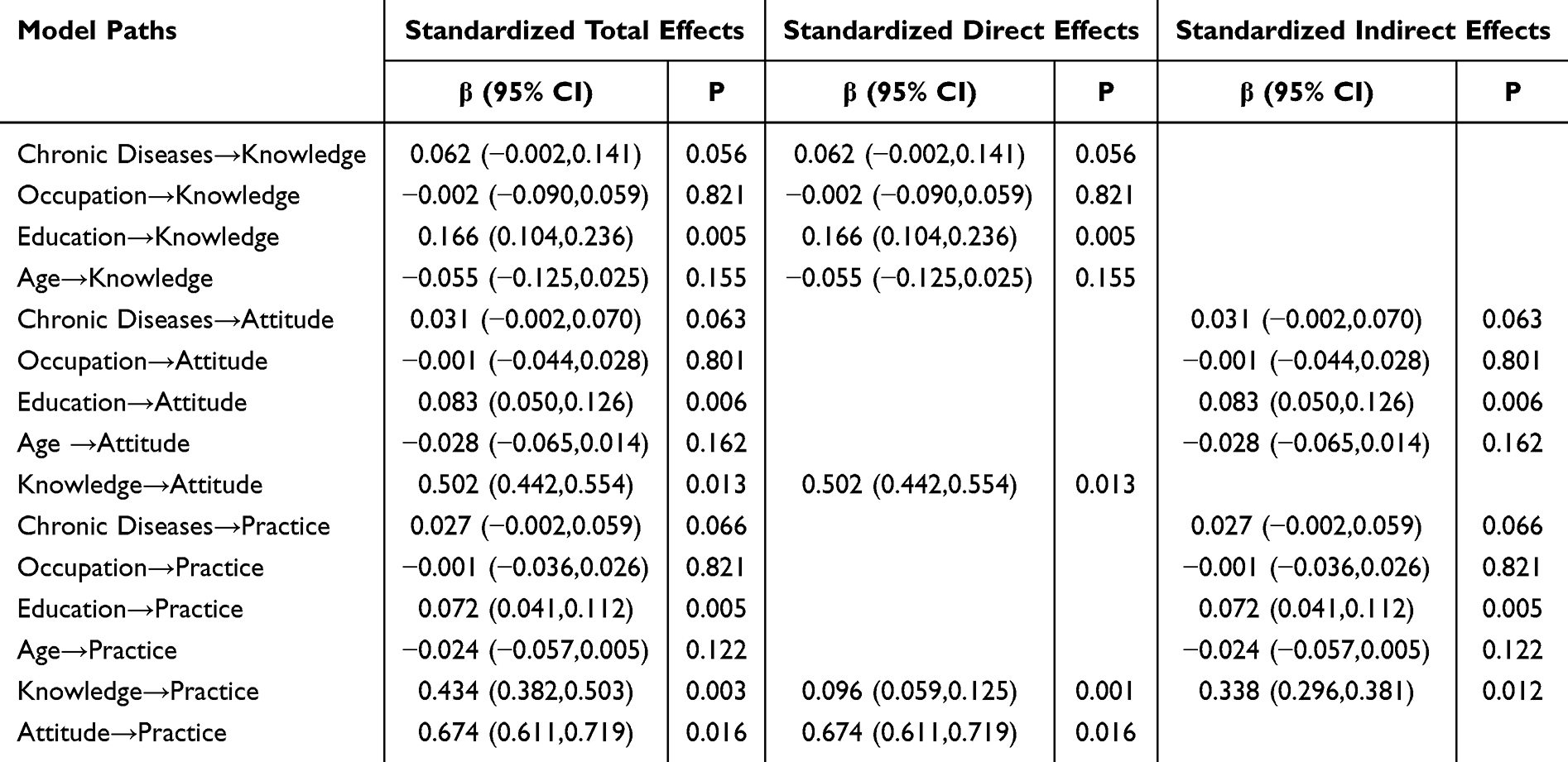 |
Table 3 Structural Equation Modeling Analysis |
 |
Figure 1 Graphical representation of the structural equation model. Notes: e1–e7 represent measurement error terms of the observed variables, reflecting unexplained variance after measurement. |
Discussion
This study found that awareness of OSA among the general population in China is relatively inadequate; however, a positive attitude and moderate practices regarding OSA management exist. The findings suggest that positive attitudes toward OSA management are closely linked to better practices, highlighting the need for education. The findings highlight barriers that contribute to the alarmingly low consultation and treatment rates among OSA patients. They can inform the development of educational interventions to enhance self-recognition and risk assessment for individuals with OSA by influencing their knowledge and attitudes.
The present study indicated that while awareness of OSA was relatively low, there was a positive attitude towards its management, and practices related to OSA were appropriate. The study’s findings are supported by recent research conducted by Pan et al,10 which indicated that only 37.2% of respondents could accurately identify key features of OSA, despite the participants being predominantly from urban areas with higher education levels. That previous study also found limited knowledge about OSA among the general Chinese population, despite a high demand for education on the topic. This underscores a substantial knowledge gap in China and the need for targeted educational interventions. Similarly, Liao et al9 found that nearly two-thirds of diagnosed OSA patients in China choose not to pursue treatment, often perceiving their condition as less serious or finding CPAP devices cumbersome. Our findings align with the notion that, while attitudes and practices are relatively positive, actual treatment-seeking behavior may be low, possibly due to insufficient awareness of the seriousness of OSA. Nevertheless, the present study builds upon previous studies by employing a SEM analysis to explore the interrelationships among KAP dimensions and other factors, revealing that education has a significant influence on knowledge, which subsequently affected attitudes and practices. Furthermore, attitudes demonstrated a substantial and direct influence on practices, underscoring their central role in translating knowledge into behavioral engagement. Knowledge also exerted an indirect effect on practice through attitudes, highlighting the mediating role of attitudinal change within the KAP pathway. Therefore, educational interventions should focus on disseminating accurate information about OSA and fostering positive attitudes toward its management. Zhang et al19 demonstrated that brief educational interventions significantly improved OSA knowledge among medical students in Guangzhou, suggesting scalable strategies for the general population. In contrast, age, occupation, and chronic disease status did not show significant associations with any of the KAP dimensions in the SEM.
The positive associations among KAP dimensions indicate that enhancing knowledge about OSA can directly improve practices and also indirectly do so through its strong effect on attitudes. It is particularly important given the low treatment rates for OSA in China, as noted by.9 Our findings suggest that targeted educational campaigns could help bridge this gap by increasing awareness of the seriousness of OSA and the benefits of treatment. For instance, interventions could focus on disseminating accurate information about OSA symptoms, risks, and treatment options through accessible channels such as social media, community health programs, and workplace wellness initiatives.
Cultural factors may also significantly influence OSA awareness and management in China.22,23 Traditional Chinese beliefs about health and sleep, as well as reliance on family and community networks, may influence how individuals perceive and respond to OSA symptoms.10,24 For example, the emphasis on family harmony in Chinese culture might lead to underreporting of symptoms to avoid burdening family members, or there may be a preference for traditional remedies over CPAP due to perceived discomfort or cultural unfamiliarity. Future educational interventions should consider integrating traditional and modern approaches to enhance acceptance and adherence to treatment. Additionally, community-based programs that leverage family and social networks could be effective in promoting OSA awareness and encouraging early diagnosis.
The findings of this study have significant implications for public health policy in China. From a public health perspective, the findings underscore the need to develop comprehensive educational strategies to enhance public understanding of OSA. Given the high prevalence of OSA and the low public awareness, nationwide educational campaigns are needed to improve understanding of symptoms, risks, and the value of early diagnosis. Additionally, integrating OSA screening into routine health check-ups for high-risk groups, such as overweight individuals or those with hypertension, could facilitate early detection. Making CPAP machines more affordable through subsidies or insurance coverage could improve treatment adherence. Policymakers should also consider cultural factors when designing intervention programs to ensure they are acceptable and effective within the Chinese cultural context. Zhang et al25 highlighted that undiagnosed OSA eventually burdens society and healthcare systems when the patient’s condition worsens or complications occur.26
Future research should explore personalized medicine approaches to OSA management in China, as suggested by Zhang.23,26,27 Given the heterogeneity of OSA, tailoring diagnostic and treatment strategies to individual patient characteristics could improve outcomes and adherence to therapy.28,29 In addition, targeted interventions for specific populations, such as older adults or individuals with comorbidities, could provide more detailed insights and guide more effective public health strategies. Recent clinical guidelines, such as the Chinese consensus report on OSA management in patients with cardiovascular disease (2024),30 emphasize multidisciplinary approaches and early intervention, which could be integrated into future research and policy.
However, this study has several limitations. First, the population was predominantly female, despite the higher prevalence of OSA among males. This discrepancy may indicate that female respondents are more interested in acquiring OSA knowledge relevant to their family members. Second, the questionnaires were distributed to hospital visitors and shared on social media, which may have introduced selection bias. Such bias could lead to overestimation of attitudes and self-reported practices, thereby affecting the internal validity of the associations observed among the KAP dimensions. While utilizing two participant sources enhanced the representativeness of the study sample, certain social groups, such as elderly individuals without internet access, were largely excluded, resulting in a mean participant age of under 50 years. Future studies should include older and underserved populations, who tend to have lower knowledge levels and may require more targeted education. Third, the responses in the practical section of the questionnaire cannot be verified without investigating the actual behaviors of participants. Consequently, further research is needed to explore the healthcare-seeking behaviors of OSA patients. Additionally, questionnaire-based studies are susceptible to social desirability bias, as participants may provide responses that align with societal expectations. For instance, they might feign a high level of knowledge or education, leading to positive answers to questions they do not fully understand. Finally, certain social groups may have been excluded from participation due to the distribution method, which could result in a skewed understanding of KAP if these groups, such as the elderly or individuals without access to social media and the internet, were included.
Despite these limitations, the present study provides important insights into the KAP regarding OSA among Chinese adults and highlights the need for targeted educational interventions. Future research should focus on developing and testing specific educational strategies that are culturally appropriate and effective in improving KAP. Longitudinal studies could also be conducted to assess the long-term impact of these interventions on OSA management behaviors and health outcomes. Additionally, qualitative studies could explore cultural barriers to treatment adherence and identify ways to integrate traditional and modern approaches to OSA management. Finally, research on personalized medicine approaches, as suggested by Su & Xiao,27 could help tailor diagnostic and treatment strategies to individual patient characteristics, potentially improving outcomes and adherence to therapy. Furthermore, important potential confounders such as health literacy and socioeconomic status were not measured in this study, and these factors may influence individuals’ knowledge levels and health-related behaviors. Future research incorporating these variables will help improve the explanatory power and validity of KAP-based models.
Conclusions
Chinese adults demonstrated a limited understanding of OSA; however, they generally exhibited positive attitudes and moderate engagement in related practices. This study emphasized the need to strengthen public knowledge about OSA, which may support improvements in attitudes and practices rather than guarantee them. The observed pathways among knowledge, attitudes, and practices suggest that efforts to increase public awareness could play an important role in shaping health-related behaviors. Addressing identified knowledge gaps and fostering supportive attitudes may encourage better health-seeking behaviors among individuals at risk of OSA. While policy and cultural considerations remain relevant, their roles should be interpreted cautiously, as they were not directly evaluated in this study.
Abbreviations
OSA, obstructive sleep apnea; KAP, knowledge, attitudes, and practices; AHI, apnea-hypopnea index; CPAP, continuous positive airway pressure; QR, quick response; SD, standard deviations; ANOVA, analysis of variance; SEM, structural equation modeling.
Data Sharing Statement
The raw data underlying this study are not publicly available due to privacy and institutional restrictions but are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All procedures were performed in accordance with the ethical standards outlined in the 1964 Declaration of Helsinki and its subsequent amendments. This study was approved by the Ethics Committee of the Second Xiangya Hospital of Central South University, China (2022 No. 735), and individual Informed consent was obtained from the study participants. The study was carried out in accordance with the applicable guidelines and regulations.
Author Contributions
Yina Wang: conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, resources, visualization, writing – original draft, and writing – review and editing.
Hu Zhou: data curation, investigation, resources, writing – original draft, and writing – review and editing.
Jing Huang: data curation, investigation, resources, writing – original draft, and writing – review and editing.
Meilong Yin: data curation, investigation, resources, writing – original draft, and writing – review and editing.
Yayong Li: conceptualization, data curation, formal analysis, investigation, methodology, resources, supervision, validation, visualization, writing – original draft, and writing – review and editing.
All authors gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Scientific Fund of Hunan Province (2023JJ30786, 2025JJ50713), Health and Health Project of Hunan Provincial Department of Finance (Xiang Cai She Zhi [2023] No. 79, Xiang Cai She Zhi [2024] No.0031), and Degree & Postgraduate Education Reform Project of Central South University (2022JGB075, 2023YJSKS035), China.
Disclosure
The authors declare that they have no competing interests.
References
1. West SD, Turnbull C. Obstructive sleep apnoea. Eye. 2018;32(5):889–10. doi:10.1038/s41433-017-0006-y
2. Rosa D, Perger E, Villa G, et al. Pharmacotherapy for obstructive sleep apnoea and coupled life: a descriptive phenomenological study of a complex interaction. Healthcare. 2022;10(10).
3. Bergeron M, Ishman SL. Persistent obstructive sleep apnea burden on family finances and quality of life. Otolaryngol Head Neck Surg. 2021;165(3):483–489. doi:10.1177/0194599820986566
4. Gnoni V, Mesquita M, O’Regan D, et al. Distinct cognitive changes in male patients with obstructive sleep apnoea without co-morbidities. Front Sleep. 2023;2:1097946. doi:10.3389/frsle.2023.1097946
5. Laczay B, Faulx MD. Obstructive sleep apnea and cardiac arrhythmias: a contemporary review. J Clin Med. 2021;10(17):3785. doi:10.3390/jcm10173785
6. Pocobelli G, Akosile MA, Hansen RN, et al. Obstructive sleep apnea and risk of motor vehicle accident. Sleep Med. 2021;85:196–203. doi:10.1016/j.sleep.2021.07.019
7. Miller MA, Cappuccio FP. A systematic review of COVID-19 and obstructive sleep apnoea. Sleep Med Rev. 2021;55:101382. doi:10.1016/j.smrv.2020.101382
8. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
9. Liao WJ, Song LJ, Yi HL, et al. Treatment choice by patients with obstructive sleep apnea: data from two centers in China. J Thorac Dis. 2018;10(3):1941–1950. doi:10.21037/jtd.2018.03.135
10. Pan Z, Ma T, Zeng Q, et al. People’s knowledge, attitudes, practice, and healthcare education demand regarding OSA: a cross-sectional study among Chinese general populations. Front Public Health. 2023;11:1128334. doi:10.3389/fpubh.2023.1128334
11. Alzahrani MM, Alghamdi AA, Alghamdi SA, Alotaibi RK. Knowledge and attitude of dentists towards obstructive sleep apnea. Int Dent J. 2022;72(3):315–321. doi:10.1016/j.identj.2021.05.004
12. Zarei F, Dehghani A, Ratansiri A, et al. ChecKAP: a checklist for reporting a knowledge, attitude, and practice (KAP) study. Asian Pac J Cancer Prev. 2024;25(7):2573–2577. doi:10.31557/APJCP.2024.25.7.2573
13. Zhang Z. Structural equation modeling in the context of clinical research. Ann Transl Med. 2017;5(5):102. doi:10.21037/atm.2016.09.25
14. Devaraj NK. Knowledge, attitude, and practice regarding obstructive sleep apnea among primary care physicians. Sleep Breath. 2020;24(4):1581–1590. doi:10.1007/s11325-020-02040-1
15. Kale SS, Kakodkar P, Shetiya SH. Obstructive sleep apnea domains: knowledge, attitude and practice results of dentists from a dental college in India. Sleep Sci. 2020;13(1):3–9. doi:10.5935/1984-0063.20190121
16. Iannella G, Pace A, Bellizzi MG, et al. The global burden of obstructive sleep apnea. Diagnostics. 2025;15(9).
17. Sia CH, Hong Y, Tan LWL, van Dam RM, Lee CH, Tan A. Awareness and knowledge of obstructive sleep apnea among the general population. Sleep Med. 2017;36:10–17. doi:10.1016/j.sleep.2017.03.030
18. Schotland HM, Jeffe DB. Development of the obstructive sleep apnea knowledge and attitudes (OSAKA) questionnaire. Sleep Med. 2003;4(5):443–450. doi:10.1016/S1389-9457(03)00073-X
19. Zhang X. Guidelines for the diagnosis and treatment of obstructive sleep apnea hypopnea syndrome (2011 revision). Chin J Tuberc Respir Dis. 2012;1:9–12.
20. He Q, Wang G, He J, et al. Knowledge, attitude and practice regarding occupational protection against COVID-19 among midwives in China: a nationwide cross-sectional study. Int J Disaster Risk Reduct. 2022;79:103184. doi:10.1016/j.ijdrr.2022.103184
21. Thirunavukkarasu A, Al-Hazmi AH, Dar UF, et al. Knowledge, attitude and practice towards bio-medical waste management among healthcare workers: a northern Saudi study. PeerJ. 2022;10:e13773.
22. Ye L, Li W, Willis DG. Facilitators and barriers to getting obstructive sleep apnea diagnosed: perspectives from patients and their partners. J Clin Sleep Med. 2022;18(3):835–841. doi:10.5664/jcsm.9738
23. Zhang R, Ou Q. What can we do for obstructive sleep apnea patients in China? Sleep Re. 2024;1(1):13–18. doi:10.1002/slp2.11
24. Lv R, Zhao Y, Wang Z, et al. Obstructive sleep apnea hypopnea syndrome in ancient traditional Chinese medicine. Sleep Breath. 2023;27(4):1597–1610. doi:10.1007/s11325-022-02708-w
25. Zheng Z, Zhu J, Liang H, et al. Validation of GOAL questionnaire as screening tool for clinical obstructive sleep apnea: a large sample study in China. Front Neurosci. 2022;16:1046603. doi:10.3389/fnins.2022.1046603
26. Wei Y, Liu Y, Ayas N, Laher I. A narrative review on obstructive sleep apnea in China: a sleeping giant in disease pathology. Heart Mind. 2022;6(4):232–241. doi:10.4103/hm.hm_49_22
27. Su L, Xiao Y. Application of personalized medicine to obstructive sleep apnea in China. Sleep Med. 2021;87:22–29. doi:10.1016/j.sleep.2021.08.014
28. Sunwoo BY, Light M, Malhotra A. Strategies to augment adherence in the management of sleep-disordered breathing. Respirology. 2020;25(4):363–371. doi:10.1111/resp.13589
29. Kraiwattanapong J, Rattanaarun K, Cunteerasup A, Papassornsiri T, Balankura T, Pavarajarn S. Clinical characteristics and treatment preferences of obstructive sleep apnea. Sci Rep. 2025;15(1):18976. doi:10.1038/s41598-025-03816-9
30. Huang Z, Zhao Q, Zhao Z, et al. Chinese consensus report on the assessment and management of obstructive sleep apnea in patients with cardiovascular disease: 2024 edition. Sleep Med. 2025;126:248–259. doi:10.1016/j.sleep.2024.12.019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.