Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Knowledge, Attitudes, and Practices Regarding Cardiac Rehabilitation Among Patients with Chronic Heart Failure and Their Families: A Cross-Sectional Study
Authors Gao X, Yang J, Cao W, Liu Y, Zhao T
Received 11 July 2025
Accepted for publication 21 October 2025
Published 31 October 2025 Volume 2025:18 Pages 7073—7087
DOI https://doi.org/10.2147/JMDH.S553152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Xiaohua Gao,1,* Jianzhou Yang,2,* Wenjun Cao,3 Yaoqiang Liu,4 Tingting Zhao1
1Department of Cardiovascular Medicine, Heping Hospital Affiliated to Changzhi Medical College, Changzhi, Shanxi, People’s Republic of China; 2Department of Public Health and Preventive Medicine, Changzhi Medical College, Changzhi, Shanxi, People’s Republic of China; 3Department of Science and Technology, Changzhi Medical College, Changzhi, Shanxi, People’s Republic of China; 4Department of Internal Medicine, Huaihai Hospital Affiliated to Changzhi Medical College, Changzhi, Shanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohua Gao, Email [email protected]
Purpose: Chronic heart failure (CHF) impairs heart function and affects patients’ well-being, while cardiac rehabilitation (CR) improves outcomes. In this cross-sectional survey, we assessed knowledge, attitudes, and practices (KAP) related to CR in patients with CHF and their family caregivers.
Patients and Methods: A cross-sectional survey was conducted at Heping Hospital, affiliated with Changzhi Medical College, from July 1 to October 10, 2024. Data were collected using questionnaires that included demographic information and evaluations of KAP scores. A total of 500 questionnaires were distributed to eligible participants.
Results: Of the 500 questionnaires distributed, 492 valid responses were obtained, yielding a response rate of 98.4%. Among the respondents, 277 (56.3%) were patients, with 191 (38.8%) aged 60 or older. The mean knowledge, attitude, and practice scores were 6.90 ± 5.63 (range: 0– 30), 33.43 ± 3.31 (range: 9– 45), and 28.01 ± 4.46 (range: 8– 40), respectively. Multivariate logistic regression analysis identified several factors associated with proactive practice: knowledge score (OR = 1.114, 95% CI: [1.053, 1.179]), college degree (OR = 3.089, 95% CI: [1.054, 9.053]), absence of medical insurance (OR = 6.762, 95% CI: [3.597, 12.713]), no family history of heart issues (OR = 4.414, 95% CI: [2.351, 8.288]), and non-participation in CR (OR = 0.206, 95% CI: [0.087, 0.489]). The SEM results showed that knowledge directly affected attitude (β = 0.321, p < 0.001) and practice (β = 0.285, p = 0.004), and attitude directly affected practice (β = 0.217, p < 0.001). Additionally, knowledge indirectly affected practice through attitude (β = 0.355, p < 0.001).
Conclusion: Patients with CHF and their families showed insufficient knowledge but positive attitudes and proactive practices regarding CR. Targeted educational interventions are recommended to improve knowledge, particularly for younger patients and those without prior CR training, to enhance rehabilitation effectiveness.
Keywords: chronic heart failure, cardiac rehabilitation, KAP, cross-sectional studies, health education
Introduction
Chronic heart failure (CHF) is a complex clinical condition characterized by structural and/or functional abnormalities, leading to impaired ventricular contraction and/or relaxation of the heart.1 As the final stage of various cardiovascular diseases, CHF severely impacts patients’ functional and psychosocial well-being, manifesting through symptoms like breathlessness, reduced endurance, and psychological distress.2 Patients with CHF often experience frequent recurrences of fatigue, dyspnea, and acute exacerbations, which limit their daily activities.3
Cardiac rehabilitation (CR) is a multidisciplinary, guideline-recommended secondary prevention program designed to improve exercise capacity, reduce cardiovascular risks, and enhance the health-related quality of life in patients with stable heart failure, regardless of preserved or reduced ejection fraction.3 Over the past decades, CR’s safety and efficacy have been well-established, and it is now widely recommended by international guidelines as a critical component of routine CHF management.4,5 However, despite the proven benefits, a significant proportion of eligible patients do not participate in CR programs. Globally, around 66.7% of countries have reached the target of providing at least 12 CR sessions on average, with 32.4% offering home-based CR programs as an alternative.6
However, data specific to China remain limited, and participation rates may differ substantially from global averages. Previous research has shown that only 16.3% of discharged patients engage in CR.7 Furthermore, it is unclear whether healthcare providers consistently provide educational interventions related to CR, and if institutional policies or clinical guidelines explicitly address this educational responsibility.8 Typically, decisions regarding patient education on CR are left to cardiologists, nurses, or pharmacists; however, standardized approaches to track or evaluate these educational efforts are limited.9
The KAP model plays a crucial role in influencing health behaviors.10 The questionnaire is commonly used to assess the KAP of specific populations in healthcare, helping to determine the need for and acceptance of relevant interventions.11 This model is grounded in the concept that knowledge positively shapes attitudes, which in turn drive practices.12 Family members are often key contributors to patient care and decision-making, making their involvement in CR critical for ensuring patient adherence and support. Understanding the KAP of both patients and their family members can reveal knowledge gaps or misconceptions that may impede effective participation in CR, thus informing more tailored interventions aimed at improving long-term outcomes in heart failure management.
To our knowledge, no KAP studies regarding CR among CHF patients and their families have been conducted in China. Thus, this study aims to assess the KAP related to CR among patients with CHF and their family members.
Materials and Methods
Study Design, Setting, and Participants
This cross-sectional study was conducted at Heping Hospital, affiliated with Changzhi Medical College, from July 1, 2024, to October 10, 2024. The participants included individuals with CHF and caregivers. Ethical approval for the study was obtained from the Ethics Committee of Heping Hospital, and informed consent was secured from all participants. Inclusion criteria were: 1) patients diagnosed with CHF, with cardiac function grades II–IV, based on the Guidelines for the Diagnosis and Treatment of Chronic Heart Failure (2014). 2) adult family members of such patients. Exclusion criteria were: 1) patients or family members unwilling to participate in the study, and 2) critically ill individuals (defined as those with severe physical or cognitive impairments preventing accurate questionnaire completion).
Questionnaire Development and Validation
A validated, structured questionnaire was used to assess knowledge, attitudes, and practices. The questionnaire was designed based on relevant references.13–16 After drafting the initial version, a small-scale pilot test was conducted with 30 participants, demonstrating good internal consistency (Cronbach’s α = 0.860). The final version of the questionnaire, written in Chinese, comprised four dimensions and a total of 52 items (Supplementary Figure 1). The KAP questionnaire was structured into four sections. Demographic data comprised 15 non-scored items. The knowledge dimension included 9 main items, with Item 5 subdivided into 3 sub-items and Item 8 into 5 sub-items, resulting in 15 scorable components. Responses were coded as 2 points for “Very familiar”, 1 point for “Have heard of”, and 0 points for “Unclear”, yielding a total score range of 0–30, categorized as insufficient (0–14), moderate (15–20), or adequate knowledge (21–30). The attitude dimension contained 9 items evaluated on a 5-point Likert scale. Items 1–4 and 7–9 were scored from “very positive” (5) to “very negative” (1), while Item 5 was reverse-scored (1–5). Total scores ranged from 9–45, classified as negative (9–22), neutral (23–31), or positive attitudes (32–45). The practice dimension included 9 items, with Item 9 as a non-scored multiple-choice question (recording participation only). Items 1–8 used a 5-point Likert scale (“always” = 5 to “never” = 1), producing a score range of 8–40, categorized as negative (8–20), moderate (21–28), or positive practice behaviors (29–40). Reverse scoring, and sub-item independence (knowledge Items 5 and 8) were rigorously validated to ensure scoring consistency.
Data Collection and Quality Control
Paper questionnaires were distributed to participants in both the outpatient and inpatient departments of the cardiology unit, as well as through WeChat groups for patients. In total, 500 questionnaires were distributed.
Three professionally trained research assistants were involved in administering the questionnaire. Participants were recruited from both inpatient and outpatient patients with CHF. Before completing the questionnaire, each question was thoroughly explained to the patients or their family members to ensure that responses were as standardized as possible. After the questionnaires were collected, they were preliminarily reviewed, and participants or their family members were re-contacted to complete the questionnaire again if any issues were identified.
Sample Size Calculation
Sample size was calculated using the formula for cross-sectional studies:17 α=0.05,  where
where  when α=0.05, the assumed degree of variability of p=0.5 maximizes the required sample size, and δ is admissible error (which was 5% here). The theoretical sample size was 480 which includes an extra 20% to allow for subjects lost during the study.
when α=0.05, the assumed degree of variability of p=0.5 maximizes the required sample size, and δ is admissible error (which was 5% here). The theoretical sample size was 480 which includes an extra 20% to allow for subjects lost during the study.
Statistical Analysis
Stata 17.0 (Stata Corporation, College Station, TX, USA) were used for statistical analysis. Descriptive analysis was conducted on the demographic data, CR status, and KAP (knowledge, attitude, and practice) scores of the respondents. Continuous variables following a normal distribution (KAP scores) are presented as mean ± standard deviation (SD). Categorical data expressed as n (%). Normally distributed data are presented as mean ± SD, and comparisons between two groups were performed using the t-test. Pearson correlation analysis was used to assess the correlation between the three dimensions (K, A, P). The Pearson’s correlation analysis was performed to explore the correlations among knowledge (K), attitude (A), practice (P). Structural equation modeling (SEM) was utilized to explore the path relationships and mediating effects between K, A, P, and demographic variables. A two-sided P-value of less than 0.05 was considered statistically significant.
Results
Questionnaire Quality
In the formal study, the internal consistency of the overall scale and each subscale was strong. The overall Cronbach’s α coefficient was 0.8962, while the values for the knowledge, attitude, and practice sections were 0.9326, 0.7020, and 0.7913, respectively.
Demographic Characteristics
Initially, 500 samples were collected. After excluding 8 samples due to missing or inconsistent data, 492 valid samples remained (98.4% valid rate). Among these, 277 (56.3%) were patients, 191 (38.8%) were aged 60 or older, 281 (57.1%) were male, 177 (36.0%) had been diagnosed with CHF for less than a year, 244 (49.6%) had experienced myocardial infarction or heart failure, and 77 (15.7%) had undergone CR. The mean knowledge, attitude, and practice scores were 6.90 ± 5.63 (possible range: 0–30), 33.43 ± 3.31 (possible range: 9–45), and 28.01 ± 4.46 (possible range: 8–40), respectively (Table S1). As shown in Table S1, the majority of participants scored high in attitude and practice but relatively low in knowledge. Knowledge scores varied significantly with factors such as family status (patient or family member) (p = 0.026), age (p < 0.001), education level (p < 0.001), employment status (p < 0.001), monthly income per capita (p < 0.001), family history of myocardial infarction or heart failure (p = 0.002), CR status (p < 0.001), and CR training (p < 0.001). Attitude scores also varied based on age (p = 0.033), education level (p = 0.003), monthly income per capita (p = 0.044), drinking habits (p = 0.024), medical or commercial insurance (p < 0.001), duration of CHF (p = 0.005), family history of myocardial infarction or heart failure (p < 0.001), and myocardial infarction or heart failure status (p = 0.001). Practice scores varied by age (p = 0.005), education level (p = 0.001), monthly income per capita (p = 0.010), medical or commercial insurance (p < 0.001), family history of myocardial infarction or heart failure (p < 0.001), myocardial infarction or heart failure status (p = 0.006), CR status (p = 0.001), and CR training (p = 0.006) (Table 1).
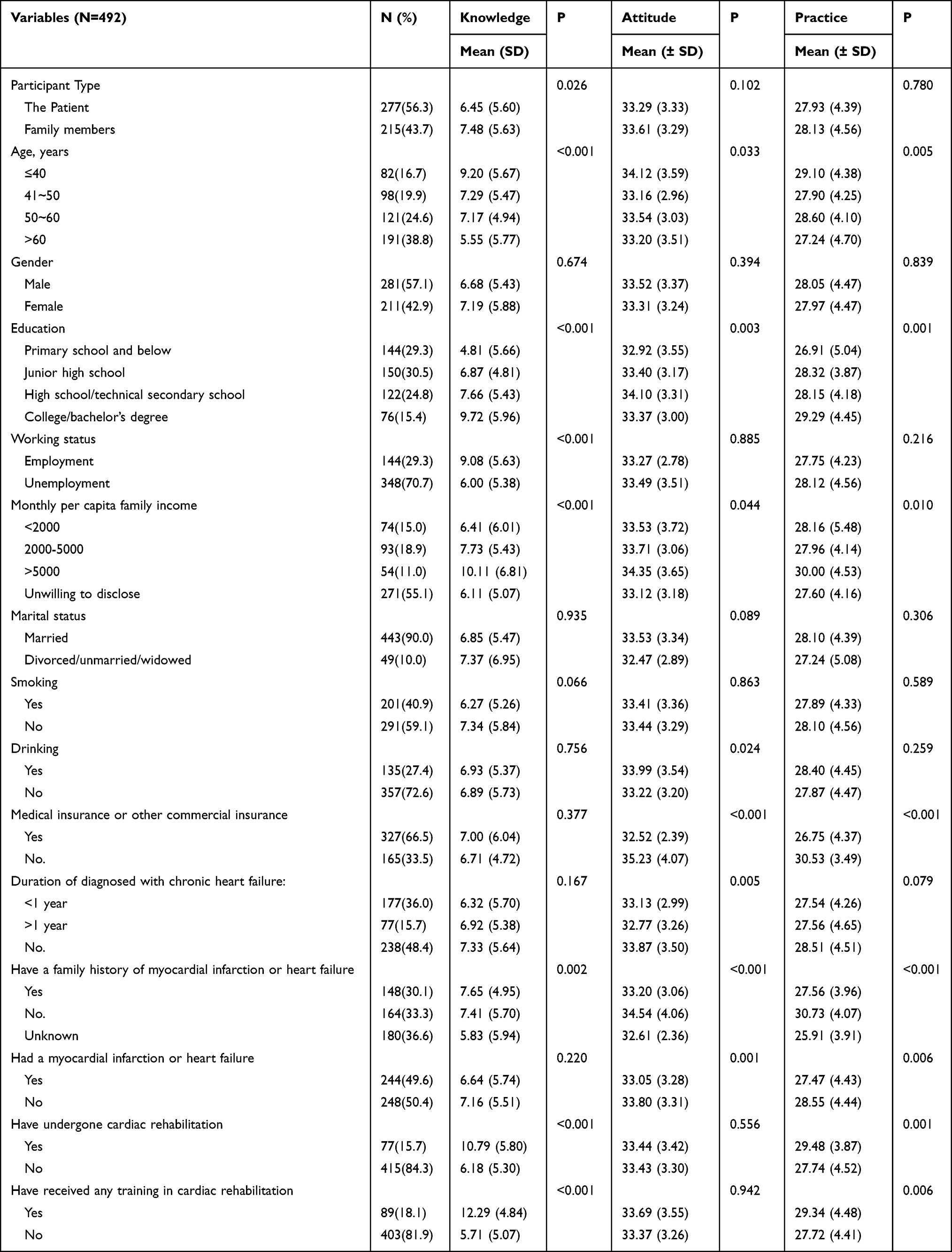 |
Table 1 Demographic Characteristics and KAP Scores |
Knowledge, Attitude, and Practice
Regarding knowledge, more than 63% of participants were unclear about the three items related to CR staging (K5.1-K5.3). Additionally, over 82.1% were unclear about certified CR centers (K8). Another item with a high rate of “Unclear” responses was “CR evaluation is a very important prerequisite for effective individualized treatment” (K6), with 50.6% of participants indicating uncertainty (Table 2). As shown in Table 2, lack of awareness about CR staging and CR centers was the most common knowledge gap.
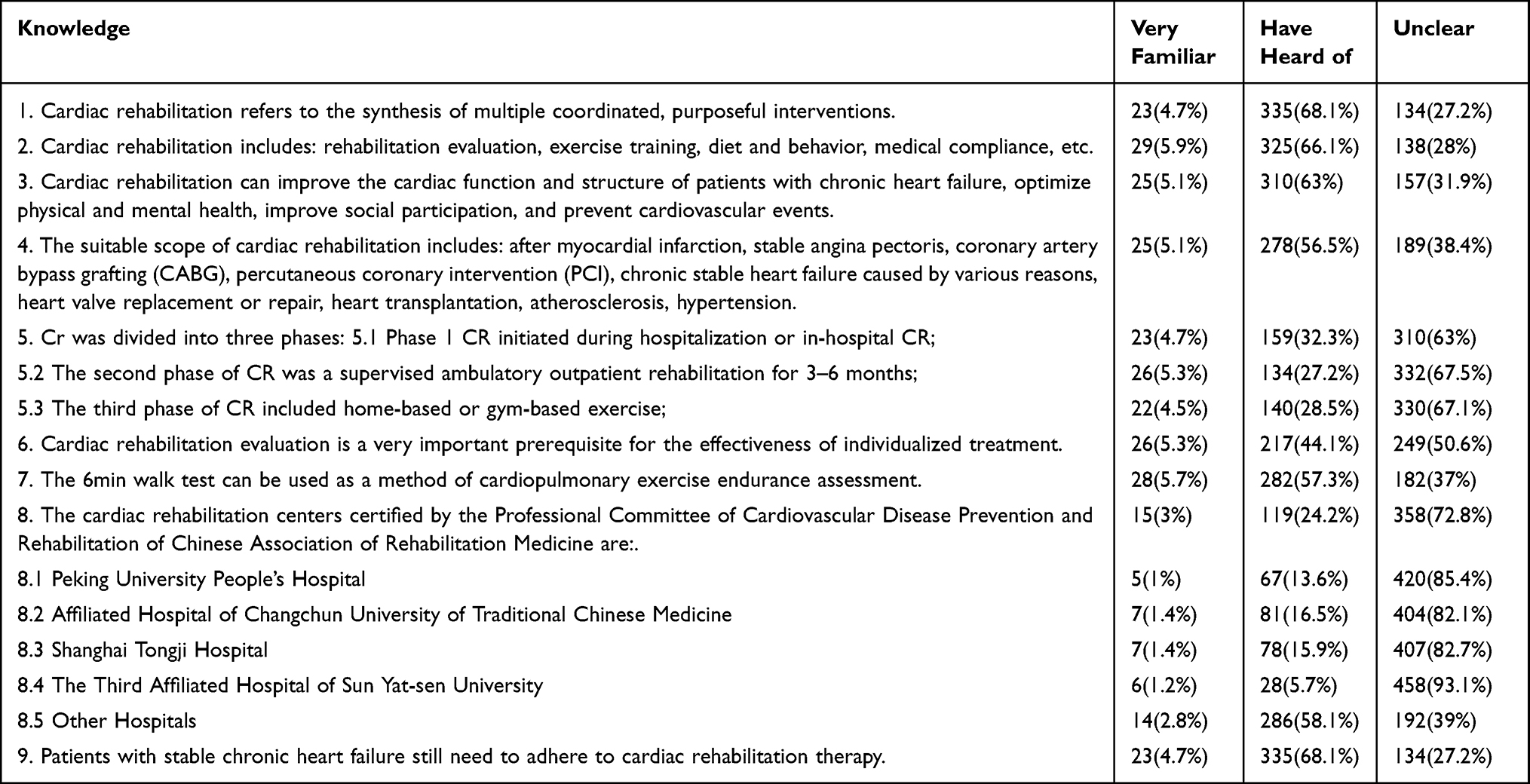 |
Table 2 Distribution of Knowledge Dimension Responses |
In terms of attitudes, 3% strongly agreed and 12.2% agreed that exercise training in CR was too strenuous for CHF patients and could potentially cause harm (A5). Conversely, 46.5% disagreed, and 4.5% strongly disagreed, that they were dissatisfied with the current CR resources and services available to them (A8) (Table 3). Table 3 illustrates that overall, participants maintained a positive attitude toward CR, despite concerns about exercise intensity.
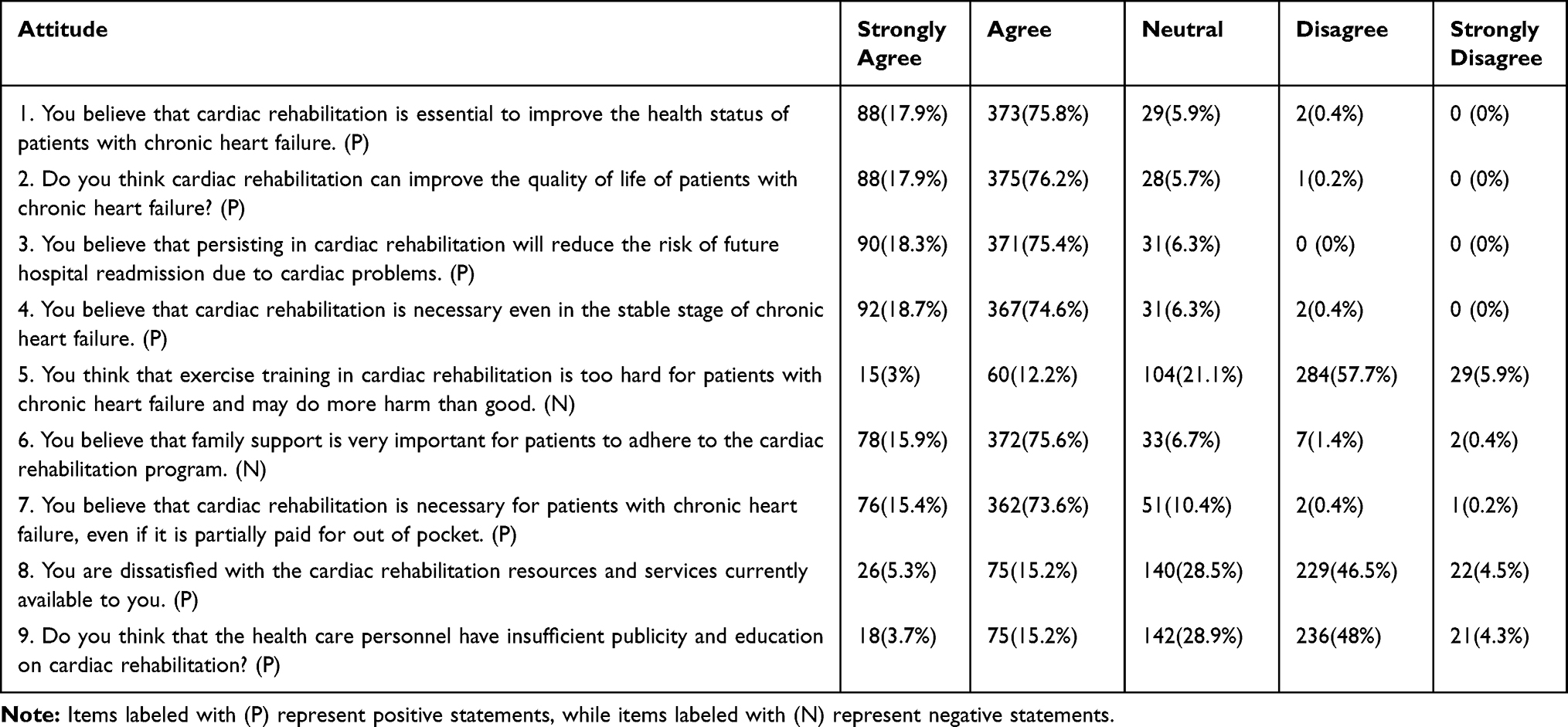 |
Table 3 Distribution of Attitude Dimension Responses |
For practices, 45.5% of participants reported that patients were not actively engaging in CR (P1), 36% did not seek out information on CR through various channels (P5), and 15.4% did not regularly communicate with the CR medical team to improve compliance (P6) (Table 4). As summarized in Table 4, active CR practice behaviors remained suboptimal among many participants.
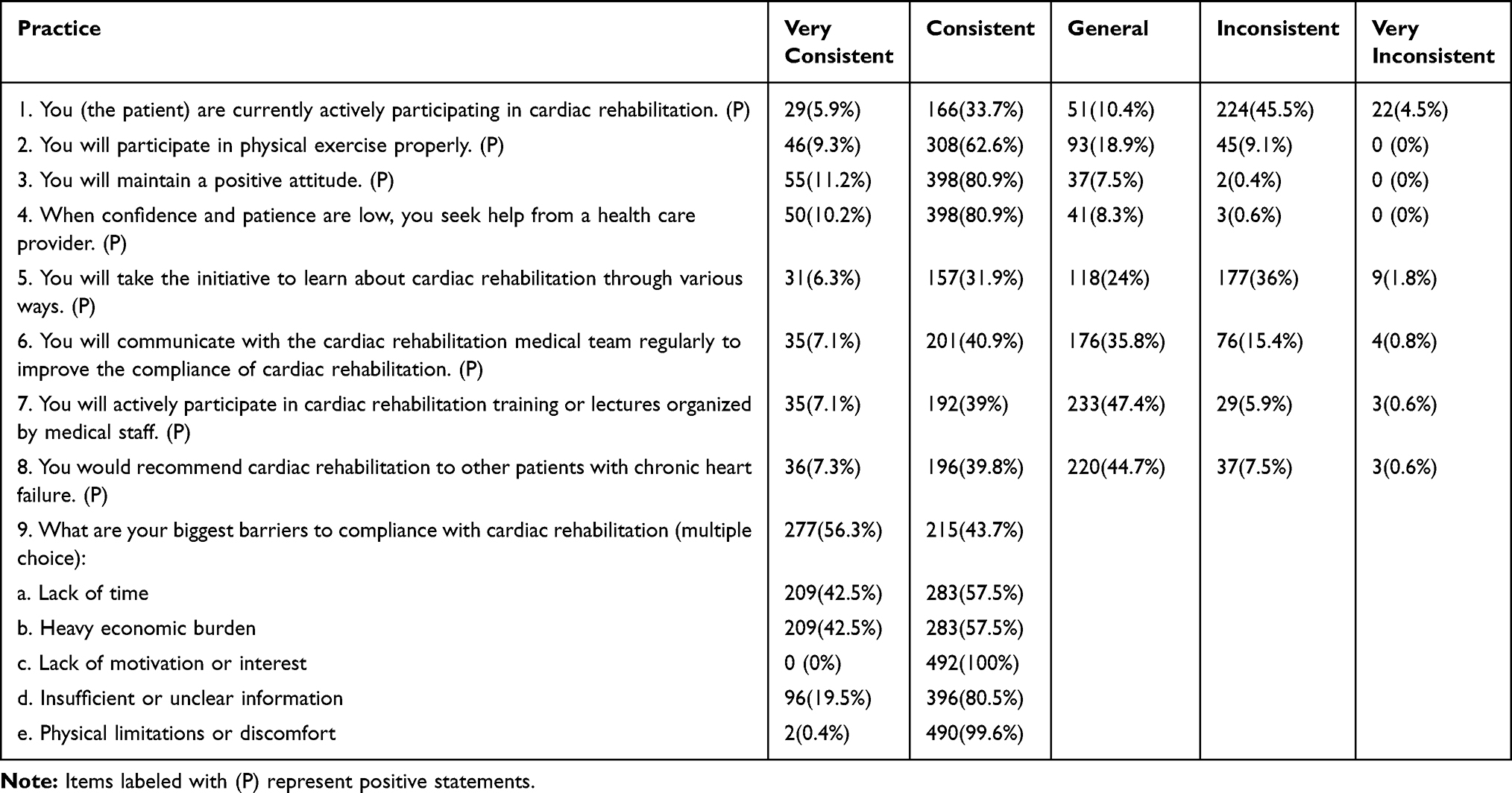 |
Table 4 Distribution of Practice Dimension Responses |
Correlations Between KAP
Correlation analysis revealed significant positive correlations between knowledge and attitude (r = 0.158, p < 0.001), as well as between knowledge and practice (r = 0.371, p < 0.001). A significant correlation was also observed between attitude and practice (r = 0.312, p < 0.001) (Tables S2 and S3). Tables S2 and S3 confirm that all three dimensions (K, A, P) were positively correlated.
Univariate and Multivariate Analysis
The median knowledge, attitude, and practice scores were used as cut-off points, dividing participants into groups. Above-median scores were observed in 51.42% for knowledge, 84.55% for attitude, and 53.25% for practice. Multivariate logistic regression analysis revealed that younger age (≤40 years, OR = 0.379, p = 0.012), higher education level (particularly college or bachelor’s degree, OR = 9.715, p < 0.001), awareness of family history (OR = 0.507, p = 0.030), participation in CR (OR = 0.371, p = 0.022), and receiving CR training (OR = 0.051, p < 0.001) were independently associated with higher knowledge scores. Concurrently, knowledge score (OR = 1.078, 95% CI: [1.016, 1.143], p = 0.013) was independently associated with a positive attitude. Moreover, knowledge score (OR = 1.114, 95% CI: [1.053, 1.179], p < 0.001), college or bachelor’s degree (OR = 3.089, 95% CI: [1.054, 9.053], p = 0.040), absence of medical or commercial insurance (OR = 6.762, 95% CI: [3.597, 12.713], p < 0.001), no family history of myocardial infarction or heart failure (OR = 4.414, 95% CI: [2.351, 8.288], p < 0.001), and non-participation in CR (OR = 0.206, 95% CI: [0.087, 0.489], p < 0.001) were independently associated with proactive practice (Tables 5 and 6). Tables 5 and 6 highlight the key predictors of higher KAP scores identified in regression analyses.
 |
Table 5 Cut-off Value and Grouping |
 |
Table 6 Univariate and Multivariate Analysis for Knowledge, Attitude and Practice |
Interactions Between KAP
SEM showed acceptable model fit indices (RMSEA = 0.079, SRMR = 0.092, TLI = 0.888, and CFI = 0.899) (Table 7). Mediation analysis demonstrated that knowledge directly influenced attitude (β = 0.321, p < 0.001) and practice (β = 0.285, p = 0.004). Attitude directly influenced practice (β = 0.217, p < 0.001), and knowledge indirectly affected practice through attitude (β = 0.355, p < 0.001) (Table 8). Detailed path coefficients are illustrated in Figure 1. As shown in Table 8 and Figure 1, SEM confirmed both direct and indirect effects among knowledge, attitude, and practice.
 |
Table 7 Index of Fit |
 |
Table 8 Analysis of Mediation |
 |
Figure 1 SEM Model. |
Discussion
Our findings highlight the persistent gap between CR knowledge and practice in CHF populations. Individuals with CHF and caregivers demonstrated inadequate knowledge, yet exhibited positive attitudes and proactive practices toward CR. These findings reveal a notable gap between knowledge and the application of attitudes in practice, underscoring the necessity of targeted educational interventions to address knowledge deficits, thereby potentially enhancing patient engagement in CR programs. This gap is consistent with findings from previous studies. For example, while physiotherapists generally understand CR well, their attitudes and practices in following exercise programs are often influenced by factors related to both clinicians and patients.18 This suggests that even with knowledge, other obstacles can impact how well rehabilitation is carried out. Practical barriers, such as absence of medical insurance coverage, also play a major role in limiting participation in CR.19 These logistical issues can further complicate the ability for patients to turn their positive attitudes and intentions into actual participation in rehabilitation programs. Additionally, patients and caregivers tend to share similar levels of understanding and beliefs about CR. Research shows that focusing on both patients and their caregivers early in the rehabilitation process, especially on their specific beliefs and understanding about the disease, can help improve outcomes for patients and caregivers alike.20
The interrelationships among KAP dimensions further support the importance of knowledge as the foundation of CR engagement. Regarding the relationships between KAP dimensions, the significant correlations between knowledge, attitude, and practice, supported by both correlation analyses and SEM, align with existing literature. The SEM indicate that knowledge directly influences attitude and practice, with attitude mediating the indirect effect of knowledge on practice. This is consistent with the theory that improved knowledge can shape more positive attitudes, which in turn lead to better health practices.21,22 These findings emphasize the critical role of knowledge as a foundational element in enhancing attitudes and practices related to CR. Previous studies have similarly found that interventions targeting knowledge improvements can lead to substantial changes in health behaviors and attitudes.23,24
Sociodemographic differences significantly shape CR-related KAP. The significant differences in KAP scores across various demographic variables, as identified in both univariate and multivariate analyses, provide further insight. Younger participants and those with higher educational attainment had significantly better knowledge and practice scores, consistent with earlier research indicating higher health literacy among these groups.25,26 Interestingly, education level was a consistent predictor across all dimensions of KAP, indicating that knowledge, attitude, and practice are heavily influenced by formal education. However, in some cases, such as income, differences were only significant for practice but not for knowledge or attitude, suggesting that financial resources might directly influence the ability to engage in rehabilitation activities but not necessarily affect perceptions or understanding.
Specific knowledge gaps persist in key areas of CR. In terms of knowledge responses, a large proportion of participants were unclear about key aspects of CR, such as its staging and the role of certified centers. This reflects findings from similar studies, which have also reported poor awareness of rehabilitation programs among patients with CHF.27 Thus, targeted educational initiatives addressing the significance of CR staging, evaluations, and certified centers are recommended. These interventions could be effectively integrated within clinical practices and community-based programs.28,29
Attitudes toward CR are generally positive, but misconceptions and dissatisfaction remain. For the attitude dimension, while participants generally expressed positive views towards CR, some misconceptions persisted. For example, a small percentage believed that CR exercises could be harmful, which may reflect fear or misunderstanding about the intensity and benefits of such programs. Healthcare professionals should emphasize individualized rehabilitation planning and clearly communicate exercise safety to alleviate patients’ concerns. Additionally, dissatisfaction with available rehabilitation resources and services points to an area for improvement. Expanding access to CR programs, possibly through telehealth options or more local centers, could alleviate this dissatisfaction.30,31
Practice behaviors reveal inadequate engagement despite positive attitudes. The practice dimension revealed that while many participants reported consistency in engaging in CR, a notable proportion reported inadequate engagement and communication with the rehabilitation team. Given that these activities are crucial for the success of CR, specific strategies should be developed to increase patient engagement. Implementing structured follow-up procedures, personalized goal-setting, and reducing economic barriers via insurance or financial support are potential strategies for enhancing patient adherence to CR.32,33
Limitations
This study has several limitations. First, as a cross-sectional survey, it only captures a snapshot of knowledge, attitudes, and practices at a single point in time, limiting our ability to assess changes over time. Second, single-center data collection may limit the generalizability of the findings. Third, self-reported data on KAP may be subject to response bias.
Conclusions
In conclusion, individuals with CHF and caregivers demonstrated inadequate knowledge, yet generally positive attitudes and proactive practices toward CR. These findings highlight the need for targeted educational interventions to address knowledge deficits and structured support strategies to enhance patient engagement to enhance participation in CR programs.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee Heping Hospital Affiliated to Changzhi Medical College (2024) 089. All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Acknowledgments
Project name: Hospital-level project of Heping Hospital Affiliated to Changzhi Medical College: Guiding value of NT-proBNP combined with USCOM in the clinical treatment of patients with ischemic cardiomyopathy and heart failure (No.: NPYJ202224).
Author Contributions
Xiaohua Gao and Jianzhou Yang carried out the studies, participated in collecting data, and drafted the manuscript. Xiaohua Gao and Jianzhou Yang performed the statistical analysis and participated in its design. Wenjun Cao, Yaoqiang Liu and Tingting Zhao participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript. All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Fundamental Research Program of Shanxi Province under Grant “Dynamic Early Warning Study of Coronary Heart Disease Prognostic Risk Based on Polygenic Risk Scores and Bayesian Multivariate Joint Models”, (202403021221210); the Changzhi City Basic Research Program under Grant “Prediction Model for Readmission Risk of Urban Elderly Heart Failure Patients Based on Multi-dimensional Data Integration and Machine Learning”, (JC202415). Youth Start-up Fund Heping Hospital Affiliated to Changzhi Medical College “The guiding value of NT-proBNP combined with USCOM in the clinical treatment of heart failure patients with ischemic cardiomyopathy” (HPYJ202224).
Disclosure
Xiaohua Gao and Jianzhou Yang are co-first authors for this study. The authors declare that they have no competing interests in this work.
References
1. Mascolo A, Di Mauro G, Cappetta D, et al. Current and future therapeutic perspective in chronic heart failure. Pharmacol Res. 2022;175:106035. doi:10.1016/j.phrs.2021.106035
2. Dellafiore F, Chung ML, Alvaro R, Zeffiro V, Ercole V, Pucciarelli G. Influence of mutuality on quality of life in heart failure patient with inadequate self-care and caregiver dyads: an actor-partner interdependence model analysis. Eur J Cardiovasc Nurs. 2022;21(4):366–373. doi:10.1093/eurjcn/zvab089
3. Wang GG, Wang SJ, Qin J, et al. Characteristics, management, and outcomes of acute heart failure in the emergency department: a multicenter registry study with 1-year follow-up in a Chinese Cohort in Beijing. Chin Med J. 2017;130(16):1894–1901. doi:10.4103/0366-6999.211880
4. Achttien RJ, Staal JB, van der Voort S, et al. Exercise-based cardiac rehabilitation in patients with chronic heart failure: a Dutch practice guideline. Neth Heart J. 2015;23(1):6–17. doi:10.1007/s12471-014-0612-2
5. Kim C, Sung J, Lee JH, et al. Clinical practice guideline for cardiac rehabilitation in Korea. Korean J Thorac Cardiovasc Surg. 2019;52(4):248–285. doi:10.5090/kjtcs.2019.52.4.248
6. Moghei M, Pesah E, Turk-Adawi K, et al. Funding sources and costs to deliver cardiac rehabilitation around the globe: drivers and barriers. Int J Cardiol. 2019;276:278–286. doi:10.1016/j.ijcard.2018.10.089
7. Beatty AL, Truong M, Schopfer DW, Shen H, Bachmann JM, Whooley MA. Geographic variation in cardiac rehabilitation participation in medicare and veterans affairs populations: opportunity for improvement. Circulation. 2018;137(18):1899–1908. doi:10.1161/circulationaha.117.029471
8. Kulju E, Jarva E, Oikarinen A, Hammarén M, Kanste O, Mikkonen K. Educational interventions and their effects on healthcare professionals’ digital competence development: a systematic review. Int J Med Inform. 2024;185:105396. doi:10.1016/j.ijmedinf.2024.105396
9. Williamson TM, Rouleau CR, Aggarwal SG, Arena R, Hauer T, Campbell TS. The impact of patient education on knowledge, attitudes, and cardiac rehabilitation attendance among patients with coronary artery disease. Patient Educ Couns. 2021;104(12):2969–2978. doi:10.1016/j.pec.2021.04.024
10. Tan J, Luo L, Zhang M, et al. A Chinese and Western medication adherence scale in patients with chronic kidney disease. Patient Prefer Adherence. 2019;13:1487–1495. doi:10.2147/ppa.S207693
11. Li L, Zhang J, Qiao Q, Wu L, Chen L. Development, reliability, and validity of the “knowledge-attitude-practice” questionnaire of foreigners on traditional Chinese medicine treatment. Evid Based Complement Alternat Med. 2020;2020:8527320. doi:10.1155/2020/8527320
12. Khalid A, Haque S, Alvi S, et al. Promoting health literacy about cancer screening among Muslim immigrants in Canada: perspectives of imams on the role they can play in community. J Prim Care Community Health. 2022;13:21501319211063051. doi:10.1177/21501319211063051
13. Chinese Medical Association OaBMDBPODaTG.
14. Wang Lemin SYDDoCRfCHFCECCCSoRM, cardiovascular disease professional committee re-election and academic development summit forum conference materials. 2012.
15. Keteyian SJ, Brawner CA. Chronic heart failure and cardiac rehabilitation. Chin J Geriatric Care Med. 2015;(1):94–96. doi:10.3969/j.issn.1672-4860.2015.01.041
16. Yang X, Li X. 心力衰竭与心脏康复运动 [Heart failure and cardiac rehabilitation exercise]. Chinese Journal of Clinical Physicians. 2018;46(5):3 (505–507). Chinese doi:10.3969/j.issn.2095-8552.2018.05.001
17. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychologic Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
18. Gondekar A, Singh VP, Rajan Samuel S, Raghavan H, Khandelwal B, Knowledge KKV. Attitude, and practice of physiotherapists about cardiac rehabilitation program adherence among patients discharged from the hospital after cardiac surgery in India. ScientificWorldJournal. 2024;2024:8825476. doi:10.1155/2024/8825476
19. Bakhshayeh S, Sarbaz M, Kimiafar K, Vakilian F, Eslami S. Barriers to participation in center-based cardiac rehabilitation programs and patients’ attitude toward home-based cardiac rehabilitation programs. Physiother Theory Pract. 2021;37(1):158–168. doi:10.1080/09593985.2019.1620388
20. Thomson P, Angus NJ, Andreis F, et al. Longitudinal evaluation of the effects of illness perceptions and beliefs about cardiac rehabilitation on quality of life of patients with coronary artery disease and their caregivers. Health Qual Life Outcomes. 2020;18(1):158. doi:10.1186/s12955-020-01405-0
21. Deveci S, Cevik C, Baydur H, Onsuz F, Tosun S, Ergor A. Validity and reliability of the COVID-19 knowledge, attitude and behavior scale. Vaccines. 2023;11(2). doi:10.3390/vaccines11020317
22. Nascimento LGP, da Silva AMC, Stedefeldt E, da Cunha DT. Job crafting and burnout as predictors of food safety behaviors in the foodservice industry. Foods. 2022;11(17):2671. doi:10.3390/foods11172671
23. Bazezew AM, Nuru N, Demssie TG, Ayele DG. Knowledge, practice, and associated factors of preoperative patient teaching among surgical unit nurses, at Northwest Amhara comprehensive specialized referral Hospitals, Northwest Ethiopia, 2022. BMC Nurs. 2023;22(1):20. doi:10.1186/s12912-023-01175-2
24. Cheewakriangkrai C, Kietpeerakool C, Charoenkwan K, et al. Health education interventions to promote early presentation and referral for women with symptoms of endometrial cancer. Cochrane Database Syst Rev. 2020;3(3):Cd013253. doi:10.1002/14651858.CD013253.pub2
25. Agner J, Meyer M, Kaukau TM, et al. Health literacy, social networks, and health outcomes among mental health clubhouse members in Hawaii. Int J Environ Res Public Health. 2023;20(1):837. doi:10.3390/ijerph20010837
26. Böhm AK, Jensen ML, Sørensen MR, Stargardt T. Real-world evidence of user engagement with mobile health for diabetes management: longitudinal observational study. JMIR Mhealth Uhealth. 2020;8(11):e22212. doi:10.2196/22212
27. Liu X, Liu L, Li Y, Cao X. The association between physical symptoms and self-care behaviours in heart failure patients with inadequate self-care behaviours: a cross-sectional study. BMC Cardiovasc Disord. 2023;23(1):205. doi:10.1186/s12872-023-03247-2
28. Son YJ, Choi J, Lee HJ. Effectiveness of nurse-led heart failure self-care education on health outcomes of heart failure patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(18). doi:10.3390/ijerph17186559
29. Alvarez P, Sianis A, Brown J, Ali A, Briasoulis A. Chronic disease management in heart failure: focus on telemedicine and remote monitoring. Rev Cardiovasc Med. 2021;22(2):403–413. doi:10.31083/j.rcm2202046
30. Świątoniowska-Lonc NA, Sławuta A, Dudek K, Jankowska K, Jankowska-Polańska BK. The impact of health education on treatment outcomes in heart failure patients. Adv Clin Exp Med. 2020;29(4):481–492. doi:10.17219/acem/115079
31. Awoke MS, Baptiste DL, Davidson P, Roberts A, Dennison-Himmelfarb C. A quasi-experimental study examining a nurse-led education program to improve knowledge, self-care, and reduce readmission for individuals with heart failure. Contemp Nurse. 2019;55(1):15–26. doi:10.1080/10376178.2019.1568198
32. Rea F, Iorio A, Barbati G, et al. Patient adherence to drug treatment in a community based-sample of patients with chronic heart failure. Int J Cardiol. 2022;349:144–149. doi:10.1016/j.ijcard.2021.11.018
33. Ling RZQ, Jiao N, Hassan NB, He H, Wang W. Adherence to diet and medication and the associated factors among patient with chronic heart failure in a multi-ethnic society. Heart Lung. 2020;49(2):144–150. doi:10.1016/j.hrtlng.2019.11.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.