Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 15
Knowledge, Attitudes and Practices of Pharmacogenomics Among Senior Pharmacy Students: A Cross Sectional Study from Punjab, Pakistan
Authors Shah S ![]() , Hanif M, Khan HU, Khan FU
, Hanif M, Khan HU, Khan FU ![]() , Abbas G
, Abbas G ![]() , Khurram H
, Khurram H ![]() , Khames A, Abdelgawad MA, Said AS
, Khames A, Abdelgawad MA, Said AS ![]() , Abourehab MAS
, Abourehab MAS ![]() , Maheen S, Chand UR, Haris M
, Maheen S, Chand UR, Haris M
Received 1 February 2022
Accepted for publication 11 April 2022
Published 25 April 2022 Volume 2022:15 Pages 429—439
DOI https://doi.org/10.2147/PGPM.S359920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Shahid Shah,1 Muhammad Hanif,2 Hafeez Ullah Khan,3 Faiz Ullah Khan,4 Ghulam Abbas,5 Haris Khurram,6 Ahmed Khames,7 Mohamed A Abdelgawad,8 Amira SA Said,9,10 Mohammed AS Abourehab,11 Safirah Maheen,3 Usman Rashid Chand,1 Muhammad Haris1
1Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Government College University Faisalabad, Faisalabad, Pakistan; 2Department of Pharmaceutics, Faculty of Pharmacy, Bahauddin Zakariya University Multan, Multan, Pakistan; 3College of Pharmacy, Department of Pharmaceutics, University of Sargodha, Sargodha, Pakistan; 4Department of Pharmacy Administration and Clinical Pharmacy, School of Pharmacy, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 5Department of Pharmaceutics, Faculty of Pharmaceutical Sciences, Government College University Faisalabad, Faisalabad, Pakistan; 6National University of Computer and Emerging Sciences, Chiniot-Faisalabad Campus, Chiniot, Pakistan; 7Department of Pharmaceutics and Industrial Pharmacy, College of Pharmacy, Taif University, Taif, 21944, Saudi Arabia; 8Department of Pharmaceutical Chemistry, College of Pharmacy, Jouf University, Sakaka, Al Jouf, 72341, Saudi Arabia; 9Clinical Pharmacy Department, Faculty of Pharmacy, Beni-Suef, Egypt; 10Clinical Pharmacy Department, College of Pharmacy, Al Ain University, Al Ain, Abu Dhabi, United Arab Emirates; 11Department of Pharmaceutics, Faculty of Pharmacy, Umm Al-Qura University, Makkah, 21955, Saudi Arabia
Correspondence: Shahid Shah; Ghulam Abbas, Email [email protected]; [email protected]
Background: Pharmacogenomics (PGx) is essential for optimizing drug therapy and reducing unwanted drug side effects. Our aim was to determine the knowledge, attitude and practice of senior pharmacy students in Punjab, Pakistan towards PGx.
Methods: A cross-sectional study was conducted among 511 undergraduate pharmacy students from different universities in Punjab, Pakistan. A validated and pilot-tested structured questionnaire was administered to respondents to assess their knowledge, attitude, and practice regarding PGx. Descriptive statistics and multivariate logistic regression model were used to describe the results of the study. A p-value of less than 0.05 was considered statistically significant.
Results: A total of 511 students (58.9% females and 41.1% males) responded to the survey. Most (87.7%) of the students knew that the drug response could be affected by genetic variations. Mean knowledge score of the students was 12.6. Good basic knowledge positively and significantly (p=0.01) affected students’ PGx test knowledge and attitudes. Most (> 70%) of students believed that human genetics affected the drug response due to interindividual variation and ethnic variation. Mean attitude score of the students was 5.23. The majority of students (> 92%) wanted to learn more about PGx and thought it could help them choose the right drug. Students’ knowledge was positively and significantly (p=0.01) affected by a good attitude. Mean practice score of the students was 11.95. When trying to solve a drug-related case study question, about 31.5% of students implemented the idea of human genetic variation. Only 28.8% of students attended a lecture related to the effects of genetic variations on drug therapy. Good practice positively and significantly (p=0.01) affected students’ knowledge of PGx tests.
Conclusion: The senior pharmacy students had good knowledge and attitudes towards PGx. However, the practice of PGx needs to be improved to facilitate the application of PGx in clinical practice in Pakistan.
Keywords: pharmacogenomics, knowledge, attitude, practice
Introduction
Pharmacogenomics (PGx) is the combination of pharmacology and genomics to observe the impact of genetic variations on drug response.1 Pharmacogenetics and pharmacogenomics are the keys to the success of personalized medicine, prescribing drugs based on the individual genetic and biological profile of the patient. However, pharmacogenomics differs from pharmacogenetics in that it deals with the response to drugs due to the influence of all genes (the genome) instead of a single gene. Drug-drug interactions and interactions between drug and molecular targets are largely affected by these genetic variants. This in turn influences the drug efficacy and avoids unwanted side effects. PGx helps to maintain the right dose for the right person thus minimizing interindividual fluctuations in drug response.2 For example, it is recommended to decrease the dose of warfarin in patients with genetic variants.3,4 For the guidance of clinicians in making pharmacotherapeutic decisions, a database (The Clinical PGx Implementation Consortium (CPIC) supported by the Pharmacogenomics Knowledge Base) has been developed. The United States Food and Drug Administration (FDA) has also proven the significance of PGx in the labeling of many other drugs.5 Despite the importance of PGx, it is not generally practiced in pharmacotherapy by the healthcare professionals, including pharmacists.6 In developed countries such as the United States, various pharmacy training programs have included PGx in their programs to improve the practice of these healthcare professionals.7 These programs significantly improved the pharmaco-therapeutic outcomes of these developed countries.8 This practice is quite less in developing countries like Pakistan. There is regional genetic variation in drug response in African, European and Asian countries as evidenced by different studies,9,10 but due to the lack of PGx practice in the developing countries, these variations are not studied leading to variations in the drug response. Assessment of current knowledge, attitudes and practices of PGx is critical to increase the awareness and implementation of PGx in clinical practice.
To the best of our knowledge, there is no PGx study conducted in Pakistan among senior pharmacists. Our aim was to determine the knowledge, attitude and practice of senior pharmacists towards PGx in Punjab, Pakistan.
Methodology
Study Design and Sample
A questionnaire-based cross-sectional study was conducted by administering the questionnaire to the pharmacy students from 6 public universities in Punjab, Pakistan, including Government College University Faisalabad, University of Agriculture Faisalabad, University of Faisalabad, University of Sargodha, Bahauddin Zakariya University Multan and University of Central Punjab. Before the study began, the Government College University Faisalabad Institutional Review Board issued permission to conduct the study, including verbal consent. Since the study did not require any clinical intervention and the participants’ involvement in the study was clearly below minimal risk, all participants gave informed verbal consent rather than written consent.
Questionnaire Development
The questionnaire was developed after literature review to identify existing instruments.11 The initial draft of the questionnaire covered demographics, educational exposure to PGx, knowledge of PGx, knowledge of FDA recommendations about PGx testing of drugs, attitudes towards PGx and the practice of PGx testing.
Validation of the Questionnaire
The survey instrument was reviewed by the investigators for content, clarity, relevance, and ease of understanding of the questions. The researchers’ views and comments were taken into consideration. Each item on the questionnaire was also linked to the objectives of the study. Thus, it shows the validity of the content. A pilot test of the questionnaire was conducted among a target sample to determine its suitability. Responses of these respondents were not used in the final analysis. Cronbach’s alpha was used to estimate the reliability of the items. The Cronbach’s alpha was 0.78 for knowledge, 0.69 for attitude and 0.71 for practice indicating good internal consistency.
Data Collection
The questionnaire prepared in the Google form was distributed through a link and in hard copies. The purpose of the study was also explained to them and an informed consent was taken describing the purpose of study. Participants were told that they could withdraw from the study if they wanted. The survey response rate was 78%. Incomplete or duplicate responses were excluded.
Measures
Dependent Variables
Dependent variables were educational exposure to PGx, students’ knowledge of PGx, knowledge of FDA recommendations on PGx testing of drugs, attitudes towards PGx and practice of PGx testing. Educational exposure to PGx was assessed using 5 questions. Students’ knowledge of PGX was determined using 10 questions. Each question had to be answered with “I know” (1 score), “I don’t know” (2 score) and “I am not sure” (3 score). A knowledge score of less than 14 was considered good knowledge. Knowledge of FDA recommendations on PGx testing of drugs was assessed using 6 questions about the labeling of different drugs as evidenced by the FDA. Students’ attitudes were assessed using 4 questions each of which was answered with “yes” (1 score), “I am not sure” (2 score) and “no” (3 score). An attitude score of less than 6 was considered a good attitude. The last section was about student practices towards PGx. This section included 5 questions each to be answered with “always”, “at least once in a month”, “at least once in a year or semester”, “at least once in a program” or “never”. A practice score in the range 5–8 was considered good practice.
Independent Variables
Independent variables consisted of student demographics, including age, gender and study institution.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences (IBM SPSS Statistics for Windows, version 21.0, Armonk, NY: IBM Corp.). Demographic variables were described by frequency percentages. Mean and standard deviation were calculated for describe the variables. Coefficient of correlation was measured to access the relation between KAP variables. Multivariate logistic regression was used to explore the impact of variable on good KAP. A p-value of less than 0.05 was considered statistically significant.
Results
Demographics
A total of 511 students (58.9% females and 41.1% males) completed the survey. Most of the students (61.6%) were of age 20–25 years. Students from different universities included 14.28% from Government College University Faisalabad, 13.69% from University of Agriculture Faisalabad, 11.15% from University of Faisalabad, 18.19% from University of Sargodha, 24.07% from Bahauddin Zakariya University Multan and 18.59% from University of Central Punjab. Table 1 represents the demographic characteristics of the students.
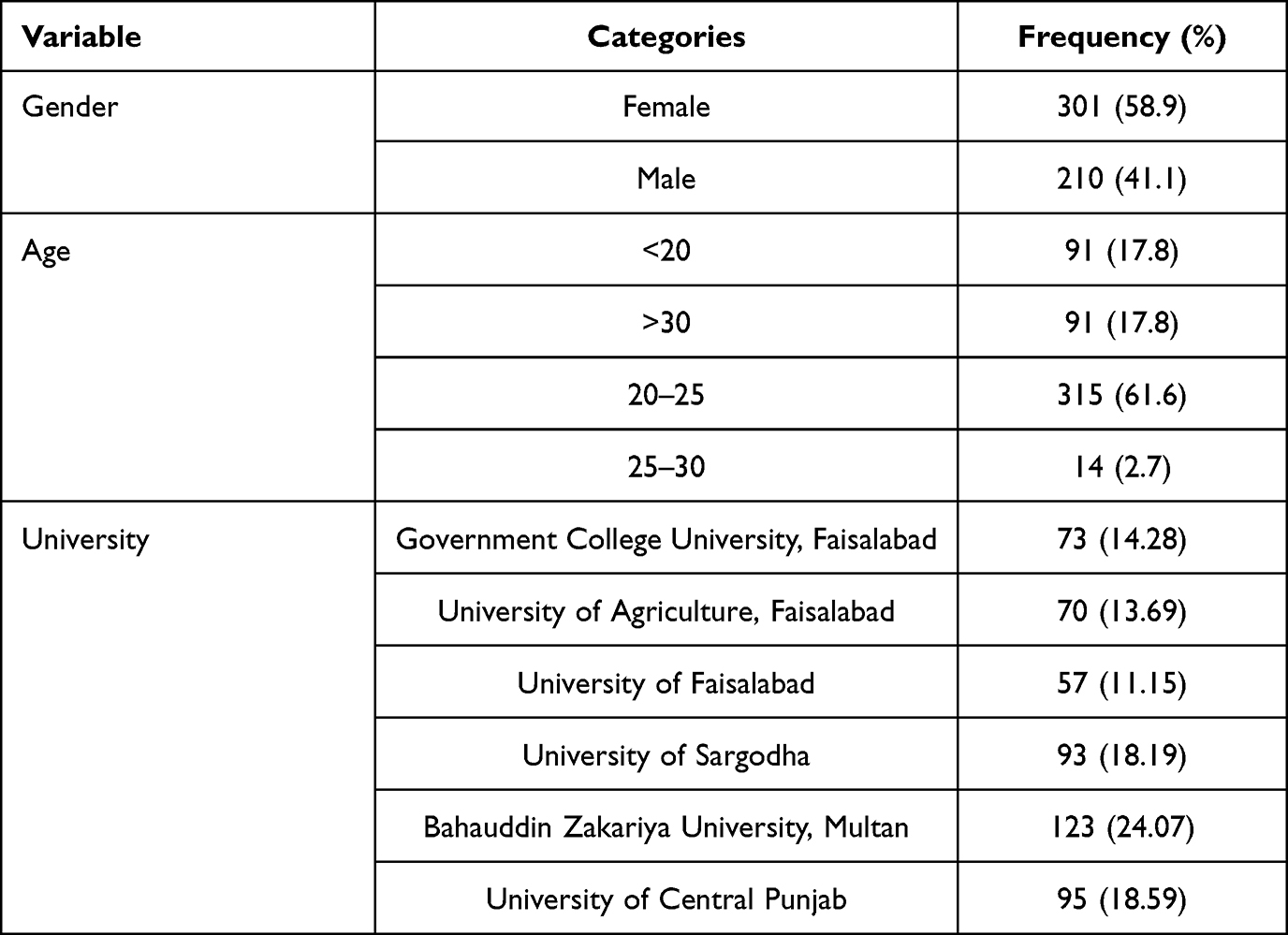 |
Table 1 Demographic Characteristic of the Students |
Educational Exposure to PGx
Most of the students (93.2%) had studied about interethnic and interindividual variations in drug response. University lectures (76.7%) were the major source of students’ knowledge about PGx. Approximately 42% of students stated that 3–5 lectures from various courses discussed the role of genetic variations in drug response. More than half of the students stated that they were able to understand the impact of genetic variations on drug response after taking pharmacy courses. 60% of the students agreed that the lectures they received clearly described the impacts of genetic variants on drug response. Table 2 represents the educational exposure of students to Pg.
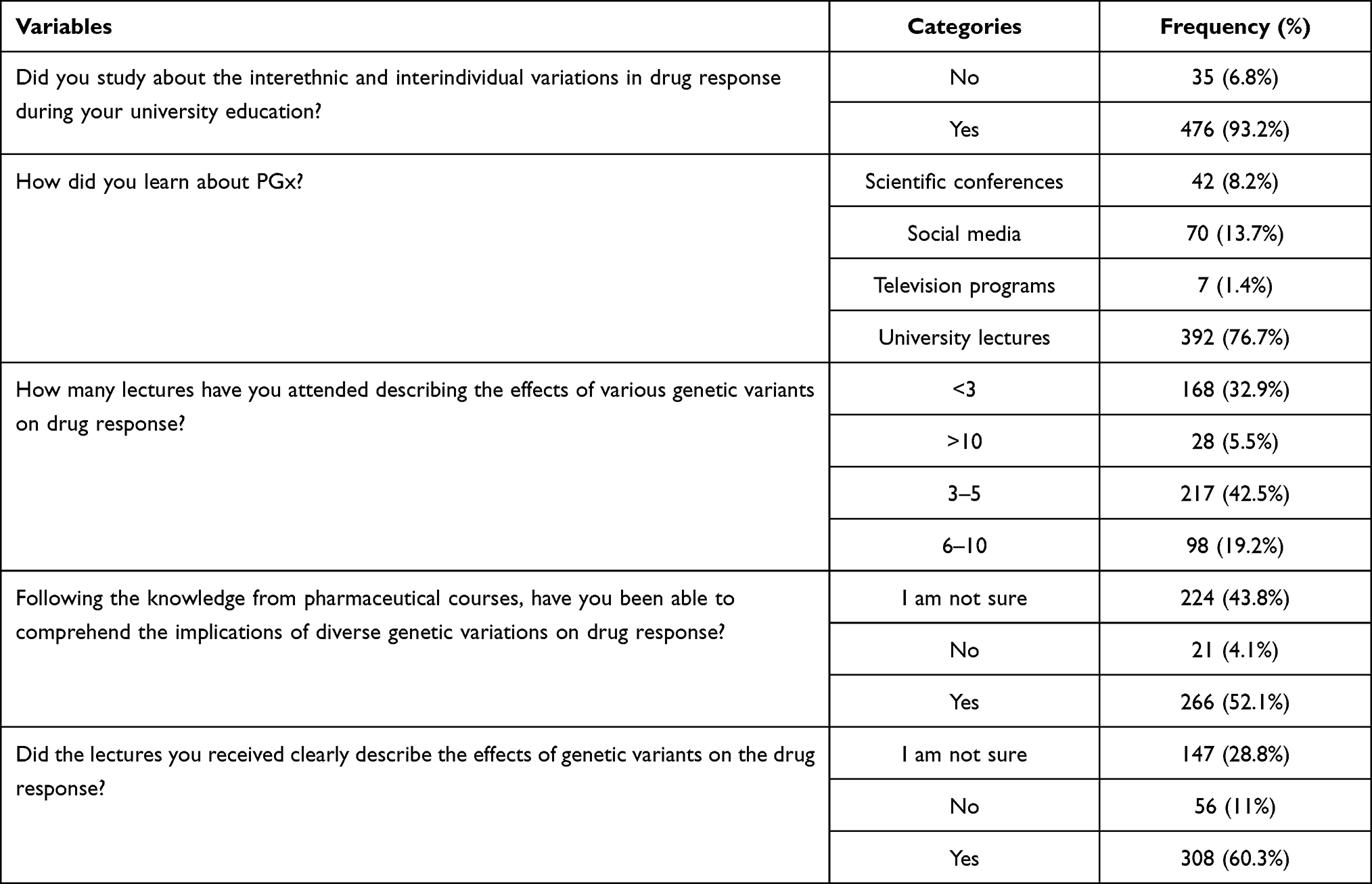 |
Table 2 Educational Exposure of Students to PGx |
Basic Knowledge of PGx
The mean knowledge score of the students was 12.6 and considered good. Most of the students knew that the drug response might be influenced by inherited genetic variants (87.7%) and that these variants could also lead to interindividual variation in drug response and could cause toxicity (80.8%). More than three quarters of the students knew that there was an interethnic variation in drug response, genetic changes could cause adverse reactions, interindividual variations in pharmacodynamics, and drug interaction with molecular targets could be due to genetic variations (76.7%). Most students were also aware that genetic variations might cause interindividual variation in pharmacokinetic parameters (75.3%), inherited genetic variants caused a high risk of drug toxicity (72.6%) and lack of response to drugs (74%) in some patients. About 69% of the students were aware that genetic biomarkers could be used to predict the drug response. Table 3 represents the knowledge of the students about PGx. Multivariate logistic regression showed that females were 2 times more likely to have good knowledge (C.I. = 1.34–3.148) compared to males. Scatterplot matrix and linear regression model also showed that females had higher knowledge than males, as represented in Figures 1 and 2 respectively. Students aged 20 to 25 years also had a higher knowledge score as compared to other age groups. Good knowledge positively and significantly (p=0.01) affected the knowledge of PGx testing and students’ attitudes.
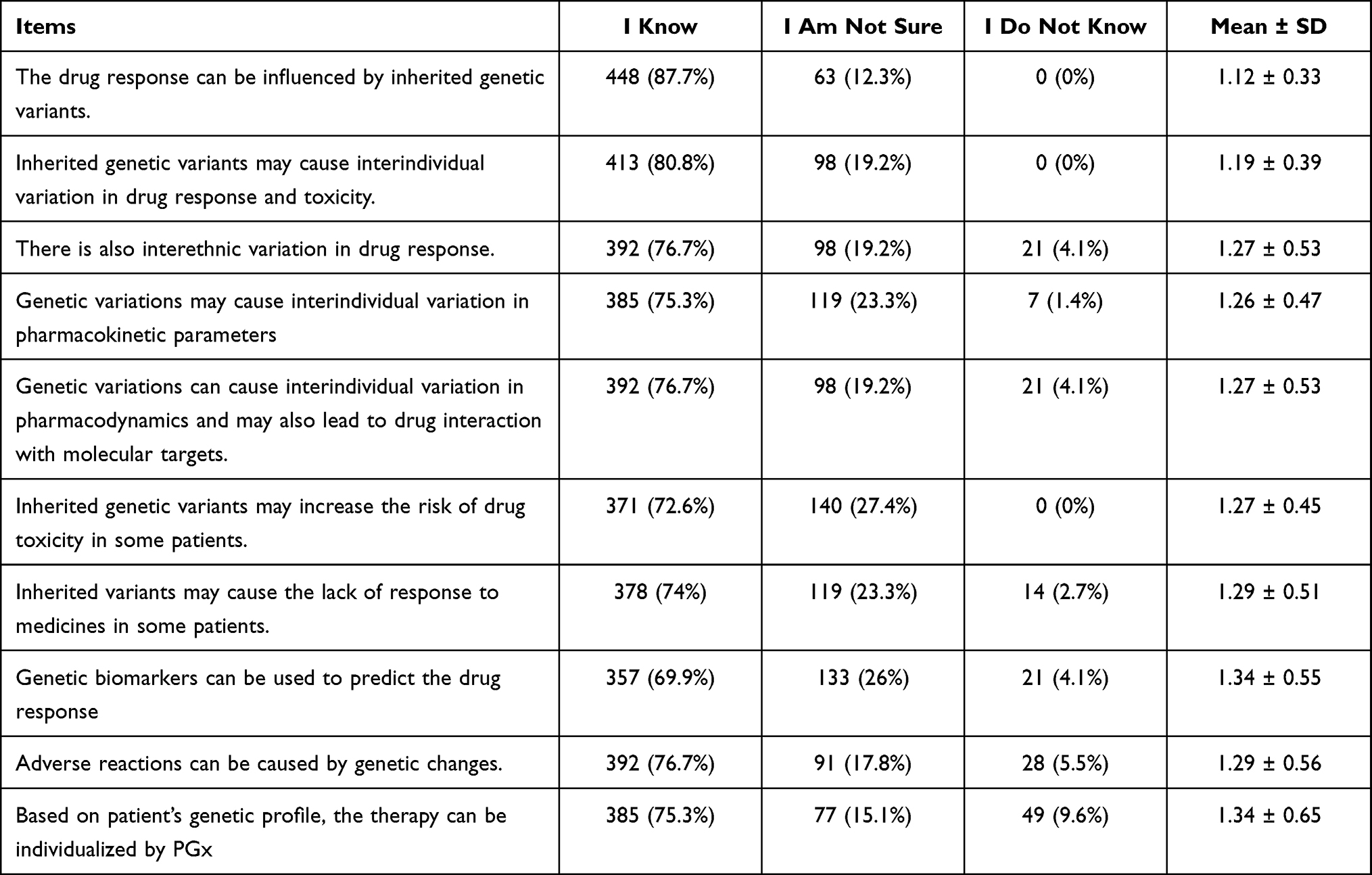 |
Table 3 Knowledge of the Students About PGx |
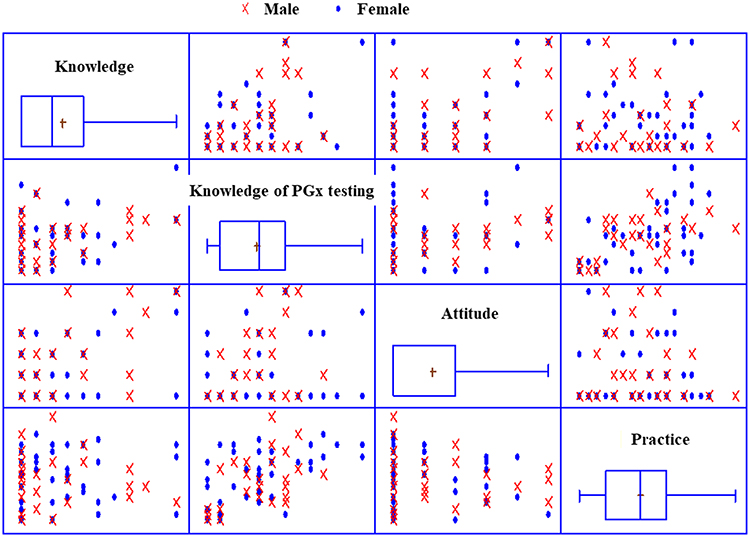 |
Figure 1 Gauge representing the level of knowledge, attitude and practice score. |
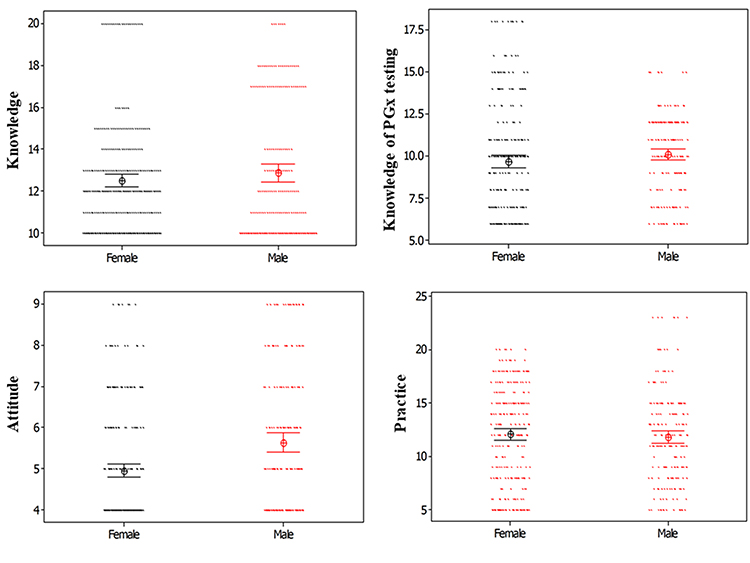 |
Figure 2 Scatterplot matrix for Gender wise comparison KAP score. |
Knowledge About Specific Validated PGx Testing
The mean knowledge score of the students was 9.84 for the PGx testing, as shown in the gauge chart in Figure 3. Most of the students (78.1%) knew that CYP2C9 variants could affect metabolism and response of warfarin. More than 40% of the students knew that VKORC1 variants could influence warfarin pharmacodynamics and its response (41.1%) and genetic variants in endothelial growth factor receptors could affect the response to erlotinib (46.6%). More than half of the participants (53.4%) knew that in the labelling of numerous drugs, the FDA presented clinical evidence for the PGx testing. About 47.9% of students knew that paroxetine was primarily metabolized by CYP2D6 and also inhibited this enzyme, and 42.5% knew that citalopram steady-state levels were not significantly different in poor metabolizers and extensive metabolizers of CYP2D6. Table 4 represents the knowledge of the students on the specific validated PGx testing. Good knowledge of the PGx testing positively and significantly (p=0.01) affected the students’ attitude and practice.
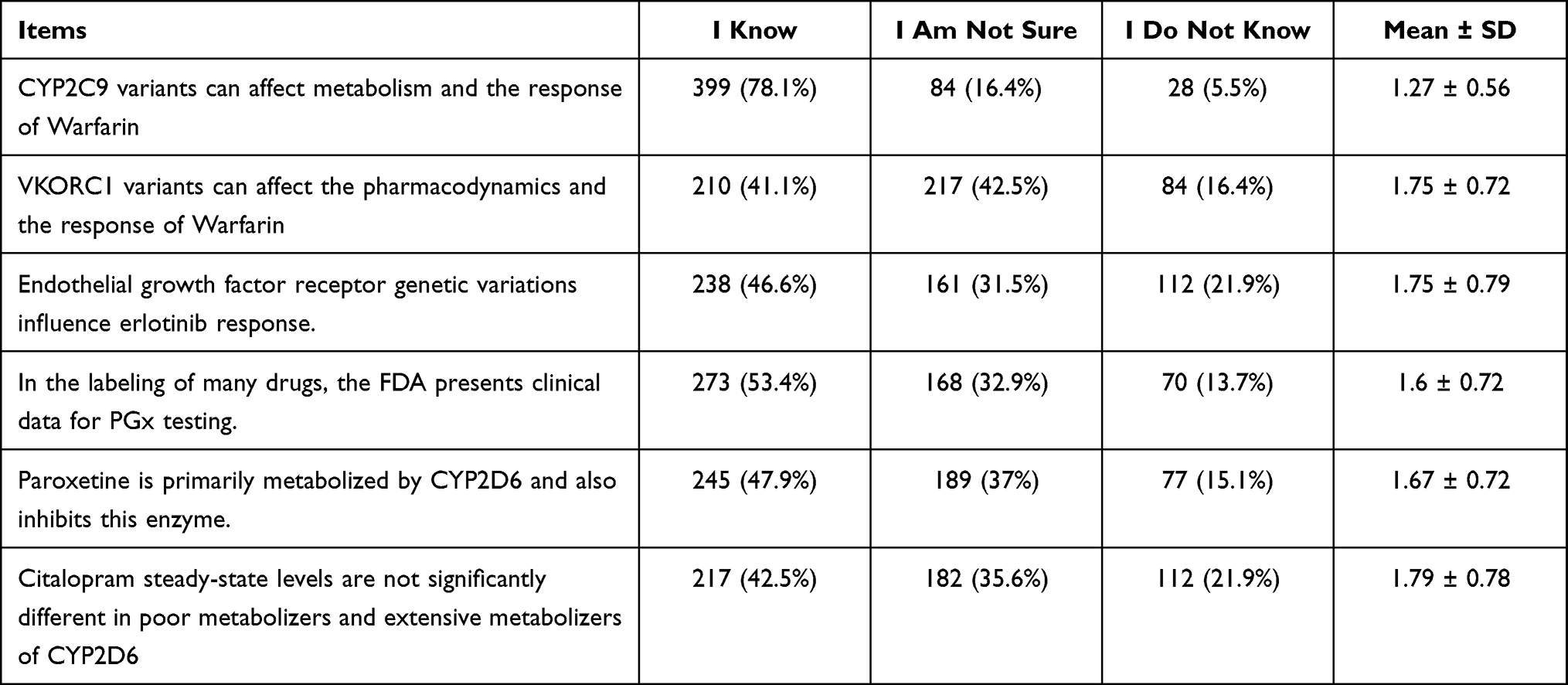 |
Table 4 Knowledge of the Students About PGx Testing According to Recommendation of US FDA |
 |
Figure 3 Individual value plots for comparison of gender-wise KAP score. |
Attitude Towards PGx
The mean attitude score of the students was 5.23. Majority of the students (more than 80%) believed that their future work could be improved by PGx testing in choosing the right drug and dose and wanted to know more about PGx. About 82% of students wanted to apply PGx in their future work and 58.9% wanted to study PGx in their postgraduate program. Table 5 represents the attitudes of the students towards PGx. Multivariate logistic regression showed that females were 2 times more likely to have a good attitude (C.I. = 1.34–3.148) compared to males. Good attitude positively and significantly (p=0.01) affected the knowledge of students. Figure 4 represents the gender and age-wise variation of attitude and practice for knowledge scores where straight line shows the linear regression model for both male and female students.
 |
Table 5 Attitudes of the Students Towards PGx |
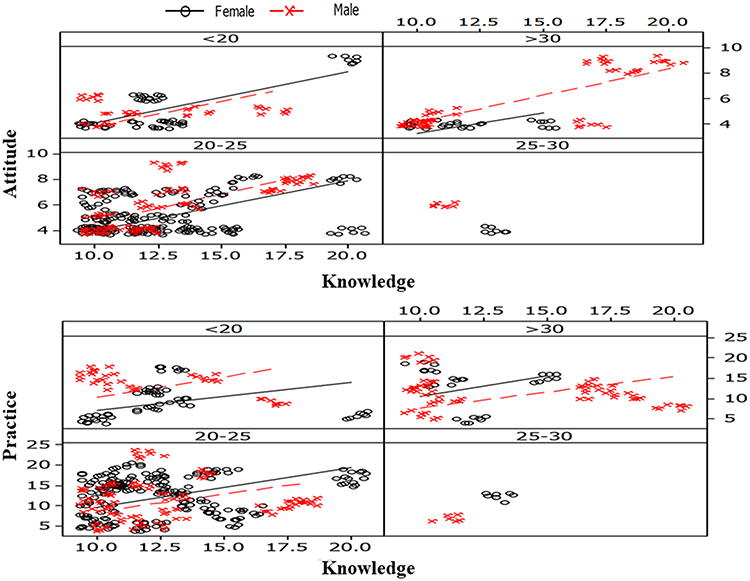 |
Figure 4 Gender and age-wise variation of attitude and practices for knowledge score and lines represent the linear regression model for male and female. |
Practice of PGx Testing
The students’ mean practice score was 11.95. 65% of the students always asked for information about ADRs and 37% always related genetic variation to ADRs. About 43% of the students always or at least once a month attended a lecture about the effects of genetic variations on drug therapy. When trying to solve a case study question related to drug, about 31.5% of the students implemented the idea of human genetic variation. 41% of the students always updated their knowledge on genetic information in relation to drugs. Table 6 represents student practice towards PGx. Good practice positively and significantly (p=0.01) affected the students’ knowledge of PGx testing, as shown in the correlation in Table 7. Multivariate logistic regression showed that females were more likely to have good practice (C.I. = 0.558–1.273) than males as represented in Table 8.
 |
Table 6 Practices of the Students Towards PGx |
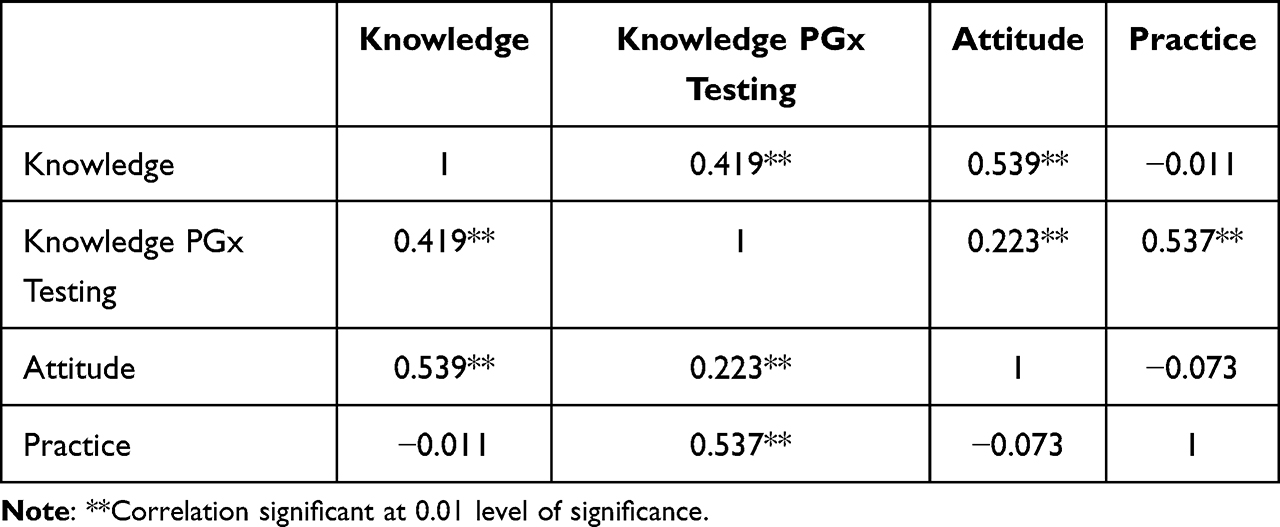 |
Table 7 Correlation of Knowledge, Attitudes and Practices of PGx |
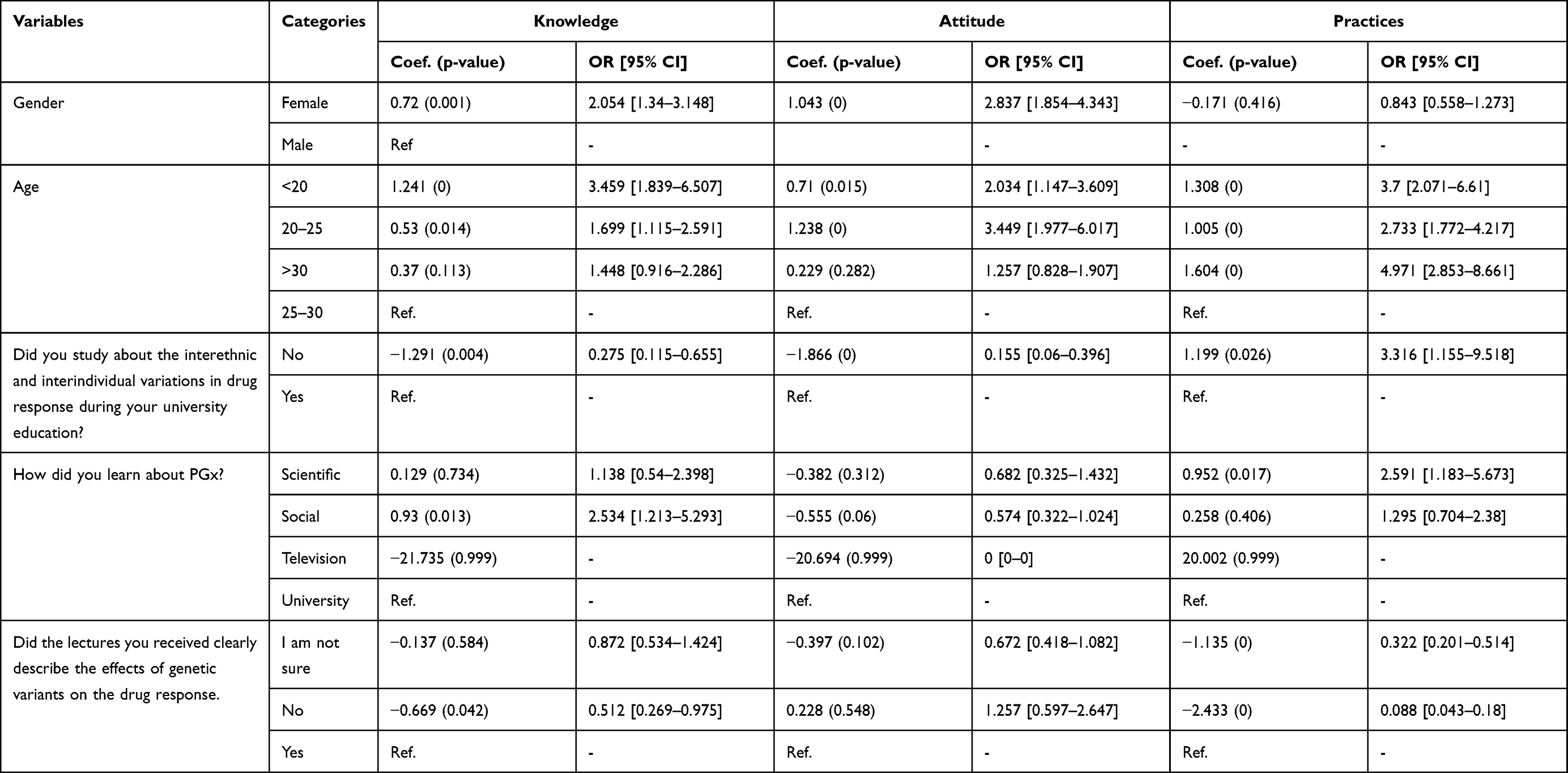 |
Table 8 Multivariate Logistic Regression Model for Factors Identification of Good KAP |
Discussion
Most of the students in study had good knowledge about PGx. The students were very knowledgeable about genetic variants and their effect on drug response. Most students were also aware of interethnic and interindividual variations in drug response. The knowledge of the students was found higher compared to the study conducted in Bosnia, where less than half of the participating students had good knowledge about PGx.12 Our data showed that students’ good knowledge had a positive and significant impact on the knowledge towards PGx testing and attitudes towards PGx. Our study revealed that female students had higher knowledge about PGx than male students. These findings were consistent with a study conducted in Jordan where most of the female students had higher knowledge levels.11 Another study showed that students had high expectations towards PGx, but most of them did not have adequate information about it.13 It was not the case in our findings because most of the students had significant knowledge about PGx. Knowledge of FDA recommendations about PGx testing of drugs was also good. Similar study conducted in Jordan reported less knowledge about PGx. This was probably because validated PGx biomarkers were not included in the training programs of clinical pharmacotherapy.11 Attitudes towards PGx were also good among students. Majority of the students considered PGx to be crucial in selecting the right drug and dose and were willing to apply PGx in their future practice. The linear regression modeling showed that female students had better attitude scores than the male students which could be due to their better focus and concentration on studies than male students. The good attitude positively and significantly affected the students’ knowledge and practice. Although, the pharmacy students had good knowledge and attitudes towards PGx, the practices regarding PGx were not quite up to the mark. Less than half of the students used the idea of human genetic variation when trying to solve a given drug-related case studies questions. Students’ knowledge of PGx testing was positively and significantly affected by their positive practice. Students in the age group of 20–25 years had better knowledge and good attitudes and practices as compared to younger students which could be due to their greater experience and application of PGx in practice. The current study indicates that there is room for improvement in senior pharmacy student practice with respect to PGx. This can be implemented through educational and motivational campaigns for the students to implement PGx.
Limitations
Our study included limited a number of questions which might not be enough to assess the knowledge, attitude and practice of PGx regarding all parameters.
Conclusions
Senior pharmacy students in Punjab, Pakistan had good knowledge and attitudes towards PGx. However, the practice in this regard is not up to the mark. There are some gaps in the students’ practice of PGx testing that need to be fulfilled to improve drug therapy and optimize the drug response.
Acknowledgments
The authors would like to acknowledge the Taif University Researchers Supporting Project number (TURSP-2020/68), Taif University, Taif, Saudi Arabia. The authors would like to thank the Deanship of scientific research at Umm Al-Qura University for supporting this work by grant code (22UQU4290565DSR16).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Aneesh TP, Sekhar S, Jose A, Chandran L, Zachariah SM. Pharmacogenomics: the right drug to the right person. J Clin Med Res. 2009;1(4):191. doi:10.4021/jocmr2009.08.1255
2. Roden DM, Wilke RA, Kroemer HK, Stein CM. Pharmacogenomics: the genetics of variable drug responses. Circulation. 2011;123(15):1661–1670. doi:10.1161/CIRCULATIONAHA.109.914820
3. Johnson J, Gong L, Whirl-Carrillo M, et al. Clinical pharmacogenetics implementation consortium: clinical pharmacogenetics implementation consortium guidelines for CYP2C9 and VKORC1 genotypes and warfarin dosing. Clin Pharmacol Ther. 2011;90(4):625–629. doi:10.1038/clpt.2011.185
4. Jarrar YB, Lee S-J. Molecular functionality of CYP2C9 polymorphisms and their influence on drug therapy. Drug Metabol Drug Interact. 2014;29(4):211–220. doi:10.1515/dmdi-2014-0001
5. Wang B, Canestaro W, Choudhry N. Clinical evidence supporting pharmacogenomic biomarker testing provided in US Food and Drug Administration drug. JAMA Intern Med. 2014;174:1938–1944.
6. Haga SB, Moaddeb J. Comparison of delivery strategies for pharmacogenetic testing services. Pharmacogenet Genomics. 2014;24(3):139. doi:10.1097/FPC.0000000000000028
7. Kisor DF, Farrell CL. Expanding pharmacist and student pharmacist access to genetics/genomics/pharmacogenomics competency education. J Med Edu Curric Develop. 2019;6:2382120519834325. doi:10.1177/2382120519834325
8. Blagec K, Koopmann R, Crommentuijn–van Rhenen M, et al. Implementing pharmacogenomics decision support across seven European countries: the Ubiquitous Pharmacogenomics (U-PGx) project. J Am Med Info Assoc. 2018;25(7):893–898. doi:10.1093/jamia/ocy005
9. Jarrar YB, Balasmeh AA, Jarrar W. Sequence analysis of the N-acetyltransferase 2 gene (NAT2) among Jordanian volunteers. Libyan J Med. 2018;13(1):1408381. doi:10.1080/19932820.2017.1408381
10. Indhumathi N, Singh D, Chong SS, Thelma B, Arabandi R, Srisailpathy CS. Fragile X CGG repeat variation in Tamil Nadu, South India: a comparison of radioactive and methylation-specific polymerase chain reaction in CGG repeat sizing. Genet Test Mol Biomarkers. 2012;16(2):113–122. doi:10.1089/gtmb.2011.0102
11. Jarrar Y, Mosleh R, Hawash M, Jarrar Q. Knowledge and attitudes of pharmacy students towards pharmacogenomics among universities in Jordan and west bank of Palestine. Pharmgenomics Pers Med. 2019;12:247. doi:10.2147/PGPM.S222705
12. Mahmutovic L, Akcesme B, Durakovic C, et al. Perceptions of students in health and molecular life sciences regarding pharmacogenomics and personalized medicine. Hum Genomics. 2018;12(1):1–15. doi:10.1186/s40246-018-0182-2
13. Bank PC, Swen JJ, Guchelaar H-J. A nationwide cross-sectional survey of pharmacy students on pharmacogenetic testing in The Netherlands. Pharmacogenomics. 2018;19(4):311–319. doi:10.2217/pgs-2017-0175
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.