Back to Journals » Patient Preference and Adherence » Volume 19
Knowledge, Attitudes, and Practices of Patients Undergoing Gastrointestinal Endoscopy Towards Painless Endoscopy: A Cross-Sectional Study
Authors Ma Z, Peng S, Shen R, Zhu M
Received 17 July 2025
Accepted for publication 24 December 2025
Published 31 December 2025 Volume 2025:19 Pages 4369—4381
DOI https://doi.org/10.2147/PPA.S554174
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Zhen Ma,* Sheng Peng,* Rongrong Shen, Ming Zhu
Department of Anesthesiology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ming Zhu, Department of Anesthesiology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, No. 725, Wanping South Road, Xuhui District, Shanghai, 200032, People’s Republic of China, Tel +86 13611944790, Email [email protected]
Background: Gastrointestinal endoscopy (GIE) is crucial for diagnosing digestive tract issues, yet discomfort remains a significant concern. This study aimed to investigate the knowledge, attitudes, and practices (KAP) of patients undergoing GIE in the Shanghai region regarding painless GIE.
Methods: We conducted a cross-sectional study at Longhua Hospital, Shanghai University of Traditional Chinese Medicine, from July 27, 2023, to November 28, 2023, using a questionnaire survey to collect data.
Results: A total of 472 valid questionnaires were collected. Among them, 273 (57.8%) were female, and 458 (97.0%) would receive painless GIE. The KAP scores were 7 (4– 9) for knowledge, 41 (36.5– 46) for attitudes, and 17 (16– 20) for practices. Correlation analyses showed that knowledge (r = 0.202, p < 0.001) and attitude (r = 0.290, p < 0.001) were positively correlated with practice. However, the correlation between knowledge and attitude was insignificant. Notably, 47.5% of patients recognized painless GIE as a safe examination method, and 37.1% affirmed its effectiveness in reducing fear. Additionally, 38.8% of respondents would recommend painless GIE to those who need it, although 30.1% would hesitate to visit the hospital because of nausea or discomfort. Multivariate analysis showed that being medical personnel was independently associated with positive practice.
Conclusion: Patients undergoing GIE in the Shanghai region exhibit limited knowledge, suboptimal attitudes, and inadequate practices regarding painless GIE. It is imperative to devise and implement targeted educational interventions to enhance patient awareness and foster the adoption of painless endoscopy techniques within clinical settings. Given the global increase in demand for patient-centered endoscopy services, our results may also serve as a useful reference for other countries or regions with similar healthcare systems, sedation practices, or cultural contexts.
Keywords: gastrointestinal endoscopy, painless gastrointestinal endoscopy, patient, knowledge, attitude, practice
Introduction
Gastrointestinal endoscopy (GIE), recognized as one of the most significant innovations in the medical field during the 20th century, has fundamentally transformed the diagnosis and management of GI disorders.1 As the role of GIE in the medical field has expanded, they have become increasingly integral in treating and diagnosing various GI tract conditions.2 The advancement of anesthesiology and the continuous development of anesthetic drugs have made it possible for endoscopic procedures, which were once painful, to be performed under anesthesia, leading to the widespread adoption of painless gastroscopy for screening diseases of the stomach, oesophagus, duodenum, and colorectum.3,4 Meanwhile, sedation-assisted gastrointestinal endoscopy has been increasingly adopted globally, with Asian countries reporting high utilization rates.5 In China, a recent national survey found that the sedation rate for gastrointestinal endoscopy was around 48% overall and only 47.9% for gastroscopy.6
Painless GIE enables patients to undergo diagnostic and therapeutic procedures under anesthesia with markedly improved comfort. These procedures are typically short, frequently performed, and rapidly executed. The use of appropriate sedation can enhance the quality of GIE examinations.7 However, painless GIE may lead to complications such as respiratory depression, reflux with aspiration, and hypotension. While other risks associated with GIE, such as bleeding, infection, and anesthetic complications, are relatively rare, they pose potential life-threatening outcomes.8 Additionally, colonoscopy exams can impact the work efficiency of up to one-third of patients, including missing workdays and/or experiencing reduced work productivity.9 These risks may influence the patient’s decision regarding painless endoscopy.
The Knowledge, Attitude, and Practice (KAP) model is a pivotal framework in public health that suggests one’s knowledge and attitudes significantly influence individual behaviors. This model is especially relevant in understanding health-related behaviors, as it integrates the assessment of knowledge, attitudes, and behavioral practices, often through KAP surveys. These surveys are instrumental in evaluating knowledge and risk perception, illuminating the intricate relationships between KAP in health contexts.10–13 While international studies have emphasized the role of sedation in improving patient tolerance and diagnostic quality during endoscopy, how these findings translate into the Chinese healthcare environment, where cultural expectations, healthcare accessibility, and sedation practices differ, remains insufficiently explored. In the specific area of painless GIE, understanding patient knowledge is essential for identifying gaps in education and informing targeted initiatives to better prepare individuals for their procedures. Assessing patient attitudes towards these procedures is critical for gaining insights into their preferences, anxieties, and expectations, which is fundamental to enhancing patient satisfaction and compliance. Moreover, an examination of the practices related to painless endoscopy provides an in-depth look into patients’ actual experiences, including how they manage pre-procedure anxiety, their perceptions of discomfort, and their post-procedure recovery. This focus is essential for the targeted population of patients undergoing GIE, as it addresses their concerns and experiences, with patient comfort and safety paramount.
Although many studies have been conducted on KAP in the field of gastrointestinal diseases, none have been carried out in this specific area14,15 Recognizing this gap, the current study aims to investigate the KAP of patients in the Shanghai region undergoing gastrointestinal endoscopy towards painless endoscopy. This investigation is poised to contribute significantly to developing more patient-centered care models, enhancing the quality of endoscopic services, and potentially increasing the uptake of screening procedures by alleviating fears and misconceptions about endoscopy. This study endeavours to optimize clinical outcomes and improve overall healthcare efficiency in gastroenterology, underscoring the critical role of patient-centered research in advancing medical practice and patient care.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted at Longhua Hospital, Shanghai University of Traditional Chinese Medicine, from July 27, 2023, to November 28, 2023. Participants were recruited from patients with different occupational backgrounds undergoing GIE at Longhua Hospital’s endoscopy department. The study was conducted in accordance with the Declaration of Helsinki and adhered to the STROBE guidelines for observational studies. This study was approved by the Ethics Committee of Longhua Hospital, Shanghai University of Traditional Chinese Medicine (No: 2023LCSY053). Before questionnaire collection, participants provided electronic informed consent, and only those consenting proceeded with the survey.
Inclusion criteria encompassed patients scheduled for GIE at Longhua Hospital, aged between 18 and 70 years, possessing clear consciousness and adequate literacy to understand and complete the questionnaire independently, as well as those who provided informed consent. Exclusion criteria included patients with mental disorders or severe cognitive impairments hindering cooperation, those who did not complete the questionnaire or did so hastily, and patients who, after verbal consent, chose to decline consent in the WeChat questionnaire’s informed consent section.
Study Setting
Longhua Hospital is a prestigious comprehensive hospital in Shanghai with advanced medical equipment and professional healthcare teams. It serves as a major regional center for gastrointestinal disease diagnosis and treatment. Before undergoing GIE, patients undergo a structured consultation process. Outpatients must visit the anesthesia clinic to consult about the benefits and risks of GIE. For inpatients, ward physicians provide procedure information and discuss painless GIE options. All patients have the autonomy to choose their preferred method unless there are clear contraindications to anesthesia. Because many participants were recruited from anesthesia clinics, where patients are already informed about and often favor painless GIE, the proportion choosing painless endoscopy in this study may be higher than in the general population.
Questionnaire Administration Process
Using a non-probability convenience sampling method, approximately 500 patients undergoing gastrointestinal endoscopy at the Endoscopy Department of Longhua Hospital, affiliated with Shanghai University of Traditional Chinese Medicine, were recruited between July and December 2023. Although convenience sampling facilitates practical and timely recruitment in a clinical setting, we acknowledge that this approach may introduce selection bias and limit the representativeness of the study population, which should be considered a methodological limitation. Prior to survey administration, all participants received comprehensive pre-procedure counseling detailing the potential risks and benefits associated with GIE anesthesia. The research team developed a structured electronic questionnaire using the Wenjuanxing online survey platform.
Questionnaire Introduction
The questionnaire design was informed by pertinent guidelines, including the “Expert Consensus on Sedation/Anesthesia for Digestive Endoscopy in China (2020 Edition)16” and existing literature. Following the initial design, input from experts in the fields of Gastroenterology and Anesthesiology was solicited to refine the questionnaire. Subsequently, a pilot test involving 60 participants was conducted, yielding a Cronbach’s α coefficient of 0.745 for the pre-experimental feedback survey. Adjustments were made to finalise the questionnaire based on feedback from pre-experimental participants and reliability analysis results.
Comprising four dimensions, the questionnaire encompasses demographic information, knowledge, attitude, and practice (Supplementary Figure 1). The knowledge dimension includes ten questions, with single-choice questions earning 1 point for correct or clear answers and 0 points for other options. For the multiple-choice question (K3), all listed options represented correct responses. Therefore, each selected option earned 1 point, and no incorrect options were present. The total possible score for the knowledge domain ranged from 0 to 14 points. The attitude dimension comprises eight questions rated on a five-point Likert scale ranging from very positive (5 points) to very negative (1 point), with a score range of 12–60 points. The practice dimension includes seven questions, with open-ended questions P2 and P3 not contributing to the score. The remaining five questions employ a five-point Likert scale ranging from always (5 points) to never (1 point), resulting in a score range of 5–25 points. Attaining scores above 70% of the maximum in each section indicates adequate knowledge, a positive attitude, and proactive practice, this cut-off has been adopted in previous KAP studies.17
Study Outcomes
The primary outcome of this study was to measure patients’ knowledge, attitudes, and practices (KAP) levels regarding painless gastrointestinal endoscopy (painless GIE) through a validated questionnaire. Knowledge was assessed using a 14-point scale, attitudes using a 60-point scale, and practices using a 25-point scale. Secondary outcomes included: (1) comparison of KAP differences among patients with different demographic and clinical characteristics, and (2) exploration of factors associated with KAP scores through correlation and multivariate analyses.
Sample Size Calculation
Following previously validated methodology for KAP studies,18 we calculated the required sample size using the formula:

where Z(1-α/2) = 1.96 (α = 0.05), p = 0.5 (to ensure a maximum sample size, we assumed that 0.5 patients had an adequate KAP), and δ = 0.05 (margin of error). This calculation yielded a minimum required sample size of 384. Accounting for an anticipated 80% effective response rate, we planned to distribute 480 questionnaires to ensure adequate statistical power.
Statistical Analysis
Statistical analysis was conducted using SPSS 26.0 (IBM Corp., Armonk, N.Y., USA). Continuous variables were described using median, 25th percentile, and 75th percentile, and between-group comparisons were performed using the Wilcoxon-Mann–Whitney test or Kruskal–Wallis analysis of variance. Categorical variables were presented as n (%). Spearman correlation analysis assessed the correlations between knowledge, attitude, and practice scores. In multivariate analysis, the median score was used as the cut-off value. Univariate variables with p<0.25 were enrolled in multivariate regression. Two-sided p<0.05 were considered statistically significant in this study.
Results
Sample Characteristics
Initially, a total of 535 questionnaires were returned in this study. The following cases were excluded: 15 disagreed to complete the questionnaire, 42 with the same IP address, and 6 with a completion time of less than 90 seconds or more than 1800 seconds, leaving 472 valid questionnaires with a validity rate of 88.22% (Figure 1). The Cronbach’s α coefficient value for all questionnaires in the formal experiment was 0.721, and the KMO value was 0.807. The sample was characterized by a relatively high socioeconomic profile, with 306 (64.8%) participants holding a bachelor’s or junior college degree and 209 (44.3%) reporting a monthly income above 10,000 Yuan. The median (25th percentile, 75th percentile) score of knowledge (possible range: 0–14), attitude (possible range: 12–60), and practice (possible range: 5–25) were 7 (4–9), 41 (36.5–46) and 17 (16–20), respectively (Table 1).
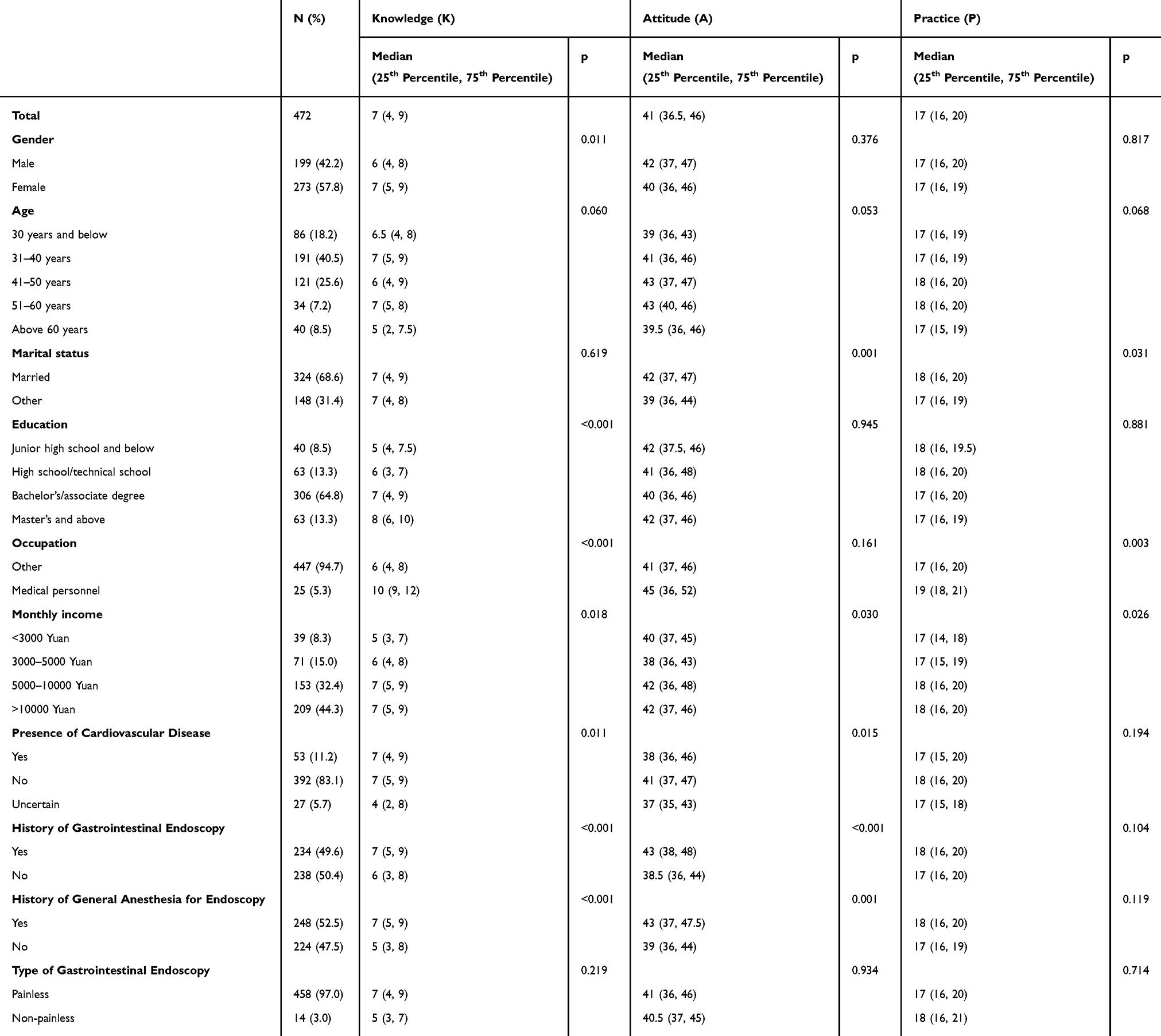 |
Table 1 Basic Information of Participants and KAP Score |
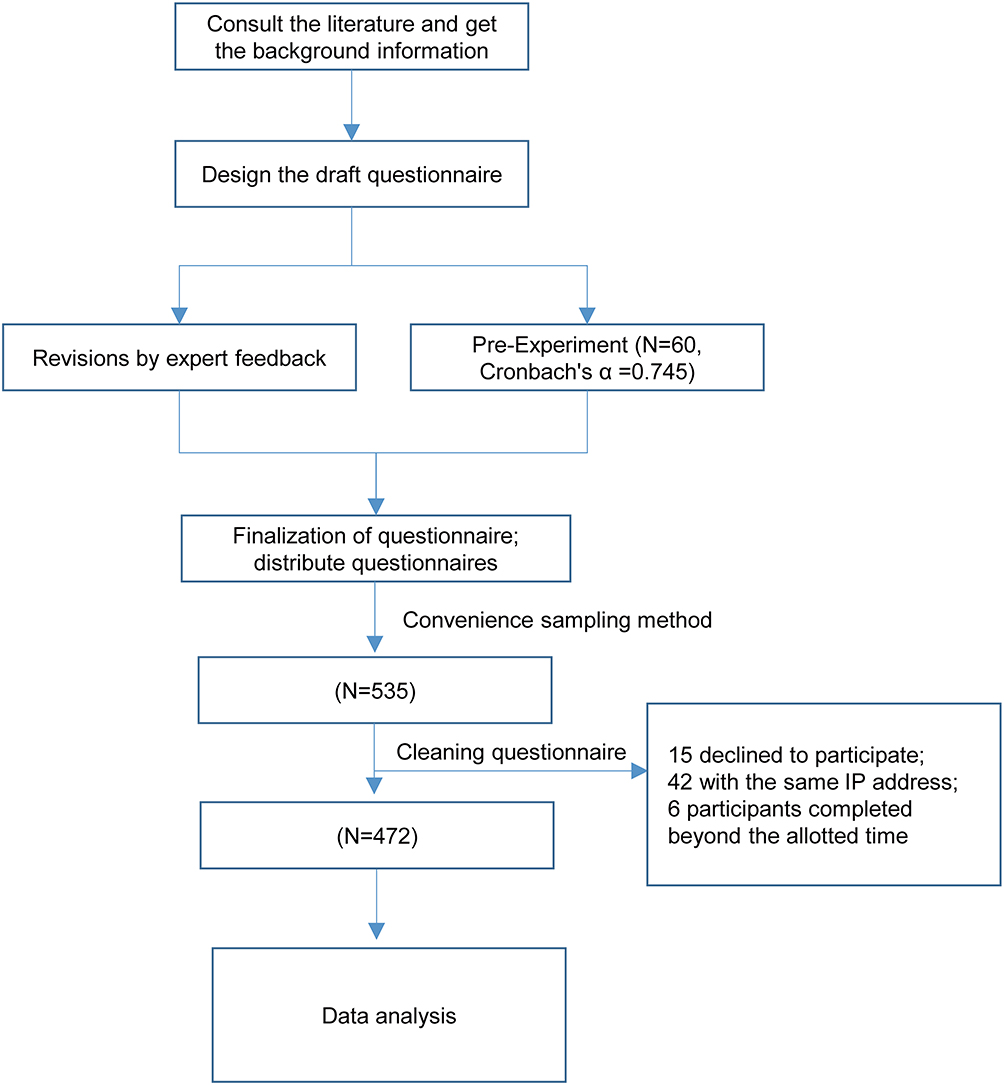 |
Figure 1 Research Design Flowchart. |
Knowledge, Attitude, and Practice Assessment Results
Most participants had heard of painless GIE, though substantial gaps remained in understanding its anesthesia process and potential complications. Awareness of traditional Chinese medicine–assisted approaches was particularly low (Table S1). Participants generally perceived painless GIE as safe and helpful in reducing procedural fear, yet notable concerns persisted regarding anesthesia-related risks and post-procedure communication (Table S2). Patients reported varying levels of proactive preparation and willingness to recommend painless GIE, although a considerable proportion still delayed examinations due to discomfort or anxiety (Table S3).
Correlation and Multivariate Analysis
Correlation analyses showed that knowledge (r = 0.202, p < 0.001) and attitude (r = 0.290, p < 0.001) were positively correlated with practice. However, the correlation between knowledge and attitude was non-significant (r = 0.053, p = 0.249) (Table 2).
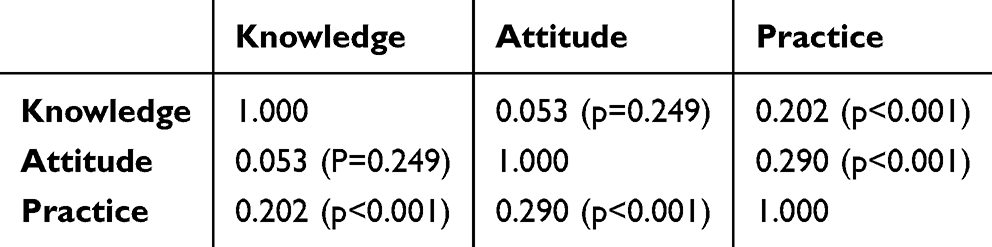 |
Table 2 Correlation Analysis of KAP Scores |
Variables with p < 0.25 in the univariate analysis were included in the multivariate analysis to assess the factors associated with the KAP; the results showed that with the education of Master’s degree and above (OR = 4.253, 95% CI: [1.792, 10.095], p = 0.001), medical personnel (OR = 8.099, 95% CI: [2.321, 28.268], p = 0.001), and without a history of general anesthesia for endoscopy (OR = 0.364, 95% CI: [0.245, 0.540], P<0.001) were independently associated with knowledge (Table S4). Meanwhile, non - married (OR = 0.599, 95% CI: [0.401, 0.896], p = 0.013) and without a history of general anesthesia for GIE (OR = 0.560, 95% CI: [0.386, 0.813], p = 0.002) were independently associated with negative attitude (Table S5). Patients with health care background were independently associated with positive practice (OR = 3.032, 95% CI: [1.021, 9.002], p = 0.0046). This finding is particularly noteworthy as it suggests that healthcare professionals’ medical knowledge and clinical experience may contribute to better practice behaviors regarding painless GIE. Their higher practice scores likely reflect a deeper understanding of the procedure’s benefits and risks, as well as greater familiarity with medical procedures in general (Table S6).
To evaluate the potential confounding effect of medical professionals, a supplementary multivariate logistic regression analysis was conducted excluding patients with a medical background. In this subset of patients, the supplementary multivariate analysis for knowledge (Table 3) revealed that higher education level (Master’s degree and above vs Junior high school and below: OR = 4.18, 95% CI: [1.52, 11.4], p = 0.005), having an uncertain cardiovascular disease status (vs Yes: OR = 0.30, 95% CI: [0.10, 0.91], p = 0.034), and not having a history of general anesthesia for endoscopy (vs Yes: OR = 0.41, 95% CI: [0.25, 0.68], p = 0.001) remained independently associated with knowledge regarding painless GIE. For attitude (Table 4), not having a history of gastrointestinal endoscopy (vs Yes: OR = 0.56, 95% CI: [0.35, 0.87], p = 0.012) was independently associated with a less positive attitude. No demographic or clinical factors were found to be independently associated with practice regarding painless GIE among patients without a medical background at the P<0.05 level (Table 5).
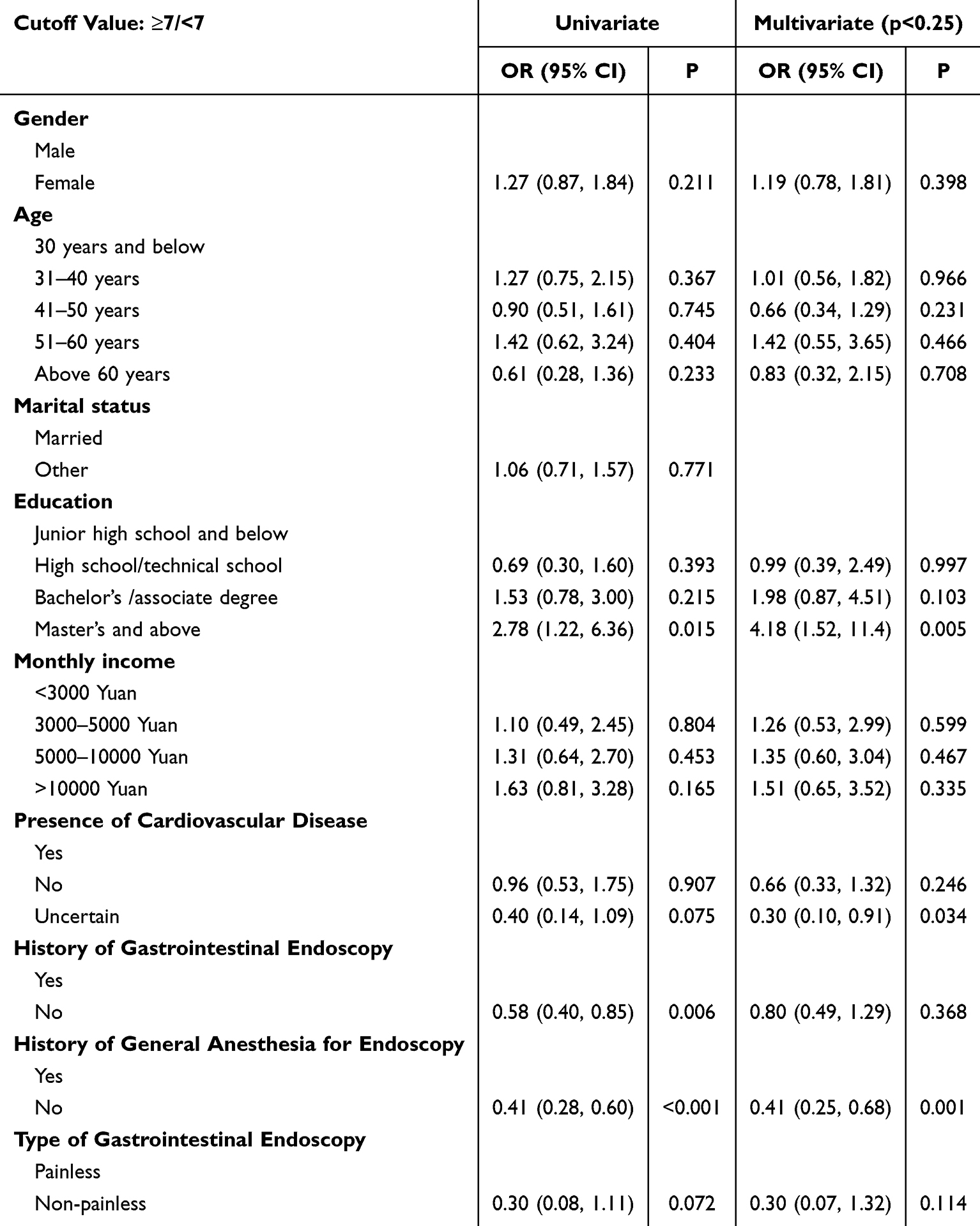 |
Table 3 Univariate and Multivariate Logistic Regression for Knowledge (Patients with Medical Background Were Excluded) |
 |
Table 4 Univariate and Multivariate Logistic Regression for Attitude (Patients with Medical Background Were Excluded) |
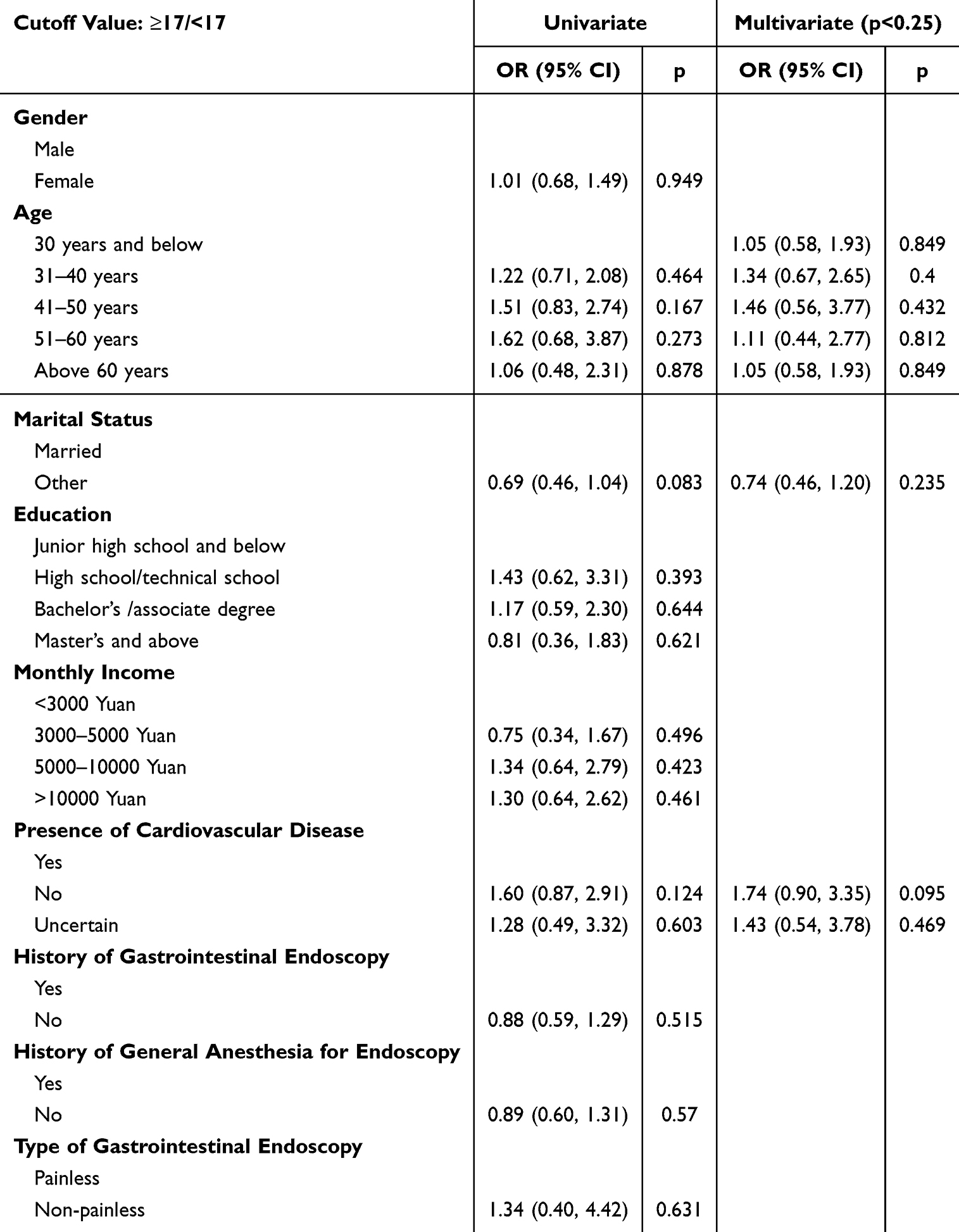 |
Table 5 Univariate and Multivariate Logistic Regression for Practice (Patients with Medical Background Were Excluded) |
Discussion
Patients undergoing gastrointestinal endoscopy in the Shanghai region exhibit inadequate knowledge, suboptimal attitudes, and practices towards painless GIE. These findings highlight the need for targeted educational interventions and improved standardized pre-procedure communication to enhance patient understanding and support clinical adoption of painless endoscopy. There is a critical need to enhance the quality and standardization of pre-procedure communication between physicians and patients. This should include comprehensive training for healthcare providers on effective patient communication, development of standardized patient education materials, and establishment of clear protocols for discussing procedural details, risks, and benefits.
Given that the study was conducted in a single tertiary hospital with a high proportion of patients visiting anesthesia clinics, the generalizability of the findings should be interpreted with caution. In particular, because most participants were recruited from anesthesia clinics within an urban tertiary hospital, the sample likely reflects higher awareness, access to sedation services, and health literacy than the general population, which further limits the external applicability of the findings. The findings of this study shed light on the existing KAP concerning painless GIE among patients in the Shanghai region. Correlation analyses unveiled significant positive associations among knowledge, attitude, and practice, indicating that patients with higher levels of expertise generally exhibit more positive attitudes and engage in healthier practices regarding painless endoscopy. However, the non-significant correlation between knowledge and attitude contradicts the expected KAP progression.19,20 This suggests that knowledge alone may not translate into attitudinal change and that other determinants, such as communication quality, prior experience, cultural beliefs, or system-level factors, may play a stronger role in shaping patients’ perceptions of painless endoscopy.
Among the significant findings, several socio-demographic factors emerge as influential determinants of patients’ KAP. Gender differences in knowledge scores indicate potential disparities in healthcare information accessibility or communication strategies, with females exhibiting higher levels of understanding. Occupation, monthly income, and medical history are significant predictors of patients’ KAP regarding painless endoscopy. Medical personnel exhibit notably higher knowledge scores, emphasizing the importance of professional background in healthcare comprehension and decision-making processes. Our findings regarding patient perspectives can be contextualized within the international literature on endoscopic procedures. International evidence similarly shows that patient engagement in endoscopic procedures is influenced by organizational factors, staff attitudes, and individual expectations.21 Consistent with our findings, prior studies have demonstrated that pre-procedure communication and patients’ expectations strongly affect satisfaction and willingness to undergo endoscopy.22 Comparable observations have also been reported in Asian settings, where awareness of endoscopic sedation varies widely and is shaped by socioeconomic and healthcare-system differences.23,24
Furthermore, income disparities highlight socioeconomic influences on healthcare-seeking behaviors and access to information, necessitating targeted interventions to address equity issues.25,26 Our initial multivariate analysis identified medical occupation, higher educational attainment, and a history of general anesthesia as key factors influencing KAP levels. However, in light of the potential influence of medical professionals, we conducted a supplementary multivariate analysis excluding healthcare personnel. The updated results confirmed that among the general patient population, postgraduate education and previous anesthesia experience remained significantly associated with knowledge about painless GIE. Yet, no demographic or clinical factors were significantly associated with either attitude or practice after excluding medical staff. This finding emphasizes the central role of professional medical background in shaping attitudes and behaviors toward painless endoscopy and suggests that for the general population, influencing factors may be more complex, requiring targeted and context-specific interventions to improve understanding and engagement.27,28 The positive association between previous endoscopy experience and higher KAP scores has important clinical implications. A recent systematic review demonstrated that prior endoscopy experience significantly reduced pre-procedural anxiety and improved procedure tolerance.29 This highlights the importance of ensuring positive first-time experiences with painless GIE, as they may significantly influence patients’ future compliance with necessary follow-up procedures. Such experiences not only shape individual patient attitudes but also contribute to the broader community perception of painless GIE through word-of-mouth recommendations and shared experiences.
Among the knowledge-related items, awareness of painless GIE garnered a high affirmative response, indicating a commendable level of familiarity with this procedure among the participants. Conversely, knowledge of the potential adverse effects of GIE, such as malignant vomiting and gastrointestinal perforation, was varied, with a significant number of participants being unsure of these risks. Additionally, knowledge of traditional Chinese medicine’s potential in alleviating endoscopy-related discomfort received notably lower scores. This suggests a potential gap in understanding alternative discomfort management methods among patients in our sample compared to recognising the procedure itself.
Turning to the attitude dimension, the results revealed a predominantly positive perception of painless GIE’s safety. Additionally, the significant reduction in fear reported by participants due to the painless nature of the procedure suggests that patient anxiety can be effectively mitigated through pain management techniques. Conversely, there were concerns about potential breaches in communication and informed consent, with a substantial proportion of participants expressing worry about not being informed of examination results after anesthesia. These apprehensions underscore the importance of transparent communication and patient involvement in healthcare decision-making processes to foster trust and mitigate fears. To address this, healthcare facilities should implement transparent communication protocols to ensure patients are fully informed about the safety of painless gastrointestinal endoscopy.30,31 Furthermore, healthcare providers should emphasize the importance of post-procedural communication, ensuring patients are reassured about the accuracy of the examination results and the thoroughness of the procedure. Additionally, establishing clear procedures for obtaining informed consent, including discussions about post-anesthesia care and result disclosure, can alleviate patient concerns and enhance trust in the healthcare provider. By fostering open and honest communication, healthcare providers can build solid patient-provider relationships and improve patient confidence in the procedure’s safety and efficacy.32,33
Regarding the practice dimension, the results highlighted a proactive approach among participants in assessing their health conditions before opting for painless GIE. This indicates a commendable effort in patient engagement and shared decision-making, vital for promoting patient autonomy and treatment adherence. However, a significant proportion of participants reported delaying endoscopic examinations due to anxiety and nausea, indicating that procedural fears remain a substantial barrier to timely healthcare utilization. These findings emphasize the need for targeted interventions addressing procedural anxieties and enhancing patient support mechanisms to facilitate timely access to healthcare services. To mitigate this, it is crucial for healthcare providers to offer comprehensive pre-procedural counseling sessions aimed at reducing patient anxiety and discomfort, thereby promoting more timely healthcare-seeking behaviors. Based on these findings, we recommend implementing practical and feasible interventions within existing clinical workflows. These include: (1) developing standardized patient education materials that can be easily distributed during routine pre-procedure consultations, (2) utilizing existing hospital information systems to deliver educational content through mobile applications or WeChat platforms, which are already widely used in our hospital system, and (3) incorporating brief, structured assessment tools during regular pre-procedure consultations to identify patients who may need additional support. These recommendations are designed to enhance patient education and support without significantly increasing the workload of clinical staff. Additionally, these interventions can be integrated into existing appointment scheduling and pre-procedure consultation processes, making them both practical and sustainable in busy clinical settings. These insights suggest a meaningful opportunity to improve patient education and enhance pre-procedure consultation protocols, particularly in similar clinical contexts.
This study has several limitations that should be acknowledged. First, the cross-sectional design restricts our ability to infer causal relationships between the studied variables, as it only captures data at a single point in time. Second, the data were collected from a single tertiary hospital located in an urban area, where patients generally have higher health literacy, better access to sedation services, and stronger preferences for painless procedures. This urban, anesthesia-clinic–based recruitment resulted in 97% of participants choosing painless GIE, which may not reflect patterns in community hospitals or rural regions. Therefore, the generalizability of our findings to broader or less medically resourced populations is limited. Additionally, the inclusion of healthcare professionals (5.3% of participants), who demonstrated significantly higher knowledge and practice scores, may have influenced our overall results. To evaluate this potential confounding, we performed a supplementary regression analysis excluding all medical professionals. The analysis confirmed that while knowledge-related predictors remained significant, no variables were associated with practices. This underscores both the strong influence of medical training and the need for cautious interpretation of our findings among non-medical populations. In addition, all attitudes and practices were self-reported, which may introduce response bias, including social desirability bias, and could affect the accuracy of participants’ reported behaviors. Third, our study did not differentiate between upper and lower GIE procedures, which may have different risk profiles and patient experiences. Future studies should consider analyzing these procedures separately to provide more procedure-specific insights. Given that these procedures may involve different levels of patient discomfort, preparation requirements, and risk considerations, future research should examine them separately to provide more targeted recommendations for each procedure type.
Conclusions
In conclusion, our study reveals that GIE patients in the Shanghai region exhibit inadequate knowledge, suboptimal attitudes, and practices toward painless GIE. These findings may also offer useful reference for other regions or countries with similar healthcare structures or sedation practices, where patient-centered endoscopy is increasingly emphasized. Healthcare providers should implement educational interventions targeting patients, particularly those with lower educational levels and those with negative attitudes towards painless GIE, to improve their understanding and acceptance of painless endoscopic procedures.
Abbreviations
KAP, knowledge, attitudes, and practices; TCM, traditional Chinese medicine.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethics Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki and adhered to the STROBE guidelines for reporting observational studies. This study was approved by the Ethic Committee of Longhua Hospital, Shanghai University of Traditional Chinese Medicine (No: 2023LCSY053). Prior to questionnaire collection, participants provided electronic informed consent, and only those consenting proceeded with the survey. I confirm that all methods were performed in accordance with the relevant guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Cheung DY, Jang BI, Kim SW, et al. Multidisciplinary and multisociety practice guideline on reprocessing flexible gastrointestinal endoscopes and endoscopic accessories. Clin Endosc. 2020;53(3):276–285. doi:10.5946/ce.2020.106
2. Galai T, Yerushalmy-Feler A, Heller NP, et al. Age and pain score before gastrointestinal endoscopies in children are predictors for post procedure pain. BMC Gastroenterol. 2020;20(1):400. doi:10.1186/s12876-020-01546-y
3. Faust AC, Rajan P, Sheperd LA, Alvarez CA, McCorstin P, Doebele RL. Impact of an analgesia-based sedation protocol on mechanically ventilated patients in a medical intensive care unit. Anesth Analg. 2016;123(4):903–909. doi:10.1213/ANE.0000000000001393
4. Hall JE, Uhrich TD, Barney JA, Arain SR, Ebert TJ. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg. 2000;90(3):699–705. doi:10.1097/00000539-200003000-00035
5. Xiong Y, Yan H, Qu L, et al. Global trends of gastrointestinal endoscopy anesthesia/sedation: a bibliometric study (from 2001 to 2022). J Pain Res. 2023;16:2393–2406. doi:10.2147/JPR.S408811
6. Zhou S, Zhu Z, Dai W, et al. National survey on sedation for gastrointestinal endoscopy in 2758 Chinese hospitals. Br J Anaesth. 2021;127(1):56–64. doi:10.1016/j.bja.2021.01.028
7. Cooper AB, Thornley KS, Young GB, Slutsky AS, Stewart TE, Hanly PJ. Sleep in critically ill patients requiring mechanical ventilation. Chest. 2000;117(3):809–818. doi:10.1378/chest.117.3.809
8. Inderjeeth AJ, Webberley KM, Muir J, Marshall BJ. The potential of computerised analysis of bowel sounds for diagnosis of gastrointestinal conditions: a systematic review. Syst Rev. 2018;7(1):124. doi:10.1186/s13643-018-0789-3
9. Fuccio L, Collatuzzo G, Frazzoni L, et al. Impact of colonoscopy on working productivity: a prospective multicenter observational study. Gastrointest Endosc. 2022;95(3):550–561.e558. doi:10.1016/j.gie.2021.11.039
10. Aerts C, Revilla M, Duval L, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. 2020;14(4):e0008149. doi:10.1371/journal.pntd.0008149
11. Liao L, Feng H, Jiao J, Zhao Y, Ning H. Nursing assistants’ knowledge, attitudes and training needs regarding urinary incontinence in nursing homes: a mixed-methods study. BMC Geriatr. 2023;23(1):39. doi:10.1186/s12877-023-03762-z
12. Mumena WA. Maternal knowledge, attitude and practices toward free sugar and the associations with free sugar intake in children. Nutrients. 2021;13(12):4403. doi:10.3390/nu13124403
13. Zhu Y, Luo Y, Li L, et al. Immune response plays a role in Mycoplasma pneumoniae pneumonia. Front Immunol. 2023;14:1189647. doi:10.3389/fimmu.2023.1189647
14. Abbasi A, Shahzad K, Shabbir RMK, et al. Demographic attributes of knowledge, attitude, practices, and one health perspective regarding Diarrhea in Pakistan. Front Public Health. 2021;9:731272. doi:10.3389/fpubh.2021.731272
15. Shao XX, Fang LY, Guo XR, Wang WZ, Shi RX, Lin DP. Knowledge, attitude, and practice of patients living with inflammatory bowel disease: a cross-sectional study. World J Gastroenterol. 2023;29(43):5818–5833. doi:10.3748/wjg.v29.i43.5818
16. Expert consensus on sedation/anesthesia for digestive endoscopy in China (2020 Edition).
17. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
18. Gebeyehu DT, Bekele D, Mulate B, Gugsa G, Tintagu T. Knowledge, attitude and practice of animal producers towards antimicrobial use and antimicrobial resistance in Oromia zone, north eastern Ethiopia. PLoS One. 2021;16(5):e0251596. doi:10.1371/journal.pone.0251596
19. Norhayati MN, Nawi ZM. Validity and reliability of the Noor Evidence-Based Medicine Questionnaire: a cross-sectional study. PLoS One. 2021;16(4):e0249660. doi:10.1371/journal.pone.0249660
20. Schäfer F, Faviez C, Voillot P, et al. Mapping and modeling of discussions related to gastrointestinal discomfort in French-speaking online forums: results of a 15-year retrospective infodemiology study. J Med Internet Res. 2020;22(11):e17247. doi:10.2196/17247
21. Dubois H, Creutzfeldt J, Törnqvist M, Bergenmar M. Patient participation in gastrointestinal endoscopy - From patients’ perspectives. Health Expect. 2020;23(4):893–903.
22. Saydy N, Moubayed SP, Desrosiers M. Patient perspectives on endoscopic sinus surgery for chronic rhinosinusitis. J Otolaryngol Head Neck Surg. 2021;50(1):34. doi:10.1186/s40463-021-00515-z
23. Park SY, Lee JK, Park CH, et al. Endoscopist-driven sedation practices in South Korea: re-evaluation considering the nationwide survey in 2019. Gut Liver. 2022;16(6):899–906. doi:10.5009/gnl210466
24. Liu X, Ren Y, Jin W, Li P, Wang L. Knowledge, attitudes, and practices regarding Post-anesthesia cognitive dysfunction in patients undergoing gastrointestinal endoscopy. BMC Anesthesiology. 2024;24(1):264. doi:10.1186/s12871-024-02629-z
25. Haggerty J, Levesque JF, Harris M, et al. Does healthcare inequity reflect variations in peoples’ abilities to access healthcare? Results from a multi-jurisdictional interventional study in two high-income countries. Int J Equity Health. 2020;19(1):167. doi:10.1186/s12939-020-01281-6
26. Rosário EVN, Severo M, Francisco D, Brito M, Costa D. Examining the relation between the subjective and objective social status with health reported needs and health-seeking behaviour in Dande, Angola. BMC Public Health. 2021;21(1):979. doi:10.1186/s12889-021-11003-4
27. Cruz D, Rodriguez Y, Mastropaolo C. Perceived microaggressions in health care: a measurement study. PLoS One. 2019;14(2):e0211620. doi:10.1371/journal.pone.0211620
28. Goldman J, MacMillan K, Kitto S, Wu R, Silver I, Reeves S. Bedside nurses’ roles in discharge collaboration in general internal medicine: disconnected, disempowered and devalued? Nurs Inq. 2018;25(3):e12236. doi:10.1111/nin.12236
29. Fung BM, Leon DJ, Beck LN, Tabibian JH. Pre-procedural preparation and sedation for gastrointestinal endoscopy in patients with advanced liver disease. Dig Dis Sci. 2022;67(7):2739–2753. doi:10.1007/s10620-021-07111-1
30. Bae JH, Han HW, Yang SY, et al. Natural language processing for assessing quality indicators in free-text colonoscopy and pathology reports: development and usability study. JMIR Med Inform. 2022;10(4):e35257. doi:10.2196/35257
31. Sun TJ, Cheng CS, Zhang HD. Optimizing the performance of magnet-controlled capsule endoscopy based on radiological and gastroscopic modeling. Exp Ther Med. 2020;19(1):248–254. doi:10.3892/etm.2019.8202
32. Matsubayashi M, Nakamura K, Sugawara M, Kamishima S. Nursing difficulties and issues in endoscopic sedation: qualitative research in Japan. Gastroenterol Nurs. 2022;45(3):174–183. doi:10.1097/SGA.0000000000000627
33. Singh K, Gandhi S, Batool R. A case-control study of the association between vitamin D levels and gastric incomplete intestinal metaplasia. Nutrients. 2018;10(5):629. doi:10.3390/nu10050629
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.