Back to Journals » Infection and Drug Resistance » Volume 15
Knowledge, Attitudes and Practices of Patients on Antibiotic Resistance and Use in Public Hospitals of Amhara Regional State, Northwestern Ethiopia: A Cross-Sectional Study
Received 29 November 2021
Accepted for publication 13 January 2022
Published 22 January 2022 Volume 2022:15 Pages 193—209
DOI https://doi.org/10.2147/IDR.S348765
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Kindu Geta,1,2 Mulugeta Kibret2
1Department of Biology, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Biology, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Kindu Geta, Email [email protected]
Background: Although inappropriate antibiotic use could contribute to the spread of antimicrobial resistance, data on the knowledge, attitude and practice of antibiotic use and resistance among patients in north-western Ethiopia are scarce. This study assessed patients’ knowledge, attitudes and practices regarding antibiotic use and resistance in selected public hospitals of Amhara regional state, Ethiopia.
Methods: A cross-sectional study was conducted in selected public hospitals of Amhara regional state from November to December 2020 to assess the knowledge, attitude, and practice of patients on antibiotic resistance and use. Data were collected from 233 participants using a structured questionnaire and analyzed using SPSS version 23.
Results: According to the findings, 60.3% of the participants obtained their antibiotics without a prescription from private pharmacies, and the most commonly used antibiotic to treat human diseases was ampicillin (70.7%). Even though 69.8% of the patients heard about antibiotics and antibiotic resistance from several sources, 68.1– 87.9% of them were unaware on the factors that contribute to the transmission of resistant bacteria to humans and the impact of antibiotic resistance on human and animal health. Using the mean score of 3.15 ± 0.08 as the cut-off, 37.5% of patients know about antimicrobial resistance and use. With a mean score of 27.6 ± 0.3, 45.3% of patients had positive attitudes toward prudent antibiotic use and resistance. About 44% of participants had a good practice, with a mean practice score of 4.95 ± 0.17. A higher level of education was associated with better knowledge, positive attitudes, and better practices regarding antibiotic use and resistance. Although 57.3% of respondents viewed poor handwashing practices in hospitals as a major factor contributing to increased antibiotic resistance, 59.9% of respondents viewed implementing hygiene, infection prevention, and control practices as a major strategy contributing to reducing antibiotic use and resistance.
Conclusion: According to the present study, there is a low level of awareness among patients about the proper antibiotics use and resistance. It is essential to raise awareness, develop, and implement interventions to reduce antimicrobial use and antibiotic resistance in the study area.
Keywords: antibiotic use, antibiotic resistance, attitude, knowledge, patients, practice
Graphical Abstract:

Introduction
In many developed and developing countries, antibiotics are the most commonly prescribed drugs. It is estimated that between 20–50% of antibiotic use is either unnecessary or inappropriate.1,2 This contributes to raising the complexity of antibiotic resistance worldwide, which harms patient outcomes.3,4 Patients’ inappropriate use of antimicrobial is a major contributor to the global spread of antimicrobial resistance.
Inappropriate and excessive antibiotic use results from a complex interaction of numerous factors related to patient knowledge and attitude, such as patient demand; incorrect self-medication habits; noncompliance; patients’ experience with antibiotics; and insufficient patient education.5,6 The situation is even worse in developing countries, where the use of antibiotics without medical supervision is facilitated by lax regulation of the distribution and sale of prescription drugs.7
Antimicrobial can be obtained without a prescription in developing countries from community pharmacies, drugstores, or even commodity shops.8 According to studies conducted in various African and Asian countries, self-medication is widely practiced on those continents.9,10 Similar findings were found in various settings in Ethiopia, indicating a high prevalence of self-medication in the country.11,12 Antimicrobial misuse is influenced by factors such as health professional incompetence, inaccessibility of healthcare facilities, and patients’ knowledge, beliefs, and perceptions about antimicrobial use.13
In response to the global health risk posed by antibiotic resistance, the National Department of Health developed the Antimicrobial Resistance National Strategy Framework, intending to reduce future increases in resistant bacterial infections and improve patient outcomes in South Africa.14 This framework emphasizes public communication to raise antibiotic awareness, as well as patient education on the dangers of antibiotic misuse.14 Antibiotic use is influenced by patients’ knowledge and attitude toward antibiotics.13,15 Antibiotic misuse by patients significantly contributes to the emergence and spread of bacterial resistance.13 Understanding patients’ antibiotic knowledge, attitudes and practices can help to maintain antibiotic effectiveness and it is a crucial step in the design of strategies to combat this public health threat.
Currently, information on patients’ knowledge, attitudes and practices regarding antimicrobial resistance (AMR) and antimicrobial use, factors that contribute to the utilization of antimicrobial and resistance, and intervention to reduce antibiotic resistance and use in patients, as well as the impact of antimicrobial resistance, is scarce in Ethiopia, particularly in north-western Ethiopia. Therefore, we conducted a study to evaluate patients’ knowledge, attitude, and practice regarding antimicrobial use and resistance in selected cities of Amhara regional state, north-western Ethiopia.
Materials and Methods
Study Design, Period, and Setting
An institutional-based cross-sectional survey study was conducted among inpatients who attend in public hospitals in Debre Tabor, Bahir Dar, and Debre Markos cities from November to December 2020 (Figure 1).
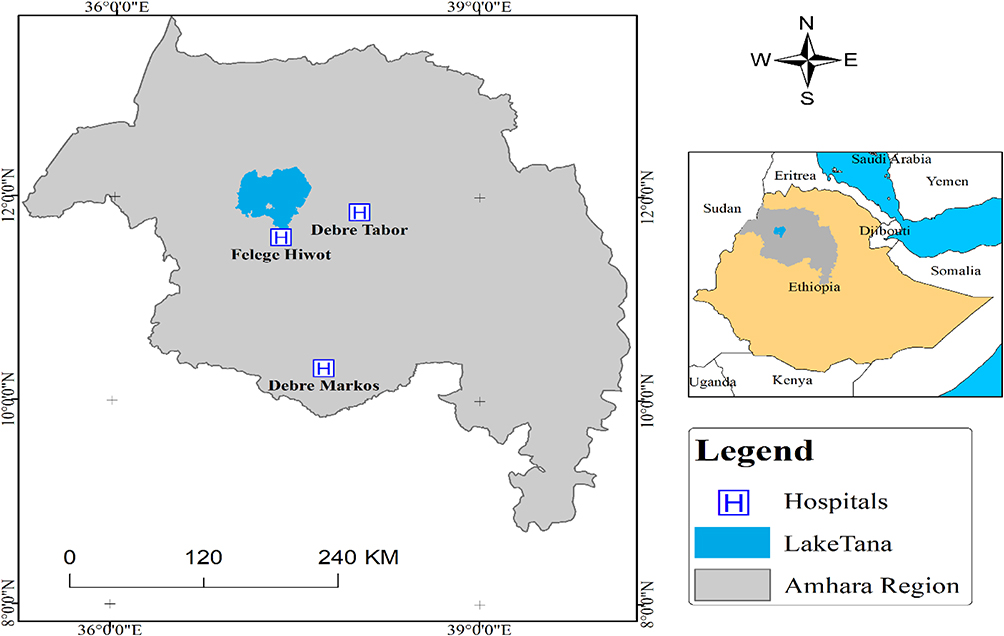 |
Figure 1 Map of the study area. |
Sample Size and Sampling Technique
A sample size of 460 was calculated using a formula developed by Daniel and Cross16 with the assumption of 5% margin of error (d), 95% confidence level (zα/2 =1.96), expected maximum correct answer on the questions about knowledge of AMR 50% will be assumed (P) and 20% contingency for non-response. All patients who attended in selected public hospitals during the study period and were willing to participate in the study were included, while those unwilling to participate in the study were excluded. To select a sample of respondents in the region, a multi-stage sampling procedure was used. First three cities were chosen at random from the Amhara region. Since each city has one public hospital all public hospitals found in the cities were used to select the participants. When the calculated sample size (460) was proportionally allocated to each stratum (livestock farm owners, physicians, and inpatients) based on their population, 232 patients were allotted. The participants were then assigned to each hospital in proportion to their population (Debre Markos Referral Hospital = 93, Bahir Dar Specialized Hospital =105, and Debre Tabor General Hospital =35), and study subjects were chosen using a simple random sampling technique.
Data Collection Tools and Procedure
The researchers developed structured questionnaires to collect data after conducting a thorough review of comparable studies.9,17 The questionnaire is divided into 7 sections. The first section included demographic information such as age, gender, religion, marital status, occupation, and level of education. In the second part, patients were asked to answer a series of questions about antibiotic use. The third and fourth parts of the questions focused on participants’ knowledge and attitudes toward antibiotic use and resistance. The fifth section of questions focused on participants’ antibiotic use practices. Participants were asked about factors that contribute to antibiotic resistance in the sixth section of the questionnaire. Participants were asked about possible measures to reduce the risk of antibiotic resistance in the final sections of the questionnaire. At the time of completing the questionnaire, the investigators were present to answer any questions from the respondents.18
Three trained data collectors (health professionals) were assigned to the data collection process, and the data collection medium was translated to Amharic. For the study participants, hard copies of written informed consent containing questionnaires were distributed. Data from uneducated participants were gathered through interviews. Then, data collectors collected completed questionnaires from study participants, and the questionnaires were checked for accuracy. Incomplete questionnaires were returned to participants in the study for completion. The questionnaires were labeled and coded using the questionnaire number after completion.18
Methods of Measurement (Scoring)
Each correct response was given a score of 1 for knowledge and practice assessment, while a wrong or doubtful response was given a score of 0. Responses to attitude-related questions were graded on a 3-point Likert scale, with a “1” to disagree and a “3” to agree. We used the mean as a cut-off point because there was no cut-off point to assess poor and better knowledge. Scores above and equal to the mean indicate better knowledge, better practice, and a positive attitude, whereas scores below the mean indicate poor knowledge, poor practice, and a negative attitude.18,19
Data Quality Control
A pilot study involving 10% of the patients who were not included in the final study was used to ensure fluency and accuracy in question design and language. The contents of the data collection tools were slightly modified based on the pilot survey. The questionnaire was then reviewed and assessed by subject experts for its content, design, relevance, and understanding. Data collectors were trained and monitored regularly by the investigators.
Statistical Data Analysis
The response options for knowledge and practice items were binary. Likert-style responses were used for attitude questions. The Statistical Package for Social Sciences (SPSS 23.0, USA) was used to enter and analyze data. One-way ANOVAs were used to compare the mean scores and assess the relationship between independent variables and knowledge, attitude, and practice of patients on AMR and use. The Chi-square test was used to assess the association between knowledge, attitude, and practice. A multivariate linear regression model was used to identify factors associated with good antibiotic resistance and use knowledge, practice, and attitudes. P-value < 0.05 (two-sided) was used to determine statistical significance. Finally, the analyzed data were organized and presented in the appropriate tabular, graphical, and narrative formats.
Ethical Consideration
Ethical clearance was obtained from the Research and Ethical Review Board of Bahir Dar University College of Science with reference number PGRCSVD/17/2019. Moreover, written informed consent was obtained from all patients and all research was performed following relevant guidelines/regulations.
Results
Socio-Demographic Characteristics of Patients
Two hundred and thirty-two patients completed the survey and only one patient did not complete and it was rejected from the analysis. Analysis of demographic parameters showed that the majority of the participants were male (63.4%), married (59.5%), and at the age of 31–45 years (36.2%). Among the 232 respondents who determined their level of education, 36.6% were uneducated. Most participants were orthodox (92.2%) and 31% were farmers (Table 1).
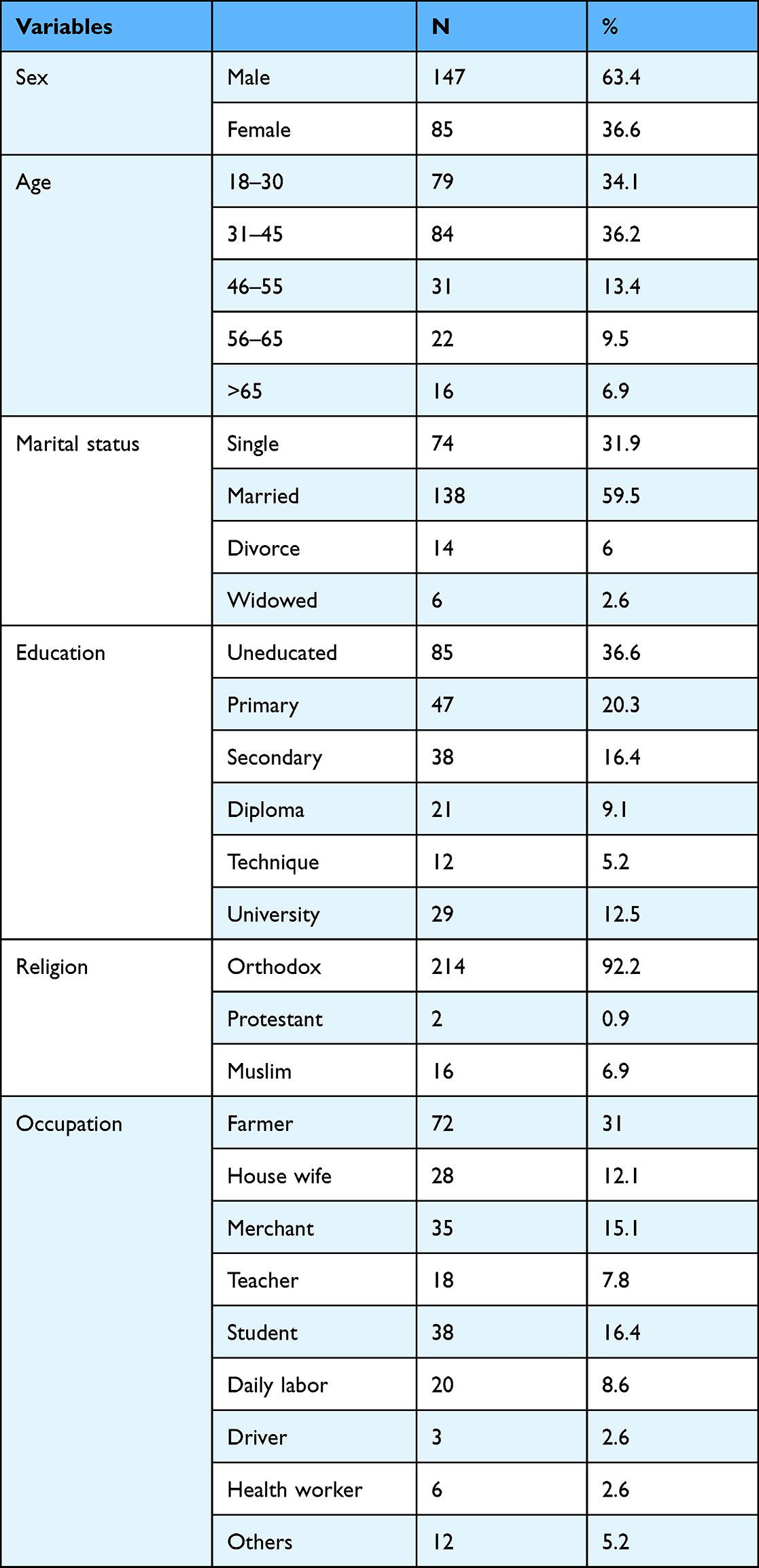 |
Table 1 Demographic Characteristics of Patients (n=232) |
Patients Information on Antibiotics, Antibiotic Resistance, and Uses
As the result shown in Table 2, all the respondents (100%) were taken antibiotics to treat different diseases from different sources and 60.3% of them bought their antibiotics from a private pharmacy without a prescription. It was found that 47.9% of patients took antibiotics more than 5 times in the 12 months before the study. A large proportion of patients (69.8%) heard about antibiotics and antibiotic resistance from different sources and 37.5% of patients heard this information from doctors and nurses (Table 2).
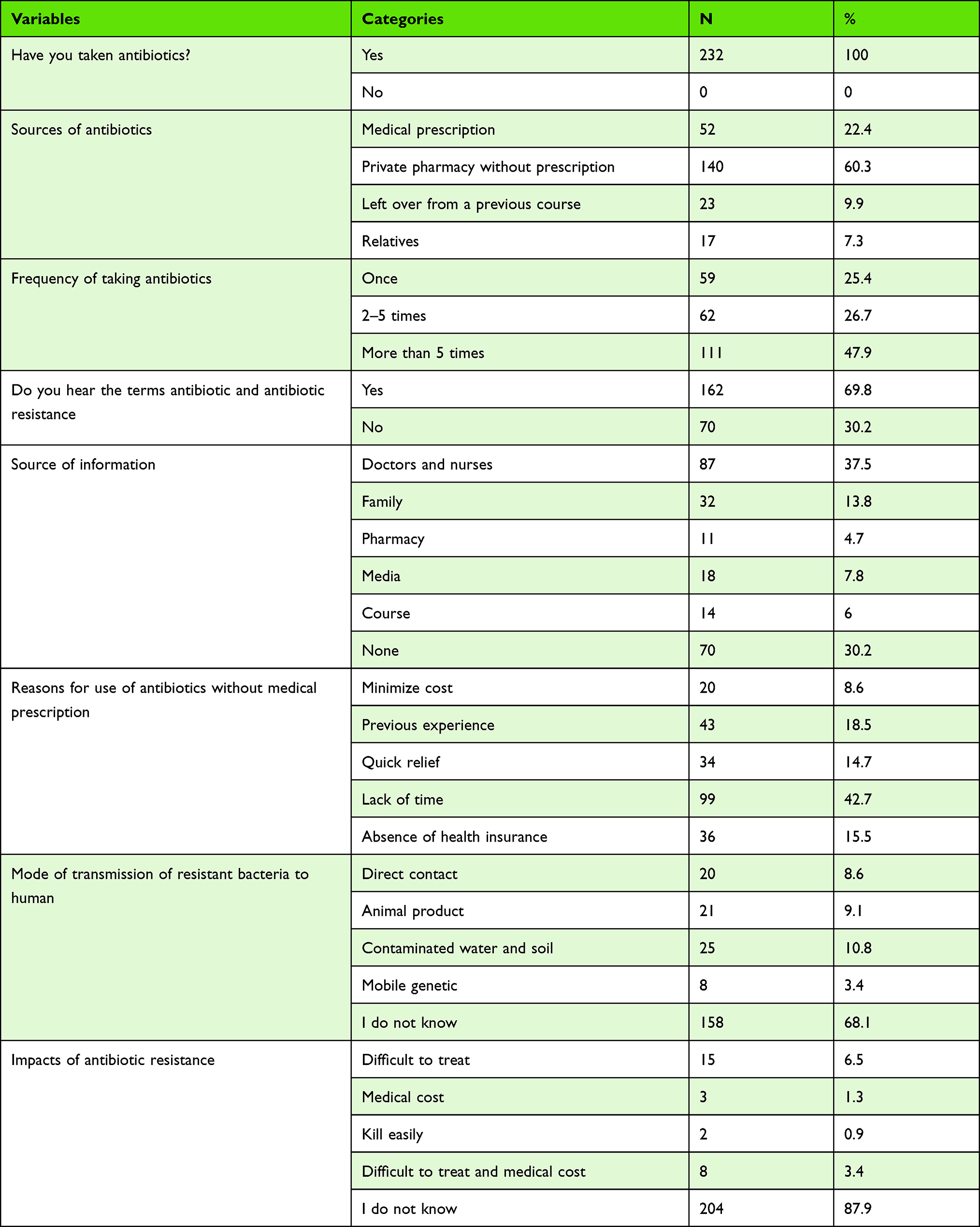 |
Table 2 Patients Information on Antibiotics, Antibiotic Resistance and Uses |
When patients in the study area were asked to answer the question of why they were using antibiotics without prescription, most of the respondents (42.7%) said that they were lack time to be examined by doctors. From the survey, it was found that 10.8% of the respondents responded that the main mode of transmission of resistant bacteria to humans was through the contaminated water and soil, while 68.1% of the respondents did not know any factors that contribute to the transmission of resistant bacteria to humans (Table 2).
Patients in the study area were asked if they knew any possible impacts of antibiotic resistance on human and animals’ health and 6.5% of respondents said that difficult to treat disease caused by resistant microorganisms was the possible impact of AMR. On the other hand, 87.9% of respondents did not know the impact of antibiotic resistance on human and animals health (Table 2). Most of the respondents could mention the brand or generic name of at least one antibiotic that they had been used to treat diseases. Ampicillin (70.7%), ciprofloxacin (59.9%), and tetracycline (57.8%) were the most frequently used groups of antibiotics (Figure 2).
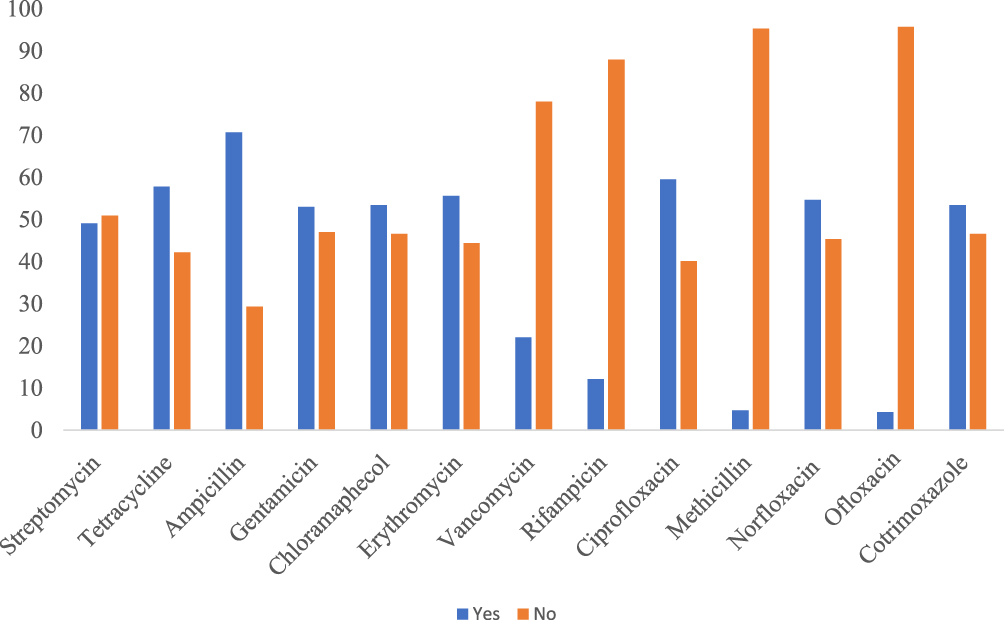 |
Figure 2 Common antibiotics used by patients. |
Knowledge, Attitudes and Practice of Patients on Antibiotic Resistance and Uses
As indicated in Table 3, the highest number of participants (59.9%) were responded to the statement that antibiotics are useful in fighting bacterial infections correctly, while the least number of participants (40%) were responded to the statement improper use of antibiotics can cause antibiotic resistance correctly. The total mean score for correctly answered knowledge questions was 3.15± 0.08 with a maximum score of 6 points. 87 participants (37.5%) scored mean and above the mean were considered to have adequate/better knowledge, while 145 (62.5%) scored below the mean and were considered to have poor knowledge. The mean knowledge scores of our study significantly correlated with the level of education and occupation of respondents (Table 4).
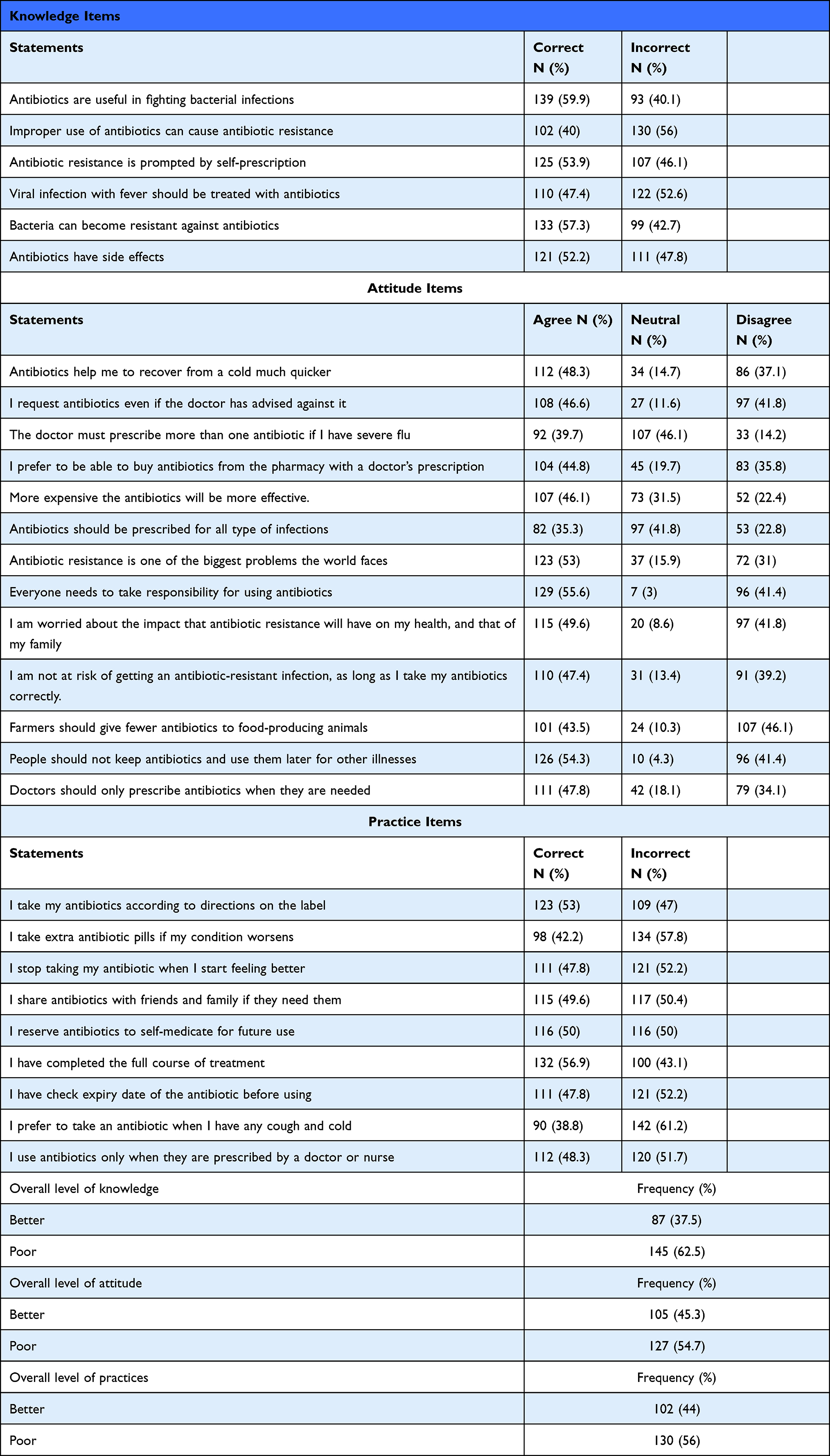 |
Table 3 Knowledge, Attitude and Practice of Patients on Antimicrobial Resistances and Use in Amhara Regional State, North Western Ethiopia (n = 232) |
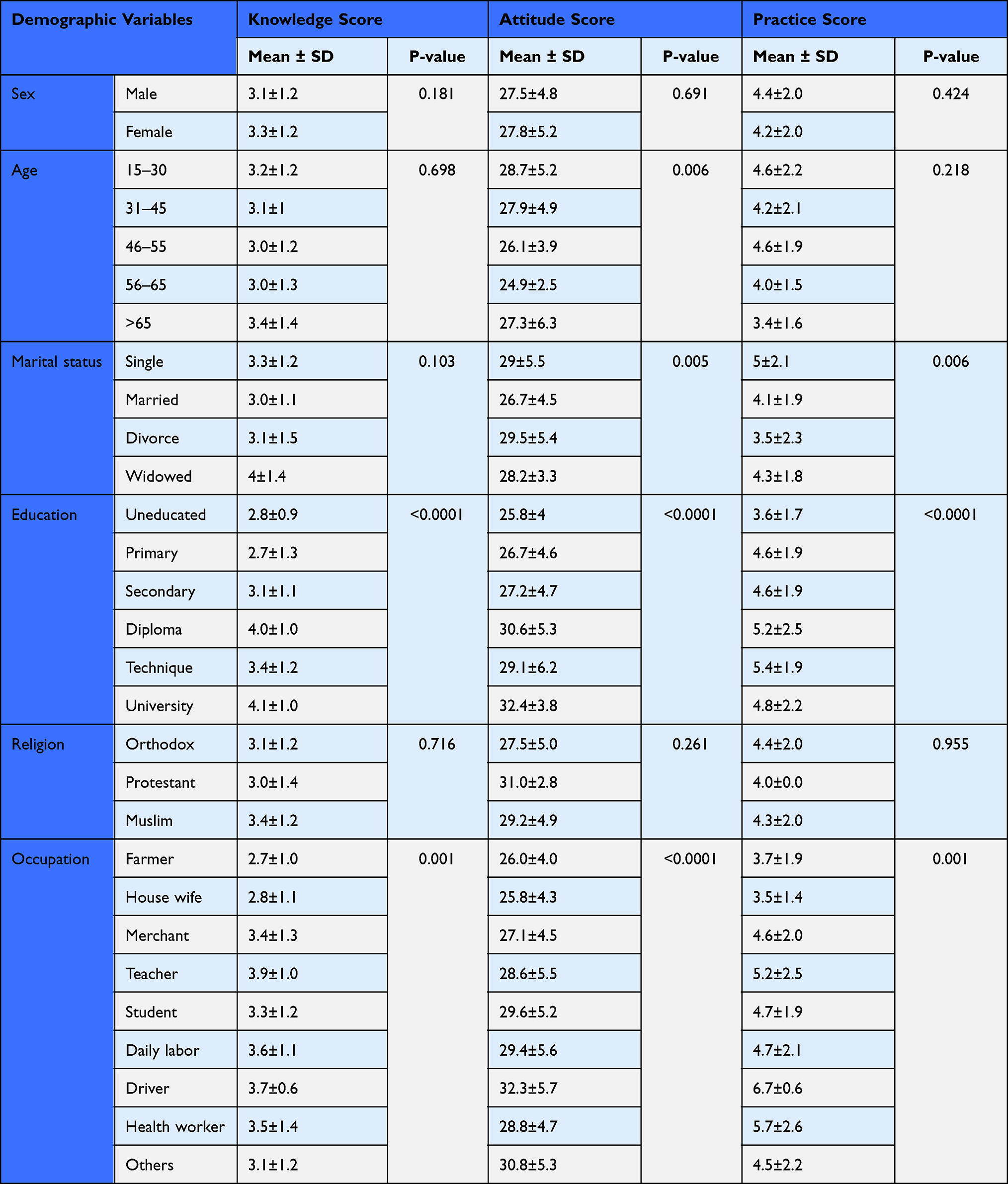 |
Table 4 Relation Between Participants’ Characteristics and Knowledge, Attitude and Behavior About Antibiotic Resistance and Use |
Regarding attitude, the majority 129 (55.6%) of the respondents strongly agreed that everyone needs to take responsibility for using antibiotics and the highest number of respondents 118 (50.9%) disagree on farmers should give fewer antibiotics to treat food-producing animals. The mean score of the participant’s attitude was 27.6 ± 0.3 with the maximum score of 39 points. Participants who scored below the mean score were 127 (54.7%) which was considered poor attitude) and above and equal to the mean score were 105 (45.3%) which was considered a good attitude) (Table 3). The mean attitude of our study was significantly varied across age groups, marital status, levels of education, and occupation (Table 4).
As shown in Table 3, 131 (56.5%) was responded correctly to the statement I have completed the full course of treatment while the least number of participants 90 (38.8%) was responded correctly to the statement I prefer to take an antibiotic when I have any cough and cold. The mean score of the participant’s practice was 4.34 ± 0.13 with a maximum score of 9 points. Participants who scored below the mean score were 130 (56%), which was considered to have poor practice) and above or equal to the mean score of 102 (44%) which was considered to have good practice) (Table 3). Practice scores significantly varied across marital status, levels of education, and occupation (Table 4).
Multiple linear regression analysis demonstrated that education levels were positively correlated with increased levels of knowledge, attitude, and practice on antibiotic use and resistance (P < 0.05). Patients who had a higher level of education(university) had 0.303 times better knowledge (95% C.I: 0.2˗0.41), 1.1 times positive attitude (95% C.I: 0.64˗1.5) and 0.23 times good practice than uneducated patients (95% C.I: 0.04˗0.42) (Table 5).
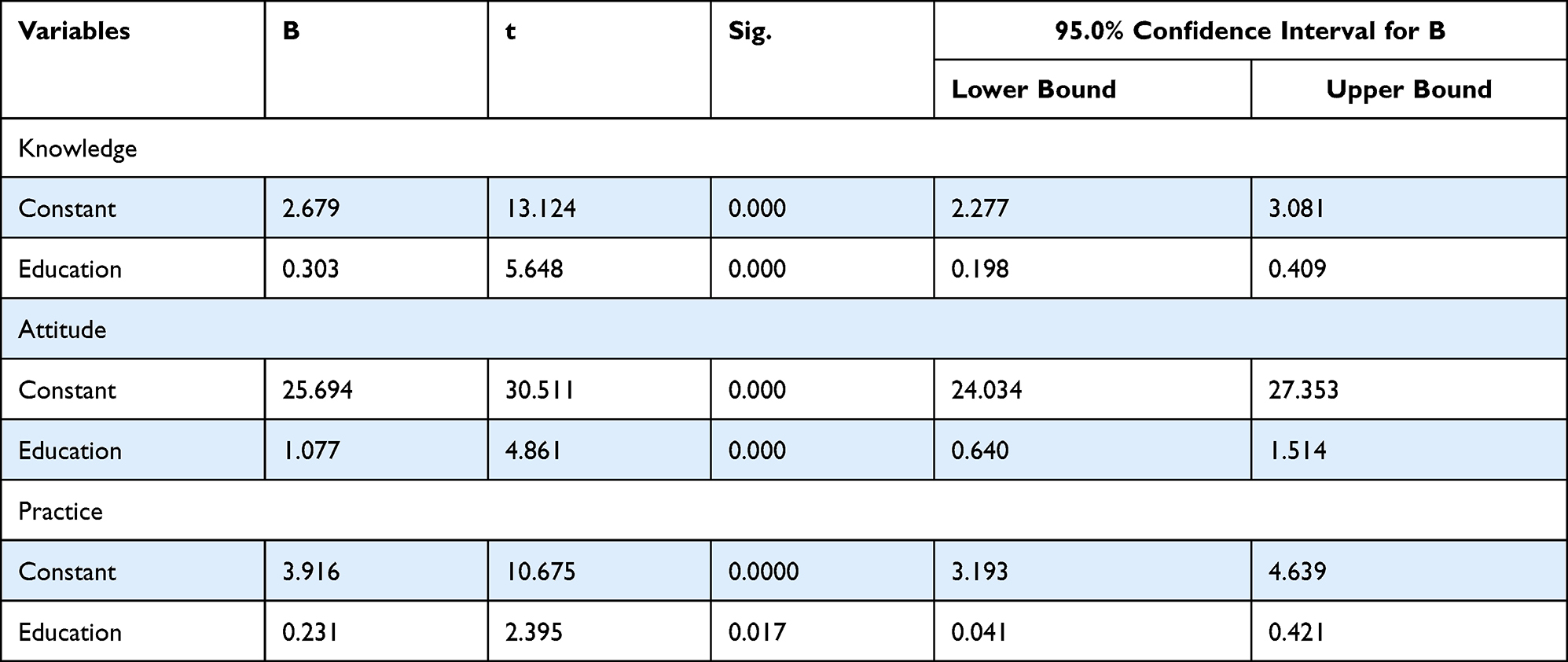 |
Table 5 Multiple Linear Regression Analyses for Predicting Score of Knowledge, Attitude & Practice |
Pearson’s correlation was used to assess the bivariate relationship between KAP scores. Among KAP scales there were positive and strongest correlations between knowledge and attitude (0.246) while practice was not significantly correlated with knowledge and attitude (Table 6).
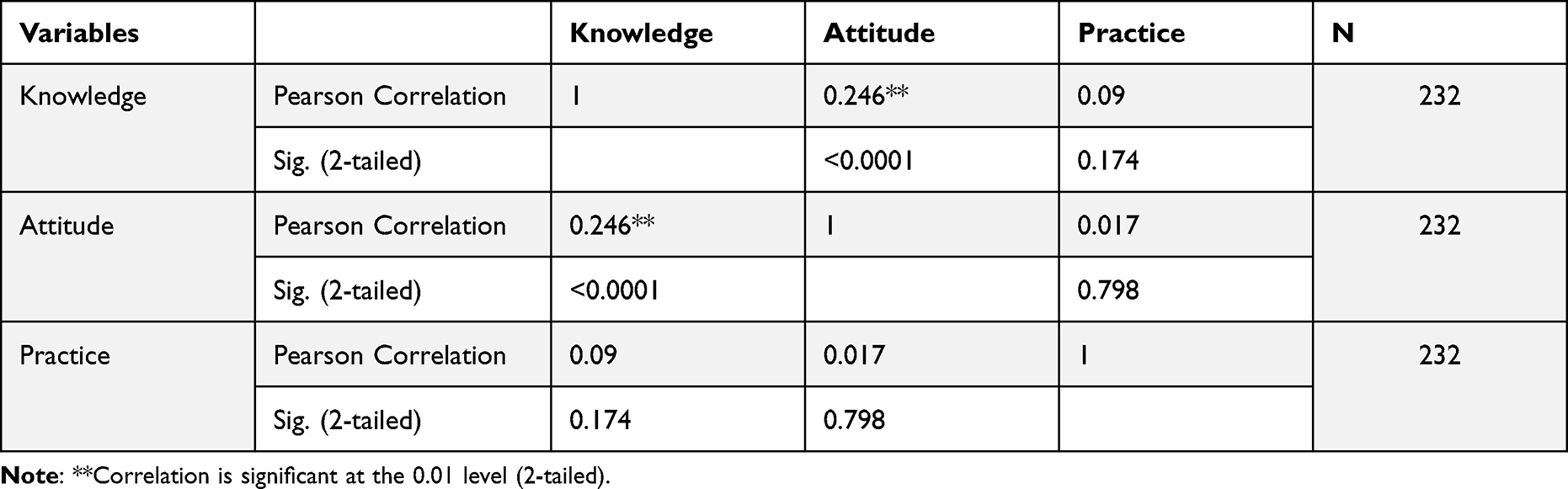 |
Table 6 Correlation Between KAP |
Factors that Contribute to Increasing Antibiotic Resistance
Although most factors were significantly perceived by the majority of respondents as important factors that contribute to increasing antibiotic resistance, poor handwashing practice in hospitals (57.3%), poor awareness of AMR (56%), use of antimicrobial for animal growth promotion (55.2%), lack of rapid and effective diagnostic techniques (54.3%) and substandard quality of antibiotics (53.4) were the most important factors. On the other hand, 58.6% perceived that widespread or overuse of antibiotics in agriculture were not the main factor that contributes to increasing antibiotic resistance (Table 7).
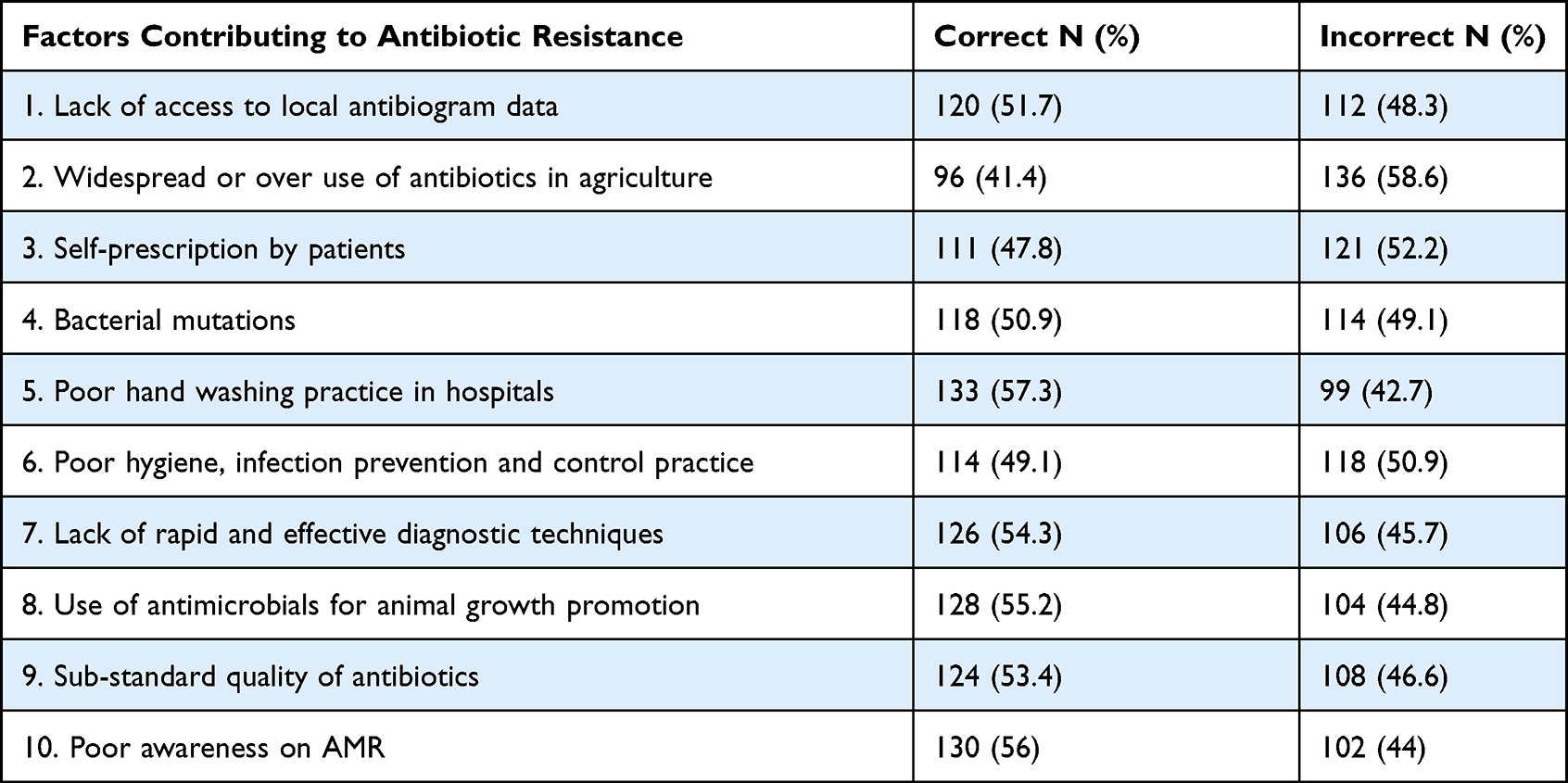 |
Table 7 Factors that Contribute to Increasing of Antibiotic Resistance |
Interventions that Contribute to Reducing Antibiotic Use and Resistance
Although most strategies were perceived by the majority of respondents as important strategies that contribute to reducing antibiotic use and resistance, implementing hygiene, infection prevention, and control practices (59.9%), developing institutional guidelines for antimicrobial use (57.8%), governments should reward the development of new antibiotics (57.8%), proper isolation of the patient (57.3%) and increasing the use of complementary treatments (56.9%) were the most important strategies. In contrast, 59.9% of the respondents perceived that reduction of antibiotic use in the outpatient setting was not the main strategy that contributes to the reduction of antibiotic resistance (Table 8).
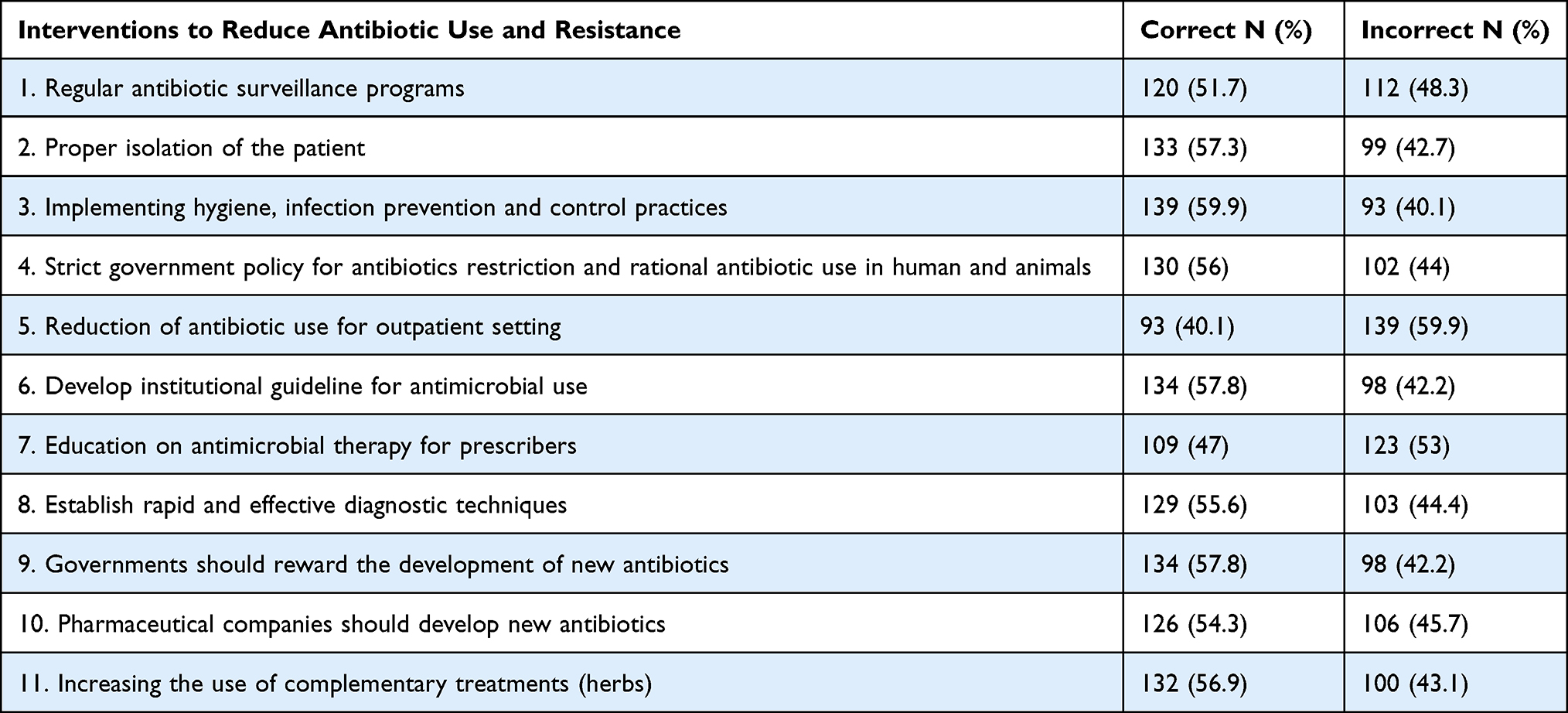 |
Table 8 Interventions that Contribute to Reduce Antibiotic Use and Resistance |
Discussion
Inappropriate antibiotic use can have adverse consequences on various levels. Knowledge, attitude, and practice of patients on drug-related issues can greatly influence the way drugs like antibiotics are used. Assessment of public use of such drugs may provide valuable information that could help toward developing interventions targeting to enhance the utilization of antibiotics.
In this study, all patients used antibiotics to treat different diseases from different sources. The majority (60.3%) of the respondents bought their antibiotics from a private pharmacy without a prescription, some of them (22.4%) provided from health institutions with a medical prescription, and others obtained the antibiotics from relatives and previously stored in their house. A significant variation was observed among the literature regarding the use of antibiotics without prescription. For example, about 76% of antibiotic use without prescription was reported in India,20 72% in Ghana,21 32.7% in Italy,22 28.8% in Saudi Arabia23 and 9% in Hong Kong.6 This difference could be due to variation of regulation and its enforcement from one area to another and knowledge, attitude, and practice of the communities. The results demonstrate the necessity for appropriate public education on the aim and action of antibiotics.
In the current study, all the patients reported that they use antibiotics a minimum of once within the 12 months before the study. This report is comparable to a study done in Namibia (80%).24 However, it is more than the study done in Lithuania 24.9%,25 in Ireland 39%26 and in Bahir Dar 35.9%.27 Many factors might be attributed to the difference seen, including the pattern of disease prevalence within the given area, data collection area, and period.
It was found that a large proportion of patients 69.8% participating in the survey was heard about antibiotics and antibiotic resistance from different sources. Most respondents heard this information from doctors and nurses (37.5%), whereas 30.2% of respondents did not hear the information from any sources. A study done in Nepal reported that only 16% of the patients had heard about different terms for antibiotics and most of them (5.6%) heard about AMR and its related terms from media (newspaper, TV, radio).28
According to the current study results, the most common reasons for using antibiotics without prescription by patients were lack of time to be examined by doctors, lack of health insurance, previous experience to use the antibiotics, minimize cost, and get quick relief from their diseases. Several studies have reported different reasons for self-medication, including non-seriousness of the illness,29–33 saving time,30–32 cost-effectiveness,31–33 ease of accessibility.30,33,34
From the survey, it has been found that most of the patients did not know any factors that were contributing to the transmission of resistant bacteria to humans, and some patients listed that contaminated water and soil, consumption of animal products, direct contact between humans and animals and mobile genetic material were the factors responsible for the transmission of resistant bacteria to humans. Most of the patients also did not know the impact of antibiotic resistance on human and animals’ health and others mentioned that difficult to treat disease caused by resistant microorganisms, high medical costs, and kill patients easily were possible impacts of antibiotic resistance on humans and animals’ health.
Most of the respondents were ready to mention the brand or generic name of a minimum of one antibiotic that they had been will not treat diseases. Ampicillin, ciprofloxacin and tetracycline were the most frequently used groups of antibiotics. The foremost common antibiotic used by the participants was amoxicillin, followed by ciprofloxacin and norfloxacin, respectively.35
This study has shown many misconceptions about antibiotic use and resistance. 47.4% of respondents correctly thought that viral infection with fever should not be treated with antibiotics. Different results were found in studies conducted in several countries. For instance, about 42.2% of respondents in Iraq reported antibiotics do not treat viral infections,36 29.8% in Kuwait,9 17.0% in Malaysia,37 65% in the USA,38 73.2% in Sweden39 and 66.4% of the population thought that antibiotics are effective against cold or cough in Saudi Arabia.40 This difference might be because of the variation in socio-demographic factors, regulation from one area to another and its enforcement, knowledge, attitude, and practice of the communities’.
The current study revealed that 59.9% of respondents reported antibiotics are useful in fighting bacterial infections. This finding is lower than the different studies conducted in Iraq 91.6%,36 Kuwait 66.5%,9 Malaysia 78.3%,37 USA 90.0%38 and Sweden 77.2%.39 A study conducted in India reported that more than half of the participants believed that antibiotics are not safe to use and can have possible adverse effects35 supports the current study, which stated that 52. 2% of respondents reported antibiotics to have side effects. In a similar study, it was found that nearly half of the participants believed that antibiotic does not cause side effects.37 In another study, more than two-thirds of the participants believed that antibiotics can have allergic reactions.41
Furthermore, 57.3% of respondents said that bacteria can become resistant to antibiotics. A similar study was conducted in Iraq36 and Sweden39 was found that 73.4 and 80.7% of respondents reported that bacteria could resist antibiotics, respectively. In this study, only 40% of participants agreed that improper use of antibiotics could lead to antimicrobial resistance. This finding is lower than the study done in Harar (78.3%),42 in Bahir Dar (71.4%),33 Namibia (72%),24 and Jordan (50%).43 The current study revealed that 87 (37.5%) of patients were classified as having adequate/better knowledge which is lower than results reported by Ramchurren et al44 who stated that 205 (53%) patients were classified as having good knowledge based on the scoring. The difference seen could be due to socio-demographic and setting differences.
Regarding the attitude, 54.3% of patients strongly agreed that people should not keep antibiotics and use them later for other illnesses. It is better than a study by Pechere et al a higher rate of wrong belief among the public was reported with 62% believing that leftover antibiotics can be saved and used again.45 A study conducted in the United Kingdom also identified a good number of respondents reported to have kept antibiotics for future use.46 Furthermore, studies conducted by Lim and Teh37 and Pavydė et al25 reported that 17% and 28.5% of respondents kept antibiotics in their homes for future use, respectively.
It is found that 105 (45.3%) of patients have adequate/better attitudes which are lower than the result reported by those who stated that than over half the sample (n = 211, 55%) of patients were classified as having good attitudes towards antibiotic use.44 The participants within this study had a low attitude score, thus it is evidence that the public holds inappropriate beliefs concerning antibiotic use, which could adversely affect the way they are used. Public education is the best way to overcome such incorrect beliefs. It is reasonable to involve strict regulatory control to make sure that antibiotics are not dispensed by pharmacists without a prescription.
Regarding the practice of patients, the current study indicated that 43.1% of the respondents have not completed the full course of treatment. In the study conducted in the UK, only 11% reported not having finished their last antibiotic course as prescribed.46 In this study, 49.6% of the participants reported that they shared antibiotics with friends and family if they need them, which was higher than other studies.42,47 A good percentage of respondents in the study in Oman was reported of exhibiting the unhealthy practice of sharing antibiotics with other members of the family or friends, which could result in the misuse of antibiotics.48 A study conducted in South Africa reported that 230 (60%) patients were classified as having good antibiotic practices44 which higher than the current study (44%).
In addition, the current study showed that the majority of the respondents perceived most of the factors as important factors that contribute to increasing antibiotic resistance, such as poor awareness of AMR, use of antimicrobial for animal growth promotion, lack of rapid and effective diagnostic techniques and substandard quality of antibiotics were the most important factors. In contrast, the majority of respondents (58.6%) perceived that widespread or overuse of antibiotics in agriculture were not the main factor that contributes to increasing antibiotic resistance.
Moreover, although the majority of respondents perceived most strategies as important strategies that contribute to reducing antibiotic use and resistance, implementing hygiene, infection prevention, and control practices, developing institutional guidelines for antimicrobial use, governments should reward the development of new antibiotics, proper isolation of the patient and increasing the use of complementary treatments (herbs) were the most important strategies. In contrast, most of the respondents supposed that reduction of antibiotic use in the outpatient setting was not the main strategy that contributes to the reduction of antibiotic resistance.
Our finding showed that there were positive and strongest correlations between knowledge and attitude which indicated that knowledge is one of several determinants of attitude. Knowledge–attitude-behavior models have theorized that knowledge is one determinant of attitude and increased knowledge is likely to lead to attitudes that are more stable and resistant to negative changes.49 The only socio-demographic factor found to be associated with knowledge, attitudes and practices relating to antibiotic use was education. Respondents with higher education had better knowledge and more appropriate attitudes and practices, a finding consistent with other studies.6,50–53 Similar observations were also reported in studies conducted in Malaysia, Palestine, and Hong Kong, which demonstrated that patients with higher levels of education were more likely to have good antibiotic knowledge and positive attitudes toward antibiotic usage.6,52,54
Limitation of the Study
The major limitation of this study was the relatively small number of participants selected from three cities of northwestern Ethiopia which might not reflect the real situation of KAP of patients in Ethiopia as a whole. In addition, the cross-sectional study design can influence the cause and effect relationship of the predictor variables and the dependent variables (knowledge, attitude, and practice) of the patients. Lack of previous related studies led the discussion looks repetition of the results particularly on possible impacts of antibiotic resistance, the main mode of transmission of resistant bacteria to humans, important factors that contribute to increasing antibiotic resistance, and important strategies that contribute to reducing antibiotic use and resistance.
Conclusion
The study’s findings revealed a knowledge gap, negative attitudes, and malpractice in the use of antimicrobial and resistance, which will hasten antimicrobial resistance development. Therefore, awareness creation programs should be planned to improve the community’s knowledge, attitude, and practice of appropriate antimicrobial use and measures should be taken to eliminate the practice of dispensing antimicrobial without prescription.
Abbreviations
KAP, Knowledge, Attitude and Practice; WHO, World Health Organization; AMU, Antimicrobial Use; AMR, Antimicrobial Resistance; ANOVAs, Analysis of Variance.
Data Sharing Statement
Please contact the author for data requests.
Ethics Approval and Consent to Participate
This study was approved by the Research and Ethical Review Board of Bahir Dar University College of Science with reference number PGRCSVD/17/2019. Moreover, all respondents were aware of the purpose of this study, consented to participate in the survey and this study was conducted following the Helsinki declaration.
Acknowledgments
The authors would like to thank all patients who participated in this study and data collectors. The authors would like to thank Mr. Gashaw Molla for his support to prepare the map of the study area and Mr. Teshager Zerihun for his support in data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any grant funds.
Disclosure
The authors declare that they have no competing interests.
References
1. Dellit TH, Owens RC, Mcgowan JE, et al. Infectious diseases society of America and the society for healthcare epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(15):159–177.
2. World Health Organization. Antimicrobial resistance global report on surveillance; 2014.
3. World Health Organization. The Evolving Threat of Antimicrobial resistance: options for action. World Health Organization; 2012.
4. Cosgrove SE. The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin Infect Dis. 2006;42:s82–s89. doi:10.1086/499406
5. Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340(7756):1120. doi:10.1136/bmj.c2096
6. You JHS, Yau B, Choi KC, Chau CTS, Huang QR, Lee SS. Public knowledge, attitudes and behavior on antibiotic use: a telephone survey in Hong Kong. Infection. 2008;36(2):153–157. doi:10.1007/s15010-007-7214-5
7. Elberry AA, Shaikh A, Al-Marzouki J, Fadul R. Evaluation of non-prescribed antibiotic use among children with upper respiratory tract infection. Int Res J Pharm Pharmacol. 2012;2(6):147–152.
8. Okeke IN. Poverty and root causes of resistance in developing countries. In: Antimicrobial Resistance in Developing Countries. New York: Springer; 2010:27–35. doi:10.1007/978-0-387-89370-9
9. Awad AI, Aboud EA. Knowledge, attitude and practice towards antibiotic use among the public in Kuwait. PLoS One. 2015;10(2):e0117910. doi:10.1371/journal.pone.0117910
10. Dhadwal DSA. Knowledge, attitudes and behaviour towards antibiotic usage and its resistance among the general public of Shimla city: a pilot study. Int J Com Health and Med Res. 2015;1(1):9–16.
11. Abay SM, Amelo W. Assessment of self-medication practices among medical, pharmacy, and health science students in Gondar University, Ethiopia. J Young Pharm. 2010;2(3):306–310. doi:10.4103/0975-1483.66798
12. Eticha T, Mesfin K. Self-medication practices in Mekelle, Ethiopia. PLoS One. 2014;9(5):e97464. doi:10.1371/journal.pone.0097464
13. Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerg Infect Dis. 1999;5(1):18–27. doi:10.3201/eid0501.990103
14. Mendelson M, Precious Matsotso M. Antimicrobial resistance national strategy framework, 2014–2024 in AMR CONTROL. Association with the world alliance against antibiotic resistance; 2015:54–61. Available from: www.globalhealthdynamics.co.uk.
15. Björkman I, Erntell M, Röing M, Lundborg CS. Infectious disease management in primary care: perceptions of GPs. BMC Fam Pract. 2011;12. doi: 10.1186/1471-2296-12-1
16. Daniel WW, Cross CL. Biostatistics a Foundation for Analysis in the Health Sciences. Tenth. John Wiley & Sons, Inc; 2013.
17. World Health Organization. Antibiotic resistance: multi-country public awareness survey; 2015. Available from: www.who.int.
18. Geta K, Kibret M. Knowledge, attitudes and practices of animal farm owners/workers on antibiotic use and resistance in Amhara region, north western Ethiopia. Sci Rep. 2021;11(1). doi:10.1038/s41598-021-00617-8
19. Wangmoi K, Dorji T, Pokhrel N, Dorji T, Dorji J, Tenzin T. Knowledge, attitude, and practice on antibiotic use and antibiotic resistance among the veterinarians and para-veterinarians in Bhutan. PLoS One. 2021;16(5). doi:10.1371/journal.pone.0251327
20. Saleem M, Sheikuduman T, Gopinath C. Assessment of public knowledge and attitude regarding antibiotic use in a tertiary care hospital. Asian J Pharm Clin Res. 2016;9(1):83–87.
21. Tagoe DNA, Attah CO. A study of antibiotic use and abuse in Ghana: a case study of the cape coast metropolis. Internet J Health. 2012;11(2). doi:10.5580/bec
22. Napolitano F, Izzo MT, Di Giuseppe G, Angelillo IF. Public knowledge, attitudes, and experience regarding the use of antibiotics in Italy. PLoS One. 2013;8(12):e84177. doi:10.1371/journal.pone.0084177
23. Aldhafar AS, Talat W. Knowledge, attitude, and practice toward the usage of antibiotics among public in Al-Ahsa, Saudi Arabia. Int J Sci Study. 2017:11. doi:10.17354/ijss/2017/39
24. Pereko DD, Lubbe MS, Essack SY. Public knowledge, attitudes and behaviour towards antibiotic usage in Windhoek, Namibia. S Afr J Infect Dis. 2015;30(4):134–137. doi:10.1080/23120053.2015.1107290
25. Pavydė E, Veikutis V, Mačiulienė A, Mačiulis V, Petrikonis K, Stankevičius E. Public knowledge, beliefs and behavior on antibiotic use and self-medication in Lithuania. Int J Environ Res Public Health. 2015;12(6):7002–7016. doi:10.3390/ijerph120607002
26. Shebehe J, Ottertun E, Carlén K, Gustafson D. Knowledge about infections is associated with antibiotic use: cross-sectional evidence from the health survey Northern Ireland. BMC Public Health. 2021;21(1). doi:10.1186/s12889-021-11018-x
27. Gebeyehu E, Bantie L, Azage M. Inappropriate use of antibiotics and its associated factors among urban and rural communities of Bahir Dar city administration, northwest Ethiopia. PLoS One. 2015;10(9):e0138179. doi:10.1371/journal.pone.0138179
28. Rijal KR, Banjara MR, Dhungel B, et al. Use of antimicrobials and antimicrobial resistance in Nepal: a nationwide survey. Sci Rep. 2021;11(1). doi:10.1038/s41598-021-90812-4
29. Shafie M, Eyasu M, Muzeyin K, Worku Y, Martín-Aragón S. Prevalence and determinants of self medication practice among selected households in Addis Ababa community. PLoS One. 2018;13(3):e0194122. doi:10.1371/journal.pone.0194122
30. Tesfamariam S, Anand IS, Kaleab G, et al. Self-medication with over-the-counter drugs, prevalence of risky practice and its associated factors in pharmacy outlets of Asmara, Eritrea. BMC Public Health. 2019;19(1). doi:10.1186/s12889-019-6470-5
31. Lei X, Jiang H, Liu C, Ferrier A, Mugavin J. Self-medication practice and associated factors among residents in Wuhan, China. Int J Environ Res Public Health. 2018;15(1):68. doi:10.3390/ijerph15010068
32. Kassie AD, Bifftu BB, Mekonnen HS. Self-medication practice and associated factors among adult household members in Meket district, Northeast Ethiopia, 2017. BMC Pharmacol Toxicol. 2018;19(1). doi:10.1186/s40360-018-0205-6
33. Tesfaye Z. Patient knowledge and practice on antimicrobial use and resistance in Felege Hiwot hospital, Bahir Dar, Ethiopia. J Basic Clin Pharma. 2017;8:S010–S015.
34. Al-Ghamdi S, Alfauri TM, Alharbi MA, et al. Current self-medication practices in the Kingdom of Saudi Arabia: an observational study. Pan Afr Med J. 2020;37(51):1–16. doi:10.11604/pamj.2020.37.51.24098
35. Jain A, Dhir S, Batta M, Singh G. Knowledge and practices in community regarding antibiotic usage. Int J Res Med Sci. 2016;4(2):610–614. doi:10.18203/2320-6012.ijrms20160325
36. Al-Yasseri BJH, Hussain NA. Public knowledge and attitudes towards antibiotics use and resistance in Baghdad, Iraq: a survey conducted in outpatient department of university teaching hospital. Open Public Health J. 2020;12(1):567–574. doi:10.2174/1874944501912010567
37. Lim KK, Teh CC. A cross sectional study of public knowledge and attitude towards antibiotics in Putrajaya, Malaysia. South Med Rev. 2012;5(2):26–33.
38. Carter RR, Sun J, Jump RLP. A survey and analysis of the American public’s perceptions and knowledge about antibiotic resistance. Open Forum Infect Dis. 2016;3(3). doi:10.1093/ofid/ofw112
39. André M, Vernby Å, Berg J, Lundborg CS. A survey of public knowledge and awareness related to antibiotic use and resistance in Sweden. J Antimicrob Chemother. 2010;65(6):1292–1296. doi:10.1093/jac/dkq104
40. Abujheisha KY, Al-Shdefat R. Public knowledge and behaviours regarding antibiotics use: a survey among the general public view project. Int J Med Res Health Sci. 2017;6(6):82–88.
41. Widayati A, Suryawati S, de Crespigny C, Hiller JE. Knowledge and beliefs about antibiotics among people in Yogyakarta City Indonesia: a cross sectional population-based survey. Antimicrob Resist Infect Control. 2012;1(38):38. doi:10.1186/2047-2994-1-38
42. Jifar A, Ayele Y. Assessment of knowledge, attitude, and practice toward antibiotic use among Harar city and its surrounding community, Eastern Ethiopia. Interdiscip Perspect Infect Dis. 2018;2018:1–6. doi:10.1155/2018/8492740
43. Darwish DA, Abdelmalek S, Abu Dayyih W, Hamadi S. Awareness of antibiotic use and antimicrobial resistance in the Iraqi community in Jordan. J Infect Dev Ctries. 2014;8(5):616–623. doi:10.3855/jidc.4086
44. Ramchurren K, Balakrishna Y, Mahomed S. Patients’ knowledge, attitudes and practices regarding antibiotic use at a regional hospital in KwaZulu-Natal, South Africa 2017. S Afr J Infect Dis. 2018;1–6. doi:10.1080/23120053.2018.1516393
45. Pechère JC, Hughes D, Kardas P, Cornaglia G. Non-compliance with antibiotic therapy for acute community infections: a global survey. Int J Antimicrob Agents. 2007;29(3):245–253. doi:10.1016/j.ijantimicag.2006.09.026
46. McNulty CAM, Boyle P, Nichols T, Clappison P, Davey P. The public’s attitudes to and compliance with antibiotics. J Antimicrob Chemother. 2007;60(SUPPL. 1):i63–i68. doi:10.1093/jac/dkm161
47. Tenaiji A, Al Redha K, Khatri F, et al. Knowledge, attitudes and behavior towards antibiotic use among parents in Al-Ain City, United Arab Emirates. Int J Infect Dis. 2008;12:e434. doi:10.1016/j.ijid.2008.05.1271
48. Jose J, Jimmy B, Al Gahliya Mohammed Saif AlSabahi G, Al Sabei A. A study assessing public knowledge, belief and behavior of antibiotic use in an Omani population. Oman Med J. 2013;28(5):324–330.
49. Fabrigar LR, Petty RE, Smith SM, Crites SL. Understanding knowledge effects on attitude-behavior consistency: the role of relevance, complexity, and amount of knowledge. J Pers Soc Psychol. 2006;90(4):556–577. doi:10.1037/0022-3514.90.4.556
50. Tshokey T, Adhikari D, Tshering T, Wangmo S, Wangdi K. Assessing the knowledge, attitudes, and practices on antibiotics among the general public attending the outpatient pharmacy units of Hospitals in Bhutan: a cross-sectional survey. Asia Pac J Public Health. 2017;29(7):580–588. doi:10.1177/1010539517734682
51. Mouhieddine TH, Olleik Z, Itani MM, et al. Assessing the Lebanese population for their knowledge, attitudes and practices of antibiotic usage. J Infect Public Health. 2015;8(1):20–31. doi:10.1016/j.jiph.2014.07.010
52. Abu Taha A, Abu-Zaydeh AH, Ardah RA, et al. Public knowledge and attitudes regarding the use of antibiotics and resistance: findings from a cross-sectional study among Palestinian adults. Zoonoses Public Health. 2016;63(6):449–457. doi:10.1111/zph.12249
53. Belkina T, Al Warafi A, Hussein EE, Tadjieva N, Kubena A, Vlcek J. Antibiotic use and knowledge in the community of Yemen, Saudi Arabia, and Uzbekistan. J Infect Dev Ctries. 2014;8(4):424–429. doi:10.3855/jidc.3866
54. Oh AL, Hassali MA, Al-Haddad MS, et al. Public knowledge and attitudes towards antibiotic usage: a cross-sectional study among the general public in the state of Penang, Malaysia. J Infect Dev Ctries. 2011;5(5):338–347. doi:10.3855/jidc.1502
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.