Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 12
Knowledge, Attitudes, and Practice Regarding COVID-19 among Patients with Musculoskeletal and Rheumatic Diseases in Nepal: A Web-Based Cross-Sectional Study
Authors Vaidya B ![]() , Bhochhibhoya M
, Bhochhibhoya M ![]() , Baral R
, Baral R ![]() , Nakarmi S
, Nakarmi S ![]()
Received 13 June 2020
Accepted for publication 6 August 2020
Published 21 August 2020 Volume 2020:12 Pages 167—173
DOI https://doi.org/10.2147/OARRR.S265816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Binit Vaidya, Manisha Bhochhibhoya, Rikesh Baral, Shweta Nakarmi
Department of Rheumatology, National Centre for Rheumatic Diseases, Kathmandu, Nepal
Correspondence: Binit Vaidya
Department of Rheumatology, National Centre for Rheumatic Diseases, Ratopul, Kathmandu, Nepal
Tel +977 1-446-4288
Email [email protected]
Purpose: The global health crisis created by coronavirus disease in 2019, ie, COVID-19, is of serious concern to rheumatologists. The relationship of rheumatic diseases, their therapies, and COVID-19 with multiple genuine and malicious information available online can influence the knowledge and attitudes of rheumatic patients. This Google Forms study was conducted to understand the knowledge, attitudes, and practices of rheumatology patients with regard to COVID-19 in Nepal.
Methods: A web-based cross-sectional study was conducted among patients with rheumatic diseases. A modified version of a questionnaire was used after consent had been obtained. It was then translated into Nepali for comprehensibility. The final questionnaire contained a total of 29 questions: six on demographic parameters and twelve, five, and six on knowledge, attitudes and practice, respectively. Simple descriptive statistics were used to describe the positive responses in each domain. Logistic regression analysis was done to observe demographic variables associated with knowledge, attitudes, and practice.
Results: Among 380 participants, 63.2% were female, the majority (42.1%) aged 18– 29 years, and all were literate. Most were aware of the clinical features of COVID-19 (91.6%), 71.5% had positive attitudes toward its control, some (31.5%) thought that they had a greater chance of contracting COVID-19 than others, and 18.9% believed that antirheumatic medications could increase their susceptibility to infection. A majority (> 94.7%) of them practiced preventive measures.
Conclusion: Patients with rheumatic diseases were aware of the general clinical features, routes of transmission, and general preventive measures regarding COVID-19 and did not significantly change their treatment practices.
Keywords: SARS-CoV-2, coronavirus, KAP, survey
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) belongs to the coronavirus family responsible for the 2019 pandemic coronavirus disease 19 (COVID-19), which was first identified in Wuhan, China in December 2019.1,2 According to a recent World Health Organizationreport (May 28, 2020), COVID-19 had been confirmed in 216 countries, with more than 5.5 million positive cases and over 350,000 confirmed deaths.3 This global health crisis created by COVID-19 is of serious concern to rheumatologists. Rheumatic diseases compromise patient immunity, and the use of immunosuppressant drugs further compounds this effect.4 After the first report of SARS-CoV-2 infection from Nepal in a student who returned from Wuhan,5 there has been a rapid implementation of countrywide lockdown and various awareness programs on social media.6
Methods
With the help of Google Forms, a cross-sectional study was conducted using a survey questionnaire to understand the knowledge, attitudes, and practices of rheumatic patients regarding COVID-19 in Nepal during the first week of April 2020.
Study Population
Patients with various rheumatologic diseases (eg, rheumatoid arthritis, systemic lupus erythematosus, fibromyalgia, osteoarthritis, and gout) were selected randomly from the patient registry of the National Centre for Rheumatic Diseases (NCRD), Kathmandu, Nepal, comprising a total of around 22,000 patients. A sample of 384 patients was calculated with an estimated 3 million population with rheumatic diseases where the margin of error was 5%. Considering a 30% response rate, 1,160 patients were invited to participate in the survey. A computer-generated random-number table was used to select survey participants based on their registration number.
Survey Instrument
A survey questionnaire constructed by Zhong et al was modified and translated into Nepali for the study.7 The corresponding author was contacted via email and permission to use the same questions with modification in terms of rheumatic patients obtained. The modified questionnaire was translated into the native language (Nepali) by two independent Nepali-speaking translators. The Nepali version synthesized by these two translators was back-translated to English by two independent translators (one with a master’s degree in journalism with an English major and a postgraduate rheumatology registrar [author MB]). A prefinal Nepali questionnaire was developed after sorting out the differences in understanding of common words after a joint meeting between all four translators and author BV. This prefinal survey instrument was distributed to randomly selected faculty members to assess its comprehensibility and appropriateness (on a score of 0–4) and refinements made as required to facilitate better comprehension and organize the questions before the final version was distributed to the study population. It contained a total of 29 questions: six pertaining to demographic parameters, including the rheumatic disease they were suffering from, twelve to knowledge about the disease, five to attitude, and six to practices. Responses were classified as true, false, or “not sure” in the knowledge and attitude sections. Open-ended questions were not kept to save the time of respondents and reduce dropout rates.8
Procedure
An SMS containing the objective of the study and invitation for participation was sent to each of the selected participants. It mentioned why they were receiving the SMS, and a link to Google Forms was attached in the SMS itself. Assurance of anonymity was mentioned. It was also mentioned that clicking the link implied consent for participation. The link provided was applicable for single use only to avoid multiple entries from the same user. Responses were collected in an Excel sheet.
Ethics
The procedures followed for the study were in accordance with the Declaration of Helsinki. Each participant was informed via SMS that clicking the link would mean implied informed consent for the study. Ethical clearance was obtained from the review board of the National Center for Rheumatic Diseses (NCRD).
Statistical Analysis
All responses were qualitative in nature. Simple descriptive statistics were used to describe the positive responses in each domain. Binary logistic regression analysis was done to observe demographic variables associated with knowledge, attitudes, and practice. SPSS version 21 was used for data analysis, and p≤0.05 was considered significant. Analysis was done to see the difference in responses in relation to education and use of immunosuppressants.
Results
Questionnaire Preparation
All consultants verifying the questionnaire reported good comprehensibility and appropriateness of the final version (score of 2 or 3). Internal consistency between each item of the questionnaire was satisfactory, with Cronbach’s α=0.769.
Survey
A total of 380 patients participated in the survey, the majority being females (63.2%). Around 132 (34.7%) had rheumatoid arthritis, 68 (17.9%) had connective tissue disease, and 40 (10.5%) had spondyloarthropathy requiring treatment with either disease-modifying antirheumatic drugs (DMARDs) or immunosuppressant therapy. The medication being used by the majority (50.5%) was DMARDs (methotrexate and sulfasalazine alone or in combination). Immunosuppressant therapy (cyclophosphamide, mycophenolate mofetil, or azathioprine) and biological agents (adalimumab, etanercept, or tofacitinib) were being used by 7.4% each. Other demographic parameters are mentioned in Table 1.
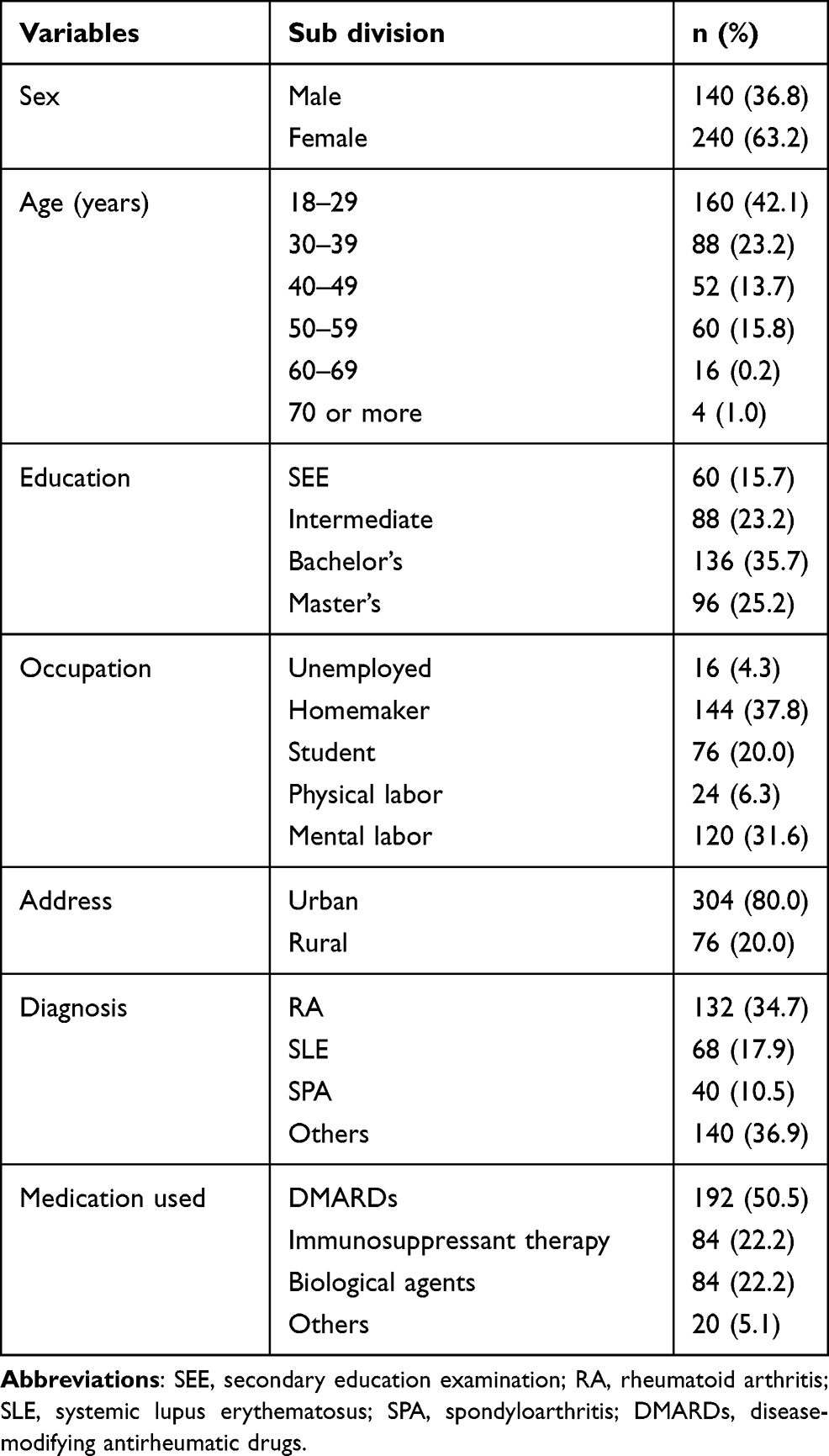 |
Table 1 Demographic Status of the Participants (n=380) |
Knowledge Domain
Most participants were aware of the clinical features, route of transmission, and methods of prevention of COVID-19 (>90%), and 70.6% knew that it could manifest in serious outcomes in patients with comorbidities. Knowledge results for participants regarding COVID-19 infection is given in Table 2, and was acceptable for most questions.
 |
Table 2 Knowledge regarding COVID-19 among participants (n=380) |
Attitude Domain
A positive attitude toward control of COVID-19 was seen in a majority (71.5%). A good proportion of participants (31.5%) thought that they had a greater chance of getting COVID-19 than the general population because of their comorbidity (rheumatic disease), and 18.9% believed that the antirheumatic medications they were taking could increase their susceptibility to infection. Responses on the attitude domain are given in Table 3.
 |
Table 3 Attitudes toward COVID-19 among patients (n=380) |
Practice Domain
Preventive measures like wearing a mask (94.7%) and avoiding public or crowded places (97.9%) were practiced by an acceptable proportion of participants, while 13.6% of patients reduced the dose of their DMARDs on their own and few admitted stopping medication for fear of infection (4.2%) or unavailability of medicine due to lockdown (8.4%). Details are given in Table 4. There was no difference in attitude or practice changes between higher and lower education (p=0.969 and 0.643, respectively). Also, no difference was observed between those using and not using DMARDs and immunosuppressants in knowledge of symptoms (p=0.196), risk of infection (p=0.607), or change in dose or discontinuation of medication (p=0.746). Binary logistic regression analysis did not show significant relationships between demographic variables like sex (p=0.669), education (p=0.891), or use of immunosuppressants (p=0.860) on responses to knowledge-, attitude-, and practice-related questions.
 |
Table 4 Practice and behavior of participants regarding COVID-19 (n=380) |
Discussion
This study found an acceptable level of knowledge among patients with rheumatic diseases regarding the symptoms of COVID-19 infection and measures required for prevention of transmission. Since the first case of SARS-CoV-2 was reported in February from Nepal, after almost 3 months of the beginning of the epidemic in Wuhan, China, we assume that most of the patients had had enough time to get acquainted with general precautionary measures.9 From 1,160 invitations, only 380 participated in this web-based survey. A majority of the participants (42%) were aged 18–29 years. This might be explained by easy access to internet services and ease of use for the younger generation. This was a web-based survey, but notably only 51.15% of Nepalese use the internet,10 which is mostly concentrated in urban Nepal. Most of these patients with easy access and internet use would also have access to various online information regarding prevention, symptoms, and recent updates regarding COVID-19, hence the higher percentage of correct responses in the domains of knowledge and attitude.11,12
There are limited sources of information regarding the risks of infection due to rheumatic disease and severity of illness. Any viral infection can have an aggressive course leading to severe disease manifestations and respiratory complications in immunocompromised patients. The true incidence of COVID-19 in patients with rheumatic disease has been reported not to be much higher than the nonrheumatic population. Also, the natural history of COVID-19 in these patients is not much different, with very few cases of severe disease reported in patients receiving biological or target-specific agents. These data still would be considered inadequate for any definite recommendation to be made. This study also shows a level of uncertainty in our patients with rheumatic disease, with around a third of patients responding that they felt that they were at increased risk of infection with SARS-CoV-2 due to their disease. A few patients also opted to reduce the dose of their medications, but this practice was not influenced by their use of DMARDs or immunosuppressants. Various societies have given directives that a reduction or withdrawal of DMARDs is not warranted prophylactically, because of the risk of flare of the underlying disease, which might increase the need for steroids instead.13 Such a reduction or withdrawal might be considered in those with symptomatic infections only.
Some commonly used drugs like hydroxychloroquine might have some role in inhibition of SARS-CoV-19 by interfering with the glycosylation of cellular receptors and increasing endosomal pH required for viral fusion.14 Some guidelines have recommended hydroxychloroquine’s use for prophylaxis and treatment of COVID-19 infection. This might lead to a false sense of security and irresponsible high-risk practice among patients taking these medications. A report suggested that there might be zero protective role of hydroxychloroquine, as 25% of rheumatic patients using this drug had concomitant COVID-19 infections.15 In contrast to our expectations, only 13.7% of patients considered their medications to have a protective effect, while 86.3% denied or were unsure of this theory. Along with hydroxychloroquine, some studies have shown that medications like JAK inhibitors, IL-1 inhibitors, IL-6 inhibitors, and some intravenous immunoglobulins might have protective actions in COVID-19 infection.16
Routine vaccination against pneumonia and flu is recommended before initiation of any DMARDs. However, in low- to middle-income countries like Nepal, this practice is seldom followed. As there was an increasing trend of self-seeking of flu vaccination during the swine- and bird-flu epidemics, we also surveyed a change in this practice in our patients after the COVID-19 outbreak. The majority (96.9%), however, denied changing their behavior regarding vaccination practice.
Nepal being in stage 3 of the COVID-19 epidemic, this knowledge regarding general symptoms, transmission, and preventive measures in patients with rheumatic disease should be considered acceptable. However, the findings of this survey highlight caveats in certain aspects of knowledge of our rheumatic patients, and it would thus be helpful to design awareness programs. Future web-based studies should include patient attitudes toward herd immunity, as this provides indirect protection from infection. In cases of SARS-Cov-2, development of herd immunity may be difficult to achieve simultaneously in all geographic regions. Furthermore, long-term natural immunity to this virus is not certain. As such, the development of a vaccine is of great importance for the control and prevention of the disease outbreak.17
Conclusion
Patients with rheumatic diseases were aware of the general clinical features, route of transmission, and general preventive measures regarding COVID-19. However, there was a significant lack of knowledge regarding susceptibility stratification and recommendations for prevention among those using DMARDs.
Ethical Approval and Informed Consent
Each participant was informed via SMS that clicking the link would mean implied informed consent for the study. Ethical clearance was obtained from the review board of the National Center for Rheumatic Diseases (NCRD).
Acknowledgments
We thank all patients who participated in the study. We would also like to thank Mr Sunil Bajimayo (preparation of Google Forms and handling the technical elements) and Miss Rakshya Joshi and Ms Sujana Kapali (for translation of the questionnaire).
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Naming the coronavirus disease (COVID-19) and the virus that causes it: World Health Organization (WHO). Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it.
2. WHO. Novel Coronavirus – china [Internet]; 2020. Available from: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/.
3. WHO. Coronavirus disease (COVID-19) outbreak situation. Available from: https://www.who.int/docs/defaultsource/coronaviruse/situationreports/20200409-sitrep-80-covid-19.pdf?sfvrsn=1b685d64_2.
4. Wiseman AC. Immunosuppressive medications. Clin J Am Soc Nephrol. 2016;11(2):332–343. doi:10.2215/CJN.08570814
5. Shrestha R, Shrestha S, Khanal P, Kc B. Nepal’s first case of COVID-19 and public health response. J Travel Med. 2020;27(3):taaa024. doi:10.1093/jtm/taaa024
6. Piryani RM, Piryani S, Shah JN. Nepal’s response to contain COVID-19 infection. J Nepal Health Res Counc. 2020;18(1):128–134. doi:10.33314/jnhrc.v18i1.2608
7. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
8. Crawford SD, Couper MP, Lamias MJ. Web surveys: perceptions of burden. Soc Sci Comput Rev. 2001;19(2):146–162. doi:10.1177/089443930101900202
9. Asim M, Sathian B, van Teijlingen E, Mekkodathil A, Subramanya SH, Simkhada P. COVID-19 pandemic: public health implications in Nepal. Nepal J Epidemiol. 2020;10(1):817–820. doi:10.3126/nje.v10i1.28269
10. Nepal telecommunications authority. MIS report [Internet]. Kathmandu; 2019. Available from: https://nta.gov.np/en/mis-reports/.
11. Kathmandupost. At Covid-19 helpline, thousands of calls from Nepalis looking for accurate information. 2020/3/17; 2020. Available from: https://kathmandupost.com/national/2020/03/17/at-covid-19-helpline-thousands-of-calls-from-nepalis-looking-for-accurate-information.
12. WHO. covid19nepal; 2020. Available from: https://www.who.int/nepal/covid19nepal.
13. Tam L-S, Tanaka Y, Handa R, et al. Care for patients with rheumatic diseases during COVID-19 pandemic: a position statement from APLAR. Int J Rheum Dis. 2020;23(6):717–722. doi:10.1111/1756-185X.13863
14. Wang M, Cao R, Zhang L, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30(3):269–271. doi:10.1038/s41422-020-0282-0
15. Parperis K. To consider or not antimalarials as a prophylactic intervention in the SARS-CoV-2 (COVID-19) pandemic. Ann Rheum Dis. 2020;
16. UNLo M A study to evaluate the safety and efficacy of tocilizumab in patients with severe COVID-19 pneumonia (COVACTA); 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT04320615.
17. Papachristodoulou E, Kakoullis L, Parperis K, Panos G. Long-term and herd immunity against SARS-CoV-2: implications from current and past knowledge. Pathog Dis. 2020;78(3). doi:10.1093/femspd/ftaa025
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.