Back to Journals » Advances in Medical Education and Practice » Volume 16
Knowledge Attitudes and Ethical Concerns About Artificial Intelligence Among Medical Students at Taibah University: A Cross-Sectional Study
Authors Alfahl S ![]()
Received 16 April 2025
Accepted for publication 7 August 2025
Published 1 September 2025 Volume 2025:16 Pages 1609—1620
DOI https://doi.org/10.2147/AMEP.S528281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sateesh Arja
Samah Alfahl
Department of Family and Community Medicine, College of Medicine, Taibah University, Madinah, Saudi Arabia
Correspondence: Samah Alfahl, Email [email protected]
Background: Artificial Intelligence (AI) is increasingly relevant tool to medical education and healthcare. Understanding the readiness of future physicians for AI integration is essential for developing effective curricula and fostering responsible use of this technology.
Methods: This cross-sectional study was conducted among 189 medical students at Taibah University using a validated, self-administered online questionnaire. The tool measured AI knowledge (7 items), attitudes (10 items), practices (7 items), and perceived barriers. Responses were captured on a 5-point Likert scale. Descriptive and inferential statistics, including one-way ANOVA, were used to analyze differences across academic years.
Results: Out of 189 respondents, 53.97% (n=102) of students reported familiarity with basic AI concepts, and 5.66% (n=11) were aware of machine learning and deep learning. Only 11.21% (n=21) had received formal AI instruction, and 21.18% (n=40) had attended dedicated courses. 74.60% (n=141) believed AI would revolutionize education, yet 41.91% (n=79) expressed concerns about AI replacing teachers. 52.02% (n=98) used AI regularly for exam preparation. In comparison, only 11.64% (n=22) used it for Objective Structured Clinical Examination (OSCE) preparation Key barriers included ethical concerns (n=44 responses), risk of plagiarism (n=56), lack of knowledge (n=46), and limited access to tools (n=28).
Conclusion: Medical students display cautious optimism about AI in education, with limited practical knowledge and concerns about ethical implications. Integrating structured AI education, training program, and ethical guideline is essential for preparing students for an AI-enhanced healthcare landscape.
Keywords: medical education, AI literacy, student attitudes, technology in healthcare, educational barriers
Introduction
(AI) which can emulate human intelligence through learning, problem solving, adaptation, and even creative expression, has become deeply integrated into numerous sectors.1,2 The influence of AI extends from finance to healthcare, driving innovation and shaping personalized experiences. A remarkable aspect of AI is its ability to recognize patterns, enabled by machine learning (ML). (ML) enables machines to analyze extensive datasets more efficiently than humans, leading to revolutionary advancements such as autonomous driving and personalized medicine.3
Deep learning (DL), a subset of (ML), utilizes complex neural networks inspired by the human brain, significantly transforming image-based diagnostics.4 This has resulted in notable successes, including the detection of lung cancer, osteoarthritis, and oral diseases. Despite these advancements, the widespread adoption of AI has raised substantial ethical concerns. UNESCO is developing a global framework to guide the ethical application of AI, address potential risks, and safeguard human rights and dignity.5,6 A critical concern is AI’s impact on education, particularly for students pursuing healthcare careers. AI-powered platforms offer personalized learning experiences; however, concerns exist about students’ overreliance on AI, which may impair their deep understanding of the subject matter. Studies suggest that AI may reduce students’ enthusiasm for specific medical specialties, such as radiology, highlighting the need for more resources and research into the role of AI in medical education and training.7,8
This study, which was conducted among medical students at Taibah University, aims to evaluate their knowledge, attitudes, and perceptions regarding AI in their educational journeys.9 The findings indicate a significant gap in AI knowledge and practical application among students. While there is general awareness of AI basics, understanding specific applications within their fields remains limited, suggesting a disconnect between theory and practice. Formal AI education is scarce, and concerns about the ethical implications and potential job impact of AI are prevalent.10 Although AI is considered a valuable educational tool, its role in medical practice elicits excitement and apprehension. There is cautious optimism about AI’s potential to revolutionize education, but concerns persist regarding these issues.11,12 Furthermore, AI is frequently used for exam preparation and multiple-choice question generation. However, its adoption for personal development and specific tasks such as OSCE preparation is limited, indicating a need for further exploration and research.13
Addressing these barriers requires a multifaceted approach; to address concerns about cheating and privacy, clear ethical guidelines for using AI in education must be developed.7 Access to training programs and technical resources must be provided to bridge the knowledge gap. AI must be incorporated into existing curricula, and collaborative learning environments must be facilitated to create more effective learning opportunities. Innovative approaches to integrate AI into educational settings without increasing workload are essential.14
Numerous studies have shown that AI may dampen students’ enthusiasm for pursuing specific medical specialties, such as radiology. Moreover, global resources for understanding AI’s implications in medical education are limited, particularly in the Middle East.15 This study seeks to assess the knowledge, attitudes, and perceptions of medical students at Taibah University regarding AI, to understand its potential benefits, challenges, and associated ethical considerations. The findings provide valuable insights into AI adoption in medical education at Taibah University, identifying opportunities for improvement and highlighting crucial areas for further research and development.
The central research problem addressed in this study is the gap in AI knowledge and practical application among medical students. This study seeks to answer the following specific questions: What is the current level of understanding among medical students about different types of AI, including generative AI and predictive modeling? How do medical students perceive the benefits and challenges of incorporating AI into their educational journey? What are AI’s ethical considerations and potential impacts on future healthcare professionals? How can AI be effectively integrated into medical education without diminishing students’ enthusiasm for their chosen specialties? This study is significant because it explores the under-researched area of AI’s impact on medical education, particularly in the context of the Middle East. By identifying the knowledge gaps and apprehensions among medical students, this research aims to provide insights that can inform the development of AI-integrated curricula and training programs. The findings contribute to the broader discourse on AI in education, highlighting the need for a balanced approach that maximizes the benefits of AI while addressing its ethical and practical challenges.
Methodology
Study Design and Setting
This cross-sectional study employed a questionnaire-based approach to assess medical students’ knowledge, attitudes, and practices regarding AI at Taibah University, Saudi Arabia. The study was conducted between January and February 2024, following approval from the Institutional Review Board (IRB registration: IORG0008716-IRB00010413) at Taibah University’s College of Medicine. All procedures adhered to the principles of the Declaration of Helsinki.
Validation of the Measurement Tool
The questionnaire used in the study has been previously published.15 In this study, some questions were added, which were then validated by the ethical committee at Taibah University. Questionnaire was pilot tested on 15 students from different level to assess clarity, relevance, and timing and based on there feedback minor change made to improve it. The reliability scores (Cronbach’s alpha) for each section, except demographics, are reported as follows: knowledge of AI (α = 0.82), attitudes toward AI applications (α = 0.85), AI practices (α = 0.80), and barriers to using AI (α = 0.77).
Questionnaire Structure
The questionnaire consisted of five sections: (1) Demographics, (2) Knowledge of AI (7 questions), 3. Attitudes toward AI applications (10 questions), 4. AI practices (7 questions), 5. Barriers to using AI. Each section utilized a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). Example questions include “I am familiar with the basic concepts of AI” for the knowledge section and “AI can significantly improve medical diagnostics” for the attitude section.
Sample Size and Distribution
A sample size of 189 was determined via a sample size calculator, assuming a total medical student population of 600 at Taibah University. The effect size, alpha level, and power value used to calculate the sample size are reported in the methodology. The samples were drawn to represent different cohorts, and details on the random selection process and sample size for each cohort were provided. The sample sizes were balanced as much as possible to ensure representativeness. The questionnaire was distributed via social media platforms. Students were approached through official university channels and personal networks. No incentives were provided for participation, ensuring that responses were voluntary and unbiased.
Statistical Analysis
The statistical analysis of the data was conducted via GraphPad Prism 10. Descriptive statistics (means, standard deviations, frequencies) were used to summarize the demographics and survey responses, whereas inferential statistics, including one-way ANOVA, were used to examine group differences. However, before conducting ANOVA, assumptions of independence, normality, and homogeneity of variance were checked. If these assumptions were not met, alternative statistical methods were considered, and the rationale for their use is discussed in the results section. The analysis also revealed potential differences between cohorts based on their year in the medical program. These cohorts were purposefully selected to ensure diverse representation across different levels of training. The sample sizes for each cohort were approximately equal, and the rationale for cohort selection is provided in the study’s design.
Results
Illustration
The survey consisted of three parts. The first part of the AI consisted of seven questions that asked about participants’ knowledge and expertise with AI, with responses recorded as either “yes” or “no”. The second part consisted of ten questions that explored participants’ beliefs about the role of AI in healthcare and education, with responses recorded as “agree”, “disagree” or “neutral”. The final part contained nine questions regarding participants’ frequency of AI usage for various purposes, with responses recorded as “all the time”, “often”, or “never”. The results are presented in three stacked bar graphs.
Statistical Analysis
A one-way ANOVA was conducted to investigate potential differences in responses across years of study. The student cohort was stratified based on their year of study, and their responses to survey questions were categorized as “agree”, “disagree”, and “neutral” for questions 8–17 and “all the time”, “often”, and “never” for questions 18–26. A comparison of responses within each year group for each question was performed, and the mean and median values were visualized. Statistically significant correlations, indicated by asterisks (*), were determined with a p-value threshold of 0.05. One asterisk signifies a significant relationship, whereas four asterisks (****) represent a highly significant correlation.
The pie chart in Figure 1 illustrates the distribution of students’ perceived familiarity with AI. Nearly half of the respondents (49%) reported being “familiar to some degree”, while 43% indicated that they were “very familiar” with AI. A smaller proportion (8%) reported that they were “not familiar” with AI. These findings suggest a generally high level of AI awareness among the surveyed students, with a minority lacking exposure or understanding.
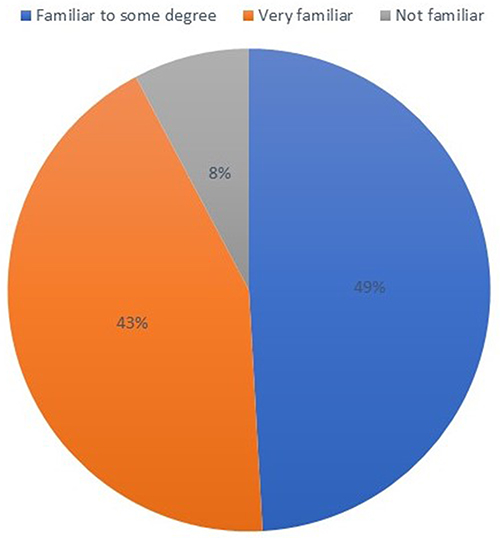 |
Figure 1 Self-reported familiarity with artificial intelligence (AI) among medical students at Taibah. |
The survey revealed a concerning gap in knowledge and experience with AI among the respondents, as depicted in Figure 2. While a majority (53.97%) reported solid knowledge of AI basics (Q1), this understanding appears to dwindle as the questions delve deeper into practical applications. A significant proportion (75.66%) of the respondents indicated familiarity with deep learning and machine learning (Q2), suggesting an essential awareness of these fundamental AI concepts. However, knowledge about specific AI applications within their fields of interest was significantly lower (40.03%, Q3). This disparity highlights a disconnect between theoretical understanding and the practical implementation of AI. Only a tiny percentage of respondents (11.21%, Q5) reported being taught AI during their undergraduate studies, and even fewer (21.18%, Q4) had attended dedicated AI courses. This limited formal exposure may have contributed to the knowledge gap observed in the survey.
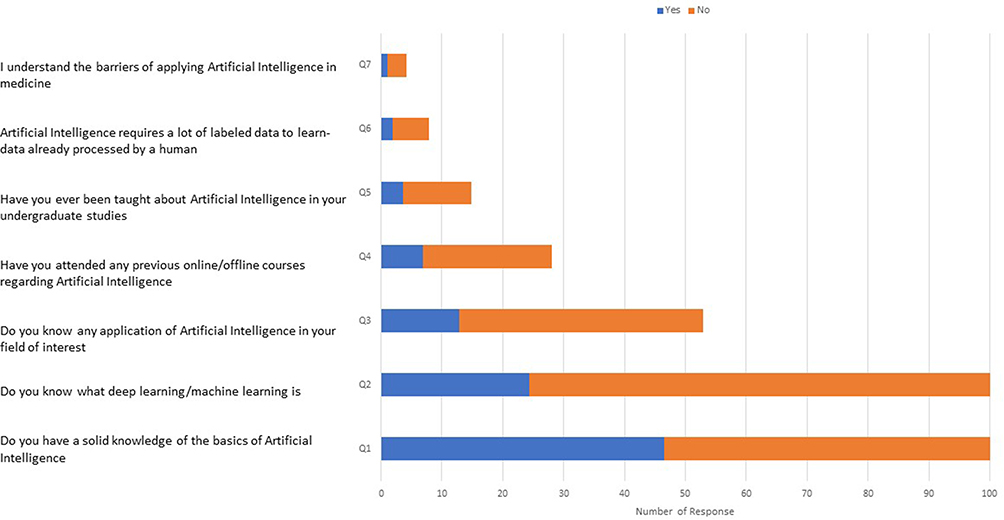 |
Figure 2 Knowledge-related responses to artificial intelligence (AI) among medical students at Taibah University. The horizontal stacked bar chart displays the number of “Yes” (blue) and “No” (Orange) responses to seven AI-related knowledge questions (Q1–Q7). |
The survey also revealed a low level of understanding regarding the barriers to applying AI in medicine (3.14%, Q7). This suggests a lack of awareness about the challenges and considerations in integrating AI into healthcare settings. Figure 3 illustrates the responses to questions 1–7 (Q1- Q7) provided by medical students at Taibah University, segmented by their respective years of study. The bar graphs depict the responses for each question, with error bars representing the standard error of the mean for each year group. Statistically significant differences between groups (p < 0.05) are indicated by asterisks (*).
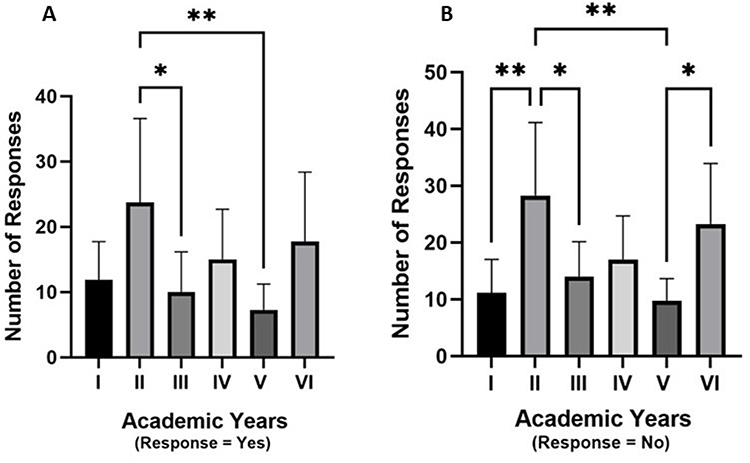 |
Figure 3 Responses to AI knowledge-related questions among medical students stratified by academic year I to VI. The figure presents students’ responses categorised as (A) Yes and (B) No, to AI knowledge and familiarity items. (A) Second-year students reported the highest number of affirmative (“Yes”) responses, with significant differences observed between second- and third-year students (p < 0.05) and second- and fifth-year students (p < 0.01), indicating greater AI awareness or exposure in earlier academic years. (B) “No” responses were highest among second-year and sixth-year students, with statistically significant differences seen between first- and second-year students (p < 0.01), second- and third-year students (p < 0.05), second- and fifth-year students (p < 0.01), and second- and sixth-year students (p < 0.05), suggesting a divergence in perceived or actual knowledge levels across cohorts. Error bars represent the standard error of the mean (SEM). Significance levels: * p < 0.05, ** p < 0.01. |
While respondents strongly believe healthcare students should learn about AI (Q8), with 68.78% strongly agreeing or agreeing, opinions about AI’s impact on medical practice are more nuanced. A majority (57.77%) are optimistic about AI surpassing human physicians in terms of accuracy (Q15), but a significant proportion (46.48%) are concerned with AI replacing certain medical specialties (Q16). Additionally, nearly 40% (38.25%) believe that AI increases diagnostic errors (Q17), highlighting skepticism about its reliability in medical diagnosis. This suggests that while AI is seen as a valuable tool for healthcare education, its role in actual medical practice remains a source of excitement and apprehension. The survey revealed mixed perspectives on the role of AI in education. While a significant majority (74.60%) believe that AI will revolutionize education (Q11), reflecting optimism about its potential to transform learning processes, a notable proportion (41.91%) are apprehensive about human teachers being replaced by AI (Q12), highlighting concerns about the impact on traditional teaching roles. However, the respondents also strongly believed (56.61%) that AI advancements would be exciting for the educational system (Q13), suggesting an overall positive anticipation of future developments. This suggests cautious optimism about AI in education, with excitement about its potential benefits tempered by concerns about its possible impact on human roles. The survey strongly recognized the need for ethical considerations in AI development and implementation (71.48%, Q10), as represented in Figure 4.
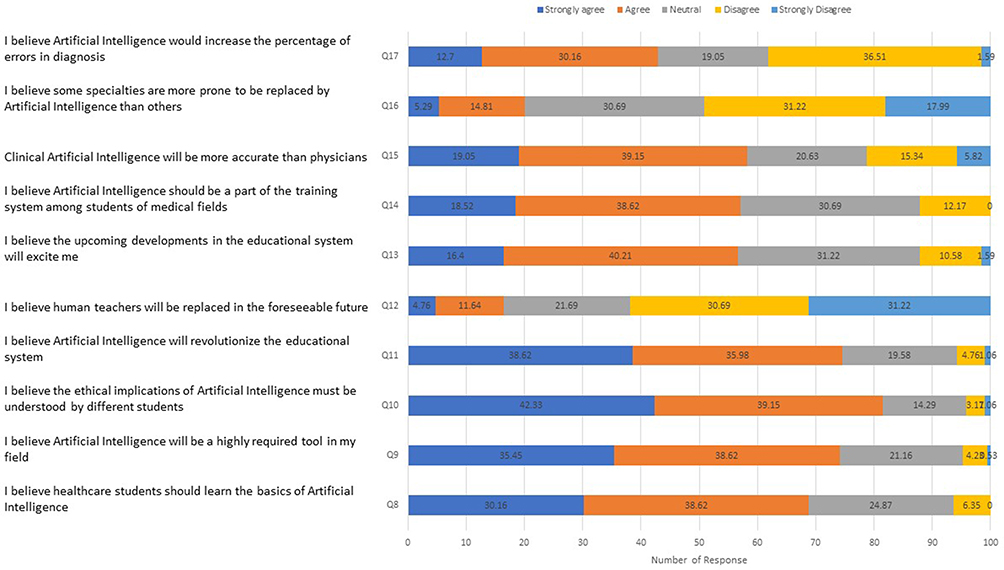 |
Figure 4 Attitudinal responses toward artificial intelligence (AI) among medical students at Taibah University. The horizontal stacked bar chart shows the distribution of students’ responses across ten attitude-related statements regarding AI. Responses were captured using a 5-point Likert scale: “Strongly agree” (dark blue), “Agree” (Orange), “Neutral” (grey), “Disagree” (yellow), and “Strongly disagree” (light blue). |
Figure 5 illustrates the distribution of responses to questions 8–17 (Q8- Q18) among Taibah University medical students, categorized by their year of study. The analysis of the “agree” responses in Figure 5A revealed a trend of increasing agreement with the statements as the students progressed through their medical education. First-year students differed significantly from second-year students in their level of agreement, suggesting that exposure to the medical curriculum influenced their perspective. Second-year students exhibited a highly significant correlation with fifth- and third-year students, indicating greater convergence of viewpoints as they gained further experience. Furthermore, a significant difference was observed between the responses of fifth-year and sixth-year students, suggesting a potential shift in perception as they approached the end of their medical training. Figure 5B, which focused on “neutral” responses, presented a different trend. First-year students’ responses significantly differed from those of second-year students, indicating a potential shift in their willingness to remain neutral on the issues. Second-year responses, however, strongly aligned with the responses of third-, fourth-, and fifth-year students, suggesting convergence toward a more neutral stance. Interestingly, a less significant correlation was observed between second-year and sixth-year responses, implying that while there might be some shared neutrality among these groups, it is not as pronounced as the correlation between second-year students and their earlier peers. Interestingly, Figure 5C, which shows “disagree” responses, did not reveal any statistically significant differences between medical students’ responses from different years.
 |
Figure 5 Number of responses to questions among medical students at Taibah University, categorized by year of study. The responses are categorized into three levels: (A) Agree, (B) Neutral and (C) Disagree. (A) Second-year students reported the highest level of agreement across AI-related statements, with statistically significant differences observed between multiple academic years, including first- and second-year students (p < 0.01), second- and third-year students (p < 0.001), and second- and fifth-year students (p < 0.0001). Sixth-year students also demonstrated significantly higher agreement levels than first-year students (p < 0.01). (B) Neutral responses showed a distinct pattern, with second-year students again exhibiting significantly different response patterns compared to first-year (p < 0.0001), third-year (p < 0.001), fourth-year (p < 0.0001), and fifth-year (p < 0.01) students. A modest but significant difference was also observed between second and sixth-year students (p < 0.05). (C) No statistically significant differences were found in the “Disagree” responses across academic years, indicating a more evenly distributed pattern of disagreement. Error bars represent the standard error of the mean (SEM). Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001. |
Figure 6 illustrates the responses where respondents reported using AI most frequently to prepare for examinations (Q18), with over half (52.02%) employing it “all the time” or “most of the time”. AI was also frequently used to suggest multiple-choice questions (Q19) and prepare for homework assignments (Q21), with over 40% using it regularly. However, AI’s use for preparing for the OSCE examination (Q20) was significantly lower, with only 11.64% using it “all the time” or “most of the time”. AI was moderately used for conducting research (Q22) and for idea generation and brainstorming (Q23), with approximately 30% using it regularly. The survey revealed limited use of AI for personal choices and career guidance (Q24), spelling and grammar checking (Q25), and personality development (Q26). This suggests that while AI is becoming increasingly integrated into academic tasks, its application for personal development remains less common.
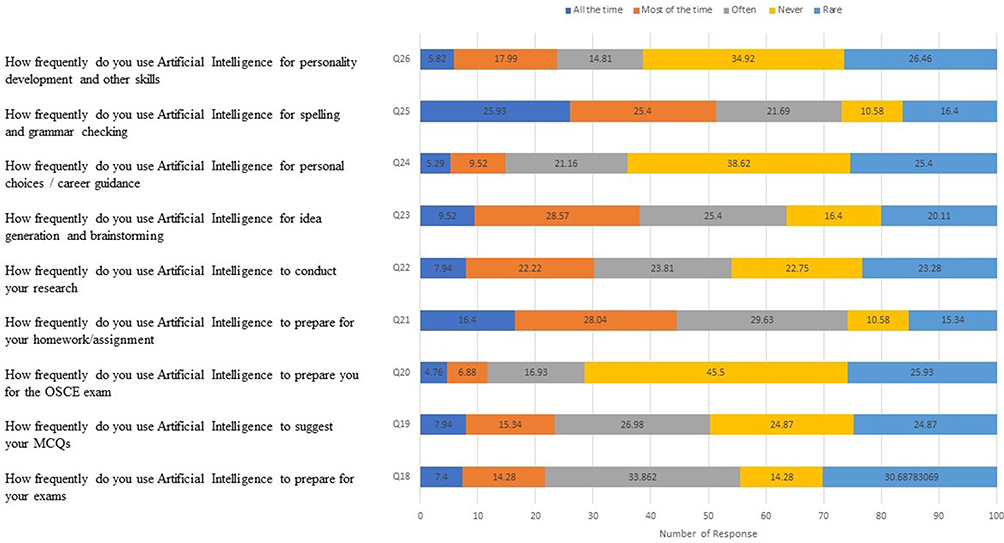 |
Figure 6 Frequency of Artificial Intelligence (AI) Usage among medical students at Taibah University. The stacked bar chart illustrates the frequency with which participants reported using AI tools. |
Figure 7 shows the responses to questions (Q18- Q26) among Taibah University medical students, grouped by their year of study. Figure 7A focuses on the responses of “all the time”. Significant differences were found between the 1st- and 2nd-year, 2nd- and 4th-year, and 5th- and 6th-year students. Moreover, highly significant differences were observed between, as well as between 2nd- and 4th-year students, for “agree” responses. Figure 7B highlights “often” responses. Significant correlations exist between 1st- and 6th-year students and 2nd- and 6th-year students. Highly significant correlations were found for “neutral” reactions between 2nd- and 3rd-year, 2nd- and 4th-year, and 5th- and 6th-year students. Figure 7C displays “never” responses. Only one statistically significant difference was noted between first- and sixth-year students.
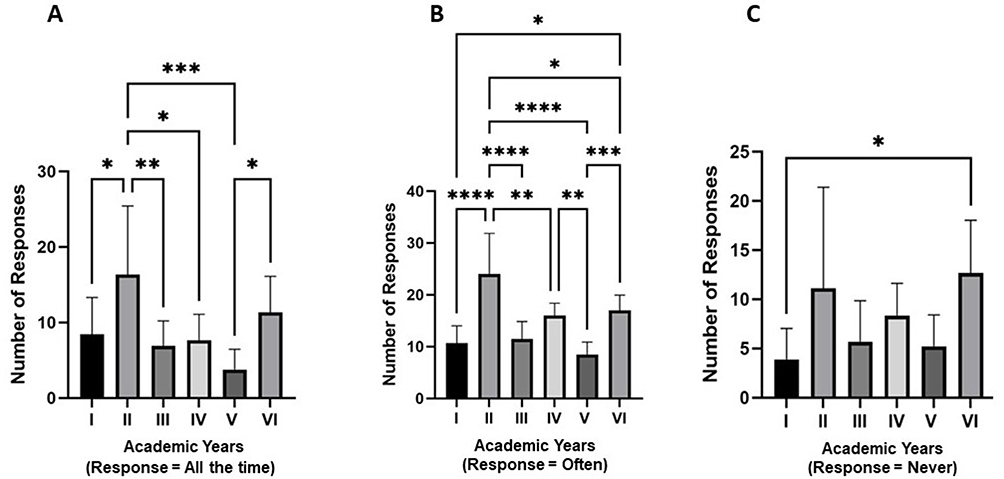 |
Figure 7 The frequency of artificial intelligence (AI) usage among medical students at Taibah University, stratified by academic year. The responses are categorized into three frequency levels: (A) All the time, (B) Often, and (C) Never. (A). Second-year students reported the highest frequency of consistent AI use, with statistically significant differences observed between multiple year groups, including first and second years (p < 0.05), and second and fifth years (p < 0.001). (B) A broader pattern of regular AI usage, with second-year students again showing significantly higher engagement than most other years. Several statistically significant and highly significant differences were observed across academic years, as indicated by multiple levels of asterisks (p < 0.05 to p < 0.0001). (C) The distribution of students who reported never using AI, with a notable significant difference between first- and sixth-year students (p < 0.05). Error bars represent the standard error of the mean. Significance levels: * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001. |
The survey results provide a picture of the increasing role of AI in the academic lives of medical students at Taibah University. While we see a firm reliance on AI for exam preparation and MCQ generation, its use for personal development activities and specific academic tasks, such as OSCE preparation, remains limited. This suggests a need for further exploration of the potential benefits of AI in these areas. It is essential to understand the factors of different tasks. This helps us identify areas where AI could be more effectively used to enhance learning and development. For example, exploring the potential benefits of AI in OSCE preparation could be particularly valuable for our future careers. By fostering a deeper understanding of AI capabilities and limitations, we can optimize its use to benefit medical education and future practice.
The survey revealed several key barriers hindering the adoption of AI (AI) among respondents, with the most prevalent concerns centering that AI facilitates cheating or plagiarism, and a lack of knowledge and expertise. Figure 8 shows the visual representation. A total of 44 respondents cited ethical and privacy concerns, indicating widespread apprehension about the potential misuse of AI and its impact on individual rights. A substantial number of respondents (56) expressed concerns about AI enabling cheating or plagiarism, highlighting a lack of clarity about responsible AI use and raising concerns about its potential to undermine academic integrity. A lack of knowledge and expertise (46 respondents) and limited access to technical equipment (28 respondents) were identified as significant barriers, suggesting a need for increased access to training, resources, and infrastructure to support AI integration. Limited integration of AI into educational curricula (34 respondents) also emerged as a significant barrier, as academics effectively incorporate AI into the educational landscape. The lack of time due to educational burdens (40 respondents) further complicates AI adoption, suggesting a need for strategies to integrate AI to maximize learning outcomes. Addressing these barriers requires a multipronged approach: developing and disseminating clear ethical guidelines for AI use in education to address concerns about cheating and privacy; providing access to training programs, workshops, and technical resources to bridge the knowledge gap and build capacity; incorporating AI into existing curricula; fostering collaborative learning environments to create more effective learning opportunities; and developing innovative approaches to integrate AI into educational settings without increasing workload. By addressing these challenges, institutions can create an environment conducive to responsible and effective AI adoption in education.
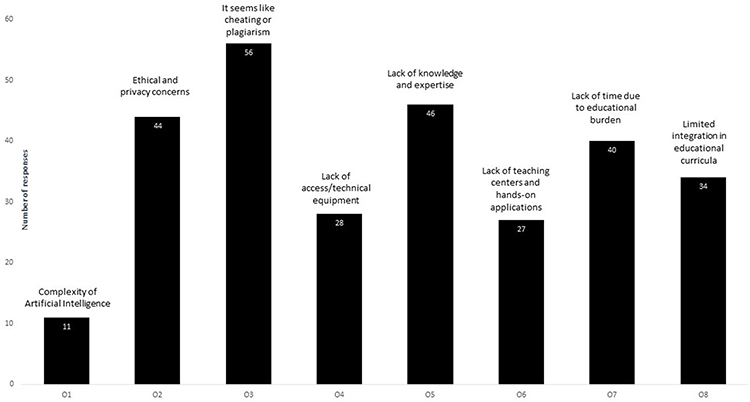 |
Figure 8 Perceived barriers to the use of artificial intelligence (AI) among medical students at Taibah University. The bar graph displays the number of responses for each identified barrier to AI adoption. |
Discussion
This study examine the knowledge, attitudes, and perceptions of medical students at Taibah University regarding AI in their medical education. The findings revealed a nuanced landscape of awareness, apprehension, and the potential for AI integration. While respondents demonstrated a foundational understanding of the basics of AI, their comprehension significantly declined when questions moved toward practical applications.14 This disconnect highlights the need for targeted educational interventions prioritizing hands-on exposure to AI tools and their applications in clinical settings.1,2 Notably, differences were observed between groups on the basis of prior exposure to AI, with students with previous experience or training showing greater confidence and a more optimistic outlook regarding the potential of AI. These findings align with existing research suggesting that practical exposure enhances AI literacy and acceptance.16 However, the limited formal instruction in AI during undergraduate studies emphasizes the necessity of integrating AI education into medical curricula.
The study also revealed diverse perceptions of AI’s impact on medical practice. While the students acknowledged AI’s ability to increase accuracy and efficiency in healthcare delivery, they expressed concerns about its reliability, ethical implications, and potential to displace certain medical specialties. These findings are consistent with recent studies on students’ behavior toward AI adoption, highlighting similar apprehensions globally.17 A unique insight emerged regarding AI’s role in preparing for the Objective Structured Clinical Examination (OSCE). Some students recognized AI’s potential to augment their learning. In contrast, others have shown a limited understanding of its practical benefits, underscoring the need for further research and case studies on AI-based learning tools in medical education.18,19
This study’s strength lies in its mixed-methods approach, which combines quantitative survey data with qualitative insights from open-ended questions. This comprehensive methodology provided a detailed understanding of medical students’ perspectives on AI. However, the reliance on convenience sampling limits the generalizability of the findings, as the participants may not represent all medical students at Taibah University. Additionally, self-reported data are subject to biases, including recall errors, which may have affected the accuracy of the responses. Future research should consider stratified sampling methods and direct observations of AI integration in educational activities to address these limitations. We suggest future studies using qualitative or longitudinal method to provide more comprehensive insight.
Our findings align with prior research showing that while medical students generally express optimism about AI’s potential, they also harbor significant concerns regarding its application in clinical practice. For example, a study reported that Romanian medical students had moderate AI knowledge but strong enthusiasm for integrating AI into medical diagnostics and education, paralleling the cautious optimism seen in our respondents.20 Another study showed that students were enthusiastic about AI but feared job displacement in specialties such as radiology, a concern echoed in our results.21
However, our study adds regional insight from the Middle East, where few prior studies have been conducted. For example, Jordanian students lacked formal AI education, which aligns with our finding that very few had formal AI instruction in undergraduate programs.22 Notably, our participants reported frequently using AI for exam preparation but underutilizing it for personal development or OSCE preparation, a nuance that is underreported in most existing studies.
Integrating AI concepts and practical applications into the medical curriculum is essential to bridge the identified knowledge gap.23 Educational reforms should include hands-on training through workshops and simulations that allow students to use AI tools in clinical scenarios, such as diagnostic decision-making and OSCE preparation.24,25 Ethics-focused education modules should address critical issues such as data privacy, bias mitigation, and the societal implications of AI in healthcare. Collaborative learning environments that involve students from medical, computer science, and engineering fields can foster a culture of innovation and exploration. Establishing dedicated research centers or innovation hubs would encourage creativity and experimentation with AI in medicine. These strategies align with the recommendations of González-Calatayud et al, who advocated for a comprehensive approach to prepare healthcare professionals for an AI-driven future. Additionally, through open discussions and collaborative research, tailored interventions should address students’ apprehensions about AI’s role in their professional careers.26–29
Future studies should adopt qualitative methods, such as focus groups or one-on-one interviews, to uncover deeper insights into the barriers to and facilitators of AI adoption among medical students.29–31 Testing AI tools in educational settings could provide empirical data on their effectiveness, particularly in enhancing OSCE preparation.30,32 Expanding the research to include other health professionals, such as nursing students, could provide a broader perspective and help identify universal challenges in integrating AI into healthcare education. Overall, this research contributes to understanding AI knowledge and perceptions among medical students in the Middle East, offering valuable insights into the need for curricular reforms. By linking these findings to practical implications, this study underscores the importance of equipping future healthcare professionals with the skills and ethical awareness needed to navigate an AI-enhanced healthcare landscape.
Conclusion
While most published studies on AI in medical education originate from Europe, North America, or East Asia, our study provides valuable insights from the Middle East, where cultural, ethical, and educational norms may influence how AI is perceived and applied. For example, concerns about privacy, religious values, or fairness in AI systems might play a different role in Saudi Arabia compared to Western contexts. Moreover, with the rise of generative AI tools like ChatGPT, which gained global prominence only in late 2022, students now encounter AI in ways that older studies did not capture. Our results suggest that, despite the availability of these tools, their application remains narrow and task-specific, underscoring the need for more targeted research and regional curriculum development. Students displayed cautious optimism regarding AI’s potential to enhance medical education and healthcare, tempered by concerns about ethical challenges, job displacement, and risks of overreliance. The findings underscore the importance of integrating AI into medical curricula to bridge the knowledge gap and promote a balanced understanding of AI capabilities and limitations. Addressing barriers such as limited access to resources, a lack of training, and ethical concerns is critical for ensuring the responsible and effective use of AI. Local barrier for AI use: Lack of AI training program for medical students, lack of ethical guideline. We recommend for medical students to have structured workshop for AI use, should have useful and clear Ethical policies for AI use. This study has Limitations, first it is a cross sectional study so it could not assess the causal relation between variables. Second it was conducted over one year, which may not reflect ongoing changes in students use and behavior toward AI. Third its conducted in one collage which may limit generalizability of findings.
Abbreviations
ML, Machine learning; DL, Deep learning; OSCE, Objective structured clinical examination; IRB, Institutional Review Board.
Data Sharing Statement
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Before data collection, ethical approval was obtained from the medical college’s Institutional Review Board (IRB) registered at the US department of health and human services IORG0008716-IRB00010413
All methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all subjects involved in this study. This study adhered to the Declaration of Helsinki.
Consent to participate is obtained via an online questionnaire, asking participants that, first, before they answer questions, they agree to participate in this study, and all the information is confidential and will be used for research purposes.
Acknowledgments
The author would like to thank Science Habitat (Ubioquitos Inc.) for reviewing the data, conducting data analysis, and completing the final review of the manuscript.
Funding
This research did not receive any specific commercial grants from funding agencies.
Disclosure
The author declares no competing interest in this work.
References
1. Eker A, Çalışkan AA, Zorali A, Kaynak B, Derin ME. Medical students’ knowledge and attitudes about artificial intelligence: a cross-sectional survey. Tip Egitimi Dünyasi. 2023;22(68):41–51. doi:10.25282/TED.1292846
2. Hopson S, Mildon C, Hassard K, Urie PM, Della Corte D. Equipping future physicians with artificial intelligence competencies through student associations. Int Med Educ. 2024;3(4):388–394. doi:10.3390/IME3040029
3. Park SH, Do KH, Kim S, Park JH, Lim YS. What should medical students know about artificial intelligence in medicine? J Educ Eval Health Prof. 2019;16:18. doi:10.3352/JEEHP.2019.16.18
4. Kolachalama VB, Garg PS. Machine learning and medical education. NPJ Digit Med. 2018;1(1). doi:10.1038/S41746-018-0061-1
5. Blease C, Kaptchuk TJ, Bernstein MH, Mandl KD, Halamka JD, Desroches CM. Artificial intelligence and the future of primary care: exploratory qualitative study of UK general practitioners’ views. J Med Internet Res. 2019;21(3):e12802. doi:10.2196/12802
6. Mehta N, Harish V, Bilimoria K, et al. Knowledge of and attitudes on artificial intelligence in healthcare: a provincial survey study of medical students. medRxiv. 2021:
7. Johnston SC. Anticipating and training the physician of the future: the importance of caring in an age of artificial intelligence. Acad Med. 2018;93(8):1105–1106. doi:10.1097/ACM.0000000000002175
8. Davenport T, Kalakota R. The potential for artificial intelligence in healthcare. Future Healthc J. 2019;6(2):94–98. doi:10.7861/FUTUREHOSP.6-2-94
9. Kaplan A, Haenlein M. Siri, Siri, in my hand: who’s the fairest in the land? On the interpretations, illustrations, and implications of artificial intelligence. Bus Horiz. 2019;62(1):15–25. doi:10.1016/j.bushor.2018.08.004
10. AlZaabi A, AlMaskari S, AalAbdulsalam A. Are physicians and medical students ready for artificial intelligence applications in healthcare? Digit Health. 2023;9. doi:10.1177/20552076231152167
11. Jha S, Topol EJ. Adapting to artificial intelligence: radiologists and pathologists as information specialists. JAMA. 2016;316(22):2353–2354. doi:10.1001/JAMA.2016.17438
12. Qin KX, Ahmad N, Soomro K, Shedu Y, Singogo TD, Rasheed AJ. Knowledge, attitude, and practice of artificial intelligence (AI) among medical students: a cross-sectional study from Ipoh, Perak. Quest Int J Med Health Sci. 2024;7(1):9–15. doi:10.5281/ZENODO.13143048
13. Khanagar S, Alkathiri M, Alhamlan R, Alyami K, Alhejazi M, Alghamdi A. Knowledge, attitudes, and perceptions of dental students towards artificial intelligence in Riyadh, Saudi Arabia. 2021.
14. Ahmed MI, Spooner B, Isherwood J, Lane M, Orrock E, Dennison A. A systematic review of the barriers to the implementation of artificial intelligence in healthcare. Cureus. 2023;15. doi:10.7759/cureus.46454
15. Al-Qerem W, Eberhardt J, Jarab A, et al. Exploring knowledge, attitudes, and practices towards artificial intelligence among health professions’ students in Jordan. BMC Med Inform Decis Mak. 2023;23(1). doi:10.1186/s12911-023-02403-0
16. Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. J Dent Res. 2020;99(7):769–774. doi:10.1177/0022034520915714
17. Darvishi A, Khosravi H, Sadiq S, Gašević D, Siemens G. Impact of AI assistance on student agency. Comput Educ. 2024;210:104967. doi:10.1016/j.compedu.2023.104967
18. Pinto Dos Santos D, Giese D, Brodehl S, et al. Medical students’ attitude towards artificial intelligence: a multicentre survey. Eur Radiol. 2019;29(4):1640–1646. doi:10.1007/s00330-018-5601-1
19. Amiri H, Peiravi S, Rezazadeh Shojaee S, et al. Medical, dental, and nursing students’ attitudes and knowledge towards artificial intelligence: a systematic review and meta-analysis. BMC Med Educ. 2024;24(1):1–12. doi:10.1186/S12909-024-05406-1/FIGURES/6
20. Onetiu F, Bratu ML, Folescu R, Bratosin F, Bratu T. Assessing medical students’ perceptions of AI-integrated telemedicine: a cross-sectional study in Romania. Healthcare. 2025;13(9):990. doi:10.3390/HEALTHCARE13090990
21. Liu DS, Abu-Shaban K, Halabi SS, Cook TS. Changes in radiology due to artificial intelligence that can attract medical students to the specialty. JMIR Med Educ. 2023;9(9):e43415. doi:10.2196/43415
22. Alzyoud M, Al-Shanableh N, Alomar S, et al. Artificial intelligence in Jordanian education: assessing acceptance via perceived cybersecurity, novelty value, and perceived trust. Int J Data Network Sci. 2024;8(2):823–834. doi:10.5267/J.IJDNS.2023.12.022
23. Miotto R, Wang F, Wang S, Jiang X, Dudley JT. Deep learning for healthcare: review, opportunities and challenges. Brief Bioinform. 2018;19(6):1236–1246. doi:10.1093/bib/bbx044
24. Shortliffe EH, Davis R, Axline SG, Buchanan BG, Green CC, Cohen SN. Computer-based consultations in clinical therapeutics: explanation and rule acquisition capabilities of the MYCIN system. Comput Biomed Res. 1975;8(4):303–320. doi:10.1016/0010-4809(75)90009-9
25. Gong B, Nugent JP, Guest W, et al. Influence of artificial intelligence on Canadian medical students’ preference for radiology specialty: a national survey study. Acad Radiol. 2019;26(4):566–577. doi:10.1016/j.acra.2018.10.007
26. Hinton G. Deep learning-A technology with the potential to transform health care. JAMA. 2018;320(11):1101–1102. doi:10.1001/jama.2018.11100
27. Kaul V, Enslin S, Gross SA. History of artificial intelligence in medicine. Gastrointest Endosc. 2020;92(4):807–812. doi:10.1016/j.gie.2020.06.040
28. Ankamah S, Gyesi K, Amponsah V. Awareness, knowledge, and attitude towards artificial intelligence: perspective of medical students in Ghana. Inf Dev. 2025;41(3):843–858. doi:10.1177/02666669241283790
29. Larentzakis A, Lygeros N. Artificial intelligence (AI) in medicine as a strategic valuable tool. Pan Afr Med J. 2021;38:184. doi:10.11604/pamj.2021.38.184.28197
30. Morris KC, Schlenoff C, Srinivasan V. A remarkable resurgence of artificial intelligence and its impact on automation and autonomy. IEEE Trans Autom Sci Eng. 2017;14(2):407–409. doi:10.1109/tase.2016.2640778
31. Hwang JY. Awareness, knowledge and attitude towards artificial intelligence in learning among faculty of medicine and health sciences students in University Tunku Abdul Rahman. 2022.
32. Mosleh R, Jarrar Q, Jarrar Y, Tazkarji M, Hawash M. Medicine and pharmacy students’ knowledge, attitudes, and practice regarding artificial intelligence programs: Jordan and west bank of Palestine. Adv Med Educ Pract. 2023;14:1391–1400. doi:10.2147/AMEP.S433255
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.