Back to Journals » Infection and Drug Resistance » Volume 13
Knowledge, Attitude, Practice, and Associated Factors Regarding the Novel Coronavirus Disease 2019 (COVID-19) Pandemic
Authors Wake AD ![]()
Received 7 August 2020
Accepted for publication 21 September 2020
Published 27 October 2020 Volume 2020:13 Pages 3817—3832
DOI https://doi.org/10.2147/IDR.S275689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Addisu Dabi Wake
Nursing Department, College of Health Sciences, Arsi University, Asella, Oromia, Ethiopia
Correspondence: Addisu Dabi Wake
Nursing Department, College of Health Sciences, Arsi University, P.O. Box: 393/04, Asella, Oromia, Ethiopia
Tel +251 910 2867 66
Email [email protected]
Abstract: It is recognized that novel coronavirus disease 2019 (COVID-19) originated from China and quickly crossed all borders by infecting individuals of all age categories throughout the entire world. Since March 11, 2020, the day the novel COVID-19 outbreak was declaration by the WHO as a COVID-19 pandemic, it has caused substantial morbidity and mortality globally. It has become a priority of global society because of the severe impact it puts in all dimensions. Therefore, the present review was intended to examine the knowledge, attitude, practice, and associated factors towards COVID-19. The review addressed the vital points for the health professionals giving care for COVID-19 patients, stakeholders participating on this pandemic virus, health policy-makers and implementers, researchers, and for the populations as a whole. The majority of the studies reflect a good knowledge, positive attitude, and good practice towards COVID-19 respective to their countries. Some studies have identified factors associated with knowledge, attitude, and practice regarding COVID-19. For instance, age, educational level, residence, monthly income, profession, gender, marital status, and news media were factors significantly associated with knowledge. Age, occupation, educational level, monthly income, gender, residence, knowledge, and practice were factors significantly associated with attitude. Age, marital status, educational level, residence, monthly income, knowledge, gender, and attitude were factors significantly associated with practice. The majority of the studies reported a good level of knowledge, optimistic attitude, and a good level of practice about COVID-19. But, some studies showed unimpressive knowledge, attitude, and practice towards COVID-19. An improvement is needed, and community education should take place as usual with a commitment by using all the strategies that could support improving the knowledge, attitude, and practice of the population. Training should be provided for healthcare workers to update and make them more effective in diagnosing, managing, and controlling this pandemic. The integration of good knowledge, a positive attitude, and sufficient practice towards COVID-19 could contribute a significant and essential role in controlling this pandemic.
Keywords: knowledge, attitude, practice, pandemic, COVID-19, novel coronavirus disease
Introduction
Primarily, in December 2019, the health authorities in Wuhan, China recognized a cluster of pneumonia cases of unknown etiology associated with the city’s South China Seafood Market. Then, a subsequent test showed a novel coronavirus, SARS-CoV-2, as an etiology of this huge outbreak.1,2 The present pandemic outbreak of COVID-19 originated from Wuhan, China and it was because of the rigorous acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with considerable mortality and morbidity rate.3 The outbreak of this pandemic virus has been brought to global consideration and was confirmed as a pandemic virus by the WHO on March 11, 2020.4 COVID-19 is an extremely contagious disease.5
The COVID-19 pandemic remains a worldwide challenge. In spite of extreme study efforts globally, the effective treatment, and vaccine options have eluded the investigators. Thus, the strategies like infection prevention protocols, early viral detection, and identification of effective treatment could offer significant tools in the controlling of the spread of this disease.6 The evidence showed that severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) caused the China epidemics with high morbidity and mortality. This infection has been transmitted to other countries.7 The COVID-19 pandemic has become one of the essential health crises of the communities worldwide. The pandemic has affected individuals of all socioeconomic groups, races, nations, and continents, while the responses have been the quarantining of entire communities, social isolation, closing of schools, and shelter in-place orders, which have suddenly changed daily life.8
Despite the rigorous global control and quarantine efforts, the incidence of COVID-19 continues to increase globally.9 COVID-19 is spreading quickly. Even though the etiology was rapidly recognized as a new coronavirus named SARS-CoV-2, the knowledge of this novel virus remains very limited. Because of the high infectivity of the virus, the large asymptomatic peoples, and lack of effective antivirals and vaccines, the management of COVID-19 has become very difficult.10 The knowledge, attitude, and practice of individuals towards this COVID-19 pandemic could play a key role in the way they accept the measures put in place to control its spread and their willingness to seek and adhere to care. The continuous rise in the number of cases and the overall good knowledge, attitude, and practice justify a further investigation to determine the effectiveness of the measures put in place to control the spread of this disease.11
Understanding the public attitudes, beliefs, and behaviors is important and significant during this pandemic situation. Encouraging the public for these behaviors suggests a chance to normalize safe practices and promote a continued use of these and other recommended personal protective behaviors to reduce the further spread of COVID-19.12 The study revealed that social media has the potential to provide rapid and effective dissemination routes for key information if used responsibly and appropriately in control of the present COVID-19 pandemic.13
Methods
The literature search conducted included the articles published up to July 30, 2020 to identify the research done on knowledge, attitude, practice, and associated factors regarding COVID-19 by using PubMed and EBSCO databases, involving both medical subject heading (MeSH) terminology and relevant keywords for search strings to locate articles that assess the knowledge, attitude, practice, and associated factors about COVID-19. The following keywords: “knowledge,” “attitude,” “practice,” and “COVID-19” were used to search for the research conducted on these topics. The present review article was done to summarize the latest articles and provide future perspectives on knowledge, attitude, and practice toward COVID-19.
Knowledge Regarding to COVID-19
As briefly summarized in Table 1, studies were conducted to assess knowledge towards COVID-19 in different countries over the world. For instance, Egypt, Pakistan, Ethiopia, Saudi Arabia, Malaysia, Bangladesh, the US and UK, Vietnam, Jordan, China, Philippines, Iran, Italy, Uganda, Nigeria, India, Tanzania, and Greece. Overall, most of these studies showed a sufficient level of knowledge towards COVID-19 with respect to their countries. The findings of each study are discussed.
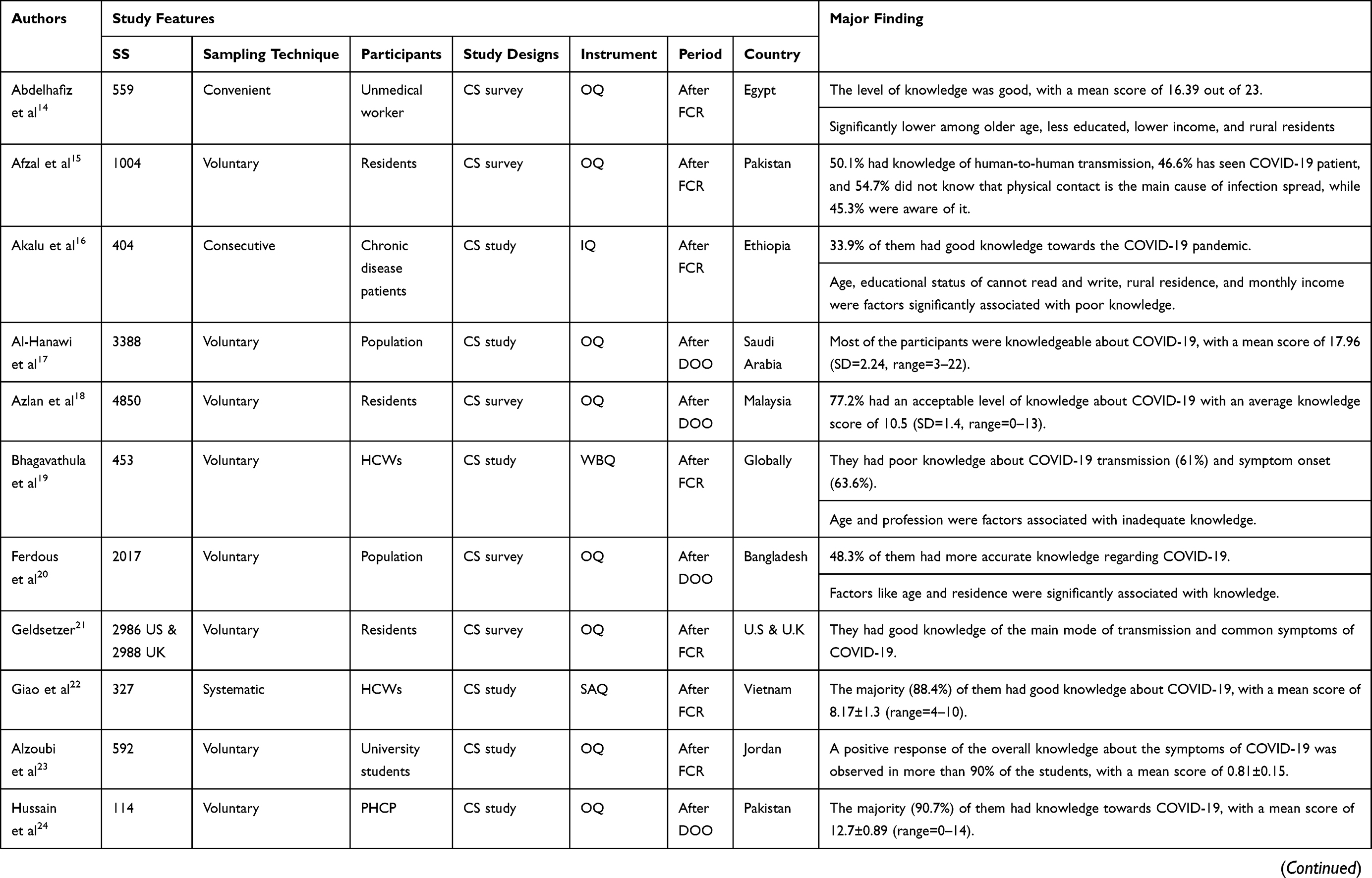 |  | 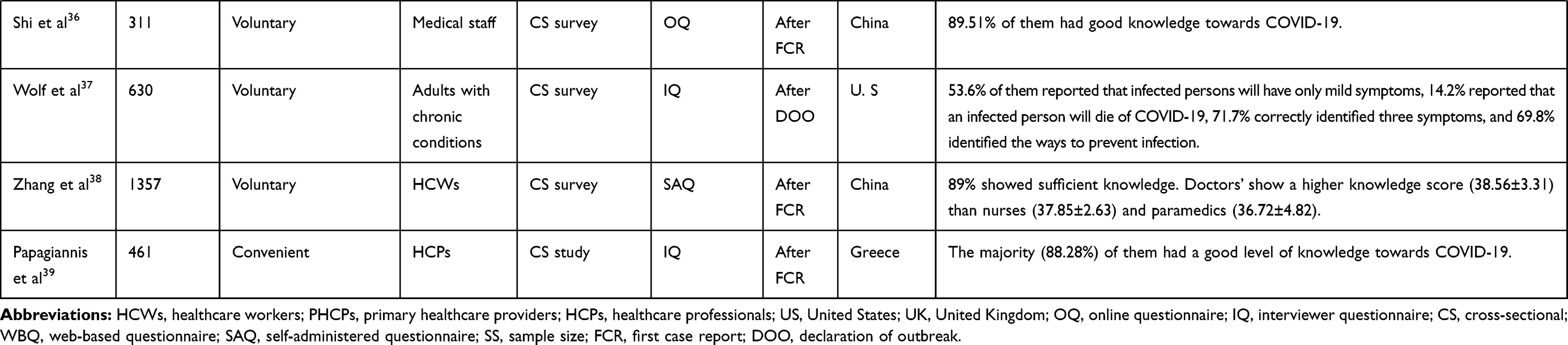 |
Table 1 Lists of the Studies Done on Knowledge and Associated Factors Regarding COVID-19 |
According to a study conducted in Egypt among 559 participants, the level of knowledge was good with a mean knowledge score of 16.39 out of 23.14 A study done in Pakistan among 1004 residents showed that 50.1% of them had knowledge of human-to-human transmission, 46.6% of them had seen a COVID-19 patient, 54.7% of them did not know that physical contact is a main cause of infection spread, while 45.3% of them were aware of it.15 A study conducted among 404 chronic disease patients in Ethiopia showed that only 33.9% of them had good knowledge towards the pandemic.16
According to a research study done among 3388 participants in Saudi Arabia, most of the participants had a high level of knowledge, with a mean knowledge score of 17.96 (SD=2.24, range= 3–22).17 A study conducted among 4850 residents in Malaysia revealed that 77.2% of them had an acceptable level of knowledge. The average knowledge score for participants was (10.5) (SD=1.4, range=0–13).18 A prospective Web-based cross-sectional study conducted among 529 healthcare workers globally showed that a significant proportion of them had poor knowledge towards COVID-19 transmission (61%) and symptom onset (63.6%).19
According to a study done among 2017 respondents in Bangladesh, less than half (48.3%) of them had more accurate knowledge regarding COVID-19.20 A study conducted among 2986 adult residents in the US and 2988 adult residents in the UK revealed that the participants had good knowledge of the main mode of disease transmission and common symptoms of COVID-19.21 In Vietnam, a study conducted among 327 healthcare workers showed that the majority (88.4%) of them had good knowledge regarding COVID-19, with a mean score of knowledge of 8.17±1.3 (range=4–10).22
A study done among 592 medical and non-medical university students in Jordan showed that a positive response regarding the overall knowledge about the symptoms of COVID-19 was observed in more than 90% of the students with the Knowledge score of 0.81±0.15.23 According to the research done among 114 primary healthcare providers in Pakistan, the majority (90.7%) of them had good overall knowledge about COVID-19, with a mean knowledge score of 12.7±0.89 (range=0–14).24 The study done among 6910 participants in China showed that the overall correct rate of the knowledge questionnaire was 90%, with a mean score of 10.8 (SD=1.6, range=0–12).25
In the Philippines, a research study conducted among 2090 respondents showed that 89.5% of them were able to identify coughing and sneezing as a transmission route, 72.6% of them recognized a transmission route was indirect hand contact, 82.2% of them recognized hand washing, 32.4% of them identified social distancing, and 40.6% of them recognized avoiding crowds as potential preventive measures.26 The study conducted among 240 medical students in Iran showed that 79.6% of them had a high, 13.8% of them had a moderate, and 6.7% of them had a low level of knowledge regarding COVID-19.27
In Italy, research done among 2046 hospital staff showed that there was good knowledge on COVID-19 control measures. The mean correct answers for questions on general aspects of the COVID-19 epidemic was 71.6% for healthcare workers and 61.2% for non-healthcare workers. The mean of correct answers for questions on COVID-19 patient management was 57.8% among healthcare workers.28 According to a study done among 2045 respondents in Bangladesh, more than half (54.87%) of them had good knowledge about COVID-19.29 A study done among 85 nurses in Iran showed that 56.5% of them had good knowledge regarding the sources, transmission, signs, symptoms, prognosis, treatment, and mortality rate of COVID-19.30 In Uganda, research conducted among 136 healthcare workers revealed that 69% of them had sufficient knowledge towards COVID-19.31
According to a study done among 589 participants in Nigeria, the majority (99.5%) of them had good knowledge about COVID-19.32 A study conducted among 662 respondents in India showed that the respondents had a moderate level of knowledge regarding COVID-19 infection and adequate knowledge about its preventive aspects. It showed that 29.5% of them answered that the virus spreads through multiple modes like touching, kissing, sneezing, and food, 43% of them regarded COVID-19 as a highly contagious disease, 97% of them acknowledged that washing hands frequently could stop the spread of infection, and 18.2% of them regarded fever as a symptom of COVID-19, which is known to be a major symptom.33
In Tanzania, a study done among 400 respondents showed that 84.4% of them had good knowledge towards COVID-19.34 According to research conducted among 414 healthcare workers in Pakistan, 93.2% of them had good knowledge about COVID-19.35 A study done among 311 medical staff in China revealed that 89.51% of them had good knowledge about COVID-19.36 In the US, a study conducted among 630 adults with chronic conditions showed that 53.6% of them reported that infected persons will have only mild symptoms, 14.2% of them reported that an infected person will die of COVID-19, 71.7% of them correctly identified three symptoms, and 69.8% of them identified the ways to prevent infection.37 Another study conducted in China among 1357 healthcare workers showed that 89% of them had sufficient knowledge about COVID-19. Doctors’ showed a higher knowledge score (38.56±3.31) than nurses (37.85±2.63) and paramedics (36.72±4.82).38 A study conducted in Greece among the healthcare professionals revealed that the majority of them (88.28%) had a good level of knowledge about SARS-CoV-2 infection.39
Factors Associated with Knowledge Regarding COVID-19
Of the listed studies in Table 1, some studies have identified factors that had an association with knowledge towards COVID-19. Below is a brief summary of the findings of each study.
According to the study conducted in Egypt among 559 adult Egyptians, knowledge towards COVID-19 was significantly lower among older age, less educated, rural residents, and lower income respondents.14 A study conducted among 404 chronic disease patients in Ethiopia showed that age, educational status of cannot read and write, rural residence, and monthly income were factors significantly associated with poor knowledge.16 A prospective Web-based cross-sectional study conducted among 529 healthcare workers globally showed that age and profession were factors associated with inadequate knowledge of COVID-19.19 According to a study done among 2017 respondents in Bangladesh, the more accurate knowledge was associated with age and residence.20
The study done among 6910 participants in China showed that knowledge was significantly different across genders, age-groups, categories of marital status, education levels, and residence.25 According to a study done among 2045 respondents in Bangladesh, knowledge was significantly diverged across age, gender, education levels, residences, income groups, and marital status.29 A study done among 85 nurses in Iran showed that age>40 years and news media were factors associated with knowledge towards COVID-19.31 In Tanzania, a study done among 400 respondents showed that the education level was significantly associated with good knowledge.34
Attitude Regarding COVID-19
Studies were done to assess attitude towards COVID-19 in different countries over the world. For example; Egypt, Pakistan, Saudi Arabia, Malaysia, Bangladesh, Vietnam, Jordan, China, Nigeria, India, Tanzania, the US, Ethiopia, Philippines, Uganda, and Greece as listed in Table 2. Generally, most of these studies showed a positive attitude regarding COVID-19 with respect to their countries. The findings of each study are briefly discussed below.
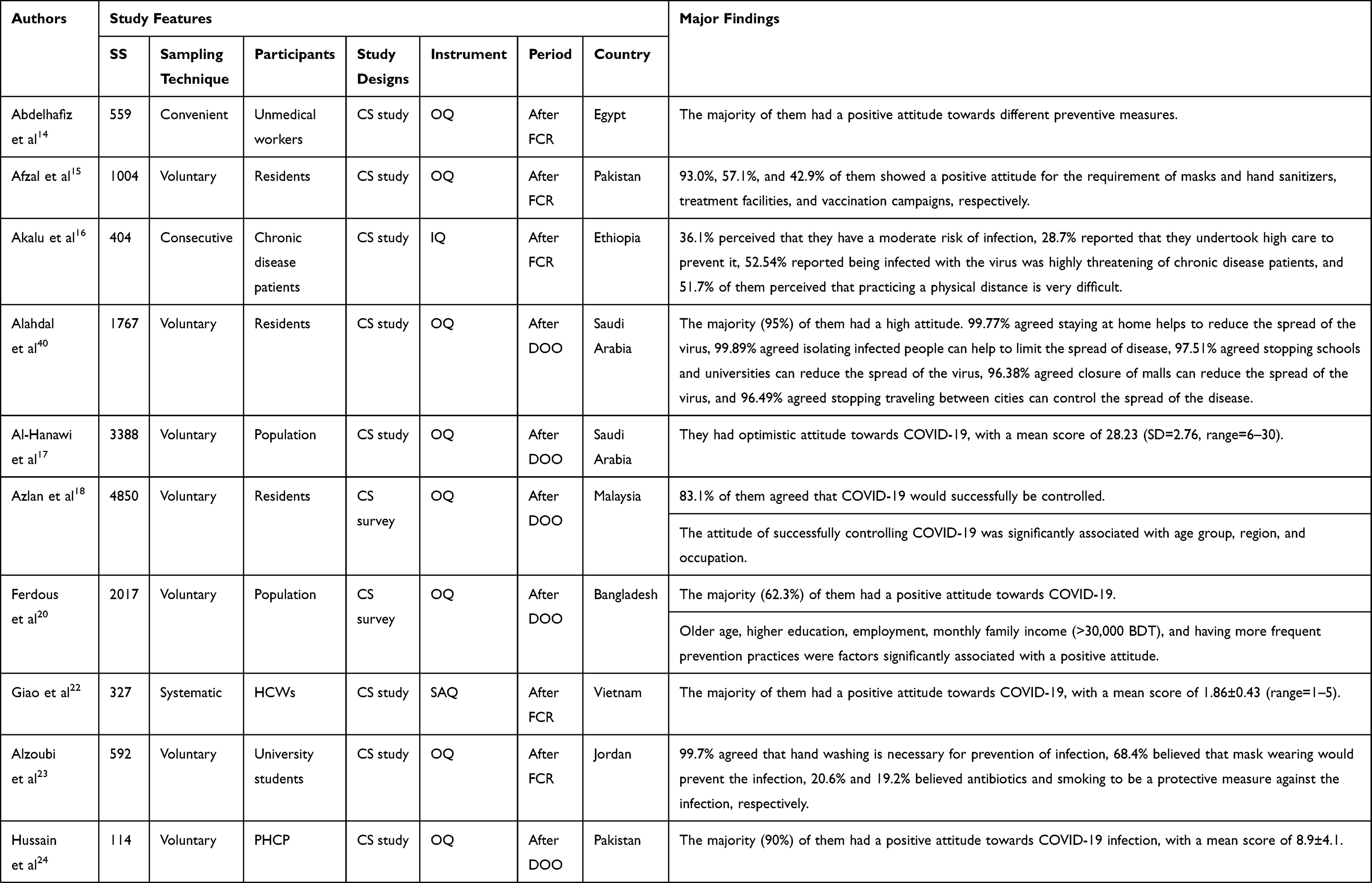 | 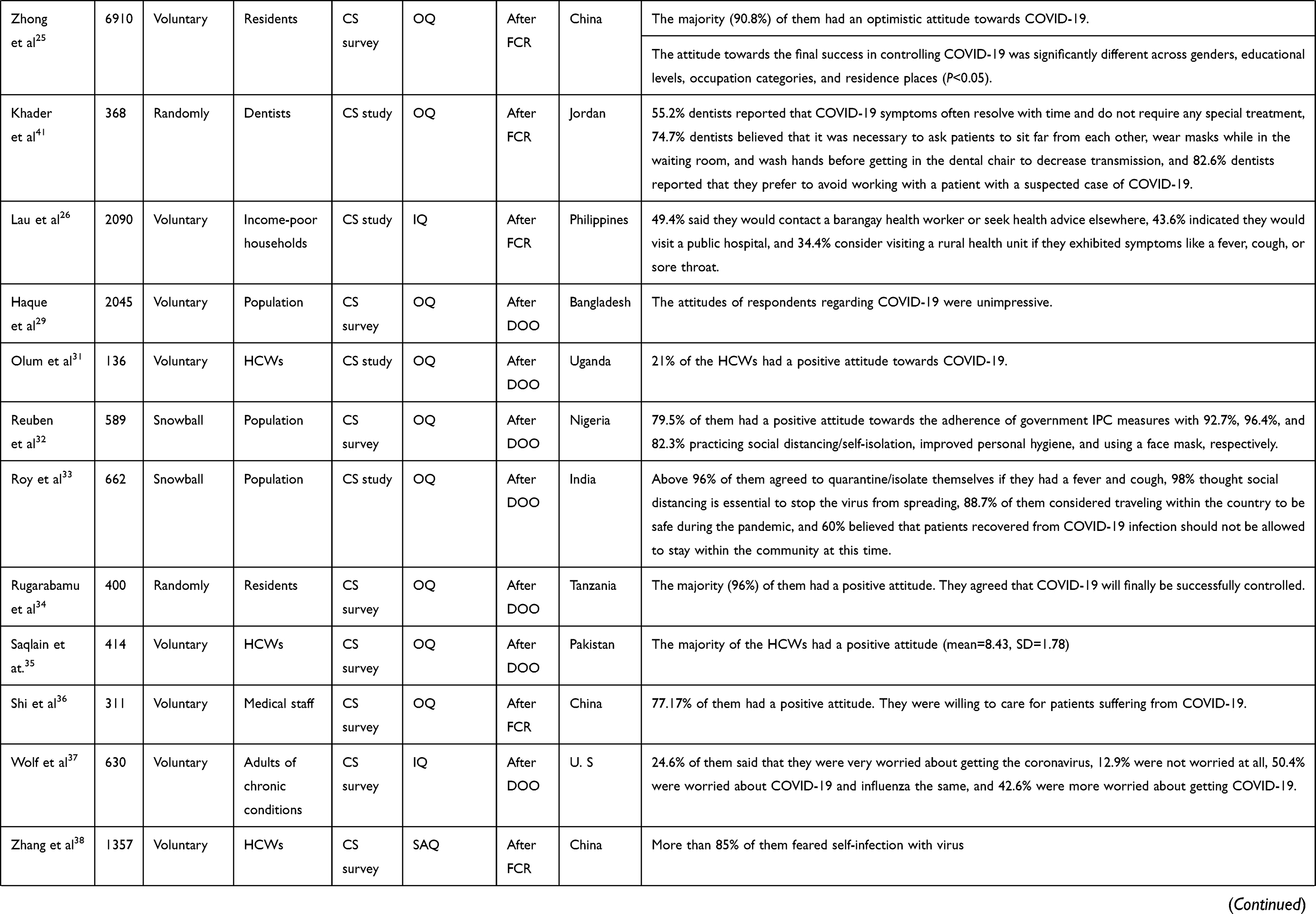 |  |  |
Table 2 The List of the Studies Conducted on Attitude and Associated Factors Towards COVID-19 |
In Egypt, a study done among 559 participants showed that the majority of them had a positive attitude towards different items of the inquired preventive measures.14 According to a study conducted among 1004 participants in Pakistan, 93.0%, 57.1%, and 42.9% of them showed a positive attitude for the requirement of masks and hand sanitizers, treatment facilities, and vaccination campaigns respectively.15 A study done among 404 chronic disease patients in Ethiopia revealed that 36.1% of them perceived that they had a moderate risk of infection with COVID-19, 28.7% of them reported that they undertook high care to prevent it, 52.54% of them reported being infected with the virus was highly threatening for chronic disease patients, and 51.7% of them perceived that practicing physical distancing is very difficult.16
In Saudi Arabia, research done among 1767 participants showed that 95% of them presented with a high attitude. About 99.77% of them agreed staying at home helps to reduce the spread of the virus, 99.89% of them agreed isolating infected people can help to limit the spread of disease, 97.51% of them agreed stopping schools and universities can reduce the spread of the virus, 96.38% of them agreed closure of malls can reduce the spread of the virus, and 96.49% of them agreed stopping traveling between cities can control the spread of the disease.40
Another study conducted in Saudi Arabia among 3388 participants showed an optimistic attitude towards COVID-19, with a mean score of 28.23 (SD=2.76, range=6–30).17 A study done among 4850 residents in Malaysia showed that 83.1% of them agreed that COVID-19 would successfully be controlled.18 In Bangladesh, research conducted among 2017 participants showed that 62.3% of them had a positive attitude towards COVID-19.20 According to the study done among 327 healthcare workers in Vietnam, the majority of them had a positive attitude towards COVID-19, with a mean score of 1.86±0.43 (range=1–5).22
In Jordan, a study conducted among 592 medical and non-medical university students showed that 99.7% of them agreed that hand washing is necessary for prevention of infection, 68.4% of them believed that mask wearing would prevent the infection, and 20.6% and 19.2% of them believed antibiotics and smoking to be a protective measured against the infection, respectively.23 According to a study done among 114 primary healthcare providers in Pakistan, the majority (90%) of them had a positive attitude towards COVID-19 infection, with a mean score of 8.9±4.1).24 A study done among 6910 participants in China revealed that the majority (90.8%) of them had an optimistic attitude towards the COVID-19 epidemic.25
In Jordan, research conducted among 368 dentists showed that 55.2% of them reported that COVID-19 symptoms often resolve with time and do not require any special treatment, 74.7% of them believed that it was necessary to ask patients to sit far from each other, wear masks while in the waiting room, and wash hands before getting in the dental chair to decrease disease transmission, and 82.6% of them reported that they prefer to avoid working with a patient with a suspected case of COVID-19.41 The study conducted among 2090 participants in the Philippines showed that 49.4% of them said they would contact a barangay health worker or seek health advice elsewhere, 43.6% of them indicated they would visit a public hospital, and 34.4% of them considered visiting a rural health unit if they exhibited symptoms like a fever, cough, or sore throat.26 According to the study conducted among 2045 participants in Bangladesh, the participants attitude regarding COVID-19 was unimpressive.29
The research done among 136 healthcare workers in Uganda showed that 21% of them had a positive attitude towards COVID-19.31 In Nigeria, research done among 589 participants revealed that 79.5% of them had a positive attitude towards the adherence of government infection prevention and control measures, with 92.7%, 96.4%, and 82.3% of them practicing social distancing/self-isolation, improved personal hygiene, and using a face mask, respectively.32 A study done among 662 participants in India showed that about 96% of them agreed to quarantine/isolate themselves if they had a fever and cough, 98% of them thought social distancing is essential to stop the virus from spreading, 88.7% of them considered traveling within the country to be safe during the pandemic, and 60% of them believed that patients recovered from COVID-19 infection should not be allowed to stay within the community at this time.33
In Tanzania, research conducted among 400 participants showed that the majority (96%) of them had a positive attitude, and they agreed that COVID-19 will finally be successfully controlled.34 According to research done among 414 healthcare workers in Pakistan, the majority of them had a positive attitude with a mean score of 8.43 (SD=1.78).35 The research conducted among 311 medical staff in China showed that 77.17% of them had a positive attitude, and were willing to care for patients suffering from COVID-19.36
According to a study conducted among 630 adults with chronic conditions in the US, 24.6% of them said they were very worried about getting coronavirus, 12.9% of them were not worried at all, 50.4% of them were worried about COVID-19 and influenza the same, and 42.6% of them were more worried about getting COVID-19.37 Another study done among 1357 healthcare workers in China revealed that 85% of them feared self-infection with virus.38 According to a study done in Greece, the majority (84.8%) of the healthcare professionals had a positive attitude concerning the prevention of infection.39
Factors Associated with Attitude Regarding COVID-19
From the listed studies in Table 2, some studies have identified factors that had an association with attitude towards COVID-19. Below is a brief summary of the findings of each study.
A study done among 4850 residents in Malaysia showed that the attitude of successfully controlling COVID-19 was significantly associated with age, region, and occupation.18 In Bangladesh, research conducted among 2017 participants showed that factors significantly associated with a positive attitude were older age, higher education, employment, monthly income (>30,000 BDT), and having more frequent prevention practices.20
A study done among 6910 participants in China revealed that the attitude towards a final success in controlling COVID-19 significantly differed across gender, educational levels, occupation categories, and residence places.25 According to a study done in Greece, the knowledge score was significantly associated with attitude score. This indicates that individuals with a high knowledge score demonstrated a more positive perception on preventive measures.39
Practice Regarding COVID-19
The studies were conducted to assess practice towards COVID-19 in different countries over the world. For instance; Pakistan, Saudi Arabia, Ethiopia, Malaysia, Bangladesh, Jordan, China, Philippines, Iran, Uganda, Nigeria, Tanzania, and Greece, as listed in Table 3. Overall, the majority of the studies showed a sufficient level of practice towards COVID-19 respective to their countries. The findings of each study are discussed.
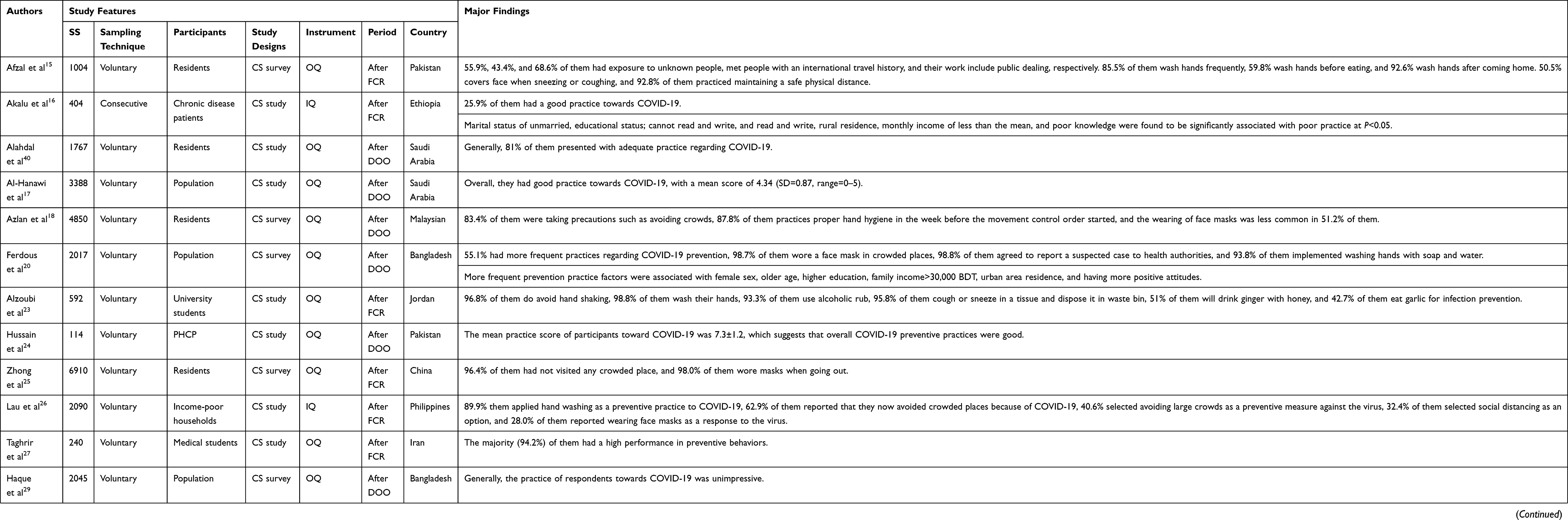 |
Table 3 The List of the Studies Conducted on Practice and Associated Factors Towards COVID-19 |
In Pakistan, research conducted among 1004 participants showed that 55.9%, 43.4%, and 68.6% of them had exposure to unknown people, met people with an international travel history, and their work included public dealing, respectively. Regarding personal hygiene, 85.5% of them wash hands frequently, 59.8% of them wash hands before eating, and 92.6% of them wash hands after coming home, while 50.5% of them cover their face when sneezing or coughing, and 92.8% of them practiced maintaining a safe physical distance.15 A study done among 404 chronic disease patients in Ethiopia indicated that the general prevalence of good practice was 25.9%.16 According to research conducted among 1767 participants in Saudi Arabia, 81% of them showed an adequate practice regarding COVID-19.40
Another study done in Saudi Arabia among 3388 participants showed that they had a good practice, with a mean score of 4.34 (SD=0.87, range=0–5).17 A study done among 4850 residents in Malaysia revealed that 83.4% of them were taking precautions such as avoiding crowds, 87.8% of them practiced proper hand hygiene in the week before the movement control order started, and the wearing of face masks was less common, at 51.2% of them.18
According to research conducted among 2017 respondents in Bangladesh, 55.1% of them had more frequent practices regarding COVID-19 prevention, while 98.7% of them wore a face mask in crowded places, 98.8% of them agreed to report a suspected case to health authorities, and 93.8% of them implemented washing hands with soap and water.20 In Jordan, a study among 592 medical and non-medical university students showed that 96.8% of them do avoid hand shaking, 98.8% of them wash their hands, 93.3% of them use alcoholic rub, 95.8% of them cough or sneeze in a tissue and dispose of it in waste bin, 51% of them will drink ginger with honey, and 42.7% of them eat garlic for infection prevention.23
Research done among 114 primary healthcare providers in Pakistan indicated that the overall COVID-19 preventive practices were good, with a mean practice score of 7.3±1.2.24 In China, research conducted among 6910 participants showed that 96.4% of them had not visited any crowded place, and 98.0% of them wore masks when going out in recent days.25 According to a study conducted among 2090 respondents in the Philippines, 89.9% of them applied hand washing as a preventive practice to COVID-19, 62.9% of them reported that they now avoid crowded places because of COVID-19, 40.6% of them selected avoiding large crowds as a preventive measure against the virus, 32.4% of them selected social distancing as an option, and 28.0% of them reported wearing face masks as a response to the virus.26
A study done among 240 medical students in Iran showed that 94.2% of them had a high performance in preventive behaviors.27 In Bangladesh, research done among 2045 respondents showed that the practices of respondents regarding COVID-19 were unimpressive.29 A study done among 136 healthcare workers in Uganda showed that 74% of the healthcare workers had a good practice towards COVID-19.31 According to the research conducted among 589 participants in Nigeria, 90.2% of them reported social distancing/avoiding crowd, 78.8% of them reported avoiding handshakes, and 74.4% of them reported avoiding face kissing as some of the practices to reduce community spread of COVID-19.32
A study done among 400 participants in Tanzania showed that the majority (77%) of them had not visited any crowded place, 80.0% of them wore masks when going out in recent days, and 98% of them correctly identified that COVID-19 is transmitted by respiratory droplets and also factors such as chronic illnesses and obesity can lead to a serious case.34 In Pakistan, research done among 414 healthcare workers showed that 88.7% of them had a good practice regarding COVID-19.35 Another study done among 1357 healthcare workers in China showed that 89.7% of them had a good practice regarding COVID-19.38 According to a study done in Greece, only 24.9% of healthcare professionals reported that they washed their hands before and after contact with the patient/patient’s environment.39
Factors Associated with Practice Regarding COVID-19
From the studies listed in Table 3, some studies have identified factors that had an association with practice towards COVID-19. Below is a brief summary of the findings of each study.
A study done among 404 chronic disease patients in Ethiopia indicated that the marital status of unmarried, educational status; cannot read and write, and read and write, rural residence, monthly income of less than a mean, and poor knowledge were factors significantly associated with poor practice.16 According to research conducted among 2017 respondents in Bangladesh, female sex, older age, higher education, monthly income (>30,000 BDT), urban residence, and having more positive attitude were factors significantly associated with the more frequent prevention practice.20 According to a study done in Greece, the knowledge score was significantly associated with practice score. This indicated that individuals with a high knowledge score would practice more preventive measures.39
What Is the Significance of Assessing KAP Regarding COVID-19?
The present review showed that there were discrepancies between the studies reported on the level of knowledge, attitude, and practice towards COVID-19, as discussed above. For instance, the studies of Egypt, Pakistan, Saudi Arabia, Malaysia, the US and UK, Vietnam, Jordan, Pakistan, China, Philippines, Iran, Italy, Bangladesh, Uganda, Nigeria, Tanzania, Greece, and the US reported that the majority of the respondents had good knowledge about COVID-19. The study of India reported that the participants had moderate knowledge towards COVID-19. However, a study of Ethiopia and Bangladesh reported a poor level of knowledge regarding COVID-19.
Concerning the attitude towards COVID-19, the studies of Egypt, Pakistan, Saudi Arabia, Malaysia, Bangladesh, Vietnam, Greece, Jordan, Nigeria, India, Tanzania, the US, and China reported that the majority of the respondents had a positive attitude. But, the studies of Ethiopia, Philippines, Bangladesh, and Uganda reported that the majority of the respondents had a negative attitude. Regarding the practice towards COVID-19, the studies of Pakistan, Saudi Arabia, Malaysia, Bangladesh, Jordan, China, Philippines, Iran, Uganda, Nigeria, and Tanzania were reported a sufficient level of practice. However, the studies of Ethiopia and Bangladesh reported unimpressive levels of practice.
Collectively, the findings from different studies showed that the majority of their participants had a sufficient knowledge, positive attitude, and good practice. This reflects that there were participants who had poor knowledge, a negative attitude, and poor practice in their studies, even though they were relatively low in number. Further, some studies reported that the majority of their participants had an inadequate knowledge, negative attitude, and insufficient practice towards COVID-19 in different countries all over the world, as briefly explained above. These reflect that there is still a gap of knowledge, attitude, and practice regarding the COVID-19 pandemic in different countries all over the world. This suggests that still extensive improvements are needed to manage and control this pandemic.
Moreover, the significance of assessing the level of KAP regarding COVID-19 is because the knowledge, attitude, and practice are inter-related. They affect each other while the effect could be positive or negative. This was supported by a study which reported that the knowledge was positively correlated with attitude and practices.15 It was also supported by a study which reported that knowledge was significantly associated with both attitude and practice. This indicates that individuals with a high knowledge score demonstrate a more positive perception on preventive measures and would practice more preventive measures.39 Further, it was also supported by a study which reported that poor knowledge was found to be significantly associated with poor practice.16 It was also supported by the study which reported that having more frequent prevention practices were factors associated with positive attitude.20 It was also supported by the study which reported that attitude was positively correlated with practices.15 Therefore, understanding the relationship of knowledge, attitude, and practice towards the COVID-19 pandemic is significant and essential to enhance the strategies required to manage and control this pandemic.
Conclusions
It was identified that a novel COVID-19 originated from China and quickly crossed all borders by infecting individuals of all age categories throughout the entire world. This COVID-19 pandemic contributes a major global challenge, with a massive yet possibly underestimated burden and numerous unidentified events. This phenomenon has several global burdens, such as morbidity, mortality, closure of schools, political crisis, economic crisis, burden on healthcare providers, and considerable public reaction.
Overall, the majority of the studies reflect good knowledge, positive attitude, and good practice towards COVID-19, respective to their countries. Further, some studies have identified factors that were associated with knowledge, attitude, and practice toward COVID-19. For instance; age, educational level, residence, monthly income, profession, gender, marital status, and news media were factors significantly associated with knowledge towards COVID-19. Age, occupation, educational level, monthly income, gender, residence, knowledge, and practice were factors significantly associated with attitude towards COVID-19. Age, marital status, educational level, residence, monthly income, knowledge, gender, and attitude were factors significantly associated with practice towards COVID-19.
Even though the majority of the studies reported good knowledge, an optimistic attitude and good practice regarding COVID-19, some studies showed unimpressive knowledge, attitude, and practice towards COVID-19. Particularly, this is more critical for healthcare workers. This is because, since the healthcare workers are at the frontline defense against the COVID-19 pandemic, insufficient knowledge, negative attitude, and poor practice can significantly affect the management and control of this pandemic. The insufficient knowledge and negative attitude could directly affect the practice and lead to poor infection control, spread of virus, delayed diagnosis, and increased morbidity and mortality. Therefore, improvement is still needed and community education should take place as usual with a commitment by using all the strategies that could support the improvement of knowledge, attitude, and practice of the population. Also, training should be provided for healthcare workers to update and make them more effective in diagnosing, managing, and controlling this pandemic.
Since the clinical presentation is mainly asymptomatic, and the specific treatment and vaccines are absent, it is clear that a good knowledge, positive attitude, and sufficient practice toward COVID-19 are vital for the management and control of this pandemic. Hopefully, the integration of these components could contribute a significant and essential role in managing and controlling this pandemic. Finally, the present review suggests further research to be conducted on COVID-19 considering the barriers that contribute for the quick distributions and the reason for the reduction of the precautions toward this pandemic virus.
Disclosure
The author declares no conflicts of interest for this work.
References
1. Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med. 2020;20(2):124–127. doi:10.7861/clinmed.2019-coron
2. Sun P, Lu X, Xu C, Sun W, Pan B. Understanding of COVID‐19 based on current evidence. J Med Virol. 2020;92:548–551. doi:10.1002/jmv.25722
3. Dariya B, Nagaraju GP. Understanding novel COVID-19: its impact on organ failure and risk assessment for diabetic and cancer patients. Cytokine Growth Factor Rev. 2020;53:43–52. doi:10.1016/j.cytogfr.2020.05.001
4. Jin Y, Yang H, Ji W, et al. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses. 2020;12(4):372. doi:10.3390/v12040372
5. Wang L, Wang Y, Ye D, Liu Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int J Antimicrob Agents. 2020;55:105948. doi:10.1016/j.ijantimicag.2020.105948
6. Lotfi M, Hamblin MR, Rezaei N. COVID-19: transmission, prevention, and potential therapeutic opportunities. Clin Chim Acta. 2020;508:254–266. doi:10.1016/j.cca.2020.05.044
7. Lu Q, Shi Y. Coronavirus disease (COVID‐19) and neonate: what neonatologist need to know. J Med Virol. 2020;92:564–567. doi:10.1002/jmv.25740
8. Shanafelt T, Ripp J, Trockel M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA. 2020;323(21):2133. doi:10.1001/jama.2020.5893
9. Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
10. Cao W, Li T. COVID-19: towards understanding of pathogenesis. Cell Res. 2020;30:367–369. doi:10.1038/s41422-020-0327-4
11. Adela N, Nkengazong L, Ambe LA, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. 2020;14:e0008700. doi:10.1371/journal.pntd.0008700
12. Czeisler MÉ, Tynan MA, Howard ME, et al. Public attitudes, behaviors, and beliefs related to COVID-19, stay-at-home orders, nonessential business closures, and public health guidance — United States, New York City, and Los Angeles, May 5–12, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:751–758. doi:10.15585/mmwr.mm6924e1
13. Chan AKM, Nickson CP, Rudolph JW, Lee A, Joynt GM. Social media for rapid knowledge dissemination: early experience from the COVID‐19 pandemic. Anaesthesia. 2020. doi:10.1111/anae.15057
14. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel Coronavirus Disease (COVID-19). J Community Health. 2020;45(5):881–890. doi:10.1007/s10900-020-00827-7
15. Afzal MS, Khan A, Qureshi UUR, et al. Community-based assessment of knowledge, attitude, practices and risk factors regarding COVID-19 among Pakistanis residents during a recent outbreak: a cross-sectional survey. J Community Health. 2020. doi:10.1007/s10900-020-00875-z
16. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949–1960. doi:10.2147/IDR.S258736
17. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a Cross-Sectional Study. Front Public Health. 2020:8. doi:10.3389/fpubh.2020.00217
18. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E, Tu W-J. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
19. Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Novel Coronavirus (COVID-19) knowledge and perceptions: a survey of healthcare workers. Inf Dis. 2020. doi:10.1101/2020.03.09.20033381
20. MostZ F, Md SI, MdT S, ASMd M, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladeshi people: an online-based cross-sectional study. Public Global Health. 2020. doi:10.1101/2020.05.26.20105700
21. Geldsetzer P. Use of rapid online surveys to assess people’s perceptions during infectious disease outbreaks: a cross-sectional survey on COVID-19. J Med Internet Res. 2020;22:e18790. doi:10.2196/18790
22. Giao H, Han NTN, Khanh TV, Ngan VK. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260.
23. Alzoubi H, Alnawaiseh N, Al-Mnayyis A, et al.; Community Medicine and Public Health Department, Faculty of Medicine, Mutah University, Department of clinical sciences, College of Medicine, Yarmouk University, Shafiq Irshidat St, Irbid 21163, Jordan, Abu- Lubad M, Departmrnt of Microbiology and Immunology, Faculty of medicine, Mu’tah University, Jordan. COVID-19 - knowledge, attitude and practice among Medical and Non-Medical University Students in Jordan. J Pure Appl Microbiol. 2020;14:17–24. doi:10.22207/JPAM.14.1.04
24. Hussain I, Majeed A, Imran I, et al. Knowledge, attitude, and practices toward COVID-19 in primary healthcare providers: a Cross-Sectional Study from three tertiary Care Hospitals of Peshawar, Pakistan. J Community Health. 2020. doi:10.1007/s10900-020-00879-9
25. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16:1745–1752. doi:10.7150/ijbs.45221
26. Lau LL, Hung N, Go DJ, et al. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: a cross-sectional study. J Glob Health. 2020;10:011007. doi:10.7189/jogh.10.011007
27. Taghrir MH, Borazjani R, Shiraly R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Arch Iran Med. 2020;23(4):249–254. doi:10.34172/aim.2020.06
28. Moro M, Vigezzi GP, Capraro M, et al. 2019-novel coronavirus survey: knowledge and attitudes of hospital staff of a large Italian teaching hospital. Acta Biomedica. 2020;91:29–34. doi:10.23750/abm.v91i3-S.9419
29. Haque T, Hossain KM
30. Nemati M, Ebrahimi B, Nemati F. Assessment of Iranian nurses’ knowledge and anxiety toward COVID-19 during the current outbreak in Iran. Arch Clin Infect Dis. 2020;15(COVID–19). doi:10.5812/archcid.102848
31. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Front Public Health. 2020;8:181. doi:10.3389/fpubh.2020.00181
32. Reuben RC, Danladi MMA, Saleh DA, Ejembi PE. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. 2020. doi:10.1007/s10900-020-00881-1
33. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
34. Rugarabamu S, Byanaku A, Ibrahim M. Knowledge, attitudes, and practices (KAP) towards COVID-19: a quick online cross-sectional survey among Tanzanian residents. Inf Dis. 2020. doi:10.1101/2020.04.26.20080820
35. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105:419–423. doi:10.1016/j.jhin.2020.05.007
36. Shi Y, Wang J, Yang Y, et al. Knowledge and attitudes of medical staff in Chinese psychiatric hospitals regarding COVID-19. Brain Behav Immun Health. 2020;4:100064. doi:10.1016/j.bbih.2020.100064
37. Wolf MS, Serper M, Opsasnick L, et al. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the U.S. outbreak. Ann Intern Med. 2020;173(2):100–109. doi:10.7326/M20-1239
38. Zhang M, Zhou M, Tang F, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hosp Infect. 2020;105:183–187. doi:10.1016/j.jhin.2020.04.012
39. Papagiannis D, Malli F, Raptis DG, et al. Assessment of knowledge, attitudes, and practices towards new coronavirus (SARS-CoV-2) of health care professionals in Greece before the outbreak period. Int J Environ Res Public Health. 2020;17:4925. doi:10.3390/ijerph17144925
40. Alahdal H, Basingab F, Alotaibi R. An analytical study on the awareness, attitude and practice during the COVID-19 pandemic in Riyadh, Saudi Arabia. J Infect Public Health. 2020;S1876034120305256. doi:10.1016/j.jiph.2020.06.015
41. Khader Y, Al Nsour M, Al-Batayneh OB, et al. Dentists’ awareness, perception, and attitude regarding COVID-19 and infection control: Cross-Sectional Study among Jordanian dentists. JMIR Public Health Surveill. 2020;6:e18798. doi:10.2196/18798
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.