Back to Journals » Infection and Drug Resistance » Volume 14
Knowledge, Attitude and Self-Reported Performance and Challenges of Hand Hygiene Using Alcohol-Based Hand Sanitizers Among Healthcare Workers During COVID-19 Pandemic at a Tertiary Hospital: A Cross-Sectional Study
Authors Assefa D, Melaku T ![]() , Bayisa B
, Bayisa B ![]() , Alemu S
, Alemu S ![]()
Received 12 November 2020
Accepted for publication 19 January 2021
Published 29 January 2021 Volume 2021:14 Pages 303—313
DOI https://doi.org/10.2147/IDR.S291690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Desta Assefa, Tsegaye Melaku, Bodena Bayisa, Sintayehu Alemu
School of Pharmacy, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Desta Assefa
School of Pharmacy, Jimma University, P.O. Box: 378, Jimma, Oromia, Ethiopia
Fax +251 4711114 50
Email [email protected]
Background and Objective: Understanding and consistent hand hygiene practice by alcohol-based hand sanitizer is a cardinal step to stay safe from the coronavirus disease (COVID-19) pandemic. This study aimed to assess the self-reported level of knowledge, attitude, practice, and challenges to practice hand hygiene by alcohol-based hand sanitizers among healthcare workers during the COVID-19 pandemic in Jimma Medical Center, Ethiopia.
Methods: Between April and June 2020, a questionnaire-based descriptive cross-sectional study was conducted using 96 study participants. Data were analyzed using SPSS version 21 and described.
Results: All of the study participants (96) were at the forefront of the fight against COVID-19. Most of the study participants were nurses (27) and pharmacists (21). Their mean age was 28.69± 4.048 years. All of them were practicing different COVID-19 prevention methods. In this study, 95.8% of the respondents used alcohol-based hand sanitizers. The majority of the respondents were knowledgeable (93.8%), had a favorable attitude (74%), and good hand hygiene practices (76%) by alcohol-based hand sanitizers. However, 84.5% of the respondents were confronted with challenges during alcohol-based hand sanitizer use due to it is unavailable 66 (68.8%), expensive 50 (52.1%), forgetting 11 (11.5%), experiencing health-associated risks (skin irritation (28.1%), skin dryness (62.5%), ocular irritation (11.5%)), etc.
Conclusion: The majority of respondents had good knowledge, attitude, and practices of alcohol-based hand sanitizer. But there were some items of their evaluation with relatively low scores that revealed some room for improvements. Additionally, the respondents reported various challenges. Therefore, to achieve and sustain changes, the hand hygiene promotion strategic plan needs a great concern.
Keywords: coronavirus disease, hand hygiene, alcohol-based hand sanitizer, healthcare worker
Background
Coronavirus disease (COVID-19) is a respiratory illness and was declared a global pandemic by the WHO on March 11, 2020. Since its emergence, it is spreading rapidly over the world and became a global health crisis of our time. These crises are devastating social, health, economic, and political problems that will leave deep scars.1–3
Coronavirus disease is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Humans are the common transmission source of SARS-CoV-2 through human to human interactions (through respiratory droplets or contact).4–6 Transmission occurs when the hands contaminated with the virus touch the mucosa of a healthy person’s mouth, nose, or eyes. The infected persons can transmit the virus even when they have no, or only mild, symptoms.3,7,8
So far, no medication therapy is available to manage COVID-19. Preventing spread is therefore extremely important to reduce the overall burden of the disease and to remain safe. Currently, WHO recommends physical distances, appropriate use of all personal protective equipment (such as masks, goggles, etc), and hand hygiene (HH) practices to reduce the spread.7
Practicing HH, which includes the use of alcohol-based hand sanitizer (ABHS) or handwashing with soap and water, is a simple and yet effective way to prevent the spread of COVID-19 in healthcare settings.9,10 Unless hands are visibly soiled, ABHS is recommended by the WHO over handwashing with soap and water in most clinical situations. It should be due to ABHS is time and cost-effective, available at the point of care, has improved skin tolerance and has a broad microbiological spectrum. The ABHS should contain at least 60% ethanol or 70% isopropanol to kill the COVID-19 virus.11–14
Following the outbreak of COVID-19, the popularity of ABHS in the community and healthcare settings has been increasing. But, different studies had been done before the COVID-19 outburst and showed that overall compliance with HH by ABHS was poor in developing countries. Additionally, it is hard to promote by using the WHO multi-modal strategy.15,16
Especially healthcare workers (HCWs) were highly ABHSs users during this COVID-19 pandemic time. Therefore, their knowledge, attitudes, challenges, and compliance with practicing ABHS at the five essential moments recommended by the WHO can affect the safety of them and their staff clients and community. Therefore, it is essential to study this situation to enhance the development of appropriate strategies to promote HH for users in the future. So, the present study was focused on identifying gaps and strengths by assessing the self-reported level of knowledge, attitude, practice, and challenges to practice WHO recommended HH procedures by ABHS among HCWs during the COVID-19 pandemic in Jimma Medical Center (JMC), Ethiopia.
Methods
Study Setting, Design, and Period
A hospital-based descriptive cross-sectional study design was conducted between April 01 and June 27, 2020. The study area was at JMC. JMC is one of the oldest hospitals in Ethiopia, and the only teaching and referral hospital in southwest Ethiopia. It has an 800-bed capacity and a catchment population of over 15 million people. More than 400,000 patients can be served at emergency, outpatient departments, and various inpatient units per budget year.
Eligibility Criteria
The volunteer HCWs who served a health institute for a minimum of 1 year, working in JMC, and ≥18 years of age during the study period were eligible to participate in the study.
Survey Population, Sample Frame, Sample Size, and Sampling Method
The survey populations were HCWs, such as clinical nurses, pharmacists, academicians, medical laboratory technologists, physicians, dental doctors, and midwives, working in JMC. The sample frame was HCWs who were on duty at JMC during the study period. The study participants were all HCWs who were on duty in the months of data collection and agreed to participate in the study. The response rate was low due to data collection was paper-based, and it can be the means of COVID-19 virus transmission. Therefore, the sample size was only 96 HCWs. The convenience sampling method was used based on the HCWs’ availability at the work area and willingness to participate in the study.
Data Collection Tool and Procedures
Data collection was done with well structured, pretested, and self-administered English questionnaire. The self-reported questionnaire included questions prepared on participant demographics, HH by ABHSs’ knowledge, attitudes, practices, and challenges on performing it. It was developed by using the WHO guidelines and other references.9–12,14–18,21–26
The data collectors were four trained health professionals. They were trained on the objectives of the study and the contents of the data collection checklist. The voluntary participants who agreed to cooperate with the study were asked for verbal agreement. Then, data collectors delivered a developed data collection checklist to the study participants when they were at the work area and collected it soon after filled. Strict supervision by the principal investigators was conducted during data collection to prevent selection bias.
Study Variables and Measurements
The study participants’ knowledge, attitude, practice, and common challenges of HH by ABHSs were assessed and described using qualitative terms of self-evaluation. The self-reported questionnaires were developed from previous studies.
The self-reported knowledge of the respondents about ABHSs for COVID-19 prevention was evaluated by using terms like agree, disagree, and not know the approved facts. Then, the respondents were categorized as knowledgeable and not knowledgeable. The study participant who agreed with the facts on the WHO guidelines on HH in health care (received 1 point) and replied correctly (agree) ≥50% of the knowledge questions were considered as knowledgeable.9–12,15
The attitude questionnaire aimed mainly at studying the attitude of HCW towards methods of improvement of handwashing practice in their workplace. For attitude description, terms like strongly agree, agree, neutral, disagree, and strongly disagree were used. The study participants who agreed or strongly agreed to the facts listed on the WHO guidelines (received 1 point) and replied ≥50% of the attitude questions correctly were considered as having a good attitude. Those who replied neutral, disagree, or strongly disagree with the facts listed on the WHO guidelines (received 0 point) and responded <50% correctly (agreed or strongly agreed) were considered as having a poor attitude.9,10,17
For evaluation of self-reported hand hygiene practices or compliance, five questions were developed based on WHO’s ‘My five moments for hand hygiene (before patient contact, before clean/aseptic procedures, after the risk of body fluids, after patient contact, and after contact with patient surroundings).9 Respondents were asked to choose from five options-always, often, sometimes, seldom, or never.
The study participants who believe that they always practice ABHS for HH at the five essential moments (received 1 point) and correctly (always) replied ≥50% of the compliance questions were considered as compliant. And those who practice ABHS often, sometimes, seldom, or never (received 0 point) and responded <50% correctly (always) were considered as non-compliant.17,18,20–23,25,26
A higher score in each domain (knowledge, practice, and attitude) indicated greater knowledge, more frequent performance, and better attitudes.
For the assessment of challenges to the practice of HH by ABHSs at the five essential moments in health care, according to the recommended handwashing practice, were evaluated. The questions were developed using related references were used.14,23–26
Data Quality Assurance and Analysis
After the pretest, the questionnaires were revised for clarity and consistency. All filled questionnaires were checked regularly for completeness individually.
Data entry, data checking, and data analysis were done with the program Statistical Package for Social Sciences (SPSS) version 21. The level of significance was set at 5% (p< 0.05). Descriptive statistics for socio-demographic characteristics, hand hygiene knowledge level, and hand hygiene practices of the respondents were reported. Categorical variables were described by frequencies and percentages and presented in a table, figure, and paragraph.
Ethics Approval and Informed Consent
Before the commencement of the study, the written proposal was presented to Jimma University Institutional Review Board for approval. The Institutional Review Board evaluated the document and waived the requirement for the documentation of written informed consent and allowed investigators to obtain verbal informed consent. Then, before the administration of the questionnaire, the data collectors explained all pertinent information (purpose, risks, benefits, alternatives to participation, etc.) for study participants and allowed them the opportunity to ask questions. Then, verbal agreement to participate in the research was obtained from the volunteers, and data collected. The collected data were kept confidential and maintained locked throughout the study. Only the principal investigators and co-authors had access to the data. This study was conducted in accordance with the Declaration of Helsinki.
Operational Definition
Academician: Health professionals giving health services in JMC and/or academic activity at Jimma University
Hand hygiene: a behavior of cleaning the hands with soap and water and by hand-rubbing using hand sanitizer without water
Handwashing: washing hands with plain or antimicrobial soap and water
Knowledge: having an adequate understanding of hand hygiene.
- Knowledgeable: earning a score of 50% and above on the knowledge questions indicating having a sufficient amount of knowledge
- Not knowledgeable: earning score of less than 50% on the knowledge questions
Practice: an act of performing a given procedure(s) according to a set standard.
- Good practice: study participants who responded to the practice questions ≥50% in line with the recommended handwashing practice
- Poor practice: study participants who responded to the practice questions <50% in line with the recommended handwashing practice
Attitude: the belief of the respondents towards the facts on the WHO guidelines on HH in health care.
- Good/favorable attitude: those who agree and strongly agree to the facts and responded ≥50% correctly to the attitude questions
- Poor attitude: who responded <50% correctly the attitude questions
Results
Demographic Characteristics of Enrolled Healthcare Workers
Of the total JMC HCWs on duty in the months of data collection, 96 of them have participated in this study. Majority of the respondents were clinical nurses 27 (28.1%); followed by pharmacists 21 (21.9%), academicians 15 (15.6%), medical laboratory technologists 13 (13.5%), physicians 7 (7.3%), dental doctors 7 (7.3%) and midwives 6 (6.3%), respectively. Their mean age was 28.69±4.048 years (Table 1). Following the outbreak of COVID-19, 39 (40.6%) of them were taken training on the measures for preventing COVID-19 transmission.
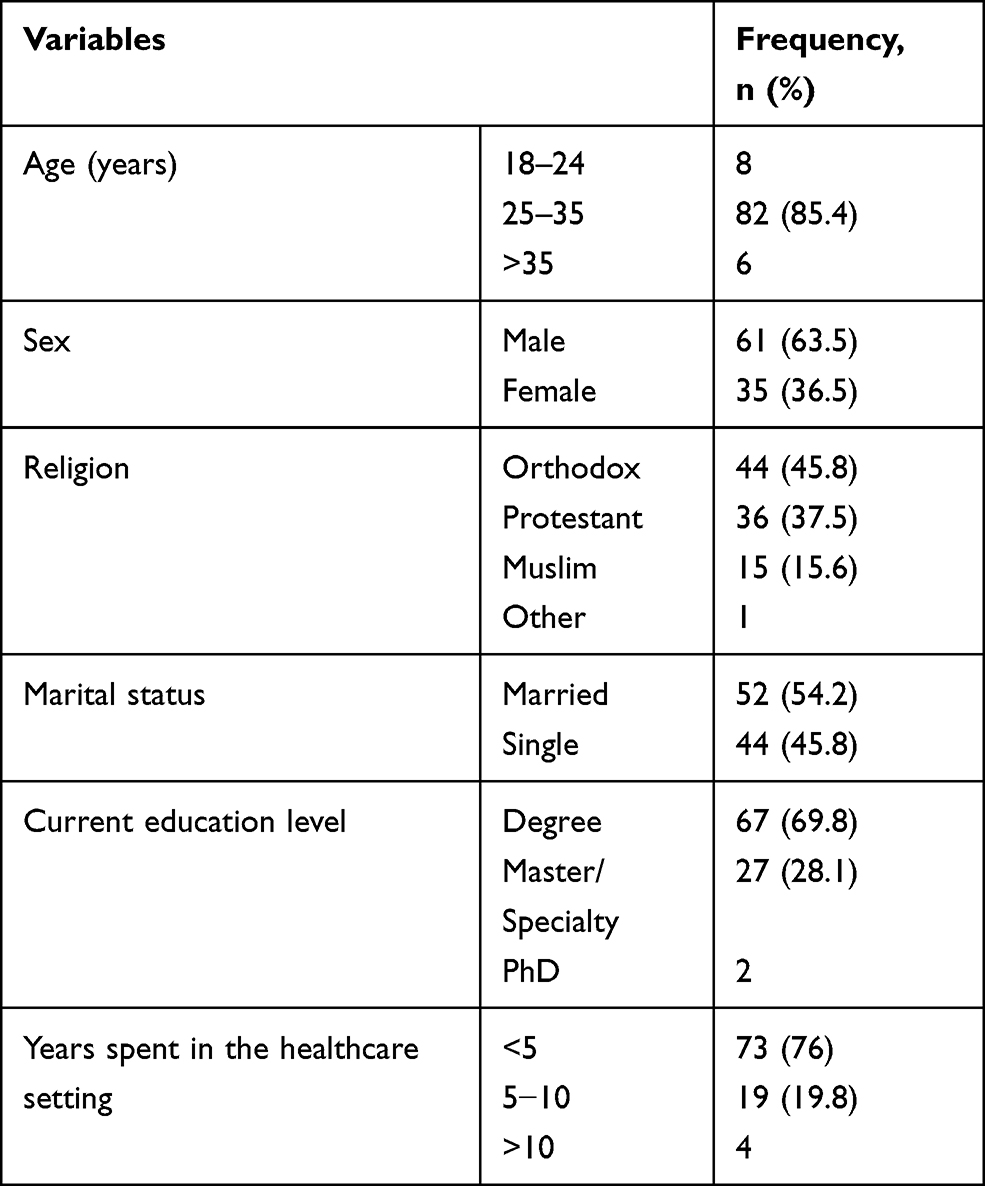 |
Table 1 Demographic Characteristics of Enrolled Healthcare Workers |
Commonly Used COVID-19 Pandemic Prevention Techniques
Since the outbreak of COVID-19, all the study participants have been at the forefront of the fight against this extremely contagious infectious disease. All of them were using different COVID-19 prevention methods. None of them were using a single method only (Table 2).
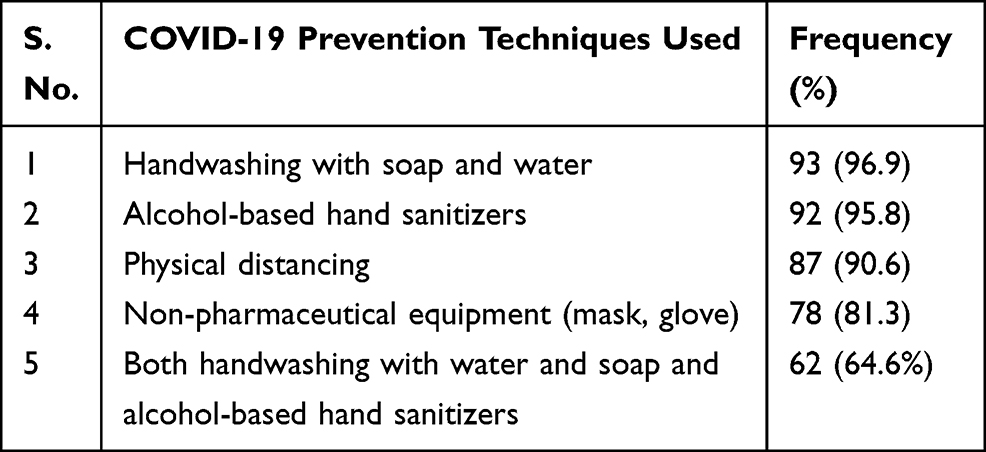 |
Table 2 COVID-19 Prevention Methods Practiced by Enrolled Healthcare Workers |
Self-Reported Knowledge of Respondents About Hand Hygiene by Alcohol-Based Hand Sanitizer
To prevent the spread of the COVID-19 pandemic, HCWs generally considered and practiced HH by ABHSs and handwashing with soap and water as an effective intervention. However, they had a different level of knowledge about HH by ABHS (Table 3).
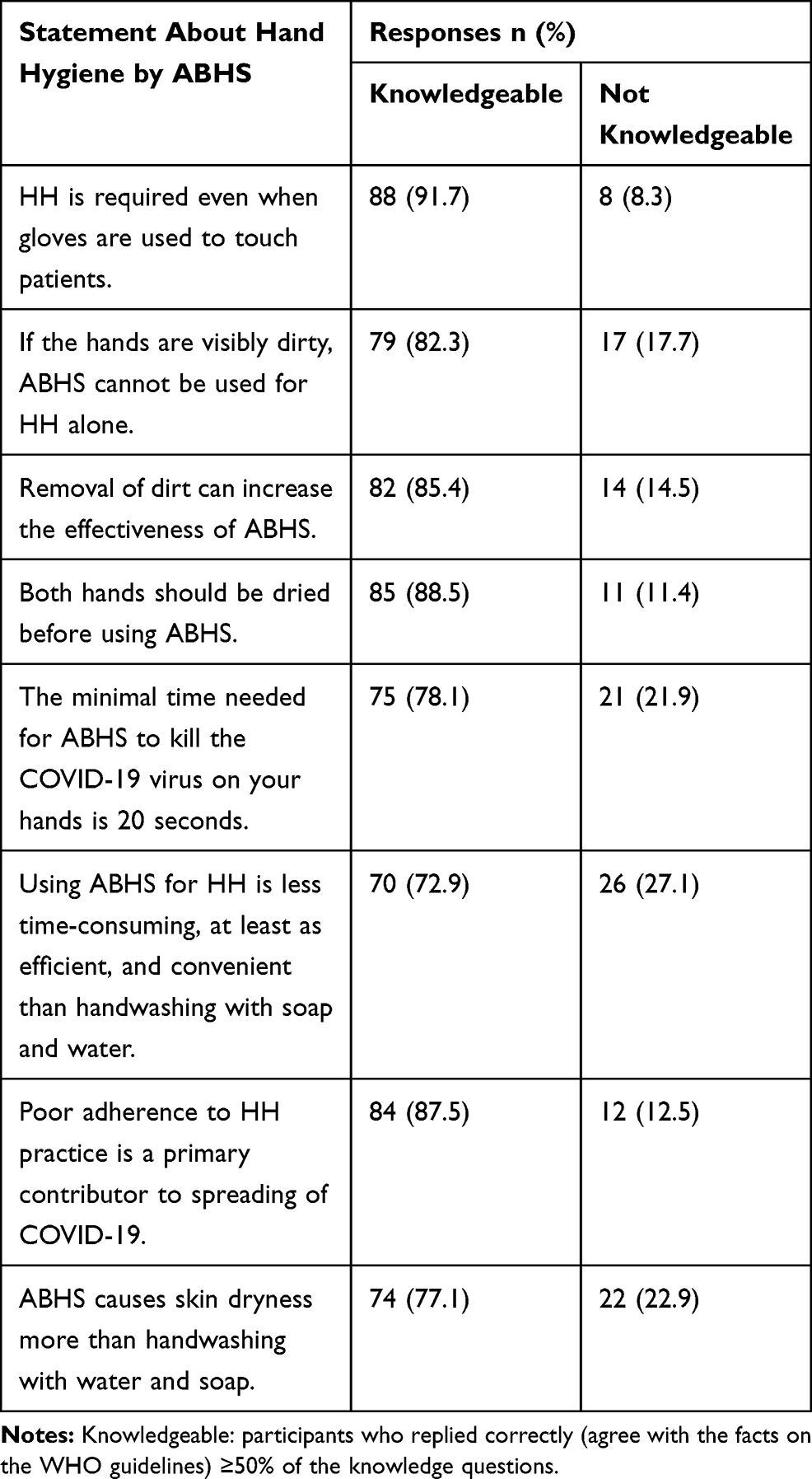 |
Table 3 Level of Respondent’s Knowledge Concerning Hand Hygiene by Alcohol-Based Hand Sanitizers |
Self-Reported Knowledge of Respondents on Alcohol-Based Hand Sanitizers Storage Condition
To keep the quality, safety, and effectiveness of ABHS, the respondents had a different level of knowledge on storage condition selection before and after use (Figure 1).
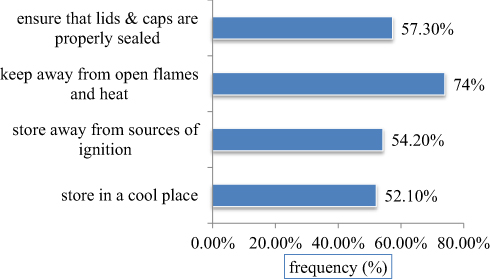 |
Figure 1 Knowledge of the respondents about the storage conditions for alcohol-based hand sanitizers. |
According to the present study, most of the study participants got information about the use of ABHS to prevent COVID-19 and its storage condition from the mass media 71 (74%); followed by books and published journals 33 (34.4%), discussion with co-workers 26 (27.1%), presence of posters for HH in the work area 14 (14.6%) and seminars conducted occasionally at hospital level 11 (11.5%).
The Self-Reported Attitude of Respondents Towards Hand Hygiene by Alcohol-Based Hand Sanitizers
According to the participants’ reply to questions used to evaluate the attitude, the entire study participants had favorable attitudes toward HH by ABHSs (Table 4).
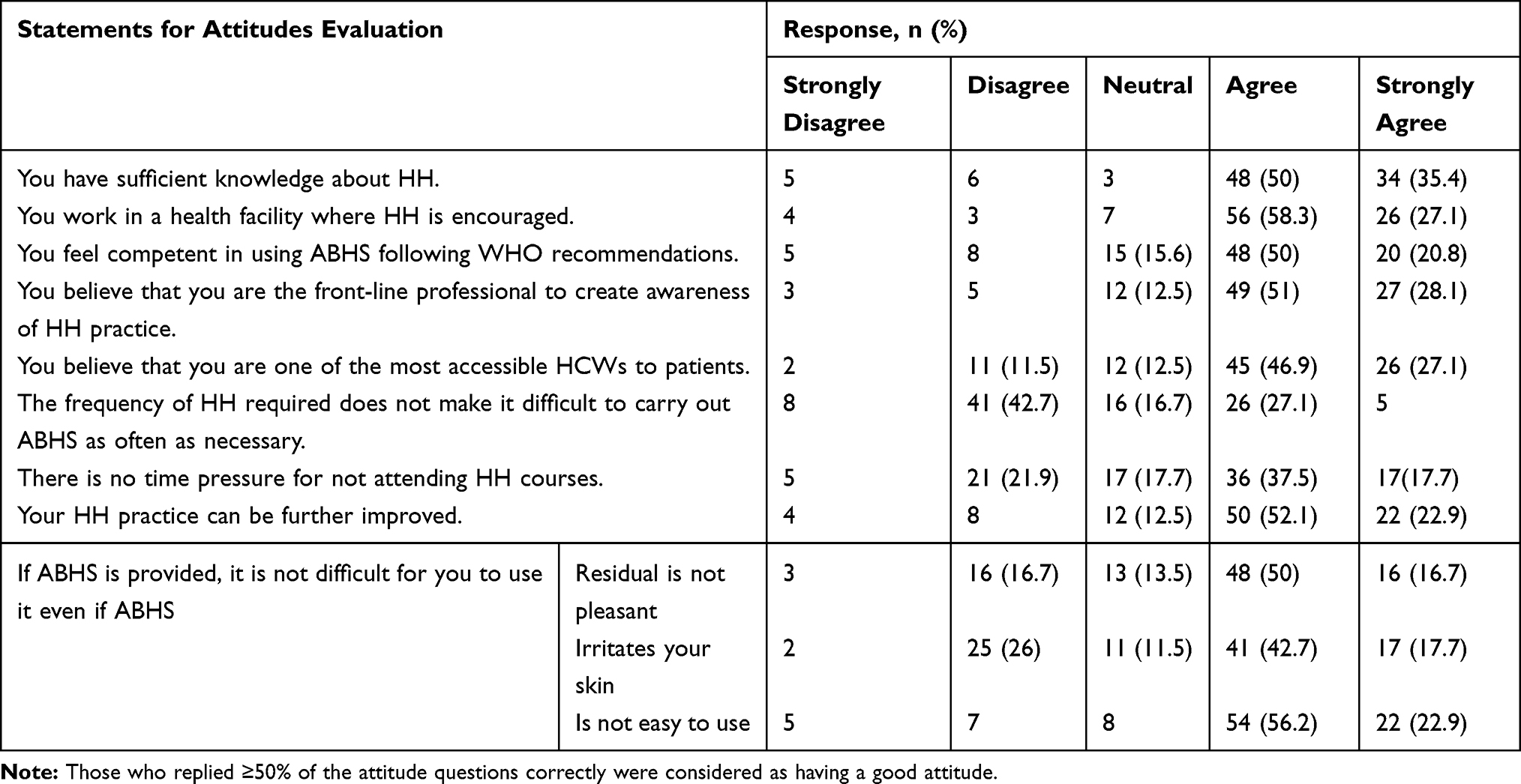 |
Table 4 The Self-Reported Attitude of Respondents Towards Hand Hygiene by Alcohol-Based Hand Sanitizers |
Self-Reported Compliance of Respondents to the WHO Recommended Alcohol-Based Hand Sanitizers Practices
Following the WHO’s current recommendation, compliance with ABHS uses at the five essential moments for HH per a single care sequence by HCWs had a gap and needed a concern (Table 5).
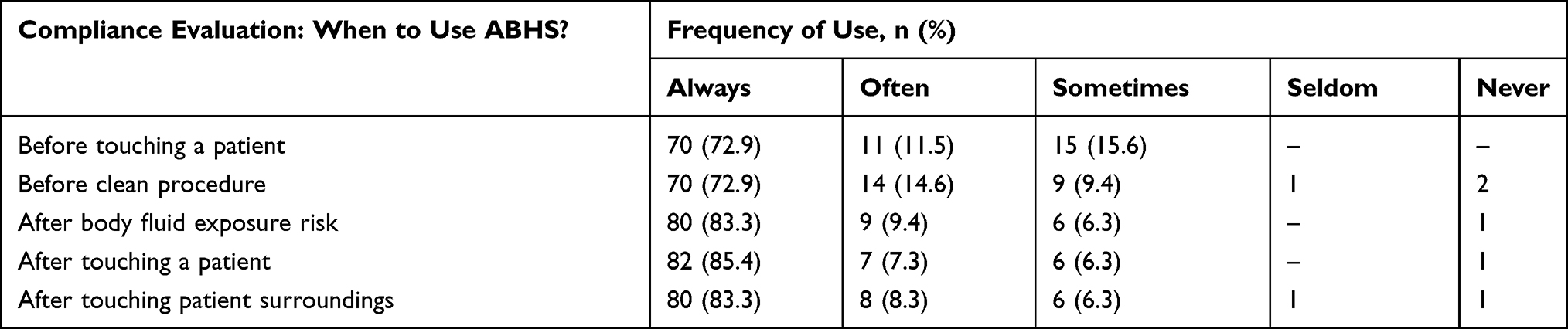 |
Table 5 Self-Reported Compliance of Respondents to Hand Hygiene Using Alcohol-Based Hand Sanitizers |
Most of the study participants (63 (65.6%)) are compliant with the ABHS duration of hand sanitizer recommended by the WHO (20–40 seconds).15 The others were non-compliant to the WHO recommendation (<20 sec= 29 (30.2%), >40 sec= 4(4.1%)).
Self-Reported Challenges During Alcohol-Based Hand Sanitizer Use
The present study finding showed that the majority of the respondents reported difficulties that might hinder the frequent and effective use of ABHR according to recommended by the WHO (Table 6).
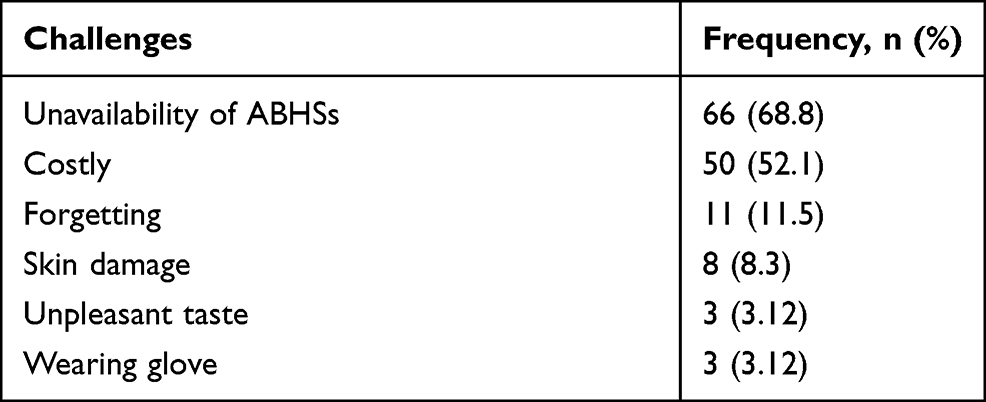 |
Table 6 Self-Reported Challenges Against Frequent and Effective Use of Alcohol-Based Hand Sanitizers |
Discussion
Following its outbreak, the alarmingly spread of COVID-19 is becoming a major global threat. Mainly HCWs are one of the highly exposed groups and had the likelihood of acquiring this disease. During the study period, there is no treatment discovered and no vaccine supply in Ethiopia. So to stay safe, HCWs practice prevention measures as the best solution. Therefore, effective prevention can be achieved through increasing their knowledge, attitude, and practice towards COVID-19 prevention and solving the challenges.
The current study assessed the knowledge, attitudes, practice, and challenges of HCWs regarding COVID-19 prevention and control. The survey data of this study demonstrated that all of the enrolled HCWs were using different prevention techniques. Commonly, they used hand hygiene (Table 2). The results might reveal that HCWs were practicing WHO recommended prevention techniques and had information on the global health crisis of COVID-19.2,19 The reasons for these positive results might include: the respondents’ educational status, their exposure to a lot of information about COVID-19 through different media, their responsibility to adhere to scientifically accepted and evidence-based principles of infection control, and the time of data collection period were during the pandemic got the attention.
The current study demonstrated that most of the HCWs were preferred and using ABHS with different justifications. The majority (93.8%) of the respondents had good knowledge about HH by ABHS uses to prevent and control the spreading of COVID-19 (Table 3). These results support recommendations reported by WHO15 and Oliveira et al (2017).25
The current study revealed that the answers to the following questions find comparatively more deficiency in the awareness of the respondents. The questions were using ABHS for HH is less time-consuming, efficient, convenient, and causes more skin dryness than handwashing with water and soap. Also, fewer than 75% of the study participants were aware of the standard storage condition recommended by the WHO (Figure 1). Therefore, HH education programs should be promptly re-viewed, and train-ing programs should be developed and implemented.
In the present study, univariate (binary logistic regression) analysis indicated that HCWs’ knowledge about HH by ABHS was not statistically associated with the sex difference (COR 0.552; 95% CI 0.105–2.894; P= 0.482) and years spent in a healthcare setting (COR 0.618; 95% CI 0.068–5.580; P =0.668). Multivariate analysis showed that HCWs who took training on COVID-19 prevention techniques were more than three times knowledgeable than untrained (AOR 3.65; 95% CI 0.41–32.56; P= 0.246) (Table 7).
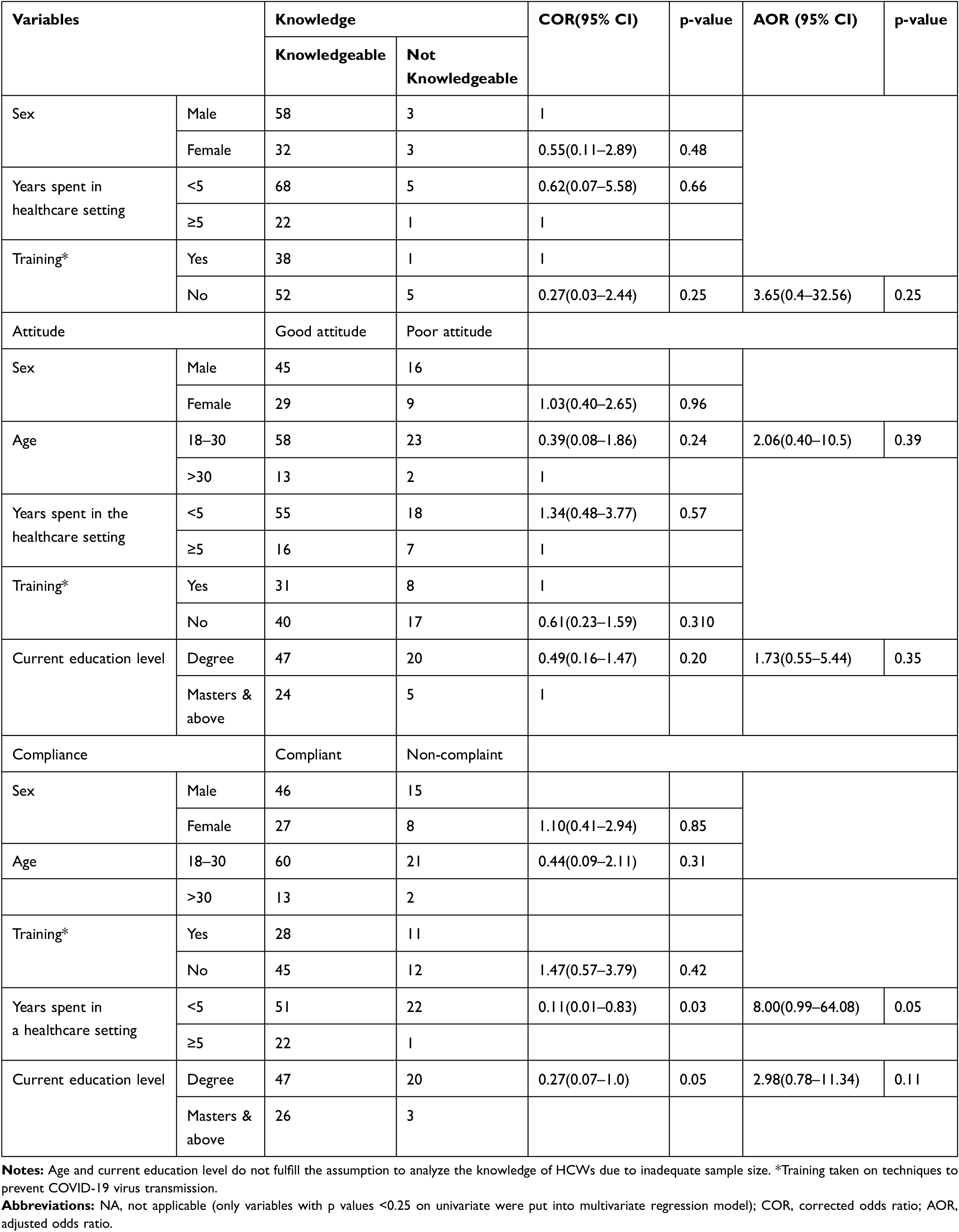 |
Table 7 Factors Related to Poor Knowledge, Attitude, and Practice of Hand Hygiene |
In the present study, most of the respondents (74%) had a favorable attitude towards their knowledge and practice of HH, mainly by ABHSs and the requirement of ABHSs in the work area. A similar finding was reported by a study done in a tertiary hospital, South West Nigeria (2011).17 The similarities might be due to the similar educational status and awareness of the study populations and similarities of the information. However, most of the respondents felt that their HH practice needed improvement. Some perception-related items that won relatively low scores should therefore be strengthened to maintain good HH.
According to this study’s results, univariate or multivariate statistical analysis (accordingly) showed that study participants’ differences in sex (p=0.96), age (p=0.39), years spent in a healthcare setting (p=0.57), and current education level (p=0.35) did not have a statistically significant association with their attitude towards HH by ABHS (Table 7). Although not statistically significant, respondents considered knowledgeable had a better attitude to ABHS than not knowledgeable (COR 0.676; 95% CI 0.118–4; P= 0.676).
The results of the current study showed that the majority of study participants (76%) were in line with the WHO suggested procedures. It showed more compliance to ABHS use at the five moments for hand hygiene than with other studies conducted at the University of Gondar teaching hospitals (2019)23 and in a tertiary university hospital in Istanbul (2014).24 The reason for this discrepancy might be due to the difference in sample size and study time. Additionally, the outbreak of COVID-19 may contribute to HCWs’ awareness of ABHS use.
Furthermore, self-evaluation of HH by ABHS showed that the lowest compliance was reported at using ABHS before touching a patient and before a clean procedure. This result of the present study (before touching a patient) was in line with the finding of a study conducted by Li et al (2015) in Inner Mongolia, China.27 The similarity might be due to similar educational status and awareness of the study populations.
The current study showed that compliance to HH by ABHS did not statistically vary with respondents’ age, taking training, current education level (Table 7). In univariate analysis, non-compliance with HH was not significantly associated with sex (COR 1.101; 95% CI 0.413–2.935; P= 0.848). This finding agrees with a study conducted in a tertiary university hospital in Belo Horizonte, Brazil (2015).25 It might be due to not a sufficient number of samples were used to identify the association.
In multivariate analysis, there was a statistical association between compliance to the five moments of HH recommended by WHO and attitude towards HH by ABHS (AOR 2.974; 95% CI 1.093 −8.093; P= 0.033). As a result, those who had a positive attitude had more than two times more compliance than the others. But there was no difference in compliance due to knowledge of ABHS use and compliance to practice it accordingly (COR 0.286; 95% CI 0.053–1.526; P= 0.143). This finding is not consistent with a study conducted in the Central Gondar Zone public primary hospitals, where knowledgeable study participants are 6.74 times more compliant than those with poor knowledge. The difference might be due to the sample size issue and study time (COVID-19 pandemic time).
A complex interplay of cognitive, socioeconomic, and technical factors may determine hand-washing practice among hospital-based HCWs. In this study, self-reported reasons for frequent lack of compliance to ABHS use included the following: lack of ABHS, increasing cost, experienced health risks, forgetting wearing the glove, and others. Lack of ABHS and increasing cost were the most common (Table 6). This finding is in line with a study conducted in Ruth K.M. Pfau Civil Hospital, Karachi (2019),26 but higher than a result from the study conducted in a tertiary university hospital in Istanbul (2014).24 The difference should be due to the more consumption of ABHS, in the healthcare setting and community, during the study period. During this study period, there was an outbreak and rapid prevalence of the COVID-19 pandemic.
According to the present study, most study participants experienced different health risks, commonly skin dryness, skin irritation, unpleasant taste, ocular irritation, cough, gastrointestinal disturbances, and others. This result agrees with a study conducted in a tertiary university hospital in Belo Horizonte, Brazil (2015)25 and Inner Mongolia, China (2015)27 These risks become one of the reasons for not adhering to the WHO recommended “My five moments for hand hygiene” to use ABHS by 8 (8.5%) respondents.
Strength and Limitation of the Study
The present study characterized the HH knowledge, attitudes, and challenges of performing HH by ABHS and identified gaps that are essential to control outbreaks (COVID-19). It provided substantial evidence to facilitate the development and implementation of an action plan for strengthening the program for the proper use of ABHS to prevent the risks. These data also showed the need for training to enhance compliance with the use of ABHS. Furthermore, the data can be used for further analysis by the scientific community.
This study is subject to limitations. As this study was not observational, this study has some limitations in terms of the self-reporting of HH performance and volunteer bias. What the study participants respond can be different from what they practice in real-life situations. Additionally, the number of study participants was not sufficient to distinguish statistically significant results and may be challenging to generalize the findings of the study.
Conclusion
Most HCWs performed HH by ABHS to prevent and monitor the transmission of the COVID-19 virus. Most of them had good self-reported knowledge and attitude toward using ABHS. There was no clear evidence showing a disparity in HCW’s knowledge and attitude towards using ABHS for HH due to sex and years of experience difference. However, study participants considered as knowledgeable had a favorable attitude towards HH by ABHS. Additionally, those who took training on COVID-19 prevention techniques had more than three times knowledgeable than untrained. Also, most of the respondents adopted the HH practice by ABHS at the five essential moments recommended by the WHO. The level of compliance significantly depends on years spent in the healthcare setting. Furthermore, the lack of ABHS and the increase in its cost were reported as the most common reasons for not using ABHS as needed. Additionally, reported skin irritation, unpleasant taste, and skin dryness as ABHS health risks were reported and may contribute to the compliance problem. Generally, there were some knowledge, attitude, and practice evaluation items with relatively low scores that showed some room for improvement.
Recommendation
The present study identified the vital gaps of HCWs’ knowledge and attitude, and non-compliance on certain occasions, as well as challenges to the success of HH by ABHS according to WHO guidelines. They warranted some room for improvements. Therefore, the authors suggested multiple strategies (multimodal and multidisciplinary approach). So the regular and public bodies should catalyze local production and supply of low irritating ABHSs (containing emollients) according to the WHO guideline, systemic and advanced HH training programs to enhance awareness, promote compliance, and behavioral change toward HH.
Abbreviations
ABHS, alcohol-based hand sanitizer; COVID-19, coronavirus disease; HH, hand hygiene; HCW, healthcare worker; JMC, Jimma Medical Center.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work and state there are no potential conflicts of interest that exist concerning the research, authorship, and publication of this article.
References
1. WHO. Novel Coronavirus–China; 2020. Available from: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/.
2. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199–1207. doi:10.1056/NEJMoa2001316
3. Lai -C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. doi:10.1016/j.ijantimicag.2020.105924
4. McKibbin WJ, Fernando R. The global macroeconomic impacts of COVID-19: seven scenarios. Available from: https://www.brookings.edu/wp-content/uploads/2020/03/20200302_COVID19.pdf.
5. Socio-economic impact of COVID-19. Available from: https://www.undp.org/content/undp/en/home/coronavirus/socio-economic-impact-of-covid-19.html.
6. COVID-19 pandemic|UNDP. Available from: https://www.undp.org/content/undp/en/home/coronavirus.html.
7. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395:1973–1987. doi:10.1016/S0140-6736(20)31142-9
8. Modes of transmission of the virus causing COVID-19: implications for IPC precaution recommendations. Available from: https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations.
9. Interim recommendations on obligatory hand hygiene against transmission of COVID-19. Available from: https://www.who.int/publications/m/item/interim-recommendations-on-obligatory-hand-hygiene-against-transmission-of-covid-19.
10. Hand hygiene recommendations. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/hand-hygiene.html.
11. Q & A for consumers: hand sanitizers and COVID-19. Available from: https://www.fda.gov/drugs/information-drug-class/qa-consumers-hand-sanitizers-and-covid-19.
12. Gold NA, Mirza TM, AVVa U Alcohol sanitizer. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513254/.
13. Kumar D, Kaushal SK, Kumar G, Prakash V, Prakash P, Nath G. Evaluation of the antibacterial activity of commonly used alcohol-based hand sanitizers on common pathogenic bacteria. Indian J Appl Res. 2015;5(3):562–564.
14. Saito H, Inoue K, Ditai J, et al. Alcohol-based hand rub and incidence of healthcare-associated infections in a rural regional referral and teaching hospital in Uganda (‘WardGel’ study). Antimicrob Resist Int. 2017;6(1):129. doi:10.1186/s13756-017-0287-8
15. World Health Organization. WHO guidelines on hand hygiene in health care: first global patient safety challenge clean care is safer care. Geneva: the Organization; 2009: Available from: https://apps.who.int/iris/bitstream/handle/10665/44102/9789241597906_eng.pdf?sequence=1.
16. Qiao F, Zong Z, Yin W, Huang W, Zhuang H. O075: successful implementation of the World Health Organization hand hygiene improvement strategy in a teaching hospital, China. Antimicrob Resist Infect Control. 2013;2(Suppl1):O75. doi:10.1186/2047-2994-2-S1-O75
17. Ekwere TA, Okafor IP. Hand hygiene knowledge and practices among healthcare providers in a tertiary hospital, southwest Nigeria. Int J Infect Control. 2013;9:i4. doi:10.3396/IJIC.v9i4.032.13
18. Onyedibe KI, Shehu NY, Pires D. Assessment of hand hygiene facilities and staff compliance in a large tertiary health care facility in northern Nigeria: a cross-sectional study. Antimicrob Resist Infect Control. 2020;9:30. doi:10.1186/s13756-020-0693-1
19. Coronavirus disease (COVID-19) situation report–104. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200503-covid-19-sitrep-104.pdf?sfvrsn=53328f46_4.
20. Jemal S. Knowledge and practices of handwashing among health professionals in Dubti Referral Hospital, Dubti, Afar, Northeast Ethiopia. Adv Prev Med. 2018;7. doi:10.1155/2018/5290797
21. A simple guide to the WHO approach to hand hygiene improvement. Available from: https://www.who.int/gpsc/news/simple_guideline/en/.
22. Ontario. Provincial infectious diseases advisory committee. Best practices for hand hygiene in all health care settings; 2010: Available from: http://www.health.gov.on.ca/english/providers/program/infectious/diseases/ic_hh.html.
23. Engdaw GT, Gebrehiwot M, Andualem Z. Hand hygiene compliance and associated factors among health care providers in Central Gondar zone public primary hospitals, Northwest Ethiopia. Antimicrob Resist Infect Control. 2019;8:190. doi:10.1186/s13756-019-0634-z
24. Karaaslan A, Kepenekli Kadayifci E, Atıcı S, et al. Compliance of healthcare workers with hand hygiene practices in neonatal and pediatric intensive care units: overt observation. Interdiscip Perspect Infect Dis. 2014;2014:1–5. doi:10.1155/2014/306478
25. Oliveira AC, Gama CS, Paula AO. Adherence and factors related to acceptance of alcohol for antiseptic hand rubbing among nursing professionals. Rev Esc Enferm USP. 2017;51:e03217. doi:10.1590/s1980-220x2016037803217
26. Ahmed J, Malik F, Memon ZA, et al. Compliance and knowledge of healthcare workers regarding hand hygiene and use of disinfectants: a study based in Karachi. Cureus. 2020;12(2):e7036.
27. Li Y, Wang Y, Yan D, Rao CY. Self-reported hand hygiene practices, and feasibility and acceptability of alcohol-based hand rubs among village healthcare workers in Inner Mongolia, China. J Hosp Infect. 2015;90(4):338–343. doi:10.1016/j.jhin.2015.04.006
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.