Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Knowledge, Attitude, and Preventive Practices Towards COVID-19 Among Students of Ethiopian Higher Education Institutions
Authors Berihun G ![]() , Walle Z
, Walle Z ![]() , Teshome D
, Teshome D ![]() , Berhanu L
, Berhanu L ![]() , Abebe M, Ademas A
, Abebe M, Ademas A ![]() , Gizeyatu A, Keleb A
, Gizeyatu A, Keleb A ![]() , Malede A
, Malede A ![]() , Atikilt G
, Atikilt G ![]() , Teym A
, Teym A ![]() , Adane M
, Adane M ![]()
Received 4 June 2021
Accepted for publication 22 July 2021
Published 10 August 2021 Volume 2021:14 Pages 2123—2136
DOI https://doi.org/10.2147/JMDH.S322495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Gete Berihun,1 Zebader Walle,2 Daniel Teshome,3 Leykun Berhanu,1 Masresha Abebe,1 Ayechew Ademas,1 Adinew Gizeyatu,1 Awoke Keleb,1 Asmamaw Malede,1 Getaneh Atikilt,2 Abraham Teym,4 Metadel Adane1
1Department of Environmental Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 3Department of Anatomy, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 4Department of Environmental Health, College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia
Correspondence: Gete Berihun Email [email protected]
Introduction: COVID-19 has been a global public health problem since December 2019. Higher education institutions are risky areas for the transmission of COVID-19. But, still there is insufficient information on the prevention of the disease in this setting.
Objective: To assess knowledge, attitude, and prevention practices towards COVID-19 among students of Ethiopian higher education institutions.
Methods: Institutin -based cross-sectional study design was conducted from December 1 to 30, 2020 among randomly selected 407 undergraduate students from higher education institutions in Ethiopia. The outcome variables were knowledge, attitude, and practices towards COVID-19. Binary logistic regression models at 95% confidence interval (CI) were used to determine the factors affecting knowledge, attitude, and practices towards COVID-19. In multivariable analysis, variables with a p-value of less than 0.05 were considered statistically significant and independently associated with outcome variables at 95% CI.
Results: About 75.9% (95% CI: 72.2– 79.9%) of University students had a good knowledge, 62.4% (95% CI: 58.2– 67.1%) had a positive attitude, and 56.8% (95% CI: 52.6– 61.9%) had a good COVID-19 prevention practices. Students over the age of 30 (AOR=5.8; 95% CI: 1.5, 10.6), third-year students (AOR=3.1; 95% CI: 1.1, 8.9), and being health science students (AOR=4.4; 95% CI: 2.2, 8.9) were significantly associated with a good knowledge towards COVID-19. Urban residents (AOR=0.6; 95% CI: 0.3– 0.9), having an average family monthly income of $75USD (AOR=3.5; 95% CI: 1.8– 6.7), use of at least one type of social media (AOR=4.7; 95% CI: 1.7– 12.9), and having a positive attitude (AOR=2.2; 95% CI: 1.3– 3.5) were significantly associated with COVID-19 prevention practices.
Conclusion: Despite three-fourths of the participants had a good knowledge, the attitude and prevention practices were low. Age, study year, College of study, presence of chronic illnesses, use of social media, family income, and residence were factors of knowledge, attitude, and prevention practices towards COVID-19. Hence, multiple information dissemination strategies using multiple media outlets should be implemented continuously.
Keywords: COVID-19, Knowledge, Attitude, Practice, Higher education, Ethiopia
Introduction
Since late December 2019, the human population became in a global health crisis due to the COVID-19 pandemic caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2).1 The virus is a zoonotic pathogen that causes and spread illnesses among humans and a variety of animals including cattle, camels, cats, and bats. The disease was initially identified in Wuhan, Hubei Province, China.2–4 The World Health Organization (WHO) declared the disease a Public Health Emergency of International Concern on January 31, 2020, and as a global pandemic on March 11, 2020.5–7
As of mid-2021, the exact mode of transmission of the novel coronavirus was unknown.8 However, it has been hypothesized that it can be transmitted through droplets, airborne transmission, and human contact.7,9,10 The signs and symptoms of the disease may range from asymptomatic to mild (such as fever, dry cough, fatigue, myalgia, dyspnea, and shortness of breath) to severe (such as pneumonia, SARS, kidney failure, cardiac injury respiratory failure, and acute respiratory distress syndrome).1,5–7 Elders and patients who have a chronic medical illnesses such as hypertension, cardiac disease, lung disease, cancer, and diabetes are more vulnerable to COVID-19 infection. Due to the absence of an effective cure, early recognition of symptoms and seeking supportive care is very important for recovery.7,10
About 44% of cases are asymptomatic but can spread the infection to others. Even though virus particles can only survive for a short time in the air, they can survive longer if they come into contact with hard surfaces.11 Effective antivirals and vaccines have begun to be administered in some countries, and effective therapeutic solutions have yet to be approved.12
COVID-19 had spread to over 219 countries across the globe. As of March 31, 2021, 10:50 a.m., there were 128,850,007 cases and 2,817,416 deaths were reported.13 The first case of COVID-19 in Ethiopia was reported on March 13, 2020,14,15 and there were 204,521 cases and deaths as of March 31, 2021. Furthermore, more than 44,000 people in Ethiopia were living with the virus as of March 31, 2021.16 Although COVID-19 affects all countries of the globe, the severity increased in developing countries, including Ethiopia. This may be due to a poor healthcare delivery system, limited resources, low living standards, cultural norms, low socioeconomic status, and environmental factors. The pandemic affects people's physical and mental health, and political, economic, and social stability.17 Many Universities across the world had moved to an emergency remote teaching via online platforms for about a year since the occurrence of COVID-19.18 Universities in Ethiopia were opened after 8 months lock down following permission from Ethiopian Ministry of Health.
The transmission of COVID-19 is very high among University students due to the presence of different contributing factors. They are very active both on social media and in the community.1 They live away from their families, who make an opportunity to make judgments by their own. Furthermore, they may participate in different activities like sport clubs, and part-time work which makes good opportunity to contact COVID-19 pandemic.12
The battle against COVID-19 is still ongoing, and almost all countries have implemented different prevention measures including partial/complete lockdown to curb the transmission of the virus.1 Furthermore, different prevention measures, such as provision of handwashing facilities, face masks on free, alcohol-based hand sanitizer, reducing the number of students by half in dormitories and classes and temperature measurement, are implemented to divert the transmission of the disease. Prevention and control of the disease requires knowledge, attitude, and prevention practices (KAP). Despite researches were done on KAP of University students in different parts of the world, there are limited studies in the case of Ethiopia. In a study conducted only in Mizan Tepi University students, 47%, 54%, and 42.8% of the students had a good knowledge, a positive attitude, and a good prevention practices towards COVID-19, respectively.19 Therefore, assessing KAP of student from different institutions has a great role in representing the whole higher education institutions in Ethiopia. Hence, the finding of the study will have a vital role in reduction disease transmission and designing an intervention to control the transmission of the disease. Therefore, the study was aimed to assess knowledge, attitude, and prevention practices towards COVID-19 among students of Ethiopian Higher Education Institutions.
Materials and Methods
Study Design, Period, and Setting
An institutional-based cross-sectional study design was conducted among students in Ethiopian higher education institutions from December 1 to 30, 2020. In Ethiopia, there are about 45 public and 5 private Universities. Ten of the public universities are found in Amhara Regional State. The study was conducted at three Universities from the Amhara Regional State, namely Wollo University, Debre Markos University, and Debre Tabor University. The public Universities of Ethiopia have an average intake capacity of more than 10,000 students.
Source and Study Population
The source population of the study was all Ethiopian higher education institution students. The study population was students from randomly selected higher education institutions in Ethiopia.
Inclusion Criteria
Undergraduate students of Ethiopian higher education institutions were included in the study.
Exclusion Criteria
First-year students, night and extension students, and those who were unable to respond due to serious illness during the data collection period were excluded from the study.
Sample Size Determination
The sample size was determined using the single population proportion formula considering the following assumptions :10
Zα/2 is the standard normal variable value at (1-α) % CI (α is 0.05 with 95% CI, Zα/2 = 1.96), an estimate of the proportion (p) of knowledge, attitude, and prevention practices was considered as 50%, and margin of error (d) 5%. The sample size becomes 384, and adding of 10% non-response rate, the final sample size was calculated to be 422.
Sampling Technique and Procedures
Initially, out of ten Universities found in the Amhara Regional State, three of them were randomly selected, namely Wollo University, Debre Tabor University, and Debre Markos University, using the lottery method. Then, the number of participants from each University was allocated proportionally based on the number of students at each University. Hence, 115 study participants from Debre Tabor University, 132 from Debre Markos University, and 160 study participants from Wollo University were selected. Then, four colleges, namely, Health Sciences, Business and Economics, Agriculture, and Natural Sciences and 12 Departments (Environmental Health Sciences, Pharmacy, Nursing, Accounting, Management, Marketing, Animal Sciences, Agro-economics, Forestry, Chemistry, Sport Science, and Statistics) were selected randomly using the lottery method from the three selected Universities. The lists of all students from the selected Departments were obtained from each Department. As a result, the selection of study participants was done by using a simple random sampling technique using the lists of the students’ grade submissions from the A+ software from the departments as a sampling frame.
Operational Definitions
Good Knowledge
Knowledge was measured using 14 questions consisting of signs and symptoms, risk groups and prognosis, methods of transmission, and preventive methods. Each question consisted of “Yes” and “No” options. Each correct answer was given 1 point, while an incorrect response was given 0 point. The knowledge score varied from 0 to 14, with a cutoff ≥11.2 or 80% and above was taken as having a good knowledge towards COVID-19.20
Poor Knowledge
Measured using 14 questions, total knowledge scores ranged from 0 to 14 while a cut-off level of <11.2 or scored less than 80% was taken as having poor knowledge towards COVID-19.20
Positive Attitude
Attitude was measured using 11 items with each response categorized based on Likert scale measurements with strongly agree (5 points), agree (4 points), neutral (3 points), disagree (2 points), and strongly disagree (1 point). The attitude scores varied from 11 to 55, with an overall score of ≥44 (80%) considered as a positive attitude toward COVID-19 prevention measures.3
Negative Attitude
The attitude scores varied from 11 to 55, with an overall score of <44 (less than 80%) considered as a negative attitude towards COVID-19 prevention measures.3
Good Practice
Practice was measured using 12 questions. A participant was given 1 point for each prevention measure practiced correctly, while 0 point was given for each one not practiced correctly. From a range of total practice scores from 0 to 12, an overall score of ≥9 (75%) was considered having a good practice of COVID-19 prevention.20,21
Poor Practice
Practice scores ranged from 0 to 12, from which an overall score of <9 (less than 75%) was considered as having a poor practice of COVID-19 prevention.20,21
Data Collection and Quality Assurance
The data was collected using a pre-tested structured questionnaire which was adapted from published articles.10,12,19,22–27 The questionnaire consisted of four sections including Part I: socio-demographic characteristics of the participants including sources of information about COVID-19 and related chronic medical history; Part II: knowledge-related items; Part III: attitude of the participants toward COVID-19 prevention measures; and Part IV: prevention practices of COVID-19. The questionnaire was prepared in English, translated to the local language (Amharic), and then re-translated to English to ensure consistency. The tool was pre-tested in 5% of the final sample size in Woldia University students to ensure the validity of the questionnaire. Based on the feedback of the pre-test, amendments, such as the ordering of questions, avoiding of less important questions, and editing of unclear questions, were done accordingly.
A one-day training was given for both data collectors and supervisors on the overall aim of the study, the contents of the tool, and ethical issues. Data were collected using a self-administered questionnaire by three Health Officers. . The supervision was conducted daily by two Master’s degree-holders in Public Health who ensured that appropriate corrections of the collected data were done accordingly. Furthermore, double data entry was done to control data entry errors, and data cleaning was carried before statistical analysis. The reliability coefficient of Cronbach’s alpha for knowledge, attitude, and infection prevention practice of COVID-19 was 0.74, 0.81, and 0.76, respectively, which is an acceptable range.
Data Management and Analysis
The data was entered into Epi-Data version 4.6 and exported to the Statistical Package for Social Science (SPSS) version 25.0 software for data cleaning and analysis. Descriptive statistics such as frequencies and percentages were determined for categorical variables, while mean with standard deviation was determined for continuous variables.
The associations between independent variables and knowledge, attitude, and infection prevention practice of COVID-19 were determined using a binary logistic regression model at 95% CI. Three models were performed to separately assess the determinant factors for knowledge, attitude, and infection prevention practice of COVID-19. Data were analyzed using bivariable analysis (COR [crude odds ratio]) and multivariable analysis (AOR [adjusted odds ratio]) using binary logistic regression at 95% CI. Those variables with p-values of less than 0.25 in the bivariable analysis were entered into the multivariable analysis. In turn, those variables with a p-value of less than 0.05 in multivariable analysis were considered as significantly associated with knowledge, attitude, and preventive practice at 95% CI.
The presence of multicollinearity among independent variables was checked for each variable using standard error at the cutoff value of −2 to +2, which showed that all independent variables in the study have no multi-collinearity. Model fitness was checked using the Hosmer–Lemeshow test and found a p-value of 0.680, 0.742, and 0.934 for knowledge, attitude, infection preventive practice, respectively, and all models were fit.
Results
Socio-Demographic Characteristics of Study Participants
A total of 407 university students participated in the study with a response rate of 96.4%. Almost half 202 (49.6%) of the participants were males. The majority of the participants were in the age range of 20–24, of Orthodox religion, and in their second year of study, with 300 (73.7%), 349 (85.7%), and 174 (42.8%), respectively. Furthermore, fewer than half 167 (41%) of the participants were Health Science students. Finally, 30 (8.1%) participants had a history of one or more chronic medical illnesses (Table 1).
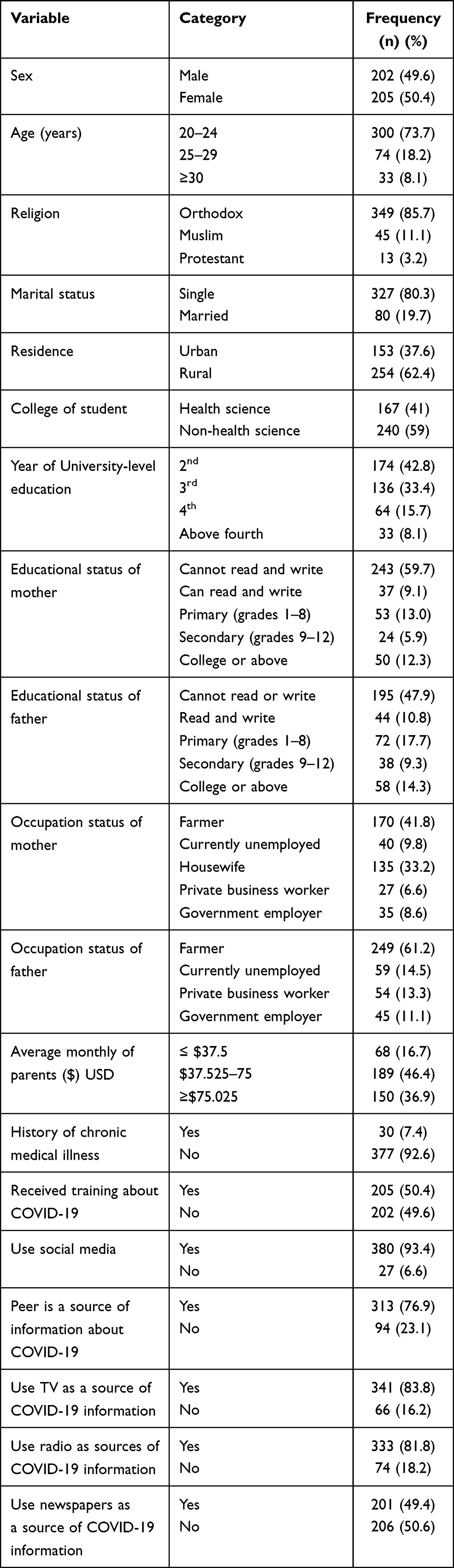 |
Table 1 Socio-Demographic Characteristics Among Students at Universities in Amhara Regional State, Ethiopia December 1 to 30, 2020 |
Knowledge of Respondents Towards COVID-19
Three-fourths 309 (75.9%; 95% CI: 72.2–79.9%) of the university students had good knowledge about COVID-19, while 98 (24.1%; 95% CI: 20.1–27.8%) of them had poor knowledge. The mean knowledge score of the respondents was 12.1±1.2 (8–14). Almost all 396 (97.3%) of the participants knew the major signs and symptoms of COVID-19 infected persons. But, more than half 235 (57.7%) of the participants knew less common signs and symptoms of COVID-19 infected persons. The finding also revealed that almost all 378 (92.9%) of the participants knew that the vaccine has been developed for COVID-19 but a lower number of participants knew that COVID-19 can be transmitted even in the absence of fever in the infected person. Furthermore, about 367 (90.2%) of the participants knew that wearing a general face mask is one of the COVID-19 preventive measures (Table 2).
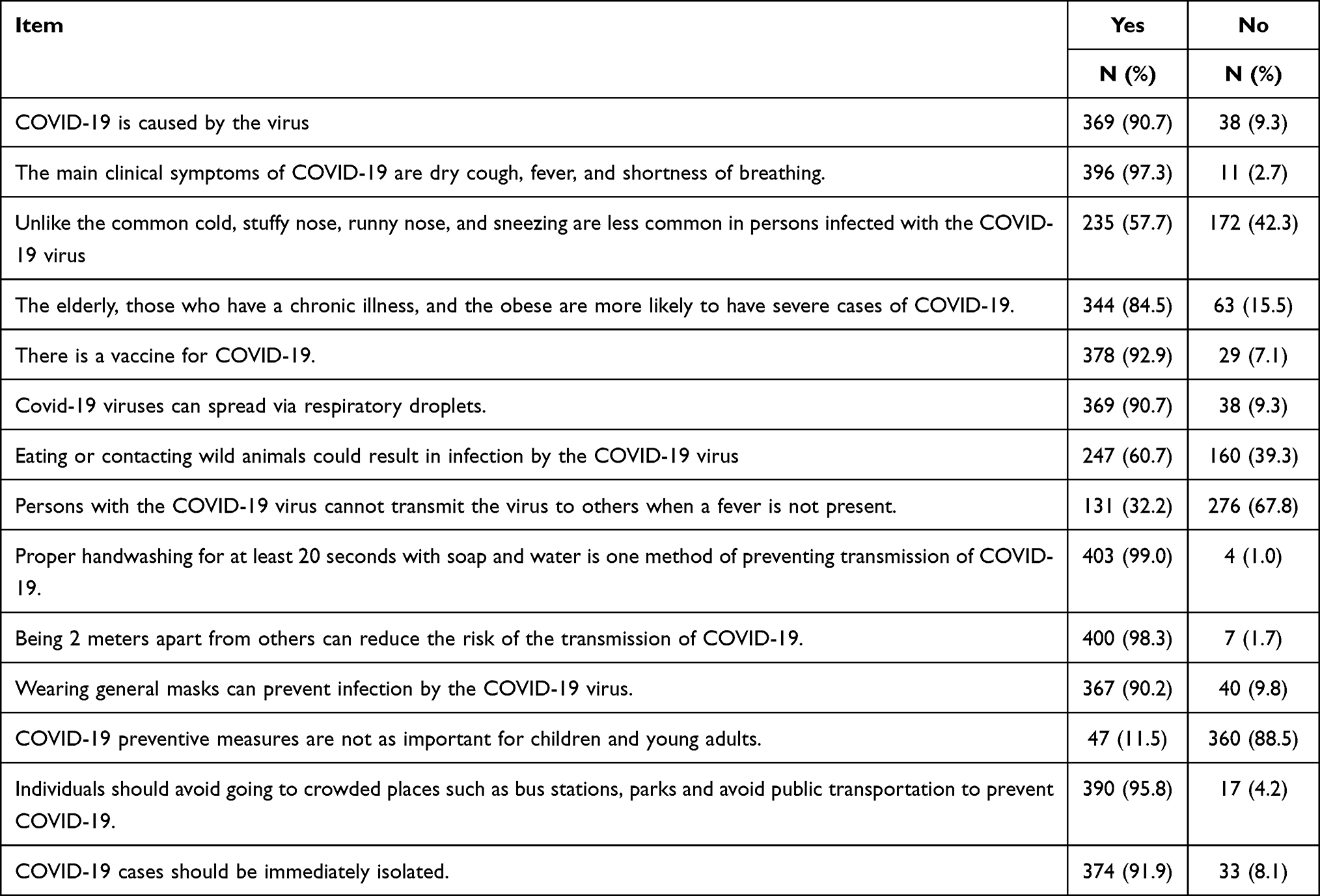 |
Table 2 Knowledge About COVID-19 Among Students at Universities in Amhara Regional State, Ethiopia from December 1 to 30, 2020 |
Attitude of Respondents Towards COVID-19
Fewer than two-thirds 254 (62.4%; 95% CI: 58.2–67.1%) of the university students had a positive attitude toward practices to prevent COVID-19, whereas 153 (37.6%; 95% CI: 32.9–41.8%) had a negative attitude. The average attitude score of the respondents was 43.4±4.8 (27–53). This study found that only 49 (12%) of participants had a positive attitude towards the belief that Ethiopia is in a good position to control the COVID-19 viruses within a short time. Furthermore, fewer than half 191 (46.9%) of the participants agreed that if they are infected with COVID-19, they will go to healthcare facilities for treatment. Just over half 222 (54.5%) of the participants agreed that they can be infected with COVID-19 despite their good immunity status (Table 3).
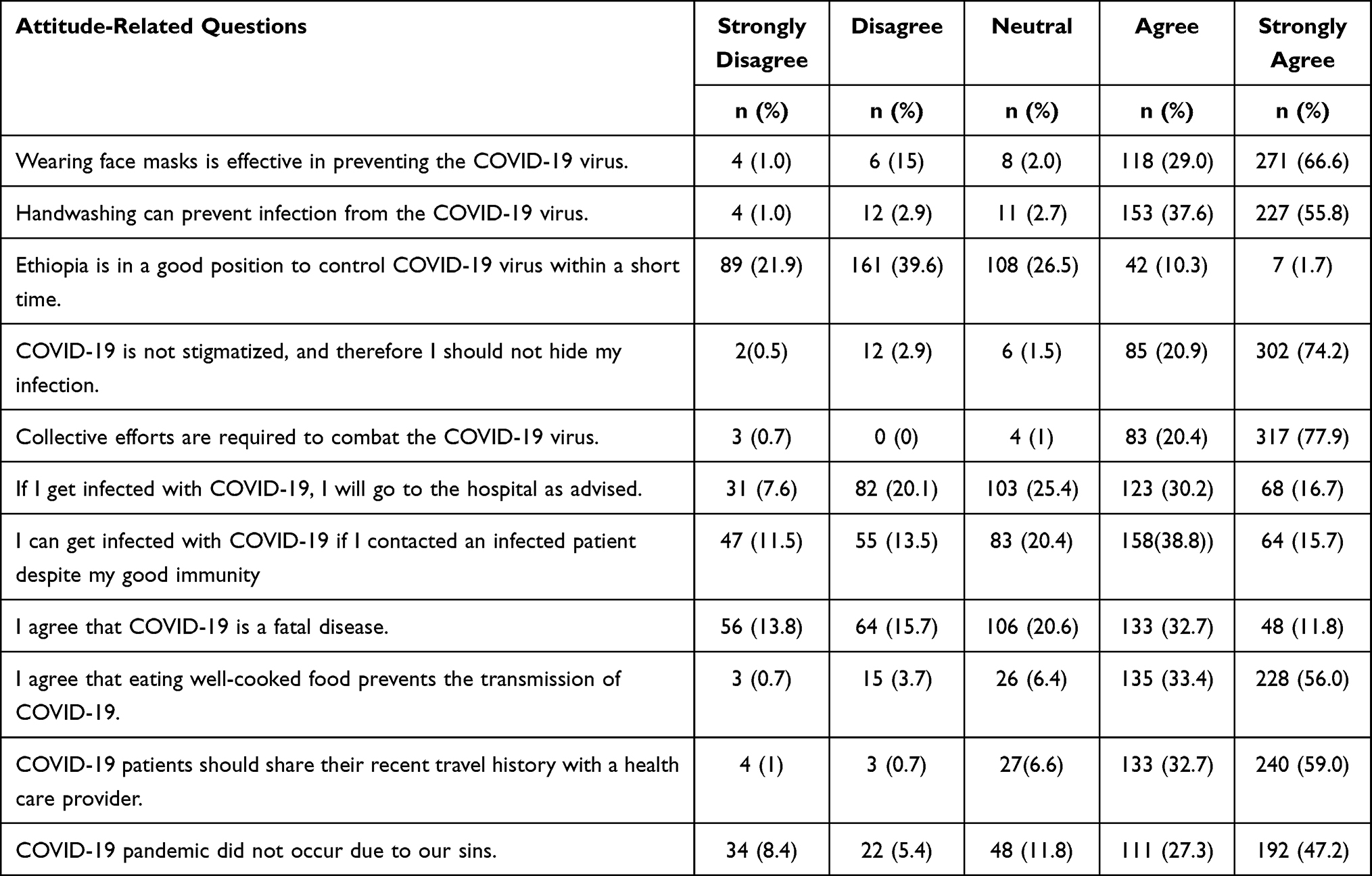 |
Table 3 Attitude Towards COVID-19 Prevention Among Students at Universities in Amhara Regional State, Ethiopia from December 1 to 30, 2020 |
Prevention Practices of Respondents Towards COVID-19
More than half 231 (56.8%; 95% CI: 52.6–61.9%) of the participants had a good COVID-19 prevention practices, while 176 (43.2%; 95% CI: 38.1–47.4%) had poor practices. The mean score of respondents towards prevention practice of COVID-19 was 8.96 ± 2.02. Almost all 363 (89.2%) of the participants frequently practiced handwashing with water and soap for at least 20 seconds. But, a lower number of participants 331 (81.3%) avoided handshaking after the occurrence of COVID-19. Further, fewer than three-fourths 296 (72.7%) of the participants used alcohol-based hand sanitizer in the absence of water and soap when outside of their dormitories. But, only 254 (62.4%) of the participants wear general facemasks frequently whenever needed as a prevention measure against COVID-19. Similarly, more than two-thirds 285 (70%) participants avoid touching mouths, noses, and eyes with unwashed hands. Finally, nearly three-quarters 301 (74%) of the participants frequently cleaned surfaces with which they had contact in their dormitories like tables, doors, light switches, desks, and phones (Table 4).
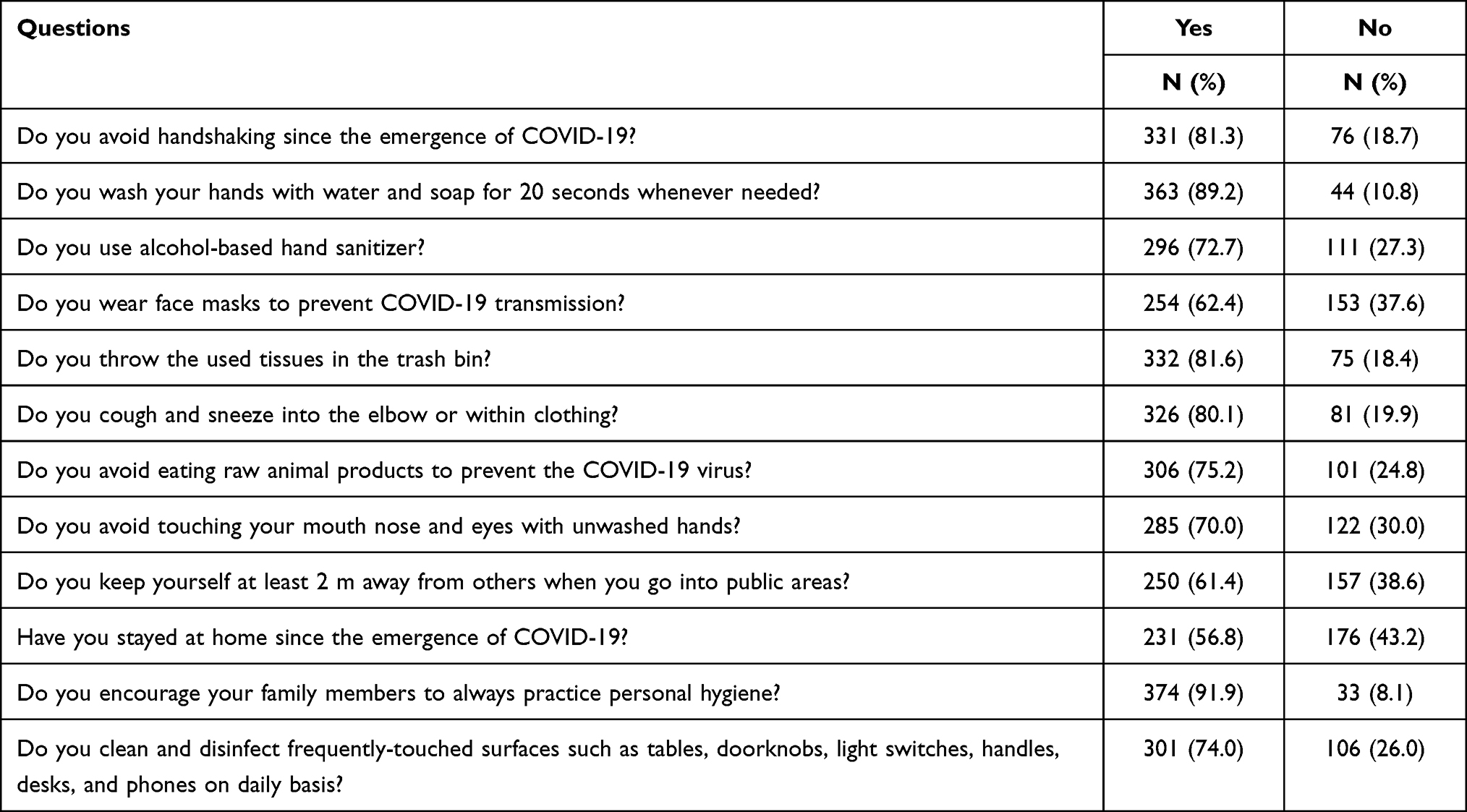 |
Table 4 Infection Prevention Practice Against COVID-19 Among Students at Universities in Amhara Regional State, Ethiopia from December 1 to 30, 2020 |
Factors Associated with Knowledge about COVID-19
A multivariable lgistic regressin analysis of the first model indicated that age of the participants, study year, college of study, and use of television as a source of information about COVID-19 were statistically significant concerning knowledge about prevention of COVID-19. The finding revealed that those respondents who were ≥30 years old were 5.8 (95% CI: 1.5–23.0) times more likely to have good knowledge about COVID-19 than those who were 20–24 years old. Similarly, participants in their fourth year of study were 3.1 (95% CI; 1.1–8.9) times more likely to have good knowledge of COVID-19 than those who were second-year students. Further, participants who were Health Science students were 4.4 (95% CI; 2.2–8.9) times more likely to have a good knowledge of COVID-19 than those who were non-Health Science students. Finally, participants who used television as a source of information about COVID-19 were 4.2 (95% CI; 1.7–10.0) times more likely to have good a knowledge about COVID-19 than those who did not use it (Table 5).
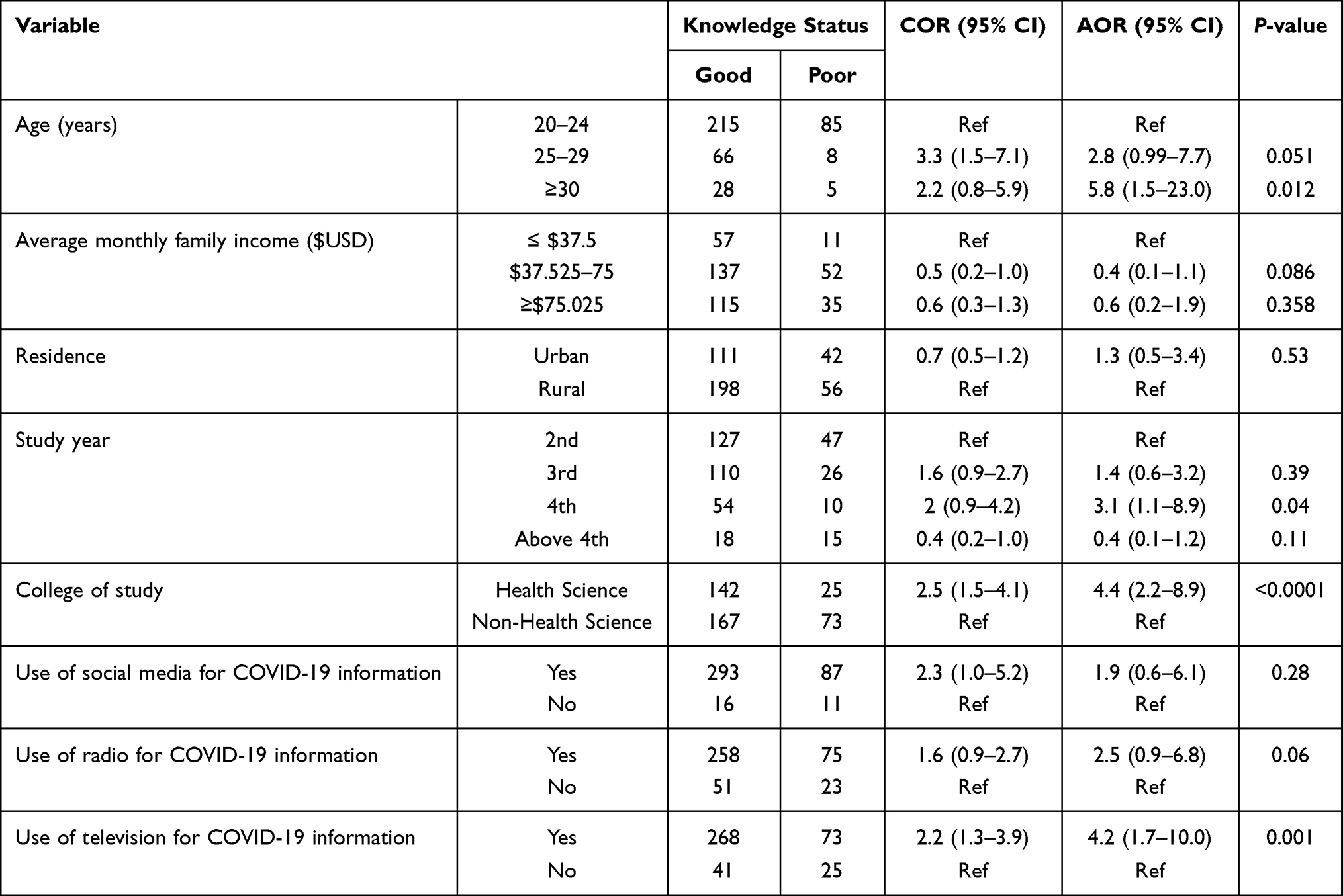 |
Table 5 Factors Associated with Knowledge about COVID-19 Among Students in Higher Education Institutions of Ethiopia December 1–30, 2020 |
Factors Associated with Attitude towards COVID-19
From a multivariable analysis, study year, college of study, presence of chronic illness, training about COVID-19, and knowledge were statistically significant concerning the attitude towards practicing COVID-19 prevention. Participants in their fourth year of study were 2.8 (1.2–6.9) times more likely to have a positive attitude towards COVID-19 prevention than second-year students. Further, Health Science students were 4.5 (95% CI: 2.5–8.0) times more likely to have a positive attitude towards COVID-19 prevention measures than non-Health Science students. Participants who had a chronic medical condition were 4.3 (95% CI: 1.1–17.5) times more likely to have a positive attitude towards COVID-19 prevention than those who did not have a chronic medical condition. Similarly, participants who took training about COVID-19 at least once were 1.9 (95% CI: 1.2–3.4) times more likely to have a positive attitude towards COVID-19 prevention than those who did not take the training. Finally, participants who had good knowledge were 3.0 (95% CI: 1.6–5.7) times more likely to have a positive attitude towards COVID-19 prevention than those who had poor knowledge about COVID-19 (Table 6).
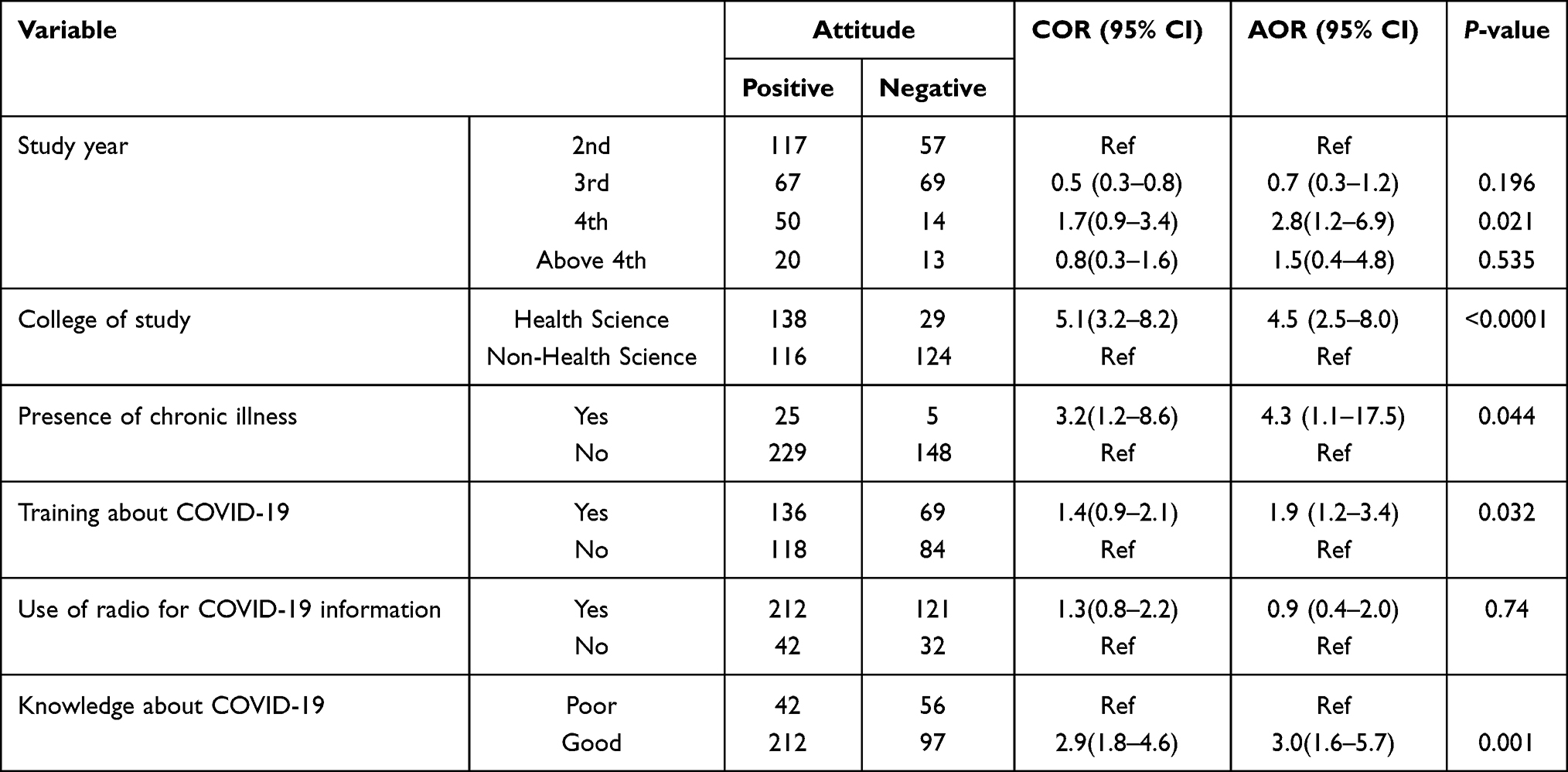 |
Table 6 Factors Associated with Attitude towards COVID-19 Prevention Practices Among Students in Higher Education Institution of Ethiopia December 1–30, 2020 |
Factors Associated with Preventive Practice Towards COVID-19
The models of the multivariable analysis revealed that residence, average family monthly income, use of social media, use of radio as a source of COVID-19 information, and a positive attitude were statistically significant related to infection COVID-19 prevention practices. Participants who were from urban areas were 40% more likely than those who were from rural areas to have good COVID-19 infection prevention practice. Further, students with an average family monthly income of > $75USD were 3.5 times more likely to have good COVID-19 infection prevention practice than those with an average monthly income of < $37.5USD. In addition to these, respondents who used at least one type of social media were 4.7 times more likely to have good infection prevention practice against COVID-19 than those who did not use social media. Similarly, participants who used radio as a source of COVID-19 information were 2.4 times more likely to have a good COVID-19 infection prevention practice than those who did not use it. Finally, participants who had a positive attitude toward practicing prevention were 2.2 times more likely than those with a negative attitude to have a good infection prevention practice against COVID-19 (Table 7).
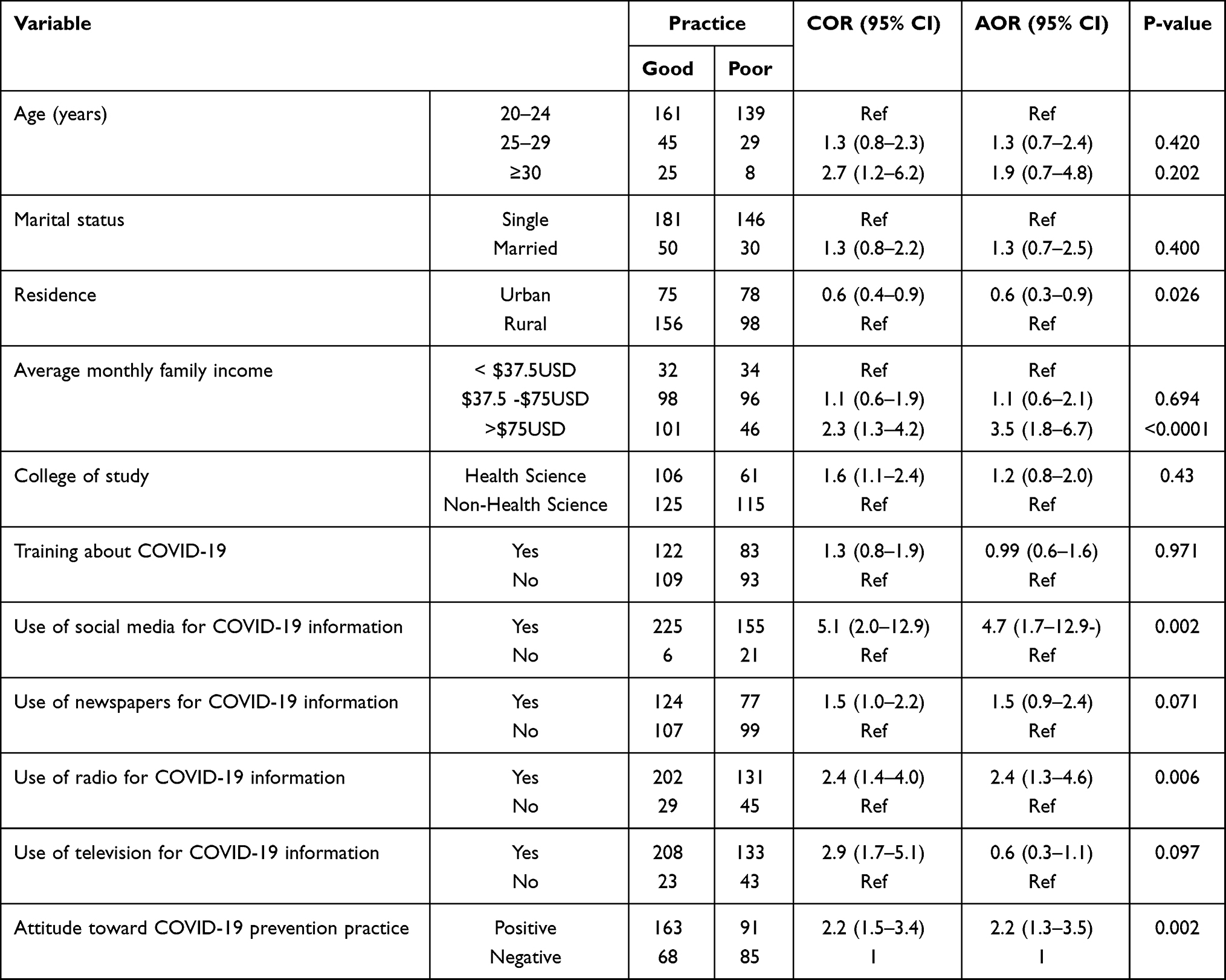 |
Table 7 Factors Associated with COVID-19 Prevention Practice Among Students in Higher Education Institutions of Ethiopia, December 1–30, 2020 |
Discussion
A facility-based cross-sectional study was conducted among students of higher education institutions of Ethiopia from December 1–30, 2020. The study aimed to assess knowledge, attitude, and COVID-19 infection prevention practice and associated factors among this population. The finding revealed that 75.9%, 62.4%, and 56.8% of the participants had good knowledge, positive attitude, and good preventive practice towards COVID-19, respectively. Age, study year, college of the study, presence of chronic illness, training about COVID-19, average monthly family income, urban or rural residence, and use of different sources of COVID-19 information such as social media, radio, and television were factors affecting the KAP of University students about COVID-19.
This finding revealed that about three-quarters 75.9% (95% CI: 72.2–79.9) of the participants had good knowledge about COVID-19 which was consistent with findings in Ethiopia (73.8%).28 But, it was higher than the finding in India (70%),29 Ethiopia (69.6%),27 (51.2%),30 (47%).19 On the contrary, it was lower than the finidng obtained in Ethiopia (88.2%),31 Nigeria (99.7%),32 healthcare providers in Delghi Primary hospital, Ethiopia (94.2%),33 Iraq (91.8%),23 Rwanda (97%),34 and India (86.7%).35 The possible reason for this variation may be a change in the educational background, study setting, and study period, and perception towards severity of the pandemic.
About 86.43% of the knowledge assessment questions were replied correctly which was consistent with a study conducted in China (90%).36 The current finding was higher than the studies conducted in Saudi Arabia (80.5%),5 Nigeria (77.36%),37 Egypt (71.26%),38 and Malaysia (76.8%).39 On the contrary, it was lower than the finding in Ethiopia (94.2%).33 The possible reason for the variation may be due the difference in the background of the participant, taking of training, and use of different sources of information towards the updated information on the COVID-19 pandemic.
The age of students was a factor significantly associated with knowledge about COVID-19, which is in line with the findings of other studies.25,27,30,40,41 College of the study was another factor affecting knowledge of students about COVID-19 which was consistent with the findings of other studies.1,19,24 Students who have a health science background showed a better knowledge towards the COVID-19 than others. This may be explained by the fact that they had an experience with other types of disease which have similar characteristics such as influenza and others. Furthermore, students who used television as sources of information towards COVID-19 were another factors of knowledge towards COVID-19 which was supported with the finding in Ethiopia.42
Less than two-thirds 62.4% (95% CI: 58.2–67.1) of the participants had a positive attitude towards COVID-19 which was lower than the finding in Iraq (90%),23 Ethiopia (72%),43 (94.7%),31 Nigeria (79.5%),32 Pakistan (82.16%),44 Ethiopia (82.4%),45 and Rwanda (74%).34 However, it was higher than the finding in Ethiopia (54.0%),19 (56.6%).27 This discrepancy may be due to variation in target population, study setting and period, and burden of the disease in their country. The current finding also showed that only 12% of the respondents agreed that Ethiopia is in a good position to control the transmission of COVID-19 within a short time, which was lower than another finding in Ethiopia (64.6%),43 and Nigeria (78.7%).37 The variation in this finding may be due to a change in the background of the study participants and low governmental commitment towards COVID-19 due to different contributing factors like current political crisis.
The average family monthly income of participants was a factor significantly affecting the attitude towards COVID-19 which was matched with the finding of other studies.19,40,42,46 Study year was also another factor affecting the attitude of students towards COVID-19 which was consistent with another finding in Ethiopia.27 Furthermore, those who had contracting one or more chronic diseases were also factor which affects the attitude of the participants which was inline with the finding in Jordan.25 Finally, participants who had good knowledge towards COVID-19 showed significantly a positive attitude towards the pandemic which was consistent with the finding in Ethiopia.28
More than half of the participants 56.8% (95% CI: 52.6–61.9) had a good preventive practice, which was in line with a finding in Ethiopia.46 However, it was lower than the finding in Iraq (75%),23 Ethiopia (67%),43 (65%),27 (65%),47 and Rwanda (90%).34 On the contrary, it was higher than the finding in Ethiopia (49.0%),42 (42.8%).19 This variation may be justified by the variation in the target population, burden of the disease in their community, the accessibility of handwashing facilities, and economical differences.
Average family monthly income was one of the factors affecting the prevention practice of COVID-19. For prevention of COVID-19, there are a number of facilities which need money for purchasing them. Therefore, economic constraints can be taken as one of the challenges for having poor preventive practice. Use of social media was also another factor affecting the prevention practice of COVID-19. University students are of the most common users of social media for different purposes. Therefore, the updated information towards COVID-19 is posted in such types of media. Therefore, they can easily adapt themselves with these information. Furthermore, attitude towards COVID-19 was also affecting its prevention practice which was consistent with other findings in Ethiopia.19,46 The current study clearly showed that for participants to have a better prevention practice, they should have a positive attitude towards the pandemics. Participants from urban origions were also had significantly a better prevention practice towards the pandemic of COVID-19 which was inline with a study conducted in Ethiopia.19 The burden of COVID-19 pandemic is usually high in urban areas than the rural setting due to the presence of different contributing factors. In urban areas there may be frequent awareness creation programs using different information dissemination strategies. Finally, sex was another explanatory variable affecting the prevention practice of COVID-19 which was consistent with a finding in India.35
Less than two-thirds 62.4% of the participants reported as they frequently used face masks whenever they left their dormitory which was higher than the finding in Ethiopia (45%).19 On the contrary, it was lower than the findings in Nigeria 84.4%,32 and 82.3%.37 The possible reason for this variation may be a change in accessibility, affordability, and average monthly income of the participants. Applying the recommended physical distancing was another problem faced in the study participation and less than two-thirds 61.4% of the participants properly applied it. Our result was lower than the findings in India (94.3%)48 and Nigeria (83%).37 Applying the recommended physical distance in such types of setting is very difficult due to the presence of different risk factors. More than 10,000 students are living within a limited space. Therefore, they may be obligated to live in a very crowded setting which may create a suitable environment for the transmission of the disease within a short time.
Limitations of the Study
This study has certain limitations. First, the data was collected by self-administered interviews. The other limitation of the study was practice-related questions were collected simply by the participants' response, not by observation of what they do as a means of COVID-19 prevention measures. Further, the findings of the study would be strong if we applied a multi-stage sampling technique to increase the sample size of the study.
Conclusion
Despite the knowledge of students towards COVID-19 was optimum, the attitude and preventive practice was low. Age, study year, college of study, presence of chronic illness, training about COVID-19, average monthly family income, residence, and use of different sources of information were factors affecting KAP of students towards COVID-19. Hence, multiple information dissemination strategies using multiple media outlets should be done to improve knowledge, attitude, and preventive practice of COVID-19. Additionally, different personal protective equipment such as facemasks, soap, hand washing facilities, alcohol-based hand sanitizer should be supplied on free by the concerned bodies.
Abbreviations
AOR, Adjusted Odds Ratio; COR, Crude Odds Ratio; CI, Confidence Interval; COVID-19, Coronavirus Infection Disease 2019; KAP, Knowledge, Attitude, and Practice; SARS, Severe Acute Respiratory Syndrome.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
The study was conducted in accordance with Helsinki Declaration. As a result, ethical review letter was obtained from the ethical review committee of College of Medicine and Health Sciences, Wollo University. Because we were unable to obtain written consent from all study participants, we relied on verbal consent after receiving approval from the ethical review committee of College of Medicine and Health Sciences, Wollo University. The objective of the study was described to each study participant prior to data collection, and they were also informed that they had the right to withdraw from the study at any time. The data obtained from study participants was kept confidential. During data collection, data collectors applied COVID-19 prevention measures, such as wearing face masks and keeping the recommended physical distancing of 2 meters away from others.
Acknowledgments
We would like to express our heartfelt gratitude to Wollo University for providing ethical clearance. We also want to extend our thanks to Wollo University, Debre Tabor University, and Debre Markos University administrators for their permission to conduct this study. We also thank the study participants who gave valuable information and took precious time with their kind cooperation. We also want to extend our appreciation to all data collectors and supervisors for their commitment and collaboration.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Hasan H, Raigangar V, Osaili T, Neinavaei NE, Olaimat AN, Aolymat I. A cross-sectional study on university students’ knowledge, attitudes, and practices toward COVID-19 in the United Arab Emirates. Am J Trop Med Hyg. 2021;104(1):75–84. doi:10.4269/ajtmh.20-0857
2. Elhadi M, Msherghi A, Alkeelani M, et al. Assessment of healthcare workers’ levels of preparedness and awareness regarding COVID-19 infection in low-resource settings. Am J Trop Med Hyg. 2020;103:828. doi:10.4269/ajtmh.20-0330
3. Saqlain M, Munir MM, Ur Rehman S, et al. Knowledge, attitude, practice and perceived barriers among healthcare professionals regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105:419–423. doi:10.1016/j.jhin.2020.05.007
4. Chowdhury S, Chakraborty PP. Universal health coverage - There is more to it than meets the eye. J Fam Med Prim Care. 2017;6(2):169–170. doi:10.4103/jfmpc.jfmpc_13_17
5. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Heal. 2020;8:217.
6. Iannone P, Castellini G, Coclite D, et al. The need of health policy perspective to protect Healthcare Workers during COVID-19 pandemic. A GRADE rapid review on the effectiveness of the N95 respirator. PLoS One. 2020;15(6):e0234025. doi:10.1371/journal.pone.0234025
7. Nallani VRR, Nadendla RR, Kavuri NSS. Knowledge, attitude, and practice among health care professionals regarding COVID-19 and barriers faced by health care professionals in South India. Int J Community Med Public Heal. 2020;7(9):3450–3459. doi:10.18203/2394-6040.ijcmph20203906
8. Hasan AA. Knowledge, attitudes, and practices of King Abdulaziz undergraduate nursing towards novel corona virus (COVID 19). Am J Nurs Stud. 2021;15(1):786.
9. Ssebuufu R, Katembo SF, Binezero SM, et al. Awareness knowledge attitude and practice towards measures for prevention of the spread of COVID-19 in the Ugandans A nationwide online cross-sectional Survey. Medrxiv. 2020.
10. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
11. Basic Education Republic of South Africa. DBE Guidelines for Schools on Maintaining Hygiene during CVID-19 pandemic. Available from: https://www.gov.za. Accessed on March 25, 2021
12. Hatabu A, Mao X, Zhou Y, Kawashita N, Wen Z. Knowledge, attitudes, and practices toward COVID-19 among university students in Japan and associated factors: an online cross-sectional survey. PLoS One. 2020;15(12):e0244350. doi:10.1371/journal.pone.0244350
13. Worldometer report COVID-19 cases in the world. 2020. Available from: https://www.worldometers.info/coronavirus/world.
14. Lone SA, Ahmad A. COVID-19 pandemic – an African perspective. Emerg Microbes Infect. 2020;9:1300–1308. doi:10.1080/22221751.2020.1775132
15. Baye K. COVID-19 prevention measures in Ethiopia current realities and prospects. The Federal Democratic Republic of Ethiopia Policy Studies Institute; 2020.
16. Worldometer report COVID-19 cases in Ethiopia. 2020. Available from: https://www.worldometers.info/coronavirus/country/ethiopia.
17. Nigussie TF, Azmach NN. Knowledge, attitude and practice towards COVID-19 among Arba Minch town, Southern Ethiopia. GSJ. 2020;8(6)1283–1307.
18. Ye Y, Wang R, Feng D, Wu R, Li Z, Long C. The recommended and excessive preventive behaviors during the COVID-19 pandemic: a community-based online survey in China. Int J Environ Res Public Health. 2020;17:6953. doi:10.3390/ijerph17196953
19. Angelo AT, Alemayehu DS, Dacho AM. Knowledge, attitudes, and practices toward covid-19 and associated factors among university students in Mizan tepi university, 2020. Infect Drug Resist. 2021;14:349–360. doi:10.2147/IDR.S299576
20. Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia: a cross-sectional survey. Trop Med Health. 2020;48:1–11. doi:10.1186/s41182-020-00254-3
21. Defar A, Molla G, Abdella S, et al. Knowledge, practice and associated factors towards the Prevention of COVID-19 among high-risk groups: a cross-sectional study in Addis Ababa, Ethiopia. PLoS One. 2021;16:e0248420. doi:10.1371/journal.pone.0248420
22. Huynh G, Nguyen TN, Vo KN, et al. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13:260. doi:10.4103/1995-7645.280396
23. Khalil NS, Al-yuzbaki DB, Tawfeeq RS. COVID-19 knowledge, attitude, and practice among medical undergraduate students in Baghdad City. Eurasian J Biosci. 2020;14:4179–4186.
24. Olaimat AN, Aolymat I, Elsahoryi N, Shahbaz HM, Holley RA. Attitudes, anxiety, and behavioral practices regarding COVID-19 among University students in Jordan: a cross-sectional study. Am J Trop Med Hyg. 2020;103(3):1177. doi:10.4269/ajtmh.20-0418
25. Olaimat AN, Aolymat I, Shahbaz HM, Holley RA. Knowledge and information sources about COVID-19 among university students in Jordan: a cross-sectional study. Front Public Heal. 2020;8:254. doi:10.3389/fpubh.2020.00254
26. Peng Y, Pei C, Zheng Y, et al. Knowledge, attitude and practice associated with COVID-19 among university students: a cross-sectional survey in China. 2020.
27. Tadesse A, Melese N, Eshetie S, Chane M, Ali A. Knowledge, attitude, and practice and associated factors towards COVID-19 among college students in Amhara region, Ethiopia; a cross-sectional study. 2020.
28. Kassie BA, Adane A, Tilahun YT, Kassahun EA, Ayele AS, Belew AK. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PLoS One. 2020;15:1–12. doi:10.1371/journal.pone.0238415
29. Prasad Singh J, Sewda A, Shiv DG. Assessing the knowledge, attitude, and practices of students regarding the COVID-19 pandemic. J Health Manag. 2020;22(2):281–290. doi:10.1177/0972063420935669
30. Degu A, Nibret G, Gebrehana H, Getie A, Getnet B. Knowledge and attitude towards the current pandemic coronavirus disease and associated factors among pregnant women attending antenatal care in Debre Tabor general hospital Northwest Ethiopia: an institutional-based cross-sectional study. Int J Women’s Health. 2021;13:61–71. doi:10.2147/IJWH.S285552
31. Jemal B, Ferede ZA, Mola S, et al. Knowledge, attitude, and practice of healthcare workers towards COVID-19 and its prevention in Ethiopia: a multicenter study. 2020.
32. Reuben RC, Danladi MM, Saleh DA, et al. Knowledge, attitudes and practices towards COVID - 19: an epidemiological survey in North - Central Nigeria. J Community Health. 2021;46:457–470.
33. Shibabaw T, Teferi B. Knowledge and practice toward prevention of sars-Cov-2 among healthcare workers at Delghi primary hospital during a massive test campaign in northwest Gondar, Ethiopia: institution-based descriptive cross-sectional survey. Infect Drug Resist. 2021;14:381–390. doi:10.2147/IDR.S289965
34. Iradukunda PG, Pierre G, Muhozi V, Denhere K, Dzinamarira T. Knowledge, attitude, and practice towards COVID-19 among people living with HIV/AIDS in Kigali, Rwanda. J Community Health. 2021;46(2):245–250. doi:10.1007/s10900-020-00938-1
35. Maheshwari S, Gupta P, Sinha R, Rawat P. Knowledge, attitude, and practice towards coronavirus disease 2019 (COVID-19) among medical students: a cross-sectional study. J Acute Dis. 2020;9(3):100. doi:10.4103/2221-6189.283886
36. Zhong B, Luo W, Li H, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16:1745. doi:10.7150/ijbs.45221
37. Okoro J, Ekeroku A, Nweze B, et al. Attitude and preventive practices towards COVID-19 disease and the impact of awareness training on knowledge of the disease among correctional officers. Emerald Open Res. 2020;2:51. doi:10.35241/emeraldopenres.13839.1
38. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;45(5):881–890. doi:10.1007/s10900-020-00827-7
39. Fatah NSA, Nurhasim MF, Kaltes IA, Jaafar ASIA, Amran I, Baharum A. Awareness kap on covid-19 among university students in sabah. Int J Adv Technol Eng Explore. 2021;8(74):161–166. doi:10.19101/IJATEE.2020.S1762135
40. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15:1–17. doi:10.1371/journal.pone.0239254
41. Tamire AH, Legesse TK. Knowledge, attitudes, and practices towards coronavirus disease-19 among health professionals in Addis Ababa. 2020:343–349.
42. Tigabu DE, Tekalign AB, Sheganew FT, Abraham TA, Nigusie ST, Chalie MT. Assessment of knowledge, practice and associated factors towards prevention of novel coronavirus among clients attending at Debre Tabor General Hospital, Debre Tabor Town, North West Ethiopia, 2020: institutional based cross-sectional study. J Community Med Heal Solut. 2020;1(1):26–34. doi:10.29328/journal.jcmhs.1001004
43. Tadesse DB, Gebrewahd GT, Demoz GT. Knowledge, attitude, practice, and psychological response toward COVID-19 among nurses during the COVID-19 outbreak in northern Ethiopia, 2020. New Microbes New Infect. 2020;38:100787. doi:10.1016/j.nmni.2020.100787
44. Hussain I, Majeed A, Imran I, et al. Knowledge, attitude, and practices toward COVID - 19 in primary healthcare providers: a cross-sectional study from three tertiary care hospitals of Peshawar, Pakistan. J Community Health. 2021;46:441–449.
45. Gebretsadik D, Ahmed N, Kebede E, Gebremicheal S, Belete MA, Adane M. Knowledge, attitude, practice towards COVID-19 pandemic and its prevalence among hospital visitors at Ataye district hospital, Northeast Ethiopia. PLoS One. 2021;16:e0246154. doi:10.1371/journal.pone.0246154
46. Abate H, Mekonnen CK. Knowledge, attitude, and precautionary measures towards covid-19 among medical visitors at the University of Gondar comprehensive specialized hospital northwest Ethiopia. Infect Drug Resist. 2020;13:4355–4366. doi:10.2147/IDR.S282792
47. Yoseph A, Tamiso A, Ejeso A. Knowledge, attitudes, and practices related to COVID-19 pandemic among adult population in Sidama Regional State, Southern Ethiopia: a community based cross-sectional study. PLoS One. 2021;16:e0246283. doi:10.1371/journal.pone.0246283
48. Singh SP, Gahlot A, Verma V, Singh M. A study of knowledge, attitude, and practices regarding SARS COV-2 infection and its control amongst medical students of Rama Medical College Kanpur (U.P). Indian J Forensic Community Med. 2020;7(3):134–139. doi:10.18231/j.ijfcm.2020.029
49. Nepal R, Sapkota K, Paudel P, et al. Knowledge, attitude and practice regarding COVID-19 among healthcare workers in Chitwan, Nepal. J Chitwan Med Coll. 2020;10(3):98–102. doi:10.3126/jcmc.v10i3.32064
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.