Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Knowledge, Attitude, and Practice Toward Lifestyle Modification Among Diabetes Mellitus Patients Attending the University of Gondar Comprehensive Specialized Hospital Northwest, Ethiopia
Authors Mekonnen CK ![]() , Abate HK
, Abate HK ![]() , Tegegne ET
, Tegegne ET ![]()
Received 21 February 2020
Accepted for publication 19 May 2020
Published 12 June 2020 Volume 2020:13 Pages 1969—1977
DOI https://doi.org/10.2147/DMSO.S250787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Chilot Kassa Mekonnen,1 Hilemichael Kindie Abate,1 Elenie Tesffaye Tegegne2
1Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Community Health Nursing, School of Nursing, College of Medicine and Health Sciences University of Gondar, Gondar, Ethiopia
Correspondence: Chilot Kassa Mekonnen Email [email protected]
Background: Diabetes, which is a non-communicable metabolic disease, imposes several complications and death worldwide. Strict lifestyle modification can prevent the progression of complications associated with diabetes. There is much evidence to show that following a healthy lifestyle such as healthy diet, moderate weight loss, and doing regular exercise can maintain normal blood glucose levels and minimize diabetes-related complications. Moreover, this lifestyle modification has a great impact on the control of hyperglycemia. Good knowledge, positive attitude, and good practice towards lifestyle modification can help to maintain a normal blood glucose level.
Objective: The aim was to assess knowledge, attitude, and practice towards lifestyle modification of diabetes patients attending the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia.
Methods: An institutional-based crossectional study was conducted among diabetes patients attending chronic follow-up clinic from November 15, 2019 to December 15, 2019. Study participants were selected using a systematic random sampling technique. Data were collected by using a structured questionnaire and analyzed using the statistical package for social science version 20. Descriptive statistics were computed to determine the knowledge, attitude, and practice of diabetes patients toward lifestyle modification.
Results: A total of 422 participants took part in this study with a response rate of 100%. In this study, 248 (59%) were knowledgeable, 223 (53%) had a positive attitude, and 172 (41%) had good practice, respectively.
Conclusion: The findings of this study showed that the knowledge and attitude toward lifestyle modification were found to be good. However, the result of practice of lifestyle modification was low.
Recommendation: Education about the disease condition and lifestyle modification (importance of physical exercise, weight loss, foot care, cessation of smoking, healthy dietary habit) to general society ought to be implemented by the responsible body.
Keywords: diabetes mellitus, knowledge, attitude, practice, lifestyle modification
Introduction
Diabetes mellitus (DM) is a chronic noncommunicable metabolic disease characterized by a raised blood plasma glucose level. It has an important public concern nowadays due to a dramatic increase in incidence and prevalence.1 It is a syndrome of hyperglycemia resulting from an absolute or relative deficiency or decreased effectiveness of the circulating insulin.2
According to WHO estimates globally, DM is a risk factor for premature mortality, cardiovascular and kidney diseases associated with unhealthy nutrition, physical inactivity or insufficient exercise, cigarette smoking, excessive consumption of alcohol, and inappropriate sleeping experience.3
According to 2016 WHO report, there were around 422 million adult diabetes patients.4 But, in 2019 it was found to be 463 million people (9.3%) and can be projected to 578 million (10.2%) by 2030 and 700 million (10.9%) by 2045. This figure is 4% in low-income countries, which is increasing and becoming a public health concern globally.5,6
Furthermore, according to WHO 2019 evidence type 2 DM makes up about 90–95% of all cases and the remaining 2–5% is type 1 DM.7 The incidence and prevalence rate of DM is higher, especially in developing countries, compared with the developed countries due to early lifestyle change.8 Lack of knowledge, negative attitude, and poor practice affect diabetes prognosis and hasten the occurrence which is preventable with early recognition.9 The majority of DM patients receive their treatment in clinics when they adhere to treatments and gain education not only to achieve glycemic control but also to halt the occurrence of complications and disabilities.10 On top of this, lifestyle modification is an integral and crucial component of diabetes control and management. Among the six important key areas recommended by American Diabetic Association (ADA), diabetic self-management support (DSMS), diabetic self-management education (DSME), dietary therapy, physical exercise, counselling of smoking cessation, and psychosocial care are crucial for diabetes management.11 DSME and self-management support programs are primarily targeted to upscale an individual’s knowledge, skill, and capability needed for self-care and management of DM.12 One significant focus of nutritional therapy is promoting and supporting healthy conditions to maintain target body weight, blood glucose, blood pressure, and lipid profile.13
Moreover, promoting physical activity and exercise are among the core components of diabetic lifestyle management. Exercise plays a significant role for reducing weight, controlling blood glucose, and minimizing cardiovascular-related complications.14 The correlation between smoking and other health consequences is already known. In this regard, there exists increased cardiovascular (macro and micro) complications and occurrence of type 2 diabetes among cigarette smokers.15 According to the International Diabetes Federation, in the African region, around 15.5 million adults who are aged 20–70 years were found to have DM. This region has a high prevalence (69.2%) with 69.2% of adults unaware of their disease condition and 55.3% of adults who lived in the urban area with changed lifestyle.16 Nowadays, Ethiopia is challenged by the raised burden of noncommunicable diseases including DM, which took fourth place in Sub-Saharan Africa in the prevalence of diabetic population. Especially type 2 DM is an important cause of admission to Ethiopias largest referral Hospital where an estimated 1.9 million people live with diabetes.17
Diabetes patients may have complications during diagnosis due to genetic predispositions and long-term asymptomatic hyperglycemia. During diagnosis, about 25% and 4.8% of diabetic patients found to have neuropathy and peripheral vascular disease respectively.14
As a result of these complications, a significant number of diabetic patients have diabetic foot ulcers and nontraumatic amputation.18,19 Evidence showed an increased burden of noncommunicable disease associated with unhealthy lifestyle.1,20
In spite of the fact that DM causes high resource wastage and life, still the management relies on pharmacological and lifestyle modifications. It is obvious that lifestyle modification plays a significant role in the prevention of diabetes occurrence and its complications. Therefore, the aim of this study was to assess the knowledge, attitude, and practice of DM patients toward lifestyle modification at UOGCSH.
Method
Study Design and Period
A cross-sectional institutional-based study conducted from November 15, 2019 to December 15, 2019.
Study Setting
The study was done at UOGCSH OPD.
The hospital is located in Gondar City in Amhara regional state. Gondar town is situated 748 km from Addis Ababa and UOGCSH has more than 400 beds and 14 different outpatient medical service units, and around 250,000 patients seen in the units. The hospital serves at a comprehensive specialized level by providing teaching, research and serving a population of more than seven million peoplein the catchment area.
Source Population
All DM patients attending DM follow-up clinic at UOGCSH.
Study Population
DM patients who are available during data collection at UOGCSH.
Inclusion and Exclusion Criteria
All adult diabetic patients who attend at UOGCSH chronic follow-up clinic. Patients who were mentally ill, unable speak and those who had a major hearing problem were excluded from the study.
Sample Size Determination and Procedures
The sample was determined using the single population by taking percentage score (p)=49.% from the study conducted in Adama21 with the following assumptions: CI=95%, marginal error (d)=5%, and 10% nonresponse rate. A structured questionnaire was used to conduct a face-to-face interview of the participants attending the diabetes follow-up clinic. There were 966 patients with chronic diabetes having follow-up during the data collection period.
The study participants were selected using a systematic random sampling technique with every two intervals. In order to avoid recycling of data due to double interviewing special markers were used in the chart of the patient interviewed. It was also strengthened by verbal confirmation whether they were interviewed in the previous consecutive data collection days.
Data Collection Tools and Procedures
A structured interviewer-administered questionnaire modified from other related studies was used to collect the data.21–23 The Cronbach’s alpha for knowledge, attitude, and practice items were (0.80, 0.78, and 0.69) respectively. Before the actual data collection, four BSc nurse data collectors who had worked outside of chronic illness and one MSc nurse supervisor had obtained one-days training about the aim of the study and the content of the questionnaire. The questionnaire had three parts which include: sociodemographic, knowledge, attitude and practice of lifestyle modification.
Data Quality Control
For data quality, a pretest was done among 21 (10%) diabetes patients. The questionnaire was translated from English to Amharic for the sake of better understanding for study participants. Then it was translated back to English by language experts in ordered to retain the original meaning. Data clearance was done at every point during collection time. Its completeness, accuracy and consistency were checked prior to entry.
Operational Definition
- Lifestyle modification: Is about nonpharmacological management including, dietary modification, physical activities, and exercise to control blood glucose level and complications.24
- Knowledge: From 10 questions of lifestyle modification if the patient answers 5 and above we say good knowledge, and if <5 poor knowledge towards LSM of DM.25
- Attitude: From 10 questions if the patient answers >5 classified as having a positive attitude and if <5 a negative attitude towards LSM of DM.21
- Practice: From 10 questions if the patient answers >5 classified as having a good practice and if <5 classified as having a poor practice towards LSM of DM.
- Fasting Blood Glucose: Blood glucose estimation obtained from a subject who has undergone an overnight fast from any food or drink (excluding water or clear, plain tea) for at least eight hours.26
- Regular follow-up: Patients who have consistent follow-up in their appointment in hospitals having a diabetic unit.27
- 28
- Family Support: This involves all family members of the diabetic patients who understand how to support the diabetes patient in terms of standard management; healthy diet, self-monitoring.29
Data Processing and Analysis
Collected data were checked for completeness, consistency, as well as accuracy prior to analysis. The data were coded, entered, and analyzed using SPSS version 20 (IBM Corporation, Armonk, NY, USA). It was processed and analyzed by using descriptive statistics like percentage and frequency. The results are presented by text and tables.
Results
Sociodemographic Characteristics
Four hundred twenty-two study participants were approached with a 100% response rate. Among 422 diabetes patients who took part in study 216 (49.1%) and 206 (48.9%) were male and female respectively. Concerning marital status 120 (28.5%) were single. Regarding the age of the participants 399 (94.6%), and 23 (5.5%) were in the age category of <30 and ≥30 years in order. In addition, 100 (23.7%) of the participants were illiterate; 168 (39.8%) of the participants attended grade 1–8,108 (25.6%) participants attended grades 9-12 and above 46 (10.9%). In occupational status 145 (34.4%) were unemployed, and 184 (43.6%) were private business. Furthermore, 15 (3.5%) were government employees, 21 (4.9%) students, and 57 (13.5%) housewives. In another way 160 (37.9%) participants who had had a monthly income of <1000 ETB, 209 (49.5%) participants had had a monthly income of reneged 1000–3000 ETB and 55 (12.5%) had ≥3000 ETB income. (Table 1)
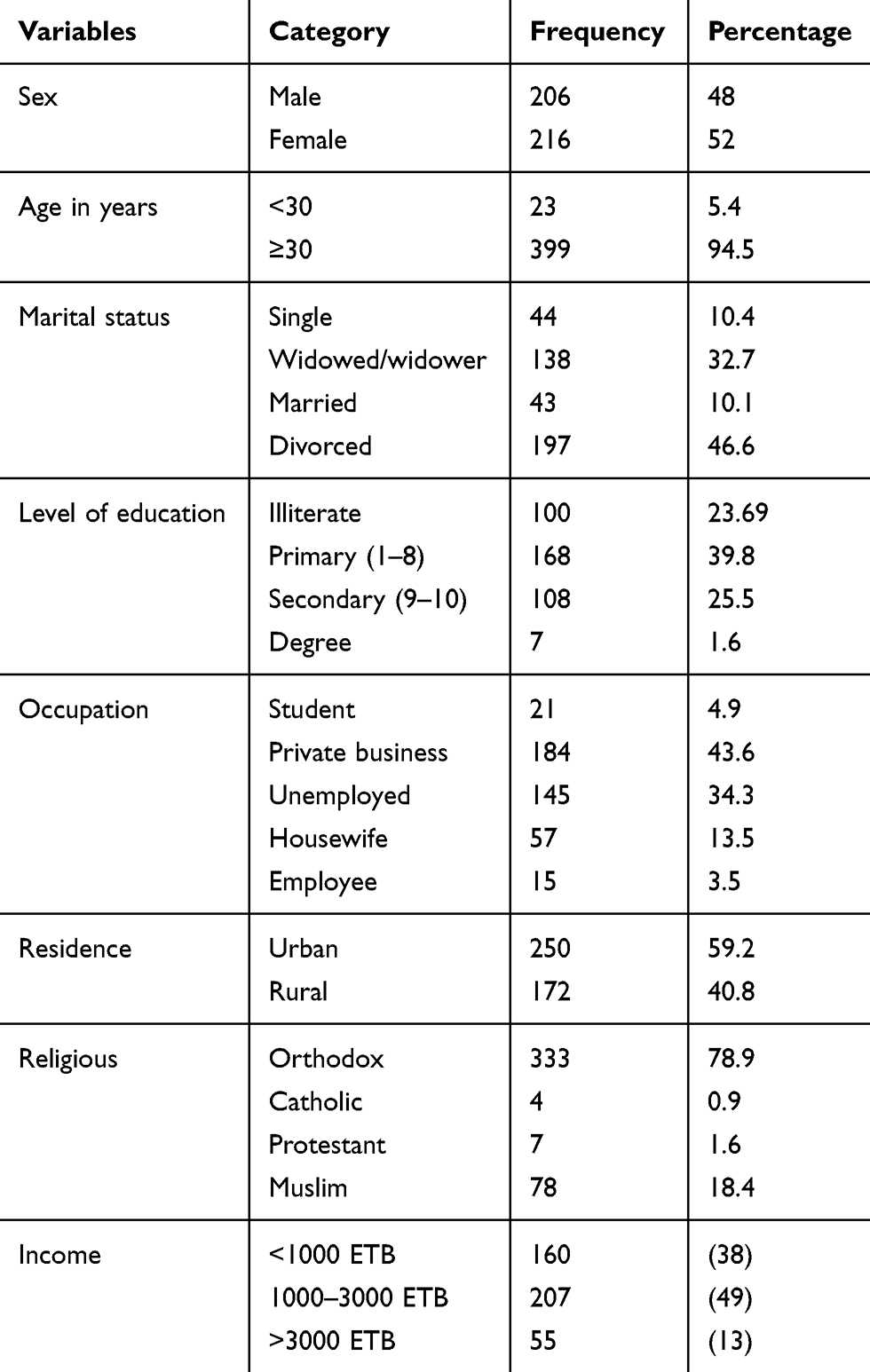 |
Table 1 Frequency Distribution of the Participants’ Sociodemographic Characteristics at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2019 (n=422) |
Knowledge of Lifestyle Modification
The majority of the participants were knowledgeable 248 (59%) (95%CI: 54.0–63.4) and 174 (41%) were poorly knowledgeable (Table 2).
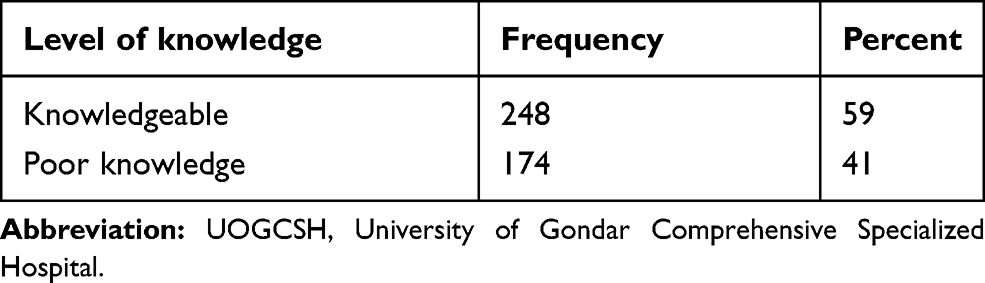 |
Table 2 Frequency Distribution of Participants’ Knowledge Score About Lifestyle Modification About Diabetes at the UOGCSH Northwest Ethiopia (n=422) |
In this study the age group >30 years old (55.5%), female 30%, separated 27.3%, employed 7.8%, urban 36.3%, orthodox 36.3%, monthly income 1000–3000 ETB, diploma and degree holders had a good knowledge respectively (Table 3).
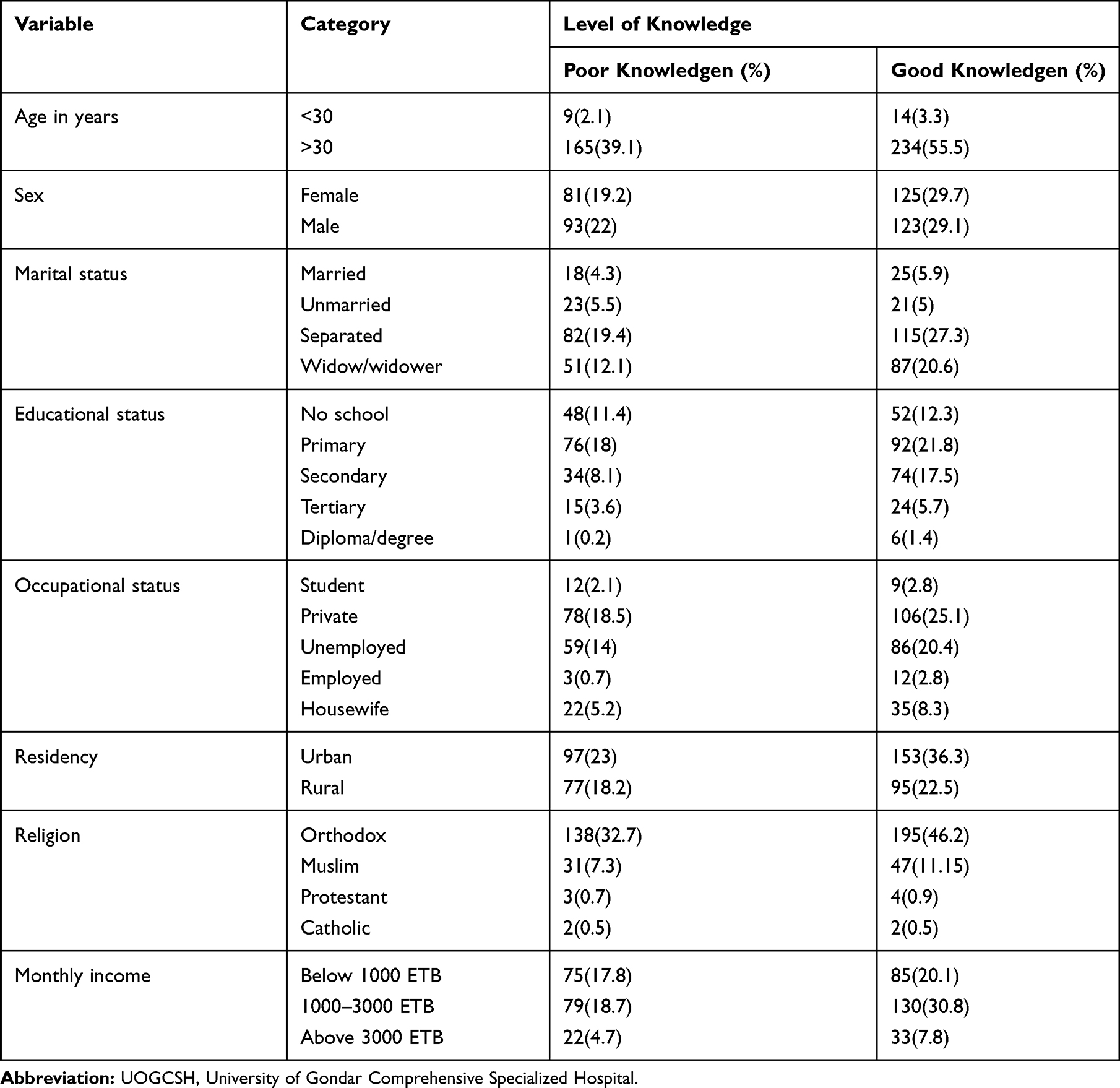 |
Table 3 Cross-tabulation of Sociodemographic Variables with Participant’s Knowledge Score About Lifestyle Modification About Diabetes at the UOGCSH Northwest Ethiopia, 2019 G.C (n=422) |
Attitude Towards Lifestyle Modifications
More than half of the participants 253 (53%) had had a positive attitude toward lifestyle modification and 199 (47%) participants had a negative attitude (Table 4).
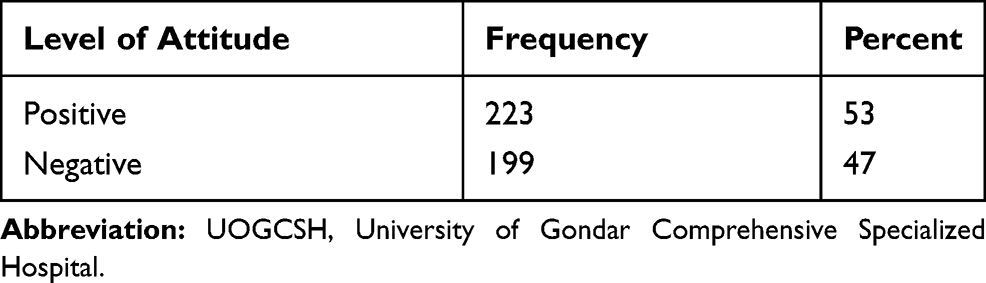 |
Table 4 Frequency Distribution of Participants’ Attitude Score About Lifestyle Modification About Diabetes at the UOGCSH, Northwest Ethiopia, 2019 G.C (n=422) |
In this study participants of the age group >30 years old 50%, being male 29.9%, widow/widower 19.4%, attended secondary school 17.1%, employed 2.4%, urban 34.1%, orthodox 42.2%, and having a monthly income of 1000–3000 ETB had a positive attitude respectively (Table 5).
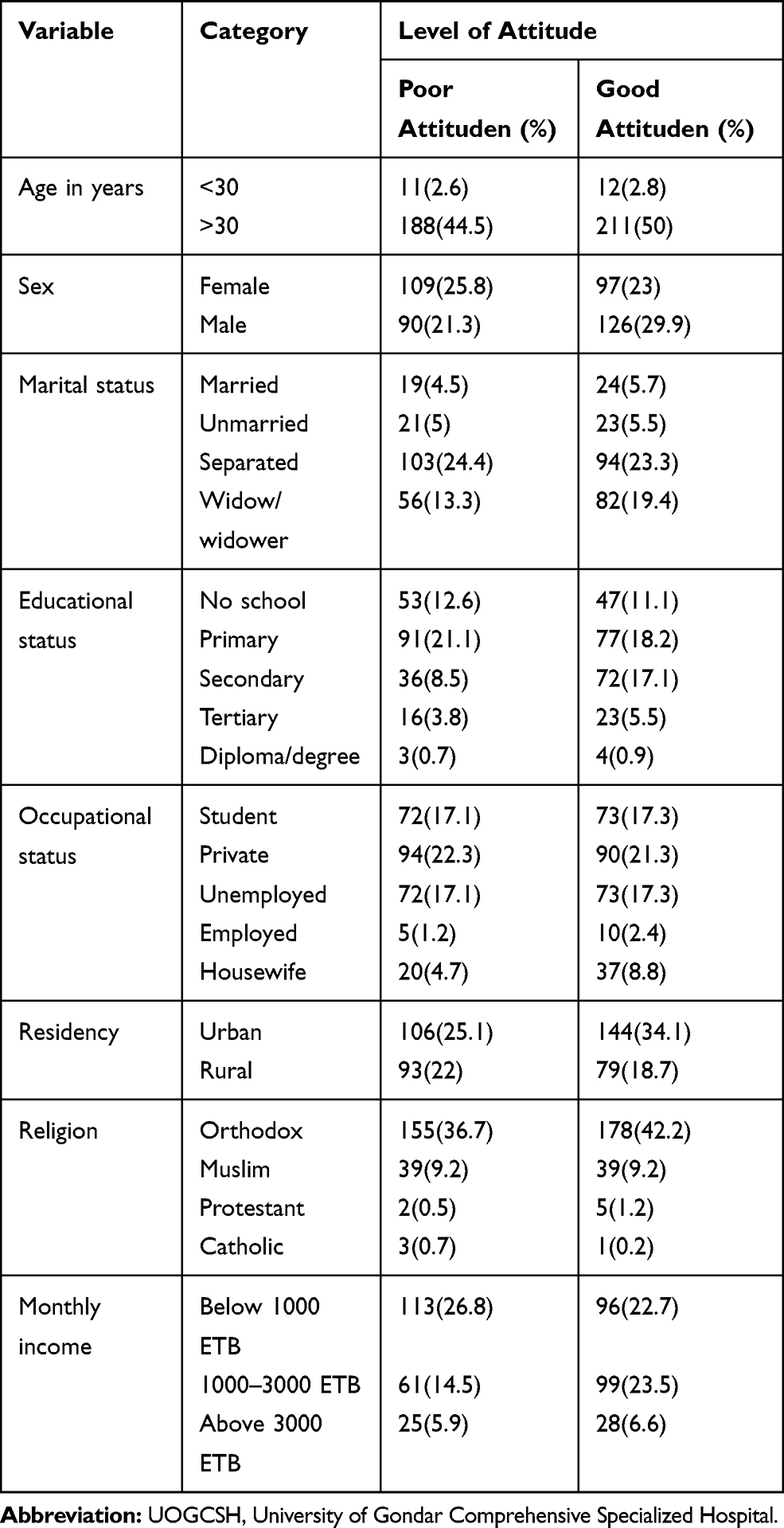 |
Table 5 Frequency Distribution of Participants’ Attitude Score About Lifestyle Modification About Diabetes at the UOGCSH, Northwest Ethiopia, 2019 G.C (n=422) |
Practice Assessment of Respondents
In this study 172 (41%) had good practice toward LSM, and 250 (59%) had poor practice (Table 6). Cessation of smoking cigarettes was not practiced in 6.2% of the participants, more than half (58.1%) and (55.0%) had worn safety shoes and had regular blood sugar checkups as recommended (Table 7).
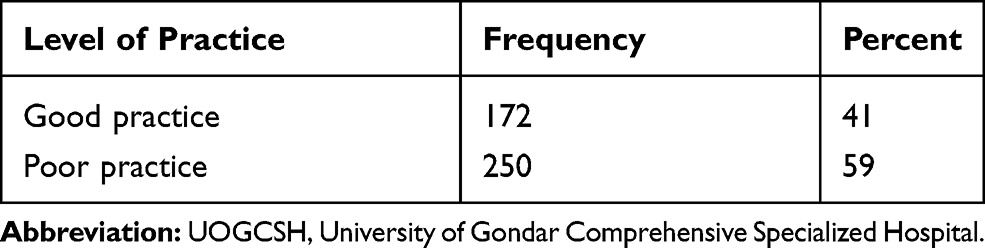 |
Table 6 Frequency Distribution of Participants’ Practice Score About Lifestyle Modification Among Diabetes at the UOGCSH, Northwest Ethiopia, 2019 G.C (n=422) |
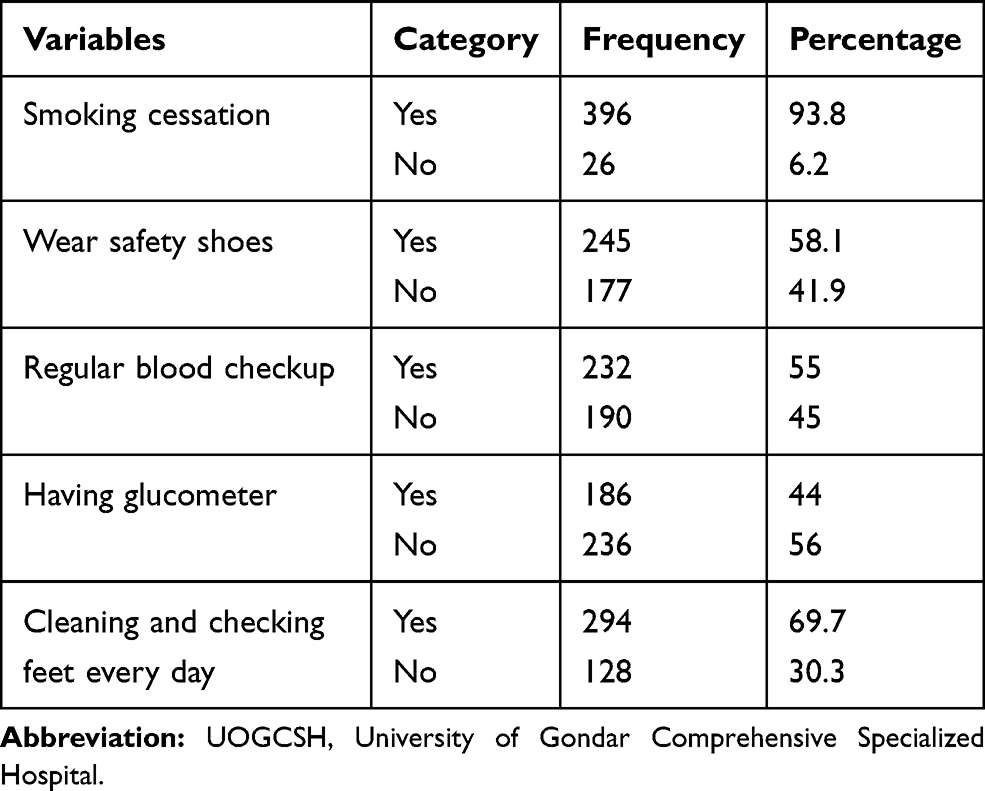 |
Table 7 Recommended Lifestyle Modification Practices of the Participants Among Diabetes at the UOGCSH, Northwest Ethiopia, 2019 G.C (n=422) |
In this study participants of the age group <30 years old 2.8%, males 22.7%, unmarried 4.3%, attended secondary school 9.2%, housewives 4.3%, protestant 0.7% and monthly income below 1000 ETB, 13.7% had poor practice toward LSM. In this study 172 (41%) had good practice toward LSM, and 250 (59%) had poor practice (Table 8).
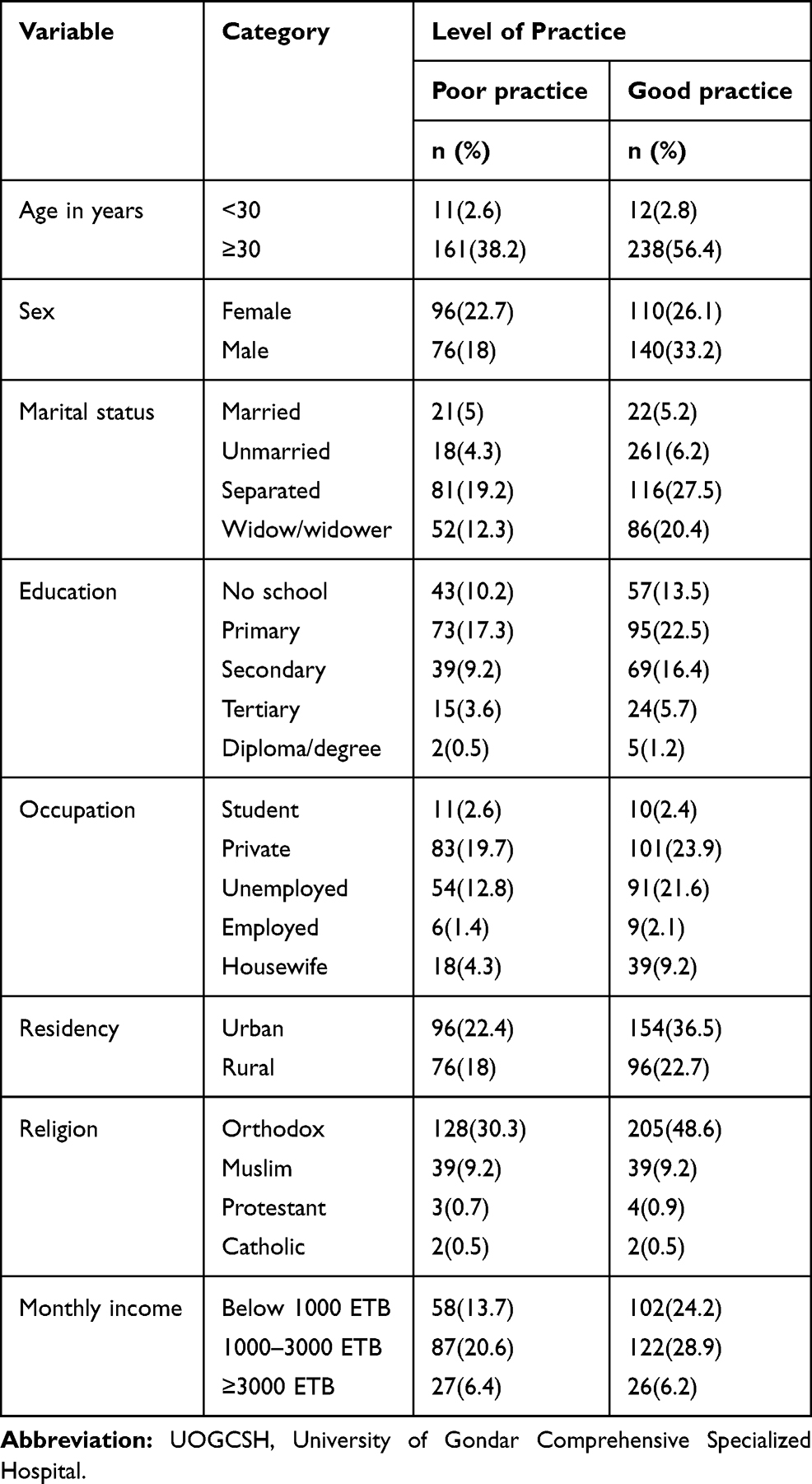 |
Table 8 Cross-tabulation Sociodemographic Variables with Participants’ Practice Score About Lifestyle Modification Among Diabetes at the UOGCSH, Northwest Ethiopia, 2019 G.C (n=422) |
Discussion
In this finding 248 (59%) were knowledgeable and 174 (41%) were poorly knowledgeable towards lifestyle modification. This result was higher than the studies conducted in South Africa30 which was 7.8%, and 9.9% in Egypt,31 (20.37%) in another study in South Africa.32 But the result was lower than the study conducted in Adama21, which was found to be 77.59%. The possible explanation might be due to the fact that there is a time gap, tool variation, and sociodemographic variations across the countries. The cross-tabulation of this study showed that participants in the age group of >30 years had good knowledge (55.5%) compared to those <30 years of age (3.3%).
The result further revealed that there was no difference between genders- related to knowledge level, females (19.2%) and (29.1%) males (22%) and (29.1%) had a poor and good level of knowledge respectively.
In this study only 5.9% unmarried participants were knowledgeable as compared with their counterpart. The lowest score might be due to the fact that unmarried participants did not get support from their spouse when they decided to get information or help. Regarding the educational status of the participants, those who were illiterate were less knowledgeable compared with their counterparts. This indicates that low level of education among participants related to poor knowledge about their illness as well as lifestyle modification since they could not get enough information through reading magazines, leaflets, and other sources of information.
In this study participants with an occupational status of unemployed were more knowledgeable than their counterparts. This might be due to the fact those unemployed had free time to read and get information.
The results further revealed that the majority of urban residents were knowledgeable compared to rural residents (36.3%). It might be that urban residents had more access to information about LSM compared to rural residents. The study also revealed that respondents with a monthly income of 1000–3000 ETB (30.8%) were more knowledgeable than other comparators. This might be due to the fact that those who have money could have access to information in different ways.
This study revealed that the positive attitude towards lifestyle modification was 53%. It was found to be lower than the studies conducted in Adama 81.89%, Botswana 89.4%, Egypt 89.3 %, and South Africa 84.3%, respectively.21,30,31,33 The possible explanations for the variations in the attitude score about diabetes lifestyle modification might be due to the fact that health service, sociodemographic, and the scoring system variation.
The cross-tabulation showed that the majority of participants in the age group of ≥30 years had a good attitude (50%) compared to <30 years of age (2.8%).
The result further revealed that male respondents had a more positive attitude (29.9%) than females. The possible explanation might be males had more information than females through being an outsider and having more contact with the social environment.
Being married was a more positive attitude than their counterparts. It might be they were more likely to get support from their spouse. This study revealed that participants without formal education had a less positive attitude (11.1%) towards lifestyle modification compared to those having a formal education.
In this study the participants with the occupational status of being employed (10%) had a more positive attitude than their comparators. The results further revealed that the majority of urban residents had a more positive attitude as compared to rural residents (34.1%). It might be that urban residents had more access to information about LSM compared to rural residents.
The results of this study with a monthly income below 1000 ETB (14.5%) and (23.5%) 1000–3000 ETB (26.8%) and (22.2%) above 3000 ETB (5.9%) and (6.6%) had a poor and good attitude on their LSM respectively. In this study, the good practice score toward lifestyle modification was found to be 41%. The result was higher than the study conducted in Egypt31 (15.3%), but lower than the study in Adama21 (49.1%) toward lifestyle modification.
The results of this study showed that the majority of participants in the age group of ≥30 years had poor practice (56.4%) compared to the age group of <30 years (2.8%). The results further revealed that males (33.2%) had a good level of practice on their LSM.
In this study participants with a diploma/degree (0.5%) and (1.2%) had a good practice on their LSM. This reflects that degree/diploma holders were at a good practice level so education was directly related to good practice of LSM.
In this study, participants with the occupational status of unemployed (21.6%) had a good practice on their LSM.
The result of further revealed that the majority of urban residents (36.5%) had relatively a good practice compared to rural residents. It might be urban residents had more access to information about LSM compared to rural residents.
The results of this study show that those with a monthly income below 1000 ETB (13.7%) and (24.2%) 1000–3000 ETB (20.6%) and (28.9%) above 3000 ETB (6.4%) and (6.2%) had a poor and good practice on their LSM, respectively.
The finding of this study was not that satisfactory since there exists much to do to enhance the knowledge, attitude, and practice of diabetes patients.
Conclusions
The finding of the study showed that knowledge and attitude towards lifestyle modification of chronic DM patients attending OPD were generally good. However, the result of practice on lifestyle modification was not good enough.
Recommendations
Lifestyle modification has a great role in the prevention and control of blood glucose raised. But, there has to be much to be done on this regard since its prevalence is increasing rapidly in worldwide especially in under-developing nations on the top of changed lifestyle, the deficit in the knowledge, attitude, and practice towards lifestyle modification. On the basis of the study findings, the following recommendations were forwarded Health education about diabetes and types of lifestyle modification has to be strengthened. Better to create awareness to the community through health education about the importance of physical exercise, weight loss, feet care, cessation of smoking, healthy dietary habit) to general society ought to be implemented by the responsible body.
Abbreviations
ADA, American Diabetic Association; DM, diabetes mellitus; DSME, diabetes self-management education; UOGCSH, University of Gondar Comprehensive Specialized Hospital; IDF, International Diabetic Federation; LSM, lifestyle modification; NCDS, noncommunicable disease; SPSS, Statical Package for Social Sciences; WHO, World Health Organization.
Consent to Publish
This is not applicable.
Data and Material Availability
The data could not be given in order to protect participants’ confidentiality by far for this study. However, the whole summary data is available in the mother document.
The Ethical Approval and Consent of Participating
The study has been performed following the ethical standards laid down in the 1964 Declaration of Helsinki. The approval of the study was done by the University of Gondar, College of Medicine and Health Sciences, School of Nursing Research and Ethical Review Committee so as to precede it. The letter of permission and support was gained from the clinical director of the hospital. All the participants of the study were well informed about the overall rationales of the study. They gave written informed consent to secure their confidentiality.
Acknowledgment
All authors would like to express our deepest appreciation to the University of Gondar College of Medicine and Health Sciences, School of Nursing Research and Ethical Review Committee for approval of the ethical clearance. The authors also would like to give great thanks to data collectors and the supervisors for their devotion and the participants for their unlimited information.
Author Contributions
All the authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All the authors had declared that we have no competing interest concerning this manuscript.
References
1. Brekke HK, Lenner RA, Taskinen M-R, et al. Lifestyle modification improves risk factors in type 2 diabetes relatives. Diabetes Res Clin Pract. 2005;68(1):18–28. doi:10.1016/j.diabres.2004.07.023
2. Kumar V, Tripathi MK, Chauhan PK, Singh PK. Different non-pharmacological approaches for management of type 2 diabetes. J Diabetol. 2013;4(1):1.
3. Yablokov A, Labunska I, Blokov I, et al. The Chernobyl Catastrophe: Consequences on Human Health. Greenpeace International; 2006.
4. Zimmet PZ, Magliano DJ, Herman WH, et al. Diabetes: a 21st century challenge. Lancet Diabetes Endocrinol. 2014;2(1):56–64. doi:10.1016/S2213-8587(13)70112-8
5. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
6. Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care. 2011;34(6):1249–1257. doi:10.2337/dc11-0442
7. WHO. Updates on HIV and Infant Feeding. Maternal, newborn: child and adolescent health; 2019.
8. Rubino F. Is type 2 diabetes an operable intestinal disease?: a provocative yet reasonable hypothesis. Diabetes Care. 2008;31(Supplement 2):S290–S296. doi:10.2337/dc08-s271
9. Levey AS, Coresh J, Balk E, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139(2):137–147. doi:10.7326/0003-4819-139-2-200307150-00013
10. Wens J, Vermeire E, Van Royen P, et al. GPs‘ perspectives of type 2 diabetes patients‘ adherence to treatment: a qualitative analysis of barriers and solutions. BMC Fam Pract. 2005;6(1):20. doi:10.1186/1471-2296-6-20
11. American Diabetes Association. Standards of medical care in diabetes—2017 abridged for primary care providers. Clin Diabetes. 2017;35(1):5.
12. Chan W, Woo J, Hui E. The role of empowerment in the management of chronic diseases in the elderly. In: Aging in Hong Kong. Springer; 2013:183–210.
13. Warshaw HS. Nutrition therapy for adults with type 2 diabetes. Am Diabetes Assoc Guide Nutri Ther Diabetes. 2012;117–142.
14. Association AD. Standards of medical care in diabetes—2010. Diabetes Care. 2010;33(Supplement 1):S11–S61.
15. De Backer G, Ambrosioni E, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of eight societies and by invited experts). Eur Heart J. 2003;24(17):1601–1610. doi:10.1016/s0195-668x(03)00347-6
16. Bekele BB. The prevalence of macro and microvascular complications of DM among patients in Ethiopia 1990–2017: article review. Diabetes Metabol Syndr. 2018.
17. Kajinga RK. Examining the Perceived Nurses’ Support for Self Management Among Type 2 Diabetes Mellitus Patients in Botswana. 2018.
18. Williams R, Van Gaal L, Lucioni C. Assessing the impact of complications on the costs of Type II diabetes. Diabetologia. 2002;45(1):S13–S17. doi:10.1007/s00125-002-0859-9
19. Abebe SM, Berhane Y, Worku A, et al. Diabetes mellitus in North West Ethiopia: a community based study. BMC Public Health. 2014;14(1):97. doi:10.1186/1471-2458-14-97
20. Obirikorang Y, Obirikorang C, Odame Anto E, et al. Knowledge and lifestyle-associated prevalence of obesity among newly diagnosed type II diabetes mellitus patients attending diabetic clinic at Komfo Anokye Teaching Hospital, Kumasi, Ghana: a hospital-based cross-sectional study. J Diabetes Res. 2016;2016.
21. Tadesse E, et al. Assessment of Knowledge, Attitude and Practices Regarding Life Style Modification Among Type 2Diabetic Mellitus Patients Attending Adama Hospital Medical College, Oromia Region, Ethiopia. Global Journal of Medical Research; 2015.
22. Worku D, Hamza L, Woldemichael K. Patterns of diabetic complications at jimma university specialized hospital, southwest ethiopia. Ethiop J Health Sci. 2010;20(1).
23. Berhe KK, KahsayBA G. Adherence to diabetes self-management practices among Type II diabetic patients in Ethiopia: a cross sectional study. Green J Med Sci. 2013;3(6):211–221. doi:10.15580/GJMS.2013.6.071813739
24. Thoma C, Day CP, Trenell MI. Lifestyle interventions for the treatment of non-alcoholic fatty liver disease in adults: a systematic review. J Hepatol. 2012;56(1):255–266. doi:10.1016/j.jhep.2011.06.010
25. Moawad S, et al. Assessment of knowledge among Saudi diabetic children/adolescent at Riyadh city. Am J Nurs Sci. 2014;3(1):5–12. doi:10.11648/j.ajns.20140301.12
26. Lowden A, Moreno C, Holmbäck U, et al. Eating and shift work—effects on habits, metabolism, and performance. Scand J Work Environ Health. 2010;36(2):150–162. doi:10.5271/sjweh.2898
27. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
28. Swift PG. Diabetes education in children and adolescents. Pediatr Diabetes. 2009;10:51–57. doi:10.1111/j.1399-5448.2009.00570.x
29. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Diabetes Educ. 2017;43(1):40–53. doi:10.1177/0145721716689694
30. Ikombele B. Knowledge, Attitudes and Practices Regarding Lifestyle Modifications Among Type 2 Diabetic Patients Attending Mamelodi Hospital, Pretoria, South Africa. University of Limpopo (Medunsa Campus); 2011.
31. Khalil SHA, Megallaa MH, Rohoma KH, et al. Prevalence of type 2 diabetes mellitus in a sample of the adult population of Alexandria, Egypt. Diabetes Res Clin Pract. 2018;144:63–73. doi:10.1016/j.diabres.2018.07.025
32. Umeh AE, Nkombua L. A study of the knowledge and practice of lifestyle modification in patients with type 2 diabetes mellitus in Middelburg sub-district of Mpumalanga. South Afr Fam Pract. 2018;60(1):26–30. doi:10.1080/20786190.2017.1364012
33. Keakile SB. Knowledge, Attitudes and Practices Amongst Diabetes Mellitus Patients About Exercise at a Primary Health Center in Gaborone Botswana. University of Limpopo; 2015.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.