Back to Journals » Vascular Health and Risk Management » Volume 18
Knowledge, Attitude, and Practice Toward Hypertension Among Hypertensive Patients Residing in Lebanon
Authors Machaalani M ![]() , Seifeddine H, Ali A, Bitar H, Briman O, Chahine MN
, Seifeddine H, Ali A, Bitar H, Briman O, Chahine MN ![]()
Received 20 March 2022
Accepted for publication 28 June 2022
Published 13 July 2022 Volume 2022:18 Pages 541—553
DOI https://doi.org/10.2147/VHRM.S367187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Marc Machaalani,1 Houssam Seifeddine,1 Abdallah Ali,1,* Hassan Bitar,1,* Oukba Briman,1,* Mirna N Chahine1– 4
1Faculty of Medical Sciences, Lebanese University, Hadath, Lebanon; 2Basic Sciences Department, Faculty of Medical Sciences, Lebanese University, Hadath, Lebanon; 3Foundation-Medical Research Institutes (F-MRI®), Beirut, Lebanon; 4Foundation-Medical Research Institutes (F-MRI®), Geneva, Switzerland
*These authors contributed equally to this work
Correspondence: Mirna N Chahine, Basic Sciences Department, Faculty of Medical Sciences, Lebanese University, Hadath, Lebanon, Tel +961 76 053292, Email [email protected]
Background and Objectives: Hypertension (HTN) is a major health concern that leads to cardiovascular disease and premature death. Assessing HTN knowledge, attitude, and practice (KAP) is crucial for controlling HTN. This study aimed to determine HTN KAP among hypertensive patients residing in Lebanon.
Methods: This cross-sectional study involved 342 hypertensive patients. A questionnaire form was used to collect data related to patients’ characteristics. SPSS was used to determine KAP scores, descriptive statistics, and correlations.
Results: Data from HTN patients was analyzed of whom 98.2% were Lebanese and 51.2% were males. The median age was 59.15 ± 13.55 years old. A proportion of 40.4% had HTN duration for at least 10 years and 67.3% had HTN family history. Patients had fair HTN knowledge and practice, but good attitude toward HTN. Only 45.3% regularly checked their blood pressure. Positive correlations were observed between HTN attitude and each of knowledge and practice. HTN knowledge and attitude were associated with many studied factors, whereas no relationship was found regarding practice.
Conclusion: Hypertensive patients had fair levels of knowledge and practice, and a good level of attitude concerning their disease. We provided a model for predictors of HTN KAP scores that will allow the development of efficient campaigns related to HTN.
Keywords: hypertension, KAP, Lebanon, hypertensive patients
Introduction
Hypertension (HTN) is a public health problem facing all countries worldwide and one of the leading causes of morbidity and mortality as it is responsible for 7.5 million premature deaths worldwide.1 Known as the “silent killer”, it is often diagnosed incidentally, affecting 31% of the world’s adult population.2 The European and American guidelines set the target blood pressure (BP) below 130/80 mm Hg.3
HTN is highly affected by predisposing factors such as diabetes, lipid disorders, overweight-obesity, hyperuricemia, metabolic syndrome, and unhealthy lifestyle habits.4 Additional risk factors include increased age (>65 years old), male gender, elevated heart rate (>80 beats/min), family history of cardiovascular disease (CVD), and others.3,5 High BP, when left untreated, can also seriously affect vital organs such as the brain, eyes, heart, and kidneys.6
Non-pharmacological strategies to reduce HTN risk and lower BP are as follows: weight loss in any patient above the upper limit of the “normal weight” ([18.5–25]kg/m2), namely overweight (BMI: [25–30]kg/m2) and obese (BMI ≥ 30 kg/m2) patients, smoke cessation, reduced alcohol consumption, dietary supplements, self-measured BP monitoring, and exercise.7,8 Dietary modification is also essential, the Dietary Approaches to Stop Hypertension (DASH) diet is the most effective diet, as well as the Mediterranean, low sodium, low carbohydrate, high protein dietary approaches that are also beneficial compared to control diet.9
In the Arab countries, the prevalence rate of HTN was about 29.5% in 2014, which corresponds to a higher prevalence of HTN compared to patients from the USA (28%) and sub-Saharan African countries (27.6%).10 In Lebanon, in that same year, a cross-sectional study reported a higher prevalence rate of HTN (31.2%) and a poor BP control rate (28.7%) and identified that age, weight, and history of CVD were significant risk factors.11 More recently, through the May Measurement Month (MMM) 2019 screening campaign intended to raise awareness, Najem et al recorded a rising prevalence rate of 36.6%,12 which is higher than the rate reported by other MMM studies in Italy (31.1%)13 and Vietnam (33.8%)14 in the same year. Despite the high prevalence of HTN in Lebanon, there is a significant lack in the identification of symptoms and complications of this disease.
It is obvious that primary prevention, early diagnosis, and BP control are recommended since early adulthood.15 The levels of knowledge, attitude, and practice (KAP) regarding HTN in hypertensive patients play a significant role in controlling modifiable risk factors and reducing burden through assessing the gaps and improving awareness and perception.16 Studies demonstrated that good knowledge of HTN is associated with higher rates of BP control,17,18 medication adherence, as well as decreasing morbidity and mortality.19
Several community-based studies regarding HTN KAP were conducted in different countries and have shown varying results.18–21 For instance, while a poor level of knowledge was reported among patients with uncontrolled HTN, by Almas et al in Karachi, Pakistan,28 Olowe et al described a moderate level of knowledge in the South African province KwaZulu-Natal,19 and hypertensive patients in Iran exhibited an average level of knowledge.21 In contrast, a good knowledge of HTN has been revealed in studies from Sudan22 and Ethiopia.23
Similarly, an attitude of moderate level has been described in South Africa19 and Nepal compared to a good level among hypertensive patients from Baghdad, Iraq, and Michigan, the United States.24,25
Practice levels toward HTN have shown varying results as well, from poor26 to fair,24 and good25 in different hypertensive communities.
Despite the aforementioned impact and role of KAP studies, no study to our knowledge has investigated KAP of hypertension in hypertensive patients in Lebanon. Therefore, in our cross-sectional study, we aimed to assess the baseline KAP of HTN among hypertensive patients residing in Lebanon, while identifying the factors affecting HTN KAP scores and the predictors of KAP score parameters in hypertensive patients.
Methods
Ethical Considerations
Prior to proceeding with our study, we were granted the IRB approval from the ethical committee of Al Hayat Hospital (Reference Number: ETC-19-2020). The beginning of the questionnaire included an informed consent that covered the background, objectives, and procedures of the work. Patients were assured of the completely voluntary nature of their participation and the freedom to decline without justification. Our study was confidential where all identities remained anonymous and filled forms were securely stored. This study was conducted in accordance with Good Clinical Practice ICH Section three, and the principles laid down by the 18th World Medical Assembly Declaration of Helsinki (Helsinki, 1964) and all applicable amendments.
Study Design and Study Population
This cross-sectional study was conducted to assess KAP towards HTN in hypertensive patients. Eligible patients were ≥18 year-old, diagnosed as hypertensive (Systolic BP ≥ 130 and/or Diastolic BP ≥ 90) by a healthcare professional, residing in Lebanon, and able to understand Arabic or English. Excluded patients were pregnant women and patients with psychiatric disorders. Using Cochran formula (Z = 1.96 and alpha error = 0.05) and knowing that the prevalence of hypertensive patients in Lebanon is 31.2%,14 the minimum required sample of hypertensive patients was 330.
Tools and Procedures of Data Collection
Questionnaire’s Translation and Validation
At the time of the interview, HTN patients, previously admitted to hospitals or private clinics, had left hospitals/private clinics in the last 6 months to 2 years preceding the interview, with more than 70% of them who had left in the last 1.5 years to 2 years. Based on their files where their residency area was mentioned, we contacted our patients and recruited them from the 8 governorates of Lebanon from December 2020 until February 2021 to have an equal representation of the hypertensive population from the whole territory”. KAP towards HTN was assessed using an electronic survey uploaded to Google Forms based on a structured questionnaire24 requiring no more than 15 minutes. Patients were asked, depending on their preference, either to fill the survey themselves (only 25% preferred this option) or to answer the questions orally over phone calls or face-to-face interviews with our well-trained team (75% preferred this option) directly into the Google Form. The questionnaire was available in both English and Arabic. The questionnaire was first translated by a professional translator from English to Arabic using the inverted method of Fortin.27 A back translation to English by a different professional translator was then performed to ensure no deviations from the original questionnaire were present. A pre-test was carried out with ten individuals who were not part of the sample in order to validate the understanding and clarity of the items and perform the necessary modifications.
Survey Tool
The survey comprised the following:
- An informed consent that encompassed a brief description of the study and its objectives as well as a statement of the voluntary nature of participation, anonymity, and confidentiality.
- Thirteen questions on socio-demographic and other patient-related characteristics (the patient’s gender, age group, nationality, residency, education, occupation, marital status, smoking, alcohol drinking, duration of HTN, family history of HTN, and source of information). A current smoker was considered as a person who had smoked at least 100 cigarettes in their lifetime and who was still smoking at the time of the study, whereas an ex-smoker had quit smoking at the time of the study. A current drinker was considered as a person who had consumed at least one alcoholic drink in their lifetime and who was still drinking at the time of the study, whereas an ex-drinker who had quit drinking at the time of the study. An uneducated individual was considered as someone who had not received any formal education. Reaching university level refers to someone who had earned at least bachelor’s degree, and a doctorate level refers to a PhD or M.D. degree. Regarding occupation, free work refers to someone who was self-employed and generating income, unemployed indicated that the person was jobless but actively looking for a job, and a homemaker was defined as a person whose main occupation is managing a household.
- Ten questions about HTN knowledge (definition, normal BP range, symptoms, risk factors, complications, treatment, and prevention), 10 questions about HTN attitude, and 10 questions about HTN practice (regular measuring of lipid profile and BP, diet plan, salt intake, adherence to treatment, exercise, etc.).
Grading of Scores
In the knowledge and practice sections, every correct answer was granted 1 point and each wrong answer a 0. In the attitude section, a 5-point Likert scale was adopted in which: 1 “strongly disagree”, 2 “disagree”, 3 “Neutral”, 4 “agree”, 5 “strongly agree” and 0 “Don’t Know”, for all items except “Increasing salt and sugar intake is beneficial for health” and “Taking treatment regularly can make hypertension a chronic disease” where the scale was reversed.
Computed scores were graded into categories and subcategories from “Limited” (Poor, Fair) to “Adequate” (Good, Excellent) levels of KAP, according to the Median of the scores and “a modified form” of the widely adopted Bloom’s cutoff points28 (Table 1).
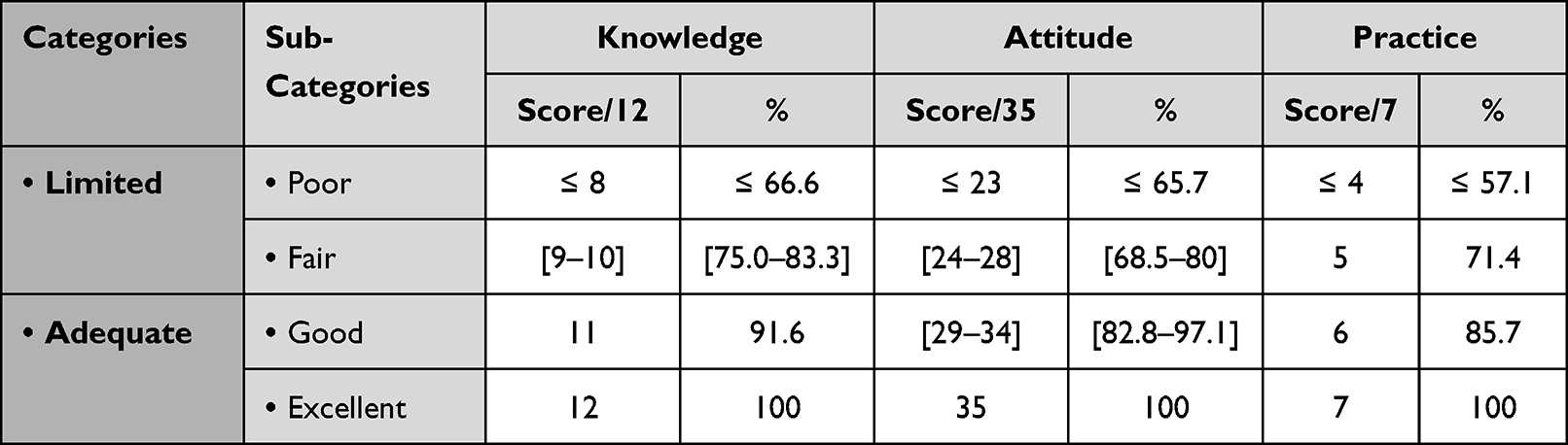 |
Table 1 Grading of Knowledge, Attitude, and Practice Scores About HTN into Categories “Limited and Adequate” and Sub-Categories “Poor, Fair, Good, and Excellent” |
Data Analysis
Collected data was analyzed using Statistical Package for Social Sciences (SPSS) software (version 25). Data were represented as frequencies and proportions of the nominal variables and as mean (±SD) for the continuous variables. Scores of KAP were computed. Reliability analysis was realized to validate each of these 3 scores by using the Cronbach’s alpha coefficient. Alpha Cronbach of 0.7 and higher indicates acceptable internal consistency of the score.
Descriptive analysis was used for the representation of the sample characteristics and KAP data. In addition, Shapiro–Wilk’s test (p < 0.05) showed that the scores were not normally distributed with a skewness and kurtoses out of the range (−1.96 and +1.96). The correlation between KAP scores and demographic characteristics was tested. Bivariate analysis and correlations were conducted using statistical analysis tests: Mann Whitney test, Kruskal Wallis test, Spearman correlation test, and Chi-Square. Multivariate linear regression was conducted in order to test the factors affecting each of the three scores. Statistical significance was indicated by a p-value less than 0.05 (using alpha error = 5%).
Results
Demographics and Other Patient-Related Characteristics
“Initially, out of 650 hypertensive patients that were contacted, 413 accepted to fill out the questionnaire (response rate of 63.5%) and only 342 patients fulfilled the inclusion criteria of our study.” A total of 336 hypertensive patients were Lebanese (98.2%), while the remaining were Syrians (1.6%). A proportion of 51.2% were males and 76.3% were married. The mean age of the patients was 59.15 ± 13.55 years with the youngest patient being 18-year-old and the oldest 91-year-old. The majority of patients had high educational level as only 12% were uneducated. A proportion of 40.4% of patients claimed a duration of HTN exceeding 10 years. Family history of HTN was reported by 67.3% of patients. Other details about demographics are found in Table 2.
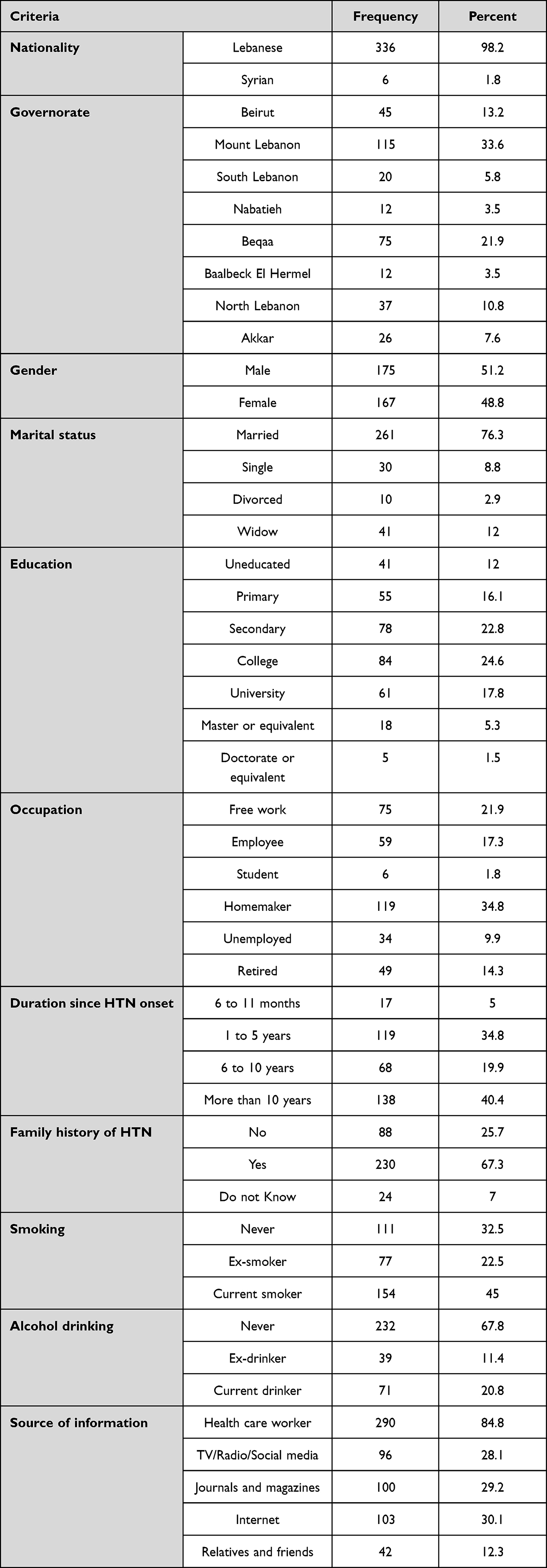 |
Table 2 Distribution of the Enrolled Hypertensive Patients According to Their Demographics and Other Characteristics (N = 342) |
HTN-Related KAP
KAP Scores
Results showed that the patients had fair levels of knowledge and practice, and a good level of attitude concerning HTN. Knowledge scores varied between 2 and 12 points with an average of 9.05 ± 2.08 over 12 (75.4%) and practice scores varied between 0 and 7 points with an average of 4.22 ± 1.58 over 7 (60.2%), whereas attitude scores varied between 21 and 35 points with an average of 30.45 ± 3.33 over 35 (87.0%). Only 25.1% and 21.9% of HTN patients demonstrated an “Adequate” Knowledge and Practice levels about HTN, respectively. However, 67.2% of HTN patients showed an “Adequate” Attitude level toward HTN (Figure 1).
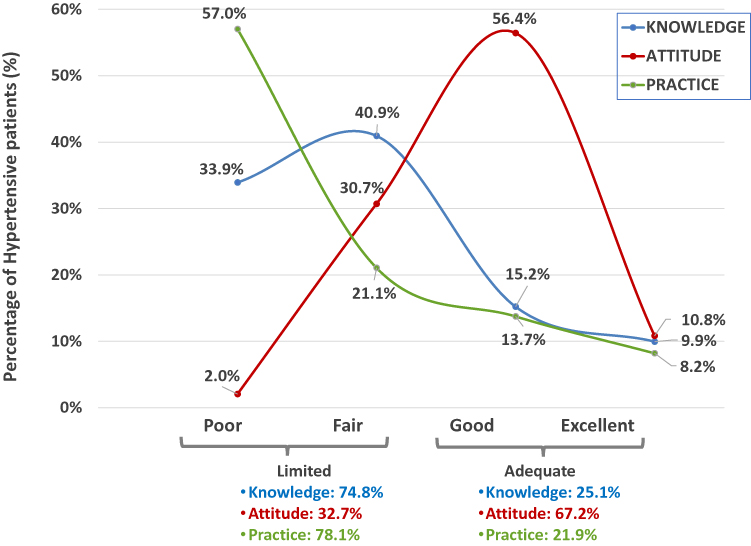 |
Figure 1 Percentage (%) of HTN patients with KAP scores represented in categories (Limited/Adequate) and sub-categories (Poor/Fair/Good/Excellent). |
HTN-Related Knowledge
A proportion of 74.85% of HTN patients reported a “Limited” (33.9% Poor and 40.9% Fair knowledge scores) Knowledge level about HTN. Only 25.15% of HTN patients showed an “Adequate” Knowledge level about HTN (Figure 1).
Results showed that our patients correctly identified that HTN can be treated by regular intake of medication (98%) and that a low salt diet was the appropriate diet for HTN (95.9%). On the other hand, very few patients knew that HTN cannot be treated by traditional medicine (39.8%) or by garlic (33.6%). Nevertheless, most of the questions were fairly identified since 80.7% of patients knew that HTN was a chronic disease, and 78.4% correctly identified that it was related to the cardiovascular system. Patients had a good knowledge of the normal range of BP as 88% knew that it was 120/80. Moreover, 80.1% of the patients answered correctly that the main symptom of HTN was a headache. A proportion of 78.9%of patients knew that obesity was a predisposing factor for HTN. Detailed responses to the knowledge section of our questionnaire are provided in Table S1.
HTN-Related Attitude
A proportion of 32.75% of HTN patients reported a “Limited” (2.0% Poor and 30.7% Fair Attitude scores) Attitude level about HTN. A percentage of 67.25% of HTN patients showed an “Adequate” Attitude level about HTN (Figure 1).
A proportion of 51.8% of patients strongly agreed and 38.6% agreed with the statement that it was better to have a normal body weight to be protected from hypertension. Thus, patients showed a good attitude towards this item with a mean score of 4.37 ± 0.8 over 5. A similar trend was observed for all remaining attitude questions as seen in Table S2. Other results, not computed within the “Attitude” score, revealed that only 8.2% and 24.3% of patients strongly agreed and agreed, respectively, that smoking causes health problems. In addition, the majority of HTN patients believed that taking treatment regularly could make HTN a chronic disease. Thus, a poor attitude score was associated with this specific item (2.04 ± 1.13). Other questions excluded from the scoring system for attitude are found in Table S2.
HTN-Related Practice
A proportion of 78.07% of HTN patients had a “Limited” (57.0% Poor and 21.1% Fair Practice scores) Practice level about HTN. Only 21.93% of HTN patients showed an “Adequate” Practice level about HTN (Figure 1).
The results revealed that 90.9% of patients regularly take their medication. In contrast, only 24.9% followed a regular continuous exercise routine, 45.3% checked their BP regularly, and 52.3% tried to reduce their weight. Nevertheless, most HTN-related practice questions were fairly identified (low salt diet, low-fat diet, avoiding physical and emotional stress). Detailed responses are presented in Table S3. Other results, not computed within the practice score, showed that 88% of the patients take their medication by themselves and half of the patients answered that the medications were expensive. Patients checked their BP predominantly using their own sphygmomanometer (89.2%) (Table S3).
Correlation Among KAP Score Parameters
The results of the Spearman correlation test revealed that knowledge was positively correlated with attitude (p-value <0.001, r = 0.351) but not with practice (p-value = 0.275) and that attitude and practice were also positively correlated (p-value=0.008, r = 0.143) (Figure 2).
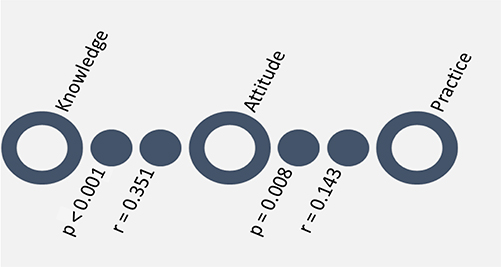 |
Figure 2 Graphical representation of the results of the Spearman correlation test: Attitude toward HTN in hypertensive patients is correlated with knowledge and practice toward HTN, yet practice and knowledge are not correlated with one another. “r” is the correlation coefficient, “p” is the probability value. |
Factors Affecting KAP Scores of the Enrolled Hypertensive Patients (Bivariate Analyses)
The highest mean knowledge score of HTN was significantly associated with the marital status of the patients, with the highest score among divorced patients (9.8 ± 1.317 over 12) and the lowest among widows (7.98 ± 2.219 over 12) (p-value = 0.002). The educational level favored a higher knowledge score (p-value <0.001). Patients with a lower duration of 6 to 11 months since HTN onset (p-value = 0.015) recorded the lowest mean knowledge score (7.76 ± 2.33) (Table 3). More details are presented in Table S4.
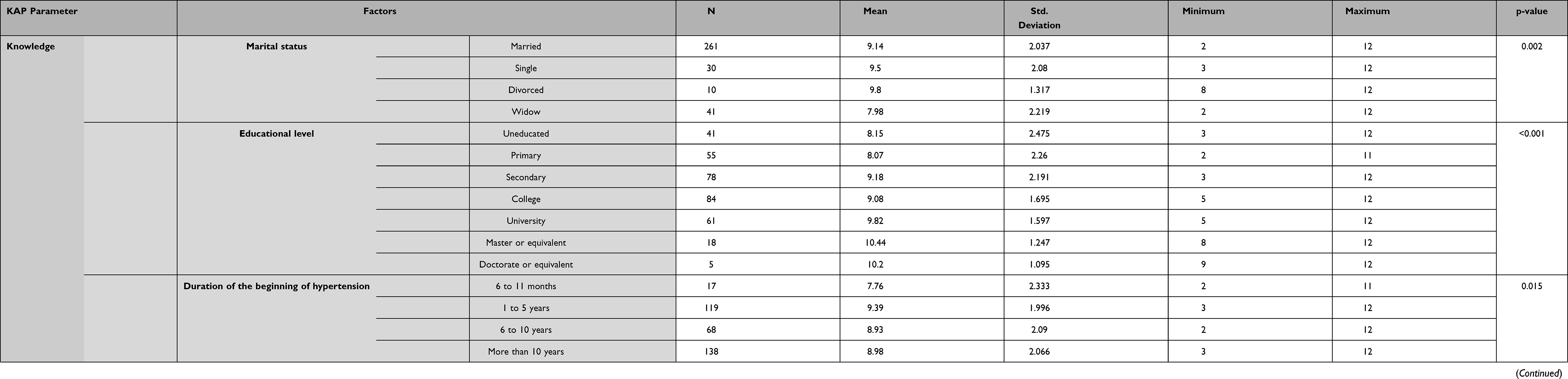 |
Table 3 Factors Significantly Affecting Knowledge and Attitude Scores Among Enrolled Hypertensive Patients in This Study (N = 342) (Bivariate Analyses) |
Mean scores of HTN-related attitude varied among patients depending on the governorate they reside in (p-value <0.001). Those living in Akkar had the highest mean attitude score (31.92 ± 1.809 over 35), whereas those living in Beqaa had the lowest score (29.08 ± 3.498 over 35) yet they still had a good attitude. Results also revealed that higher educational level (p-value = 0.004), and longer duration of HTN onset (more than 10 years) (p-value = 0.01) and non-smoker status (p-value = 0.015) were significantly positively correlated with the best attitude in comparison with their counterparts as seen in Table 3. More details are presented in Table S5.
No significant correlation was reported between the mean practice scores concerning HTN and any of the studied factors: nationality, governorate, gender, marital status, educational level, work, duration of HTN onset, family history of HTN, and smoking or alcohol consumption (all p-values >0.05). More details are presented in Table S6.
Spearman correlation test revealed a significant negative correlation between age and knowledge (p-value <0.001, r = −0.213) but no correlation was found between age and each of the attitude and practice scores (p-values ˃0.05).
Predictors of KAP Among Hypertensive Patients
Multiple linear regression was applied to identify predictors of knowledge about HTN among hypertensive patients. Knowledge about HTN increased with education (β = 0.311, p < 0.001). Better attitude toward HTN was favored by a good knowledge about HTN, longer duration since HTN onset, and living outside Beqaa (β = 0.39, β = 0.133, β = −0.176, respectively, all p < 0.001). Finally, a better practice toward HTN improved with a better attitude toward HTN. (p = 0.003, β= 0.161) (Figure 3).
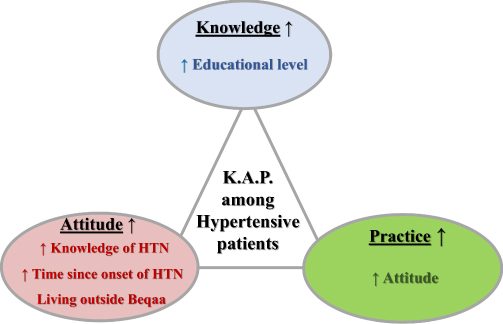 |
Figure 3 Major factors affecting KAP among patients with hypertension. |
Discussion
This study aimed to determine the Knowledge, Attitude, and Practice (KAP) toward hypertension (HTN) among hypertensive patients residing in Lebanon while identifying the factors affecting and parameters predicting the HTN KAP scores in these patients. Results showed that 40.4% of patients had hypertension for more than 10 years and 67.3% had a family history of HTN compared to 53% and 21.1% in Sri Lanka29 and Ethiopia,30 respectively. In 2015, it was reported in Lebanon by Matar et al that 30% of the studied 1697 adults were graded as pre-HTN and 36.9% as hypertensive.31 We also found that 45% of HTN patients were current smokers and 20.8% were current alcohol drinkers.
Knowledge About Hypertension
Our results showed that 74.8% of patients had “Limited” knowledge about HTN (Figure 1). Similarly, a study assessing HTN KAP among hypertensive patients in Iran showed that patients had average HTN knowledge.21 In contrast, a good knowledge toward HTN has been reported in 2 studies in Sudan22 and Ethiopia.23 Of the hypertensive patients enrolled in our study, 88% knew the normal BP range and 78.9% knew that obesity is a risk factor. These rates are very close to the ones reported in the KAP study in Iran.21 Although 98% of patients knew that HTN can be treated by regular intake of medication, some mistakenly thought that it could be treated using traditional medicine (17%) or garlic intake (40.4%). Additionally, the use of complementary alternative medicine and herbal treatments is a common practice among hypertensive patients in South Africa.32 Our study also revealed that the knowledge related to HTN in hypertensive patients was significantly associated with the marital status, educational level, duration of HTN onset, and age, with the latter showing an inverse correlation between increased age and knowledge about HTN. It was not surprising to find that an increased level of education directly correlated to an increased knowledge score (Figure 3), which is in agreement with the results of Rashidi et al21 and Oliveria et al, the latter showing that higher education level correlated with better awareness, attitudes, and perceptions related to HTN.25 In addition, the older the patient, the lower the knowledge about HTN. While no associations between gender and HTN KAP scores were reported in our study (p-values >0.05), some studies found better knowledge of HTN among males.18,24
Attitude Toward Hypertension
Our findings showed that 67.2% of HTN patients had an “Adequate” Attitude toward HTN (Figure 1). For instance, 62.3% of the studied patients strongly agreed and 35.5% agreed that regular exercise improves their health. This was in disagreement with the results of a study conducted by Shrestha et al in which only 41.5% answered correctly that regular exercise is good for a healthy life.26 In that same study, however, our results showed similar correct answers regarding the harmful effects of salt and sugar intake.25 Moreover, we found that attitudes varied depending on factors like location, educational level, duration of HTN onset, and smoking. A positive correlation was observed between attitude and knowledge (Figure 2). The attitude score also improves as the duration of HTN increases (Figure 3), contrary to the findings of Rashidi et al which reported that the duration was not associated with any KAP score parameter.21
Practices Towards Hypertension
Furthermore, this study revealed that 78.1% of HTN patients had a “Limited” practice levels in relation to HTN (Figure 1). To illustrate such poor practices towards HTN, only 45.3% of patients in our study regularly check their BP. In accordance with our results (90%), a good level of adherence to antihypertensive medications has been reported in Sri Lanka29 and Ethiopia.30 In contrast, a fair level of practice and inadequate adherence to HTN treatment and prevention measures have been described in Iraq.24 We found that 88% of hypertensive patients took their medication by themselves, 89.2% checked their BP at home, and 50% found medications expensive. Abbas et al reported that Lebanese hypertensive patients tend to routinely measure their BP at home (72%) and that the major barrier to HTN treatment non-adherence was forgetfulness (89.2%) rather than high cost (2.7%).33
In this study, positive correlations were observed between attitude and knowledge (p-value <0.001, r = 0.351) as well as between attitude and practice (p-value = 0.008, r = 0.143) (Figure 2). Similar results were found in Ethiopia, where good practice was related to a good attitude toward HTN.23
Study Limitations
This study was subject to some biases: selection, volunteering, and reporting biases.
- Volunteering bias: Eventually, only those who think to know better about HTN, mostly accepted to participate in our study (response rate: 63.5%).
- Selection/sampling bias: The surveying method limited the ability to reach uneducated or underprivileged populations. In addition, a slight sampling bias may have originated from the fact that, although all HTN patients had left hospitals/private clinics when the survey was conducted; however, 30% and 70% of them had left 6 months and between 1.5 and 2 years before the survey was conducted, respectively. This difference may have affected the levels of KAP toward HTN to be eventually higher (but not necessarily) in those who have left the hospitals 6 months earlier compared with those who had left 2 years earlier; however, the former ones were in minor proportion (30%).
- Self-reporting bias. The self-reporting nature of the questionnaire may have given the patient enough time to check the internet or textbook sources to respond correctly to knowledge and practice questions about HTN, for example. Therefore, to reduce this bias, our team was well trained to address around 75% of the overall HTN patients via face-to-face or phone interviews, thus limiting the time for patients to provide biased data.
Study Perspectives
This is the most recent HTN KAP study in Lebanon involving hypertensive patients residing in Lebanon from different backgrounds. HTN KAP assessment among those patients is the cornerstone for the development of targeted interventions to improve HTN self-management behaviors in Lebanon. The understanding of the impact of different sociodemographic factors on HTN KAP can facilitate the implication of multisystemic interventions that involve patients, clinicians, healthcare organizations, and communities, which may lead to substantial improvements in HTN control with a further reduction of HTN burden on the Lebanese society. Future studies should evaluate HTN KAP in the general Lebanese population as this will be beneficial in assessing the risk of HTN and allocating gaps in knowledge and flawed practices that should be corrected even before the manifestation of the disease per se (prevention). Studies should also focus on the adherence of hypertensive patients to their treatment, identify some barriers, and assess their risk of developing HTN sequelae.
Conclusion
This study revealed that hypertensive patients residing in Lebanon had fair levels of knowledge and practice, and a good level of attitude concerning HTN. The predictors of HTN KAP in hypertensive patients identified in this study were the educational level, duration since hypertension onset, marital status, location, and smoking status. Thus, effective awareness campaigns should be tailored according to their gaps in knowledge, malpractices, and poor attitudes. Such guidance can be achieved through national campaigns on social media or on television, providing reliable resources on the Internet, and increasing emphasis on educating HTN patients about their condition during doctor visits.
Acknowledgments
Abdallah Ali, Hassan Bitar and Oukba Briman all contributed equally to this work. We are grateful to every patient with hypertension who participated in our study. We are extremely thankful to Mr. Bachir Atallah for his contribution to the statistical analysis of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. A global brief on hypertension. Who.int; 2014. Available from: https://www.who.int/cardiovascular_diseases/publications/global_brief_hypertension/en/.
2. Lawes CM, Vander Hoorn S, Rodgers A. International Society of Hypertension. Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371(9623):1513–1518. doi:10.1016/S0140-6736(08)60655-8
3. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):2199–2269. doi:10.1016/j.jacc.2017.11.005
4. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. doi:10.1016/S0140-6736(06)68770-9
5. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. doi:10.1161/HYPERTENSIONAHA.120.15026
6. Buang NFB, Rahman NAA, Haque M. Knowledge, attitude and practice regarding hypertension among residents in a housing area in Selangor, Malaysia. Med Pharm Rep. 2019;92(2):145–152. doi:10.15386/mpr-1227
7. Oza R, Garcellano M. Nonpharmacologic management of hypertension: what works? Am Fam Physician. 2015;91(11):772–776.
8. Paffer Filho S, Toscano Paffer M, Moura MP1, Barros L1, Caminha N1, Toscano Paffer T. Non-pharmacological treatment for hypertension. J Hypertens. 2019;37:e251–e252. doi:10.1097/01.hjh.0000573216.49484.4c
9. Schwingshackl L, Chaimani A, Schwedhelm C, et al. Comparative effects of different dietary approaches on blood pressure in hypertensive and pre-hypertensive patients: a systematic review and network meta-analysis. Crit Rev Food Sci Nutr. 2019;59(16):2674–2687. doi:10.1080/10408398.2018.1463967
10. Tailakh A, Evangelista LS, Mentes JC, Pike NA, Phillips LR, Morisky DE. Hypertension prevalence, awareness, and control in Arab countries: a systematic review. Nurs Health Sci. 2014;16(1):126–130. doi:10.1111/nhs.12060
11. Cherfan M, Blacher J, Asmar R, et al. Prevalence and risk factors of hypertension: a nationwide cross-sectional study in Lebanon. J Clin Hypertens. 2018;20(5):867–879. doi:10.1111/jch.13268
12. Najem RN, Halawi A, Tanios B, et al. May measurement month 2019: an analysis of blood pressure screening results from Lebanon. Eur Heart J Suppl. 2021;23(Suppl B):B92–B94. doi:10.1093/eurheartj/suab037
13. Torlasco C, Faini A, Pengo MF, et al. May measurement month 2019: an analysis of blood pressure screening results from Italy. Eur Heart J Suppl. 2021;23(Suppl B):B77–B81. doi:10.1093/eurheartj/suab054
14. Minh HV, Poulter NR, Viet NL, et al. Blood pressure screening results from may measurement month 2019 in Vietnam. Eur Heart J Suppl. 2021;23(Suppl B):B154–B157. doi:10.1093/eurheartj/suab035
15. Miura K, Daviglus ML, Dyer AR, et al. Relationship of blood pressure to 25-year mortality due to coronary heart disease, cardiovascular diseases, and all causes in young adult men: the Chicago Heart Association Detection Project in Industry. Arch Intern Med. 2001;161(12):1501–1508. doi:10.1001/archinte.161.12.1501
16. Aung MN, Lorga T, Srikrajang J, et al. Assessing awareness and knowledge of hypertension in an at-risk population in the Karen ethnic rural community, Thasongyang, Thailand. Int J Gen Med. 2012;5:553–561. doi:10.2147/IJGM.S29406
17. Sharma S, Kc B, Alrasheedy AA, Kaundinnyayana A, Khanal A. Impact of community pharmacy-based educational intervention on patients with hypertension in Western Nepal. Australas Med J. 2014;23(Supplement_B):304–313. doi:10.4066/AMJ.2014.2133
18. Almas A, Godil SS, Lalani S, Samani ZA, Khan AH. Good knowledge about hypertension is linked to better control of hypertension; a multicentre cross sectional study in Karachi, Pakistan. BMC Res Notes. 2012;5:579. doi:10.1186/1756-0500-5-579
19. Olowe OA, Ross AJ. Knowledge, adherence and control among patients with hypertension attending a peri-urban primary health care clinic, KwaZulu-Natal. Afr J Prim Health Care Fam Med. 2017;9(1):e1–e7. doi:10.4102/phcfm.v9i1.1456
20. Levinthal BR, Morrow DG, Tu W, Wu J, Murray MD. Cognition and health literacy in patients with hypertension. J Gen Intern Med. 2008;23(8):1172–1176. doi:10.1007/s11606-008-0612-2
21. Rashidi Y, Manaflouyan H, Pournaghi Azar F, Nikniaz Z, Nikniaz L, Ghaffari S. Knowledge, attitude and practice of Iranian hypertensive patients regarding hypertension. J Cardiovasc Thorac Res. 2018;10(1):14–19. doi:10.15171/jcvtr.2018.02
22. Abdalla AA. Knowledge, attitude and practice towards therapeutic lifestyle changes in the management of hypertension in Khartoum State. Cardiovasc J Afr. 2021;32(4):198–203. doi:10.5830/CVJA-2021-011
23. Bogale S, Mishore KM, Tola A, Mekuria AN, Ayele Y. Knowledge, attitude and practice of lifestyle modification recommended for hypertension management and the associated factors among adult hypertensive patients in Harar, Eastern Ethiopia. SAGE Open Med. 2020;8:2050312120953291. doi:10.1177/2050312120953291
24. Sadeq R, Latfa R. Knowledge, attitude and practice about hypertension in hypertensive patients attending hospitals in Baghdad, Iraq. South East Asia J Public Health. 2017;7(1):29–34. doi:10.3329/seajph.v7i1.34676
25. Oliveria SA, Chen RS, McCarthy BD, Davis CC, Hill MN. Hypertension knowledge, awareness, and attitudes in a hypertensive population. J Gen Intern Med. 2005;20(3):219–225. doi:10.1111/j.1525-1497.2005.30353.x
26. Shrestha S, Adhikari B, Poudel RS, et al. Knowledge, attitude and practice on hypertension among antihypertensive medication users. JNMA J Nepal Med Assoc. 2016;55(204):86–92. doi:10.31729/jnma.2848
27. Fortin MF, Gagnon J. Fondements et étapes du processus de recherche: Méthodes quantitatives et qualitatives.
28. Seid MA, Hussen MS. Knowledge and attitude towards antimicrobial resistance among final year undergraduate paramedical students at University of Gondar, Ethiopia. BMC Infect Dis. 2018;18(1):312. doi:10.1186/s12879-018-3199-1
29. Ralapanawa U, Bopeththa K, Wickramasurendra N, Tennakoon S. Hypertension knowledge, attitude, and practice in adult hypertensive patients at a tertiary care hospital in Sri Lanka. Int J Hypertens. 2020;2020:1–6. doi:10.1155/2020/4642704
30. Worku Kassahun C, Asasahegn A, Hagos D, et al. Knowledge on hypertension and self-care practice among adult hypertensive patients at university of Gondar comprehensive specialized hospital, Ethiopia, 2019. Int J Hypertens. 2020;2020:5649165. doi:10.1155/2020/5649165
31. Matar D, Frangieh AH, Abouassi S, et al. Prevalence, awareness, treatment, and control of hypertension in Lebanon. J Clin Hypertens. 2015;17(5):381–388. doi:10.1111/jch.12485
32. Hughes GD, Aboyade OM, Clark BL, Puoane TR. The prevalence of traditional herbal medicine use among hypertensives living in South African communities. BMC Complement Altern Med. 2013;13:38. doi:10.1186/1472-6882-13-38
33. Abbas H, Kurdi M, Watfa M, Karam R. Adherence to treatment and evaluation of disease and therapy knowledge in Lebanese hypertensive patients. Patient Prefer Adherence. 2017;11:1949–1956. doi:10.2147/PPA.S142453
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.