Back to Journals » Infection and Drug Resistance » Volume 14
Knowledge, Attitude and Practice Toward COVID-19 Pandemic Among Population Visiting Dessie Health Center for COVID-19 Screening, Northeast Ethiopia
Authors Gebretsadik D ![]() , Gebremichael S
, Gebremichael S ![]() , Belete MA
, Belete MA ![]()
Received 12 December 2020
Accepted for publication 4 February 2021
Published 5 March 2021 Volume 2021:14 Pages 905—915
DOI https://doi.org/10.2147/IDR.S297047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Daniel Gebretsadik, Saba Gebremichael, Melaku Ashagrie Belete
Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Daniel Gebretsadik
Department of Medical Laboratory Science, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Tel +251-910541073
Email [email protected]
Background: Coronavirus 2019 (COVID-19) is currently a global health threat and an international public health emergency. As of 21 January 2021, 97.8 million cases with more than two million deaths were recorded worldwide while in Ethiopia 132,326 confirmed cases and 2057 deaths were reported. Hence, the aim of the present study was to determine the magnitude of knowledge, attitude, and practice toward COVID-19 among the population who visited the health center for COVID-19 screening.
Methods: A health institution-based cross-sectional study was conducted among the 384 study population visiting Dessie health center for COVID-19 screening from September 1, to October 21, 2020 using a simple random sampling technique. A structured questionnaire was used to obtain information related to sociodemographic characteristics, Knowledge (eleven questions), attitude (six questions) and practice (nin questions). Both bivariable and multivariable logistic regression analyses with a 95% confidence interval were used to identify factors associated with poor knowledge and practice. A P-value of < 0.05 was considered statistically significant.
Results: Out of the total study participants 61.5% were males, 52.6% of them were aged between 30 and 49 years and 85.2% of them were living in urban areas. The magnitude of poor knowledge and poor practice was 187 (48.7%) and 160 (41.7%), respectively. Poor knowledge had statistically significant association with Illiteracy (AOR= 5.53, 95%CI= 1.03-29.68, P= 0.046) and having no contact history (AOR=0.39, 95%CI=0.21– 0.73, P=0.003). Statistically significant association existed between poor practice and parameters which addressed educational status, travel history, and poor knowledge level of study participants.
Conclusion: Alarmingly high poor knowledge, negatively skewed attitude, and poor practice regarding the COVID-19 pandemic was indicated. Therefore, health education programs aimed at mobilizing and improving COVID-19-related knowledge, attitude, and practice are urgently needed, especially for those who are illiterate, having travel and contact history, or generally among underprivileged populations.
Keywords: COVID-19, KAP, Ethiopia
Background
Coronaviruses are a group of large enveloped viruses with single stranded, positive-sense RNA genome that can cause a variety of respiratory diseases in humans, from the mild common cold to severe acute respiratory syndrome (SARS).1,2 Coronavirus had previously caused outbreaks of SARS in 2003 in China and Middle East respiratory syndrome (MERS) in the Middle East in 2013 due to SARS-CoV and MERS-CoV, respectively.3–5
A novel coronavirus now known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first reported as the pathogen causing coronavirus disease (COVID-19) in the city of Wuhan, Hubei province, China in December 2019.6–8 This outbreak is believed to have an epidemiological linkage to the epicenter, the Huanan Seafood Wholesale Market where bats, snakes, and different raw sea foods were sold. The WHO declared COVID-19 a pandemic disease on January 30, 2020.9
COVID-19 is currently a global health threat and an international public health emergency. The pandemic is now reported to have spread to almost all countries of the world raising great public health concern globally; and since the start of the outbreak, the global pandemic has surpassed 97.8 million cases worldwide with more than two million deaths to January 21, 2021. Among the total of more than 220 countries and territories affected by the pandemic, the highest rates of infection and death have been recorded in the USA, India, and Brazil.10–13
Africa has been affected by the pandemic lately and a total of 3.3 million cases and 82,601 deaths were recorded as of January 21, 2021.14 Despite its anticipated vulnerability, mainly as a result of poor health system and economy, a relatively low number of cases have been reported from the African region compared to other continents around the world. This is mainly due to the low testing capacity and poor reporting habits. The first confirmed case of COVID-19 in Ethiopia was reported on March 13, 2020.15 The number of COVID-19 cases continues to escalate in Ethiopia with a total of 132,326 confirmed cases and 2057 deaths as of 21 January 2021.12
The pandemic affects nearly all countries in the world impacting the majority of human activities including the economy and health systems. Currently, despite promising progress towards effective vaccine, there is no effective cure for COVID-19. Moreover, the newly deployed containment measures, such as increased testing, contact tracing, isolation of confirmed cases, quarantine of contact and suspected cases and nonpharmacological interventions like social distancing, staying in home, working from home, self-monitoring, public awareness, self-quarantine are likely to impede (slow down) the actual epidemic growth, but will not stop it.16,17 For instance, the initial most affected countries, such as China and South Korea, could contain disease spread by deploying liberal population testing, strict quarantine of people under investigation, and isolation of the positive cases.17
Therefore, early identification of symptoms and prompt seeking of supportive medical care and prevention practices promote better recovery from the deadly disease and halt the spread of the virus. Moreover, despite there having been imminent prevention strategies imposed by the Ethiopian government such as social distancing, hand washing, travel restrictions, and use of alcohol hand rub and face masks, these preventive and control measures are not currently being applied throughout the country. Such effective prevention and control of COVID-19 is attained through improving the knowledge, attitude, and practice of the general community and most importantly, the high-risk population groups such as suspected cases toward COVID-19. Hence, this study aimed to assess the knowledge, attitude, and practice that inform efforts to combat COVID-19 among screened cases at Dessie Health Center.
Methods
Study Design, Area, and Period
A health-facility based cross-sectional study was conducted from September 1, to October 21, 2020 at Dessie health center, Dessie town, Northeastern Ethiopia. Dessie is located 401 km from Addis Ababa, the capital city of Ethiopia and the town has a total area of 15.08 km2 (5.82 square miles). Its geographical location is 11°8′ N latitude and 39°38′ E longitude with an elevation between 2400 and 3200 meters above sea level. In Dessie town, there are several health institutions (one referral hospital, one district hospital, eight health centers, three private general hospitals, five higher private clinics, and one public health institute). Dessie Health Center was founded in 1951 and currently there are around 81 staff working there. The health center is serving as sample collection and quarantine site of COVID-19. The health center is found near to one of the three COVID-19 testing locations in the east Amhara area.
Source and Study Populations
All individuals who visited Dessie Health Center for COVID-19 screening were the source population. Study participants who came to the health center to provide oropharyngeal specimen for COVID-19 testing during the study period were the study population.
Sample Size Determination and Sampling Technique
A single population proportion formula, n=[(Zα/2)2P(1-P)]/d2, was used to calculate the sample size. Until this study was conducted there were no published data about the knowledge, attitude, and practice toward COVID-19 among individuals who came to health facilities for COVID-19 screening in the study area. So a 50% proportion was used to get the maximum sample size by taking into account 95% confidence interval (Zα/2=1.96), marginal error (d) of 5%. In line with the above consideration, the minimum calculated sample size was 384. In order to recruit the study population we used simple random sampling technique. The number of people who came to Dessie Health Center for the sake of COVID-19 screening was fluctuating daily. Prior to the actual data collection time we checked the number of population flow at the health center for the screening purpose and we have determined the average number on a daily basis. For the purpose of the current study we have determined to take 10 study participants daily and each study participant was requested to provide response for the knowledge, attitude, practice (KAP) questions.
Data Collection
A structured interview-based questionnaire was used to obtain information of the study participants related to sociodemographic characteristics, awareness, and KAP toward COVID-19. The questionnaire assessing KAP toward COVID-19 was answered on a yes/no basis. The total knowledge score ranged from 0 to 11 using Bloom’s cutoff point, as good if the score was between 80 and 100% (7–11 points), and poor if the score was less than 80% (<7 points).18 In the same way, nine practice assessing questions were answered on a yes/no basis. If the score was between 80 and 100% (5–9 points) it would labeled as good. If the score was less than 80% (<5 points) it would labeled as poor. Attitude of participants toward COVID-19 was assessed by six questions. Data were collected under strict supervision of six BSc nurses working in the health center and three supervisors who hold MSc with specialty of microbiology and infectious diseases.
Quality Assurance
To generate quality and reliable data, the questioner was pretested on 20 study participants who are coming to Wollo University quarantine center who were having similar demographic characteristics. Based on the pretest feedback, necessary modifications of the questionnaire were carried out. The reliability of the knowledge, attitude, and practice questions were checked, data collectors were trained and there was regular supervision.
Statistical Analysis
Data were entered in to Microsoft Excel, exported to SPSS version 22 software (IBM Corporation, Armonk, NY, USA), and analyzed. Descriptive statistics were summarized in tables and graphs. Binary logistic regression was employed to show the association of each variable with the dependent variable. Moreover, a multivariable analysis was computed to identify factors that independently influence the occurrence of the dependent variable. Variables which show significance at P-value of 0.2 during bivariable analysis were selected for multivariable analysis. The level of significance was set to 0.05 (α=5%) with 95% confidence interval.
Results
Sociodemographic Characteristics
A total of 384 study participants were included in this study. The mean age of the study participants was 35.5 with ±13.0 standard deviation. Majority of study participants (61.5%) were males and about 52.6% of the study participants were aged between 30 and 49 years. Regarding residence of the study participants, most (85.2%) of them were living in urban areas. The majority of study participants had college and above educational achievement, and the majority of them did not have history of travel or contact with known or suspected cases of COVID-19 (Table 1).
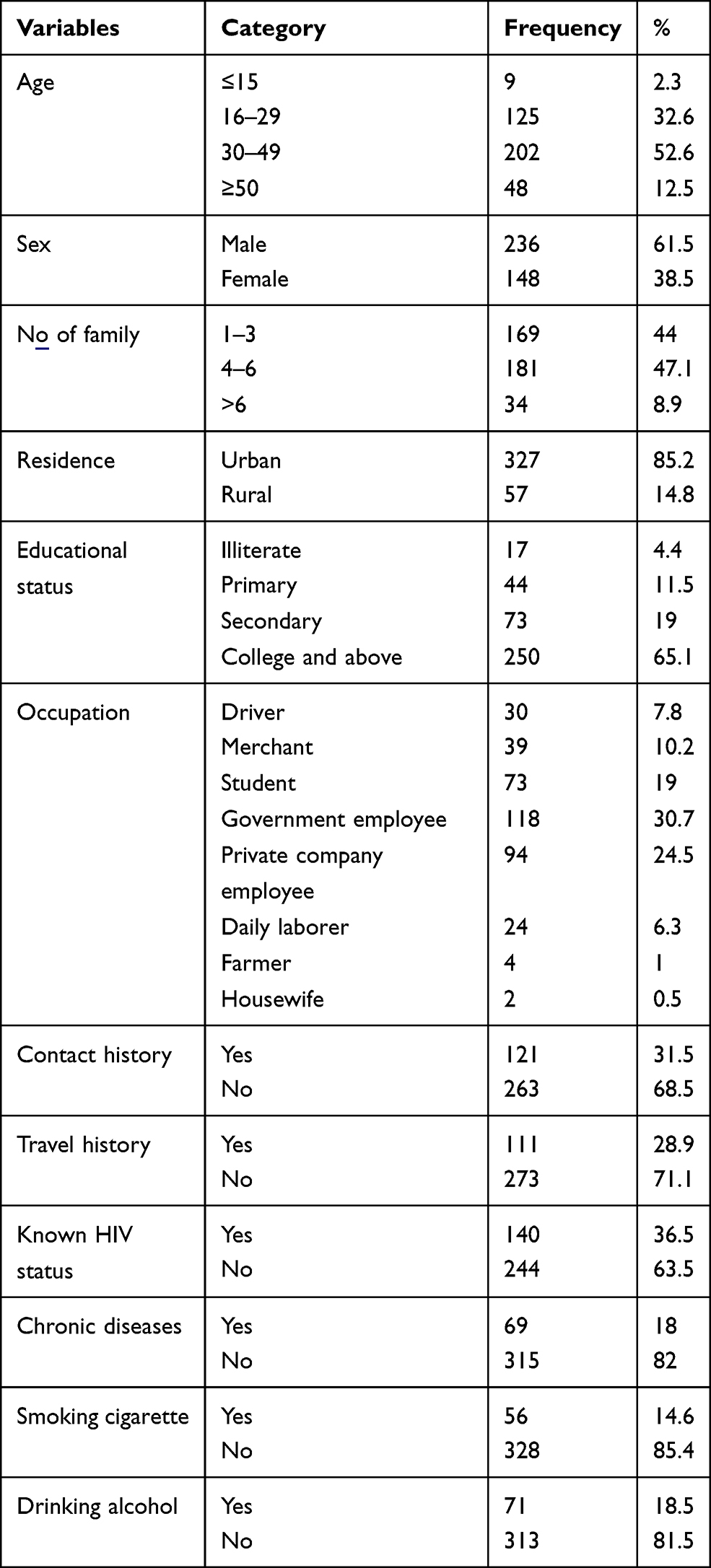 |
Table 1 Sociodemographic Characteristics of the Study Participants, Dessie, South Wollo Zone, Northeastern Ethiopia |
Awareness of the Study Participants on COVID-19
All patients (100%) had heard about the COVID-19 pandemic. The primary sources of information for the majority of study participants were television and radio (85.9%) whereas colleagues (15.6%) and academic training courses (4.7%) were found the least sources of information (Figure 1).
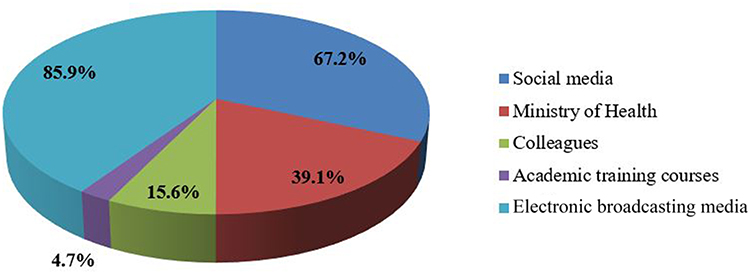 |
Figure 1 Primary source of knowledge about COVID-19 among the study participants. |
Knowledge of Study Participants on COVID-19
The magnitude of good and poor knowledge among the study participants was found to be 197 (51.3%) and 187 (48.7%), respectively. A high number of study participants had a poor knowledge about the major symptoms; fever, cough, sore throat, muscle pain, and difficulty of breathing, of COVID-19. Moreover, 311 (81.0%) of the participants were aware of the helpfulness of avoiding crowded places for the prevention and control of COVID-19. On the contrary, 317 (82.6) of the participants were not providing the correct response for the question about the possibility of transmission of the disease by asymptomatic persons (Table 2).
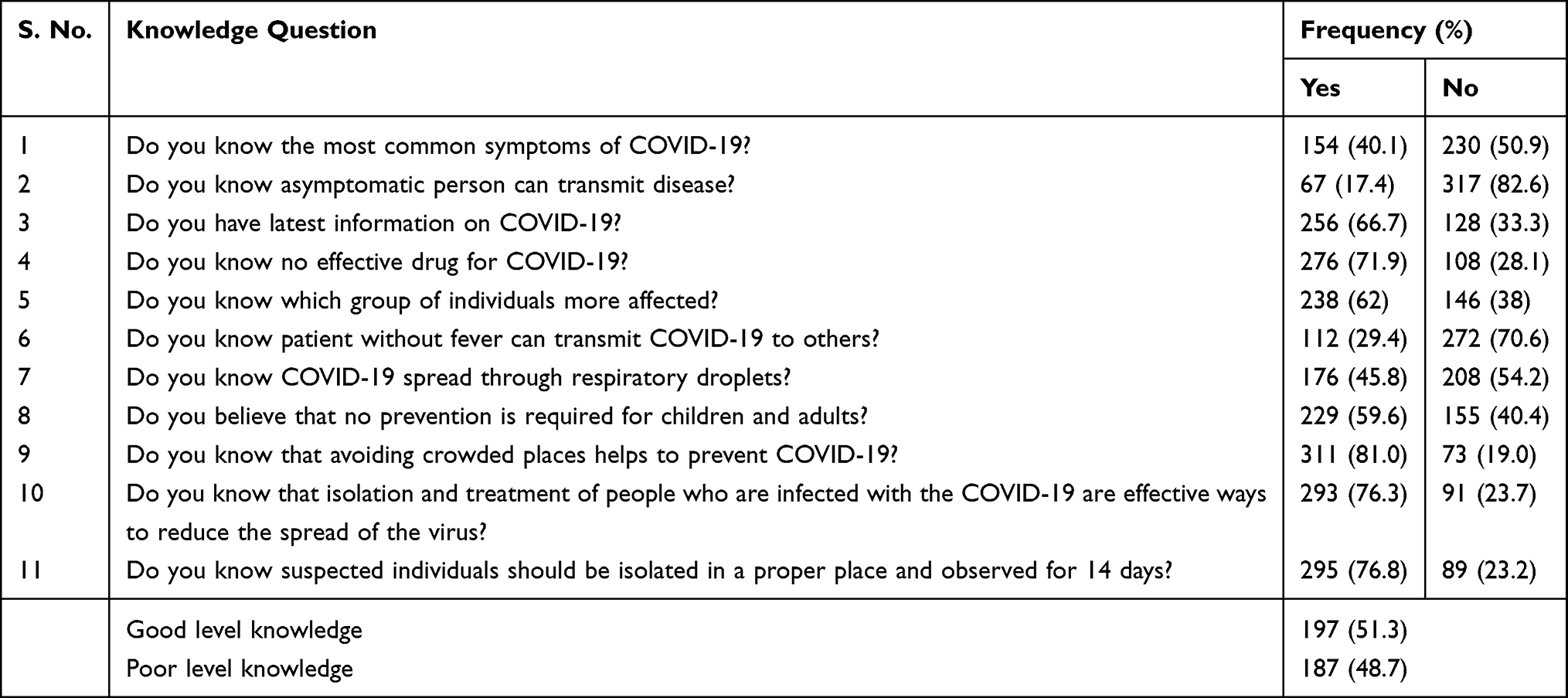 |
Table 2 Frequency of Responses by the Study Participants for Knowledge Questions |
Associated Factors of Poor Knowledge on COVID-19
Analysis of data using logistic regression model showed that educational status and contact history were significantly associated with poor knowledge at P<0.05. The odds of having poor knowledge among study participants who had no formal education (Illiterates) was 5.5 times higher than study participants who had college and above educational achievement (AOR= 5.53, 95%CI= 1.03-29.68, P= 0.046). Study participants who had secondary level educational achievement had 2.8 times the likelihood of having poor knowledge about COVID-19 (AOR= 2.79, 95%CI= 1.44-5.4, P= 0.002). The study participants who have no contact history had an inverse statistically significant association (AOR= 0.39, 95%CI= 0.21–0.73, P= 0.003) with having poor knowledge than those with contact history (Table 3).
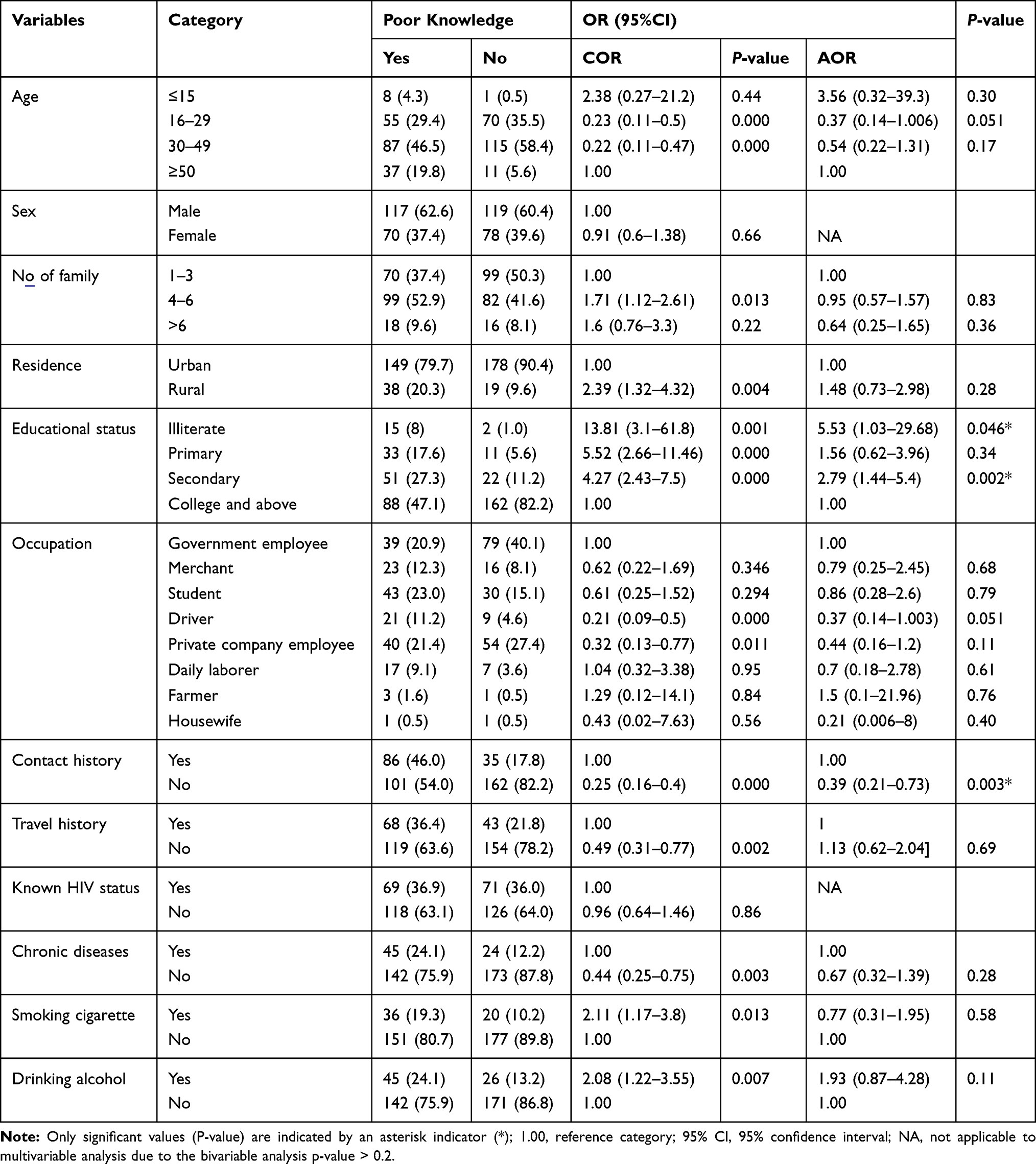 |
Table 3 Poor Knowledge and Associated Factors of Study Participants of Dessie, South Wollo Zone, Northeastern Ethiopia |
Attitude of the Study Participants Toward COVID-19 Prevention
As indicated in Table 4, majority of the study participants (71.9%) perceived that traditional medicines like eating garlic are not helpful to prevent infection with the new coronavirus. About 49.2% of the study participants perceived that COVID-19 cannot affect young people and high number of study participants will not go to a quarantine center if they develop the disease. The majority of study participants perceived that the measurements taken by Ethiopian Ministry of Health are helpful and the country can win the battle against COVID-19 (Table 4).
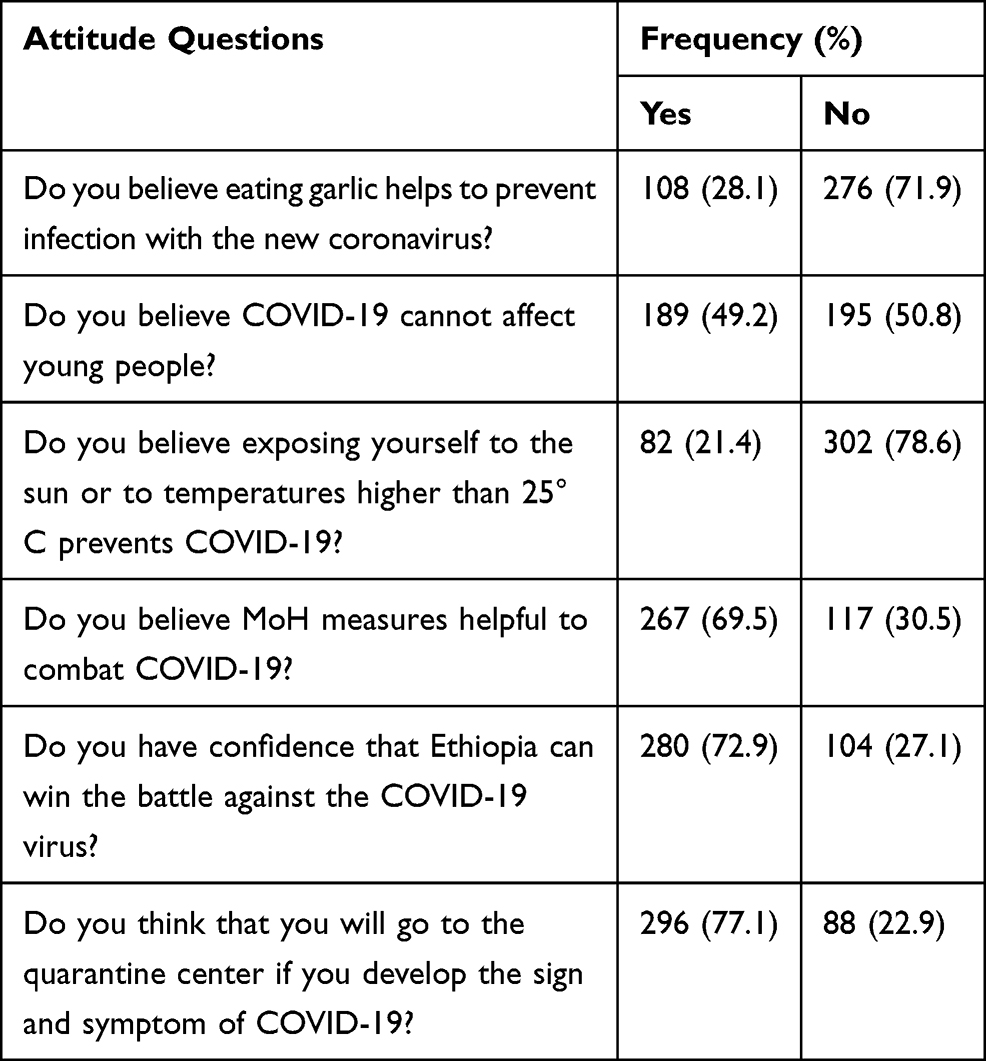 |
Table 4 Frequency of Response for Attitude Questions of Study Participants of Dessie, South Wollo Zone, Northeastern Ethiopia |
Practice of COVID-19 Prevention Among Study Participants
The magnitude or level of poor practice in the current study was found to be 41.7%. Two hundred and forty (62.5%) study participants reported that they went to crowded places. The majority (69.3%) of the respondents used a face mask when they leave their home but the number of study participants who did not use a face mask is also higher. The other less frequently practiced preventive measures (10.4%) were avoiding recontamination after hand washing from pipe or any other water container materials and practicing physical distancing (45.1%). About 55% of study participants did not keep the recommended distance when they speak in front of others (Table 5).
 |
Table 5 Frequency of Response for Practice Questions, of Study Participants of Dessie, South Wollo Zone, Northeastern Ethiopia |
Associated Factors of Poor Practice on COVID-19 Prevention
Statistical analysis between dependent variable (poor practice) and independent variables (all sociodemographic characteristics and possible associated factors) were performed. It was revealed that significant association existed between poor practice toward COVID-19 prevention and control measures and parameters which address educational status, travel history, and poor knowledge of study participants. The odds of poor practice in participants who had no travel history was 2.37 times (AOR=2.37, 95%CI=1.3–4.32, P=0.005) higher than those participants who had contact with confirmed cases. Study participants who had no formal education (illiterates) had five times AOR=5.12, 95%CI=1.33–19.7, P=0.02) the likelihood of having poor practice toward control and prevention of COVID-19. Study participants who had poor knowledge showed more than two time higher odds of having poor practice (AOR= 2.14, 95%CI= 1.32-3.47, P= 0.002) (Table 6).
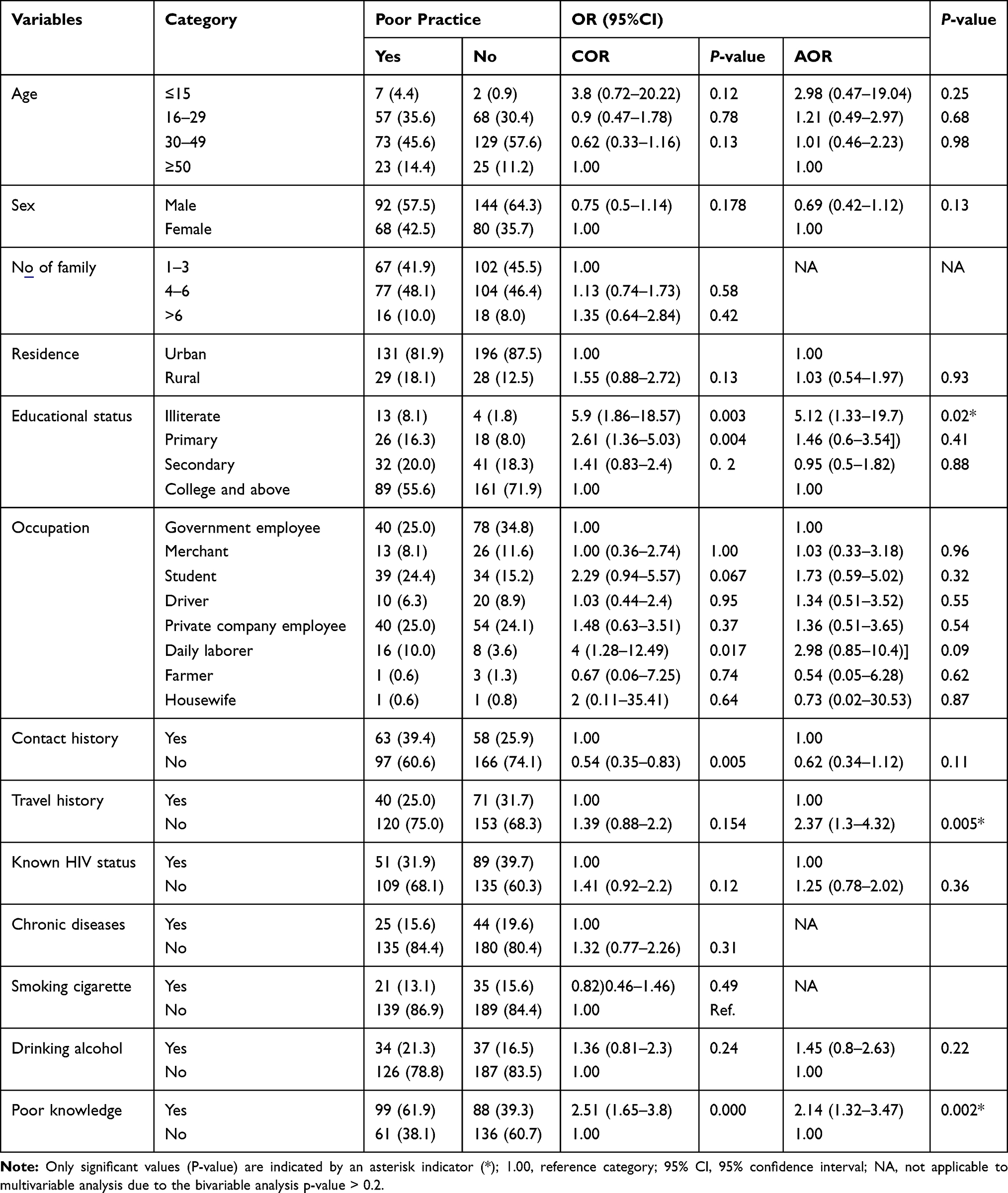 |
Table 6 Factors Associated with Poor Practice for Study Participants of Dessie, South Wollo Region of Ethiopia |
Discussion
The current worldwide spread of the coronavirus pandemic is a major threat to human beings irrespective of race, economy, and geographical location. The pandemic affects nearly all countries in the world impacting the majority of human activities including the economy and health systems.19,20 Due to the fact that effective medication and vaccine are not still available particularly for African countries, prevention remains the only option to combat the virus. As a result, effective prevention and control of COVID-19 is attained through improving the knowledge, attitude and practice of high-risk population groups toward COVID-19.
According to results of the current study, awareness of study participants regarding COVID-19 was found to be high. Media such as television and radio serve as a major source of information (85.9%) for creating awareness regarding the pandemic. This proportion regarding source of information toward COVID-19 in the present study is higher than another study conducted in Ethiopia.18 This high awareness of study participants has its roots partly in their high exposure to the information provided by the government and media about the virus since the start of the outbreak.
In this study, more than half (51.3%) of the study participants had good knowledge regarding the COVID-19 pandemic while the remaining 48.7% had poor knowledge about the disease. This finding is different from studies conducted in Iran and China,21,22 which reported a knowledge score of 85% and 90%, respectively. The possible reason for this discrepancy might be the fact that nearly all participants in these previous studies possess an academic degree or higher; and would actively grasp knowledge, respond actively to the severe condition of the pandemic and the overwhelming news reports, by collecting information from reliable sources such as official health related websites. Moreover, the magnitude of poor knowledge (48.7%) in this study was found to be higher than study reports from Kenya,23 USA,24 Bangladesh,25 and China,26 which is mainly attributed to differences in access for electricity and internet for accessing social media and other reliable source of information.
Our study further revealed that only 17.4% of the respondents knew the fact that an asymptomatic person can transmit the disease; which is attributable to obsessed information gaining habit in the country. Most of the population in Ethiopia is overwhelmed with repeated announcements and death news due to the pandemic; however, detailed information from the health and medical perspective is still inadequate and as a result most people have different viewpoints and perceptions toward the virus. This results in the community concentrating only on widely and repeatedly broadcast messages; for instance, the majority (81.0%) of the study participants believed that avoiding crowded places helps to prevent COVID-19. Moreover, the overload of information may have caused confusion and difficulty ascertaining correct information. Such knowledge gaps will have their own severe outcomes. Mainly attributable to the information gap for the public, about 59.6% of the respondents believed no prevention strategy is required for children and adults.
In the present research work it was indicated that study participant’s age and gender did not show statistically significant association with poor knowledge. A similar study conducted in Malaysia showed that the younger population were associated with good knowledge27 and a study in Cameroon indicated the presence of statistically significant association of gender with knowledge on transmission of the disease.28 Another study finding from Bangladesh25 reported that young individuals had more knowledge than the older counterparts. In the same scenario a study from Addis Zemen, Ethiopia18 and USA,29 revealed that an increase in age was associated with poor knowledge.
On the other hand, those with low educational status had statistically significant association with poor COVID-19 knowledge. In reference to college and above, study participants who had no educational level (Illiterate) had 5.5 times the likelihood of having poor knowledge and this is in line with a study conducted in Addis Zemen, Ethiopia.18 Moreover, in the present study, not having contact history with those diagnosed with the virus is significantly associated with having poor COVID-19 knowledge (AOR=0.39, 95%CI=0.21–0.73, P=0.003) meaning respondents who have not come into contact with confirmed COVID-19 cases pertain poor knowledge regarding the virus.
Only 40.1% of the study participants knew the main clinical symptoms of COVID-19 such as fever, cough, sore throat, muscle pain, and difficulty in breathing. This finding is low compared to a study from the Philippines in which 89.5% of respondents knew about the main clinical symptoms and transmission routes.30 Moreover, about 29.4% of the respondents believed that COVID-19 would not be transmitted if people did not have a fever. This further reflects the ineffectiveness of social media in the creation of awareness about COVID-19 pandemic within the Ethiopian population; for instance, some media platforms often exaggerate the risk associated with COVID-19 pandemic and often associate the disease with only fever.
In this study, the attitude of the study participants seems skewed. Almost half of the respondents (49.2%) believed COVID-19 cannot affect young people. This is mainly due to misinformation in the community. Mainly attributable to high dependence and certainty in scientifically unproven traditional medicine, more than a quarter of participants in this study reported that eating garlic and exposing oneself to the sun or to temperatures higher than 25°C helps to prevent infection with the new coronavirus. In the present study, the majority (69.5%) believed sticking to MoH measures is helpful to combat COVID-19. This finding is in line with reports from Nigeria31 and Saudi Arabia.32
The majority of the respondents (72.9%) have confidence that Ethiopia can win the battle against COVID-19. This finding is in line with KAP study reports from China, Malaysia, Bangladesh, and India,22,25,27,33 which reported high levels of positive attitudes towards combating the pandemic. The authors in these previous studies attributed the positive attitudes to the drastic measures taken by their governments (such as traffic limits and the lockdown of cities and counties) in mitigating the spread of the virus. However, the positive attitude reported in our study is not a result of justifiable reasoning rather it is a result of believing that Africans are resistant to the disease and partly from religious perspectives. On the contrary, a study report from Egypt revealed that the majority (88.3%) of respondents were pessimistic and were afraid the country would not win the battle against the pandemic due to the poor quality of most of Egyptian hospitals.34
In this study, the extent of poor practice regarding COVID-19 prevention was 41.7% which is a relatively large figure. Overall, participants in this study reported partially adopting the practices recommended to limit the spread of COVID-19. The majority of the participants reported wearing a mask when outside the home, and washing their hands for at least 20 seconds with soap or using hand sanitizer continuously according to WHO recommendations and covering nose and mouth with hand or tissue while sneezing or coughing. However, most of the respondents testified that they were not avoiding crowded places, touching mouth, nose and eyes frequently, greeting relatives and were not maintaining the recommended two meter-distance from other people. This finding is in line with previous reports from Jimma, Ethiopia,35 and Jordan.36
Illiterate people, individuals not having contact and travel histories, and those having an alcohol drinking habit as well as poor knowledge level were found to have a statistically significant association with poor practice toward COVID-19 prevention. Illiterate study participants showed 5.12 times (AOR=5.12, 95%CI=1.33–19.7)) poor practices in comparison with study participants who had achieved college and above educational level.
Conclusion
The magnitude of study population’s knowledge, attitude and preventive practices such as proper hand washing, avoidance of handshaking, and physical distancing were modest to protect themselves from this highly contagious pandemic virus. Notably, there is alarmingly high poor knowledge, negatively skewed attitude, and poor practice regarding the COVID-19 pandemic, which needs urgent improvement. Low educational status and having contact with confirmed COVID-19 cases are significantly associated with poor knowledge whereas poor practice was found significantly associated with poor knowledge, low educational level and having travel history. Therefore, health education programs aimed to improve COVID-19 related knowledge, attitude and practice are urgently needed, especially for those who are illiterate, having travel and contact history, or generally among underprivileged populations. Further studies are needed which could use open-ended questions, in-depth interviews or focus group discussion for adequate assessment of attitudes and practices of the population toward COVID-19 and might add more insight into the biopsychological impact of COVID-19 in the country with poor economy and health infrastructure.
Limitation of the Study
For the prevention and control of COVID-19 pandemic knowledge, attitude, and practice of the people all over the world is highly important. Assessing the knowledge and practice of an individual once up on a time may not be a guarantee to conclude the people’s level of knowledge and practice is good or not good. So, future research in different study designs should be performed to monitor the population’s level of knowledge and practice in a continuous manner. Another limitation of the present study is that it did not include COVID-19 test results. It would help the readers to correlate the study participants' KAP assessment with their result.
Abbreviations
COVID-19, coronavirus disease 2019; KAP, knowledge, attitude, practice; COR, crude odds ratio; AOR, adjusted odds ratio.
Data Sharing Statement
There are no material outputs from this study, and all data are those presented in the manuscript.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from Institutional ethical and review committee, College of Medicine and Health Sciences, Wollo University. A permission letter was also obtained from the study site. The purpose and procedures of the study was explained to the study participants and to a parent/guardian. Besides, participants over the age of 18 provided informed consent and a parent or legal guardian provided written informed consent for participants under the age of 18 years. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge Wollo University and Dessie Health Center for their facility support during the whole research activity and to all study participants and Dessie Health Center staff members.
Author Contributions
All authors made significant contributions to the conception and design, involved in data collection, data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No external funds were obtained; only institutional support from Wollo University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cui J, Li F, Shi Z-L. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol. 2019;17(3):181–192. doi:10.1038/s41579-018-0118-9
2. Su S, Wong G, Shi W, et al. Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol. 2016;24(6):490–502. doi:10.1016/j.tim.2016.03.003
3. Drosten C, Günther S, Preiser W, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348(20):1967–1976. doi:10.1056/NEJMoa030747
4. Zaki AM, Van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 2012;367(19):1814–1820. doi:10.1056/NEJMoa1211721
5. Zhong N, Zheng B, Li Y, et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003. Lancet. 2003;362(9393):1353–1358. doi:10.1016/S0140-6736(03)14630-2
6. Hui DS, Azhar EI, Madani TA, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 2020;91:264–266. doi:10.1016/j.ijid.2020.01.009
7. Tan W, Zhao X, Ma X, et al. A novel coronavirus genome identified in a cluster of pneumonia cases—Wuhan, China 2019− 2020. China CDC Weekly. 2020;2(4):61–62. doi:10.46234/ccdcw2020.017
8. Yang W, Dang X, Wang Q, et al. Rapid detection of SARS-CoV-2 using reverse transcription RT-LAMP method. medRxiv. 2020.
9. World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV), Geneva, Switzerland, 30 January 2020.
10. Hopkins J. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE). Coronavirus Resource Center; 2020.
11. Vodičar PM, Valenčak AO, Zupan B, et al. Low prevalence of active COVID-19 in Slovenia: a nationwide population study of a probability-based sample. Clin Microbiol Infect. 2020.
12. Sahu KK, Mishra AK, Lal A, Sahu SA. India fights back: COVID-19 pandemic. Heart Lung. 2020;49(5):446–448. doi:10.1016/j.hrtlng.2020.04.014
13. Woolf SH, Chapman DA, Lee JH. COVID-19 as the leading cause of death in the United States. JAMA. 2020. doi:10.1001/jama.2020.24865
14. WHO. COVID W. 19: Situation Update for WHO African Region. World Health Organization; 2020:1–5.
15. Snoeck CJ, Vaillant M, Abdelrahman T, et al. Prevalence of SARS-CoV-2 infection in the Luxembourgish population: the CON-VINCE study. medRxiv. 2020.
16. Hellewell J, Abbott S, Gimma A, et al. Centre for the mathematical modelling of infectious diseases COVID-19 working group, feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob Health. 2020;8(4):e488–e96. doi:10.1016/S2214-109X(20)30074-7
17. Sahu KK, Mishra AK, Lal A. Trajectory of the COVID-19 pandemic: chasing a moving target. Ann Transl Med. 2020;8(11):11. doi:10.21037/atm-20-2793
18. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S258736
19. Ahmad T, Haroon MB, Hui J, Hui J. Coronavirus disease 2019 (COVID-19) pandemic and economic impact. Pak J Med Sci. 2020;36(COVID19–S4):S73. doi:10.12669/pjms.36.COVID19-S4.2638
20. Tandon A, Roubal T, McDonald L, et al. Economic Impact of COVID-19: Implications for Health Financing in Asia and Pacific. World Bank; 2020.
21. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ. 2020;30.
22. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745. doi:10.7150/ijbs.45221
23. Austrian K, Pinchoff J, Tidwell JB, et al. COVID-19 Related Knowledge, Attitudes, Practices and Needs of Households in Informal Settlements in Nairobi, Kenya. 2020.
24. Alobuia WM, Dalva-Baird NP, Forrester JD, Bendavid E, Bhattacharya J, Kebebew E. Racial disparities in knowledge, attitudes and practices related to COVID-19 in the USA. J Public Health (Bangkok). 2020;42(3):470–478. doi:10.1093/pubmed/fdaa069
25. Hossain MA, Jahid MIK, Hossain KMA, et al. Knowledge, attitudes, and fear of COVID-19 during the rapid rise period in Bangladesh. PLoS One. 2020;15(9):e0239646. doi:10.1371/journal.pone.0239646
26. Taghrir MH, Borazjani R, Shiraly R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Arch Iran Med. 2020;23(4):249–254. doi:10.34172/aim.2020.06
27. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E, Tu W-J. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
28. Adela N, Nkengazong L, Ambe LA, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. 2020;14(9):e0008700. doi:10.1371/journal.pntd.0008700
29. Wolf MS, Serper M, Opsasnick L, et al. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the US outbreak: a cross-sectional survey. Ann Intern Med. 2020;173(2):100–109. doi:10.7326/M20-1239
30. Lau LL, Hung N, Go DJ, et al. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: a cross-sectional study. J Glob Health. 2020;10(1). doi:10.7189/jogh.10.011007.
31. Reuben RC, Danladi MM, Saleh DA, Ejembi PE, Noonan D, Simmons LA. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. 2020;45(1):1–14. doi:10.1007/s10900-019-00710-0
32. Almofada SK, Alherbisch RJ, Almuhraj NA, et al. Knowledge, attitudes, and practices toward COVID-19 in a Saudi Arabian population: a cross-sectional study. Cureus. 2020;12(6). doi:10.7759/cureus.8905.
33. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
34. Kasemy ZA, Bahbah WA, Zewain SK, et al. Knowledge, attitude and practice toward COVID-19 among Egyptians. J Epidemiol Glob Health. 2020. doi:10.2991/jegh.k.200909.001
35. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A, Tu W-J. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
36. Alzoubi H, Alnawaiseh N, Al-Mnayyis A, Lubad M, Aqel A, Al-Shagahin H. COVID-19-knowledge, attitude and practice among medical and non-medical university students in Jordan. J Pure Appl Microbiol. 2020;14(1):17–24. doi:10.22207/JPAM.14.1.04
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.